Neonatalmicrostructuraldevelopmentoflesuperior4temporal ... · perinatal physiological risk...
1
Neonatal microstructural development of le3 superiortemporal gyrus and cerebral white ma:er correlates with cogni;ve development at 1820 months in verylowbirthweight preterm children Rachel Vassar BA 1 , Naama BarneaGoraly MD 2 , Katelyn CahillRowley MS 1 , David K Stevenson MD 2 , Susan R Hintz MD, MS Epi 2 , and Jessica Rose PhD 1 1 Department of Orthopaedic Surgery, 2 Center for Interdisciplinary Brain Sciences Research, 3 Division of Neonatology and Developmental Medicine, Stanford University School of Medicine, Stanford, CA, IntroducNon Results At nearterm age, the brain undergoes rapid growth and microstructural development. AbnormaliNes idenNfied during this period have been recognized as potenNal predictors of neurodevelopment in children born preterm. 1,2 Children born preterm with verylowbirthweight (VLBW) are at high risk for neuromotor problems including cerebral palsy, developmental and cogniNve impairment and language delay. 2 The incidence of auNsm spectrum disorder is 23 Nmes higher among VLBW preterm infants compared to term infants. 3,4 Certain morbidiNes and clinical factors, including bronchopulmonary dysplasia (BPD), have been shown to be associated with higher risk for adverse outcomes. Previous studies have also demonstrated widespread differences in white maZer (WM) development and regional corNcal volumes in infants born VLBW compared to agematched full term infants. 5 Nearterm brain MRI has been suggested as a potenNal tool for enhanced prognosis for VLBW infants and to guide early intervenNon at a Nme of opNmal neuroplasNcity. Diffusion tensor imaging (DTI) allows analysis of brain microstructure based on paZerns of water diffusion. As the brain develops, brain water content decreases, extracellular spaces diminish, and cellular microstructures become more complex and organized, all changes quanNfiable with DTI. To examine the relaNonship between brain development at nearterm, clinical variables, and cogniNve development at 1820 months. Subjects: 102 VLBW infants (≤1500g BW; ≤32 weeks GA) admiZed to the NICU who had rouNne near term brain MRI between 1/1/1012/31/11 were recruited to parNcipate, represenNng 74% of eligible infants; 66 of these infants also had DTI. This analysis examined the subpopulaNon of 59 neonates who received DTI scans at nearterm age and were administered the CogniNve subtest of the Bayley Scales of Infant DevelopmentIII (BSIDIII) assessment at 1820 months of age, corrected for prematurity. Methods References 1. Rose J, Butler EE, Lamont LE, et al. Neonatal brain structure on MRI and diffusion tensor imaging, sex, and neurodevelopment in VLBW preterm children. Dev Med Child Neurol. 2009; 51(7):526–535. 2. Woodward LJ, Clark CAC, Bora S, et al. Neonatal White MaZer AbnormaliNes an Important Predictor of NeurocogniNve Outcome for Very Preterm Children. PLoS ONE. 2012; 7(12):e51879. 3. Movsas TZ, PintoMarNn JA, Whitaker AH, et al. AuNsm Spectrum Disorder Is Associated with Ventricular Enlargement in a Low Birth Weight PopulaNon. The Journal of Pediatrics. 2013; 163(1):738. 4. Limperopoulos C, Bassan H, Sullivan NR, et al. PosiNve Screening for AuNsm in Expreterm Infants: Prevalence and Risk Factors. Pediatrics. 2008; 121(4):758–765. 5. Lee AY, Jang SH, Lee E, et al. Radiologic differences in white maZer maturaNon between preterm and fullterm infants: TBSS study. Pediatric Radiology. 2012; 43(5):6129. 6. Oishi K, Mori S, Donohue PK, et al. MulNcontrast human neonatal brain atlas: applicaNon to normal neonate development analysis. Neuroimage. 2011;5 6(1):8–20. Figure 1. Neonatal brain white maZer regions idenNfied in a representaNve parNcipant on trace image, based on the JHU neonatal atlas and LDDMM transformaNon. DTI Parameters and Processing: Brain MRI was performed on 3T MRI at LPCH. DTI raw images were processed using DTIStudio and DiffeoMap (www.mristudio.org) using the FA and trace maps to perform a large deformaNon diffeomorphic metric mapping (LDDMM) transformaNon. Each brain was normalized to map onto the JHU neonatal atlas 6 and automaNcally segmented into 126 regions, using threshold values of trace <0.006 mm 2 s −1 and FA >0.15. Regions analyzed (Fig. 1) included WM regions that are wellvisualized at nearterm age and thought to be related