Neck Pain. What is in… Cervical spondylosis Cervical spondylitis Cervical spondylolisthesis/disk...
70
Neck Pain
-
Upload
ella-maxwell -
Category
Documents
-
view
236 -
download
4
Transcript of Neck Pain. What is in… Cervical spondylosis Cervical spondylitis Cervical spondylolisthesis/disk...

Neck Pain

What is in…
• Cervical spondylosis
• Cervical spondylitis
• Cervical spondylolisthesis/disk bulges

• What is it?• Causes• Risk factors• Symptoms• Signs• Complications• Tests• Pharmacological/surgical management• Physiotherapy management
Cervical Spondylosis

• CS is a disorder in which there is abnormal wear on the cartilage and bones of the cervical vertebrae
• A common cause of chronic neck pain

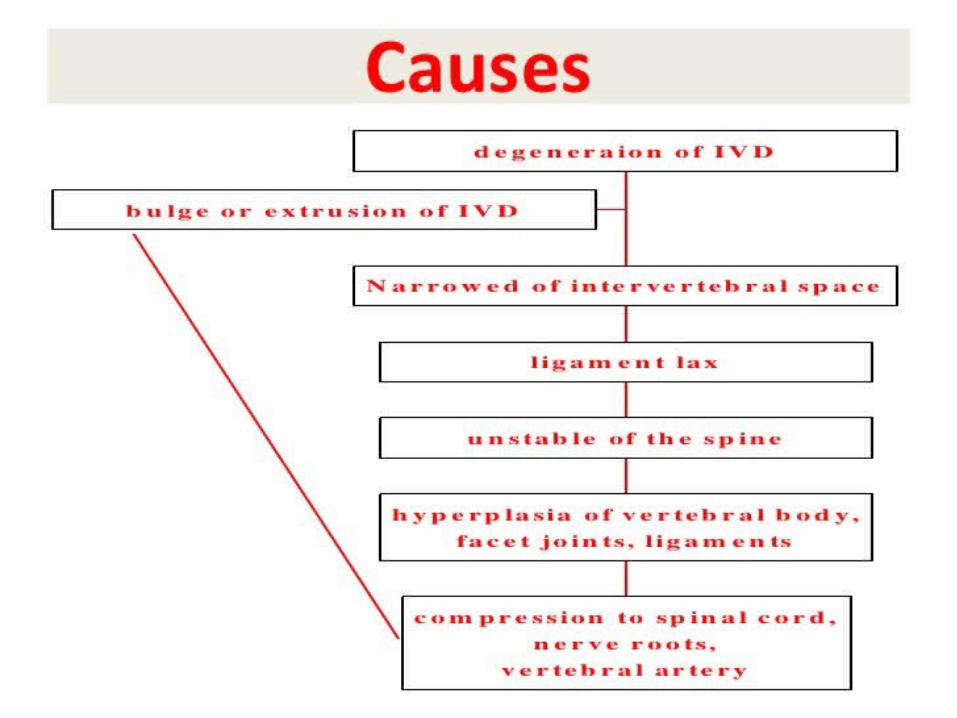
Causes
• CS is caused by chronic wear on the cervical spine• This includes the disks
between the neck vertebrae and the joints between the bones of the cervical spine
• There may be abnormal growths or "spurs" on the vertebrae

• These changes can, over time, compress one or more of the nerve roots. In advanced cases, the spinal cord becomes involved
• Everyday wear and tear may start these changes
• People who are very active at work or in sports may be more likely to have them

