
National health workforce strategic plan - South-East Asia ... · National Health Workforce...
106
National Health Workforce Strategic Plan 2014–2018 Ministry of Health and Gender Republic of Maldives
Transcript of National health workforce strategic plan - South-East Asia ... · National Health Workforce...
0
National Health Workforce
Strategic Plan
2014–2018
Ministry of Health and Gender
Republic of Maldives

0

1
Contents
Abbreviations ....................................................................................... 6
Executive summary ............................................................................... 7
Background ....................................................................................... 7
Main HRH issues ................................................................................ 7
Conclusion ........................................................................................ 8
Section A: Introduction ............................................................................ 9
Background ......................................................................................... 9
Methodology ...................................................................................... 10
Review of records, reports and literature ............................................. 10
Interviews, group discussions and consultation ..................................... 11
Site visits and discussions with representatives .................................... 11
Section B: HRH situation analysis ............................................................ 12
Framework for situation analysis ........................................................... 12
External factors influencing HRH ........................................................... 13
Geographic factors ........................................................................... 13
Demographic factors ......................................................................... 15
Epidemiological factors...................................................................... 19
Sociocultural factors ......................................................................... 22
Political factors ................................................................................ 23
Economic factors .............................................................................. 24
Internal factors affecting HRH ................................................................. 25
Health care delivery system ............................................................... 25
HRH situation and trends ..................................................................... 30

2
Availability ...................................................................................... 31
Distribution ..................................................................................... 32
Recruitment and retention ................................................................. 34
Skill mix and competencies ................................................................ 36
HRH policy ......................................................................................... 36
HRH education ................................................................................... 37
Pre-service training of health professionals .......................................... 37
Postgraduate training of health professionals ....................................... 45
Continuous professional development ................................................. 47
HRH management systems .................................................................. 48
Recruitment and bonding .................................................................. 48
Remuneration .................................................................................. 51
Non-financial incentives/working conditions ......................................... 53
Performance management ................................................................. 55
Quality assurance ............................................................................. 56
HRH information and evidence for decision-making ............................... 57
HRH leadership ................................................................................... 59
Current HRH coordination mechanism and champions ........................... 59
HRH stewardship .............................................................................. 60
HRH partnerships ................................................................................ 61
HRH financing .................................................................................... 63
HRH requirements .............................................................................. 63
Scenario 1: Achieving staffing standards (Tables 18 and 19) .................. 64
Scenario 2: Reducing the expatriate health workforce (Tables 23 and 24) 68

3
SECTION C: Health workforce strategic plan .............................................. 72
Vision ................................................................................................ 72
Mission .............................................................................................. 72
Guiding principles ............................................................................... 72
Strategies and interventions ................................................................. 75
Strategic line 1: Policy, leadership and management systems ................. 75
Strategic line 2: HRH education and training ........................................ 80
Strategic line 3: HRH Financing and partnerships .................................. 84
Section D: The way forward .................................................................... 86
Annexes ............................................................................................... 88
Annex 1. Technical working group ......................................................... 88
Annex 2. Stakeholders engaged in development and validation ................. 90
Annex 3. HRH positions approved by the CSC for health-care facilities under
the MOHG (staffing standards) ............................................................. 92
Annex 4. Distribution of expatriate/local HRH, standards and vacancy rates in
hospitals level 1–4 (regional/atoll) (Source: MOHG) ................................. 95
Annex 5. Distribution of expatriate/local HRH, standards and vacancy rates in
health centres level 1–4 (Source: MOHG) ............................................... 97
Annex 6. Distribution of HRH, standards and vacancy rates in all health
facilities under the MOHG (MOHG + institutions information missing) ......... 98
References .......................................................................................... 101

4
List of tables
Table 1 Population distribution among atolls 18
Table 2 Concentration of population in islands 19
Table 3 Key health indicators for Maldives 20
Table 4 Incidence of selected communicable diseases 21
Table 5 Ten leading causes of mortality 21
Table 6 Utilization of regional hospitals, 2011 26
Table 7 Utilization of atoll hospitals, 2011 27
Table 8 Vacancy rates by cadre in hospitals, levels 1–4 31
Table 9 Vacancy rates by cadre in health centres, levels 1–4 32
Table 10 Ratio of population to health workers 33
Table 11 Number of local health workers employed in the atolls 33
Table 12 Pass rates at GCE O-Level examination 38
Table 13 Number of students sitting GCE A-Level examination 38
Table 14 Number of students enrolled and graduated in different courses
offered by FHS
42
Table 15 Expected year of return for postgraduate trainees (other than
medical) sent for training overseas by the MOHG (Source
MOHG)
45
Table 16 Postgraduate medical education enrolment supported by MOHG
and international partners, since 2000
46
Table 17 Postgraduate medical students graduated, since 2000 47
Table 18 Cost of training priority cadres to reach staffing standards 66
Table 19 Proposed calendar to achieve staffing standards for key cadres 67
Table 20 Cost of training medical doctors (general and specialists) to
replace all expatriates
69
Table 21 Cost of training other health professionals to replace expatriates
70
Table 22 Forward plan 86
5
List of figures
Figure 1 The conceptual framework 13
Figure 2 Map of Maldives 15
Figure 3 Projected mid-year population, 2013–2018 16
Figure 4 Projected population pyramids for Maldives, 2014 and
2018
17
Figure 5 Trends in infant mortality rate, under-5 mortality rate
and maternal mortality ratio, 2001–2011
20
Figure 6 MMC registrations and requests for certificates of good
standing
35
Figure 7 Total number of medical graduates registered under MMC
(up to June 2013)
39

6
Abbreviations
CHW community health worker
CPD continuous professional development
CSC Civil Services Commission
FHS Faculty of Health Sciences
GCE A-Level General Certificate of Education, Advanced Level
GCE O-Level General Certificate of Education, Ordinary Level
GHWA Global Health Workforce Alliance
HRDMC Human Resource Development and Management Committee
HRH Human Resources for Health
IGMH Indira Gandhi Memorial Hospital
IMF International Monetary Fund
MBBS Bachelor of Medicine, Bachelor of Surgery
MNDF Maldives National Defense Forces
MDG Millennium Development Goal
MIHIS Maldives Integrated Health Information System
MMC Maldives Medical Council
MOHG Ministry of Health and Gender
QAI Quality Assurance and Improvement
WHO World Health Organization
7
Executive summary
Background
The Republic of Maldives has achieved remarkable health gains over the past
few decades. Being a small island nation, Maldives is highly vulnerable to the
effects of globalization as well as epidemiological, socioeconomic, cultural and
political changes. The Human Resources for Health (HRH) situation of the
country is determined by a complex interplay of these factors as well as internal
issues governing HRH such as health financing, policy, management and
training.
Main HRH issues
• Weak health workforce leadership and management at all levels
• Fragmented information management systems leading to limitations in
evidence-based decision making
• Difficulties in attracting and retaining health workers in atolls and islands
leading to high turnover and high vacancy rates
• Overdependence on expatriate health professionals
• Inequitable distribution of health workers between Male’ and atolls
• Lack of career and professional development opportunities
• Difficulties in legally binding staff to service/training bonds
• Variability in the quality of pre-service, postgraduate and professional
continuous education
• Underfunding and inefficient use of existing financial resources for HRH

8
Strategic actions
1. Strengthening the systems and structures to effectively manage and support
HRH; improving policies, regulatory frameworks and institutions, and fostering
leadership capacities to adequately perform the essential HRH management and
monitoring functions.
2. Enhancing education and training outputs harmonized with national health
care needs.
3. Increasing financial inputs from public, private and international sources;
streamlining the multi-stakeholder coordination processes, and fostering
bilateral partnerships with organizations, entities, institutions and countries.
Conclusion
To address complex issues in HRH, a well thought out and holistic plan is
needed. A systematic approach to HRH policy, management, leadership,
education and training, and the promotion of partnerships as well as financial
components, should be used in combination to improve the HRH situation of the
country.
9
Section A: Introduction
Background
HRH is a crucial component and pillar of a health system.1 In order to provide
the entire population with access to qualified and efficient services, HRH of an
adequate quantity and skill mix are required, which are equitably distributed,
well-supported and sufficiently motivated.
The World Health Report 2006 – Working together for health reveals an
estimated shortage of almost 4.3 million doctors, midwives, nurses and support
workers worldwide.2 Maldives is not among the 57 countries that face a serious
shortage of health workforce, which negatively influences health-related
Millennium Development Goals (MDGs). However, there are critical issues
regarding the sustainability of the health workforce and inequitable distribution
of HRH, as well as some concerns about quality. The First Global Forum on HRH,
convened by the Global Health Workforce Alliance (GHWA), agreed on the
Kampala Declaration and Agenda for Global Action to provide guidance to
countries through six interacting strategies focusing on all stages of health
workers' careers from entry to health training, from job recruitment through to
retirement.3
In recent years, challenges in HRH have prompted the Ministry of Health and
Gender (MOHG) in Maldives to put greater focus and emphasis on the health
workforce. By achieving better HRH management and development, the MOHG
expects to ensure that all Maldivians have equitable access to comprehensive
health services provided by a competent and professional health workforce.

10
During the past decade, the MOHG made attempts to solve HRH issues by
implementing the National Human Resources for Health Plan (2001–2010).4 The
MOHG made significant progress in expanding and upgrading regional, atoll and
island level health facilities, and in increasing the number of local and expatriate
HRH as planned. However, important HRH issues persist.
Since challenges associated with HRH concern a wide range of stakeholders,
solving such complex issues requires a well thought out strategic plan resulting
from intense policy dialogue among all related actors, following the country
coordination and facilitation approach delineated by the GHWA.3,5 Thus, the
MOHG developed a structured approach to analyse the HRH situation and put
together the National Health Workforce Strategic Plan 2014–2018 based on the
findings of this analysis. The strategic plan will: a) guide MOHG action in
securing support for HRH development; b) provide a framework for making
consistent decisions for planning HRH and their capacity-building; c) help
monitor MOHG action on HRH development and management; d) identify gaps
in the system that need to be addressed; and e) help estimate the costs of
human resource training and deployment, and assess the sustainability of the
existing workforce by modelling different scenarios. In turn, the HRH strategic
plan will help secure better finances from the national budget by prioritizing
HRH as a critical area with documented evidence.
Methodology
In order to ensure current and accurate information to support evidence-based
recommendations, several approaches were used for data collection.
Review of records, reports and literature
An extensive study of available documents and databases from the MOHG,
WHO, Faculty of Health Sciences (FHS) and other sources was undertaken.

11
These documents were analysed and discussed with the relevant authorities and
stakeholders.
Interviews, group discussions and consultation
A series of consultative meetings was conducted with representatives, key
stakeholders and/or decision-makers from several organizations including WHO,
MOHG, FHS, Maldives Medical Council (MMC), Maldives Nursing Council and
Maldivian Board of Health Services.
Site visits and discussions with representatives
Site visits and discussions with those engaged in HRH action have been carried
out, including the FHS, Indira Gandhi Memorial Hospital (IGMH), HulhuMale’
Hospital, ADK Hospital and health centres. A technical working group was
established comprising all concerned stakeholders, including the MOHG, FHS,
private sector, Civil Service Commission (CSC) and Ministry of Finance and
Treasury.
This HRH strategic plan was developed through a participatory and consultative
process, with the lead role taken by the technical working group (Annex 1) and
findings from two stakeholders’ consultations (Annex 2) representing various
government agencies, regulatory bodies and developmental partners.
The findings were presented in a multi-stakeholder meeting, for validation of
the situation analysis and dialogue on the proposed strategies. This process was
complemented by means of an online consultation with all stakeholders for
reviewing, revising and finalizing this strategic document. A full revision of the
NHWSP proposal was undertaken adjusting to new policies and plans of the new
government. The final version was presented at a national launching meeting in
April 2014.

12
Section B: HRH situation analysis
Framework for situation analysis
The HRH situation is dynamic as it is affected by the interplay of complex
conditions at local, country and global levels. A country’s HRH situation is
affected by factors both external and internal to the health system. The various
transitions in global and regional contexts often influence HRH systems. At the
same time, changes in the sociodemographic profile and in epidemiological,
socioeconomic, political and cultural circumstances have both direct and indirect
effects on health systems and HRH. The HRH situation is determined by a
complex interplay of these external factors as well as internal factors governing
the health workforce.
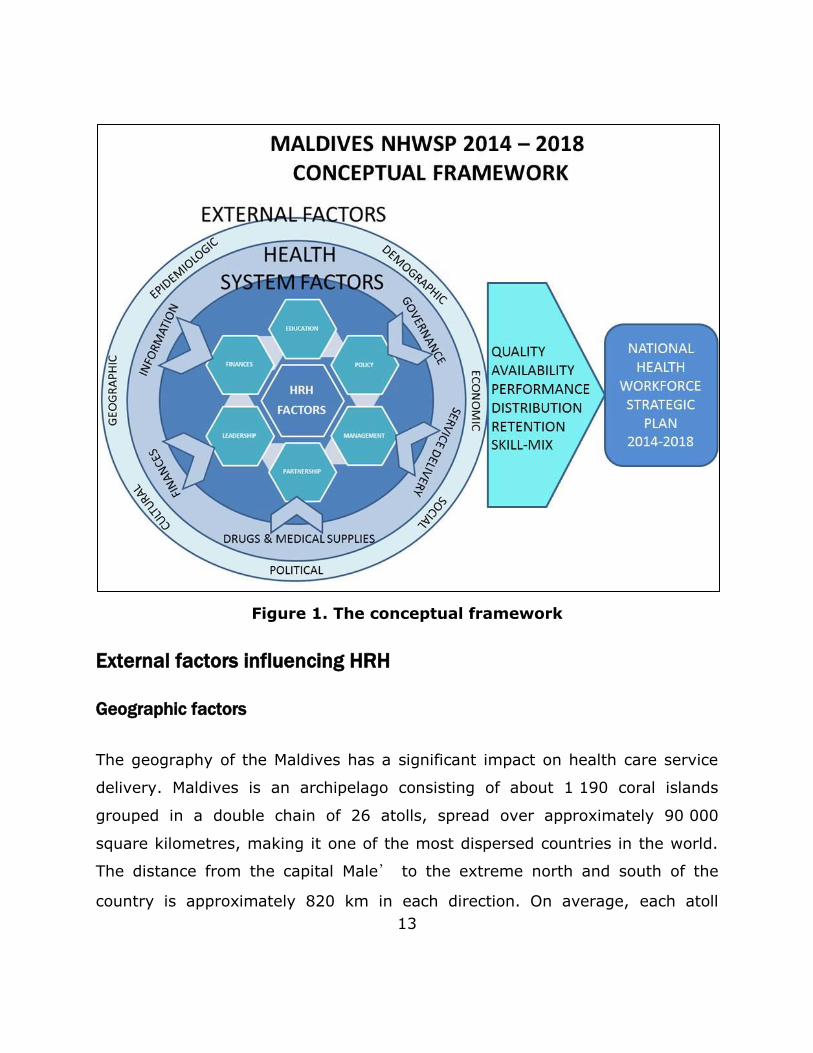
The conceptual framework shown in Figure 1 is an adaptation of the HRH Action
Framework developed by the GHWA. It is designed to facilitate an
understanding of the current HRH situation in Maldives from a broad
perspective, taking into account factors both external and internal to the health
sector and the link between these driving forces and the different dimensions of
the health workforce.
This HRH situation analysis was guided by the conceptual framework.
Geographic, epidemiological, sociocultural, political and economic factors were
assessed. In order to assess the HRH system, the six dimensions of the HRH
Action Framework (HRH management, leadership, partnership, finance,
education and policy) were analysed. This situation analysis provides evidence-
based information for the development of HRH strategies (as detailed in Section
C).
13
Figure 1. The conceptual framework
External factors influencing HRH
Geographic factors
The geography of the Maldives has a significant impact on health care service
delivery. Maldives is an archipelago consisting of about 1 190 coral islands
grouped in a double chain of 26 atolls, spread over approximately 90 000
square kilometres, making it one of the most dispersed countries in the world.
The distance from the capital Male’ to the extreme north and south of the
country is approximately 820 km in each direction. On average, each atoll

