Neonatal Respiratory Pathology nSigns and Symptoms nCommon (Major) Neonatal Diseases.
44
Neonatal Respiratory Pathology Signs and Symptoms Common (Major) Neonatal Diseases
-
Upload
charla-norton -
Category
Documents
-
view
224 -
download
4
Transcript of Neonatal Respiratory Pathology nSigns and Symptoms nCommon (Major) Neonatal Diseases.
Neonatal Respiratory Pathology
Signs and Symptoms Common (Major) Neonatal Diseases
Normal Neonatal Vital Signs
Smaller = faster Normal heart rate 120-160/minute Normal respiratory rate 40-60/minute Normal blood pressure– pre term 50/30 mm Hg
– increases with size
Signs & Symptoms of Respiratory Distress
Tachypnea Nasal flaring Expiratory grunting Retractions See saw breathing Central cyanosis (as opposed to
acrocyanosis) Apnea
Periodic Breathing vs Apnea
Periodic breathing– normal in preterm
– seen in 25 to 50% of all preterms
– cessation of breathing for 10 seconds with no changes
Apnea– cessation of breathing for 20 seconds with
changes
– deteriorating color, SaO2, bradycardia
Common Neonatal Respiratory Diseases
Hyaline Membrane Disease Transient Tachypnea of the Newborn Bronchopulmonary Dysplasia Meconium Aspiration Syndrome Persistent Fetal Circulation Retinopathy of Prematurity

Hyaline Membrane Disease
Abbreviated HMD Also known as RDS type I Seen in premature infants Caused by immature surfactant system
HMD Pathology
Restrictive lung disease
HMD Pathology
Restrictive lung disease Decreased lung compliance– increased elastic recoil
– increased surface tension
– increased work of breathing

HMD Pathology (cont.)
Atelectasis– decreased diffusion due to surface area
– Increased AaDO2 (aA ratio)
– increased intrapulmonary shunting (Qs/Qt)

