
Nephrolithiasis - newbp.bmj.comnewbp.bmj.com/topics/en-us/225/pdf/225.pdfPrognosis 37 Guidelines 38...
49
Nephrolithiasis The right clinical information, right where it's needed Last updated: Sep 12, 2018
-
Upload
phungquynh -
Category
Documents
-
view
234 -
download
0
Transcript of Nephrolithiasis - newbp.bmj.comnewbp.bmj.com/topics/en-us/225/pdf/225.pdfPrognosis 37 Guidelines 38...

Nephrolithiasis
The right clinical information, right where it's needed
Last updated: Sep 12, 2018

Table of ContentsSummary 3
Basics 4
Definition 4
Epidemiology 4
Etiology 4
Pathophysiology 4
Classification 5
Prevention 6
Primary prevention 6
Secondary prevention 6
Diagnosis 8
Case history 8
Step-by-step diagnostic approach 8
Risk factors 10
History & examination factors 12
Diagnostic tests 13
Differential diagnosis 15
Treatment 18
Step-by-step treatment approach 18
Treatment details overview 22
Treatment options 24
Follow up 36
Recommendations 36
Complications 36
Prognosis 37
Guidelines 38
Diagnostic guidelines 38
Treatment guidelines 38
References 40
Disclaimer 48

Summary
◊ Common condition with a 7% to 10% lifetime risk for women and men, respectively.
◊ Patients typically present with acute renal colic, although some patients are asymptomatic.
◊ Multiple risk factors include chronic dehydration, diet, obesity, positive family history, specificmedications, and various metabolic abnormalities.
◊ Non-contrast computed tomography scan of the abdomen/pelvis is the imaging modality with thehighest sensitivity and specificity to diagnosis stones. Plain x-ray (KUB) and renal ultrasound can beutilized for diagnosis in some cases, such as a desire to reduce or eliminate radiation exposure.
◊ Treatment consists of both medical and surgical therapies.
◊ 24-hour urine tests are recommended for most stone formers to determine cause of stone formationand optimal treatment to help prevent future stone episodes.

Nephrolithiasis BasicsBA
SIC
S
DefinitionNephrolithiasis refers to the presence of crystalline stones (calculi) within the urinary system (kidneys andureter). Such renal stones are composed of varying amounts of crystalloid and organic matrix. Uretericstones almost always originate in the kidney but then pass down into the ureter.[1]
EpidemiologyThe lifetime prevalence of nephrolithiasis in the US is estimated to be between 5% and 12%, with theprobability of having a stone varying according to age, gender, race, and geographic location.[5] [6] [7]Nephrolithiasis typically affects adult men more commonly than adult women, with a male to female ratioof 2 or 3:1.[8] [9] [10] However, there is evidence that this difference in incidence between men and womenis narrowing.[11] In US men, the highest prevalence of nephrolithiasis is found in white men, followed byHispanic men, Asian men, and black men.[9] Among US women, the prevalence is highest among whitewomen but lowest among Asian women.[12] However, the rate of stone incidence is increasing at a fasterrate for black people compared to white, and particularly for black women compared to men.[13] Historically,stone occurrence was relatively uncommon before age 20 years but the incidence of stones in childrenand adolescents is rising.[13] In adults, stone incidence peaks in the fourth to sixth decades of life.[14]Nephrolithiasis has a higher prevalence in hot, arid, or dry climates, such as the mountains, desert, ortropical areas. Worldwide, regions of high stone prevalence include the US, British Isles, Scandinavian andMediterranean countries, northern India and Pakistan, northern Australia, central Europe, portions of theMalay peninsula, and China.[15] [16] Heat exposure and dehydration are risk factors for nephrolithiasis. Theprevalence and incident risk of nephrolithiasis are directly correlated with weight and BMI in both genders,although the magnitude of this association is greater in women than in men.[17] [18]
EtiologyRenal stones are crystalline mineral depositions that form from microscopic crystals in the loop of Henle,distal tubules, or the collecting duct. This is usually in response to elevated levels of urinary solutes,such as calcium, uric acid, oxalate, and sodium, as well as decreased levels of stone inhibitors, such ascitrate and magnesium. Low urinary volume and abnormally low or high urinary pH also contribute to thisprocess. All of these can lead to urine supersaturation with stone-forming salts and subsequent stoneformation.[19] Supersaturation depends on urine pH, ionic strength, solute concentration, and solutechemical interaction. The higher the concentration of 2 ions, the more likely they are to precipitate out ofsolution and form crystals. As ion concentrations increase, their activity product reaches the solubility product(Ksp). Concentrations above this point can initiate crystal growth.[1] Once crystals are formed, they eitherpass out with the urine or become retained in the kidney, where they can grow and stones can form. In urine,even when the concentration of calcium oxalate exceeds the solubility product, crystallization may not occurbecause of prevention from urinary inhibitors. Both urinary calcium and oxalate are important and equalcontributors to calcium oxalate stone formation.[20] Several factors increase calcium oxalate supersaturationin urine. These include low urine volume and low citrate, and increased calcium, oxalate, and uric acid.[20]
PathophysiologyThere are differing theories as to the exact pathophysiology of stone formation. Free and fixed particletheories of stone formation are still being debated. Therefore, it is not known whether stones form by
4 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis Basics
deposition of microscopic crystals in the loop of Henle, distal tubules, or the collecting duct. In one study,renal papillary plaques were examined in idiopathic calcium oxalate stone formers.[21] Plaques werecomposed of calcium phosphate/apatite deposits, localized to the basement membrane of the thin loopof Henle and extending into the papillary interstitium. Once these plaques form, they erode through theurothelium and constitute a stable, anchored surface on which calcium oxalate crystals can nucleate andgrow as attached stones. Plaque lesions though reached the basement membrane of collecting ducts, butdid not affect the ductal cells. The papillary surfaces of nonstone formers did not show any plaques. Inthe same study papillary areas of patients with stones due to obesity-related bypass procedures did nothave such plaques, but instead had intratubular hydroxyapatite crystals in collecting ducts, with dilation anddamage to lining cells proximal to obstruction,[21] hence indicating that stone formation is a heterogeneousprocess.
Renal colic from nephrolithiasis is secondary to obstruction of the collecting system by the stone. Thestretching of the collecting system or ureter is due to an increase in intraluminal pressure. This causes nerveendings to stretch and therefore the sensation of renal colic.[1] Pain from urinary calculi can also be due tolocal inflammatory mediators, edema, hyperperistalsis, and mucosal irritation.[1]
ClassificationChemical composition of renal calculiThere is no formal classification system for renal stones, but they can be classified by composition. Forpatients with recurrent nephrolithiasis, 24-hour urine measurements allow risk factors to be identified andcorrected, which may direct ongoing medical management. A working classification is:
• Calcium stones: 80% of renal calculi[2]• Calcium oxalate: 80% of all calcium stones; risk factors include low urine volume, hypercalciuria,
hyperuricosuria, hyperoxaluria, and hypocitraturia• Calcium phosphate (hydroxy apatite or brushite): 20% of all calcium stones; risk factors include low
urine volume, hypercalciuria, hypocitraturia, high urine pH, and associated conditions include primaryhyperparathyroidism and renal tubular acidosis
• Uric acid stones: 10% to 20% of renal calculi; most commonly due to urinary pH <5.5, althoughhyperuricosuria can also contribute[3]
• Cystine stones: 1% of renal calculi; caused by an inborn error of metabolism, cystinuria, an autosomal-recessive disorder that results in abnormal renal tubular reabsorption of the amino acids cystine,ornithine, lysine, and arginine[2]
• Struvite stones: 1% to 5% of renal calculi, also known as infection stones; composed of magnesium,ammonium, and phosphate. They frequently present as staghorn calculi and may be associated withurea-splitting organisms, such as Proteus , Pseudomonas, and Klebsiella species. E coli is not aurease-producing organism.[4]
BAS
ICS
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
5

Nephrolithiasis PreventionPR
EVEN
TIO
N
Primary preventionThe most important primary prevention measure to help prevent nephrolithiasis is adequate hydration. Fluidintake should be at least 2 to 3 liters per day. Dietary factors are also important. Measures should includedecreasing dietary fat, protein, and sodium intake.[1]
Secondary preventionLong-term dietary modification is essential for preventing future calculi. Aim should be to obtain a 24-hoururine volume of at least 2 liters. Orange juice is able to bring the urinary citrate levels up much more thanlemon juice because of its high potassium content.
Diet should be balanced with contributions from all food groups, without excesses of any kind.[38]
• Fruits, vegetables, and fibers: fruit and vegetable intake should be encouraged because of thebeneficial effects of fiber. The alkaline content of a vegetarian diet also gives rise to a desirableincrease in urinary pH.
• An excessive intake of oxalate-rich products should be limited or avoided to prevent an oxalate load.This includes fruit and vegetables rich in oxalate such as wheat bran. This is particularly important inpatients in whom a high oxalate excretion has been demonstrated. The following products have a highcontent of oxalate:
• Rhubarb, 530 mg oxalate/100 g• Spinach, 570 mg oxalate/100 g• Cocoa, 625 mg oxalate/100 g• Tea leaves, 375 to 1450 mg oxalate/100 g• Nuts, 200 to 600 mg oxalate/100 g• Vitamin C is a precursor of oxalate, taking more than 500 to 1000 mg/day is not recommended.
• Animal protein should be limited to 0.8 to 1 g/kg body weight. An excessive consumption of animalprotein may give rise to hypercalciuria, hypocitraturia, low pH, hyperoxaluria, and hyperuricosuria.
• Calcium intake should not be restricted unless there are very strong reasons because of the inverserelationship between dietary calcium and calcium stone formation. The minimum daily requirementfor calcium is 800 mg and the general recommendation is 1000 mg/day (refers to elemental calcium).Calcium supplements are not recommended except in cases of enteric hyperoxaluria.
• A high consumption of sodium causes hypercalciuria by reduced proximal tubular reabsorption ofcalcium. Urinary citrate is reduced. The risk of forming sodium urate crystals is increased and theeffect of thiazide in reducing urinary calcium is counteracted by a high sodium intake. The daily sodiumintake should not exceed 3 g.
• The intake of food particularly rich in urate should be restricted in patients with hyperuricosuric calciumoxalate stone disease, as well as in patients with uric acid stone disease. The intake of urate shouldnot exceed 500 mg/day. Examples of food rich in urate include:
• Calf thymus, 900 mg urate/100 g• Liver, 260 to 360 mg urate/100 g• Kidneys, 210 to 255 mg urate/100 g• Poultry skin, 300 mg urate/100 g• Herring with skin, sardines, anchovies, sprats, 260 to 500 mg urate/100 g.
6 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis PreventionWhere specific metabolic abnormalities exist and are not responsive to dietary modification, specificpreventive therapies may be required.[46] These include:
• Uric acid stones: urinary alkalinization with potassium citrate or sodium bicarbonate• Hyperuricosuria, recurrent calcium oxalate stones, and normal urine calcium: allopurinol or febuxostat
• An increased risk of death has been reported with febuxostat compared to allopurinol.[92]Febuxostat should only be prescribed for patients who can not tolerate allopurinol or wheretreatment with allopurinol has failed, and who have been counselled regarding cardiovascularrisk[91]
• Hypercalciuria and recurrent calcium stones: thiazide diuretic with or without potassiumsupplementation (potassium citrate or potassium chloride)
• Hypocitraturia and recurrent calcium stones: urinary alkalinization (e.g., potassium citrate; sodiumbicarbonate or sodium citrate can be considered if the patient is at risk for hyperkalemia)
• Hyperoxaluria: oxalate chelator (e.g., calcium, magnesium, or cholestyramine), potassium citrate,pyridoxine
• Cystinuria: urinary alkalinization with potassium citrate, thiol binding agent (e.g., tiopronin which istolerated better than d-penicillamine)
• Struvite stones: urease inhibitor (e.g., acetohydroxamic acid), which is best reserved for complex/recurrent struvite stones in which surgical management has been exhausted. Secondary caresupervision should be employed as it can produce severe adverse effects such as phlebitis andhypercoagulability.
PREVEN
TION
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
7

