Natural History Study Interim Results - Alnylam … History Study Interim Results Anderson KE,...
14
1 Natural History Study Interim Results Anderson KE, Bloomer JR, Balwani M, Bissel DM, Rees DC, Stölzel U, Phillips JD, Kaupinnen R, Langendonk JG, Desnick RJ, Deybach JC, Bonkovsky HL, Parker C, Naik H, Badminton M, Stein P, Frank J, Gouya L, Minder E, Windyga J, Martasek P, Cappellini M, Ventura P, Sardh E, Harper P, Sandberg S, Aarsand A, Alegre M, Ivanova M, Meissner P, Marsden J, Chan A, Bettencourt B, Querbes W, Penz C, and Amy Simon on behalf of the Explore Investigators International Congress on Porphyrins and Porphyrias 15 September 2015
Transcript of Natural History Study Interim Results - Alnylam … History Study Interim Results Anderson KE,...

1
Natural History Study Interim Results
Anderson KE, Bloomer JR, Balwani M, Bissel DM, Rees DC, Stölzel U, Phillips JD, Kaupinnen R, Langendonk JG, Desnick RJ, Deybach JC, Bonkovsky HL, Parker C, Naik H, Badminton M, Stein P, Frank J, Gouya L, Minder E, Windyga J, Martasek P, Cappellini M, Ventura P, Sardh E, Harper P, Sandberg S, Aarsand A, Alegre M, Ivanova M, Meissner P, Marsden J, Chan A, Bettencourt B, Querbes W, Penz C, and Amy Simon on behalf of the Explore Investigators International Congress on Porphyrins and Porphyrias 15 September 2015

2
Study Design Overview
Design • Observational, multinational, prospective natural
history study in up to 100 patients Key Eligibility Criteria • Males or Females ≥ 18 years old • Diagnosis of acute hepatic porphyria (AHP) by
specialist, including acute intermittent porphyria (AIP), hereditary coproporphyria (HCP) and variegate porphyria (VP), with biochemical and molecular confirmation
• Recurrent attacks ◦ 3+ attacks* within 12 months of screening ◦ Using heme or GnRH analogs prophylactically
Key Objectives Characterize natural history and current AHP management
◦ Medical history and medication usage ◦ Porphyria signs and symptoms ◦ Biomarkers ◦ Quality of life ◦ Healthcare utilization
*Attacks defined as acute porphyria symptoms requiring increase in treatment (heme, pain medications, carbohydrates) or hospitalization ClinicalTrials.gov Identifier: NCT02240784
·
Study Schedule
6 months
Clinic Visit
Clinic Visit
(Option to extend time on study to 12 months)
Presenter
Presentation Notes
If no mutation, patient needs: dec PBGD activity or determined by porphyria specialist to have biochemical evidence of AIP, HCP or VP. At least one of the attacks had to have biochemical confirmation (PBG > 4x ULN)

3
Data Captured in Assessments and Labs
Screening Visit 2 Month Call 4 Month Call 6 Month Visit
Patient Questionnaires
• Symptoms and Porphyria History
• EQ-5D-5L • Healthcare Utilization
• Symptoms and interval medical course
• Symptoms and interval medical course
• Symptoms and interval medical course
• EQ-5D-5L
Lab Samples
• Chemistry and Hematology
• Urinalysis • ALA/PBG (urine and
plasma) • ALAS1 mRNA
• Urine ALA/PBG • ALAS1 mRNA
• Urine ALA/PBG ALAS1 mRNA
• Chemistry and Hematology
• Urinalysis • ALA/PBG (urine
and plasma) • ALAS1 mRNA
Questionnaires and Forms
Lab Samples
If Patients Experience an Attack (depending on treatment location)
Attack Symptom Inventory (patient) Attack Treatment Form (investigator)
ALA/PBG ALAS1 mRNA
4
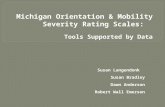
Participating Sites and Enrollment
Enrollment Update • Study to include 22 sites in 14 countries (USA and EU) • 68 patients enrolled • Patients enrolled to-date in USA, UK, Germany, Switzerland, Poland, Italy, Finland, Netherlands,
and Bulgaria
Data as of 14 AUG 2015
Total: N=68

