Natural history of HCV infection - Virology...
39
Natural history of HCV infection Krzysztof Simon MD.PhD.Prof Division of Infectious Diseases and Hepatology Wrocław Medical University, I Department of Infectious Diseases,Regional Specialistic Hospital ,Wrocław
Transcript of Natural history of HCV infection - Virology...
-
Natural history of HCV infection
Krzysztof Simon MD.PhD.Prof
Division of Infectious Diseases and Hepatology Wrocław Medical University,
I Department of Infectious Diseases,Regional Specialistic Hospital ,Wrocław
-
Disclosure Author has acted as an advisor and lecturer for Roche-Polska, Gilead, BMS, Abbvie, MSD, Janssen, Alfa-Wassermann, Baxter; and has received research support from Bayer, Gilead, EISAI,Tobira
-
Hepatitis C Viruses: Genomes and Molecular Biology.Tan SL, editor.Norfolk (UK): Horizon Bioscience; 2006.M
http://www.horizonbioscience.com/
-
Chronic HCV infection is leading cause of end- stage liver disese ,HCC and liver related deaths in the Western world
-
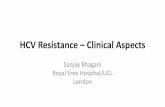
Growing problem of HCV infection
Ly KN, et al. Ann Intern Med 2012;156:271–8
Annu
al a
ge-a
djus
ted
mor
talit
y (R
ate
per 1
00,0
00 p
erso
ns)
7
6
5
4
3
2
1
0 1999 2000 2001 2002 2003 2004 2005 2006 2007
Year
HIV Hepatitis C Hepatitis B
HCV mortality increased
-
Reduced survival In US people with chronic hepatitis B or C lived about 2 decades less on average than those who did not have these infections; chronic viral hepatitis was the 15th leading cause of death in the U.S. in 2010,
During 2010 in USA there were a total of 18,473 deaths (0.7%) with hepatitis A, B, or C listed among the causes of death. 90% of these deaths listed hepatitis C. These deaths occurred mostly among people in the 45-64 age group (about three-quarters of such deaths). Among people who died of the same primary causes, decedents with hepatitis B or C listed as an additional cause died, on average, 22-23 years earlier than decedents who did not have these infections listed.
KN Ly, J Xing, RM Klevens, et al. Causes of Death and Characteristics of Decedents With Viral Hepatitis, United States, 2010. Clinical Infectious Diseases 58(1):40-49. January 1, 2014.
-
HCV characteristics
Family Flaviviridae Enveloped Positive-sense single-stranded RNA(9,6kd) 3000-amino acid polyprotein No RNA polymerase proofreading ability Quasispecies Half-life-2,7 hours Daily production 10 trilion(10 12 ) virions
Lauer,Walker.N.Eng.J.Med.2001
-
HCV life cycle
Hepatitis C Viruses: Genomes and Molecular Biology.Tan SL, editor.Norfolk (UK): Horizon Bioscience; 2006.M
http://www.horizonbioscience.com/
-
Worldwide prevalence of HCV- 180mln
Centers for Disease Control and Prevention. CDC Health Information for International Travel 2012. New York: Oxford University Press; 2012.
-
Epidemiology HCV World - 180mln infected? In 2010 y. deaths from HCV related cirrhosis :287400
and HCC:195000 In Europe seroprevalence of anti HCV
-low (0,4%):Sweden,Netherlands,Germany -high(2-3%) Mediterranean countries
Poland-2013 y. (0,95 -1,4%)-700 000.
-but only
-
HCV-list of the different genotypes 7 genotype(1-7) ( differences 30-50%) > 50 subgenotype (np.1a,1b, itd.) ( differences 15-30% ) isolates ( differences 5-15% ) „quasispecies” (1-5% nucleotide differences ) Western Europe USA – 1a, 1b, 2a, 3a Eastern Europe – 1b North Afrika – 4 Japan, China, Tajwan – 2 Hongkong, Makao – 6 POLAND : G1b-75%, G1a-5%, G3a-17%, G4c+d 1% (differences between regions) Each genotype is actually a mixture of closely-related viruses called quasi-species. These quasi-species have the ability to mutate very quickly and become immune to current treatments, which explains why chronic hepatitis C infection was so difficult to treat.