14
includes 5–10 inhabited islands. The average land area of an island is only 1–2
square kilometres. These geographical characteristics, and the fact that the
population is extremely dispersed, have a significant impact on the delivery of
services at central, atoll and island levels.
Health facilities are scattered across the country. The geographically dispersed
layout and a weak transportation network often lead to disparities in access to
health services between different atolls. Patients travel from the islands to the
nearest atoll hospital; more complex patients are referred to Male’, where the
only tertiary health care facility (IGMH) is located. As a result of the high cost of
patient transportation, and other elements such as seasonal extreme weather
conditions, access to health care is becoming increasingly challenging.
This is further complicated by the lack of a structured national transportation
network between islands/atolls and Male’. Moreover, the transport network
that has evolved over the years is mostly oriented towards developing links
between the islands and their atoll capital, and between atolls and Male’. In
some situations, even links between the islands and the relevant atoll capital
are not well developed whenever the capital is deemed too far, and links have
preferentially been developed with Male’. Links between atolls are often weak;
therefore, it can be more convenient and cheaper to refer patients to the
tertiary hospital in Male’ rather than a regional hospital, even if the latter is
geographically closer to the island. This situation is generating huge pressure on
IGMH.
The following map of Maldives (Figure 2) illustrates the logistical challenges in
providing equitable health care, due to the unique geographical nature of the
country.

15
Figure 2. Map of Maldives
Demographic factors
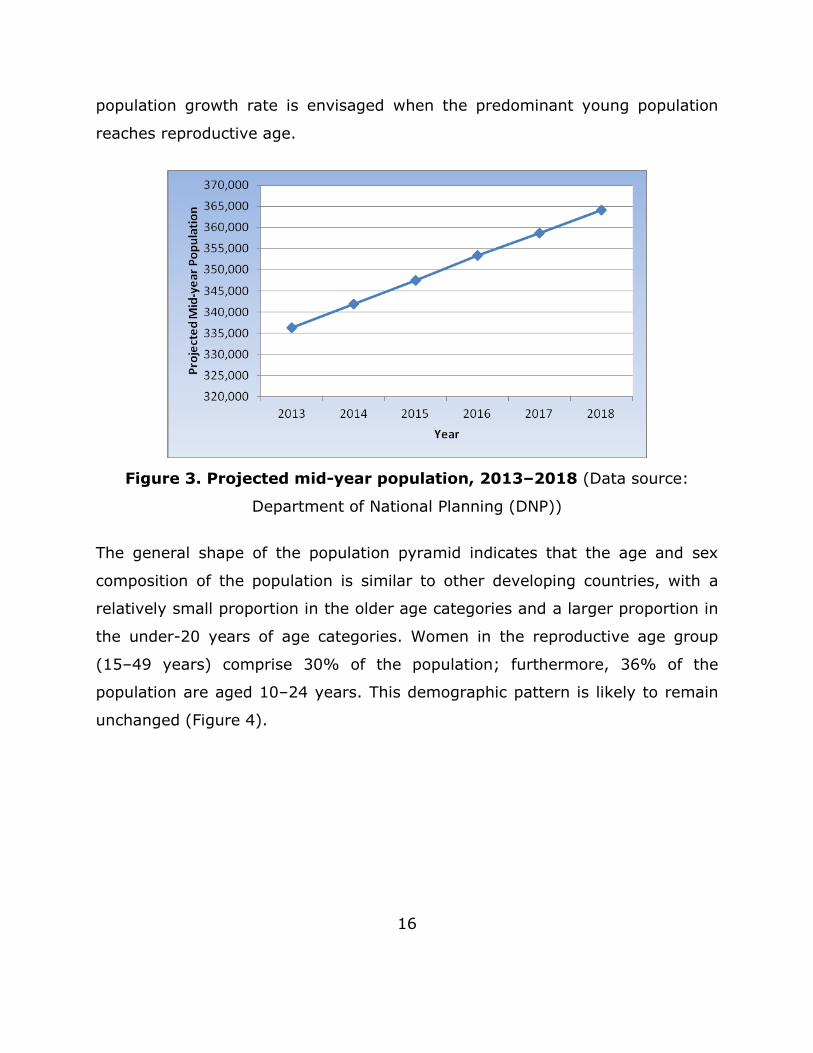
The Population and Housing Census of Maldives 2006 indicated that the
population was 298 968, with an annual average population growth rate of
1.6%. The estimated mid-year population for 2013 was 335 000. Figure 3
provides population projections from 2013 to 2018.6 The population growth rate
shows a trend towards stabilization, mostly due to a decline in birth and death
rates during the first years of the last decade. However, it should be noted that
birth rates have been slowly increasing in recent years and a discrete rise in
16
population growth rate is envisaged when the predominant young population
reaches reproductive age.
Figure 3. Projected mid-year population, 2013–2018 (Data source:
Department of National Planning (DNP))
The general shape of the population pyramid indicates that the age and sex
composition of the population is similar to other developing countries, with a
relatively small proportion in the older age categories and a larger proportion in
the under-20 years of age categories. Women in the reproductive age group
(15–49 years) comprise 30% of the population; furthermore, 36% of the
population are aged 10–24 years. This demographic pattern is likely to remain
unchanged (Figure 4).

17
Figure 4. Projected population pyramids for Maldives, 2014 and 2018
(Data source: DNP)
According to the Household Income and Expenditures Survey 2009–2010,
estimated average household size is 6.7 people per household (7 in Male’ and
5.9 in atolls). Around 35% of the population is based in Male’ and 65% in the
atolls. Rapid and unplanned urbanization of Male’ has seen one of the world’s
smallest capitals double its population within 16 years, from 55 000 inhabitants
in 1990 to 152 000 in 2006, making it by far the most densely populated island
in the country and one of the world’s most densely populated capitals. Much of
this is a result of inward migration from other atolls, due to the availability of
better education, social services and job opportunities in Male’.6 Table 1 details
the population distribution among atolls.6

18
Table 1. Population distribution among atolls
Atoll Population
( Census 2006 )
North Thiladhunmathi (HA) 13 495
South Thiladhunmathi (HDh) 16 237
North Miladhunmadulu (Sh) 11 940
South Miladhunmadulu (N) 10 015
North Maalhosmadulu (R) 14 756
South Maalhosmadulu (B) 9 578
Faadhippolhu (Lh) 9 190
Male’ Atoll (K)* 119 134
North Ari Atoll (AA) 5 776
South Ari Atoll (ADh) 8 379
Felidhu Atoll (V) 1 606
Mulakatholhu (M) 4 710
North Nilandhe Atoll (F) 3 765
South Nilandhe Atoll (Dh) 4 967
Kolhumadulu (Th) 8 493
Hadhdhunmathi (L) 11 990
North Huvadhu Atoll (GA) 8 262
South Huvadhu Atoll (GDh) 11 013
Fuvahmulah (Gn) 7 636
Addu Atoll (S) 18 026
(Data source: DNP)
*Includes the population of Male’, the capital of Maldives
Out of 1190 islands in Maldives, only 194 are considered as administrative
islands with inhabitants. There is only one island (Male’) with a population over
25 000, whereas there are 72 islands with a population less than 500 (Table 2).
Due to economies of scale, providing equitable health services for this widely
dispersed population is challenging.

19
Table 2. Concentration of population in islands
Population size range Number of islands
Administrative islands 194
<500 72
500–999 66
1 000–1 999 42
2 000–4 999 12
5 000–24 999 3
25 000 and over 1
Non-administrative islands*
100–399 111
(Data source: DNP)
*Non-administrative islands include tourist resorts (104), industrial islands and islands used
for other purposes.
Epidemiological factors
The health status of the Maldivian people has improved in the past few decades.
In 1977, life expectancy at birth was 46.5 years. In 2011, it was 73 years for
males and 75 years for females. In 1990, 34 babies per 1000 live births died
before reaching the age of one. In 2011, the comparative infant mortality rate
was 9 per 1000 live births, with a majority of the infant deaths occurring in the
neonatal period. The maternal mortality ratio declined from about 500 per
100 000 live births in 1990 to 56 per 100 000 live births in 2011, and the MDG
target of reducing maternal mortality ratio by half by 2015 has already been
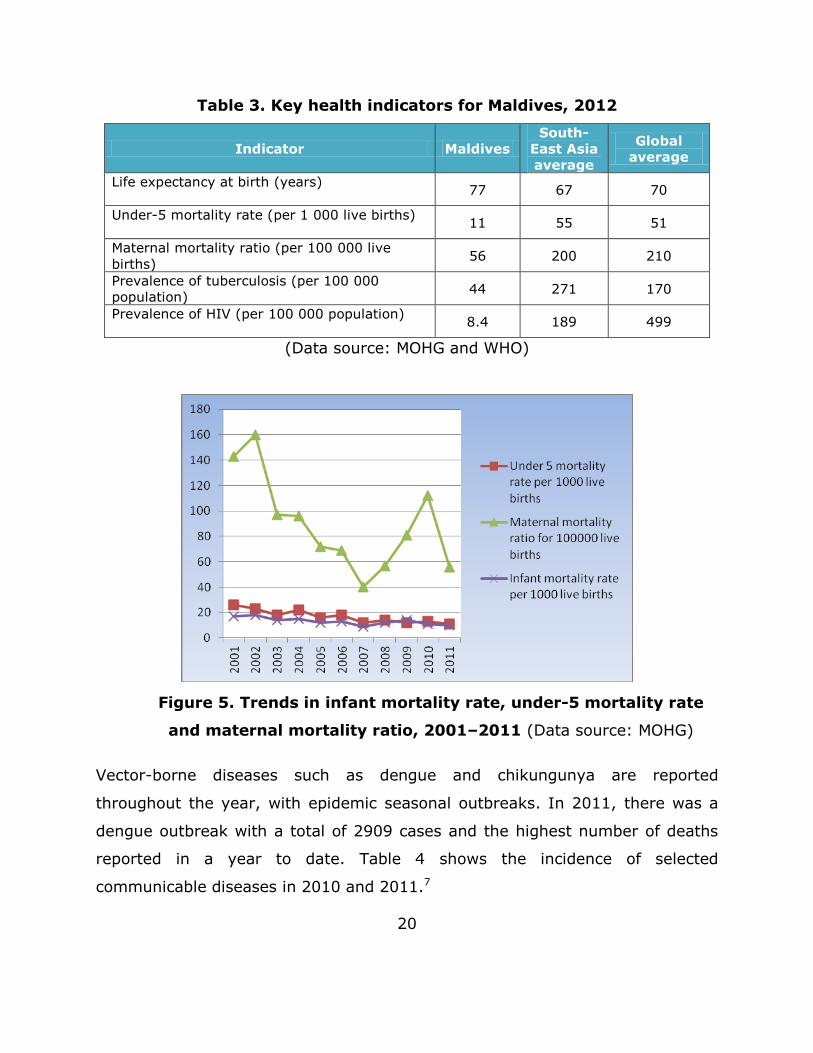
achieved.7 Table 3 provides key health indicators for Maldives, while Figure 5
illustrates the trends in some of these indicators.
20
Table 3. Key health indicators for Maldives, 2012
Indicator Maldives
South-
East Asia
average
Global
average
Life expectancy at birth (years)
77 67 70
Under-5 mortality rate (per 1 000 live births)
11 55 51
Maternal mortality ratio (per 100 000 live
births) 56 200 210
Prevalence of tuberculosis (per 100 000
population) 44 271 170
Prevalence of HIV (per 100 000 population)
8.4 189 499
(Data source: MOHG and WHO)
Figure 5. Trends in infant mortality rate, under-5 mortality rate
and maternal mortality ratio, 2001–2011 (Data source: MOHG)
Vector-borne diseases such as dengue and chikungunya are reported
throughout the year, with epidemic seasonal outbreaks. In 2011, there was a
dengue outbreak with a total of 2909 cases and the highest number of deaths
reported in a year to date. Table 4 shows the incidence of selected
communicable diseases in 2010 and 2011.7