Nephrolithiasis DiagnosisD
IAG
NO
SIS
Case historyCase history #1A 45-year-old man presents to the emergency department with a 1-hour history of sudden onset of left-sided flank pain radiating down toward his groin. The patient is writhing in pain, which is unrelieved byposition. He also complains of nausea and vomiting.
Other presentationsMany patients with nephrolithiasis are actually asymptomatic, as their stone may be in the kidney andnonobstructing. In these patients, diagnosis may be made following imaging (CT scan, abdominal x-ray,renal ultrasound, etc.) for other reasons. In contrast, other patients may present with gross hematuria,evidence of an obstructive uropathy or sepsis with fever, tachycardia, and hypotension.
Step-by-step diagnostic approachA diagnosis of nephrolithiasis may be suspected based on the clinical history, physical exam findings, andlaboratory test results, and is confirmed with imaging studies.
Clinical historyObstructed renal and ureteric stones can cause renal colic: severe, acute flank pain that may radiateto the ipsilateral groin, commonly associated with nausea and vomiting. Rarely, this is accompanied bymacroscopic hematuria. As stones pass and get lodged in the distal ureter or intramural tunnel, this canlead to bladder irritation manifested as urinary frequency or urgency. Ipsilateral testicular and groin painmay occur rarely in men with obstructive stones. However, in the absence of obstruction, calculi may beasymptomatic.
Physical examIn patients with renal colic, costovertebral angle and ipsilateral flank tenderness may be pronounced.Signs of sepsis, including fever, tachycardia, and hypotension, might indicate an obstructing stone withinfection, warranting urgent urology referral.
Laboratory testsInitial laboratory tests in all patients with suspected nephrolithiasis are urinalysis, CBC, and serumchemistry to include electrolytes, BUN/creatinine (to assess renal function), calcium, phosphorus, and uricacid. Urinalysis is helpful in confirming a diagnosis of renal stones as microscopic hematuria is presentin the majority of patients. However, the absence of hematuria does not exclude nephrolithiasis.[22]Presence of more than 5 to 10 WBCs per high-powered field in urine or pyuria could indicate presenceof urinary tract infection or be secondary to inflammation. Urinary crystals of calcium oxalate, uric acid,or cystine may indicate the nature of the calculus, although only cystine crystals are pathognomonic forthe underlying type of stones. A urine pH greater than 7 suggests presence of urea-splitting organisms,such as Proteus , Pseudomonas , or Klebsiella species, and struvite stones. A urine pH less than 5.5suggests uric acid stones.
8 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
Nephrolithiasis Diagnosis
An elevated WBC count may indicate infection (pyelonephritis or urinary tract infection). Hypercalcemiamay suggest hyperparathyroidism as an underlying etiology; hyperuricemia may indicate gout. In womenof childbearing age, a pregnancy test should be done prior to imaging with ionizing radiation and to ruleout ectopic pregnancy as a cause of symptoms.
Twenty-four-hour urine sampling is not always necessary in a first-time stone former without significantrisk for recurrence. However, it is indicated in recurrent stone formers; those with bilateral or multiplestones, history of inflammatory bowel disease, chronic diarrhea, bowel surgery or malabsorption; thosewith primary hyperparathyroidism, gout or renal tubular acidosis, nephrocalcinosis or stones formedof cystine, uric acid or calcium phosphate; in children; and in interested first-time stone-formers. Basicmeasurements should include volume, pH, creatinine, calcium, sodium, oxalate, uric acid, and citrate.Analysis of stone composition provides information on chemical composition and etiology. Stones areanalyzed after they are extracted during surgery or when patients expel and collect them for analysis.A urine screen for cystine, if the diagnosis of cystinuria is not excluded by stone analysis, should beconsidered. Serum parathyroid hormone is only measured in cases of high or high-normal serum calciumresults.
ImagingIf there is suspicion for nephrolithiasis based on the history, physical exam, and laboratory tests, thenimaging is indicated.
Noncontrast helical computed tomography (NCCT) scan is the preferred imaging modality due to its highsensitivity and specificity. Computed tomography (CT) accurately determines presence, size, and locationof stones; if it is negative, nephrolithiasis can be ruled out with high likelihood. A low-dose noncontrastCT (<4 mSv) is preferred for patients with a body mass index (BMI) ≤30 kg/m², as this limits the potentialradiation exposure while maintaining both sensitivity and specificity at 90% or higher.[32] However, low-dose CT is not recommended for those with a BMI >30 kg/m², owing to lower sensitivity and specificity inthese patients. Patients with indinavir and ritonavir stones from anti-HIV medication may have radiolucentstones on CT scan. However, this makes up only a tiny fraction of patients. CT scans are also used whenpatients with known stones have new onset of renal colic because stones commonly change location ornew ones are formed. However, there is a risk of significant radiation exposure with repeated CT scans,and a physician should use his or her judgment.
Plain abdominal radiography (KUB) can determine whether stones are radiopaque and can be usedto monitor disease activity. Calcium oxalate and calcium phosphate stones are radiopaque, whereaspure uric acid and indinavir stones are radiolucent and cystine stones are partially radiolucent. The KUBradiograph can suggest the fluoroscopic appearance of a stone, which determines whether it can betargeted with extracorporeal shock wave lithotripsy (ESWL).
Renal ultrasound can be used to diagnose renal stones, particularly in pregnancy or other situationswhere avoiding radiation exposure is advised, although it can be operator dependent and has lowsensitivity for diagnosing mid and distal ureteric stones. The combination of renal ultrasonography withKUB has been proposed as a reasonable initial evaluation protocol when a CT scan cannot be performedor is unavailable. For a known stone-former who has previously had radiopaque stones, it has beensuggested that a combination of renal ultrasonography and KUB are a viable option for follow-up imaging;sensitivities of 58% to 100% and specificities of 37% to 100% have been reported for this combination ofmodalities.[33] [34] [35]
DIAG
NO
SIS
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
9

Nephrolithiasis DiagnosisD
IAG
NO
SIS
Renal ultrasound and CT have been investigated for their safety and efficacy as an initial diagnostic testfor patients who present to the emergency department with suspected nephrolithiasis. The results of alarge, multicenter study showed no significant difference in high-risk diagnoses, serious adverse events,subsequent emergency room visits, or hospitalizations in those undergoing CT or renal ultrasound in thissetting. However, some patients who had an ultrasound did go on to need CT imaging, but it is not clearfrom this study what factors predicted the need for CT. Further study in this regard would help determinein which patients to use renal ultrasound as an initial diagnostic tool.[36]
An intravenous pyelogram (IVP) can provide both anatomic and functional information on stones and theurinary tract and, before NCCT, was the traditional imaging modality. However, IVP is now less commonlyused due to the improved sensitivity of CT scans. Disadvantages include the need for intravenouscontrast material, which may provoke an allergic response or renal failure, and the need for multipledelayed films in certain cases and concerns for radiation exposure.
Renal ultrasound is the first-line imaging modality for pregnant patients. For pregnant patients whenrenal ultrasound is nondiagnostic, transvaginal ultrasound can assist with diagnosis by determining ifureteral dilation extends beyond the pelvic brim; it can also diagnose stones in the distal ureter. Magneticresonance imaging (MRI), which confers no radiation to the patient, is a second-line imaging modalitybecause stones are not directly visible on MRI and only seen as a filling defect in the collecting system.Radiation doses of <50 mGy have not been associated with increased risk of fetal anomalies or loss;therefore, low-dose protocol CT (<4 mGy) can be used as a last-line option in pregnant women after thefirst trimester to aid in difficult-to-diagnose cases.[37] [38] [32]
Renal ultrasound should be the preferred modality for evaluating children because of radiation risks;however, low-dose CT should be considered if renal ultrasound is nondiagnostic.[38] [32]
Risk factorsStronghigh protein intake• A higher energy diet with more protein may be associated with a higher incidence of stones.[22]
This is secondary to the increased prevalence of hyperuricosuria, hypocitraturia, and hypercalciuriaassociated with this diet.
high salt intake• Higher sodium intake is associated with higher urinary sodium and calcium levels, and decreased
urinary citrate. This promotes calcium salt crystallization due to urinary saturation of monosodiumurate and calcium oxalate/calcium phosphate being increased. Salt excess can also can lead to boneloss, thereby worsening hypercalciuria.
white ancestry• In US men, the highest prevalence of nephrolithiasis is found in white men, followed by Hispanic men,
Asian men, and black men.[9] Among US women, the prevalence is highest among white women butlowest among Asian women.[12]
10 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis Diagnosis
male gender• Nephrolithiasis typically affects adult men more commonly than adult women, with a male to female
ratio of 2 or 3:1.[8] [9] [10] However, there is evidence that this difference in incidence between menand women is narrowing.[23]
dehydration• Fluid intake is very important and should be at least 2 to 3 liters per day.[22] In two large observational
studies, fluid intake was found to be inversely related to the risk of renal stone formation.[24] [25] Alow urine output can produce a higher concentration of urinary solutes, therefore leading to stoneformation.
obesity• Two large prospective cohort studies of men and women found that the prevalence and incident risk
of nephrolithiasis were directly correlated with higher weight and BMI in both genders, although themagnitude of the association was greater in women than in men.[24] [25]
• Evidence linking obesity with low urine pH and uric acid stones and an association with hypercalciuriacould account for an increased risk of uric acid and/or calcium stones in obese patients.[26]
crystalluria• Stone formers (especially calcium oxalate stones) frequently excrete more calcium oxalate crystals in
the urine. Increased urinary excretion of cystine, struvite, and uric acid crystals is also a risk factor forstone formation.[22]
Weakoccupational exposure to dehydration• Dehydration and heat exposure are risk factors for nephrolithiasis. Those exposed to high
temperatures demonstrate lower urine volumes and pH, higher uric acid levels, and higher urinespecific gravity, leading to higher urinary saturation of uric acid, as well as calcium oxalate. As a result,people exposed to dehydration and heat are at increased risk for forming stones.[26]
warm climate• Seasonal variation in nephrolithiasis is likely related to temperature because of fluid losses through
perspiration. It has been reported that the highest incidence of nephrolithiasis is in the summermonths - July through September - with the peak occurring within 1 to 2 months of maximal meantemperatures.[27] [28] [29]
• In the US, prevalence of nephrolithiasis in the southeastern states (“stone belt”) is nearly double that inother areas.
family history• A positive family history of nephrolithiasis is associated with an increased risk of forming stones.
A stone former is twice as likely as a non-stone former to have a first-degree relative with ahistory of stones. Patients with family history have a higher incidence of multiple stones and earlyrecurrence.[22]
DIAG
NO
SIS
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
11

Nephrolithiasis DiagnosisD
IAG
NO
SIS
precipitant medications• Medications that are associated with an increased risk of stone formation include calcium-containing
antacids, carbonic anhydrase inhibitors, sodium and calcium-containing medications, vitamin C, andvitamin D. Most of these medications lead to higher urinary levels of calcium, uric acid, sodium, oroxalate, in turn promoting stone formation. Other medications are poorly soluble with high urinaryexcretion, favoring direct crystallization and stone formation in urine. These include protease inhibitors(e.g., indinavir, atazanavir), ephedrine, guaifenesin, triamterene, and sulfadiazine.[30] Antibioticexposure (sulfas, cephalosporins, fluoroquinolones, nitrofurantoin, broad-spectrum penicillins) isassociated with an increased likelihood for nephrolithiasis, with the greatest odds for recent exposureand exposure at younger age.[31]
History & examination factorsKey diagnostic factorsacute, severe flank pain (common)• Classical renal colic is described as severe, acute flank pain that radiates to the ipsilateral groin.
However, cases may have no radiation and some stones are asymptomatic.
Other diagnostic factorsprevious episodes of nephrolithiasis (common)• More than 50% of patients with renal stones will have another episode within 10 years.[39] [40]
nausea and vomiting (common)• Commonly associated with acute episode.
urinary frequency/urgency (common)• As stones pass and get lodged in the distal ureter or intramural tunnel, this can lead to bladder
irritation manifested as urinary frequency or urgency.
hematuria (common)• Microscopic hematuria is present on urinalysis in up to 85% to 90% of cases of nephrolithiasis.[22]
Rarely, macroscopic hematuria can be present.
testicular pain (common)• As stones pass through the ureter, flank pain can radiate toward the groin and testicle, leading to
testicular pain.
obesity (common)• Increased incidence of renal stones is correlated with increased body mass index (BMI) for both sexes.
family history (uncommon)• May be positive for nephrolithiasis in first-degree relatives. If so, this could suggest an underlying
metabolic abnormality.
precipitant medications (uncommon)
12 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis Diagnosis
• Potential medications that can play a role in formation of renal stones include antacids, carbonicanhydrase inhibitors, sodium- and calcium-containing medications, vitamins C and D, and proteaseinhibitors.[30]
groin pain (uncommon)• As stones pass through the ureter, flank pain can radiate toward the groin.
fever (uncommon)• If also associated with urinary obstruction, urgent decompression is needed. May be a sign of struvite
stones, which most commonly occur in association with a urinary infection.
tachycardia (uncommon)• May indicate urosepsis.
hypotension (uncommon)• May indicate urosepsis.
costovertebral angle and ipsilateral flank tenderness (uncommon)• May be pronounced in acute renal colic.
Diagnostic tests1st test to order
Test Resulturinalysis
• Microhematuria is seen in the majority of patients with renal stones.may be normal; dipstickpositive for leukocytes,nitrates, blood;microscopic analysispositive for WBCs, RBCs,or bacteria
CBC and differential• An elevated WBC may suggest infection (pyelonephritis or urinary
tract infection).
variable
serum electrolytes, BUN, and creatinine• These include sodium, potassium, chloride, bicarbonate, creatinine,
BUN, calcium, uric acid, and phosphorus.• Hypercalcemia may suggest hyperparathyroidism as an underlying
etiology; hyperuricemia may indicate gout.
variable
urine pregnancy test• Prior to exposure to ionizing radiation.• To exclude ectopic pregnancy.
negative
DIAG
NO
SIS
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
13

