Native Controlling Hypertension and Risk Through Technology …€¦ · 108-132 86 101 116 133-142...
44
This work is supported by grant U54 MD011240 – funded by the National Institute on Minority Health and Health Disparities Native Controlling Hypertension and Risk Through Technology (Native-CHART) Webinar Series Introduction Gladys Rowe Partnerships for Native Health at Washington State University
Transcript of Native Controlling Hypertension and Risk Through Technology …€¦ · 108-132 86 101 116 133-142...

This work is supported by grant U54 MD011240 – funded by the National Institute on Minority Health and Health Disparities
Native Controlling Hypertension and Risk Through Technology (Native-CHART)
Webinar Series Introduction
Gladys Rowe Partnerships for Native Health at Washington State University

Agenda
• Institute for Research and Education to Advance Community Health (IREACH) and Partnerships for Native Health Introductory Slides (5 minutes)
• Native-CHART Presentation: Hypertension: History, Impact, and Interventions, Dr. Jason Umans (45 minutes)
• Question and Answer, Closing (15 minutes)
• Post-webinar survey link: $30.00 gift card drawing

Institute for Research and Education to Advance
Community Health
We challenge the status quo and advance community health through partnerships and collaboration.
IREACH

IREACH
Rural Health and
Health Networks
Partnerships for
Native HealthLatinx Health
Native Hawaiian and
Pacific Islander Health
Behavioral Health
Innovations

• Achieving health equity
• Community outreach and engagement
• Training and education
• ~160 partners: tribal colleges, Native organizations, tribes, and universities
Partnerships for Native Health
• Community-based research and education to improve health and reduce health disparities among American Indians, Alaska Natives, Native Hawaiians, and Pacific Islanders

Native-CHART
The Center aims to improve control of blood pressure and other risk factors for cardiovascular disease in American Indians, Alaska Natives, Native Hawaiians, and Pacific Islanders with diagnosed hypertension. It comprises three community-based intervention projects and four supporting Cores.
IREACH.WSU.EDU/NCHART
Native Controlling Hypertension and Risk Through Technology

• Post-webinar evaluation: enter to win a $30 gift card
• The webinar recording and presentation slides will be available at ireach.wsu.edu/nchart
• Please enter questions for Dr. Umans in the Q&A box
Native-CHART Webinar

This work is supported by grant U54 MD011240 – funded by the National Institute on Minority Health and Health Disparities
HYPERTENSION: History, Impact, Interventions
Practice and Guidelines
Jason G. Umans, MD, PhDNative-CHART Methods CoreGeorgetown-Howard Universities Center for Clinical and Translational Science and MedStar Health Research Institute

•What is hypertension?
•Is it bad for you?
•How should we measure BP?
•What goes wrong in patients with high BP?
•Which patients should be treated, and how?
•How do we pick our BP treatment targets, and how do we get there?
Key questions we will address in this (fly-by) talk

•1896-1905-noninvasive BP measurement
•1913- high BP associated with stroke, CHF, renal failure
•Association, but no evidence of causality
•1925-Society of Actuaries report on >0.5 million men: high BP increases mortality
•They didn’t really care about causality, just prediction
•1939-62-Actuaries, Life Insurance Industry and Metropolitan Life tables: Progressive increases in mortality (along with stroke, cardiovascular and renal disease) with increases in either SBP or DBP
Hypertension: A Brief and Selective History

Relative Increase in CVD Deaths With BP
1941 Life Insurance Data
Diastolic BP → 54-83 84-93 94-116
Systolic BP
108-132 86 101 116
133-142 108 137 171
143-177 175 201 293

Target Organ Damage “Malignant” Hypertension
500 Untreated Hypertensives-1955 % Pts Survival-mo
Enlarged Heart (by CXR) 74 8
CHF/Pulmonary Edema 50 4
Angina Pectoris 16 5
Encephalopathy 2 1
Stroke 12 4
Proteinuria 42 5
Azotemia 18 1
Accelerated Hypertension 7 1

Stroke and IHD Mortality vs Usual Sys BP by Age
IHD=ischemic heart disease
Prospective Studies Collaboration. Lancet. 2002;360:1903-1913.
Mo
rtality
(Flo
ati
ng
Ab
so
lute
Ris
k a
nd
95%
CI)
Usual Systolic BP (mm Hg)
50-59 years
60-69 years
70-79 years
80-89 years
Stroke Age at risk:
256
128
64
32
16
8
4
2
1
0
120 140 160 180
IHD
Usual Systolic BP (mm Hg)
50-59 years
60-69 years
70-79 years
80-89 years
Age at risk:
40-49 years
256
128
64
32
16
8
4
2
1
0
120 140 160 180