Dore G.J,Ward J,Thursz M.Hepatitis C disease burden and strategies to manage the burden.J.Viral.Hepatitis,2014,21,suppl.1,1-4
-
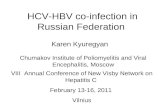
HCV genotype distribution
Hajarizadeh B, et al. Nat Rev Gastroenterol Hepatol 2013;10:553–62
Canada
USA
Mexico
Columbia
Chile Argentina
Brazil
Italy
Spain Portugal
France
Germany
UK
Belgium
Norway Sweden Finland
Poland Turkey
Syria
Russia
Japan
Republic of Korea
China
Australia
Thailand
India
Saudi Arabia
South Africa
Greece
Pakistan
G1 Genotypes
G1a G1b G2 G3 G4 G5 G6 Mixed or other
2.9% Not studied
-
HCV infection: risk factors
Current or former injection drug users, including those who injected only once many years ago Recipients of clotting factor concentrates made before 1987, when more advanced methods for manufacturing those products were developed Recipients of blood transfusions or solid organ transplants before July 1992, when better testing of blood donors became available Chronic hemodialysis patients Persons with known exposures to HCV, such as: – health care workers after needlesticks involving HCV-positive blood – recipients of blood or organs from a donor who tested HCV-positive – body piercing/scarring/tattooing etc (HIV: 0,3%, HCV: 5-15% , HBV: > 60% (HBeAg + ),< 30% (HBeAg -)
Persons with HIV infection Children born to HCV-positive mothers Intranasal cocaine users Sex with mutiple partners ,particulary anal
Terrault NA, Dodge JL, Murphy EL i wsp. Hepatology. 2013 Mar;57(3):881-9.
Madaliński i wsp Med.Sci.Rev.Hepatologia 2012,12,70-72 Sexually Transmitted Diseases Treatment Gudelines MMWR 2010;59(RR-12)
http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5912a1.htm?s_cid=rr5912a1_e
-
HCV infection: risk factors
The mean volume of an accidental drop was 29 mcl (range 20-33 mcl).
At storage temperatures of 4° and 22° C, viable HCV was recovered from low titer spots after up to 6 weeks. At 37° C, infectious HCV was recovered only up to 7 days. HCV infectivity declined rapidly during the first 2 weeks of storage, followed by a slower decline. Bleach (1:10 dilution) was the most effective antiseptic tested, with 1 minute of exposure eliminating infectious HCV in 100% of spots, followed by the commercial medical disinfectant CaviCide (1:10 dilution; 94% of spots) and 70% ethanol (87% of spots).
E Paintsil, M Binka, A Patel, et al. Journal of Infectious Diseases, Nov.23, 2013
-
Acute hepatitis
Chronic hepatitis
Cirrhosis Death
Liver insufficiency
23% / y 1
HCC
LTR
. 1.Marcelin P. Liv.Int., 2009, 2.Asselah T.Semin Liv.Dis.2007 3. Wasmuth J Ch,W :Short guide to hepatitis C. red Mauss S,Berg T, Rockstroh J, Sarrazzin Ch, Wedemayer H, Flying Publisher and Kamps, 2011
HCV clinical manifestations-liver disease progression
20-30% patients with CHC2
Asymptomatic HCV carrier
4% / y
Spontaneus elimination
of HCV
Spontaneus elimination of HCV
66-82%
Extrahepatic manifestations
After successful LTR
-
HCV clinical manifestations –extra-hepatic HCV
-
HCV infection-basic facts
The transition from acute to chronic heatitis C is usually sub-clinical The acute illness is clinically mild and is typically unrecognised and
undiagnosed Risk of chronicity variable: 18-34% The natural history of chronic hepatitis C remains incompletly defined; generally this is the slowly progressive disease Risk of cirrhosis (without cofactors!!!) 10-20% within 30 years Cirrhosis related mortality 1-5%/year Incidence of HCC in patients with HCV cirrhosis 1-4%/year
Westbrook R.H.,Dusheiko G.Natural history of hepatitis C.J.of Hepatology, 2014,61,S58-S68
-
Morevoer the effects of chronic HCV infection extend beyond liver related mortality and decreased the quality of life
-
Clinical picture is influenced by 1.host- 2.viral- 3.enviromental factors
-
Factors influencing natural history and accelerating progression of the HCV infection
genotypes pseudotypys mutants level of replication immune response immunosupression
Route of transmission Infectious viral load dosis Acute phase/asymptomatic infection Older age at time of infection >40 years Polimorfism of HLA-II (DQB1*0301, DRB1*01) Race Gender : m>f BMI Insuline resistance Previous NAFLD Previous hemosiderosis/hemochromatosis HIV(!), HBV(!), Herpesvirusy coinfection? Previuos or concurrent alcohol consumption
Blackard, Hepatology ,2008,47,1,321-331 Marcelin P. Liv.Int., 2009,29 (s1) 1-8 Bugianesi E.,Salamone F,Negro F,. Hepatol.2012, suppl1, 56,S56-s65 Westbrook R.H.,Dusheiko G.Natural history of hepatitis C. J.of Hepatology, 2014,61,S58-S68
-
Acute hepatitis C
In those persons who do develop symptoms, the average time period from exposure to symptom onset is 4–12 weeks (range: 2–24 weeks). Persons with newly acquired HCV infection usually are asymptomatic or have mild symptoms that are unlikely to prompt a visit to a health care professional. Approximately 20%–30% of those newly infected with HCV experience some symptoms; they can include
Fever Fatigue Dark urine Clay-colored stool Abdominal pain Loss of appetite Nausea Vomiting Joint pain Jaundice
Acute resolution of HCV is not associated with any long-term sequelae
-
Acute hepatitis C
Estimates of World annual incidence indicate that 3-4 mln people are newly infected each year The CDC estimates approximately 29,718 cases occurred in 2013, after adjusting for asymptomatic infection and underreported The number of acute cases of hepatitis C reported in the US increased from, 1,778 in 2012 to 2,138 in 2013. Where are others acute cases?