5
Demographics and Baseline Characteristics
Demographics Mean (median; range)
Age 37.5 (36.5; 19-68)
Weight (kg) 67.7 (62.0; 40-130)
BMI (kg/m2) 24.9 (23.3; 16-47)
*N=44, as other patients screen during a porphyria attack, LCMS Method
Percent (n)
Sex – Female Male
91 (62) 9 (6)
Race - White/Caucasian Asian Black/African American
96 (65) 3 (2) 2 (1)
AHP Disease Characteristics
Percent (n)
AIP 91 (62)
VP 4 (3)
HCP 4 (3)
Patient genotyped 87 (59)
Relatives with AHP 68 (46)
Mean (median;range)
Years with AHP Diagnosis
9.7 (7.0;0-38)
Baseline PBG* (mmol/mol Cr)
33.2 (34.5; 0.04 -88.9)
Baseline ALA* (mmol/mol Cr)
15.2 (15.3; 0.6-35.8)
ULN: ALA <3.1 m/mol Cr; PBG <1.2 mmol/mol Cr
Data as of 14 AUG 2015
Presenter
Presentation Notes
Normal BMI 24.9 obese is > or equal to 30 Apc paper: 48% with relative with AHP

6
Patient-reported Attack Number Porphyria Screening Questionnaire
0
5
10
15
Number of Attacks Past Year (per patient)
Cou
nt
Mean: 10.6 Median: 6 Min, Max: 0, 52
Attack Treatment Location
Percent (mean; range)
Home 36 (4; 0-50)
Outpatient 36 (4; 0-40)
Hospital 27 (3; 0-18)
0 20 40 60
Porphyria Type
AIP
HCP
VP
Data as of 14 AUG 2015
Presenter
Presentation Notes
Treatment Location: Inpatient 39% (7); ED 28% (5); Home 28% (5); Clinic 5% (1)
7
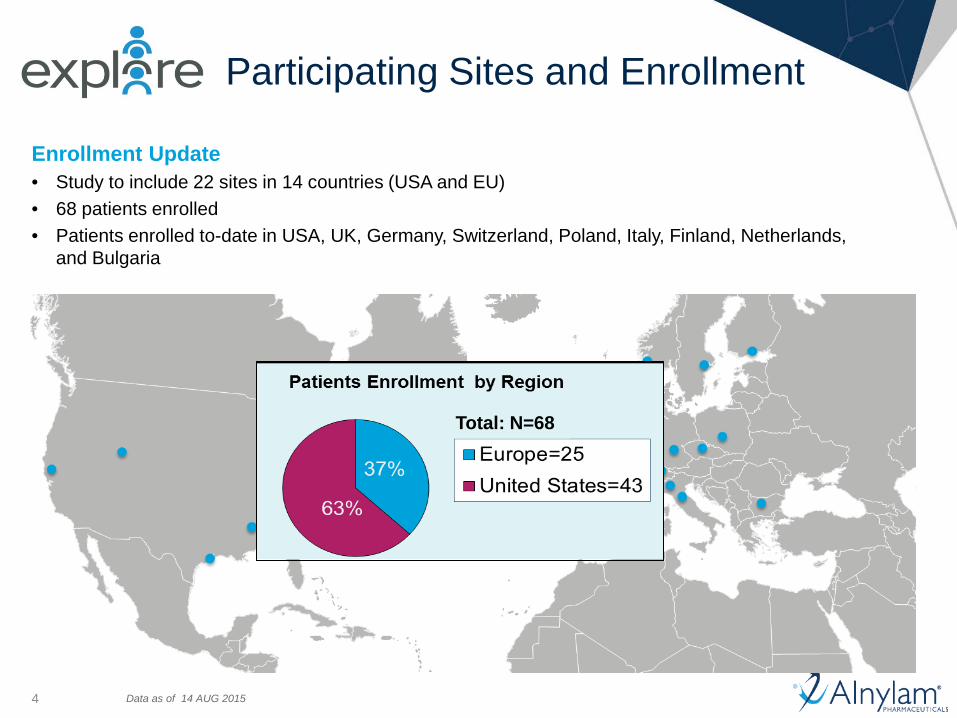
Patient-reported Attack Symptoms Screening Questionnaire
0
10
20
30
40
50
60
70
80
90
100
Abd
omin
al p
ain
Bac
k pa
inA
rm/L
eg p
ain
Mus
cle
pain
Hea
dach
eN
umbn
ess
Ski
n pa
inO
ther
pai
nB
liste
rs/R
ashe
sTi
redn
ess
Trou
ble
slee
ping
Anx
iety
Trou
ble
conc
entra
ting
Feel
ing
sad
Feel
ing
unm
otiv
ated
Feel
ing
diso
rient
edH
allu
cina
tions
Nau
sea
Loss
of a
ppet
iteV
omiti
ngC
onst
ipat
ion
Hea
rtbur
nFe
elin
g th
irsty
Dia
rrhe
aO
ther
dig
estiv
eW
eakn
ess
Cha
nge
in u
rine
colo
rFa
st h
eart
beat
Sw
eatin
gS
haki
ness
Chi
lls/F
ever
Pain Mood/Sleep GI Other
Sym
ptom
Ass
ocia
ted
with
Atta
ck (%
of p
atie
nts)
In addition, some attack symptoms present chronically (i.e. all the time) in 49% of patients • Most common chronic symptoms: pain, tiredness, N/V, constipation, and anxiety
Data as of 14 AUG 2015
Presenter
Presentation Notes
In recent natural history study from the APC which had AIP patients of which 85% were manifest, but not all recurrent attack patients, chronic(nearly constant) symptoms were seen in 18%. Andersson study 53% had fatigue only 15 % confusion