21
Table 4. Incidence of selected communicable diseases
Disease 2010 2011
Acute respiratory infections 92 553 113 834
Viral fever 54 718 70 608
Acute gastroenteritis/diarrhoea 18 509 18 979
Conjunctivitis 4 606 2 878
Dengue fever 920 2 909
Typhoid fever 137 61
Scrub typhus 61 91
Mumps 50 69
Leprosy 7 13
(Data source: MOHG)
In general, Maldives is in transition from the burden of communicable diseases
to a higher burden of noncommunicable diseases. In 2011, the leading cause of
death was other forms of heart disease (Table 5). 7
Table 5. Ten leading causes of mortality, 2011
Cause Number of deaths
Other forms of heart disease 130
Ill-defined and unknown causes 120
Ischaemic heart diseases 113
Cerebrovascular diseases 108
Chronic lower respiratory diseases 80
Hypertensive disease 79
Malignant neoplasms 78
Accidental injury 37
Diabetes mellitus 36
Renal failure 28
(Data source: MOHG)
22
Sociocultural factors
Maldivian culture is extensive and varied. Cultural aspects influence both the
health system in general, and the health workforce specifically.
Among Maldivians, the level of attractiveness of health-related occupations
varies depending on the occupation. ”Low level” jobs are perceived as
unattractive by youth; health attendants and similar positions, for example, are
mainly held by expatriate workers. The explanations given include the low
remuneration and lack of social recognition and prestige for these jobs. Young
people prefer to remain unemployed rather than apply for these jobs, and their
families support this behaviour. Youth and their families expect an office job
(preferably within a tourist resort) or a Civil Service job after completion of
their ordinary or advanced-level qualifications, or a job in a shop at worst. A job
in a health facility where they would have to give hygiene-related care is not
considered as desirable.
The global predominance of female nurses is taken to the limit in Maldives,
where no male nurses are present among the entire workforce. Nursing being
considered a woman’s profession leads to young Maldivian men not applying for
nursing training. Despite a global tendency towards feminization of the medical
profession, in Maldives it remains being a predominantly male profession.6
However, there are some women among the predominantly male community
health workers (CHWs).
As in other Islamic countries, Maldivians are in general reluctant to accept
health care requiring the physical examination of a woman by a male
professional. Such cultural and religious factors pose additional challenges for
staffing, particularly in smaller health posts in remote areas.
23
Expectations about access, availability and quality of health services are very
high among the Maldivian population. Even on the smaller islands (less than
500 inhabitants), there is a strong demand for a full-time medical doctor, as
well as a secondary grade school and full-time teacher. This aspect might have
been induced by politically-influenced decisions and promises made to the
population in the past.
Political factors
The Executive of the country is the President, who is both Chief of State and
Head of Government. The Cabinet of ministers is appointed by the President.
There are 16 ministries at present. The Legislative is a unicameral entity called
the People's Council or People's Majlis (77 seats; members are elected by direct
vote to serve 5-year terms). A new Government was elected in November 2013.
In Maldives, an ongoing decentralization process has devolved power to 20 atoll
councils, including some public health responsibilities, as stated in Chapter 4,
article 24 of the Decentralization of the Administrative Division of the Maldives
Act: “The island council shall provide the following municipal services to the
people of the island: … (f) In accordance with the Law of the Maldives, provide
primary health care and other basic health security services”. The atoll council
plays a coordinating, guiding and supportive role in managing the islands’
development and guiding stakeholders in planning development programmes.
The MOHG has kept its central role in the delivery of health care services and
has maintained a partnership with local councils to provide primary health care
services. However, the Decentralization Act does not provide a definition or
define the services comprised under the term ”primary health care”. The MOHG
felt the need for a strong network linking health centres with other levels of the
health care system, and has kept them under the MOHG umbrella to avoid
fragmentation of government-funded health services.

24
Economic factors
Maldives ranks among the lower segment of the middle-income countries.
However, its gross domestic product (GDP) has grown at an annual rate of
6–8% over the past two decades, driven by investments in tourism and the low
level of inflation. Significant progress has also been achieved in human and
social development over the past two decades, lifting Maldives from its status
as one of the 20 poorest countries in the 1970s to one that shares the
characteristics of a lower-middle income country today, with a GDP of MVR
29 936 million (US$ 1 941 million) and a per capita GDP of US$ 6 067.8
However, Maldives is now facing an alarming escalation in health care costs,
which places a burden on the Government. The population profile and disease
patterns have caused the Government to greatly reconsider its financial
commitment to the health system. This has led to a blueprint for health reform
focusing on the most pressing issues, particularly the introduction of a
mandatory universal national health insurance scheme (Aasandha) at the
beginning of 2012. Furthermore, in recent years the country’s financial situation
has deteriorated. According to an assessment by the International Monetary
Fund (IMF) in 2012, the economy is slowing, inflation has risen, and the fiscal
position is in a critically vulnerable state. Overestimated revenues and
underestimated expenditures are creating a significant budgetary gap (11% of
GDP estimated for 2013) which will need to be financed, creating major
concerns about debt sustainability. This might have an impact on the health
care sector if two of the avenues proposed by the IMF – reducing Aasandha
coverage and reducing the public wage bill – were to be applied.9
25
Internal factors affecting HRH
Health care delivery system
Public sector
The MOHG is the main health service provider in Maldives. The health system is
organized into a broad three-tier referral system, comprising the national
referral hospital, regional and atoll hospitals, and health centres. There are 20
hospitals (excepting IGMH) in the country. Hospitals are graded (level 1–4)
depending on capacity, population covered and workload.
With 275 beds, IGMH delivers tertiary-level curative care and serves as the
central referral hospital for the entire country. In 2011, 37% of hospital
inpatient care was provided by IGMH, with all other health facilities in the
country accounting for 63%.1 Similar proportions were observed with regards to
the provision of outpatient care. This over-utilization of the national referral
hospital highlights serious issues related to the implementation of the referral
system, the overall management of the national health system, and the health-
seeking behaviour of the population.6
There are six regional hospitals providing secondary-level curative services and,
through public health units, implementing preventive health programmes. The
regional hospitals provide inpatient and outpatient care, diagnostic services and
specialty care, as well as emergency care for patients referred from other
centres. Hulhumale Hospital near the capital is considered a level 1 hospital but
due to its close distance to IGMH doesn’t function as a regional hospital.
The utilization of regional hospitals is variable (Table 6). While the reasons
affecting utilization could be multifactorial, a statistically significant high
correlation (r=0.63) was found between the bed occupancy rate and the
26
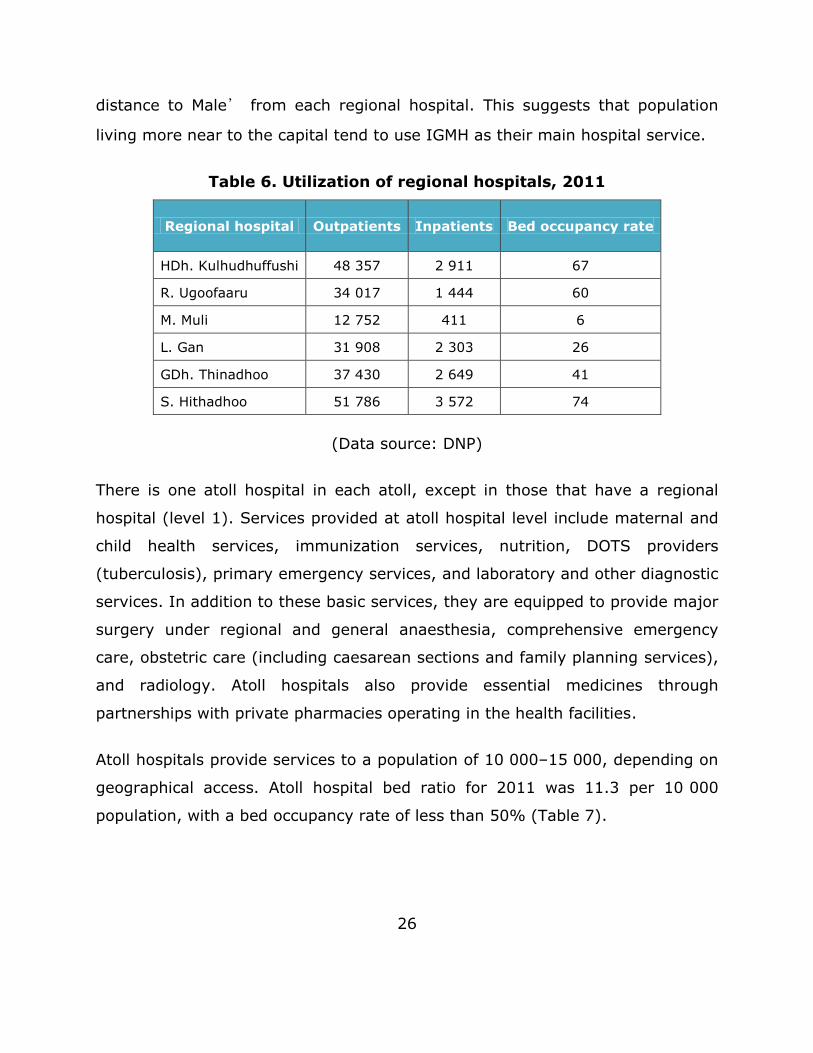
distance to Male’ from each regional hospital. This suggests that population
living more near to the capital tend to use IGMH as their main hospital service.
Table 6. Utilization of regional hospitals, 2011
Regional hospital Outpatients Inpatients Bed occupancy rate
HDh. Kulhudhuffushi 48 357 2 911 67
R. Ugoofaaru 34 017 1 444 60
M. Muli 12 752 411 6
L. Gan 31 908 2 303 26
GDh. Thinadhoo 37 430 2 649 41
S. Hithadhoo 51 786 3 572 74
(Data source: DNP)
There is one atoll hospital in each atoll, except in those that have a regional
hospital (level 1). Services provided at atoll hospital level include maternal and
child health services, immunization services, nutrition, DOTS providers
(tuberculosis), primary emergency services, and laboratory and other diagnostic
services. In addition to these basic services, they are equipped to provide major
surgery under regional and general anaesthesia, comprehensive emergency
care, obstetric care (including caesarean sections and family planning services),
and radiology. Atoll hospitals also provide essential medicines through
partnerships with private pharmacies operating in the health facilities.
Atoll hospitals provide services to a population of 10 000–15 000, depending on
geographical access. Atoll hospital bed ratio for 2011 was 11.3 per 10 000
population, with a bed occupancy rate of less than 50% (Table 7).

27
Table 7. Utilization of atoll hospitals, 2011
Hospital Inpatient Outpatient Bed occupancy
rate
HA. Dhiddhoo 22 677 1 108 9
Sh. Funadhoo 10 428 547 33
N. Manadhoo 12 476 674 22
B. Eydhafushi 17 613 648 29
Lh. Naifaru 25 951 1 014 41
AA. Rasdhoo 6 735 221 10
ADh. Mahibadhoo 18 340 592 20
V. Felidhoo 3 955 109 5
F. Nilandhoo 10 110 456 23
Dh. Kudahuvadhoo 14 851 615 11
Th. Veymandoo 16 024 765 17
Ga. Villigilli 19 961 698 30
Gn. Fuahmulah 33 851 2 174 35
Hulhumale Hospital 1 368 133 24
(Data source: DNP)
Regional hospitals, or atoll hospitals in atolls with no regional facility, coordinate
and supervise the work of health centres in the different islands of each atoll.
There are 121 health centres in Maldives, graded as level 1–4 depending on the
population covered, patient load, and average bed occupancy based on
inpatient bed capacity. Each atoll has between 3 to 13 health centres serving a
population ranging from 500–10 000, with an average of 1 health centre per
2300 population. Even the smallest island population is served through a public-

28
financed health-care facility. About 85% of health centres are staffed by at least
one medical officer (levels 1–3). The remaining 15% (level 4) are staffed by
trained health workers such as nurses, midwives and CHWs.
Health centres provide a comprehensive service in all areas of primary health
care, including maternal and child health services, immunization services,
communicable diseases, noncommunicable diseases, DOTS providers
(tuberculosis), primary emergency services and laboratory services. Some
health centres have provision for simple medical and surgical care, and basic
emergency obstetric care. However, space for inpatient care is limited.
Level 4 health centres were previously referred to as health posts. There is a
total of 27 level 4 health centres; each is primarily equipped with 1–2
observation beds, a consultation room and office space. Level 4 health centres
provide basic health care and preventative services. They are staffed by trained
CHWs, nurses, midwives and support staff. CHWs play an important role in
these settings in the absence of medical officers. They have clinical, managerial
and public health roles with a mandate to strengthen the link between the
community and the health system. A level 4 health centre serves a population
of less than 500.
The utilization of health centres is low. The reasons appear to be multifactorial,
with several management-related issues. Health centres and atoll hospitals lack
proper maintenance, and the 2013 costing survey indicated that these health
facilities frequently experience shortages in supplies, drugs and equipment.
There has been a continuing depletion of experienced professionals at all levels.
Human resources are inadequate in number to provide the basic package of
services. In addition, there is a high turnover of staff at all levels, which has a
negative impact on continuity of care. Expensive medical equipment is

29
sometimes dispatched to health centres with no adequate training provided to
health care workers.10
Another major issue is the absence of a gatekeeping referral system. The
population often seek specialist care without any referral from a general
practitioner or CHW, leading to important inefficiencies, overloaded tertiary-care
services and patients being at risk of receiving inappropriate care. This health-
care-seeking behaviour is nowadays extended to areas where traditionally mid-
level cadres were successfully delivering high-quality care at the primary health
care level; for example, maternal and neonatal care, including normal deliveries
provided by midwives. There is now a growing expectation that even
uncomplicated deliveries should be attended by an obstetrician and that a
paediatrician should attend to each and every newborn.
There is a small 21 beds military hospital (Sehahiya Hospital) in Male staffed
with around 57 workers including 22 specialist and 7 general doctors providing
services to all uniformed bodies (MNDF, police, customs, etc.) and their families’
Private sector
There are three private hospitals in Maldives: ADK and Medica hospitals located
in Male’, and the International Medical and Diagnostic Centre located in
Hithadhoo, Addu Atoll. There are 99 private medical clinics of small capacity: 10
eye clinics; 2 ear, nose and throat clinics; 13 dental centres; and 290
dispensing pharmacies. The majority of private clinics are located in Male’.
These private facilities incurred 11% of total health care expenditure in 2011.6
In terms of HRH, the private sector comprises of 357 employees of whom 33
are doctors, 54 are nurses and 244 are pharmacists. However, dual practice
(public/private) is common in Maldives.