Perz JF,et all.J.Hepatolog,2006,45,529-538 Westbrook R.H.,Dusheiko G.Natural history of hepatitis C. J.of Hepatology, 2014,61,S58-S68
-
Reinfection after clearance of acute hepatitis C
-The risk of reinfection and superinfection remains a possibility after clearance of acute hepatitis C -Particular risk groups:
MSM PWID / IDU
Terrault NA, Dodge JL, Murphy EL i wsp. Hepatology. 2013 Mar;57(3):881-9.
-
Chronic hepatitis C
persistance >6 months of positive HCVRNA most persons with chronic HCV infection are asymptomatic however, many have chronic liver disease, which can range from mild to severe chronic liver disease in HCV-infected persons is usually insidious, progressing slowly without any signs or symptoms for several decades spontaneus resolution of chronic hepatitis C is relatively rare, but occur 0,5% year
Mauss S,Berg T.,Rockstroh J.,Sarrazin Ch.,Wedemeyer H.Hepatology 2015,Flying Publisher
-
Probability of fibrosis progression to F4 according to age at infection
Rates of fibrosis progression is 0,1-0,2 per year; In patients infected in age >70 300x fold higher than in age
-
Liver cirrhosis and HCV
Wide range of: symptoms, signs and consequences
-
Wilson, S. R. et al. Am. J. Roentgenol. 2009;193:55-60
-
Clinical course of cirrhosis:1-year outcome probabilities according to clinical stages
Stage 1
Stage 2
Stage 3
Stage 4
No varices No ascites
Varices No ascites
Varices Ascites +/-
Variceal bleeding +-
Ascites
1%
3,4%
20%
57%
DEATH 4%
7%
6,6%
7,6%
4,4%
D’Amico G.Complication of portal hypertension.EASL Postgraduate Course,Milan, 2008,10-15
-
HCC and HCV
Chronic HCV infection is the leading cause of hepatocellular carcinoma (HCC ) in the Western world
But RNA viral genome is not observed in HCC cells >90% patients with HCC infected with HCV have had
inductors /co-factors of carcinogenesis: -cirrhosis particulary active -alcohol consuption in past history -aflatoksyny (B1) -”nonalcoholic steatohepatitis” -congenital metabolic disturbances
Huang J-F. i wsp.Hepatology,2013,57,5,1882-1892 De Lope C.R. i wsp. Management of HCC.J.of Hepatol.2012,56,supl.1,S75-S87 Akkari L.,Gregoire D.,Floch N i wsp.J.of Hepatol.2012,57,5,1021-1028 Akuta N Seko Y, Kawamura Y i wsp.Complicated relationships of amino acid substitution in hepatitis C virus core region and IL28B genotype influencing hepatocarcinogenesis. Hepatology. 2012 Dec;56(6):2134-41. doi: 10.1002/hep.25949.
-
How can we change natural history of chronic HCV infection? Milestones of success
Early diagnosis Proper treatment
-
Acute hepatitis C- therapy
In the acute phase of the infection HCV is highly vulnerable to therapy with PEGIFNalfa.