10090-99
80-8975-79
70-74<70 <120
120-
139
140-
159
160
48
3735 44
38
81
31
2625
2525
25
24
17
1413
1312
21
1012
99
9
Effect of Systolic and Diastolic BP on CHD Mortality: MRFIT Screenees (N=316,099)*
*Men aged 35 to 57 years followed up for a mean of 12 years.
Adapted from: Neaton et al. Arch Intern Med. 1992;152:56-64.
Death rate
per 10,000
person-years
Diastolic BP
(mm Hg)Systolic BP
(mm Hg)

•1945- FDR dies of stroke with (due to?) uncontrolled hypertension
•1948- Beginning of Framingham study
•1940s-50s-First treatments, from Kempner rice diet or sympathectomy to early sympatholytic drugs
•1967-VA Cooperative Trial 1 (3 drugs for DBP >115 saves lives-trial stopped early-this trial made hypertension into a real disease
•1989-Beginning of the Strong Heart Study-this study showed that American Indians were not (somehow) immune to CVD and that hypertension was a powerful risk factor
Hypertension: A Brief and Selective History

The VA Cooperative Study I (DBP>115)Assessable Morbid/Fatal Events
Placebon=70
Active Rx*n=73
Accelerated
hypertension12 0
Stroke 4 1
Coronary event 2 0
CHF 2 0
Renal damage 2 0
Deaths 4 0
VA Cooperative Study Group. JAMA. 1967;202:1028-1034.
*P<0.001 active drug therapy vs placebo

Placebon=194
Active Rx*n=186
Accelerated hypertension 4 0
Stroke 20 5
Total coronary event 13 11
Fatal coronary event 11 6
Congestive heart failure 11 0
Renal damage 3 0
Deaths 19 8
The VA Cooperative Study II (DBP 90-115) Assessable Morbid/Fatal Events
VA Cooperative Study Group. JAMA. 1970;213:1143-1152.*P<0.001

Hypertension Treatment Effect Mirrors Observational Data
0
2
4
6
8
10
12
CV
D I
ncid
en
ce
120 140 160 180 200 220
Systolic BP (mmHg)

•Hypertension is both a marker and cause of CVD
•Risk increases with the severity of hypertension
•Benefits of BP lowering (treatment) mirror the risks of hypertension severity in observational studies
•Recent and ongoing trials seek answers to specific treatment questions in well defined patient groups
Summary

•How much hypertension is out there?
•Are we “on top” of it?
•How do we define and grade it?
•How does it interact with other co-morbid risk factors?
•How is it actually going to kill us?
Hypertension: Definitions and Burden

Hypertension Prevalence by Age and Ethnicity in Men and Women: NHANES 1999-2000
95% CIs. Weighted to the US population. Hajjar et al. JAMA. 2003;290:199-206.
100
80
60
40
20
0Hyp
ert
en
sio
n P
revale
nce,
%
Non-
Hispanic
White
Non-
Hispanic
Black
Mexican
American
Men Women
18-39 40-59 60
Non-
Hispanic
White
Non-
Hispanic
Black
Mexican
American

2
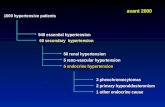
Zhang Y, Moran A, Hypertension. 70:736-742, 2017
Prevalence,
Awareness,
Treatment, and
Control of
Hypertension,
1999 to 2014

Framingham Heart Study, CVD
outcomes by BP (2001)
Optimal <120/<80
Normal 120-129
High Normal 130-139
In JNC7 (SysBP only),
Optimal became “normal”
Normal became “PreHtn”
High Normal became “PreHtn”
In new guidelines (SysBP only),
Optimal is “normal”
Normal is “elevated”
High Normal is “Stage 1 Htn”

Additive Effect of Cholesterol and Systolic BP on Risk of CHD Death
Neaton et al. Arch Intern Med. 1992;152:56-64.
34
21
17
13
12
23
12
810
6
17.7
10.9
8.6
6.3
5.5
17
88
6
4
14
56
33
142+
125-131
<182
182-202
203-220
221-244
<118
118-124
132-141
Deaths /10,000 pt-yr
245+

Microalbuminuria increases CHD risk of high BP
Borch-Johnsen K, et al. Arterioscler Thromb Vasc Biol. 1999;19(8):1992-1997.