HMD Pathology (cont.)
Atelectasis– decreased diffusion due to surface area
– Increased AaDO2 (aA ratio)
– increased intrapulmonary shunting (Qs/Qt)
Formation of hyaline membrane– decreased diffusion secondary to thickness
HMD Histology
Surfactant helps keep lung dry HMD, alveolar leakage Fluid rich in protein, fibrin, dying epithelial
cells Forms a hyaline membrane Membrane forms within first 24 to 48 hours Around 72 hours, phagocytosis begins
HMD Clinical Findings
Premature infant Grunting and retractions “Crash” within first 24 to 48 hours
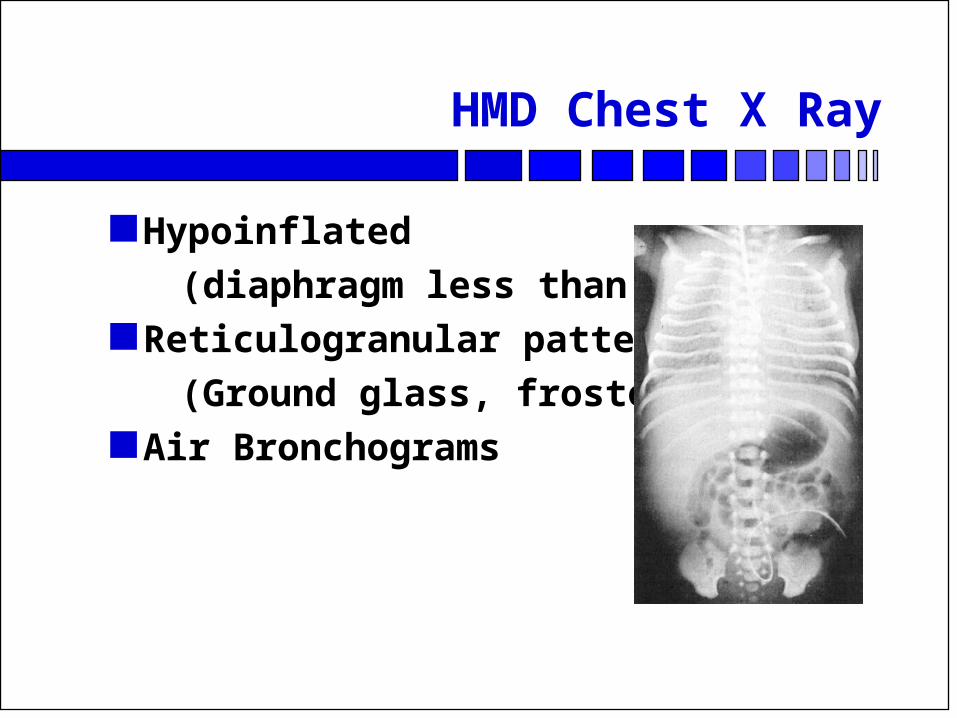
HMD Chest X Ray
Hypoinflated
(diaphragm less than 8 ribs) Reticulogranular pattern
(Ground glass, frosted glass) Air Bronchograms
HMD Treatment
Artificial Surfactants “Textbook Management”– Increasing Severity - Hood O2 to CPAP to Vent
–Weaning - Vent to CPAP to Hood
Disease runs course 5 to 7 days
Transient Tachypnea of the Newborn
Also known as RDS type II Also known as Wet Lung Syndrome Abbreviated as TTN, TTNB Seen in infants delivered via C sections A disease of retained Fetal Lung Liquid
TTNB Pathology
Interstitial edema Increased Raw (until fluid absorbed)
TTNB Clinical Findings
C-section infants Good Apgars at birth Mild hypoxemia within first 24 hours
TTNB Chest X Ray
Lymphatic engorgement
(white strings) Hyperinflation
(diaphragm greater than 10 ribs)
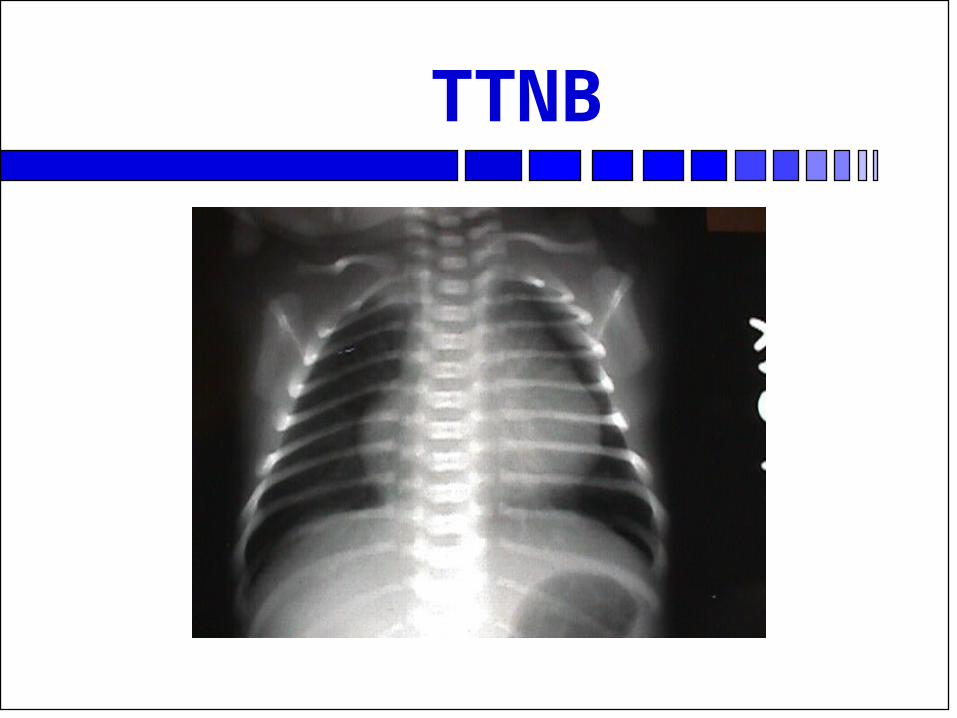
TTNB
TTNB Treatment
Hood O2 within first 24 to 48 hours Infant on room air
Bronchopulmonary Dysplasia
Abbreviated as BPD Obstructive disease Definition - O2 useage, 28 days post partum Causitive factors:– O2
– Airway Pressure
– Time of exposure
BPD Pathology
Stage I - same as HMD
BPD Pathology
Stage I - same as HMD Stage II– occurs at 3 to 4 days
– alveolar necrosis, development of smooth muscle
BPD Pathology (cont.)
Stage III– continued smooth muscle development
– interstitial fibrosis
– emphysematous bullae
BPD Pathology (cont.)
Stage III– continued smooth muscle development
– interstitial fibrosis
– emphysematous bullae
Stage IV– around one month
– emphysema, interstitial fibrosis, pulmonary hypertension
Summary BPD Pathology
Increased Raw Areas of increased and decreased Clt Hyperinflated Interstitial edema many have PDA (L to R)