Risk factors
• The major risk factor is aging {by age 60, most women and men (men>women) show signs of CS on x-ray}
• Being overweight and not exercising• Having a job that requires heavy lifting or a lot of
bending and twisting• Past neck injury (often several years before)
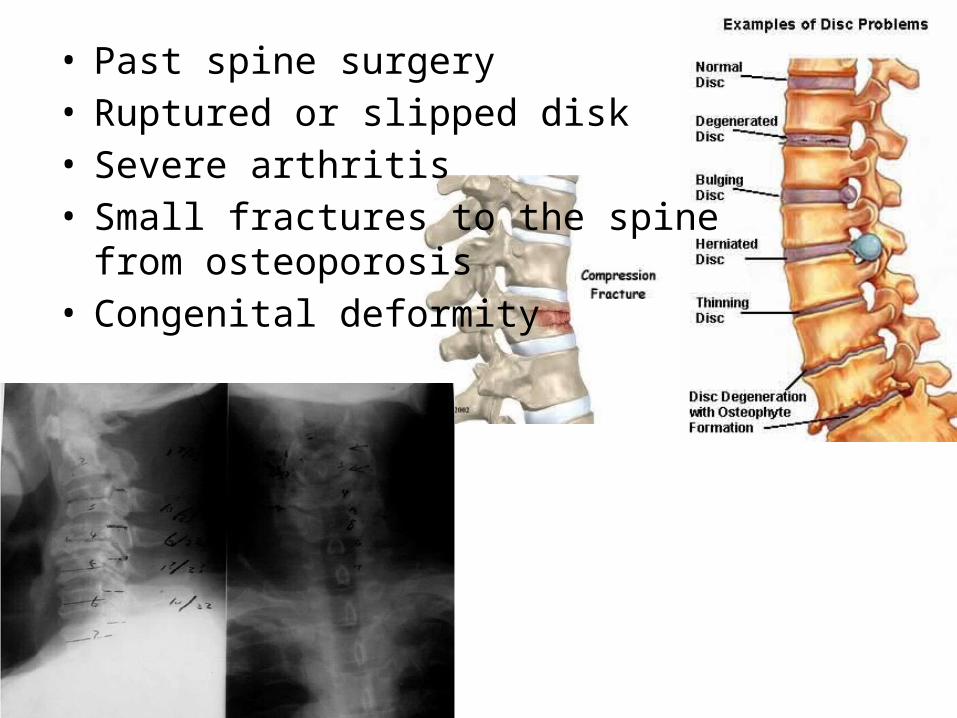
• Past spine surgery• Ruptured or slipped disk• Severe arthritis• Small fractures to the spine
from osteoporosis• Congenital deformity

Symptoms
• Neck or shoulder pain, stiffness of the neck, and difficulty turning or bending the neck from side-to-side
• Symptoms may get worse with turning, extending, or bending the neck
• Pain that shoots down the arm, and numbness, weakness, or pains in the arm
• Muscles spasm and popping sound near the neck

• Symptoms are caused by imposition on the spinal cord or the nerves as they exit the spine, or both
• A stiff neck is most often one of the very first signs• Neck stiffness tends to grow progressively worse over
time• Radiating pain (stabbing, burning, or dull ache) to the
bottom of the skull and/or to the shoulder and down the arm
• Can be accompanied by paresthesias and muscle weakness in the neck, shoulders, arms, and hands; numb, clumsy hands syndrome
Patterns of CS
• Radicular pattern• Vertebral artery pattern• Myelopathy pattern• Sympathetic pattern• Combination pattern

Pathology – radicular pattern
• Posterolateral protrusion of the cervical disc• Hyperplacia, hypertrophy of the facet joint• Stimulate or compress nerve roots as they emerge
from the cord to pass peripherally through the intravertebral foramen


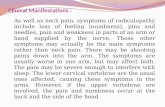
Clinical manifestation
• Symptoms– Neck pain: radiating to the ipsilateral upper extremity– Paresthesia– Muscle weakness in appropriate distribution
• Pain and paresthesia may be intensified by neck movement, especially by extension or lateral flexion to the side of the herniation
• May be improved by traction on the neck

• Signs– Stiffness of the neck– Tenderness, spasm of paraspinous muscles– Limitation of active and passive motion of the neck and
affected upper extremity

Radiographic studies
Pathology – myelopathy pattern
• Midline herniation of nucleus pulposus• Osteophyte of posterior rims of vertebral body• Hyperplasia of the ligamentum flavum• Calcification of the posterior longitudinal ligament
• These all lead to compression of the spinal cord