Nephrolithiasis DiagnosisD
IAG
NO
SIS
Test Resultnoncontrast helical CT scan
• Noncontrast helical computed tomography scan (NCCT) is thepreferred imaging modality for nephrolithiasis due to its highsensitivity and specificity, and should be ordered as soon asnephrolithiasis is suspected.
• A low-dose scan (<4 mSv) is preferred for patients with a body massindex (BMI) ≤30 kg/m², as this imaging study limits the potentialradiation exposure while maintaining both sensitivity and specificityat 90% or higher. However, low-dose computed tomography (CT) isnot recommended for those with a BMI >30 kg/m², owing to lowersensitivity and specificity in these patients.[32] A size-adjusted,reduced-dose CT protocol has been shown to be 96% sensitive forthe detection of ureteral stones requiring intervention in all patients,regardless of BMI.[41]
• NCCT accurately determines presence, size, and location of stones;if negative, nephrolithiasis can be ruled out with high likelihood.
• Radiation doses of <50 mGy have not been associated withincreased risk of fetal anomalies or loss, therefore, low-dose protocolCT (<4 mGy) can be used as a last-line option in pregnant womenafter the first trimester to aid in difficult-to-diagnose cases.[37] [38][32]
calcification seen inrenal collecting system orureter; hydronephrosis;perinephric stranding(indicative ofinflammation or infection)
stone analysis• Provides information on chemical composition and etiology. Stones
are analyzed after they are extracted during surgery or when patientsexpel and collect them for analysis.
stone composition
Other tests to consider
Test Resultplain abdominal radiograph (KUB)
• Plain abdominal film could be ordered initially along with computedtomography (CT) scan to determine whether stone is radiolucent. Upto 85% of stones are visible on KUB, although uric acid stones areradiolucent.[42]
• A KUB x-ray should be performed if the stone is not visible on a CTscout, so that patients with stones identifiable on initial KUB x-ray orCT scout can be followed by KUB.[32]
• Before definitive surgical therapy, a KUB should be ordered in anasymptomatic patient to ensure that patient has not already passedthe stone.
calcification seen withinurinary tract
renal ultrasound• In pregnancy, renal ultrasound is the first-line imaging modality.
It should also be the modality of choice when there is a desire toreduce or eliminate radiation exposure, such as for evaluation ofchildren. Low-dose computed tomography (CT) can be considered inchildren if renal ultrasound is nondiagnostic.[32]
calcification seen withinurinary tract, along withdilation
14 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis Diagnosis
Test Resultintravenous pyelogram (IVP)
• This test has for the most part been replaced by the computedtomography (CT) scan (the new diagnostic standard) for theevaluation and diagnosis of renal stones; however, it is still useful toassess renal function and collecting system drainage.
calcification seen withinurinary tract or a fillingdefect seen when dyeis passing through thekidney and down theureter
24-hour urine monitoring• Helps in determining underlying metabolic cause or etiology for
nephrolithiasis. Should be ordered once the patient is stone free.• Basic measurements should include volume, pH, creatinine, sodium,
calcium, oxalate, uric acid, and citrate.• Patients with recurrent renal stones should have subsequent periodic
24-hour urine monitoring.
increased or decreasedvalues for urinaryelectrolytes; reducedurine volume
spot urine for cystine• A urine screen for cystine should be considered if the diagnosis of
cystinuria is not excluded by stone analysis.
cystinuria
Differential diagnosis
Condition Differentiating signs /symptoms
Differentiating tests
Acute appendicitis • Usually presents with rightlower quadrant pain, fever,and signs of peritonitis.
• Urinalysis is negative.• Noncontrast helical
computed tomography scan(NCCT) shows dilation ofappendix and absence ofrenal stones.
Ectopic pregnancy • Woman of childbearingage presents with missedmenstrual period, right lowerquadrant pain, or pelvic painwith some degree of vaginalbleeding or spotting. Cervicalmotion tenderness may bepresent on pelvic exam.
• Urine pregnancy test ispositive and serum hCGelevated.
• Ultrasound reveals presenceof mass in fallopian tubes.
Ovarian cyst • May present with lowerpelvic/abdominal discomfortand/or dyspareunia; may becyclical.
• Palpable mass on pelvicexam.
• Abdominal ultrasound showscystic adnexal lesion; freefluid in the peritoneum.
• NCCT shows absence ofrenal stones.
Diverticular disease • May present with left lowerquadrant pain or abdominalpain as opposed to flankpain.
• Technetium pertechnetatescan may showenhancement of diverticulumif gastric mucosa is present.
• NCCT shows absence ofrenal stones.
DIAG
NO
SIS
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
15

Nephrolithiasis DiagnosisD
IAG
NO
SIS
Condition Differentiating signs /symptoms
Differentiating tests
Bowel obstruction • Bowel obstruction patientspresent with abdominaldistension, vomiting, andconstipation.
• Abdominal x-ray may showvolvulus.
• NCCT shows collapsedbowel with proximal dilationand absence of renal stones.
Acute pancreatitis • History of gallstones oralcohol abuse.
• These patients typically haveepigastric pain that radiatesto the back, as opposed toflank pain.
• NCCT shows inflammation ofthe pancreas and absence ofrenal stones.
• The diagnosis of pancreatitiscan usually be distinguishedfrom renal stones on clinicalgrounds, but in rare casesit might be necessary tomeasure serum amylase andlipase, which are elevatedin pancreatitis and usuallynormal in stone disease.
Peptic ulcer disease • May or may not have ahistory of peptic ulcerdisease. Pain is abrupt,severe in intensity, and maybe localized to right lowerquadrant; often related toeating meals.
• Erect chest x-ray andabdominal x-ray may showfree air under the diaphragm.
• Endoscopy shows pepticulcer.
• NCCT shows absence ofrenal stones.
Gastroenteritis • These patients typically havediffuse abdominal pain andno flank pain. Vomiting isprominent and patient mayhave diarrhea.
• Stool specimen may bepositive for culture.
• NCCT shows absence ofrenal stones.
Abdominal aorticaneurysm
• Pain typically presents assudden onset of intermittentor continuous abdominalpain, radiating to the back;patient may collapse.
• Ultrasound/CT of theabdomen can show thepresence of abdominal aorticaneurysm.
Pyelonephritis • Patients may presentwith costovertebral angletenderness and urinarysymptoms of dysuria,frequency, and hesitancy;flank pain may radiate toback; fever, chills, fatiguemay be present.
• Positive urinalysis and/orurine culture.
Tubo-ovarian abscess • Patients typically presentwith acute lower abdominalpain, fevers, and vaginaldischarge.
• Pelvic ultrasound showsmultilocular adnexal masses.
• NCCT shows thick-walledrim-enhancing adnexalmasses in the absence ofrenal stones.
16 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis Diagnosis
Condition Differentiating signs /symptoms
Differentiating tests
Uteropelvic junctionobstruction
• Patients may presentwith intermittent flank orabdominal pain, often worseduring brisk diuresis.
• Renal ultrasound or NCCTshows hydronephrosiswithout a dilated ureter in theabsence of a renal stone.
Testicular torsion • Patients typically presentwith lower abdominal pain,scrotal pain (testicle),nausea, and/or vomiting.
• Ultrasound shows enlarged,heterogeneous testicle withdecreased or absent Dopplerflow.
• NCCT shows enlargededematous testicle inabsence of renal stones.
Ovarian torsion • Patients typically presentwith lower abdominal pain,nausea, and/or vomiting.
• Ultrasound shows enlarged,heterogeneous ovary withdecreased or absent Dopplerflow.
• NCCT shows enlargededematous ovary in absenceof renal stones.
Musculoskeletal back pain • Patient may present withunilateral or bilateral middleand/or lower back pain.
• Point tenderness uponmuscular palpation.
• NCCT is normal withabsence of renal stones.
Mesenteric ischemia • Patients typically presentwith acute periumbilicalabdominal pain with nauseaand vomiting.
• NCCT shows bowel wallthickening, intestinalpneumatosis, portal venousgas, with absence of renalstones.
Constipation • Patients typically presentwith left lower quadrant painand abdominal distension.
• NCCT shows excessivestool in colon or rectum inabsence of renal stones.
Cholecystitis or biliarycolic
• Patient may present withright upper quadrant and/orepigastric pain, fevers, andleukocystosis.
• Abdominal ultrasoundwill show gallstones withgallbladder wall thickening.
• NCCT shows gallstones,gallbladder wall edema, andhigh attenuation bile in theabsence of renal stones.
DIAG
NO
SIS
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
17