BPD Chest X Ray Stages
Stage I - HMD like Stage II - increased ‘white out’ Stage III - ‘sponge like’, bullae and white
out Stage IV - ‘honeycomb’
BPD Treatment
Supportive Steroids
Meconium Aspiration Syndrome
Abreviated as MA, MAS Meconium is infant stool Presence indicates delivery stress Found in approx. 10% of all deliveries
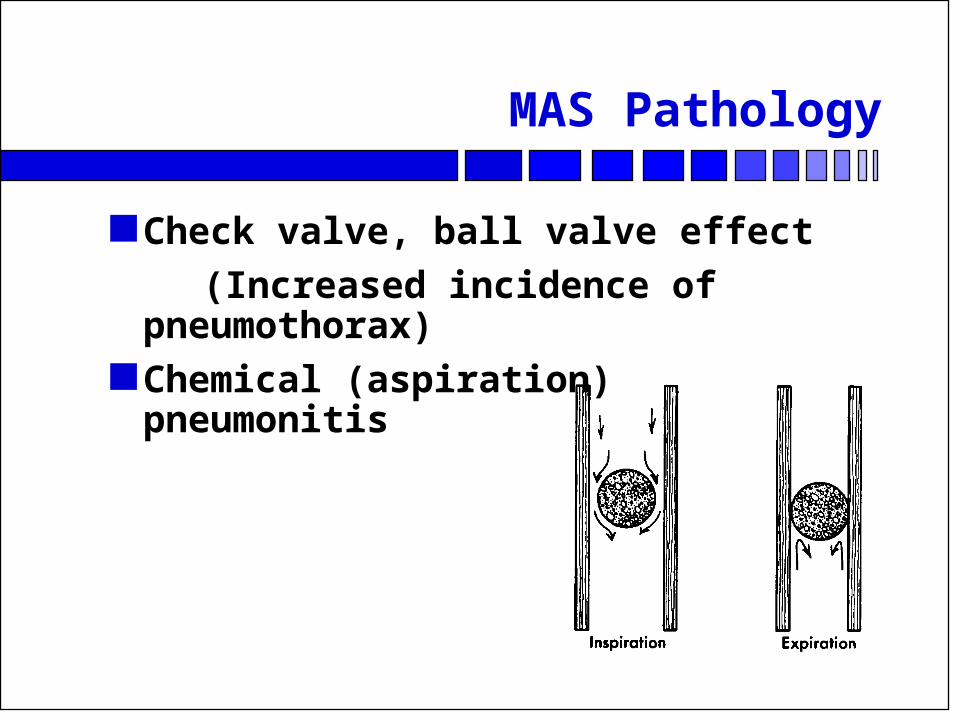
MAS Pathology
Check valve, ball valve effect
(Increased incidence of pneumothorax) Chemical (aspiration) pneumonitis
MAS Clinical Findings
Commonly post mature– larger infants
– long fingernails, peeling skin
Delivered through stained amniotic fluid Yellow or greenish nails, chord
MAS Chest X Ray
Increased patchy density Hyperinflation
MAS Treatment
Deep tracheal suctioning at birth Supportive Chest physiotherapy

Persistent Fetal Circulation
Also known as Persistent Pulmonary Hypertension of the Newborn
Abbreviated as PFC, PPH, PPHNB
Page 81, Whitaker ******Comprehensive Perinatal & Pediatric Respiratory Care*****
PFC Pathology
Continuance of Fetal Circulation post partum
R to L shunting through PDA R to L shunting through FO Severe hypoxemia
PFC Clinical Findings
Infants tend to be term Non responsive hypoxemia Right sided PaO2 (preductal) 15 torr higher
than left

Differential Diagnosis of PFC
Hyperoxia test (100% hood)– PaO2 > 100 is lung disease
– PaO2 = 50 to 100 is either lung or heart disease
– PaO2 < 50 is fixed right to left shunt

Differential Diagnosis of PFC (cont.)
If fixed R to L shunt is suspected– Obtain pre and post ductal PaO2
– Difference < 15 torr, no ductal shunting
– Difference > 15 torr, ductal shunting present

Differential Diagnosis of PFC (cont.)
Perform Hyperoxic - Hyperventilation Test– Hyperventilate with 100% O2 until PaCO2 20
to 25 torr
– If PaO2 > 100 torr, then PFC is present
– If PaO2 < 100 torr, then congenital heart disease

PFC Treatment
High vent settings (shoot for PaCO2 20-25 torr)
? Paralysis Allow PaO2 to be 80 to 100 torr Use vasodilator Priscolene (Tolazoline)
– Nitric Oxide
Use of ECMO
Retinopathy of Prematurity
Also known by older name of Retrolental Fibroplasia (RLF)
Page 303, Whitaker ******Comprehensive Perinatal & Pediatric Respiratory Care
Abbreviated as ROP Visual disturbances secondary to O2 use
ROP Pathology
Stage I - vascoconstrictive response of immature retinal vessels when PaO2 is increased
Stage II - (proliferative stage), new vessels form to oxygenate retina, retinal hemorrhage
Causative Factors of ROP
PaO2 Retinal Maturity Duration of Hyperoxia

ROP Treatment
Closely monitor PaO2 or SaO2 Closely monitor FiO2 ‘Cryo’ therapy Ophthalmic examination at discharge