Prehypertension, Diabetes, and Cardiovascular Disease Risk in a Population-Based
Sample, Volume: 47, Issue: 3, Pages: 410-414, DOI:
(10.1161/01.HYP.0000205119.19804.08)
Prehypertension, Diabetes (120-139/80-89) and CVD in the SHS (2006)

Lower BP Targets in high risk
patients are because of
SPRINT (2015)
Sys BP <140 vs <120; 9361
older pts with Sys BP 130-180
and elevated CVD risk
We should have already
known this from SANDS
(2008). 499 AIs with DM,
randomized to sysBP <115 vs
<130 and tight vs very tight
LDL and non-HDL-C:
improved IMT and LVMI

•UKPDS (<85 DBP) 2.7
•ABCD (<75 DBP) 2.8
•MDRD (<92 MAP) 3.6
•HOT (<80 DBP) 3.3
•AASK (<92 MAP) 3.8
•ACCORD (<120 SBP) 3.4
•SPRINT (<120 SBP) 2.8
•SANDS (<130 SBP) 1.6
•SANDS (<115 SBP) 2.3
Number of Antihypertensive Drugs Needed to Reach BP Goals in Prospective Trials

JAMA. 2018;320(17):1760-1763. doi:10.1001/jama.2018.16068
Yano, CARDIA Study; Sun, 2.5M Korean young adults, both with mean age in 30s
Hypertension Definitions: Evolution and Disagreement

•There is still a lot of unrecognized and under-treated hypertension (by any definition)
•Hypertension is a major cardiovascular risk and its effect is multiplied by other risk factors
•Treatment (which almost always requires more than one drug) should be tailored to severity of hypertension and co-morbidities
•Risk increases with even modestly abnormal BP
•Hypertension (and what we used to call prehypertension) tends to keep bad company
Summary

•Sphygmomanometry (with auscultation)-importance of proper technique
•Home (automated, oscillometric) BP monitors• Home (BPs, if confirmed to be accurate, predict CVD outcomes and
verify control much better than office BPs
•ABPM-might it be important?• Only method that gets at nocturnal pressures
• What goes for home BPs is even better in ABPM
•Problems with devices and their use, both in the clinic and in research
BP Measurement

2
% +/-
(mm Hg)
≦5 ≦10 ≦15 Mean
Diff
SysBP 62% 87% 95% 0+/-7
DiaBP 58% 90% 98% -4+/-5
Validation of the HEM-907
1-This is the ~$700 device used in SPRINT Trial
2-Compared to Hg/Auscultation Gold Std
3-Two observers had 100% agreement
4-For comparison treatment effect size in most
BP clinical trials is 2-6 mm Hg
El Assaad et al, Bl Press Mon. 7:237-241, 2002

•A lot of unsuspected hypertension is diagnosed by proper careful BP measurement
•A lot of hypertension is cured by proper careful BP management
•Home BP management can be an important adjunct to diagnosis and treatment, but accuracy has to be assessed in each patient before trusting the values
Key Messages on BP Measurement

•Diet interventions work, but with real problems and unknowns regarding persistence—i.e., needs research•DASH, Low Sodium
• Interaction of Na and K
•On average, equivalent to ~1 BP drug (recalling that most patients need 2 or more drugs except for mild hypertension
•Not just limited adherence by patients but also therapeutic inertia and lack of aggressive titration by clinicians lead to poor control---i.e., needs research
Two Key Messages on BP Control of Relevance to Native-CHART

BP Control by
DASH Diet and
Salt Restriction
DASH lowers BP by
~6mm Hg when on
(usual) high salt diet. A
low salt diet has a similar
effect.
With both DASH and
lower salt intake, BP
goes down more but the
incremental benefit of
DASH decreases

Pettiti. N Engl J Med. 2001;344:1717.
-7
-6
-5
-4
-3
-2
-1
0
1
0 5 10 15 20 25 30 35 40
PREMIER, 2003
DASH-Sodium, 2001
TOHP-II, 1997
TOHP-I, 1992
HPT, 1990
Months of Intervention
Diffe
ren
ce
in
SB
P (
mm
Hg
)
Na+ Restriction and BP Trials

In a large VA hypertension clinic patients were not followed more closely if BP
was uncontrolled, did not have BP measured at every visit, and did not
routinely have medications adjusted or testing performed if response was
suboptimal N Engl J Med 1998; 339:1957-1963
Physicians Conspire with Patients to Avoid BP Control