30
Alternative medical system
The MOHG is attempting to register traditional healers in order to have a better
record of the overall health system in Maldives. It is estimated that there are
more than 200 traditional healers in the country, with an average of 2 per
island. However, only 50 of these practitioners have registered to date, all of
whom are located in Male’. There are traditional healers who charge fees for
their services, but there is no mechanism to get them registered. Practitioners
working informally or in shadow clinics are difficult to count, since there is no
tracking mechanism for them. However, the general opinion is that this
category is much larger than the 50 practitioners currently registered. The
category comprises native traditional practitioners and practitioners of Indian
and Chinese medicine.
HRH situation and trends
The Maldivian health service system has a high dependence on expatriate
health professionals, especially doctors and nurses. Although there has been a
gradual increase in the number of local health professionals, the expansion of
health services, high turnover of staff and limited capacity to locally produce
health professionals has led to reliance on international recruitment.
In 2010, there were 525 doctors in Maldives with a ratio of 1 doctor per 610
persons; however, 81% of these doctors were expatriates. The number of
registered nurses totalled 1868, of which 55% were expatriates. At the
community level, there were 805 paramedical workers in the public sector, 278
CHWs, 313 family health workers and 214 traditional birth attendants, all of
whom were local.6

31
The major HRH challenges that the Maldivian health system faces include
inequitable distribution, overall shortages of HRH, retention of staff in the
islands, and inadequate skill mix and competencies.
Availability
Although the size of the health workforce has gradually increased in Maldives,
the health service system is facing HRH shortages in island facilities, particularly
shortages of doctors and nurses. At the time of writing, there were no official
staffing standards approved in Maldives. The number of positions approved by
the CSC is used as a proxy for planning purposes. Overall vacancy rate is 43%,
with 40% in hospitals (excepting IGMH) and 55% in health centres (see Tables
8 and 9). IGMH is the best staffed health facility in the country with a 17.6%
vacancy rate. However, there are key specific cadres that are in low availability
such as anaesthesiologists (60% vacancy rate) or paediatricians (50%); see
Annexes 4, 5 and 6.
Table 8. Vacancy rates by cadre in hospitals, levels 1–4
Total posts
approved
Total occupied Total gap Vacancy rate
Specialist doctors 186 77 109 59%
General doctors 100 94 6 6%
Nurses 1 051 666 385 37%
CHWs (all categories) 70 5 65 93%
Regional/atoll
Manager 20 8 12 60%
(Data source: MOHG)

32
Table 9. Vacancy rates by cadre in health centres, levels 1–4
Total posts
approved
Total occupied Total gap Vacancy rate
General doctors 114 110 4 4%
Nurses 956 545 411 43%
Midwives 141 0 145 100%
CHWs (all categories) 182 26 156 86%
Laboratory technicians 114 68 46 40%
(Data source: MOHG)
Due to the absence of a medical school in Maldives and the limitations in
production capacity of other health professionals in local academic institutions,
the number of local health workers is limited. Therefore, there is a strong need
to rely on the foreign health workforce. This high dependence on expatriates
poses important challenges in regard to the management of the Maldives HRH
system.
Distribution
About 90% of health professionals were employed in the public sector in 2010,
an increase since 2005 (from 85%). The distribution of health staff by
geographical location in 2010 showed that 27% of medical and paramedical
staff (including nurses) were deployed in Male’, whereas 72% were deployed
in the atolls. The relation between population and HRH in Male’ and the atolls
is shown in Table 10. The ratio of population to doctors was 507:1 in Male’
compared to 683:1 in the atolls. However, the ratio for nurses was much more
equitable (168:1 in Male’ compared with 173:1 in atolls).6
It is worth noting that the HRH density in Maldives (as defined by number of
doctors, nurses and midwives per 1000 population) is 7.5 per 1000, which falls
well above the minimum recommended by WHO of 2.28 per 1000.

33
Table 10. Ratio of population to health workers
Profession
Maldives
(pop = 320 000)
Male’
(pop = 110 998)
Atolls
(pop = 209 012)
All doctors 609:1 507:1 683:1
General doctors 970:1 1 047:1 933:1
Specialists 1 641:1 982:1 2 549:1
Nurses 171:1 168:1 173:1
(Data source: DNP)
Table 11 illustrates the increasing preference of local health workers for working
in Male’ rather than the atolls. The proportion of local doctors working in the
atolls decreased from 7.3% in 2005 (14 out of 190) to 1.2% (4 out of 324) in
2012. The situation for nurses and other cadres, despite following a similar
trend, is not as acute: in 2005 the proportion of nurses working in the atolls
was 61.4% (312 out of 508), while in 2012 it was 48.8% (627 out of 1282).
Table 11. Number of local health workers employed in the atolls
Profession
2005 2009 2010 2012*
Expat Local Expat Local Expat Local Expat Local
All doctors 176 14 317 0 300 6 320 4
General
doctors 124 12 237 0 218 6 248 3
Specialists 52 2 80 0 82 0 72 1
Nurses 196 312 719 481 639 569 655 627
Laboratory
technicians 50 27 79 41 94 41 113 40
CHWs 0 186 0 228 0 276 0 N/A
Family
health
workers
0 340 0 283 0 313 0 N/A
Data sources: DNP (2007–2012), * MOHG (2012)

34
At present, the majority of local staff prefer a posting in Male’, and the
majority of expatriates are sent to rural areas (small islands). There is currently
no health sector specific policy on internal staff movement, other than that of
the CSC and MOHG. The MOHG is unable to accommodate staff transfer
requests from the islands to Male’, and from lower service levels to higher
levels due to the difficulty in filling the vacancies of technical positions.
Recruitment and retention
The number of new Maldivian doctors (MBBS) and specialists registered with the
Maldives Medical Council (MMC) has seen an exponential increase in the past
few years. However, there is only a marginal increase in the number of local
doctors working in the public sector, from 85 in 2005 to 98 in 2012. This
indicates that local doctors have been drained from public health services,
either to the private sector or to other countries. Looking to the number of
requests to the MMC for certificates of good standing – which is a mandatory
requirement for registration with medical councils in other countries and
therefore a proxy to intention to emigrate – there has been an increase from 3
in 208 to 20 in 2013 (Figure 6).
There is a high staff turnover in the islands, particularly among doctors and
nurses. The causes of low retention, given by professionals appointed in these
facilities, are (besides those derived from the remote and isolated environment)
derived from weaknesses of the health system, such as poorly equipped and
maintained facilities and shortages of drugs and medical materials.

35
Figure 6. MMC registrations and requests for certificates of good
standing (Source: MMC)
The lack of essential services such as schools, banks and other facilities is also
reported as a disincentive to accept appointments in remote islands. Some
expatriate professionals also report hostile relationships with local populations,
particularly when there are complications or fatal outcomes. A small population
generates a professionally unchallenging environment, particularly for younger
professionals. Most international staff use appointments in remote areas as a
stepping-stone, to acquire experience which helps them to move somewhere
else. Salaries in neighbouring countries have also increased in the last few
years, which make Maldivian wages less attractive for foreign professionals.
In the past, nurses trained at FHS were immediately recruited to island health
facilities due to the existence of service bonds. However, despite tuition fees
still being highly subsidised by the Government, there are currently no bonding
contracts and direct recruitment of nurses is not possible anymore. Therefore,
graduate nurses need to apply for posts advertised through the official
recruitment system. Compared to nurses, most positions for CHWs are based in
0
5
10
15
20
25
0
10
20
30
40
50
60
70
Go
od
Sta
nd
ing C
ert
ific
ate
s
Re
gis
tra
tio
ns
MMC registrations and Good Standing
Certificates
MBBS Specialists Good standing certificate

36
island health facilities with a limited number in Male’; hence, compared to
other cadres, their retention in remote settings is higher.6
Skill mix and competencies
Despite national health policy aiming at a primary health care orientation of the
health system, Maldivian curative services absorb a large proportion of the
health workforce. The demand for curative health services has been strongly
promoted among the population during the past decades. The health system
initially centred on primary health care during the 1950s to the 1990s, but then
shifted towards a more curative focus with the expansion of infrastructure and
the introduction of doctors in atolls and islands. The limited capacity of the HRH
system in producing technical cadres to provide curative services, and the
subsequent increasing reliance on international recruitment of professionals
from different countries and with different levels of education, together with
some weaknesses in quality assurance mechanisms, poses a challenge to the
quality of care provided.
HRH policy
The Health Master Plan 2006–2015 is the principal planning document of the
Government’s health sector.11 One of its national health goals revolves around
the health workforce including HRH production, recruitment, attraction and
retention, HRH development and provision of appropriate skills. However, due
to several constraints, the HRH component of the plan has not been fully rolled
out.
The national decentralization programme posed important challenges to the
country’s health system. During 2009 to 2012, the Government decided to
devolve health care provision by constituting public health facilities into public–
37
private entities. Health services corporations were established in eight regions,
and all responsibility for public hospitals and health centres was transferred to
these without specific regulatory frameworks. As a result, health services and
HRH were managed differently by each corporation. However, in 2012, the
decentralization was reversed and the assets and responsibilities for health
service delivery were returned to the MOHG. Health workforce management was
transferred back to the CSC and the Central Ministry of Health. These changes
have sometimes left health workers disoriented and unclear about their roles
and reporting channels. Several issues related to HRH derive from these radical
changes such as salary structure, incentive schemes, career advancement etc.,
and are currently being addressed.
HRH education
Pre-service training of health professionals
Pool of applicants for pre-service training programmes for health
professionals
In Maldives, school education for future potential trainees in the health
professions remains an area of concern. Only a small percentage of students
meet the English language, mathematics, science skills and knowledge
requirements to pursue health professions training programmes, with most
students from the atolls not having the opportunity to pursue these subjects in
their local schools. Thus, their background does not sufficiently prepare them to
access nursing, medical or paramedical education. Even some of those who do
have the opportunity to pursue science subjects up to the General Certificate of
Examination Ordinary Level (GCE O-Level) do not have the minimum
competencies required,4 often having to undertake foundation courses to bridge
the gap. The pass rates at GCE O-Level are poor, although improvements have
been achieved in recent years (Table 12). In 2011, only 55% of candidates

38
passed three or more subjects, which is the minimum entry requirement for
degree courses offered by the FHS.6
Table 12. Pass rates at GCE O-Level examinations
2009 2010 2011
Candidates Passed % Candidates Passed % Candidates Passed %
Total 7 137 2 282 32 6 920 2 404 35 6 432 3 538 55
Male’ 1 902 1 054 55 1 894 1 017 54 1 802 1 045 58
Atolls 5 235 1 228 23 5 026 1 387 28 4 630 1 379 30
(Data source: DNP)
There is a sharp fall in enrolment for higher secondary education (21%). The
main reason for this is that only 38 out of the 225 schools in the country offer
education at that level12 (see Table 13).
Table 13. Number of students sitting GCE A-Level examinations
2005 2006 2007 2008 2009 2010 2011
Total 833 1 006 1 024 1 325 1 194 1 338 1 515
Male’ 729 703 780 774 741 847 816
Atolls 104 303 244 551 453 491 699
(Data source: DNP)
Registration, accreditation and quality assurance of health professionals’
education
Doctors need to register with the MMC in order to practice. For expatriates,
approval for registration with MMC requires previous registration with the
medical council in their respective country.13,14 The MMC is currently planning to
implement licensing exams for all doctors wanting to practice in Maldives.
Registration of nurses is under the responsibility of the Maldives Nursing
Council, which defines and regulates the criteria to enter into the profession.

39
Registration of all other health professionals is under the responsibility of the
Maldives Board of Health Sciences.
Doctors registered by the MMC to date represent over 300 medical schools
worldwide, leading to a wide variation in the quality of training standards. The
MMC does not screen applicants according to the medical school from which
they graduated. The majority of doctors registered under the MMC to date are
graduates from India, followed by Pakistan and China (Figure 7). A total of 212
expatriate health professionals were recruited in 2012 and 222 in 2013
(excluding December).
Figure 7. Total number of medical graduates registered under MMC (up
to June 2013) (Data source: MMC)

40
In-country training of health professionals
The FHS is the only public institution for training of health professionals in the
country. It has its main campus in Male’, plus there are campuses in four other
locations around the country: GDh. Thinadhoo, HDh. Kulhudhuffushi, S.
Hithadhoo and Laamu. Peripheral campuses have great potential to improve the
attraction and retention of health professionals to atoll and island health
facilities. Theory-related training and the initial training on practical procedures
takes place within the premises of FHS. For clinical practice and fieldwork
students are sent to IGMH, regional hospitals and health centres.
The pre-service training programmes conducted by FHS are:
Advanced Certificate in Counselling (2 semesters)
Advanced Certificate in Nursing (2 semesters)
Advanced Certificate in Pharmacy (2 semesters)
Advanced Certificate in Primary Health Care (3 semesters)
Bachelor of Primary Health Care (8 semesters)
Bachelor of Nursing (8 semesters)
Diploma in Medical Laboratory Technology (4 semesters)
Diploma in Nursing (5 semesters)
Diploma in Pharmacy (4 semesters)
Diploma in Counselling (4 semesters)
Certificate in Social Services (1 semester)

41
Advanced Diploma in Critical Care Nursing (6 semesters)
Advance Diploma in Midwifery (6 semesters)
MSc in Nursing (4 semesters)
MSc in Public Health (4 semesters), starting from January 2014
New courses planned by the FHS include a BSc in Medical Laboratory
Technology as well as an Advanced Diploma in Physiotherapy. Table 14 shows
the number of students enrolled and graduated from the different courses
offered by FHS.
In the past decade, 4947 students have enrolled in training courses at FHS with
an output of 1836 health professionals graduated in the same period. Enrolment
and graduation capacity has gradually increased in key health professions, such
as nursing and laboratory technology. To carry out this considerable workload in
the training of health professionals for the country, FHS has several strengths
including purpose-built infrastructure, flexible articulation between training
programmes, availability of a well-equipped state-of-the-art clinical skills
laboratory and, most importantly, very dedicated staff working under
constraints.
Curricula for the courses offered are coordinated by the Curriculum Committee
at FHS and developed by FHS staff in consultation with professional bodies,
such as Maldives Nursing Council and the service sector. Draft curricula have to
be approved by the professional bodies and then submitted to the Academic
Board of the Maldives National University. The Committee comprises
representatives from the MOHG, IGMH, FHS, and private health sector.