Clinical manifestation
• Symptoms– Weakness– Loss of balance– Cannot handle small objects– Neck pain not obvious– Numbness– Dysfunction of upper motor neuron is gradually present
from the lower part of the body to the upper– Spastic paraplegia or quadriplegia– Loss of control of the bladder or bowels
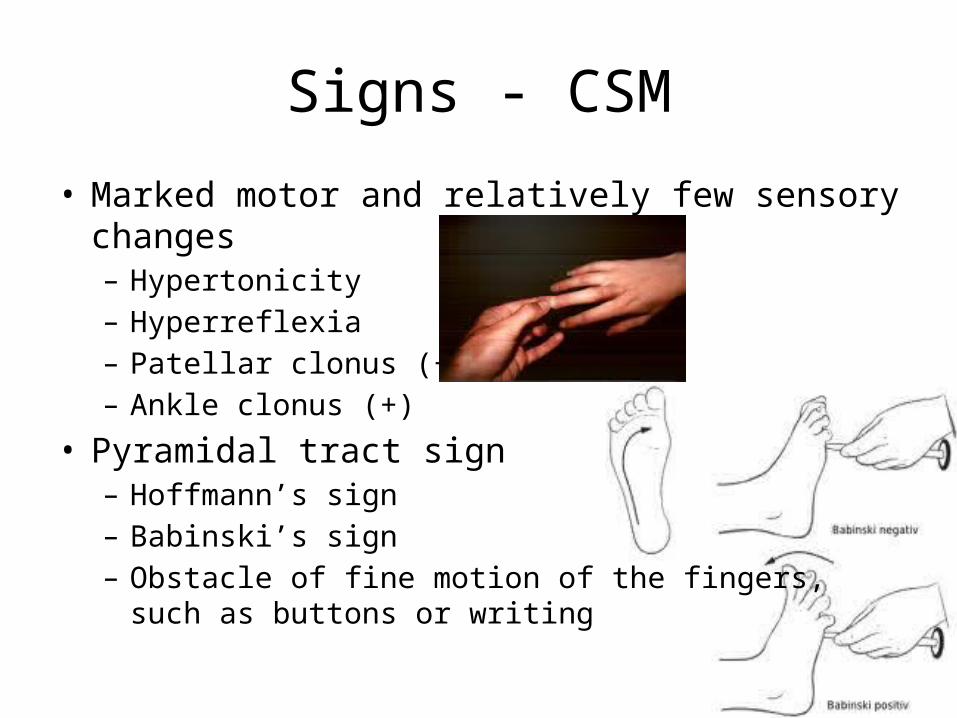
Signs - CSM
• Marked motor and relatively few sensory changes– Hypertonicity– Hyperreflexia– Patellar clonus (+)– Ankle clonus (+)
• Pyramidal tract sign– Hoffmann’s sign– Babinski’s sign– Obstacle of fine motion of the fingers,
such as buttons or writing

Calcification of the posterior longitudinal ligament

MRI
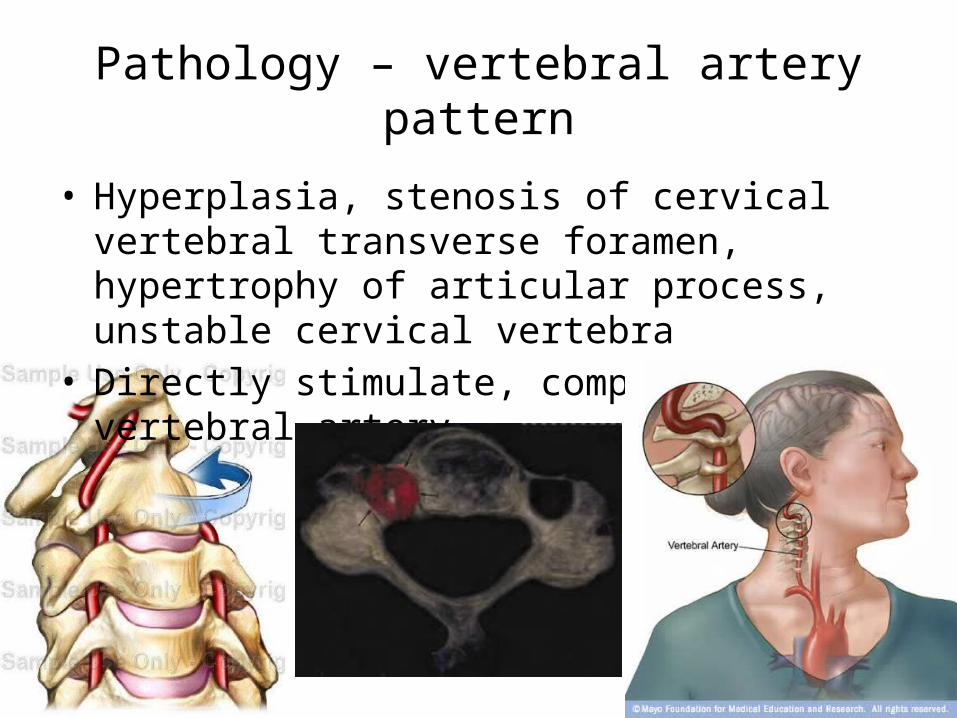
Pathology – vertebral artery pattern
• Hyperplasia, stenosis of cervical vertebral transverse foramen, hypertrophy of articular process, unstable cervical vertebra
• Directly stimulate, compress vertebral artery

