neonatal Jaundice
43
-
Upload
babylon-medical-college -
Category
Health & Medicine
-
view
349 -
download
7
Transcript of neonatal Jaundice
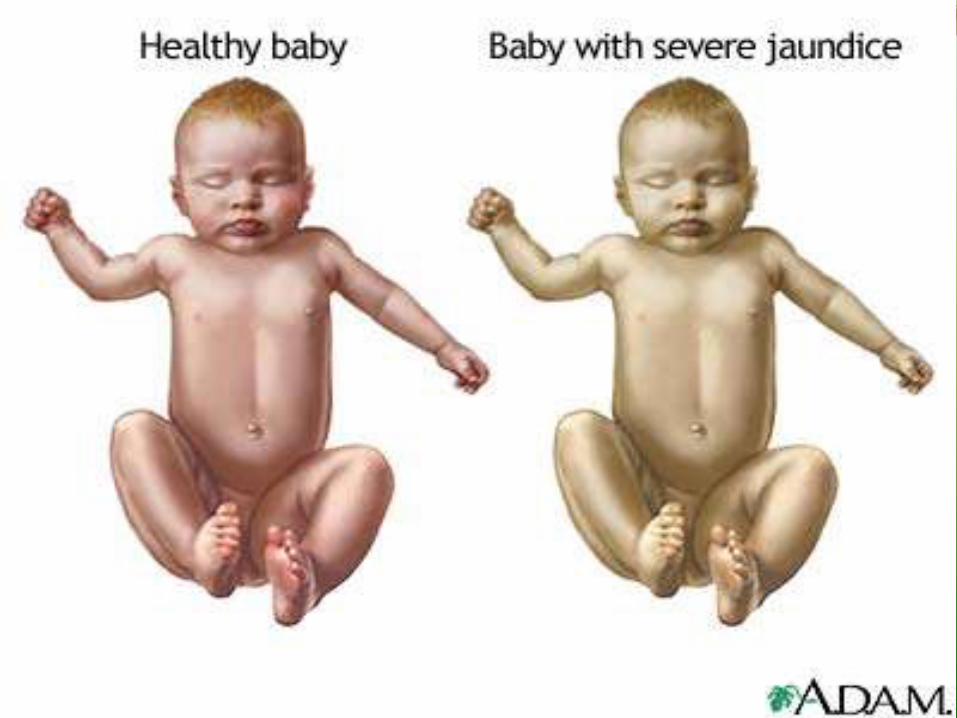
INTRODUCTIONDefinition: Hyperbilirubinemia refers to an excessive level of bilirubin in the blood and is characterized by a yellowish discoloration of the skin, sclerae, mucous membranes and nails.
Occurs in 60% of term and 80% of preterm neonates
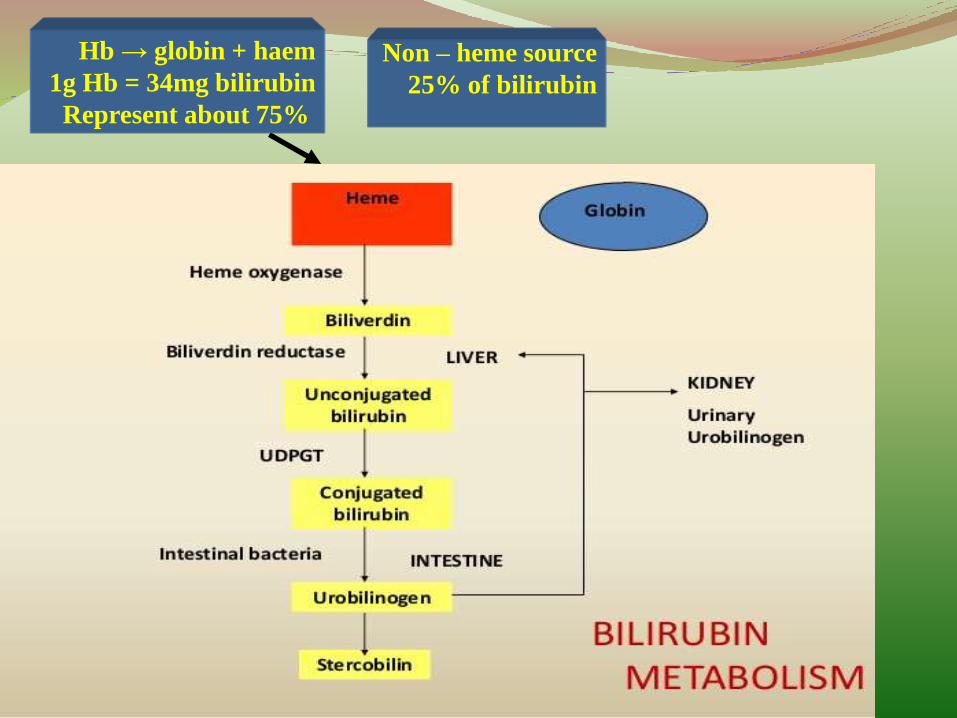
Bilirubin is the end product of heme degradation
Most of the daily production comes from the breakdown of RBCs in the RES
Heme biliverdin bilirubin
Bilirubin is released & bound to serum albumin
Bilirubin is uptake & conjugated with glucuronic acid
Finally conjugated bilirubin is excreted in bile
Bilirubin
Non – heme source
25% of bilirubin