42
Table 14. Number of students enrolled and graduated in different courses offered by FHS
(Source: FHS 2013)
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
TO
TA
L
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
TO
TA
L
Advanced Certificate in Counselling 2 semesters 17 23 24 19 22 11 22 19 22 179 11 11 10 16 8 11 - 11 9 87
Advanced Certificate in Family Health (disrupted in 2009) 2 semesters 21 14 21 42 17 1 - - - 116 0 14 23 15 - - - - 52
Advanced Certificate in Midwifery (disrupted in 2006)1 semester (full) or
2 semesters (part)18 16 - - - - - - 34 0 12 - - - - - - 12
Advanced Certificate in Nursing 2 semesters 83 58 41 38 93 151 77 123 68 72 804 83 48 41 34 - 66 64 59 25 47 467
Advanced Certificate in Pharmacy 2 semesters 19 15 23 10 16 10 28 31 76 228 19 13 23 15 7 4 - 9 9 32 131
Advanced Certificate in Primary Health Care 3 semesters 26 36 28 29 57 86 46 51 39 40 438 0 23 20 12 14 26 22 16 - 13 146
Advanced Certificate in Social Services Work (being adapted) 2 semesters 0 35 18 14 - - 67 0 27 - 15 - - 42
Advanced Certificate in Traditional and Complementary Medicine (disrupted) 2 semesters 15 11 - - - - - - 26 8 11 - - - - - - 19
Bachelor of Health Sciences in Health Services Management (disrupted) 4 semesters - 38 15 1 - - 54 - - 16 2 - - 18
Bachelor of Nursing - Conversion (phased out) 7 14 1 14 12 12 20 80 7 13 0 12 - - 32
Bachelor of Primary Health Care 8 semesters - - - - - 41 41 - - - - - - 0
Certificate III in Pharmacy (disrupted) - - 14 - - - 14 - - 12 13 - - 25
Certificate III in Social Services Work 1 semester 20 1 0 - - 22 43 16 0 - 4 - 14 34
Diploma in Critical Care Nursing (upgraded to Adv. Diploma) 10 - - - - - 10 - - - - - - 0
Diploma in Medical Laboratory Technology 4 semesters 6 31 29 49 48 50 54 71 65 73 476 0 19 14 7 11 12 12 7 9 16 107
Diploma in Midwifery (upgraded to Adv. diploma) 8 15 0 41 9 25 34 27 159 5 15 0 15 8 - 10 20 73
Diploma in Nursing 6 semesters 79 38 74 84 120 148 135 194 169 258 1299 0 0 24 15 22 23 55 23 42 67 271
Diploma in Nursing - Conversion (phased out) 23 19 7 29 13 32 62 37 110 332 0 16 7 10 11 2 26 1 14 87
Diploma in Pharmacy 4 semesters 12 0 17 5 - - 12 46 10 - - 5 - - - 15
Diploma in Primary Health Care 5 semesters 37 25 35 32 29 25 20 35 31 49 318 0 0 13 20 22 30 41 7 24 49 206
Diploma in Primary Health Care - Conversion I (phased out) 1 semester 6 4 9 11 16 4 9 8 27 94 6 4 - - - - - - 10
Diploma in Primary Health Care - Conversion III (phased out) 2 semesters 5 0 28 27 2 2 25 89 2 - - - - - - 2
MSc Nursing - - - - - - 0 - - - - - - 0
MSc Public Health - - - - - - 0 - - - - - - 0
COURSES Duration
Enrolled last 13 years Graduated last 13 years
43
Challenges faced by the FHS include the availability of clinical training facilities,
faculty development and infrastructure facilities. Currently, the FHS has to
depend on IGMH (275 beds) and regional hospitals (30–50 beds in 6 hospitals)
to provide clinical skills training. However, these facilities are inadequate to
cater for the training requirements of all the courses conducted at FHS. Already
the facilities are overloaded and cannot accommodate more than 5–6 students
in each ward during a shift. In addition, some of the procedures are not
available to students during their clinical rotation period, which is a matter of
particular concern in the area of midwifery. For this reason, internships are
often arranged overseas.
There are only 40 full-time academics available at FHS, resulting in a teacher to
student ratio of 1:20 with only three teachers in the senior lecturer category.
Part-time teachers and visiting lecturers share a considerable proportion of the
teaching load. There is a need for training of teachers in clinical supervision,
some specialty areas such as diagnosis and treatment, pharmacology, health
promotion, health service management, counselling skills and different areas of
medical laboratory techniques.
Currently, there is no regular staff development programme at FHS. However,
some faculty get upgraded by pursuing their own postgraduate education
through other means (currently there are three staff with postgraduate
qualifications in medical/health professions education)
Research activity is very limited at FHS, which has important connotations for
academic excellence and also on the availability of local evidence to support
decision-making in the health sector. It is expected that, with the recent launch
of new masters-level courses, research activity will increase considerably.

44
Collaboration between the FHS and MOHG is an important area for
improvement. Introduction of new courses at FHS needs to be linked with the
human resource requirements of the health sector. The link between production
of health professionals at FHS and the needs defined by the dynamics of the
health labour market requires strengthening.
Training for general medical doctors
All Maldivian doctors are trained abroad. Thirty four students have been sent for
training in the last 6 years, with support from the MOHG and international
partners (see Table 16). The Department of Higher Education provides soft
loans for students willing to pursue their MBBS abroad. In 2012, 95 applications
were accepted for funding. The places currently available are at medical schools
in Nepal and Bangladesh. The official figure for students who are self-funded is
not available, but it is estimated that over 100 self-funded medical students are
currently undergoing medical training overseas. Due to problems in enforcing
bonding mechanisms and the lack of information in this regard, it is difficult to
precisely calculate educational outputs. However, the number of registrations
with MMC, which is a good proxy with no great significance as an educational
indicator but useful for labour market analysis, shows a sharp increase in
medical education outputs. The number of Maldivian MBBS graduates registered
was 9 in 2011, 23 in 2012 and 46 in 2013.
Maldives National University and several international organizations have
expressed interest in establishing a medical school in Maldives. In 2013, WHO
supported the development of standards for medical education,16 proposing two
basic models that could be considered: either a government initiative linked to a
centre of excellence abroad, or through direct foreign investment. However,
there are several challenges to establishing a medical school, including the lack
of faculty (around 75 faculty staff would be required as per WHO assessment,
but currently there are no trained medical teachers in Maldives), lack of

45
infrastructure, issues regarding availability of clinical material and case mix
(IGMH: 275 beds) and an estimated cost of approximately US$ 12 million. A
medical school entirely owned, technically and financially operated and
supported by Maldives alone, is not viable at this time and hence will not be
considered further.
Postgraduate training of health professionals
The FHS is the main institution providing postgraduate and post-basic training
programmes for health professionals in the country. FHS offers postgraduate
education in midwifery, critical care, family health, pharmacy, social work and
traditional and complementary medicine. New courses planned by FHS include a
master’s degree programme in nursing and more recently, a master’s degree
programme in public health in collaboration with the University of Sydney,
Australia.
The MOHG provides scholarships for health professionals to obtain overseas
postgraduate qualifications. Table 15 shows the number and expected year of
return for postgraduate trainees (other than medical) sent for overseas training
by the MOHG.
Table 15. Expected year of return for postgraduate trainees (other than medical) sent for training overseas by the MOHG (Source MOHG)
Course Level 2013 2014 2015 2016 2017
Food Science Masters 1 - - - -
Human Science (Sociology) Degree 1 - - - -
Bachelor of Science Degree - 1 - - -
Psychology (Hons) Degree - 1 - - -
Biomedical Engineering Degree - - 2 2 -
Economics (Hons) Degree - - 1 - -
46
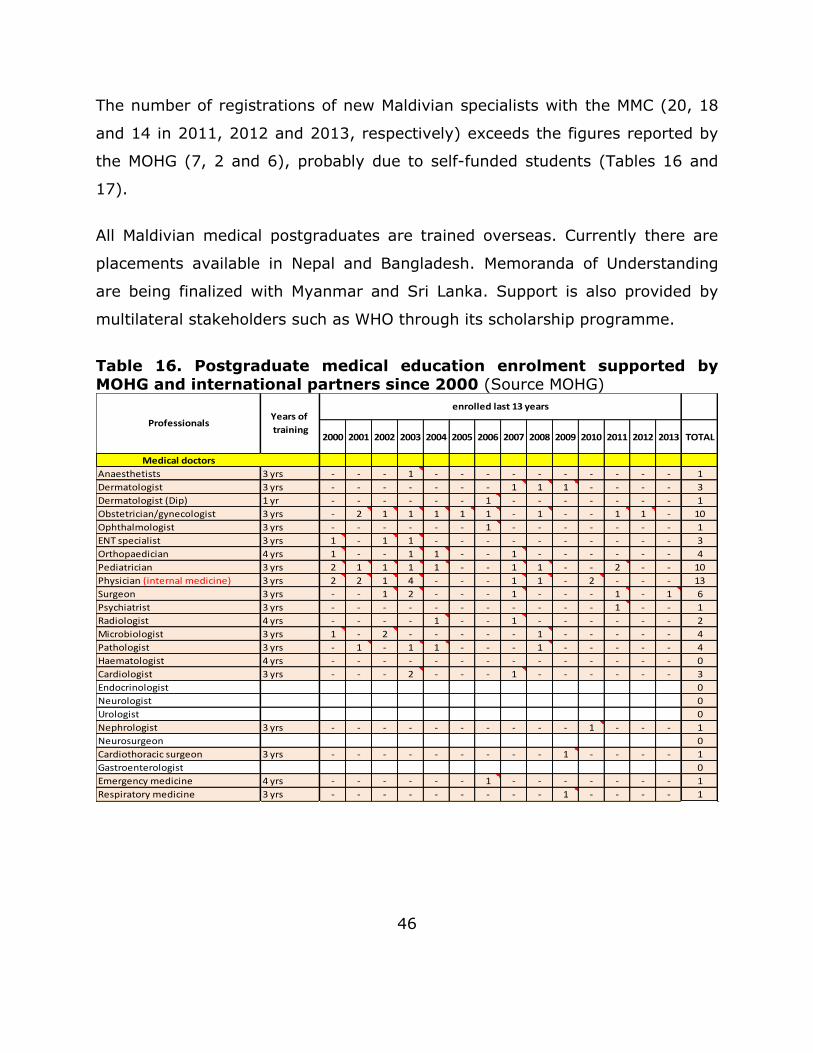
The number of registrations of new Maldivian specialists with the MMC (20, 18
and 14 in 2011, 2012 and 2013, respectively) exceeds the figures reported by
the MOHG (7, 2 and 6), probably due to self-funded students (Tables 16 and
17).
All Maldivian medical postgraduates are trained overseas. Currently there are
placements available in Nepal and Bangladesh. Memoranda of Understanding
are being finalized with Myanmar and Sri Lanka. Support is also provided by
multilateral stakeholders such as WHO through its scholarship programme.
Table 16. Postgraduate medical education enrolment supported by MOHG and international partners since 2000 (Source MOHG)
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 TOTAL
Medical doctors
Anaesthetists 3 yrs - - - 1 - - - - - - - - - - 1
Dermatologist 3 yrs - - - - - - - 1 1 1 - - - - 3
Dermatologist (Dip) 1 yr - - - - - - 1 - - - - - - - 1
Obstetrician/gynecologist 3 yrs - 2 1 1 1 1 1 - 1 - - 1 1 - 10
Ophthalmologist 3 yrs - - - - - - 1 - - - - - - - 1
ENT specialist 3 yrs 1 - 1 1 - - - - - - - - - - 3
Orthopaedician 4 yrs 1 - - 1 1 - - 1 - - - - - - 4
Pediatrician 3 yrs 2 1 1 1 1 - - 1 1 - - 2 - - 10
Physician (internal medicine) 3 yrs 2 2 1 4 - - - 1 1 - 2 - - - 13
Surgeon 3 yrs - - 1 2 - - - 1 - - - 1 - 1 6
Psychiatrist 3 yrs - - - - - - - - - - - 1 - - 1
Radiologist 4 yrs - - - - 1 - - 1 - - - - - - 2
Microbiologist 3 yrs 1 - 2 - - - - - 1 - - - - - 4
Pathologist 3 yrs - 1 - 1 1 - - - 1 - - - - - 4
Haematologist 4 yrs - - - - - - - - - - - - - - 0
Cardiologist 3 yrs - - - 2 - - - 1 - - - - - - 3
Endocrinologist 0
Neurologist 0
Urologist 0
Nephrologist 3 yrs - - - - - - - - - - 1 - - - 1
Neurosurgeon 0
Cardiothoracic surgeon 3 yrs - - - - - - - - - 1 - - - - 1
Gastroenterologist 0
Emergency medicine 4 yrs - - - - - - 1 - - - - - - - 1
Respiratory medicine 3 yrs - - - - - - - - - 1 - - - - 1
ProfessionalsYears of
training
enrolled last 13 years

47
Table 17. Postgraduate medical students graduated since 2000 (Source MOHG)
Continuous professional development
Continuous professional development (CPD) programmes are designed to
support workers to achieve the competencies required for optimal job
performance. A comprehensive approach towards CPD should be based on
country-specific health needs. The ultimate goals of the programme are to
reassure patients and the public that health professionals remain competent,
confident and compassionate throughout their career and to improve patients’
care, outcomes and satisfaction by setting standards for good practice.18 CPD
programmes also have important connotations for the motivation of health
workers.
TOTAL 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 TOTAL
Medical doctors
Anaesthetists 1 1 - - - - - - - 1
Dermatologist 3 - - - - 1 1 - 1 3
Dermatologist (Dip) 1 - - - - - - - - 0
Obstetrician/gynecologist 10 1 1 - 1 - - - 1 4
Ophthalmologist 1 - - - 1 - - - - 1
ENT specialist 3 - - - - - - - - 0
Orthopaedician 4 - 2 - - - 1 - - 3
Pediatrician 10 - - 1 3 1 - 1 - - - - 2 - - 8
Physician (internal medicine) 13 - - - 2 2 1 1 - - - 1 - - 2 9
Surgeon 6 - 1 1 - - 1 1 - - - 1 - - - 5
Psychiatrist 1 - 1 - - - - - - - - - - - - 1
Radiologist 2 - - - - - - - - 1 - - 1 - - 2
Microbiologist 4 - - - 1 - 2 - - 1 - - - 1 - 5
Pathologist 4 - - - - - - 1 1 - - - 1 - - 3
Haematologist 0 - 2 - - - - - - - - - - - - 2
Cardiologist 3 - - - - - - - - - - - 1 - 1 2
Endocrinologist 0 0
Neurologist 0 0
Urologist 0 0
Nephrologist 1 - - - - - - - - - - - - - - 0
Neurosurgeon 0 0
Cardiothoracic surgeon 1 - - - - - - - - - - - - 1 - 1
Gastroenterologist 0 0
Emergency medicine 1 - - - - - - - - - - 1 - - - 1
Respiratory medicine 1 - - - - - - - - - - - - - 1 1
Graduated last 13 years
Professionals

48
CPD in Maldives is neither systematic nor planned. Local workshops and
seminars are generally conducted within the MOHG and IGMH on an ad hoc
basis. The FHS also conducts in-service training workshops and seminars, and
invites nominations from the MOHG and IGMH. MOHG/IGMH personnel may be
funded by the MOHG or nominated for funding by other agencies, for
participation in short-term training-related activities out-of-country.
Opportunities for CPD are further limited due to the scattered nature of the
islands, together with the limited regular transport links between them. As a
result, in smaller hospitals and health centres on remote islands, health workers
remain professionally isolated and have less access for further study or career
advancement. Given this fact, distance and online learning could be considered
as a feasible option for delivery of CPD.19
HRH management systems
Recruitment and bonding
The MOHG is in charge of recruiting doctors, nurses and other cadres for each of
its facilities.
There are no official staffing standards defined at the moment. After the HRH
decentralization of 2009–2011, different corporations used different standards
to staff their health facilities. The CSC and MOHG are currently in the process of
addressing this issue. All staff records have been now transferred to the CSC
database. The next step should include a definition of staffing standards by the
MOHG and approval from the CSC.