Clinical manifestation
• Symptoms– Vertigo is main, induced by rotating neck– Migraine– Sudden blackout/diplopia, recovered in a short time– Cataplexy caused by sudden spasm of artery due to
stimulation, come to normal at once after falling to the ground
• Sign– Positive neck rotation test
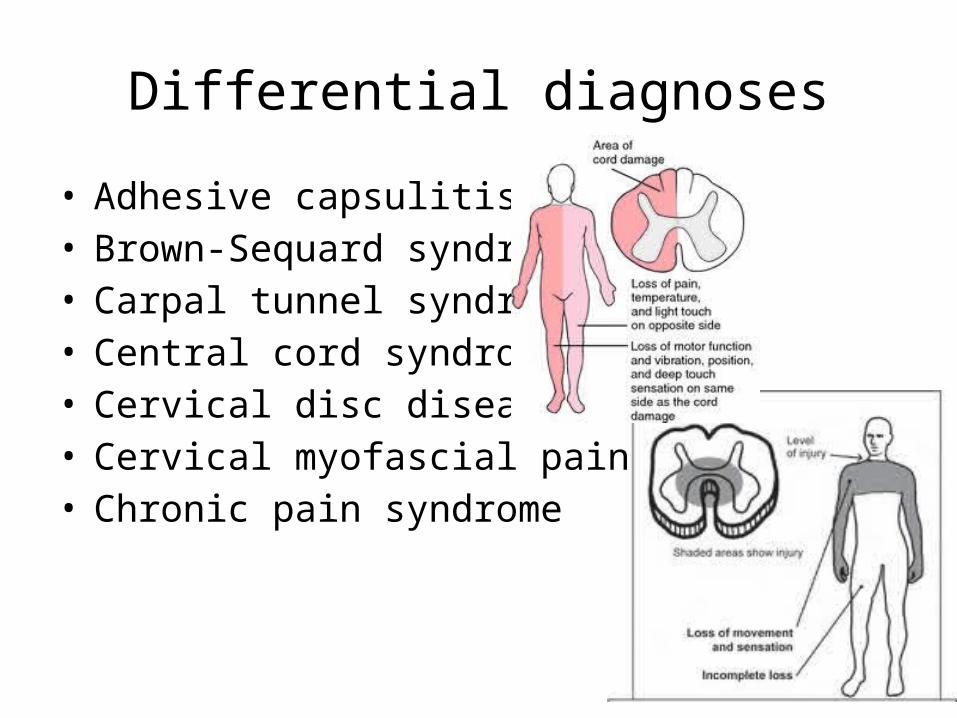
Differential diagnoses
• Adhesive capsulitis• Brown-Sequard syndrome• Carpal tunnel syndrome• Central cord syndrome• Cervical disc disease• Cervical myofascial pain• Chronic pain syndrome

• Diabetic neuropathy• Multiple sclerosis• Myofascial pain• Neoplastic brachial plexopathy• Osteoporosis and spinal cord injury• Radiation-induced brachial plexopathy• Rheumatoid arthritis• Traumatic brachial plexopathy