Hb → globin + haem
1g Hb = 34mg bilirubin
Represent about 75%
Normally s. bilirubin level vary between 0.3 - 1.2mg/dl. A bilirubin level of more than 2 mg/dl manifest biochemically where as level of >5 mg/dL manifests clinically in neonates
UNCONJUGATED B.
1- Insoluble in water can not be excreted in urine
2-Tightly compounded to s. albumin
3- Toxic
CONJUGATED B.
1-Water soluble& can be excreted in urine
2- Loosely bound to albumin.
3-Non toxic
RISK FACTORS FOR DEVELOPMENT OF SEVERE HYPERBILIRUBINEMIAIN INFANTS ≥35 WEEKS OF GESTATION
MAJOR RISK FACTORS
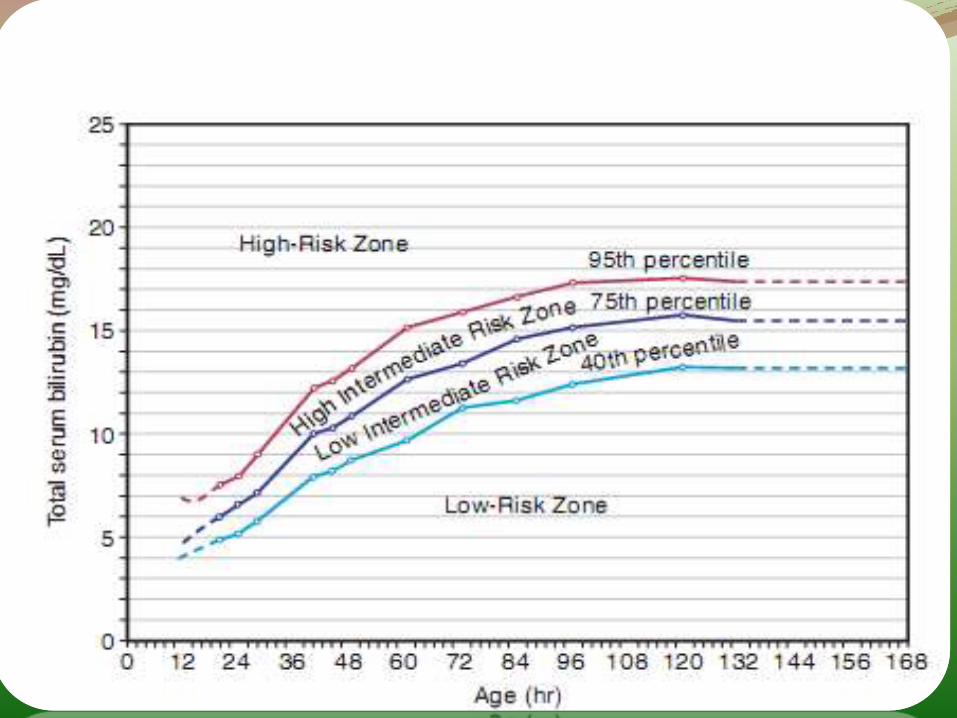
1-Predischarge TSB or TcB level in the high-risk zone
2-Jaundice observed in the frst 24 hr
3-Blood group incompatibility with positive direct coombs test,other known hemolytic disease (glucose-6-phosphatedehydrogenase defciency).