8
Patient-reported Attack Characteristics Porphyria Screening Questionnaire
Data as of 14 AUG 2015
Presenter
Presentation Notes
Most common triggers: stress (80%); menses (40%); diet (34%); meds (22%); illness (12%); insomnia (10%)
9
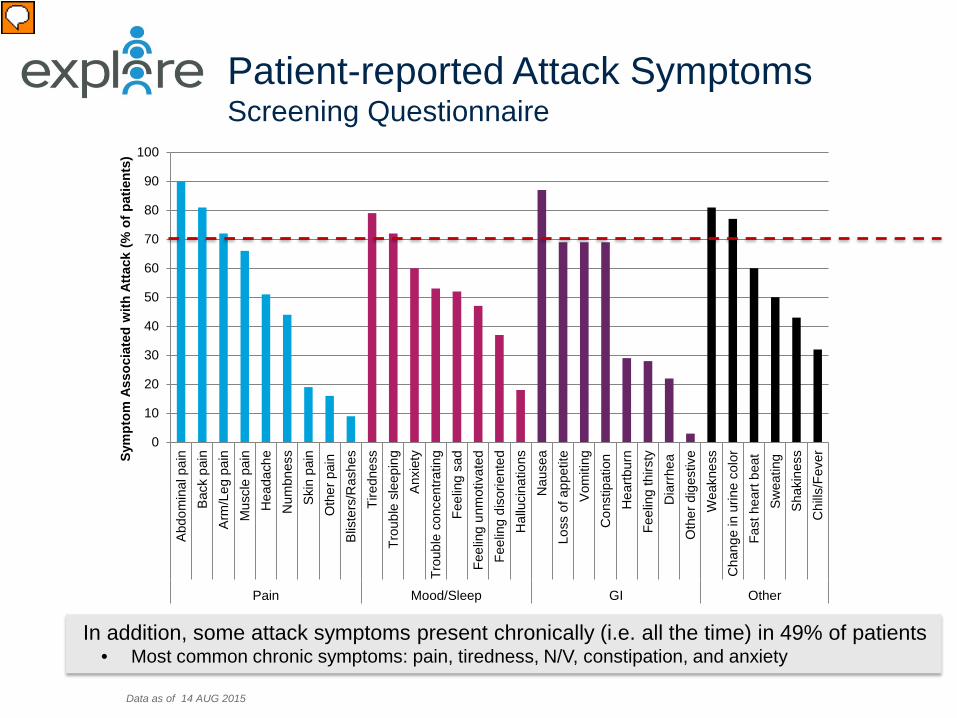
Quality of Life: EQ-5D-5L at Screen
Nordenfelt et al., Allergy Asthma Proc 2014 Lin et al., BMC Med Res Method 2014 Lubetkin et al., Qual Life Res 2005 Millward et al., J Inherit Metab 2001 Data as of 14 AUG 2015
0 10 20 30 40 50 60 70 80 90
Extremely anxious or depressedSeverely anxious or depressed
Moderately anxious or depressedSlightly anxious or depressed
Not anxious or depressedExtreme pain
Severe painModerate pain
Slight painNo pain
Unable to do my usual activitiesSevere Problems
Moderate problemsSlight problems
No problemsUnable to wash or dress myself
Severe ProblemsModerate problems
Slight problemsNo problems
Unable to walkSevere Problems
Moderate problemsSlight problems
No problems
Motility/Walking
Self-Care
Usual Activities
Pain/Discomfort
Anxiety/Depression 37%
46%
29%
7%
24%
N=68 EQ-5D Mean Summary Index = 0.74 • 0.79 in patients with diabetes mellitus • 0.78 in patients with heart disease • 0.82 in patients with hereditary angioedema
Presenter
Presentation Notes
Generic health measure that looks at 5 domains. Scoring of 5 domain collapses into an index from 1 no problem on any dimension to -0.59 extreme problems on all dimensions Millward study in had EQ Index in 0.71 (manifest) and of 0.76 (in latent ). That study had 63% AIP, 30% VP and rest HCP). About 50% manifest and rest latent