Nephrolithiasis TreatmentTR
EAT
MEN
T
Step-by-step treatment approachThe main goal of initial treatment for an acute stone event is symptomatic relief with hydration and analgesia/antiemetics as needed. If signs and symptoms of infection are present, and the patient has a stone in thekidney or ureter, immediate urologic consultation should be initiated as urinary tract infection in the settingof an obstructing stone is an emergency that requires antibiotics and renal decompression to decrease thechance of life-threatening septic shock.[49] If the patient has a stone present without signs and symptoms ofinfection, he or she can be managed conservatively with opioids and nonsteroidal anti-inflammatory drugs(NSAIDs). NSAIDs have been shown to offer effective pain relief from acute kidney stone related pain withfewer side effects than opioids and acetaminophen.[50] If the pain cannot be managed with conservativetherapy, then renal decompression or definitive stone treatment should be considered.[22] There is evidenceto support that medical expulsive therapy (MET), namely alpha-blockers, may increase ureteral stonepassage rate and decrease the time to stone passage, particularly in distal ureteral stones <10 mm insize.[51] However, if a 4- to 6-week trial of MET has been attempted without successful stone passage, thepatient should undergo definitive surgical management.
For patients at risk for, or with a history of recurrent stones, secondary preventive measures should betailored toward underlying metabolic factors that promote stone formation. For all such patients, dietarymodification with adequate hydration is an essential aspect of ongoing management.
Urgent consideration: obstruction and infectionPatients with urinary calculi along with fever and other signs or symptoms of infection need emergencyurologic consultation for drainage and intravenous antibiotics. Failure to perform rapid renaldecompression can perpetuate urosepsis and result in death. Drainage can be accomplished in twoways. A urologist can place a ureteric stent past the obstruction and achieve drainage. Alternatively, apercutaneous nephrostomy tube can be placed by interventional radiology.
Management of stones <10 mm and no complicationsAcute medical treatment for renal or ureteric colic includes conservative therapy, such as hydration,analgesia (intravenous pain relief with morphine or the NSAID ketorolac), and antiemetics.
Patients with newly diagnosed ureteric stones <10 mm without complicating factors (urosepsis, intractablepain and/or vomiting, impending acute renal failure, obstruction of a solitary or transplanted kidney, orbilateral obstruction) can be managed expectantly.[52] Many ureteric stones <10 mm pass spontaneously,with exact passage rate related to both stone size and location.[53]
MET using an alpha-blocker such as tamsulosin, alfuzosin, or silodosin may be of benefit in promotinglarger (but still <10 mm) distal ureteral stone passage; however, efficacy rates have been questioned.[54][55] [56] [57] [58] [59] [60] [61] These agents can cause ureteric relaxation of smooth muscle andantispasmodic activity of the ureter leading to stone passage.[62] Patients should be made aware thatprescribing alpha-blockers for this indication is considered an off-label use of these drugs. Additionally,tamsulosin has been associated with intraoperative floppy iris syndrome, therefore it should not beprescribed if a patient has planned cataract surgery.
If there is spontaneous passage of stones, most pass within 4 to 6 weeks. Surgical intervention isindicated in the presence of persistent obstruction, failure of stone progression, sepsis, or persistentor increasing colic. Such patients in general are followed up with periodic imaging, with either a KUB
18 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
Nephrolithiasis Treatment
and renal ultrasound or a noncontrast computed tomography (CT) abdomen and pelvis to monitor stoneposition and degree of hydronephrosis.
Management of stones ≥10 mm or smaller stones that fail to passwith METManagement can be affected by stone size, location, and composition, in addition to anatomic and clinicalfeatures. For larger stones (≥10 mm), and for smaller stones that remain despite conservative therapies,additional surgical treatment is necessary. Historically, open surgery was the only way to remove stones.However, with the development and success of endourology, a term used to describe less invasivesurgical techniques that involve closed manipulation of the urinary tract with scopes, open surgery is nowrarely performed.
Calculi between 10 mm and 20 mm are in general treated with extracorporeal shock wave lithotripsy(ESWL) or ureteroscopy as first-line therapy. However for ESWL, the results for lower pole stonesare inferior (55%) to upper and mid pole stones (71.8% and 76.5%, respectively).[63] Percutaneousnephrostolithotomy (PCNL) for calculi between 10 mm and 20 mm achieves better stone-free rates forlower pole stones than ESWL (73% versus 57%).[64] Similarly, cystine stones >15 to 20 mm and brushitestones respond poorly to ESWL.[65] Hence, patients with features predictive of poor outcome, obesity, ora body build not conducive to ESWL, may be advised alternatives such as PCNL or ureteroscopy, whichshow superior results.[66] Patients with stones >20 mm should primarily be treated with PCNL unlessspecific indications for an alternate procedure are present. While PCNL is the first-line therapy for largestones, ureteroscopy has been reported to achieve a mean stone-free rate as high as 93.7% (77.0% to96.7%) for stones >20 mm in size (mean 25 mm) with acceptable overall complication rates (10.1%).However, this requires an average of 1.6 procedures per patient.[67] [68]
For solitary renal calculi <10 mm, ESWL and ureteroscopy are both valid options. Ureteroscopy orPCNL can be utilized when ESWL fails, or in the presence of anatomic abnormalities or other specialcircumstances.[69]
• Extracorporeal shock wave lithotripsy (ESWL) is the least invasive method of definitive stonetreatment and is suitable for most patients with uncomplicated stone disease. In ESWL, shockwaves are generated by a source external to the patient's body and are then propagated intothe body and focused on a renal stone. The shock waves break stones by both compressiveand tensile forces. The stone fragments then pass out in the urine. Limitations to ESWL includestone size and location. ESWL has the potential benefit of being done under intravenoussedation/analgesia, without need for general anesthesia. Treatment with tamsulosin appearsto be effective in assisting stone clearance in patients with renal and ureteric calculi.[70] WhileESWL has been shown to have limited success with lower pole stones there is evidence tosuggest that ancillary maneuvers such as percussion, diuresis, and inversion increase stone-freerates.[71] Contraindications to ESWL treatment include pregnancy, severe skeletal malformations,severe obesity, aortic and/or renal artery aneurysms, uncontrolled hypertension, disorders of bloodcoagulation, and uncontrolled urinary tract infections.[72] [73]
• Ureteroscopy involves placing a small semi-rigid or flexible scope per urethra and into the ureterand/or kidney. Once the stone is visualized, it can be fragmented using a laser and/or grasped witha basket and removed. The procedure is more invasive than ESWL, but is generally thought to havea higher stone-free rate. General anesthesia is routinely used, and a ureteric stent may be placedat the end of the procedure.[74] The procedure can be safely performed in coagulopathic patientsusing a holmium laser.
TRE
ATMEN
T
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
19

Nephrolithiasis TreatmentTR
EAT
MEN
T
• For patients requiring stone removal, both ESWL and ureteroscopy are considered acceptablefirst-line surgical treatments for stones in the ureter.[52] [75] Ureteroscopic stone-free rates arebetter than ESWL rates for distal ureteric stones regardless of size and for proximal ureteric stones>10 mm.[76] [77] However, uroscopic removal has a higher complication rate and longer hospitalstay.[78] [79]
• Percutaneous antegrade ureteroscopy involves percutaneous antegrade removal of ureteric stones,and can be considered in select cases with very large (>15 mm) stones impacted in the upperureter or when retrograde access is not possible.[80] [81] [82]
• Percutaneous nephrostolithotomy (PCNL) is a minimally invasive form of treatment that is usuallyreserved for renal and proximal ureteric stones (i.e., in the lower pole) and those that are large(>20 mm), have failed therapy with ESWL and ureteroscopy, or are associated with complex renalanatomy.[83] Percutaneous access into the kidney is gained from the flank and then a large sheathis placed into the kidney. Once this is done, a nephroscope is used to help remove the stone. Forlarge stones, ultrasound lithotripsy is usually used to break and remove the stone. PCNL usuallyrequires a hospital stay and has more potential complications than either ESWL or ureteroscopy.In stones of 20 mm to 30 mm, ESWL is associated with poor stone-free rates (34%) comparedto those achieved with PCNL (90%). ESWL is further associated with an increased number ofprocedures and need for ancillary treatments as the stone size increases.[84]
• Laparoscopic stone removal is another minimally invasive method to remove ureteric or renalstones. However, it is still more invasive, requires a longer hospital stay, and has a much higherlearning curve than ureteroscopy or ESWL. With the advances in ESWL and endourologic surgery(i.e., ureteroscopy and PCNL) during the past 20 years, the indications for open stone surgeryhave markedly diminished. Laparoscopic or open surgical stone removal may still be indicatedin rare cases where ESWL, ureteroscopy, and percutaneous ureteroscopy fail or are unlikely tobe successful; anatomic deformities preclude a minimally invasive approach; the patient requiresconcomitant open surgery, pyeloplasty, or a partial nephrectomy; or in patients with a large stoneburden requiring a single clearance procedure.[52] [75]
Stones during pregnancyA symptomatic stone occurs in 1 out of every 200 to 1500 pregnancies with 80% to 90% of theseoccurring in the second or third trimester.[85] It has been reported that 48% to 80% of stones passspontaneously during pregnancy.[32] [86]
Pregnant women with renal colic that is not controlled with oral analgesia or with an obstructing stoneand signs of infection (fever or urinalysis/urine culture showing a possible urine infection) should receivea ureteric stent or percutaneous nephrostomy tube. Of note, these tubes should be changed moreoften (every 6 to 8 weeks) due to concern for rapid encrustation as a result of the metabolic changesseen with pregnancy. If the patient has no evidence of infection, definitive therapy with ureteroscopymay be performed and has been demonstrated to be safe.[87] ESWL and PCNL are contraindicated inpregnancy.
Ongoing medical therapy and dietary modificationOral alkalinization therapy with medications such as potassium citrate and sodium bicarbonate maybe beneficial in dissolving uric acid stones and preventing uric acid supersaturation. It may be used fortreating uric acid stones that do not require urgent surgical treatment, as well as asymptomatic stones.The ideal goal for alkalinization therapy for uric acid stones is to maintain the urine pH between 6.5 and7.0. Potassium citrate is the first-line therapy. In patients with CHF or renal failure, extra care should
20 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis Treatment
be taken when prescribing alkalinization therapy. Alkalinization therapy also plays an important role inpreventing calcium and cystine stones.
Long-term dietary modification is essential for preventing future calculi. This modification is centered onincreasing fluid intake. At least 2 liters of urine output daily should be recommended to help prevent futureepisodes of stone formation.[88]
Decreased dietary sodium, protein, and oxalate should be recommended for stone prevention. Increasedcitrus fruit intake is recommended to prevent stone recurrence.[89] Normal calcium intake (i.e., 1000mg/day to 1200 mg/day) is recommended.[89] Dietary calcium restriction can lead to less binding ofcalcium to oxalate in the GI tract, promoting hyperoxaluria and potentiating the risk for stone formation;furthermore, it could have detrimental effects on bone health.
Where specific metabolic abnormalities exist and are not responsive to dietary modification, specificpreventive therapies may be required.[46] [90] These include:
• Uric acid stones: urinary alkalinization with potassium citrate or sodium bicarbonate• Hyperuricosuria, recurrent calcium oxalate stones, and normal urine calcium: allopurinol or
febuxostat
• Febuxostat should only be prescribed for patients who can not tolerate allopurinol orwhere treatment with allopurinol has failed, and who have been counselled regardingcardiovascular risk[91]
• The double-blind Cardiovascular Safety of Febuxostat or Allopurinol in Patients withGout (CARES) safety trial found that cardiovascular death and all cause mortality weresignificantly more common among patients taking febuxostat than allopurinol (4.3% vs.3.2%, HR 1.34 [95% CI 1.03 to 1.73]; 7.8% vs. 6.4%, HR 1.22 [95% CI 1.01 to 1.47],respectively).[92] Treatment group did not differ with respect to a primary composite outcomeof cardiovascular events.
• Hypercalciuria and recurrent calcium stones: thiazide diuretic with or without potassiumsupplementation (potassium citrate or potassium chloride)
• Hypocitraturia and recurrent calcium stones: urinary alkalinization (e.g., potassium citrate; sodiumbicarbonate or sodium citrate can be considered if the patient is at risk for hyperkalemia)[93]
• Hyperoxaluria: oxalate chelator (e.g., calcium, magnesium, or cholestyramine), potassium citrate,pyridoxine
• Cystinuria: urinary alkalinization with potassium citrate, thiol binding agent (e.g., tiopronin which istolerated better than d-penicillamine)
• Struvite stones: urease inhibitor (e.g., acetohydroxamic acid), which is best reserved for complex/recurrent struvite stones in which surgical management has been exhausted. Secondary caresupervision should be employed as it can produce severe adverse effects such as phlebitis andhypercoagulability.
Most of these strategies are applied to children with nephrolithiasis, although there is a limited number ofwell-designed trials in this age group.[94] [95] TR
EATM
ENT
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
21

Nephrolithiasis TreatmentTR
EAT
MEN
T
Treatment details overviewPlease note that formulations/routes and doses may differ between drug names and brands, drugformularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
Initial ( summary )acute renal colic nonpregnant
1st conservative management (hydration, paincontrol, and antiemetics)
Acute ( summary )confirmed stone: no evidence ofobstruction nonpregnant
1st hydration, pain control, and antiemetics
demonstrated bacteriuria adjunct antibiotic therapy
adjunct surgical decompression
stones <10 mm adjunct medical expulsive therapy (MET)
stones ≥10 mm or failedmedical therapy
adjunct surgical removal
confirmed stone: with evidence ofobstruction nonpregnant
1st hydration, pain control, and antiemetics
plus surgical decompression
plus surgical removal
with infection plus antibiotic therapy
pregnant
1st specialist referral
Ongoing ( summary )following an acute episodenonpregnant
1st hydration and dietary modification
hyperuricosuria and/oruric acid stones
adjunct xanthine oxidase inhibitor ± alkalinizationtherapy
hypercalciuria adjunct diuretics/alkalinization
hypocitraturia adjunct alkalinization
hyperoxaluria adjunct oxalate chelator/alkalinization
22 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis Treatment
Ongoing ( summary )cystinuria adjunct alkalinization/thiol binding agent/cystine
chelator
struvite stones adjunct urease inhibitor
TRE
ATMEN
T
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
23