4-Gestational age 35-36 wk
5-Previous sibling received phototherapy
6-Cephalohematoma or signifcant bruising
7-Exclusive breast-feeding, particularly if nursing is not going welland weight loss is excessive
8-East Asian race*
MINOR RISK FACTORS
1-Predischarge TSB or TcB level in the high intermediate-risk zone
2-Gestational age 37-38 wk
3-Jaundice observed before discharge
4-Previous sibling with jaundice
5-Macrosomic infant of a diabetic mother
6-Maternal age ≥25 yr
7-Male gender
DECREASED RISK (these factors are associated with decreased risk of
signifcant jaundice)
1-TSB or TcB level in the low-risk zone
2-Gestational age ≥41 wk
3-Exclusive bottle-feeding
4-Black race
5-Discharge from hospital after 72 hr
Etiology:1- increases the load of bilirubin to be metabolized by the liver
(hemolytic anemias, polycythemia, bruising or internal hemorrhage, shortened red blood cell life as a result of immaturity or transfusion of cells, increased enterohepaticcirculation, infection)
2-damages or reduces the activity of the transferaseenzyme or other related enzymes (genetic defciency, hypoxia, infection thyroid defciency)
3- competition for blockage of the transferase enzyme (drugs and other substances requiring glucuronic acid Conjugation)
4- absence or decreased amounts of the enzyme or reduction of bilirubin uptake by liver cells (genetic defect, and prematurity).
5-hypoproteinemia
6- displacement of bilirubin from its binding sites on albumin by competitive binding of drugs such as Sulfafurazole and moxalactam, acidosis, and increased free fatty acid concentration secondary to hypoglycemia, starvation, or hypothermia.
Types of jaundice
In new born babies bilirubin metabolism is immature which results in the occurrence of hyperbilirubinemia in the first few days of life.
Many factors are implicated:
1-increased destruction of RBC
2-increase enterohepatic circulation
3-decreased ability of the liver to conjugate bilirubin
4-decreased uptake by the liver due to low level of ligandin
Characteristics of Physiological Jaundice
1-First appears between hours of age
2-Maximum intensity seen on 4-5th day in term and 7th day in preterm neonates
3-Does not exceed 15 mg/dl
4-Clinically undetectable after 14 days.
5-No treatment is required but baby should be observed closely for signs of worsening jaundice.
6- does not rise more than 5mg/dl/day
1-Appears within 24 hours of age
2-Increase of bilirubin > 5 mg / dl / day
3-Serum bilirubin > 15 mg / dl
4-Jaundice persisting after 14 days
5-Stool clay / white colored and urine staining clothes yellow
6-Direct bilirubin> 2 mg / dl
Causes of jaundice:
Appearing within 24 hours of age
1-Hemolytic disease of NB : Rh, ABO
2-Infections: TORCH, malaria, bacterial
3-G6PD deficiency
4-thalassemia
5-spherocytosis
Appearing between 24-72 hours of life
1-Physiological
2-Sepsis
3-Polycythemia
4-Intraventricular hemorrhage
5-Increased entero-hepatic circulation
After 72 hours of age
1-Sepsis
2-Cephalhaematoma
3-Neonatal hepatitis
4-Extra-hepatic biliary atresia
5-Breast milk jaundice
Causes of prolonged jaundice:
A-unconjugated hyperbilirubinemia1-Breast feeding jaundice
In exclusively breast feed infants
Appears at 24-48 hrs of age
Occur during first wk of life
Disappears by 3rd week
Its related to inadequate B.F
T/t:Proper & adequate B.F
2-Breast milk jaundice
In 2-4 % EBF babies after the 7th day of life
SBr>10mg/dl beyond 3rd-4th week
Should be differentiated from Hemolytic jaundice, hypothyroidism, G6PD def
T/t: Some babies may require PT
Continue breast feeding
Usually declines over a period of time
3-congenital hypothyroidism
4-spsis
5-intestinal stasis, hirschsprung dz, meconium ileus
6-criggler najjar syndrome
B-conjugated hyperbilirubinemia: fraction >10% of total SBR
1-infection
2-galactosemia, fructosemia, tyrosinemia
3-cystic fibrosis
4-dubin johnson syndrome
5-rotors syndrome
6-ideopathic neonatal hepatitis
7-alpha 1 anti-trypsin def.