to motor and cogniNve funcNon. Regional FA and MD values were analyzed and correlaNons were assessed between DTI values and cogniNve score on the BSIDIII at 1820 months corrected age. (Table 2). Diffusion tensor imaging (DTI): reflects fiber coherence, direcNonality, diameter, density, and myelinaNon Frac;onal anisotropy (FA): direcNonality of diffusion Mean diffusivity (MD): mean diffusion on 3 axes, (λ 1 +λ 2 +λ 3 ) /3 λ 1 λ 2 λ 3 Bundle of fibers Total population Neonates with BSID, DTI, without BPD Neonates with BSID, DTI, with BPD Total n= 102 34 25 Males/Females, (%) 41% / 59% 32% / 68% 44% / 56% Birthweight (g), mean (SD) 1087 (279) 1179 (248) 915 (217) GAatbirth (wks), mean (SD) 28.7 (2.4) 30.0 (2.0) 27.0 (1.7) PMAatscan (wks), mean (SD) 36.6 (1.8) 36.1 (1.0) 37.2 (1.4) Cognitive score, BSIDIII at 18mo 95.4 (12.3) 99.0 (12.8) 92.0 (12.7) Bronchopulmonary dysplasia (%) 37% 0% 100% Table 1. ParNcipant demographics Discussion We wish to thank Alex SoxHarris for staNsNcal consultaNon and Dr. Ximena Stecher Guzman for neuroradiological consultaNon. This research is supported in part by the NIH Clinical and TranslaNonal Science Award 1UL1 RR025744 for the Stanford Center for Clinical and TranslaNonal EducaNon and Research (Spectrum) and by the Lucile Packard FoundaNon for Children's Health. This material is based upon work supported by the NaNonal Science FoundaNon Graduate Research Fellowship under Grant No. DGE1147470. Methods Table 2. CorrelaNons between nearterm brain DTI values of FA and MD and BSIDIII cogniNve subscore at 1820 months, corrected for PMAatscan. Results indicate that BSIDIII cogniNve subscore at 1820 months was lower in infants with history of BPD, although they were also of lower BW and GA and more likely to be male. Mean motor and language subscore were not different between the group with and without BPD. CorrelaNons between cogniNve composite score and brain DTI values differed between the group with and without BPD. The subpopulaNon without BPD demonstrated strong posiNve correlaNons between nearterm FA and cogniNve development at 1820 months. Correlations between FA and BSIDIII Cognitive Score Correlations between MD and BSIDIII Cognitive Score Brain Region Without BPD (n=34) With BPD (n=25) Total (n=59) Without BPD (n=34) With BPD (n=25) Total (n=59) CC Genu 0.359* (p = .040) 0.576** (p = .003) 0.058 (p = .667) 0.126 (p = .484) 0.203 (p = .343) 0.193 (p = .761) CC Body 0.112 (p = .537) 0.272 (p = .199) 0.041 (p = .762) 0.189 (p = .293) 0.162 (p = .449) 0.196 (p = .141) CC Splenium 0.075 (p = .680) 0.237 (p = .264) 0.042 (p = .755) 0.039 (p = .831) 0.133 (p = .535) 0.041 (p = .141) SCR L R 0.390* (p = .025) 0.117 (p = .588) 0.115 (p = .390) 0.127 (p = .483) 0.208 (p = .328) 0.089 (p = .505) 0.326 (p = .064) 0.368 (p = .077 ) 0.052 (p = .697) 0.065 (p = .717) 0.115 (p = . 592) 0.035 (p = .796) PCR L R 0.340 (p = .053) 0.426* (p = .038) 0.056 (p = .677) 0.247 (p = .166) 0.007 (p = .973) 0.111 (p = .407) 0.446** (p = .009) 0.325 (p = .122) 0.103 (p = .441) 0.169 (p = .346) 0.080 (p = .710) 0.085 (p = .526) ALIC L R 0.403* (p = .020) 0.252 (p = .235) 0.153 (p = .251) 0.181 (p = .313) 0.083 (p = .701) 0.042 (p = .752) 0.271 (p = .128) 0.221 (p = .300) 0.078 (p = .563) 0.312 (p = .077) 0.043 (p = .844) 0.105 (p =.435) PLIC L R 0.386* (p = .026) 0.171 (p = .425) 0.122 (p = .360) 0.437* (p = .011) 0.289 (p = .171) 0.356** (p = .006) 0.344 (p = .050) 0.210 (p = .324) 0.069 (p = .609) 0.303 (p = .086) 0.149 (p = .287) 0.211 (p =.112) RLC L R 0.530** (p = .002) 0.385 (p = .064) 0.169 (p = .206) 0.284 (p = .109) 0.186 (p = .384) 0.177 (p = .184) ) 0.395* (p = .023) 0.217 (p = .309) 0.086 (p = .522) 0.105 (p = .562) 0.343 (p = .101) 0.069 (p = .604) ) EC L R 0.467** (p = .006) 0.271 (p = .200) 0.087 (p = .517) 0.151 (p = .400) 0.268 (p = .205) 0.109 (p = .414) 0.519** (p = .002) 0.215 (p = .312) 0.131 (p = .328) 0.062 (p = .733) 0.209 (p = .328) 0.035 (p = .796) StriaT L R 0.377* (p = .031) 0.427* (p = .037) 0.069 (p = .607) 0.212 (p = .237) 0.251 (p = .236) 0.005 (p = .968) ) 0.473** (p = .005) 0.193 (p = .366) 0.212 (p = .109) 0.106 (p = .558) 0.245 (p = .248) 0.046 (p = .732) ST Gyrus L R 0.036 (p = .842) .021 (p = .922) 0.031 (p = .820) 0.351* (p = .045) 0.066 (p = .760) 0.219 (p =.098) 0.114 (p =.528) 0.021 (p = .924) 0.090 (p = .502) 0.168 (p = .349) 0.123 (p =.567) 