Nephrolithiasis TreatmentTR
EAT
MEN
T
Treatment optionsPlease note that formulations/routes and doses may differ between drug names and brands, drugformularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
Initialacute renal colic nonpregnant
1st conservative management (hydration, paincontrol, and antiemetics)
Primary options
» crystalloids--AND--
» ketorolac: 30 mg intravenously initially,followed by 15 mg every 6-8 hours for 3 daysonly-and/or-» morphine sulfate: 1-5 mg intravenouslyevery 4 hours when required
--AND--» ondansetron: 4 mg intravenously every 8hours when required
» Acute medical treatment for suspected renalor ureteric colic includes conservative therapiessuch as hydration, analgesia (nonsteroidal anti-inflammatory drugs [NSAIDs] such as ketorolacare used initially if normal renal function), and anantiemetic.
» NSAIDs have been shown to offer effectivepain relief from acute kidney stone relatedpain with fewer side effects than opioids andacetaminophen.[50]
»
Acuteconfirmed stone: no evidence ofobstruction nonpregnant
confirmed stone: no evidence ofobstruction nonpregnant
1st hydration, pain control, and antiemetics
Primary options
» crystalloids--AND--
» ketorolac: 30 mg intravenously initially,followed by 15 mg every 6-8 hours for 3 daysonly-and/or-» morphine sulfate: 1-5 mg intravenouslyevery 4 hours when required
24 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis Treatment
Acute--AND--
» ondansetron: 4 mg intravenously every 8hours when required
» Patients with newly diagnosed ureteric stones<10 mm without complicating factors (urosepsis,intractable pain and/or vomiting, impendingacute renal failure, obstruction of a solitary ortransplanted kidney, or bilateral obstruction) canbe managed expectantly.[52]
» Conservative treatment for confirmed stoneswith renal or ureteric colic includes hydration,analgesia (nonsteroidal anti-inflammatory drugs[NSAIDs] such as ketorolac are used initially ifnormal renal function), and an antiemetic.
» NSAIDs have been shown to offer effectivepain relief from acute kidney stone relatedpain with fewer side effects than opioids andacetaminophen.[50]
»demonstrated bacteriuria adjunct antibiotic therapy
Treatment recommended for SOME patients inselected patient group
Primary options
» sulfamethoxazole/trimethoprim: 160 mgorally twice daily for 1-2 weeksDose refers to trimethoprim component.
OR
» nitrofurantoin: 100 mg orally twice daily for1-2 weeks
» If infection is present, but no obstruction orsigns of sepsis, the patient can be treated withconservative therapy and antibiotics.
» Empiric antibiotic therapy should be startedpending sensitivity results based on urinalysiscultures.
adjunct surgical decompression
Treatment recommended for SOME patients inselected patient group
» Drainage can be accomplished in two ways. Inthe acute setting, a urologist can place a uretericstent past the obstructing stone and achieverenal drainage. Alternatively, percutaneousnephrostomy by an interventional radiologistmay be performed. Failure to perform rapid renaldecompression can lead to urosepsis and death.
TRE
ATMEN
T
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
25

Nephrolithiasis TreatmentTR
EAT
MEN
T
Acutestones <10 mm adjunct medical expulsive therapy (MET)
Treatment recommended for SOME patients inselected patient group
Primary options
» tamsulosin: 0.4 mg orally once daily
OR
» alfuzosin: 10 mg orally once daily
OR
» silodosin: 8 mg orally once daily
» There is evidence to support that MET canincrease ureteral stone passage rate anddecrease the time to stone passage in stones<10 mm in size.[51]
» Using an alpha-blocker, such as tamsulosin,alfuzosin, or silodosin may be of benefit inpromoting larger (but still <10 mm) distal ureteralstone passage; however, efficacy rates havebeen questioned.[58] [55] [56] [54] [57] [59] [60][61]
» These agents should be given for 4 to 6 weeksor until the stone is passed. If the stone has stillnot passed by that time, surgical intervention isrecommended.
» Patients should be made aware thatprescribing alpha-blockers for this indicationis considered an off-label use of these drugs.Additionally, tamsulosin has been associatedwith intraoperative floppy iris syndrome,therefore it should not be prescribed if a patienthas planned cataract surgery.
stones ≥10 mm or failedmedical therapy
adjunct surgical removal
Treatment recommended for SOME patients inselected patient group
» For smaller stones that fail conservativetherapies (e.g., uncontrolled symptoms, failureof stone to progress, or persistent obstruction),additional surgical treatment is necessary.
» Extracorporeal shock wave lithotripsy (ESWL)and ureteroscopy are considered first-linetreatments. However, ureteroscopy in generalis associated with better stone-free rates thanESWL.
26 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis Treatment
Acute» Percutaneous antegrade ureteroscopy involvespercutaneous antegrade removal of uretericstones, and can be considered in select caseswith very large (>15 mm) stones impacted in theupper ureter or when retrograde access is notpossible.
» Percutaneous nephrostolithotomy (PCNL) isminimally invasive and usually reserved for renaland proximal ureteric stones (i.e., in the lowerpole) and those that are large (>20 mm), havefailed therapy with ESWL and ureteroscopy, orare associated with complex renal anatomy.[83]
» Laparoscopic or open surgical stone removalmay be considered in rare cases where ESWL,ureteroscopy, and percutaneous ureteroscopyfail, or are unlikely to be successful.
confirmed stone: with evidence ofobstruction nonpregnant
1st hydration, pain control, and antiemetics
Primary options
» crystalloids--AND--
» ketorolac: 30 mg intravenously initially,followed by 15 mg every 6-8 hours for 3 daysonly-and/or-» morphine sulfate: 1-5 mg intravenouslyevery 4 hours when required
--AND--» ondansetron: 4 mg intravenously every 8hours when required
» Patients with obstructed urinary calculiwith infection require emergency urologicconsultation and surgical drainage, withintravenous antibiotics and supportive measures(hydration, analgesia, and antiemetics) asnecessary.
» If obstruction is present without infection, thepatient can be managed conservatively; if thepain cannot be managed with nonsteroidal anti-inflammatory drugs (if renal function normal)and opioids, then decompression should beconsidered.[22] If obstruction is present withinfection decompression and antibiotics areessential to minimize risk for life-threateningsepsis.
plus surgical decompression
Treatment recommended for ALL patients inselected patient group
TRE
ATMEN
T
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
27

Nephrolithiasis TreatmentTR
EAT
MEN
T
Acute» Drainage can be accomplished in two ways. Inthe acute setting, a urologist can place a uretericstent past the obstructing stone and achieverenal drainage. Alternatively, percutaneousnephrostomy by an interventional radiologist maybe performed.
plus surgical removal
Treatment recommended for ALL patients inselected patient group
» For smaller stones that fail conservativetherapies (e.g., uncontrolled symptoms, failureof stone to progress, or persistent obstruction),additional surgical treatment is necessary.
» Extracorporeal shock wave lithotripsy (ESWL)and ureteroscopy are considered first-linetreatments. However, ureteroscopy in generalis associated with better stone-free rates thanESWL.
» Percutaneous antegrade ureteroscopy involvespercutaneous antegrade removal of uretericstones, and can be considered in select caseswith very large (>15 mm) stones impacted in theupper ureter or when retrograde access is notpossible.
» Percutaneous nephrostolithotomy (PCNL) isminimally invasive and usually reserved for renaland proximal ureteric stones (i.e., in the lowerpole) and those that are large (>20 mm), havefailed therapy with ESWL and ureteroscopy, orare associated with complex renal anatomy.[83]
» Laparoscopic or open surgical stone removalmay be considered in rare cases where ESWL,ureteroscopy, and percutaneous ureteroscopyfail, or are unlikely to be successful.
with infection plus antibiotic therapy
Treatment recommended for ALL patients inselected patient group
Primary options
» gentamicin: 1.5 mg/kg intravenously every 8hours
OR
» ampicillin: 2 g intravenously every 6 hours-and-» gentamicin: 1.5 mg/kg intravenously every 8hours
OR
28 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis Treatment
Acute
» cefuroxime sodium: 750-1500 mgintravenously every 8 hours-or-» cefotetan: 1-2 g intravenously every 12-24hours-or-» ceftriaxone: 1-2 g intravenously every 24hours
--AND--» gentamicin: 1.5 mg/kg intravenously every 8hours
OR
» ceftriaxone: 1-2 g intravenously every 24hours
Secondary options
» piperacillin/tazobactam: 3.375 gintravenously every 6 hoursDose consists of 3 g of piperacillin plus 0.375g of tazobactam.
OR
» piperacillin/tazobactam: 3.375 gintravenously every 6 hoursDose consists of 3 g of piperacillin plus 0.375g of tazobactam.-and-» gentamicin: 1.5 mg/kg intravenously every 8hours
» Patients with urinary calculi along with feverand other signs or symptoms of infection needemergency urologic consultation for drainageand intravenous antibiotics.
» Empiric broad-spectrum antibiotic therapyshould be started pending sensitivity resultsbased on urinalysis cultures.[96] Empiricregimens differ across locations, and localguidance with the aid of a local antibiogramshould be sought.
» Patients should be treated with 14 days ofculture-specific antibiotics.
»
pregnant
1st specialist referral
TRE
ATMEN
T
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
29

Nephrolithiasis TreatmentTR
EAT
MEN
T
Acute» The principles of treatment for the acute stoneepisode are similar in pregnant and nonpregnantpatients. However, analgesics, antibiotics,antiemetics, and intravenous fluids are givenrelative to their safety and risk for that particulartrimester. Nonsteroidal anti-inflammatory drugsshould not be used during the first or secondtrimester. Alpha-blockers (e.g., tamsulosin) areFDA pregnancy category B.
» Similarly antibiotics are given according to theirrisk benefit ratio.
» Temporary measures for symptomaticobstruction or intractable symptoms include aureteric stent or percutaneous nephrostomytube. However, they need frequent changesbecause of increased encrustation risk. If thepatient has no evidence of infection, definitivetherapy with ureteroscopy may be performedand has been demonstrated to be safe.[87]Extracorporeal shock wave lithotripsy (ESWL)and percutaneous nephrostolithotomy (PCNL)are contraindicated in pregnancy.
Ongoingfollowing an acute episodenonpregnant
following an acute episodenonpregnant
1st hydration and dietary modification
» Long-term dietary modification is essentialfor preventing future calculi. This modificationis centered on increasing fluid intake. Atleast 2 liters of urine output daily should berecommended to help prevent future episodes ofstone formation.[88]
» Decreased dietary sodium, protein, andoxalate should be recommended for stoneprevention. Increased citrus fruit intake isrecommended to prevent stone recurrence.[89]
» Normal calcium intake is recommended.[89]Dietary calcium restriction can lead to lessbinding of calcium to oxalate in the GI tract,promoting hyperoxaluria and increased stoneformation.[97]
hyperuricosuria and/oruric acid stones
adjunct xanthine oxidase inhibitor ± alkalinizationtherapy
Treatment recommended for SOME patients inselected patient group
Primary options
30 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis Treatment
Ongoing» potassium citrate: 30-60 mEq/day orallygiven in 3-4 divided doses
OR
» allopurinol: 100-300 mg orally once daily
OR
» potassium citrate: 30-60 mEq/day orallygiven in 3-4 divided doses-and-» allopurinol: 100-300 mg orally once daily
Secondary options
» sodium bicarbonate: 4 g orally initially,followed by 1-2 g every 4-6 hours, maximum16 g/day
OR
» sodium bicarbonate: 4 g orally initially,followed by 1-2 g every 4-6 hours, maximum16 g/day-and-» allopurinol: 100-300 mg orally once daily
Tertiary options
» febuxostat: 40-80 mg orally once dailyAn increased risk of death has been reportedwith febuxostat compared to allopurinol. TheFDA recommends that febuxostat should onlybe prescribed in patients who cannot tolerate,or have failed treatment with, allopurinol.US Food and Drug Administration. FDAadds Boxed Warning for increased risk ofdeath with gout medicine Uloric (febuxostat).21 February 2019 [internet publication].https://www.fda.gov/Drugs/DrugSafety/ucm631182.htm
» Hyperuricosuria is treated with allopurinol.Elevated urinary uric acid levels (>800 mg/day) promote calcium oxalate and uric acidstones. Allopurinol is effective; it may workespecially well in patients with gout. Febuxostatis an alternative agent which, at high dose,lowers urinary uric acid to a greater extentthan allopurinol.[98] Febuxostat should onlybe prescribed for patients who can not tolerateallopurinol or when treatment with allopurinolhas failed, and who have been counselledregarding cardiovascular risk.[91]The double-blind Cardiovascular Safety of Febuxostat orAllopurinol in Patients with Gout (CARES)
TRE
ATMEN
T
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
31