8-hypothyroidism, hypopitutarism
9-biliary atresia
Kernicterus
Kernicterus is a neurologic syndrome resulting from the deposition of unconjugated (indirect) bilirubin in the basal ganglia and brainstem nuclei. There is neuronal loss ,necrosis & giliosis .The pathogenesis of kernicterus is multifactorial and involves an interaction between unconjugated bilirubin levels, albumin binding and unbound bilirubin levels, passage across the blood-brain barrier, and neuronal susceptibility to injury
Brain damage caused by bilirubin depends on:
1-level of s.bilirubin & albumin
2-bilirubin binding by albumin
3-status of BBB
4-susceptibility of the CNS
Risk factor for kernicterus:
1-asphyxia
2-acidosis
3-hypoglycemia
4-prematurity
5-severe hyperbilirubinemia
6-G6PD def.
7-Crigler-Najjar syndrome type I
8-Gilbert's syndrome
CLINICAL FEATURES OF KERNICTERUS
ACUTE FORM
Phase 1 (1st 1-2 days): poor suck, stupor, seizures
Phase 2 (middle of 1st wk): hypertonia of extensormuscles, opisthotonus, fever, high pitched cry, retracted neck
Phase 3 (after the 1st wk): hypotonia
CHRONIC FORM
1st year: hypertonia, active deep tendon refexes, delayed motor skills