0.131 (p = .328) * Significant correlations, p< 0.05 ** Significant correlations, p< 0.01 Preliminary results suggest that the observed associaNon between BPD and adverse neurodevelopmental outcome may be explained in part by brain microstructural WM injury. The ongoing research may further elucidate these links to guide NICUbased quality of care improvements and targeted postdischarge early intervenNon. Acknowledgments Aim CC Genu CC Body CC Splenium Superior Corona Radiata (SCR) Posterior Corona Radiata (PCR) Anterior Limb of Internal Capsule (ALIC) Posterior Limb of Internal Capsule (PLIC) RetrolenNcular Part of Internal Capsule (RLC) Stria Terminalis (StriaT) External Capsule (EC) Superior Temporal Gyrus (ST Gyrus) R² = 0.22854 R² = 0.27778 0.17 0.18 0.19 0.2 0.21 0.22 0.23 65 75 85 95 105 115 125 Frac;onal anisotropy (FA) BSIDIII Cogni;ve Score EC (lew) EC (right) R² = 0.28808 0.21 0.23 0.25 0.27 0.29 0.31 0.33 0.35 0.37 65 75 85 95 105 115 125 Frac;onal anisotropy (FA) BSIDIII Cogni;ve Score RLC (lew) R² = 0.19214 1.00E03 1.05E03 1.10E03 1.15E03 1.20E03 1.25E03 1.30E03 65 75 85 95 105 115 125 Mean diffusivity (MD) BSIDIII Cogni;ve Score ST Gyrus (lew) Figure 2. DTI of the (A) external capsule FA (B) retrolenNcular capsule FA, and (C) lew superior temporal gyrus MD, in relaNon to BSIDIII cogniNve score at 1820 months among infants without BPD A B C A P
Transcript of Neonatalmicrostructuraldevelopmentoflesuperior4temporal ... · perinatal physiological risk...

Neonatal microstructural development of le3 superior-‐temporal gyrus and cerebral white ma:er correlates with cogni;ve development at 18-‐20 months in very-‐low-‐birth-‐weight preterm children
Rachel Vassar BA 1, Naama Barnea-‐Goraly MD 2, Katelyn Cahill-‐Rowley MS1, David K Stevenson MD2, Susan R Hintz MD, MS Epi2 , and Jessica Rose PhD1
1Department of Orthopaedic Surgery, 2Center for Interdisciplinary Brain Sciences Research, 3Division of Neonatology and Developmental Medicine, Stanford University School of Medicine, Stanford, CA,
Neonatal Neural Correlates, Physiological Risk Factors, and Early Motor Development in Very Low Birth Weight Preterm Children: A Diffusion Imaging Study
Jessica Rose PhD1, 2, Rachel Vassar BA2,5, Katelyn Cahill-Rowley MS4, Susan R. Hintz MD, MS Epi3, David K. Stevenson MD3, Naama Barnea-Goraly MD5
1Motion & Gait Analysis Laboratory, Lucile Packard Children�s Hospital, 2Department of Orthopaedic Surgery, 3Division of Neonatology and Developmental Medicine, 4Department of BioEngineering, 5Center for Interdisciplinary Brain Sciences Research, Stanford University School of Medicine, Stanford, CA
Objectives Results
Discussion
Initial results suggest left PLIC MD may have prognostic value for early motor function. This WM region includes corticospinal tract descending motor pathways. The stronger association found in the left PLIC may be explained by a majority of participants who demonstrated right hand preference. Cortical GM regions that mediate motor control may also have prognostic value for later fine and gross motor function. Limitations include partial volume effects with the relatively small size of the cortex in preterm infants, thus our defined cortical regions likely contain both GM and WM. This line of research may reveal brain structure-function relations that influence motor development. Preliminary analysis of this ongoing research may provide neonatal clues to later motor deficits and ultimately, may guide early intervention to improve motor control and quality of life for preterm children.
Results Methods
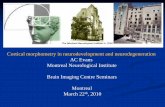
Figure 2. Axial and Sagittal DTI showing motor regions of interest (ROI).
Figure 3. Partial correlation plots (N=30) of relationship between motor development on BSID-III Composite Motor score at 18-20 months in relation to neonatal brain DTI: A) Left PLIC MD B) Combined Left PLIC + Right Cuneus MD controlling for GA-at-scan.
Table 1 . Demographics and perinatal physiological risk factor data.
Acknowledgements: We wish to thank Sue Thiemann and Alex Sox-Harris for valuable statistical consultation. This research is supported in part by the NIH Clinical and Translational Science Award 1UL1 RR025744 for the Stanford Center for Clinical and Translational Education and Research (Spectrum) and by the Lucile Packard Foundation for Children's Health.