• Nonadherence of patients to prescribed medication is a challenge in all chronic conditions, with typical adherence rates at 1 year:
• About 50% for drugs
• About 10% for lifestyle changes
• "Compliance" of physicians with treatment guidelines is also suboptimal, especially regarding an appropriate increase in intensity of treatment:
• In the VA system in 1997, only ~6% of patients with SBP >160 mm Hg had their BP medications increased
• In ALLHAT, ~94% of those with BP >140/90 mm Hg did not have their BP medications increased
Adherence and Compliance
Haynes et al. JAMA. 2002;288:2880-2883.
Berlowitz et al. N Engl J Med. 1998;339:1957-1963

• Hypertension kills!
• You have to measure BP (properly) to find hypertension
• The specific cause of hypertension matters• Salt sensitivity and others, not discussed
• Hypertension magnifies all other cardiovascular risks
• Antihypertensive treatment helps tremendously
• All patient groups (e.g., elderly, diabetes, kidney disease, prevalent CVD) benefit from treatment
• By extension, but with precious little data, all of these messages probably apply to Native populations, perhaps more so (e.g. SANDS)
• It is sometimes difficult to control hypertension and both physicians and patients can often share in the blame
Summary and Take Home Messages

This work is supported by grant U54 MD011240 – funded by the National Institute on Minority Health and Health Disparities
Thank you!
Questions?

Nonpharmacologi
-cal InterventionDose Approximate Impact on SBP
Hypertension Normotension
Weight loss Weight/body fat Best goal is ideal body weight, but aim
for at least a 1-kg reduction in body
weight for most adults who are
overweight. Expect about 1 mm Hg for
every 1-kg reduction in body weight.
-5 mm Hg -2/3 mm Hg
Healthy diet DASH dietary pattern
Consume a diet rich in fruits,
vegetables, whole grains, and low-fat
dairy products, with reduced content
of saturated and total fat.
-11 mm Hg -3 mm Hg
Reduced
dietary sodium
Dietary sodium Optimal goal is <1500 mg/d, but aim
for at least a 1000-mg/d reduction in
most adults.
-5/6 mm Hg -2/3 mm Hg
Enhanced
dietary
potassium
Dietary potassium
Aim for 3500–5000 mg/d, preferably
by consumption of a diet rich in
potassium.
-4/5 mm Hg -2 mm Hg
*Type, dose, and expected impact on BP in adults with a normal BP and with hypertension.
DASH indicates Dietary Approaches to Stop Hypertension; and SBP, systolic blood pressure.
Resources: Your Guide to Lowering Your Blood Pressure With DASH—How Do I Make the DASH?
Available at: https://www.nhlbi.nih.gov/health/resources/heart/hbp-dash-how-to.
Top 10 Dash Diet Tips. Available at: http://dashdiet.org/dash_diet_tips.asp

Nonpharmacologica
l Intervention
Dose Approximate Impact on SBP
Hypertension Normotension
Physical
activity
Aerobic ● 90–150 min/wk
● 65%–75% heart rate reserve
-5/8 mm Hg -2/4 mm Hg
Dynamic resistance ● 90–150 min/wk
● 50%–80% 1 rep maximum
● 6 exercises, 3 sets/exercise, 10
repetitions/set
-4 mm Hg -2 mm Hg
Isometric resistance ● 4 × 2 min (hand grip), 1 min rest
between exercises, 30%–40%
maximum voluntary contraction, 3
sessions/wk
● 8–10 wk
-5 mm Hg -4 mm Hg
Moderation
in alcohol
intake
Alcohol
consumption
In individuals who drink alcohol,
reduce alcohol† to:
● Men: ≤2 drinks daily
● Women: ≤1 drink daily
-4 mm Hg -3 mm
*Type, dose, and expected impact on BP in adults with a normal BP and with hypertension.
†In the United States, one “standard” drink contains roughly 14 g of pure alcohol, which is typically found in 12 oz
of regular beer (usually about 5% alcohol), 5 oz of wine (usually about 12%
alcohol), and 1.5 oz of distilled spirits (usually about 40% alcohol).

0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60R
ela
tive r
isk (
95
% C
I)
Stroke CHD
Active Therapy vs. Placebo
CHF Death
0.63
0.46
0.68
0.87
CVD
0.75
SHEP: Cardiovascular Disease Endpoints
SHEP Research Group. JAMA. 1991;265:3255-3264.
SHEP=Systolic Hypertension in the Elderly Program
CHD=coronary disease; CHF=congestive heart failure; CVD=cardiovascular disease