After 1st yr: movement disorders (choreoathetosis,ballismus, tremor), upward gaze, sensorineuralhearing loss, dental dysplasia , MR
preventable causes of kernicterus: (1) early discharge (<48 hr) with no early follow-up (within 48 hr of discharge); this problem is particularly important in near-term infants (35-37 wk of gestation); (2) failure to check the bilirubin level in an infant noted to be jaundiced in the first 24 hr; (3) failure to recognize the presence of risk factors for
hyperbilirubinemia; (4) underestimation of the severity of jaundice by clinical (visual) assessment; (5) lack of concern regarding the presence of jaundice; (6) delay in measuring the serum bilirubin level despite marked jaundice or delay in initiating phototherapy in the presence of elevated bilirubin levels; (7) failure to respond to parental concern regarding jaundice, poor feeding, or lethargy
historyonset / duration
pain
nausea & vomiting
loss of weight
itching
color of stool
color of urine
past history
family history

examinationcolor of skin
severity of jaundice
anemia
liver
spleen
gall bladder
Ascites
Rash or petechiae
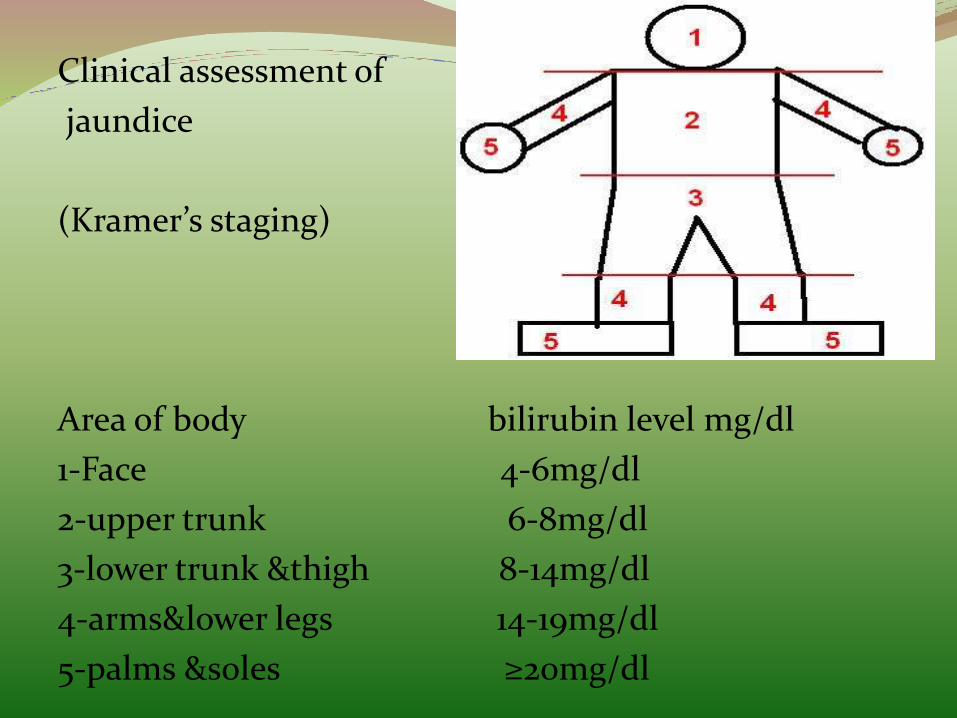
Clinical assessment of
jaundice
(Kramer’s staging)
Area of body bilirubin level mg/dl
1-Face 4-6mg/dl
2-upper trunk 6-8mg/dl
3-lower trunk &thigh 8-14mg/dl
4-arms&lower legs 14-19mg/dl
5-palms &soles ≥20mg/dl
Investigation: it depend on the suspected cause and include
1- s. bilirubin (total, direct ,indirect)
2-ABO & Rh of baby and mother
3-Hb ,retic. , blood film
4-coombs test, G6PD assay
5-blood culture
6-TORCH screen
7-LFT
8-blood sugar
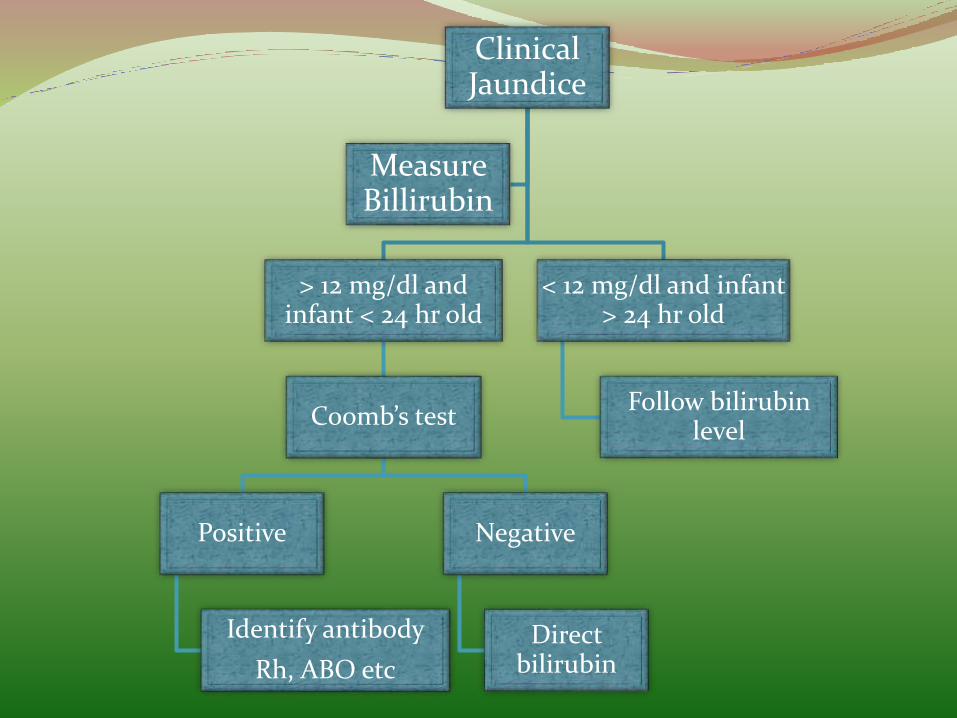
Clinical Jaundice
> 12 mg/dl and infant < 24 hr old
Coomb’s test
Positive
Identify antibody
Rh, ABO etc
Negative
Direct bilirubin
< 12 mg/dl and infant > 24 hr old
Follow bilirubinlevel
Measure Billirubin
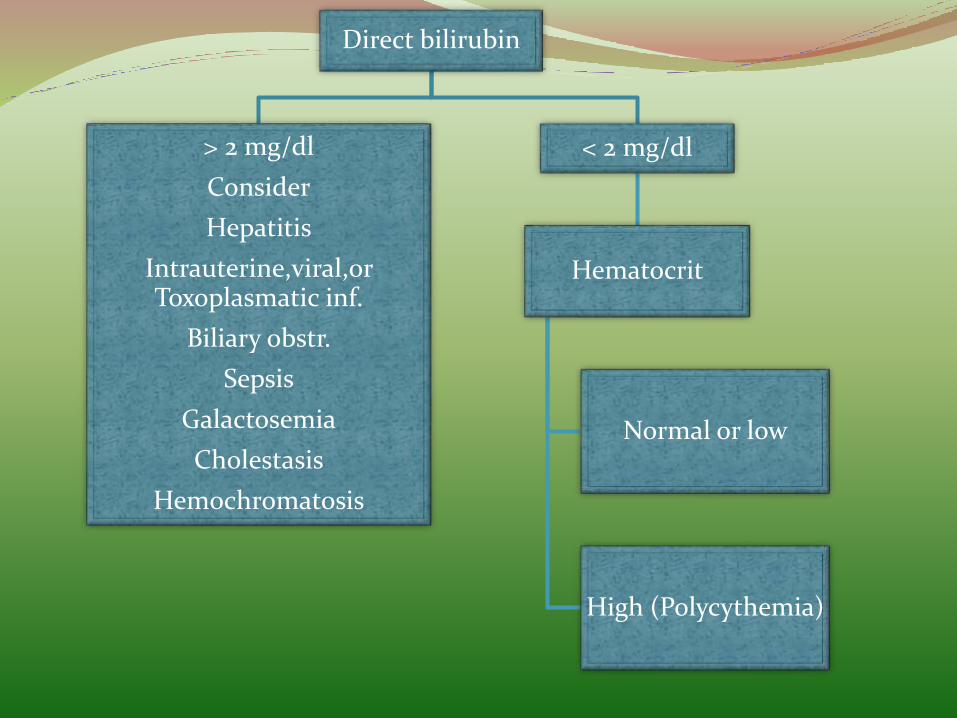
Direct bilirubin
> 2 mg/dl
Consider
Hepatitis
Intrauterine,viral,orToxoplasmatic inf.
Biliary obstr.
Sepsis
Galactosemia
Cholestasis
Hemochromatosis
< 2 mg/dl
Hematocrit
Normal or low
High (Polycythemia)
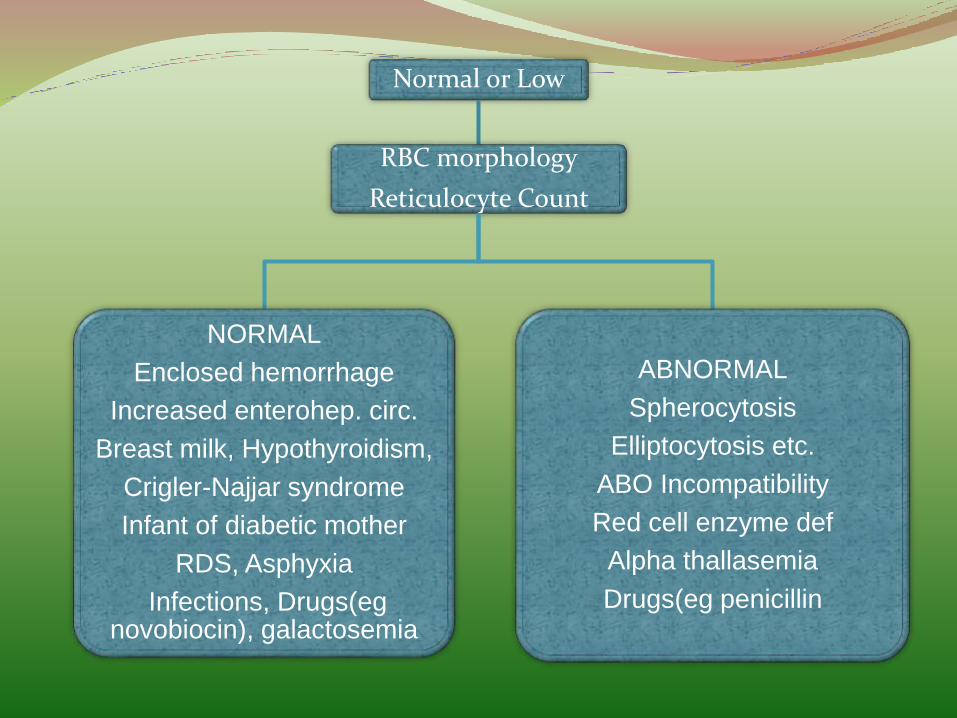
Normal or Low
RBC morphology
Reticulocyte Count
NORMAL
Enclosed hemorrhage
Increased enterohep. circ.