Acknowledgements
Cerebral palsy is the most prevalent childhood motor disorder, affecting approximately 3/1000 children in the US. and is defined as “a group of disorders affecting the development of movement and posture, attributed to non-progressive disturbances to the developing fetal or infant brain” (CDC 2012, Bax 2005). The incidence of CP is substantially higher in children born prematurely, affecting ~15% of very low birth weight (VLBW) preterm children (<1500g, <32 wks gestation). An additional number of preterm children (~ 40%) may develop mild to severe motor impairment by school age, a prevalence 3-4 times that of the general population (Williams et al., 2010, Spittle et al, 2011). Early prognosis of motor function in preterm infants can guide early treatment at a time when there i s o p t i m a l n e u r o p l a s t i c i t y, r a p i d musculoskeletal growth, and an opportunity to improve motor control and prevent growth-related deformities. Diffusion tensor imaging (DTI) provides quantitative regional analysis of brain microstructure based on patterns of water diffusion. DTI may offer more accurate neonatal prognosis of risk of motor deficits compared to structural MRI (Rose et al., 2007, 2009). As the brain develops, brain water content decreases, extracellular spaces diminish in size, and intra and intercellular microstructures become more complex and organized. With development, new barriers to water mobility are formed, such as cell membranes of axons, dendrites, and white matter (WM) myelination and coherence, and diffusion becomes more restricted. DTI may offer a more sensitive measure to detect microstructural abnormalities that lead to CP. Aim: To develop a neonatal prognostic index for upper and lower-limb motor function in preterm children, based on near-term brain DTI as well as other perinatal risk factors.
102 VLBW infants (<1500g BW;<32weeks GA) admitted to the NICU who had routine n e a r - t e r m b r a i n - M R I b e t w e e n 1/1/10-12/31/11 were recruited to participate, representing 74% of eligible infants, 68 of these infants also had DTI. To date, 45 infants (91% retention) returned for follow-up evaluation of neurodevelopment at 18-20 months corrected age, 30 also had DTI. Brain MRI scans performed on 3T MRI(GE-Discovery MR750,GE 8-Channel HD head coil) included T1, T2-weighted scans and diffusion-weighted scans. DTI was processed using an infant atlas and DiffeoMap (www.mristudio.org), thresholded for CSF, for calculations of mean diffusivity (MD). White matter motor tracts analyzed included posterior limb of internal capsule (PLIC). Grey matter (GM) regions known to mediate motor control were analyzed including medial and lateral frontal orbital gyri (FOG) and Cuneus.
Figure 1. Diffusion tensor image axial view showing corticospinal tracts traversing the posterior limb of internal capsule (PLIC). Motor development at 18-20 months adjusted-age was assessed on Bayley Scales of Infant Development (BSID-III). Age adjusted Composite Motor score and Fine and Gross Motor Scaled scores are reported. Directional hypotheses were tested and 2-tailed significance reported.
Initial findings are reported from an ongoing prospective study of neonatal brain structure on MRI and diffusion-tensor imaging (DTI), perinatal physiological risk factors, and early neurodevelopment at 18-20 months of age in VLBW preterm children.
BSI
D-I
II C
ompo
site
Mot
or S
core
Left PLIC MD
At 18-20 months of age the mean BSID-III Composite Motor Percentile score was 44%, Mean Fine Motor age equivalence was 19.5+3.6 months and Gross Motor was 16.6+2.5 months. Table 2. Correlations examined a prioi hypotheses regarding neonatal brain development on DTI MD at near-term age and motor function on BSID-III at 18-22 months of age.
BSI
D-I
II C
ompo
site
Mot
or S
core
Figure 3a.
Figure 3b.
Demographics:. Population!n=102!Female/male! 60/42!Birth!Weight,!g,!mean!±!SD! 1088!±!278!GA!at!birth,!weeks,!mean!±!SD! 28.7!±!2.4!GA!at!MRI,!weeks,!mean!±!SD! 36.6!±!1.8!Mean!maternal!age,!years! 31.6!±6.0!.Perinatal.Clinical.Measures:.
.Prevalence:.
Bronchopulmonary!dysplasia!(BPD)! 40%!Retinopathy!of!prematurity!(ROP)! 71%!Sepsis! 20%!Necrotizing!enterocolitis!(NEC)! 11%!Premature!rupture!of!maternal!membranes!(PPROM)! 31%!Mechanical!ventilation!required! 62%!Abnormal!structural!MRI! 37%!Mean!Total!Serum!Bilirubin!(TB)!in!first!two!weeks,!mg/dl,!mean!�!SD!(range)!
5.4!�1.3!(2.9\10.0)!
Mean!Peak!Total!Serum!Bilirubin!(PTB)!in!first!two!weeks!!mg/dl,!mean!�!SD!(range)!
7.9!�1.9!(4.5\16.3)!
!
Brain&Regions:&1°&Hypothesis&&
Mean%Diffusivity%Mean%±%SD%
Composite%Motor%Score%%
Fine%Motor%Score%%
Gross%Motor%Score&
Left%Posterior%Limb%of%Internal%Cap%Right%Posterior%Limb%of%Internal%Cap%
.00116%±.&00004%
.00116%±&.00004%E.474,%p=.009*%E.315,%p=.096%
E.417,%p=.025*%E.259,%p=.176%
E.258,%p=.177%E.167,%p=.387%
2°&Hypotheses&& % % & %Right%Cuneus% .00142%±&.00005%% E.443,%p=.016*% E.428,%p=.020*% E.206,%p=.283%
Right%Medial%Frontal%Orbital%Gyrus% .00148%±&.00007%% E.188,%p=..330% E.033,%p=.867% E.346,%p=.066%Right%Lateral%Frontal%Orbital%Gyrus& .00150%±&.00005% E.171,%p=.375% E.042,%p=.831% E.361,%p=.055%
*%Significance%p%<%%.05%
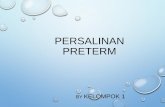
As expected, MD decreased with older GA-at-scan: Left PLIC MD vs GA-at-scan R= -.407, p=.001 Right Cuneus MD vs GA-at-scan R= -.528, p=.000. Thus, correlations between MD and BSID-III scores are reported controlling for GA-at-scan (Partridge et al. 2004, Rose et al 2007).