Nephrolithiasis TreatmentTR
EAT
MEN
T
Ongoingsafety trial found that cardiovascular deathand all cause mortality were significantly morecommon among patients taking febuxostat thanallopurinol (4.3% vs. 3.2%, HR 1.34 [95% CI1.03 to 1.73]; 7.8% vs. 6.4%, HR 1.22 [95% CI1.01 to 1.47], respectively).[92] Treatment groupdid not differ with respect to a primary compositeoutcome of cardiovascular events.
» Uric acid stones are treated with alkalinizationtherapy, with or without allopurinol. Oralalkalinization therapy with medications suchas potassium citrate and sodium bicarbonatemay be beneficial for dissolving uric acid stonesand preventing uric acid supersaturation. It maybe used for treating uric acid stones that donot require urgent surgical treatment, as wellas asymptomatic stones. The ideal goal foralkalinization therapy is to maintain urine pHbetween 6.5 and 7.0. In patients with CHF orrenal failure, extra care should be taken whenprescribing alkalinization therapy. Potassiumcitrate is first-line therapy.
hypercalciuria adjunct diuretics/alkalinization
Treatment recommended for SOME patients inselected patient group
Primary options
» chlorthalidone: 25-50 mg orally once daily
OR
» hydrochlorothiazide: 25-50 mg orally twicedaily
OR
» indapamide: 1.25 to 2.5 mg orally oncedaily
Secondary options
» potassium citrate: 10-20 mEq orally three tofour times daily
» Given until urinary calcium normalizes.
» Thiazide diuretics are generally combined withpotassium citrate to prevent the development ofhypokalemia and hypocitraturia associated withthis therapy.
hypocitraturia adjunct alkalinization
Treatment recommended for SOME patients inselected patient group
32 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis Treatment
OngoingPrimary options
» potassium citrate: 30-60 mEq/day orallygiven in 4 divided doses
» Hypocitraturia is treated with oral alkalinizationtherapy.
hyperoxaluria adjunct oxalate chelator/alkalinization
Treatment recommended for SOME patients inselected patient group
Primary options
» calcium carbonate: 1-2 g/day orally given in3-4 divided dosesDose refers to elemental calcium.
OR
» calcium citrate: 1-2 g/day orally given in 3-4divided dosesDose refers to elemental calcium.
OR
» potassium citrate: 30-60 mEq/day orallygiven in 4 divided doses
OR
» magnesium oxide: 400-800 mg orally two tothree times daily
OR
» cholestyramine: 2-4 g orally four times daily
OR
» pyridoxine (vitamin B6): 250-500 mg orallyonce daily
» For patients with elevated urinary oxalatelevel secondary to small bowel or ileal disease,oral administration of calcium with meals isrecommended.[99]
» Cholestyramine is also effective forhyperoxaluria due to intestinal disease, but ispoorly tolerated.
» Treatment with potassium citrate can fix themetabolic acidosis and hypokalemia that may bepresent and can increase the urinary citrate.
TRE
ATMEN
T
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
33
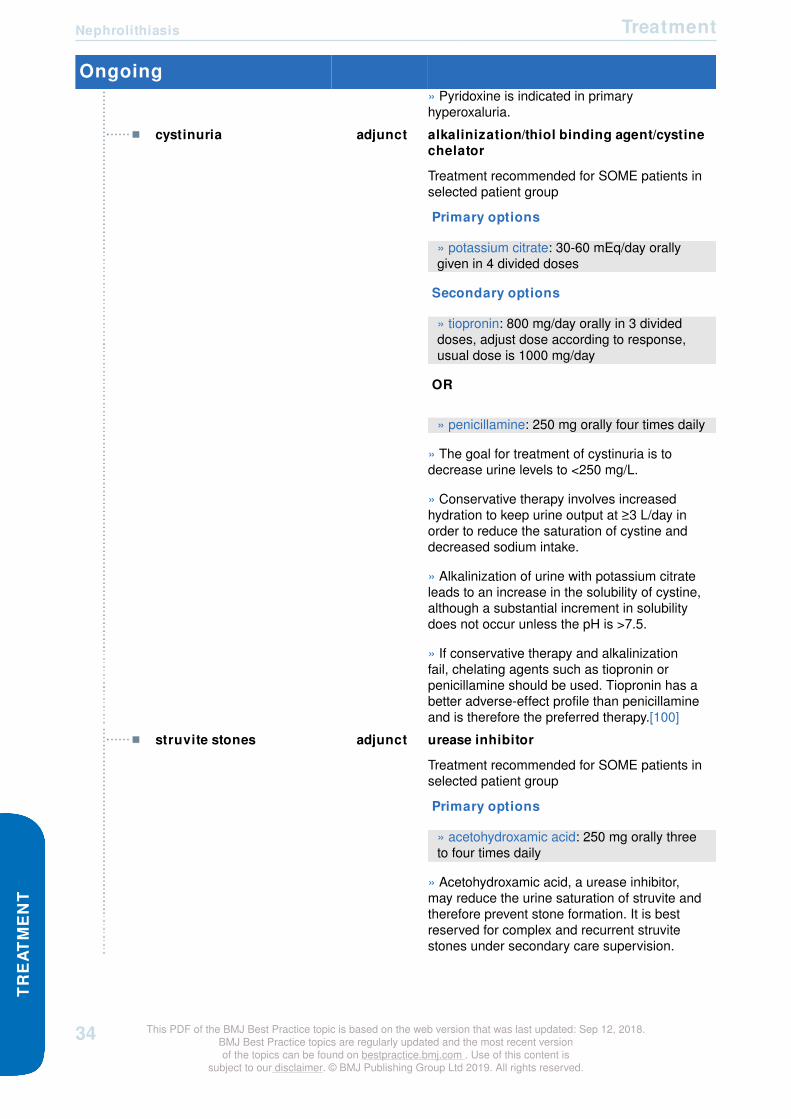
Nephrolithiasis TreatmentTR
EAT
MEN
T
Ongoing» Pyridoxine is indicated in primaryhyperoxaluria.
cystinuria adjunct alkalinization/thiol binding agent/cystinechelator
Treatment recommended for SOME patients inselected patient group
Primary options
» potassium citrate: 30-60 mEq/day orallygiven in 4 divided doses
Secondary options
» tiopronin: 800 mg/day orally in 3 divideddoses, adjust dose according to response,usual dose is 1000 mg/day
OR
» penicillamine: 250 mg orally four times daily
» The goal for treatment of cystinuria is todecrease urine levels to <250 mg/L.
» Conservative therapy involves increasedhydration to keep urine output at ≥3 L/day inorder to reduce the saturation of cystine anddecreased sodium intake.
» Alkalinization of urine with potassium citrateleads to an increase in the solubility of cystine,although a substantial increment in solubilitydoes not occur unless the pH is >7.5.
» If conservative therapy and alkalinizationfail, chelating agents such as tiopronin orpenicillamine should be used. Tiopronin has abetter adverse-effect profile than penicillamineand is therefore the preferred therapy.[100]
struvite stones adjunct urease inhibitor
Treatment recommended for SOME patients inselected patient group
Primary options
» acetohydroxamic acid: 250 mg orally threeto four times daily
» Acetohydroxamic acid, a urease inhibitor,may reduce the urine saturation of struvite andtherefore prevent stone formation. It is bestreserved for complex and recurrent struvitestones under secondary care supervision.
34 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
Nephrolithiasis Treatment
Ongoing» This medication has a high rate of adverseeffects including deep vein thrombosis, tremors,and headaches.[22]
TRE
ATMEN
T
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
35

Nephrolithiasis Follow upFO
LLO
W U
P
RecommendationsMonitoringAfter stone passage or successful medical/surgical treatment, patients with risk of recurrence should beevaluated metabolically with serum studies and 24-hour urine for metabolic studies to determine whetherany metabolic abnormalities exist that predispose to recurrent stone formation. Patients can then altertheir diet/lifestyle or be placed on the appropriate medication if needed.
Periodic 24-hour urine monitoring should be performed to assess the efficacy of dietary/lifestyle changesand medications. Imaging with noncontrast computed tomography (CT) scan or KUB should be carriedout every 6 to 12 months to monitor for recurrence or increase in the size of existing stones.
Patient instructionsPatients with nephrolithiasis should be advised to have a fluid intake of at least 2 to 2.5 liters per day, alow-protein diet, and a low-sodium diet to prevent nephrolithiasis.[103]
Complications
Complications Timeframe Likelihoodpost-percutaneous nephrostolithotomy (PCNL)bleeding
short term medium
Can occur from creation of nephrostomy tract when gaining access to the kidney. A nephrostomy tubewill usually tamponade the bleeding in the immediate postoperative period. Gross hematuria a week afterPCNL should be evaluated with renal arteriogram to evaluate for pseudoaneurysm or arterial-venousfistula which can be treated with embolization.
post-extracorporeal shock wave lithotripsy (ESWL)hematoma
short term low
Occurs due to disruption of blood vessels around and near kidney by shock waves. Managedconservatively with expectant management and blood transfusion if needed.
post-ESWL, PCNL, or ureteroscopy treatment urosepsis short term low
Should be treated with intravenous antibiotics and vasoactive medication when needed. Perform imagingto rule out obstruction or abscess.
post-ESWL steinstrasse short term low
Occurs due to stone fragments obstructing ureter and subsequent fragments not being able to pass.Patient may need a stent to adequately drain the kidney or a nephrostomy tube which facilitatesspontaneous stone passage.
36 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis Follow up
Complications Timeframe Likelihoodpost-ESWL, PCNL, or ureteroscopy ureteric injury short term low
Can occur from scope, laser, or basket causing ureteric damage. Short-term ureteric stent isrecommended.
visceral organ injury short term low
Can occur from creation of nephrostomy tract leading to bowel or liver injury.
pneumothorax short term low
May occur from creation of the nephrostomy tract with violation of the pleural cavity. Should be treated witha chest tube.
ureteric stricture long term low
Can be a long-term sequela from ureteric injury. Patient may need subsequent procedure such as dilationor incision of the stricture.
Prognosis
Nephrolithiasis is a lifelong disease process. The rate of recurrence of nephrolithiasis in first-time stoneformers is 50% at 5 years and 80% at 10 years.[1] The patients at highest risk for recurrence are frequentlythose who are not compliant with medical therapy and dietary/lifestyle modifications, or where underlyingmetabolic abnormalities exist. Residual stone fragments from surgery will usually spontaneously pass aslong as their size is <4 mm.
The Return of Kidney Stones (ROKS) nomogram can be used to help to predict the risk of a second kidneystone.[102]
FOLLO
W U
P
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
37

Nephrolithiasis GuidelinesG
UID
ELIN
ES
Diagnostic guidelines
International
Surgical management of stones [43]Published by: American Urological Association; Endourology Society Last published: 2016
CUA guideline on the evaluation and medical management of the kidneystone patient [44]Published by: Canadian Urological Association Last published: 2016
ACR Appropriateness Criteria: acute onset flank pain - suspicion of stonedisease (urolithiasis) [45]Published by: American College of Radiology Last published: 2015
Medical management of kidney stones [46]Published by: American Urological Association Last published: 2014
ACR Appropriateness Criteria: hematuria [47]Published by: American College of Radiology Last published: 2014
ACR Appropriateness Criteria: acute nonlocalized abdominal pain [48]Published by: American College of Radiology Last published: 2012
Guidelines on urolithiasis [38]Published by: European Association of Urology Last published: 2018
Treatment guidelines
International
Surgical management of stones [52]Published by: American Urological Association; Endourology Society Last published: 2016
CUA guideline on the evaluation and medical management of the kidneystone patient [44]Published by: Canadian Urological Association Last published: 2016
Prevention of recurrent nephrolithiasis: dietary and pharmacologic options [101]Published by: American College of Physicians Last published: 2015
Medical management of kidney stones [46]Published by: American Urological Association Last published: 2014
38 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis Guidelines
International
Urolithiasis [38]Published by: European Association of Urology Last published: 2018
GU
IDELIN
ES
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
39