49
For the purpose of defining HRH requirements in this strategy, positions
officially approved for each health facility by the CSC have been accepted as the
staffing norms (see Annex 3).
According to the bonding system currently in place, doctors or other
professionals who obtained financial support from the Government are bound to
return and work in the public sector for a minimum of 10 years. However,
implementation of this policy is ineffective. This problem is not restricted to the
health sector, but affects most areas of the Government where education
abroad is required.
The immediate consequence of this problem is human resource losses to the
system, with an increasing number of bonded health professionals – particularly
doctors – leaving the country, as indicated by the increasing number of requests
to the MMC for certificates of good standing. Professionals either repay the bond
or simply leave without paying, since there is no effective legal mechanism to
manage the breach of bonding contracts. Some cases have been sent to the
Prosecutor General’s Office but there has not been any prosecution engaged so
far.
Only a small number of doctors opt to work in the islands. In the absence of an
effective bonding system or other legal obligation, added to an ineffective
incentive system, the attraction of doctors to work in the islands even for a
short time period is very limited.
Bonding for nurses was implemented in the past through government
scholarships. Nurses with an island background were returning to work in their
home islands after graduation. However, since 2012 when the FHS became
independent from the MOHG, the students have had to pay 13% of the tuition
fees themselves with the Government still subsidising the rest (87%), but

50
bonding contracts were discontinued. As for doctors, most nurses choose to
work in Male’ instead of going to the islands.
Expatriates are recruited on a 1-year contract with a 3-month probation period.
After the first year, they have a performance assessment after which (if passed)
they are renewed on yearly basis. Performance assessment is undertaken by
medical managers at atoll facilities. If any problem is found during the
assessment, doctors are sent to the Health Service Division at MOHG central
level for further assessment. Problems identified are often not related to clinical
standards, but more to issues related to their adaptation to the new
environment. Sometimes problems are due to conflicting personal relations, in
which case redeployment to another location can often solve the issue. When
problems identified are related to the quality of care provided, cases are
referred to the MMC for further technical assessment and action.
There are some issues concerning recruitment and deployment of expatriate
professionals. These include financial and legal matters between private
recruitment agencies and the MOHG; issues related to immigration, such as
work permit cancellations; delayed payments; and, withholding of identification
papers of the recruited expatriate professionals. The MOHG is currently
changing its policy and discontinuing the use of recruitment agencies. Instead,
the department of international recruitment will get in touch with professionals
directly, either via word-of-mouth between colleagues or through other
institutions. Some of the agencies previously working for the MOHG are also
facilitating contact. International recruitment is done on a discretionary and
case-by-case basis. No batch recruitment is currently being undertaken.
Currently, there are no restrictions regarding from which medical school
applicants graduated or quality assurance mechanisms other than the
administrative requirements established by the MMC. The MMC plans to
51
introduce a licensing examination in 2014. At present, foreign applicants are
only requested to provide documentation, including proof of graduation and
completion of internship; testimonial from the dean of the medical school where
the professional graduated; postgraduate medical degree (for specialist
applications); certificate of good standing from their original medical council;
certificate of registration with any other licensing authority; English language
proficiency qualification (e.g. level 7 IELTS or TOEFL) and a letter of verification
of expertise from an employer (e.g. MOHG for applicants to public sector).
As mentioned above, retention of foreign doctors in the atolls and islands is
often poor, with 50% not staying beyond 1 or 2 years. Part of the problem is
unrealistic expectations of the applicants about the living conditions and health
service standards that they will find in Maldives. Poor information provided by
the employer prior to registration is probably the main reason behind this.
There are no induction programmes for new employees in place; however, the
MMC is currently developing guidelines and information packages to address
this problem. In the future, a better organized international recruitment process
will allow for more elaborated and interactive programmes to help professionals
manage their expectations in a more realistic way, adjust better to their new
environment and obtain a better general experience. This will most probably
have a positive impact on the retention of these professionals.
Remuneration
During decentralization, terms of employment with regard to work site, hours
and benefits (including remuneration) were different from one corporation to
another, even for the same categories of health professionals and for the same
jobs. This was especially the case for expatriate general medical doctors and
specialists.

52
With the full integration of the health workforce into the Civil Service, the basic
salary structure will be similar for all health care workers in the same
categories. Neighbouring countries have increased salaries for medical
professionals in the last few years, which has weakened the income differential
factor that was previously attracting professionals to Maldives. For doctors, a
cabinet decision was made that a new salary structure would be implemented
from January 2014. Nurses’ and other professionals’ salary scales will also be
revised soon. Given the great burden that the wage bill contributes to the
overall health budget (around 79%), the financial impact of relying so heavily
on an expatriate workforce will need to be evaluated and alternative options
may have to be found soon.
Currently, take-home pay is different between the local and expatriate health
workforce. Expatriates get a migration allowance, utility allowance, and food
allowance whereas local health workers do not, which may have a negative
impact in terms of job satisfaction for local professionals.
Although there is a small monetary allowance for doctors working in the islands,
it is not enough to constitute an effective incentive to attract these professionals
to work in peripheral facilities. There is a need to develop an effective incentive
policy, including both financial and non-financial rewards.
Income received in the public sector is slightly lower compared to the private
sector, but not significantly so. Since there are a limited number of private
services, income differential is unlikely to be the only factor draining doctors
and nurses from the public to the private sector. Other factors more related to
the work environment, health service management and leadership may also
contribute, such as equipment and medical supply availability, or consistent
supervision.

53
Non-financial incentives/working conditions
The health service system in the islands faces difficulties in balancing peoples’
expectations and the availability of health resources. While there are high
expectations regarding the quality of services provided, the availability of health
workforce, particularly paramedical and support staff, is often limited. Vacancy
rates among medical officers is relatively low (around 5%) compared to that for
nursing positions in hospitals (37%), or CHWs in health centres (86%). As
mentioned above, there are no effective non-monetary incentives in place to
attract and retain the health workforce in the islands.
Housing provision
Housing is provided at some regional hospitals for some health staff. In island
facilities, atoll hospitals or health centres, housing is not available. For those
who do not originate from the islands where they are working, an
accommodation allowance (MVR 1500) and a living allowance (MVR 1800) are
provided. However, these amounts do not cover the relatively high cost of life in
the islands.
Drugs and medical supply provision
During the decentralization period, procurement of drugs and medical
equipment was devolved to the corporations. Weak management capacity often
led to inefficiencies, with stock ruptures and weak supply occurring in some atoll
and island facilities. This affected patients’ care-seeking behaviour, increasing
self-referral to higher levels of the system, often to IGHM in Male’.
Furthermore, these problems have caused job dissatisfaction among the health
workforce on the islands.
Recently, the MOHG has decided to establish a central procurement unit which
is expected to contribute towards a more cost-effective, timely, and reliable

54
medical procurement system. This in turn should have an impact on access to,
and utilization of, health services by local populations and improve staff morale
and professional esteem.
Workplace environment
Health workers’ perceptions regarding working in the islands are mixed. It is
often reported that it is a relaxing experience with the benefits of good
teamwork. Some health workers have a good relationship with patients and
their families, and can provide a holistic approach to care. For those who are
interested in preventive care and health promotion, sometimes there are
opportunities to carry out research or specific projects (often funded by
international agencies) which help expand their professional experience.
However, working in the islands has several drawbacks. Isolation from family,
friends and professional groups are among the main issues. In some islands,
the population is small and most of the patients seen at health services suffer
from common diseases. This lack of exposure to challenging clinical conditions
can make working in the islands professionally unattractive. Cultural and
language barriers may also contribute to an uncomfortable working atmosphere.
Poor managerial support from central and regional levels and inadequate
orientation for new employees also add to the problems. Sometimes, the lack of
an effective grievance and complaints policy affects the safety of foreign
professionals, who are threatened by patients or their families when
expectations are not satisfied or unexpected outcomes occur.
Career development
Career advancement is better for professionals working in the secondary and
tertiary levels. After working for 3 years in hospitals, doctors are automatically
promoted to senior medical officer which, following specialization, can lead to
different grades of consultancy categories. Doctors working in primary health

55
care reach their professional ceiling after promotion to senior doctor, following 3
years of work.
Other health professionals, such as nurses and CHWs, have limited career
advancement possibilities. Despite nurses having had a well-structured career
path in the past, recent changes introduced with corporatization and then by
recentralization processes have created some regulatory loopholes that
currently do not support their professional advancement. Similarly, in the past,
CHWs’ career structure ranked from assistant CHW, CHW, to senior CHW (the
highest position). A new CSC policy defines career progression within each
subcategory, greatly limiting the professional career span and potential for
promotion. A committee has now been established at the CSC to revise career
structures for all cadres within the health services, which is expected to be
completed during 2014.
Family aspect
Family-related reasons often explain health workers’ unwillingness to work in
atoll and island health services. Job availability for spouses, education for
children and lack of services are reasons often given by health workers for not
taking up rural positions. Professionals with an island background are also often
attracted to live in Male’ and reject rural positions for similar reasons.
Migration from the islands to Male’ has greatly increased in the last decade.
Performance management
Performance appraisal was introduced by CSC in 2009 to improve the quality,
productivity and efficiency of health workers. Each individual sets their own
targets, and these are to be reviewed and assessed by supervisors annually.
However, the appraisal is not linked with any salary increase or career
promotion. The supervisors rarely use the appraisal results to score individuals

56
for the purpose of competition for a higher position. The general feeling is that
high and poor performers are treated equally.
Quality assurance
The quality assurance of health services is the responsibility of the Quality
Assurance and Improvement (QAI) section which is under the Health Service
Division. Its roles include development of standards and guidelines, health
facility inspections and service audits, management of service complaints,
services registration and quality improvement. Some clinical guidelines are
currently being developed to assist each health facility in quality improvement.
They are to be implemented at all health facilities when they have been
approved by the MOHG. Due to staff limitations within the QAI section, regular
inspections are mostly limited to private health facilities in Male’. For the same
reason, and due to transport limitations, there are no regular inspections of
island health facilities. A quality improvement plan for the islands was
developed during the decentralization period. The plan stated that all regional
hospitals should designate quality improvement officers to oversee, inspect and
ensure quality assurance for all health facilities in each region. However, the
plan was never rolled out.
As the majority of care providers are expatriates, trained from various medical/
nursing schools and exposed to health systems with different standards, the
quality of services is difficult to assure. At each hospital, the hospital manager
and a specialist doctor provide technical support to lower-level health facilities.
Four selected hospitals offer telemedicine consultations to lower-level health
facilities in 39 islands; however, the telemedicine programme has not yet been
fully implemented. Professional councils also play a role in assuring the
standards of practice of individual professionals. However, their role in
inspecting and auditing is limited, as there are shortages of staff in the councils.

57
Policies for referrals are in place. Health centres refer patients to atoll/regional
hospitals or IGMH depending on the severity of the case and the need for
specialised care. However, lack of gatekeeping at the lower levels of the system
has made these policies ineffective, leading to self-referral of patients (often to
IGMH in Male’) which greatly contributes to inefficiencies and misuse of
services.
The new Government is trying to address some of the quality assurance issues
presented above.
HRH information and evidence for decision-making
Timely and accurate HRH information is essential for planners, health-care
providers and managers to make decisions on HRH effectively. Despite data
about the health workforce being relatively available in Maldives, information is
not generated, managed and used appropriately. Fragmentation of the existing
Health Information and Research Section (HIRS) is partially a consequence of
the strong administrative orientation of the Human Resources Department (e.g.
data are generated exclusively for administrative purposes such as calculation
of overtime, payroll, etc. rather than for strategic workforce planning). Data are
often dispersed among different sections and institutions, and there is no
consolidated database that permits a comprehensive data analysis. The process
of decentralization had a strong negative impact on the HIRS, as much of the
information flow was disrupted when workforce management was devolved to
the corporations.
There is currently a new plan to develop a Maldives Integrated Health
Information System (MIHIS) by the HIRS, under the Policy and Planning
Division. The aim of the proposed MIHIS is to promote evidence-based decision-
making in the health sector to strengthen capacity on health information

58
production, use and management and to ensure an appropriate reporting
system. The MIHIS is a uniform information system which is intended to include
all individual, independent, public and private entities of the health sector, as
well as external authorities with service links to the health sector, through
developmental phases. The system is intended to serve both the operational
management of the health system as well as its strategic development. In a
first phase, the plan envisions to undertake a system requirements assessment,
to develop the required software for implementation in 21 hospitals between
July 2014 and December 2015. The cost of this first phase is around MVR 13
million; however, funding for the plan is not yet secured. Initially the system
will concentrate on individual information (e.g. health service activity,
morbidity, mortality, etc.) and it is not planned to include HRH information. In a
second phase, different specific modules including HIRS will be developed. In
order to bridge the existing gap in HRH information to allow for strategic
workforce decision-making, a transitory solution needs to be found.
Besides HRH data, health workforce evidence and knowledge are the main
contributors to appropriate decision-making. There is very limited health system
and services research undertaken in Maldives. Therefore, decisions are often
made ad hoc or based on anecdotal evidence.
The HIRS under the Policy and Planning Division has a mandate to support
research and production of evidence for policy-making. However, understaffing
and an unclear functional role of the Section in regard to research leave this
area relatively neglected. In 2013, a research agenda was developed through
an interactive process with all sections of the MOHG. However, there is no
research topic proposed for the area of HRH. The agenda is currently not being
implemented, mainly due to overall limited research capacity in the country and
lack of specific funding.
59
HRH leadership
Current HRH coordination mechanism and champions
The prime responsibility for the health workforce in Maldives lies with the
MOHG. However, coordination with other involved stakeholders such as the
CSC, Ministry of Education, professional councils and Ministry of Finance and
Treasury to address HRH issues at the national level is often weak. At the
MOHG, there is a Human Resource Development and Management Committee
(HRDMC) chaired by the Permanent Secretary and with representatives from all
departments and support divisions. The Secretariat, based in the Human
Resources Department, meets on weekly basis. Although the Committee is
mandated to carry on important functions, such as HRH policy development and
strategic planning or HRH management and development, the existing functions
are mostly limited to solving day-to-day issues. This adds to the problem
already identified at the Human Resources Department regarding the narrow
focus of their operations. The main constraints preventing the HRDMC from
being fully operational in the fields of HRH policy, planning and development are
the limited technical capacity of the Committee members, together with a lack
of technical assistance and lack of time.
Currently, a joint working committee from the MOHG and CSC has been
established to develop a new salary structure for the health workforce. This is
an ad hoc committee that has been set up by CSC to provide information to
define the salary structure. The committee comprises MOHG officials and
health-care providers from different cadres.
Coordination between the public health sector and training institutions was very
strong in the past when FHS was under the responsibility of the MOHG. Since
responsibility for the FHS was transferred to the Maldives National University,
interaction between both institutions has weakened with the MOHG being just a