Left PLIC + Right Cuneus MD
R = -.474 p = .009
R = -.566 p = .004
Neonatal Neural Correlates, Physiological Risk Factors, and Early Motor Development in Very Low Birth Weight Preterm Children: A Diffusion Imaging Study
Jessica Rose PhD1, 2, Rachel Vassar BA2,5, Katelyn Cahill-Rowley MS4, Susan R. Hintz MD, MS Epi3, David K. Stevenson MD3, Naama Barnea-Goraly MD5
1Motion & Gait Analysis Laboratory, Lucile Packard Children�s Hospital, 2Department of Orthopaedic Surgery, 3Division of Neonatology and Developmental Medicine, 4Department of BioEngineering, 5Center for Interdisciplinary Brain Sciences Research, Stanford University School of Medicine, Stanford, CA
Objectives Results
Discussion
Initial results suggest left PLIC MD may have prognostic value for early motor function. This WM region includes corticospinal tract descending motor pathways. The stronger association found in the left PLIC may be explained by a majority of participants who demonstrated right hand preference. Cortical GM regions that mediate motor control may also have prognostic value for later fine and gross motor function. Limitations include partial volume effects with the relatively small size of the cortex in preterm infants, thus our defined cortical regions likely contain both GM and WM. This line of research may reveal brain structure-function relations that influence motor development. Preliminary analysis of this ongoing research may provide neonatal clues to later motor deficits and ultimately, may guide early intervention to improve motor control and quality of life for preterm children.
Results Methods
Figure 2. Axial and Sagittal DTI showing motor regions of interest (ROI).
Figure 3. Partial correlation plots (N=30) of relationship between motor development on BSID-III Composite Motor score at 18-20 months in relation to neonatal brain DTI: A) Left PLIC MD B) Combined Left PLIC + Right Cuneus MD controlling for GA-at-scan.
Table 1 . Demographics and perinatal physiological risk factor data.
Acknowledgements: We wish to thank Sue Thiemann and Alex Sox-Harris for valuable statistical consultation. This research is supported in part by the NIH Clinical and Translational Science Award 1UL1 RR025744 for the Stanford Center for Clinical and Translational Education and Research (Spectrum) and by the Lucile Packard Foundation for Children's Health.
Acknowledgements
Cerebral palsy is the most prevalent childhood motor disorder, affecting approximately 3/1000 children in the US. and is defined as “a group of disorders affecting the development of movement and posture, attributed to non-progressive disturbances to the developing fetal or infant brain” (CDC 2012, Bax 2005). The incidence of CP is substantially higher in children born prematurely, affecting ~15% of very low birth weight (VLBW) preterm children (<1500g, <32 wks gestation). An additional number of preterm children (~ 40%) may develop mild to severe motor impairment by school age, a prevalence 3-4 times that of the general population (Williams et al., 2010, Spittle et al, 2011). Early prognosis of motor function in preterm infants can guide early treatment at a time when there i s o p t i m a l n e u r o p l a s t i c i t y, r a p i d musculoskeletal growth, and an opportunity to improve motor control and prevent growth-related deformities. Diffusion tensor imaging (DTI) provides quantitative regional analysis of brain microstructure based on patterns of water diffusion. DTI may offer more accurate neonatal prognosis of risk of motor deficits compared to structural MRI (Rose et al., 2007, 2009). As the brain develops, brain water content decreases, extracellular spaces diminish in size, and intra and intercellular microstructures become more complex and organized. With development, new barriers to water mobility are formed, such as cell membranes of axons, dendrites, and white matter (WM) myelination and coherence, and diffusion becomes more restricted. DTI may offer a more sensitive measure to detect microstructural abnormalities that lead to CP. Aim: To develop a neonatal prognostic index for upper and lower-limb motor function in preterm children, based on near-term brain DTI as well as other perinatal risk factors.
102 VLBW infants (<1500g BW;<32weeks GA) admitted to the NICU who had routine n e a r - t e r m b r a i n - M R I b e t w e e n 1/1/10-12/31/11 were recruited to participate, representing 74% of eligible infants, 68 of these infants also had DTI. To date, 45 infants (91% retention) returned for follow-up evaluation of neurodevelopment at 18-20 months corrected age, 30 also had DTI. Brain MRI scans performed on 3T MRI(GE-Discovery MR750,GE 8-Channel HD head coil) included T1, T2-weighted scans and diffusion-weighted scans. DTI was processed using an infant atlas and DiffeoMap (www.mristudio.org), thresholded for CSF, for calculations of mean diffusivity (MD). White matter motor tracts analyzed included posterior limb of internal capsule (PLIC). Grey matter (GM) regions known to mediate motor control were analyzed including medial and lateral frontal orbital gyri (FOG) and Cuneus.
Figure 1. Diffusion tensor image axial view showing corticospinal tracts traversing the posterior limb of internal capsule (PLIC). Motor development at 18-20 months adjusted-age was assessed on Bayley Scales of Infant Development (BSID-III). Age adjusted Composite Motor score and Fine and Gross Motor Scaled scores are reported. Directional hypotheses were tested and 2-tailed significance reported.