Nephrolithiasis ReferencesR
EFER
ENC
ES
Key articles
• Pearle MS, Calhoun EA, Curhan GC. Urologic diseases in America project: urolithiasis. J Urol. 2005Mar;173(3):848-57. Abstract
• Moore CL, Daniels B, Ghita M, et al. Accuracy of reduced-dose computed tomography for ureteralstones in emergency department patients. Ann Emerg Med. 2015 Feb;65(2):189-98.e2. Abstract
• Pearle MS, Goldfarb DS, Assimos DG, et al.; American Urological Association. Medical managementof kidney stones: AUA guideline. J Urol. 2014 Aug;192(2):316-24. Full text Abstract
• Assimos D, Krambeck A, Miller NL, et al. Surgical management of stones: American UrologicalAssociation/Endourological Society Guideline. 2016 [internet publication]. Full text
• Türk C, Neisius A, Petrik A, et al. European Association of Urology. Guidelines on urolithiasis. 2018[internet publication]. Full text
References
1. Stoller ML. Urinary stone disease. In: Tanagho EA, McAninch JW, eds. Smith's General Urology, 16thedition. New York, NY: McGraw-Hill: 2004: 256-291.
2. Wilson DM. Clinical and laboratory approaches for evaluation of nephrolithiasis. J Urol. 1989Mar;141(3 Pt 2):770-4. Abstract
3. Pak CY, Poindexter JR, Adams-Huet B, et al. Predictive value of kidney stone composition in thedetection of metabolic abnormalities. Am J Med. 2003 Jul;115(1):26-32. Abstract
4. Griffith DP, Osborne CA. Infection (urease) stones. Miner Electrolyte Metab. 1987;13(4):278-85.Abstract
5. Norlin A, Lindell B, Granberg PO, et al. Urolithiasis. A study of its frequency. Scand J Urol Nephrol.1976;10(2):150-3. Abstract
6. Sierakowski R, Finlayson B, Landes RR, et al. The frequency of urolithiasis in hospital dischargediagnoses in the United States. Invest Urol. 1978 May;15(6):438-41. Abstract
7. Scales CD Jr, Smith AC, Hanley JM, et al. Prevalence of kidney stones in the United States. Eur Urol.2012 Jul;62(1):160-5. Full text Abstract
8. Hiatt RA, Dales LG, Friedman GD, et al. Frequency of urolithiasis in a prepaid medical care program.Am J Epidemiol. 1982 Feb;115(2):255-65. Abstract
9. Soucie JM, Thun MJ, Coates RJ, et al. Demographic and geographic variability of kidney stones in theUnited States. Kidney Int. 1994 Sep;46(3):893-9. Abstract
40 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
Nephrolithiasis References
10. Pearle MS, Calhoun EA, Curhan GC. Urologic diseases in America project: urolithiasis. J Urol. 2005Mar;173(3):848-57. Abstract
11. Lieske JC, Peña de la Vega LS, Slezak JM, et al. Renal stone epidemiology in Rochester, Minnesota:an update. Kidney Int. 2006 Feb;69(4):760-4. Abstract
12. Sarmina I, Spirnak JP, Resnick MI. Urinary lithiasis in the black population: an epidemiological studyand review of the literature. J Urol. 1987 Jul;138(1):14-7. Abstract
13. Tasian GE, Ross ME, Song L, et al. Annual incidence of nephrolithiasis among children and adultsin South Carolina from 1997 to 2012. Clin J Am Soc Nephrol. 2016 Mar 7;11(3):488-96. Full text Abstract
14. Marshall V, White RH, De Saintonage M, et al. The natural history of renal and ureteric calculi. Br JUrol. 1975 Apr;47(2):117-24. Abstract
15. Finlayson B. Symposium on renal lithiasis. Renal lithiasis in review. Urol Clin North Am. 1974Jun;1(2):181-212. Abstract
16. Sorokin I, Mamoulakis C, Miyazawa K, et al. Epidemiology of stone disease across the world. World JUrol. 2017 Sep;35(9):1301-20. Abstract
17. Curhan GC, Willett WC, Rimm EB, et al. Body size and risk of kidney stones. J Am Soc Nephrol. 1998Sep;9(9):1645-52. Full text Abstract
18. Taylor EN, Stampfer MJ, Curhan GC. Obesity, weight gain, and the risk of kidney stones. JAMA. 2005Jan 26;293(4):455-62. Full text Abstract
19. Worcester EM. Inhibitors of stone formation. Semin Nephrol. 1996;16:474-486. Abstract
20. Pearle M, Lotan Y. Urinary lithiasis: etiology, epidemiology, and pathogenesis. In: Walsh P, RetikA, Vaughan ED Jr, Wein A, eds. Campbell's Urology, 8th edition. Philadelphia, PA: WB Saunders;2002:1363-1371.
21. Evan AP, Lingeman JE, Coe FL, et al. Randall's plaque of patients with nephrolithiasis begins inbasement membranes of thin loops of Henle. J Clin Invest. 2003;111:607-616. Full text Abstract
22. Stoller ML. Urinary stone disease. In: Tanagho EA, McAninch JW, eds. Smith's General Urology, 16thedition. New York, NY: McGraw-Hill: 2004: 256-91.
23. Stamatelou KK, Francis ME, Jones CA, et al. Time trends in reported prevalence of kidney stones inthe United States: 1976-1994. Kidney Int. 2003 May;63(5):1817-23. Abstract
24. Curhan GC, Willett WC, Rimm EB, et al. A prospective study of dietary calcium and other nutrients andthe risk of symptomatic kidney stones. N Engl J Med. 1993 Mar 25;328(12):833-8. Full text Abstract
25. Curhan GC, Willett WC, Speizer FE, et al. Comparison of dietary calcium with supplemental calciumand other nutrients as factors affecting the risk for kidney stones in women. Ann Intern Med. 1997 Apr1;126(7):497-504. Abstract
REFER
ENC
ES
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
41

Nephrolithiasis ReferencesR
EFER
ENC
ES
26. Pearle M, Lotan Y. Urinary lithiasis: etiology, epidemiology, and pathogenesis. In: Walsh P, RetikA, Vaughan ED Jr, Wein A, eds. Campbell's Urology, 8th edition. Philadelphia, PA: WB Saunders;2002:1363-71.
27. Prince CL, Scardino PL, Wolan CT. The effect of temperature, humidity and dehydration on theformation of renal calculi. J Urol. 1956 Feb;75(2):209-15. Abstract
28. Prince CL, Scardino PL. A statistical analysis of ureteral calculi. J Urol. 1960 May;83:561-5. Abstract
29. Geraghty RM, Proietti S, Traxer O, et al. Worldwide impact of warmer seasons on the incidence ofrenal colic and kidney stone disease: evidence from a systematic review of literature. J Endourol. 2017Aug;31(8):729-35. Abstract
30. Daudon M, Frochot V, Bazin D, et al. Drug-induced kidney stones and crystalline nephropathy:pathophysiology, prevention and treatment. Drugs. 2018 Feb;78(2):163-201. Abstract
31. Tasian GE, Jemielita T, Goldfarb DS, et al. Oral antibiotic exposure and kidney stone disease. J AmSoc Nephrol. 2018 Jun;29(6):1731-40. Abstract
32. Fulgham PF, Assimos DG, Pearle MS, et al. Clinical effectiveness protocols for imaging inthe management of ureteral calculous disease: AUA Technology Assessment. J Urol. 2013Apr;189(4):1203-13. Full text Abstract
33. Ripollés T, Agramunt M, Errando J, et al. Suspected ureteral colic: plain film and sonography vsunenhanced helical CT. A prospective study in 66 patients. Eur Radiol. 2004 Jan;14(1):129-36.Abstract
34. Gorelik U, Ulish Y, Yagil Y. The use of standard imaging techniques and their diagnostic value in theworkup of renal colic in the setting of intractable flank pain. Urology. 1996 May;47(5):637-42. Abstract
35. Dalla Palma L, Stacul F, Bazzocchi M, et al. Ultrasonography and plain film versus intravenousurography in ureteric colic. Clin Radiol. 1993 May;47(5):333-6. Abstract
36. Smith-Bindman R, Aubin C, Bailitz J, et al. Ultrasonography versus computed tomography forsuspected nephrolithiasis. N Engl J Med. 2014 Sep 18;371(12):1100-10. Full text Abstract
37. ACOG Committee on Obstetric Practice. Committee opinion no. 723: Guidelines for diagnostic imagingduring pregnancy and lactation. Obstet Gynecol. 2017 Oct;130(4):e210-6. Full text Abstract
38. Türk C, Neisius A, Petrik A, et al. European Association of Urology. Guidelines on urolithiasis. 2018[internet publication]. Full text
39. Worcester EM, Coe FL. Clinical practice. Calcium kidney stones. N Engl J Med. 2010 Sep2;363(10):954-63. Full text Abstract
40. Uribarri J, Oh MS, Carroll HJ. The first kidney stone. Ann Intern Med. 1989 Dec 15;111(12):1006-9.Abstract
42 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis References
41. Moore CL, Daniels B, Ghita M, et al. Accuracy of reduced-dose computed tomography for ureteralstones in emergency department patients. Ann Emerg Med. 2015 Feb;65(2):189-98.e2. Abstract
42. Levine JA, Neitlich J, Verga M, et al. Ureteral calculi in patients with flank pain: correlation of plainradiography with unenhanced helical CT. Radiology. 1997 Jul;204(1):27-31. Abstract
43. Assimos D, Krambeck A, Miller NL, et al. Surgical management of stones: American UrologicalAssociation/Endourological Society Guideline. J Urol. 2016 Oct;196(4):1153-60. Full text Abstract
44. Dion M, Ankawi G, Chew B, et al. CUA guideline on the evaluation and medical management of thekidney stone patient - 2016 update. Can Urol Assoc J. 2016 Nov-Dec;10(11-12):E347-58. Full text Abstract
45. ACR Appropriateness Criteria: cute onset flank pain - suspicion of stone disease (urolithiasis). 2015[internet publication]. Full text
46. Pearle MS, Goldfarb DS, Assimos DG, et al.; American Urological Association. Medical managementof kidney stones: AUA guideline. J Urol. 2014 Aug;192(2):316-24. Full text Abstract
47. American College of Radiology. ACR Appropriateness Criteria: hematuria. 2014 [internet publication]. Full text
48. American College of Radiology. ACR Appropriateness Criteria: acute nonlocalized abdominal pain.2012 [internet publication]. Full text
49. Sammon JD, Ghani KR, Karakiewicz PI, et al. Temporal trends, practice patterns, and treatmentoutcomes for infected upper urinary tract stones in the United States. Eur Urol. 2013 Jul;64(1):85-92.Abstract
50. Pathan SA, Mitra B, Cameron PA. A systematic review and meta-analysis comparing the efficacy ofnonsteroidal anti-inflammatory drugs, opioids, and paracetamol in the treatment of acute renal colic.Eur Urol. 2018 Apr;73(4):583-95. Abstract
51. Eisner BH, Goldfarb DS, Pareek G. Pharmacologic treatment of kidney stone disease. Urol Clin NorthAm. 2013 Feb;40(1):21-30. Abstract
52. Assimos D, Krambeck A, Miller NL, et al. Surgical management of stones: American UrologicalAssociation/Endourological Society Guideline. 2016 [internet publication]. Full text
53. Jendeberg J, Geijer H, Alshamari M, et al. Size matters: the width and location of a ureteral stoneaccurately predict the chance of spontaneous passage. Eur Radiol. 2017 Nov;27(11):4775-85. Fulltext Abstract
54. Campschroer T, Zhu X, Vernooij RW, et al. Alpha-blockers as medical expulsive therapy for ureteralstones. Cochrane Database Syst Rev. 2018;(4):CD008509. Full text Abstract
55. Sridharan K, Sivaramakrishnan G. Efficacy and safety of alpha blockers in medical expulsivetherapy for ureteral stones: a mixed treatment network meta-analysis and trial sequential analysis ofrandomized controlled clinical trials. Expert Rev Clin Pharmacol. 2018 Mar;11(3):291-307. Abstract
REFER
ENC
ES
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
43