>90% of patients can be cured with IFN-alfa 6 months monotherapy -start time- after 12 weeks of diesease
Acute genotype 1 HCV infection in HIV infected men PEGIFNalfa/RBV/TVR v PR 12 weeks therapy 84% v.63%
Resolution fo HCV is not associated with any long-term sequelea
-
Jan–Jun
Chronic hepatitis ,cirrhosis, HCC HCV-therapy 2015
Nuc: nucleotide polymerase inhibitor; NS5A: hepatitis C virus non-structural protein 5a protease inhibitor
Jul–Dec Jan–Jun Jul–Dec Jan–Jun Jul–Dec Jul–Dec Jan–Jun Jul–Dec
Telaprevir
Boceprevir
Interferon Free
Terapia trójlekowa
Sofosbuvir (G1,2,3,4,5,6)
Sofosbuvir +
RBV
G2/3 + Asunaprevir
Daclatasvir ±
BMS-325
Daclatasvir (G1, 2, 3, 4)
Sofosbuvir+ Ledipasvir
FDC
Ombitasvir
Dasabuvir
+ ABT-450/r
RBV
+
±
2011 2012 2013 2014 2015
IFN
-free
IF
N-b
ased
Simeprevir (G1, 4)
EU akceptacja
RBV
±
Protease inhibitor Nuc inhibitors NS5A NS5B inhibitor
Sofosbuvir +
Simeprevir
G1/4
± RBV
Grazoprevir+ Elbasvir.
-
I-free therapies Following on from the recently available IFN-free combinations many more are expected in the near future SOF + LDV ± RBV
SOF + other agents Abbvie combination ± RBV
DCV + ASV MK-5172 + MK-8732 ± RBV
There is no clear direction with regard to the next tranche of standard of care The guidelines are rapidly changing
SMV + SOF – OPTIMIST 1 and 2
SMV + DCV + RBV – SATURN SMV + samatasvir – HELIX-1
-
0
20
40
60
80
100
IFN 6 mo.
.. IFN+RBV 6 mo.
IFN+RBV 12 mo.
PEG 12 mo.
PEG+RBV 12 mo.
PI+PEG +RBV
6-12 mo. LDV/SOF 3D Abbvie
2-3 mo.
68-75
54-56
39 42 34
16
6
90
1986 1998 2002 2001 2011 2013
SVR
(%)
SMV+PEG +RBV
6-12 mo.
80-81
2014*
SOF+PEG +RBV 3 mo
94-99 Poszczególne lata nie są ułożone według skali
Overall SVR-HCVG1
trader DB, et al. Hepatology 2004;39:1147-71. INCIVEK [PI]. Cambridge, MA: Vertex Pharmaceuticals; 2013. VICTRELIS [PI]. Whitehouse Station, NJ: Merck & Co; 2014. Jacobson I, et al. EASL 2013. Amsterdam. The Netherlands. Poster #1425. Manns M, et al. EASL 2013. Amsterdam. The Netherlands. Oral #1413. Lawitz E, et al. APASL 2013. Singapore. Oral #LB-02; Afdhal N, et al. N Engl J Med 2014; 370: 1889-98; Kowdley K, et al. N Engl J Med 2014; 370: 1879-88.
*
Chart1
6
16
34
42
39
542
687
801
90
945
Series 1
Series 2
Sheet1
Series 1Series 2
6
16
34
42
39
542
687
801
90
945
-
Achievement of SVR in any stage of HCV related diseases change natural history of HCV infection- reduce (but not fully eliminate) progression of liver cirrhosis, risk of HCC and lowers liver related mortality
Morgan RI et al. Ann.Intern. Med.2013,158,329-337 Aleman S. et al. Clin Infect. Dis.2013,57,23-236 Morgan TR.et al Hepatology 2010,52,833-844
Natural history of HCV infection Slide Number 2Slide Number 3Slide Number 4Growing problem of HCV infection Reduced survivalHCV characteristicsHCV life cycleWorldwide prevalence of HCV- 180mlnEpidemiology HCV HCV-list of the different genotypes HCV genotype distributionHCV infection: risk factorsHCV infection: risk factorsHCV clinical manifestations-liver disease progressionSlide Number 16HCV infection-basic factsSlide Number 18Slide Number 19Factors influencing natural history and accelerating progression of the HCV infectionAcute hepatitis CAcute hepatitis CReinfection after clearance of acute hepatitis CChronic hepatitis CSlide Number 25Liver cirrhosis and HCVSlide Number 27Slide Number 28Slide Number 29Slide Number 30Slide Number 31Clinical course of cirrhosis:1-year outcome probabilities according to clinical stagesHCC and HCVHow can we change natural history of chronic HCV infection? Milestones of success �Acute hepatitis C- therapyChronic hepatitis ,cirrhosis, HCC �HCV-therapy 2015I-free therapiesOverall SVR-HCVG1Slide Number 39