Breast milk, Hypothyroidism,
Crigler-Najjar syndrome
Infant of diabetic mother
RDS, Asphyxia
Infections, Drugs(egnovobiocin), galactosemia
ABNORMAL
Spherocytosis
Elliptocytosis etc.
ABO Incompatibility
Red cell enzyme def
Alpha thallasemia
Drugs(eg penicillin
Prevention:
1-promote&support breastfeeding
2-perform a thorough risk assessment for all infant
3-provide parents with written & verbal inform. About newborn jaundice
4-provide appropriate follow-up
5-identify preterm infant and provide close monitoring
6-interpret all bilirubin levels according to infant age in hours
7-establish nursery protocols for identifying & evaluating hyperbilirubinemia
8-recognize that visual assessment of bilirubin levels is inaccurate
9-measure bilirubin levels in all infants with jaundice in the first 24 hours after delivery
10-treat newborns as indicated with physiotherapy or exchange transfusion
TreatmentPurposes:
1- reduce level of serum bilirubin and prevent bilirubintoxicity
2-Prevention of hyperbilirubinemia: early feeds, adequate hydration
Reduction of bilirubin levels either by phototherapy or exchange transfusion
Phototherapy: refers to the use of light to convert bilirubinmolecules in the body into water soluble isomers that can be excreted by the body. Bilirubin absorb light in the blue range wavelength(420-470nm)
Phototherapy reduce bilirubin level about 2-3mg/dl per day .But intensive phototherapy can reduce level of bilirubinby 10mg/dl per day
The therapeutic effect of phototherapy depends on: 1- the light energy emitted in the effective range of wavelengths 2-the distance between the lights and the infant 3-and the surface area of exposed skin 4-the rate of hemolysis
5- the intensity of light
6-hydration

Serum bilirubin levels and hematocrit should be monitored every 4-8 hr in infants with hemolytic disease and those with bilirubin levels near toxic range for the individual infant. Serum bilirubin monitoring should continue for at least 24 hr after cessation of phototherapy.
Complication: 1-loose stools, erythematous macular rash, purpuric rash
2-overheating, dehydration (increased insensible water loss, diarrhea) 3-hypothermia from exposure
.
4-bronze baby syndrome occurs in the presence of direct hyperbilirubinemia , The term bronze baby syndrome refers dark, grayish brown skin discoloration in infants undergoing
phototherapy. Almost all infants observed with this syndrome have had signifcant elevation of direct-reacting bilirubin and other evidence of obstructive liver disease. The discoloration may be due to photo-induced modifcation of porphyrins
5-skin damage
6- skin rash
7-damage to immature retina
8-blocked nose
9- hypocalcemia
10- decrease LV output which lead to decrease renal perfusion
11- agitation & distress
B-exchange transfusion:
Double-volume exchange transfusion is performed if intensive phototherapy has failed to reduce bilirubinlevels to a safe range and if the risk of kernicterus exceeds the risk of the procedure. ET replace 85% of infant blood & reduce bilirubin level by 50%. It should be used for any newborn with a total serum bilirubin of greater than 428 μmol/l ( 25 mg/dL )
Complication:
A-early complication:
1-metabolic acidosis 2-electrolyte abnormalities 3-hypoglycemia 4-hypocalcemia
5-thrombocytopenia 6-volume overload
7-arrhythmias 8-NEC, infection
B-late complication:
1-late onset anemia
2-GVH disease
3- portal hypertension & portal vein thrombosis
4- inspissated bile syndrome
Other therapy:
1-intravenous immunoglobulin: 500mg/kg especially in coombs +ve test
2-Metalloporphyrins: The mechanism of action is competitive enzymatic inhibition of conversion of hemeprotein to biliverdin. A single intramuscular dose on the 1st day of life may reduce the need for subsequent phototherapy. particularly in patients with ABO incompatibility or G6PD defciency.
Complications from metalloporphyrins include transient erythema if the infant is receiving phototherapy
C-phenobarbital: promote liver enzymes and protein synthesis to induce hepatic bilirubin metabolism
D-protoporphyrin: inhibit conversion of biliverdin to bilirubin by heme oxygenase
PrognosisEarly recognition and treatment of hyperbilirubinemia prevents severe brain damage. But brain damage due to kernicterusremain a devastating event
THANKS FOR LISTENING
Presented by:
Haider Faroon