Signs – summary
• An examination may show that patient has trouble moving head toward shoulder and rotating head
• Ask patient to bend head forward and to the sides while putting slight downward pressure on the top of the head - increased pain or numbness during this test is usually a sign that there is pressure on a nerve in patient’s spine
• Weakness or loss of feeling can be signs of damage to certain nerve roots or to the spinal cord (reflexes are often reduced)

Special tests
• Cervical range of motion– The patient is seated and cervical rotation is measured with a standard
goniometer– Considered positive if the patients ipsilateral cervical rotation is less
than 60°
• Upper limb tension test– Considered positive if:– 1) Symptoms are reproduced– 2) Side-to-side differences in elbow extension are greater than 10°– 3) If contralateral lateral flexion of the cervical spine increases
symptoms or ipsilateral lateral flexion decreases symptoms

Upper limb tension test
• Axial loading– Spurling maneuver– Lateral flexion and extension of the neck, and then axial pressure on
the spine
• Neck distraction/axial manual traction test– One hand under the patient’s chin and the other hand around the
occiput, then slowly lift the patient’s head as axial traction force is gradually applied up to 30 pounds
– Positive if the pain is relieved when the head is distracted
• Shoulder abduction– Place the hand of the affected extremity on the head– A positive response is alleviation of patient symptoms
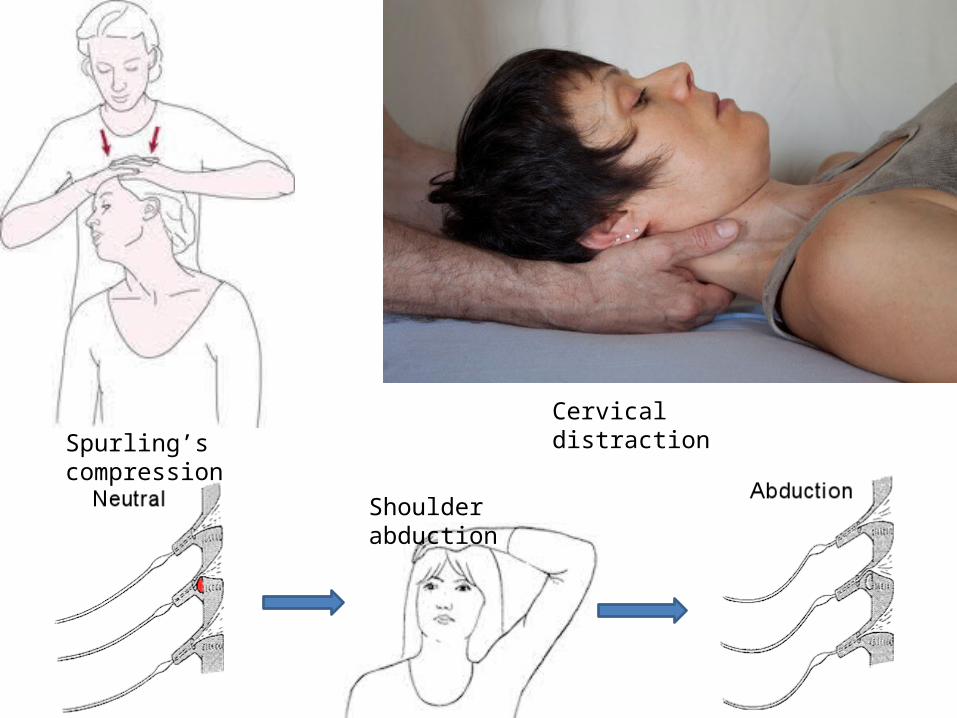
Spurling’s compressionCervical distraction
Shoulder abduction

Sensitivity & Specificity Of Tests - (according To Viikari-Juntura et al)
Test Position Sensitivity Specificity
Spurling Compression
Seated 40-60% 92-100%
Shoulder Abduction
Seated 43-50% 80-100%
Neck Distraction
Supine (10-15kg)
40-43% 100%