60
member of the commission in charge of the student selection process. This
weak coordination has important connotations in terms of adjusting the
production of health workers to the needs of the public health system.
There are four professional councils under the MOHG: MMC, Maldives Nursing
Council, Maldives Board of Health Sciences and Maldives Board of Traditional
Medicines. The Secretariat of these councils lies in the Regulatory Boards and
Councils entity overseen by the Directorate General of Health Services. The
roles of each council are to regulate their respective health professionals
working in the country, regulate/approve new curriculum at the universities,
and register expatriates. Currently, only pharmacists are requested to sit a
licensing examination. However, all other professional councils plan to introduce
this measure soon. Although the roles of the professional councils are to
monitor and ensure the standard of practice of their respective health
professionals, currently they have some limitations in carrying out this task
mainly due to a lack of qualified staff and financial means.
HRH stewardship
All HRH management functions previously performed by the health service
corporations are now centrally coordinated by the MOHG. However, some of the
functions are still delegated to atoll level.
Excepting IGMH, all health managers in Maldives are non-clinical health
professionals. Most of them are from a public health background with long
experience of working in the health system. Most health managers are not
formally trained; they have learned management skills through their past
experience. Only a few of them have attended formal training courses. The
medical officers in charge are appointed to oversee and manage the clinical
work. The need to improve managerial skills in HRH is strongly perceived. It is

61
realized that effective management skills could contribute to improving
efficiency and quality within the health system.
A Bachelor of Health Sciences in Health Service Management used to be
provided by FHS, but it was discontinued after the introduction of the Maldives
National Qualifications Framework in 2009 and is currently being revised.
Although the Civil Service Training Institute provides courses in administration
and management, the curriculum is not specifically for health managers. There
are human resource management courses provided by private education
institutions, but none is specific to the health sector.
HRH partnerships
Maldives has a relatively long history of collaboration with international agencies
and foreign governments/entities in relation to HRH. The main HRH
collaborative issues are production and development. The lack of training
institutions for some key disciplines has forced Maldives to seek collaborations
with neighbouring countries. The need to recruit internationally has also
triggered some bilateral agreements. Multilateral international partners also
play a role in supporting HRH production and development, particularly for
postgraduate education and continuous professional development. Being a
middle-income country, Maldives is often not eligible for concessional loans.
However, the country is still receiving aid from various donors.
At country level, the main stakeholders within the health sector involved in HRH
(besides the MOHG) are FHS, MMC, Maldives Nursing Council, Maldives Board of
Health Sciences, and representatives of the private sector. The private sector
has expanded to play an important role in HRH. There are three private
hospitals, two of which are located in Male’, and some small clinics. The impact
of the private sector on the availability of HRH varies, depending on categories.
For specialists, the impact is more significant with 171 specialists in the public

62
sector and 24 in the private sector (14%), while the proportion of private-sector
general practitioners and nurses is low. Crucial stakeholders from other sectors
include the Ministry of Finance and Treasury, Ministry of Education, CSC and, to
some extent, local authorities.
Public and private partnership for HRH in Maldives is strong in the case of
pharmacists. Except for the pharmacy operated by the State Trading
Organization (a Government-shared private entity), all pharmacies in the
country are within the private sector. These private pharmacies have signed
Memoranda of Understanding to provide pharmacy services for a fixed number
of hours per day and to pay a rent for their premises. All 21 hospitals in the
country have similar organization for the delivery of pharmaceutical services.
Owing to the remote and small population in many islands, and the need to
ensure access to essential medicines and preventive health services, the
Government supports women’s or youth committees to establish community
pharmacies. However, the programme is implemented inconsistently.
There are some civil society-based initiatives contributing to service provision
for vulnerable populations most directly affected by shortage of HRH. For
example, the Aged Care Maldives (Manfaa Clinic) provides empowerment and
awareness programmes for the elderly and their caregivers, and the Care
Society conducts community-based programmes for persons with disabilities.
These partnerships, although having informal linkages with the MOHG, have
played an important role in increasing non-formal HRH to provide health
services in the remote or island areas, as well as enabling community
participation.

63
HRH financing
The health workforce absorbs a considerable share of the health budget, which
is generally consistent with the pattern of spending in developing countries. The
total spending on HRH was estimated at almost MVR 174 million in 2011
(National Health Accounts 2011). Total spending on the health workforce as a
percentage of the recurrent health budget is in the order of 79%, falling within
the normal 60–80% range for developing countries;10 however, it is relatively
higher than other countries in the region.
HRH financing in Maldives is resourced from tax revenues managed by the
Ministry of Finance and Treasury. Most staff salaries are paid centrally.
Nevertheless, financing recurrent health facility expenses, including payment of
salaries to some specific support cadres, is decentralized to the atolls and
sometimes to the islands.
HRH requirements
To provide services that are high quality, cost-effective and accessible to the
people, HRH availability needs to match with HRH requirements in terms of
numbers, skills and distribution.
The HRH requirement projections are calculated based on two scenarios.
Scenario 1: Achieving staffing standards.
Scenario 2: Reducing the number of expatriate health workers.
Given the high number of HRH required, the period planned for achieving these
scenarios goes beyond the period covered by this strategic plan. It greatly
depends, on the one hand, on the capacity of the Government to allocate
enough funds or to generate enough investment from the private sector and/or
64
international partners to support students to graduate in health
disciplines/educational programmes not available in the country; and, on the
other hand, on scaling up the existing capacity of the FHS to produce cadres
locally.
As previously stated, there are no official staffing standards approved in
Maldives at present. This analysis has used positions approved by the CSC for
each level of health service delivery as the standard (see Annex 4).
Lack of information about losses in each cadre (attrition) has made it impossible
to introduce this variable into the analysis. In order to balance this limitation,
rounding up of calculations has been applied.
Scenario 1: Achieving staffing standards (Tables 18 and 19)
This scenario aims at reducing vacancy rates and calculates the number of
health workers required to achieve current staffing standards in each specific
cadre. As mentioned above, vacancy rates are relatively high, particularly in
some key cadres. It is proposed that in order to fill vacancies, Maldivian
resources are produced either locally or abroad rather than recruiting
internationally, to reduce dependency on expatriates and increase workforce
sustainability in the long run.
In line with Government priorities for the orientation of the health system
towards primary health care, it is recommended to first concentrate on
producing those cadres that are most needed in peripheral facilities (island, atoll
and regional facilities) and to continue relying on expatriates for specialities that
are available only at the central level (IGMH). Maldivian doctors willing to go for
specialization should adjust their speciality choice to the needs of the country,
with financial support offered by the Government, moving exclusively to those
specialities that are most required. Priority should be given to internal medicine

65
specialists, surgeons, anaesthetists, obstetricians, paediatricians and
orthopaedic surgeons. Other priority cadres include nurses, midwives, CHWs,
laboratory technicians, radiographers and physiotherapists. Managers should
also be included as a top priority, as currently most senior and mid-level health
management positions are vacant with a potentially severe negative impact on
health service efficiency.
Due to a lack of information about cost and programmes for some of the
medical specialities, assumptions were made about the cost and duration of
training; however, for other cadres it was impossible to calculate costs.
The cost of achieving staffing standards (Table 18) for priority cadres by
training Maldivians is approximately MVR 350 million (US$ 22.5 million) and it
could be achieved in approximately 11 or 12 years (Table 19).

66
Table 18. Cost of training priority cadres to reach staffing standards (Source: MOHG)
#
Posts
NEEDS TO
REACH SS
TRAINING
LOCAL/
ABROAD
YEARS OF
TRAINING COST OF TRAINING (MVR)
TOTAL FUNDING REQUIRED
(MVR)
TOTAL FUNDING REQUIRED
Exchange Rate(US$) 15.42
4 Physician 15 A 3 799 877.19 11 998 157.82 778 090.65
5 Orthopaedic Surgeon 8 A 3 799 877.19 6 399 017.51 414 981.68
9 Radiology 1 A 3 799 877.19 799 877.19 51 872.71
14 Gynaecologist 21 A 3 799 877.19 16 797 420.95 1 089 326.91
15 Anaesthesiologist 18 A 3 799 877.19 14 397 789.39 933 708.78
16 Surgeon 15 A 3 799 877.19 11 998 157.82 778 090.65
17 Paediatrician 15 A 3 799 877.19 11 998 157.82 778 090.65
22 General Practitioner (Senior Medical
Officer/Medical Officer /Registrar) 32 A 6 1 630 541.64 52 177 332.48 3 383 744.00
23 Dentist 5 A 5 1 670 544.00 8 352 720.00 541 680.93
26 Radiographer 7 A 3 796 580.00 5 576 060.00 361 612.19
30 Physiotherapist 11 A 26 months 13 078.11 143 859.17 9 329.39
33 Laboratory Technician 45 A 26 months 13 337.55 600 189.80 38 922.81
37 Nurses 865 L 4 164 680.00 142 448 200.00 9 237 885.86
38 Nurse Midwife 141 L 3 146 226.33 20 617 913.00 1 337 089.04
41 Regional Health
Administrator/Director/Manager 19 L 4 25 876.00 491 644.00 31 883.53
42 Assistant Manager / Deputy Manager 13 L 3 16 006.00 208 078.00 13 494.03
44 Community Health Worker 221 L 4 198 382.67 43 842 569.33 2 843 227.58
TOTAL 348 847 144.28 22 623 031.40

67
Table 19. Proposed calendar to achieve staffing standards for key cadres
POST NEED
S
TIME
years
TRAINING RECRUITMENT
20
14
20
15
20
16
20
17
20
18
20
19
20
20
20
21
20
22
20
23
20
24
20
14
20
15
20
16
20
17
20
18
20
19
20
20
20
21
20
22
20
23
20
24
Physician 15 3 3 3 3 3 3
3 3 3 3 3
Orthopaedic
Surgeon 8 3 2 2 2 2
2 2 2 2
Radiology 1 3 1
1
Gynaecologist 21 3 3 3 3 3 3 3 3
3 3 3 3 3 3 3
Anaesthesiologist 18 3 3 3 3 3 3
3 3 3 3 3 3
Surgeon 15 3 3 3 3 3 3
3 3 3 3 3
Paediatrician 15 3 3 3 3 3 3
3 3 3 3 3
Medical Officer 32 6 8 8 8 8
8 8 8 8 8
Pharmacist 2 5 2
2
Radiographer 7 3 2 2 2 1
2 2 2 1
Physiotherapist 11 26 m 3 3 3 2
Laboratory
Technician 45 26 m 8 8 8 8 8 5
Nurses 865 4 110 110 110 110 110 110 110 110
110 110 110 110 110 110 110
Nurse Midwife 141 3 25 25 25 25 25 25
25 25 25 25 25 25 25
Senior Manager 19 4 5 5 5 4
5 5 5 4
Assistant Mgr. 13 3 5 5 3
5 5 3
CHW 221 4 35 35 35 35 35 35 21
35 35 35 35 35 35 21
Red cells: categories for which calculations could not be made due to lack of information.