10
Attack Data: Site Treatment Log
• 101 attacks total with mean duration of 7.9 days • 41/68 (60%) patients reported 1+ attack during study
Data as of 14 AUG 2015
Attack Number
Current Heme Prophylaxis
No (60%, n=41) Yes (40%, n=27)
Mean (SD) Days on Study 137.7 (102.9) 180.5 (80.2)
# of Attacks* , total= 101 63 38
Annualized Attack Rate 4 attacks/per person 3 attacks/per person
Presenter
Presentation Notes
26% reported heme prophy in APC trial (but manifest AIP and not required to have recurrent attacks) Look up numbers on changed attack freq on heme

11
Individual Patient ALA and PBG Changes Relative to Baseline
Notes: ALA and PBG normalized to urinary creatinine Data as of 14 AUG 2015
•Curated list of 16 patients with ≥ 1 asymptomatic measure and ≥1 attack measure •Graph in Ln scale; arrows show mean and (median) fold change in actual scale •BIORAD assay results; similar trends seen with LC-MS assay
Attack-post-Rx Attack-post-Rx Attack-post-Rx

12
p<0.0001+
p<0.0001+
ALAS1 mRNA Data
p< 0.001^
^ P value from unpaired t test + P values from pairwise comparisons under repeated measures mixed mode with Subject as random and Visit Type as fixed effects
•Mean ALAS1 mRNA is increased >4-fold in asymptomatic AIP patient compared to normal healthy volunteers (NHV)
•ALAS1 mRNA further increased in AIP patients during acute attack

13
Interim Study Summary and Next Steps
General AHP Disease Findings • Approximately 50% of patients experience chronic porphyria symptoms even
when not having an attack • Patients have diminished quality of life even when not having an acute attack Porphyria Attack Findings • Current mean attack rate on study ~ 4 /per person/ per year • Patients on heme prophylaxis are still experiencing attacks • Early urinary ALA/PBG data suggest it may be useful attack biomarker Exploratory circulating ALAS1 mRNA assay (cERD) • Mean ALAS1 mRNA 4-fold higher in asymptomatic AHP patients than NHVs • ALAS1 mRNA further induced in AHP patients during acute attacks and may have
utility as attack biomarker Explore Study is ongoing • Study completion and publication of full study data planned in 2016

14
Acknowledgements ALN-AS1 Core Team • Bill Querbes (PL) • Tanya Sengupta (PM) • Amy Simon • Craig Penz • Amy Chan • Scott Barros • Lauri Binne • Jason Costigan • Satya Kuchimanchi • Anshul Gupta • Rena Denoncourt
• Nate Taneja • Jon O’Shea • Sarfraz Shaikh • Mano Manoharan • Rajeev Kallanthottathil • Jeff Rollins • Lubo Nechev • John Frenz • Jolly Bhatia • Patrick Igwenagu • Husain Attarwala • Renta Hutabarat • Ju Liu • Krishna Aluri • Chris Tran • Yongli Gu • Minggeng Gao • Qianfan Wang • Xuemei Zhang • Mary Carioto • Julia Hettinger • Garvin Warner • Mike Placke • Matt Algarin • Dave Mosher • Svetlana Shulga Morskaya • Meghan Collins • Tim Mooney
EXPLORE Investigators • Karl Anderson • Herb Bonkovsky • Montgomery Bissel • John Phillips • Charles Parker • Manisha Balwani • Joseph Bloomer • Pauline Harper • Eliane Sardh • David Rees • Mike Badminton • Penny Stein • Raili Kauppinen • Ulrich Stölzel • Jorge Frank • Elisabeth Minder • Jean Charles Deybach • Laurent Gouya • Pavel Martesek • Janne Langendonk • Sverre Sandberg • Felix Alegre • Aneta Ivanova • Paolo Ventura • Maria Cappellini • Jerzy Wingyga • Joanne Marsden • Peter Meissner
ALN-AS1 Advisors and Extended Team • Abigail Liebow • Tim Racie • Brian Bettencourt • Kirsten McCarthy • Siddharth Jain • Don Foster • Stu Milstein • Rick Duncan • Jared Gollob • Martin Maier • Klaus Charisse • Matthias Kretschmer • Lauren Melton • Akshay Vaishnaw • Jeff Cehelsky • Kevin Fitzgerald • Rachel Meyers • Dave Watkins • Oved Amitay • Sara Nochur • Carol Pitcher Towner • Donna Mackey • Ligang Zhang • Lubomir Tchangov • Karen Dobson • Jeff Kopacz • Jennifer Pena • Kelley Hanson
Most importantly,
we thank the patients for participating
APF • Desiree Lyon • Jessica Hungate • Natalia Sturza Mount Sinai • Hetanshi Naik • Robert Desnick