Other special tests
1. Tension arm test2. Percussion head test3. Jackson test4. Compression shoulder test
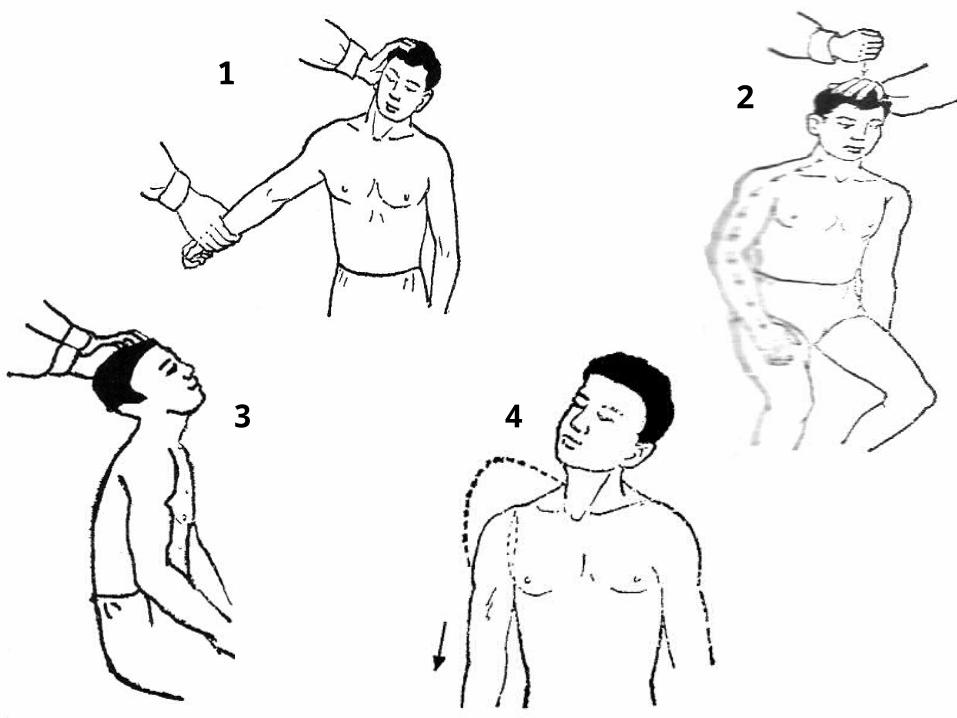
12
3 4

Vertebrobasilar circulation assessment
• Vascular Insufficiency may be aggravated by positional change in the cervical spine
• Assessment of the vertebrobasilar circulation must be done if cervical adjustment or manipulation is to be performed
• Positional change in the cervical spine compresses the vertebral artery at the atlantoaxial junction on the side opposite of rotation

Testing
• Barre-Lieou sign• Maigne’s test• Dekleyn’s test• Hautant’s test• Underburg’s test• Hallpike’s maneuver

Complications
• Chronic neck pain• Progressive loss of muscle function or feeling• Poor balance• Permanent disability (occasionally)• Use of a neck brace to immobilize the neck• Inability to retain feces• Urinary incontinence

Diagnostic tests - Imaging
• Neck x-ray (lateral)– Bony outgrowths at the margin of the joints– Reduced space between the vertebrae of neck– Narrowed opening between the bones
• CT scan• MRI of the neck (when there is severe pain, weakness, numbness)
– Loss of normal curvature of neck– Vertebral bone canal diameter is decreased– Spinal canal is narrowed

Cervical x-ray




Cervical MRI

Nerve function tests - Diagnostic tests
• Electromyelogram (EMG)• Nerve conduction velocity test