Nephrolithiasis ReferencesR
EFER
ENC
ES
56. Meltzer AC, Burrows PK, Wolfson AB, et al. Effect of tamsulosin on passage of symptomatic ureteralstones: a randomized clinical trial. JAMA Intern Med. 2018 Aug 1;178(8):1051-7. Full text Abstract
57. Hollingsworth JM, Canales BK, Rogers MA, et al. Alpha blockers for treatment of ureteric stones:systematic review and meta-analysis. BMJ. 2016 Dec 1;355:i6112. Full text Abstract
58. Wang RC, Smith-Bindman R, Whitaker E, et al. Effect of tamsulosin on stone passage for ureteralstones: a systematic review and meta-analysis. Ann Emerg Med. 2017 Mar;69(3):353-61.e3. Abstract
59. El Said NO, El Wakeel L, Kamal KM, et al. Alfuzosin treatment improves the rate and time forstone expulsion in patients with distal uretral stones: a prospective randomized controlled study.Pharmacotherapy. 2015 May;35(5):470-6. Abstract
60. Sur RL, Shore N, L'Esperance J. Silodosin to facilitate passage of ureteral stones: a multi-institutional,randomized, double-blinded, placebo-controlled trial. Eur Urol. 2015 May;67(5):959-64. Abstract
61. Yang D, Wu J, Yuan H, et al. The efficacy and safety of silodosin for the treatment of ureteral stones: asystematic review and meta-analysis. BMC Urol. 2016 May 27;16(1):23. Full text Abstract
62. Micali S, Grande M, Sighinolfi MC, et al. Medical therapy of urolithiasis. J Endourol. 2006Nov;20(11):841-7. Abstract
63. Saw KC, Lingeman JE. Lesson 20: management of calyceal stones. AUA Update Series.1999;20:154-9.
64. Havel D, Saussine C, Fath C, et al. Single stones of the lower pole of the kidney. Comparativeresults of extracorporeal shock wave lithotripsy and percutaneous nephrolithotomy. Eur Urol.1998;33(4):396-400. Abstract
65. Kachel TA, Vijan SR, Dretler SP. Endourological experience with cystine calculi and a treatmentalgorithm. J Urol. 1991 Jan;145(1):25-8. Abstract
66. Grasso M, Ficazzola M. Retrograde ureteropyeloscopy for lower pole caliceal calculi. J Urol. 1999Dec;162(6):1904-8. Abstract
67. Aboumarzouk OM, Monga M, Kata SG, et al. Flexible ureteroscopy and laser lithotripsy for stones >2cm: a systematic review and meta-analysis. J Endourol. 2012 Oct;26(10):1257-63. Abstract
68. Kang SK, Cho KS, Kang DH, et al. Systematic review and meta-analysis to compare success rates ofretrograde intrarenal surgery versus percutaneous nephrolithotomy for renal stones >2 cm: an update.Medicine (Baltimore). 2017 Dec;96(49):e9119. Full text Abstract
69. Lingeman JE, Matlaga BR, Evan AP. Surgical management of upper urinary tract calculi. In: Wein AJ,Kavoussi LR, Novick AC, et al., eds. Campbell's urology. 9th ed. Philadelphia, PA: Saunders Elsevier;2007:1431-1507.
70. Zhu Y, Duijvesz D, Rovers MM, et al. Alpha-blockers to assist stone clearance after extracorporealshock wave lithotripsy: a meta-analysis. BJU Int. 2010 Jul;106(2):256-61. Abstract
44 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis References
71. Liu LR, Li QJ, Wei Q, et al. Percussion, diuresis, and inversion therapy for the passage of lower polekidney stones following shock wave lithotripsy. Cochrane Database Syst Rev. 2013;(12):CD008569. Full text Abstract
72. Loughlin KR. Management of urologic problems during pregnancy. Urology. 1994 Aug;44(2):159-69.Abstract
73. Ignatoff JM, Nelson JB. Use of extracorporeal shock wave lithotripsy in a solitary kidney with renalartery aneurysm. J Urol. 1993 Feb;149(2):359-60. Abstract
74. Wang H, Man L, Li G, et al. Meta-analysis of stenting versus non-stenting for the treatment of ureteralstones. PLoS One. 2017 Jan 9;12(1):e0167670. Full text Abstract
75. Türk C, Neisius A, Petrik A, et al. European Association of Urology. Guidelines on urolithiasis. 2018[internet publication]. Full text
76. Dell'Atti L, Papa S. Ten-year experience in the management of distal ureteral stones greater than 10mm in size. G Chir. 2016 Jan-Feb;37(1):27-30. Full text Abstract
77. Cui X, Ji F, Yan H, et al. Comparison between extracorporeal shock wave lithotripsy and ureteroscopiclithotripsy for treating large proximal ureteral stones: a meta-analysis. Urology. 2015 Apr;85(4):748-56.Abstract
78. Drake T, Grivas N, Dabestani S, et al. What are the benefits and harms of ureteroscopy compared withshock-wave lithotripsy in the treatment of upper ureteral stones? A systematic review. Eur Urol. 2017Nov;72(5):772-86. Abstract
79. Aboumarzouk OM, Kata SG, Keeley FX, et al. Extracorporeal shock wave lithotripsy (ESWL) versusureteroscopic management for ureteric calculi. Cochrane Database Syst Rev. 2012;(5):CD006029. Full text Abstract
80. Maheshwari PN, Oswal AT, Andankar M, et al. Is antegrade ureteroscopy better than retrogradeureteroscopy for impacted large upper ureteral calculi? J Endourol. 1999 Jul-Aug;13(6):441-4. Abstract
81. el-Nahas AR, Eraky I, el-Assmy AM, et al. Percutaneous treatment of large upper tract stones afterurinary diversion. Urology. 2006 Sep;68(3):500-4. Abstract
82. Wang Q, Guo J, Hu H, et al. Rigid ureteroscopic lithotripsy versus percutaneous nephrolithotomy forlarge proximal ureteral stones: a meta-analysis. PLoS One. 2017 Feb 9;12(2):e0171478. Full text Abstract
83. Lingeman JE, Matlaga BR, et al. Surgical management of upper urinary tract calculi. In: Walsh P, RetikA, Vaughan ED Jr, Wein A, eds. Campbell's Urology, 8th edition. Philadelphia, PA: WB Saunders;2002: 1431-1507.
84. Lingeman JE, Coury TA, Newman DM, et al. Comparison of results and morbidity of percutaneousnephrostolithotomy and extracorporeal shock wave lithotripsy. J Urol. 1987 Sep;138(3):485-90.Abstract
REFER
ENC
ES
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
45

Nephrolithiasis ReferencesR
EFER
ENC
ES
85. Semins MJ, Matlaga BR. Kidney stones during pregnancy. Nat Rev Urol. 2014 Mar;11(3):163-8.Abstract
86. Burgess KL, Gettman MT, Rangel LJ, et al. Diagnosis of urolithiasis and rate of spontaneous passageduring pregnancy. J Urol. 2011 Dec;186(6):2280-4. Abstract
87. Semins MJ, Trock BJ, Matlaga BR. The safety of ureteroscopy during pregnancy: a systematic reviewand meta-analysis. J Urol. 2009 Jan;181(1):139-43. Abstract
88. Cheungpasitporn W, Rossetti S, Friend K, et al. Treatment effect, adherence, and safety of highfluid intake for the prevention of incident and recurrent kidney stones: a systematic review and meta-analysis. J Nephrol. 2016 Apr;29(2):211-9. Full text Abstract
89. Pak CY. Kidney stones. Lancet. 1998 Jun 13;351(9118):1797-801. Abstract
90. Gambaro G, Croppi E, Coe F, et al; Consensus Conference Group. Metabolic diagnosis and medicalprevention of calcium nephrolithiasis and its systemic manifestations: a consensus statement. JNephrol. 2016 Dec;29(6):715-34. Full text Abstract
91. US Food and Drug Administration. FDA adds Boxed Warning for increased risk of death with goutmedicine Uloric (febuxostat). 21 February 2019 [internet publication]. Full text
92. White WB, Saag KG, Becker MA, et al. Cardiovascular safety of febuxostat or allopurinol in patientswith gout. N Engl J Med. 2018 Mar 12;378(13):1200-10. Full text Abstract
93. Phillips R, Hanchanale VS, Myatt A, et al. Citrate salts for preventing and treating calcium containingkidney stones in adults. Cochrane Database Syst Rev. 2015;(10):CD010057. Full text Abstract
94. Kern A, Grimsby G, Mayo H, et al. Medical and dietary interventions for preventing recurrent urinarystones in children. Cochrane Database Syst Rev. 2017;(11):CD011252. Full text Abstract
95. Barreto L, Jung JH, Abdelrahim A, et al. Medical and surgical interventions for the treatment of urinarystones in children. Cochrane Database Syst Rev. 2018;(6):CD010784. Full text Abstract
96. Bonkat G, Pickard R, Bartoletti R, et al. European Association of Urology. Guidelines on urologicalinfections. 2018 [internet publication]. Full text
97. Escribano J, Balaguer A, Roqué i Figuls M, et al. Dietary interventions for preventing complications inidiopathic hypercalciuria. Cochrane Database Syst Rev. 2014;(2):CD006022. Full text Abstract
98. Goldfarb DS, MacDonald PA, Gunawardhana L, et al. Randomized controlled trial of febuxostat versusallopurinol or placebo in individuals with higher urinary uric acid excretion and calcium stones. Clin JAm Soc Nephrol. 2013 Nov;8(11):1960-7. Full text Abstract
99. Worcester EM. Stones from bowel disease. Endocrinol Metab Clin North Am. 2002 Dec;31(4):979-99.Abstract
100. Pak CY, Fuller C, Sakhaee K, et al. Management of cystine nephrolithiasis with alpha-mercaptopropionylglycine. J Urol. 1986 Nov;136(5):1003-8. Abstract
46 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Nephrolithiasis References
101. Hauk L. Prevention of recurrent nephrolithiasis: dietary and pharmacologic options recommended bythe ACP. Am Fam Physician. 2015 Aug 15;92(4):311. Full text
102. Rule AD, Lieske JC, Li X, et al. The ROKS nomogram for predicting a second symptomatic stoneepisode. J Am Soc Nephrol. 2014;25:2878-2886. Abstract
103. Borghi L, Meschi T, Schianchi T, et al. Urine volume: stone risk factor and preventive measure.Nephron. 1999;8(suppl 1):31-7. Abstract
REFER
ENC
ES
This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.
47

Nephrolithiasis DisclaimerD
ISC
LAIM
ER
DisclaimerThis content is meant for medical professionals. The BMJ Publishing Group Ltd (“BMJ Group”) tries toensure that the information provided is accurate and uptodate, but we do not warrant that it is. The BMJGroup does not advocate or endorse the use of any drug or therapy contained within nor does it diagnosepatients. Medical professionals should use their own professional judgement in using this information andcaring for their patients and the information herein should not be considered a substitute for that.
This information is not intended to cover all possible diagnosis methods, treatments, follow up, drugs and anycontraindications or side effects. We strongly recommend that users independently verify specified diagnosis,treatments and follow up and ensure it is appropriate for your patient. This information is provided on an “asis” basis and to the fullest extent permitted by law the BMJ Group assumes no responsibility for any aspect ofhealthcare administered with the aid of this information or any other use of this information.
View our full Website Terms and Conditions.
Contact us
+1 855-458-0579 (toll free from USA)[email protected]
BMJ Americas Office2 Hudson Place,Suite 300Hoboken,New Jersey 07030
48 This PDF of the BMJ Best Practice topic is based on the web version that was last updated: Sep 12, 2018.BMJ Best Practice topics are regularly updated and the most recent versionof the topics can be found on bestpractice.bmj.com . Use of this content is
subject to our disclaimer. © BMJ Publishing Group Ltd 2019. All rights reserved.

Contributors:
// Authors:
Jodi Antonelli, MDAssistant ProfessorDepartment of Urology, University of Texas Southwestern Medical Center, Dallas, TXDISCLOSURES: JA is a member of the Scientific Advisory Board for Boston Scientific. JA has receiveda research grant from the US National Institutes of Health to study strategies to reduce recurrence ofnephrolithiasis and reduce stent-associated pain.
Naim Maalouf, MDAssociate Program DirectorAssociate Professor, University of Texas Southwestern Medical Center, Dallas, TXDISCLOSURES: NM has received a research grant from the US National Institutes of Health to studystrategies to reduce recurrence of nephrolithiasis and reduce stent-associated pain.
// Acknowledgements:Dr Jodi Antonelli and Dr Naim Maalouf would like to gratefully acknowledge Dr Brian Eisner, Dr Michael E.Lipkin, Dr Muhammad Iqbal, Dr Keith Xavier, and Dr Mantu Gupta, previous contributors to this monograph.BE has received fees for consulting from Boston Scientific, Olympus/Gyrus ACMI, PercSys, and The RavineGroup. MEL declares that he is a consultant for Boston Scientific Corporation. MI, KX, and MG declare thatthey have no competing interests.
// Peer Reviewers:
Robert Tompkins, MDAssociate ProfessorDepartment of Family Medicine, University of Texas Health Science Center, Tyler, TXDISCLOSURES: RT declares that he has no competing interests.
Lynda Frassetto, MDAssociate Professor of MedicineDivision of Nephrology, University of California at San Francisco, CADISCLOSURES: LF declares that she has no competing interests.
Irfan Moinuddin, MDAssistant ProfessorChicago Medical School, Rosalind Franklin University, Lombard, ILDISCLOSURES: IM declares that he has no competing interests.
Nagaraja Rao, MBBS, ChM, FRCSConsultant Urological SurgeonSpire Manchester Hospital, Manchester, UKDISCLOSURES: NR declares no competing interests.


