Initial findings are reported from an ongoing prospective study of neonatal brain structure on MRI and diffusion-tensor imaging (DTI), perinatal physiological risk factors, and early neurodevelopment at 18-20 months of age in VLBW preterm children.
BSID
-III C
ompo
site
Mot
or S
core
Left PLIC MD
At 18-20 months of age the mean BSID-III Composite Motor Percentile score was 44%, Mean Fine Motor age equivalence was 19.5+3.6 months and Gross Motor was 16.6+2.5 months. Table 2. Correlations examined a prioi hypotheses regarding neonatal brain development on DTI MD at near-term age and motor function on BSID-III at 18-22 months of age.
BSID
-III C
ompo
site
Mot
or S
core
Figure 3a.
Figure 3b.
Demographics:. Population!n=102!Female/male! 60/42!Birth!Weight,!g,!mean!±!SD! 1088!±!278!GA!at!birth,!weeks,!mean!±!SD! 28.7!±!2.4!GA!at!MRI,!weeks,!mean!±!SD! 36.6!±!1.8!Mean!maternal!age,!years! 31.6!±6.0!.Perinatal.Clinical.Measures:.
.Prevalence:.
Bronchopulmonary!dysplasia!(BPD)! 40%!Retinopathy!of!prematurity!(ROP)! 71%!Sepsis! 20%!Necrotizing!enterocolitis!(NEC)! 11%!Premature!rupture!of!maternal!membranes!(PPROM)! 31%!Mechanical!ventilation!required! 62%!Abnormal!structural!MRI! 37%!Mean!Total!Serum!Bilirubin!(TB)!in!first!two!weeks,!mg/dl,!mean!�!SD!(range)!
5.4!�1.3!(2.9\10.0)!
Mean!Peak!Total!Serum!Bilirubin!(PTB)!in!first!two!weeks!!mg/dl,!mean!�!SD!(range)!
7.9!�1.9!(4.5\16.3)!
!
Brain&Regions:&1°&Hypothesis&&
Mean%Diffusivity%Mean%±%SD%
Composite%Motor%Score%%
Fine%Motor%Score%%
Gross%Motor%Score&
Left%Posterior%Limb%of%Internal%Cap%Right%Posterior%Limb%of%Internal%Cap%
.00116%±.&00004%
.00116%±&.00004%E.474,%p=.009*%E.315,%p=.096%
E.417,%p=.025*%E.259,%p=.176%
E.258,%p=.177%E.167,%p=.387%
2°&Hypotheses&& % % & %Right%Cuneus% .00142%±&.00005%% E.443,%p=.016*% E.428,%p=.020*% E.206,%p=.283%
Right%Medial%Frontal%Orbital%Gyrus% .00148%±&.00007%% E.188,%p=..330% E.033,%p=.867% E.346,%p=.066%Right%Lateral%Frontal%Orbital%Gyrus& .00150%±&.00005% E.171,%p=.375% E.042,%p=.831% E.361,%p=.055%
*%Significance%p%<%%.05%
As expected, MD decreased with older GA-at-scan: Left PLIC MD vs GA-at-scan R= -.407, p=.001 Right Cuneus MD vs GA-at-scan R= -.528, p=.000. Thus, correlations between MD and BSID-III scores are reported controlling for GA-at-scan (Partridge et al. 2004, Rose et al 2007).
Left PLIC + Right Cuneus MD
R = -.474 p = .009
R = -.566 p = .004
IntroducNon Results
At near-‐term age, the brain undergoes rapid growth and microstructural development. AbnormaliNes idenNfied during this period have been recognized as potenNal predictors of neurodevelopment in children born preterm.1,2 Children born preterm with very-‐low-‐birth-‐weight (VLBW) are at high risk for neuromotor problems including cerebral palsy, developmental and cogniNve impairment and language delay.2 The incidence of auNsm spectrum disorder is 2-‐3 Nmes higher among VLBW preterm infants compared to term infants.3,4 Certain morbidiNes and clinical factors, including bronchopulmonary dysplasia (BPD), have been shown to be associated with higher risk for adverse outcomes. Previous studies have also demonstrated widespread differences in white maZer (WM) development and regional corNcal volumes in infants born VLBW compared to age-‐matched full-‐term infants.5 Near-‐term brain MRI has been suggested as a potenNal tool for enhanced prognosis for VLBW infants and to guide early intervenNon at a Nme of opNmal neuroplasNcity. Diffusion tensor imaging (DTI) allows analysis of brain microstructure based on paZerns of water diffusion. As the brain develops, brain water content decreases, extracellular spaces diminish, and cellular microstructures become more complex and organized, all changes quanNfiable with DTI.
To examine the relaNonship between brain development at near-‐term, clinical variables, and cogniNve development at 18-‐20 months.
Subjects: 102 VLBW infants (≤1500g BW; ≤32 weeks GA) admiZed to the NICU who had rouNne near-‐term brain MRI between 1/1/10-‐12/31/11 were recruited to parNcipate, represenNng 74% of eligible infants; 66 of these infants also had DTI. This analysis examined the sub-‐populaNon of 59 neonates who received DTI scans at near-‐term age and were administered the CogniNve subtest of the Bayley Scales of Infant Development-‐III (BSID-‐III) assessment at 18-‐20 months of age, corrected for prematurity.