Pharmacological/surgical management
• Treatment is aimed at relieving pain and preventing permanent spinal cord and nerve root injury
• Treatments include:– Anti-inflammatory medication (NSAIDs)– Cortisone injections– Narcotics or opioids (if pain is very severe)– Cognitive behavioral therapy (talk therapy) may be helpful
if the pain is having a serious impact on life (helps better understand pain and teaches how to manage it)
– Surgery to remove bone and disc tissue to relieve the pressure on the nerves or spinal cord (foraminotomy, laminectomy, spinal fusion)
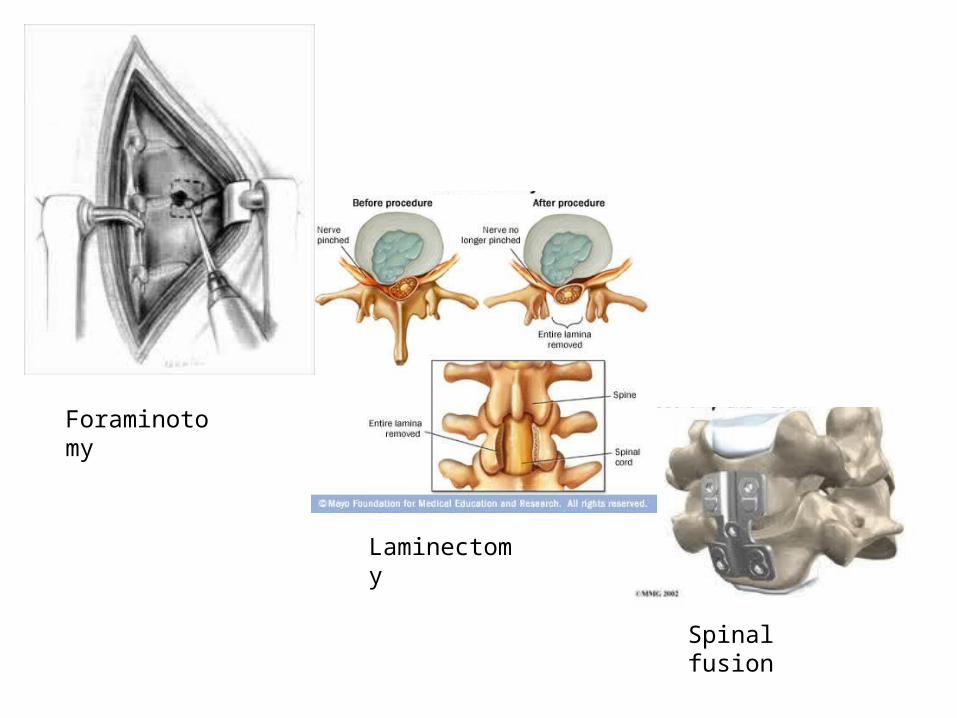
Spinal fusion
Laminectomy
Foraminotomy

Physiotherapy management
• Cervical traction• Postural education• Exercises– Stretching– Strengthening
• Manual therapy• Cold packs and heat therapy




















Tips to a healthier neck
• Always stretch before exercise or other strenuous physical activity
• At home or work, make sure the work surface is at a comfortable height
• Don’t lean when standing or sitting. When standing keep the weight balanced on the feet.
• Sit in a chair with good lumbar support and proper position and height for the task. Keep the shoulders back. Switch sitting positions often and periodically walk around the office or gently stretch muscles to relieve tension. If one must sit for a long period of time, rest the feet on a low stool.
• Wear comfortable, low heeled shoes.• Avoid weight lifting in poor postures.• Sleep on the side to reduce ay curve in the spine.
Always sleep on a firm surface.• Maintain proper nutrition and diet to reduce and
prevent excessive weight. A diet with sufficient daily intake of calcium, phosphorus, and vitamin D helps to promote proper bone growth.
• If one smokes, quit smoking. Smoking reduces blood flow to the spine and causes the spinal discs to degenerate.
• Avoid excessive stress. Stress will also contribute to the pain intensity.

References
• Google images• A.D.A.M. Medical Encyclopedia (04 June, 2011). Cervical spondylosis. PubMed
Health. Available at: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001472/. Accessed on: 31 August, 2012.
• Shrotriya, Rajesh (Not Available). Cervical spondylosis. Dr. Rajesh A Shrotriya's Blog. Available at: http://drrajeshshrotriya.wordpress.com/cervical-spondylosis/. Accessed on: 31 August, 2012.
• Cervical spondylosis/degenerative neck disease (Not Available). MedIndia. Available at: http://www.medindia.net/patients/patientinfo/cervicalspondylosis_diagnosis.htm. Accessed on: 31 August, 2012.
• Cervical spondylosis (12 July, 2012). Mayo Clinic. Available at: http://www.mayoclinic.com/health/cervical-spondylosis/DS00697/DSECTION=tests-and-diagnosis. Accessed on: 31 August, 2012.