Methods
References 1. Rose J, Butler EE, Lamont LE, et al. Neonatal brain structure on MRI and diffusion tensor imaging, sex, and neurodevelopment in VLBW preterm children. Dev Med Child Neurol. 2009; 51(7):526–535. 2. Woodward LJ, Clark CAC, Bora S, et al. Neonatal White MaZer AbnormaliNes an Important Predictor of NeurocogniNve Outcome for Very Preterm Children. PLoS ONE. 2012; 7(12):e51879. 3. Movsas TZ, Pinto-‐MarNn JA, Whitaker AH, et al. AuNsm Spectrum Disorder Is Associated with Ventricular Enlargement in a Low Birth Weight PopulaNon. The Journal of Pediatrics. 2013; 163(1):73-‐8. 4. Limperopoulos C, Bassan H, Sullivan NR, et al. PosiNve Screening for AuNsm in Ex-‐preterm Infants: Prevalence and Risk Factors. Pediatrics. 2008; 121(4):758–765. 5. Lee AY, Jang SH, Lee E, et al. Radiologic differences in white maZer maturaNon between preterm and full-‐term infants: TBSS study. Pediatric Radiology. 2012; 43(5):612-‐9. 6. Oishi K, Mori S, Donohue PK, et al. MulN-‐contrast human neonatal brain atlas: applicaNon to normal neonate development analysis. Neuroimage. 2011;5 6(1):8–20.
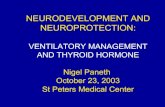
Figure 1. Neonatal brain white maZer regions idenNfied in a representaNve parNcipant on trace image, based on the JHU neonatal atlas and LDDMM transformaNon. DTI Parameters and Processing: Brain MRI was performed on 3T MRI at LPCH. DTI raw images were processed using DTIStudio and DiffeoMap (www.mristudio.org) using the FA and trace maps to perform a large deformaNon diffeomorphic metric mapping (LDDMM) transformaNon. Each brain was normalized to map onto the JHU neonatal atlas6 and automaNcally segmented into 126 regions, using threshold values of trace <0.006 mm2
s−1 and FA >0.15. Regions analyzed (Fig. 1) included WM regions that are well-‐visualized at near-‐term age and thought to be related to motor and cogniNve funcNon. Regional FA and MD values were analyzed and correlaNons were assessed between DTI values and cogniNve score on the BSID-‐III at 18-‐20 months corrected age. (Table 2).
Diffusion tensor imaging (DTI): reflects fiber coherence, direcNonality, diameter, density, and myelinaNon Frac;onal anisotropy (FA): direcNonality of diffusion Mean diffusivity (MD): mean diffusion on 3 axes, (λ1+λ2 +λ3) /3
λ1
λ2
λ3
Bundle of fibers
Total population Neonates with BSID, DTI, without BPD
Neonates with BSID, DTI, with BPD
Total n= 102 34 25
Males/Females, (%) 41% / 59% 32% / 68% 44% / 56%
Birthweight (g), mean (SD) 1087 (279) 1179 (248) 915 (217)
GA-‐at-‐birth (wks), mean (SD) 28.7 (2.4) 30.0 (2.0) 27.0 (1.7)
PMA-‐at-‐scan (wks), mean (SD) 36.6 (1.8) 36.1 (1.0) 37.2 (1.4)
Cognitive score, BSID-‐III at 18-‐mo 95.4 (12.3) 99.0 (12.8) 92.0 (12.7)
Bronchopulmonary dysplasia (%) 37% 0% 100%
Table 1. ParNcipant demographics
Discussion
We wish to thank Alex Sox-‐Harris for staNsNcal consultaNon and Dr. Ximena Stecher Guzman for neuroradiological consultaNon. This research is supported in part by the NIH Clinical and TranslaNonal Science Award 1UL1 RR025744 for the Stanford Center for Clinical and TranslaNonal EducaNon and Research (Spectrum) and by the Lucile Packard FoundaNon for Children's Health. This material is based upon work supported by the NaNonal Science FoundaNon Graduate Research Fellowship under Grant No. DGE-‐1147470.
Methods
Table 2. CorrelaNons between near-‐term brain DTI values of FA and MD and BSID-‐III cogniNve subscore at 18-‐20 months, corrected for PMA-‐at-‐scan.
Results indicate that BSID-‐III cogniNve subscore at 18-‐20 months was lower in infants with history of BPD, although they were also of lower BW and GA and more likely to be male. Mean motor and language subscore were not different between the group with and without BPD. CorrelaNons between cogniNve composite score and brain DTI values differed between the group with and without BPD. The sub-‐populaNon without BPD demonstrated strong posiNve correlaNons between near-‐term FA and cogniNve development at 18-‐20 months.
Correlations between FA and BSID-‐III Cognitive Score Correlations between MD and BSID-‐III Cognitive Score
Brain Region
Without BPD (n=34)
With BPD (n=25)
Total (n=59)
Without BPD (n=34)
With BPD (n=25)
Total (n=59)
CC Genu
0.359* (p = .040)
-‐0.576** (p = .003)
-‐0.058 (p = .667)
0.126 (p = .484)
0.203 (p = .343)
0.193 (p = .761)
CC Body 0.112 (p = .537)
-‐0.272 (p = .199)
-‐0.041 (p = .762)
0.189 (p = .293)
0.162 (p = .449)
0.196 (p = .141)
CC Splenium
0.075 (p = .680)
-‐0.237 (p = .264)
-‐0.042 (p = .755)
0.039 (p = .831)
0.133 (p = .535)
0.041 (p = .141)
SCR L R
0.390* (p = .025)
-‐0.117 (p = .588)
0.115 (p = .390)
-‐0.127 (p = .483)
-‐0.208 (p = .328)
-‐0.089 (p = .505)
0.326 (p = .064)
-‐0.368 (p = .077 )
-‐0.052 (p = .697)
-‐0.065 (p = .717)
-‐0.115 (p = . 592)
-‐0.035 (p = .796) PCR L
R
0.340 (p = .053)
-‐0.426* (p = .038)
-‐0.056 (p = .677)
-‐0.247 (p = .166)
-‐0.007 (p = .973)
-‐0.111 (p = .407)
0.446** (p = .009)
-‐0.325 (p = .122)
0.103 (p = .441)
-‐0.169 (p = .346)
-‐0.080 (p = .710)
-‐0.085 (p = .526)
ALIC L R
0.403* (p = .020)
-‐0.252 (p = .235)
0.153 (p = .251)
-‐0.181 (p = .313)
0.083 (p = .701)
-‐0.042 (p = .752)
0.271 (p = .128)
-‐0.221 (p = .300)
0.078 (p = .563)
-‐0.312 (p = .077)
0.043 (p = .844)
-‐0.105 (p =.435)
PLIC L R
0.386* (p = .026)
-‐0.171 (p = .425)
0.122 (p = .360)
-‐0.437* (p = .011)
-‐0.289 (p = .171)
-‐0.356** (p = .006)
0.344 (p = .050)
-‐0.210 (p = .324)
0.069 (p = .609)
-‐0.303 (p = .086)
-‐0.149 (p = .287)
-‐0.211 (p =.112)
RLC L R
0.530** (p = .002)
-‐0.385 (p = .064)
0.169 (p = .206)
-‐0.284 (p = .109)
-‐0.186 (p = .384)
-‐0.177 (p = .184) ) 0.395*
(p = .023) -‐0.217 (p = .309)
0.086 (p = .522)
-‐0.105 (p = .562)
-‐0.343 (p = .101)
-‐0.069 (p = .604) )
EC L R
0.467** (p = .006)
-‐0.271 (p = .200)
0.087 (p = .517)
-‐0.151 (p = .400)
-‐0.268 (p = .205)
-‐0.109 (p = .414) 0.519**
(p = .002) -‐0.215 (p = .312)
0.131 (p = .328)
-‐0.062 (p = .733)
-‐0.209 (p = .328)
-‐0.035 (p = .796) StriaT L
R
0.377* (p = .031)
-‐0.427* (p = .037)
0.069 (p = .607)
-‐0.212 (p = .237)
0.251 (p = .236)
-‐0.005 (p = .968) ) 0.473**
(p = .005) -‐0.193 (p = .366)
0.212 (p = .109)
-‐0.106 (p = .558)
0.245 (p = .248)
0.046 (p = .732)
ST Gyrus L R
-‐0.036 (p = .842)
.021 (p = .922)
-‐0.031 (p = .820)
-‐0.351* (p = .045)
0.066 (p = .760)
-‐0.219 (p =.098)
-‐0.114 (p =.528)
-‐0.021 (p = .924)
-‐0.090 (p = .502)
-‐0.168 (p = .349)
-‐0.123 (p =.567)
-‐0.131 (p = .328)
* Significant correlations, p< 0.05 ** Significant correlations, p< 0.01
Preliminary results suggest that the observed a s so c i aNon be tween BPD and adve r se neurodevelopmental outcome may be explained in part by brain microstructural WM injury. The ongoing research may further elucidate these links to guide NICU-‐based quality of care improvements and targeted post-‐discharge early intervenNon.
Acknowledgments Aim
CC Genu CC Body CC Splenium Superior Corona Radiata (SCR) Posterior Corona Radiata (PCR) Anterior Limb of Internal Capsule (ALIC) Posterior Limb of Internal Capsule (PLIC) RetrolenNcular Part of Internal Capsule (RLC) Stria Terminalis (StriaT) External Capsule (EC) Superior Temporal Gyrus (ST Gyrus)
R² = 0.22854 R² = 0.27778
0.17
0.18
0.19
0.2
0.21
0.22
0.23
65 75 85 95 105 115 125
Frac;o
nal anisotrop
y (FA)
BSID-‐III Cogni;ve Score
EC (lew)
EC (right)
R² = 0.28808
0.21
0.23
0.25
0.27
0.29
0.31
0.33
0.35
0.37
65 75 85 95 105 115 125
Frac;o
nal anisotrop
y (FA)
BSID-‐III Cogni;ve Score
RLC (lew)
R² = 0.19214
1.00E-‐03
1.05E-‐03
1.10E-‐03
1.15E-‐03
1.20E-‐03
1.25E-‐03
1.30E-‐03
65 75 85 95 105 115 125
Mean diffu
sivity (M
D)
BSID-‐III Cogni;ve Score
ST Gyrus (lew)
Figure 2. DTI of the (A) external capsule FA (B) retrolenNcular capsule FA, and (C) lew superior temporal gyrus MD, in relaNon to BSID-‐III cogniNve score at 18-‐20 months among infants without BPD
A
B
C
A
P