68
Scenario 2: Reducing the expatriate health workforce (Tables 23 and 24)
Maldives, as most health systems in the world, needs to rely on expatriates to
complete its health workforce. However, current levels of international
recruitment are proving unaffordable. As described earlier, there are other
problems attached to international recruitment than just the financial element.
This scenario envisions a progressive reduction of the expatriate workforce and
their replacement with Maldivians. Emphasis should be put on those cadres for
which local education is available, such as nurses, midwives and laboratory
technicians, by scaling up their production. However, increasing production will
not solve the problem by itself. Other measures such as improvements in
attraction and retention, strengthening management and leadership, or
improving working environment will need to be in place to ensure that good
quality Maldivian health workers remain in the public health system working
productively and efficiently.
As mentioned in the previous scenario, in order to be consistent with the
primary health care orientation of the Maldivian public health system, cadres
working at the primary and secondary levels (e.g. health centres and
atoll/regional hospitals) should be given priority.
The total cost of training Maldivians to fully replace the existing expatriate
health workforce (health professionals only) would be around MVR 662 million
(Tables 20 and 21). The timing of replacement will largely depend on the
funding available for training local resources.
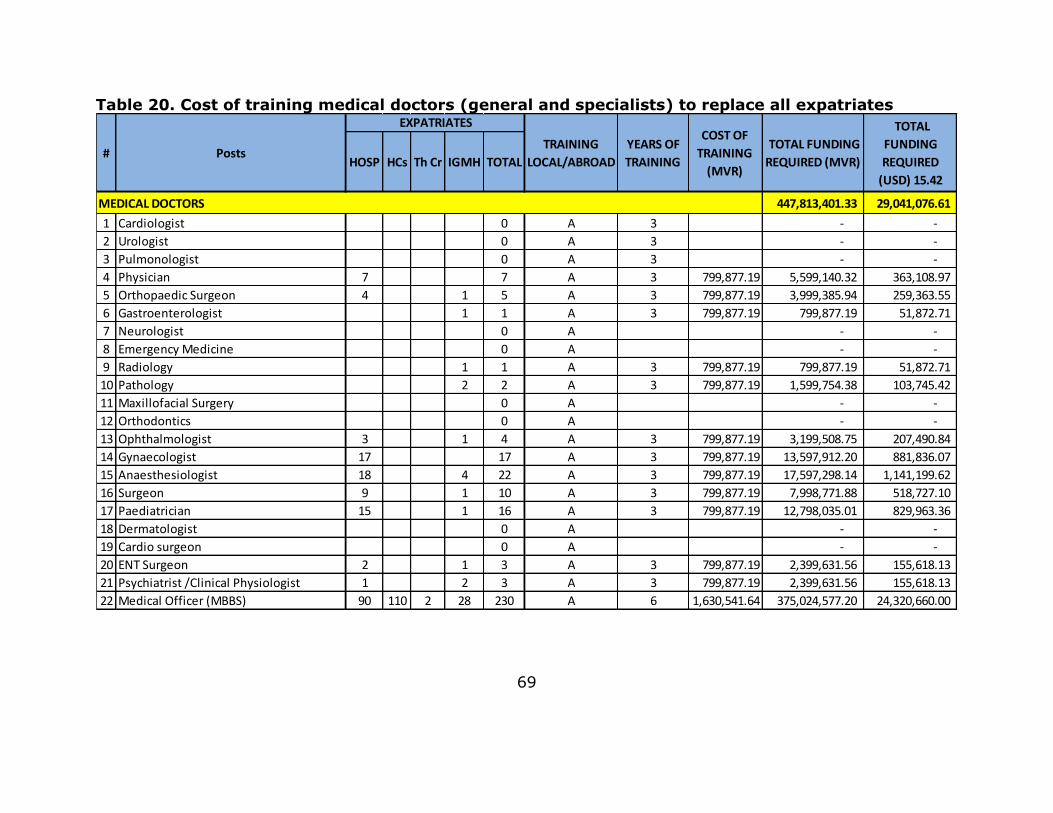
69
Table 20. Cost of training medical doctors (general and specialists) to replace all expatriates
HOSP HCs Th Cr IGMH TOTAL
MEDICAL DOCTORS 447,813,401.33 29,041,076.61
1 Cardiologist 0 A 3 - -
2 Urologist 0 A 3 - -
3 Pulmonologist 0 A 3 - -
4 Physician 7 7 A 3 799,877.19 5,599,140.32 363,108.97
5 Orthopaedic Surgeon 4 1 5 A 3 799,877.19 3,999,385.94 259,363.55
6 Gastroenterologist 1 1 A 3 799,877.19 799,877.19 51,872.71
7 Neurologist 0 A - -
8 Emergency Medicine 0 A - -
9 Radiology 1 1 A 3 799,877.19 799,877.19 51,872.71
10 Pathology 2 2 A 3 799,877.19 1,599,754.38 103,745.42
11 Maxillofacial Surgery 0 A - -
12 Orthodontics 0 A - -
13 Ophthalmologist 3 1 4 A 3 799,877.19 3,199,508.75 207,490.84
14 Gynaecologist 17 17 A 3 799,877.19 13,597,912.20 881,836.07
15 Anaesthesiologist 18 4 22 A 3 799,877.19 17,597,298.14 1,141,199.62
16 Surgeon 9 1 10 A 3 799,877.19 7,998,771.88 518,727.10
17 Paediatrician 15 1 16 A 3 799,877.19 12,798,035.01 829,963.36
18 Dermatologist 0 A - -
19 Cardio surgeon 0 A - -
20 ENT Surgeon 2 1 3 A 3 799,877.19 2,399,631.56 155,618.13
21 Psychiatrist /Clinical Physiologist 1 2 3 A 3 799,877.19 2,399,631.56 155,618.13
22 Medical Officer (MBBS) 90 110 2 28 230 A 6 1,630,541.64 375,024,577.20 24,320,660.00
#
COST OF
TRAINING
(MVR)
TOTAL FUNDING
REQUIRED (MVR)
TOTAL
FUNDING
REQUIRED
(USD) 15.42
EXPATRIATES
YEARS OF
TRAINING
TRAINING
LOCAL/ABROADPosts
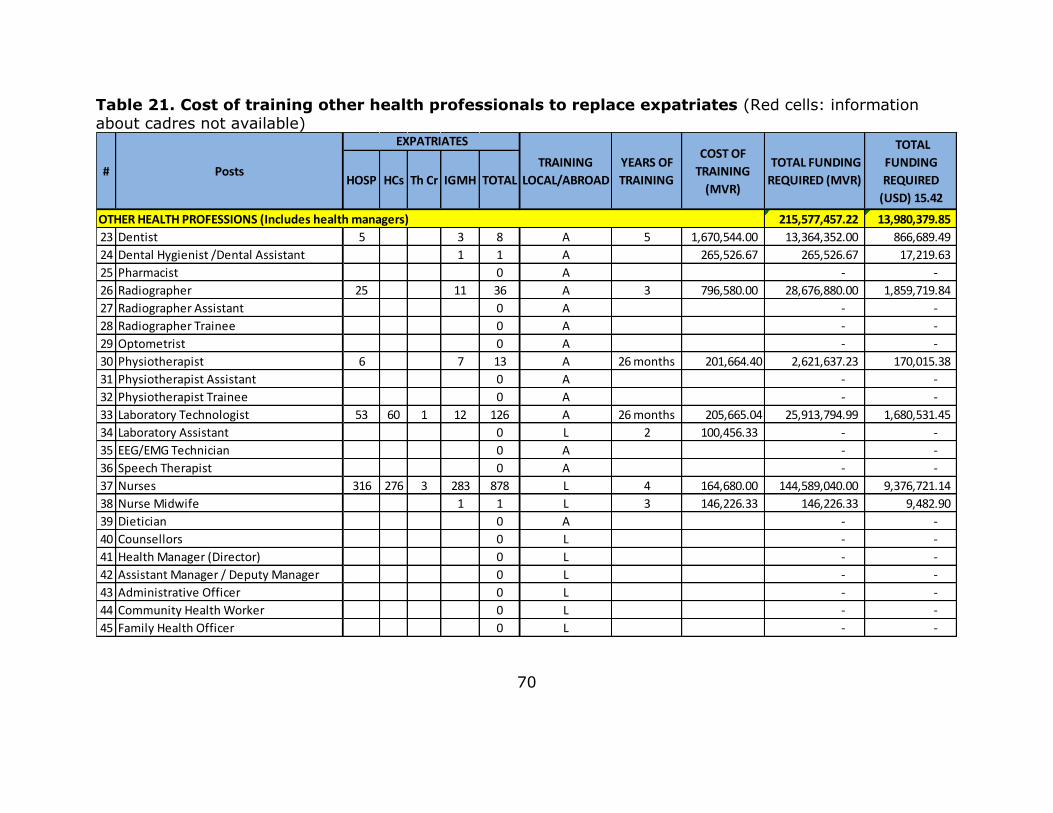
70
Table 21. Cost of training other health professionals to replace expatriates (Red cells: information about cadres not available)
HOSP HCs Th Cr IGMH TOTAL
OTHER HEALTH PROFESSIONS (Includes health managers) 215,577,457.22 13,980,379.85
23 Dentist 5 3 8 A 5 1,670,544.00 13,364,352.00 866,689.49
24 Dental Hygienist /Dental Assistant 1 1 A 265,526.67 265,526.67 17,219.63
25 Pharmacist 0 A - -
26 Radiographer 25 11 36 A 3 796,580.00 28,676,880.00 1,859,719.84
27 Radiographer Assistant 0 A - -
28 Radiographer Trainee 0 A - -
29 Optometrist 0 A - -
30 Physiotherapist 6 7 13 A 26 months 201,664.40 2,621,637.23 170,015.38
31 Physiotherapist Assistant 0 A - -
32 Physiotherapist Trainee 0 A - -
33 Laboratory Technologist 53 60 1 12 126 A 26 months 205,665.04 25,913,794.99 1,680,531.45
34 Laboratory Assistant 0 L 2 100,456.33 - -
35 EEG/EMG Technician 0 A - -
36 Speech Therapist 0 A - -
37 Nurses 316 276 3 283 878 L 4 164,680.00 144,589,040.00 9,376,721.14
38 Nurse Midwife 1 1 L 3 146,226.33 146,226.33 9,482.90
39 Dietician 0 A - -
40 Counsellors 0 L - -
41 Health Manager (Director) 0 L - -
42 Assistant Manager / Deputy Manager 0 L - -
43 Administrative Officer 0 L - -
44 Community Health Worker 0 L - -
45 Family Health Officer 0 L - -
#
COST OF
TRAINING
(MVR)
TOTAL FUNDING
REQUIRED (MVR)
TOTAL
FUNDING
REQUIRED
(USD) 15.42
EXPATRIATES
YEARS OF
TRAINING
TRAINING
LOCAL/ABROADPosts

71
The HRH situation in Maldives is determined by a complex interplay of factors
including the effects of globalization and changes in the epidemiological,
socioeconomic, cultural and political situation, as well as internal factors
governing HRH such as health financing, policy, management and training. The
HRH challenges in relation to the shortage of local health professionals,
inequitable distribution, high turnover rate of health staff in the islands, and
inappropriate skill mix and competencies, need to be addressed. This situation
analysis found the following contributory factors.
1. Inadequacy of HRH management policies and support to provide equitable
distribution with an appropriate skill mix, or attract and retain HRH in the
islands.
2. Lack of policies and regulatory frameworks for quality assurance towards an
enhanced health workforce performance and productivity, and absence of
HRH database and evidence-based information to advocate policies.
3. Pre-service and in-service training outputs are not aligned with the needs of
the health service system in terms of number and quality.
4. Limitations of leadership capacities to adequately perform the essential HRH
management and monitoring functions.
5. Lack of a multi-stakeholder coordination mechanism for policy dialogue,
consultation, planning, implementation and monitoring of HRH outcomes.
6. Lack of national policy and plan to enhance the HRH resources from the
national budget as well as other resources.

72
SECTION C: Health workforce strategic plan
Vision
A competent and sustainable health workforce in the Maldives health system,
based on primary health care to deliver quality health services to the people.
Mission
To produce, deploy and retain a well-trained, competent, gender-balanced,
well-supported and motivated health workforce in sufficient quantity with the
appropriate skill mix. To gradually increase the number of local health
professionals to ensure delivery of equitable, cost-effective, efficient, good
quality, and ethically and culturally acceptable health services to all inhabitants
of Maldives.
In line with the national health policy recognizing the right of the population to
quality health care, provided by a pool of qualified and competent health
workers, with a right mix in accordance to the local health needs.
Prime attention is given to national health and development priorities, within
the regional and global health agenda.
Guiding principles
In developing the HRH Strategic Plan 2014–2018, due consideration has been
given to the following guiding principles.
Availability: Increasing opportunities and openings for needs-based pre-
service training for sufficient quality of skilled domestic health workforce with a
required skill mix.
73
Accessibility and equity: Ensuring access to health services for all, through
the equitable distribution of competent, supported and well-motivated HRH at
all levels of the health care system.
Acceptability and gender equality: Culturally-appropriate health services
promoting related strategies for ethics, respect for sociocultural values and
equal opportunities for both women and men.
Quality: Adequate quality standards in training and services to deliver
acceptable health care to the population, with high professional standards in
accordance with global health developments.
Feasibility: Interventions to be achievable within the expected resource
envelope and integrated within the overall health sector planning and
development framework, taking into account other external factors and support
processes.
Cost-effectiveness: The selected strategies and interventions should be the
best value for money.
Sustainability: Developing investment and interventions that ultimately lead
towards a sustainable and indigenous health workforce.
Health systems approach: Strategies and interventions to be mainstreamed
and integrated with other components of the health system, based on a primary
health care approach.
Responsive to current and projected health needs: Guided by the evidence
and through rigorous scientific situation analysis, strategies should respond to
current and projected health needs.

74
Accountability and transparency: Accountability and transparency to be
maintained throughout the implementation of the plan through the ownership
and leadership of the national Government.
National stewardship: National capacity, particularly the HRH Department of
the MOHG, should play a central role as a coordinating entity with enhanced
capacity for management and leadership.
Partnerships and collaboration: Promoting a policy dialogue and consultative
process for strong partnerships with developmental partners, the private sector,
professional associations and other related stakeholders to strengthen HRH
planning, financing, implementation and monitoring.
Public and private partnership: The potential of the private sector to be fully
mobilized towards health inputs, with a focus on HRH development.

75
Strategies and interventions
Strategic line 1: Policy, leadership and management systems
Strategic
objective 1
Strengthening the systems and structures to effectively
manage and support HRH; improving policies, regulatory
frameworks and institutions, and fostering leadership
capacities to adequately perform the essential HRH
management and monitoring functions.
Rationale
The main challenge for HRH in the Maldives health system is
the difficulty in attracting and retaining HRH in the islands,
particularly doctors, nurses and qualified health managers.
Strengthening the health workforce is recognized as a priority
in the Health Master Plan. Previous HRH policies and plans
were not fully implemented. Several policy issues related to
HRH urgently need to be addressed.
Leadership and managerial skills are deficient at all levels of
the system, either due to lack of appropriate staff or limitation
in capacity of existing managers.
Expected
outcome
The national health system efficiently managing and
supporting the health workforce through evidence-based
policies and practices, leading it towards the agreed vision.
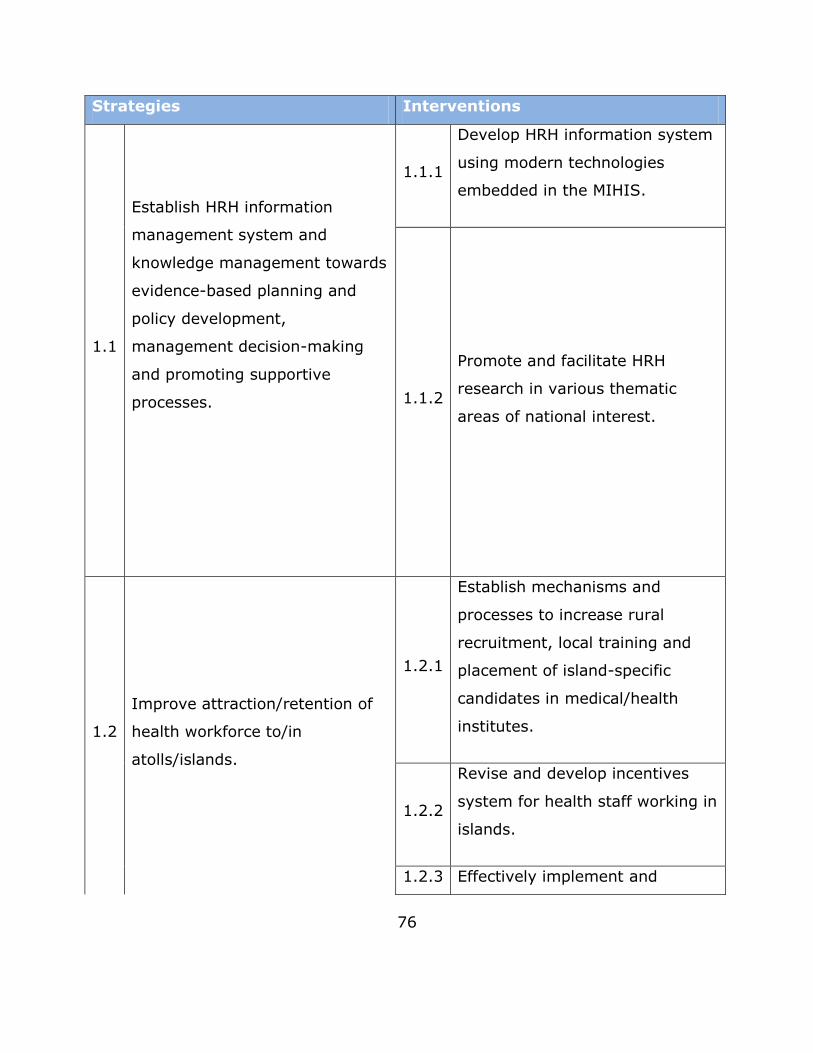
76
Strategies Interventions
1.1
Establish HRH information
management system and
knowledge management towards
evidence-based planning and
policy development,
management decision-making
and promoting supportive
processes.
1.1.1
Develop HRH information system
using modern technologies
embedded in the MIHIS.
1.1.2
Promote and facilitate HRH
research in various thematic
areas of national interest.
1.2
Improve attraction/retention of
health workforce to/in
atolls/islands.
1.2.1
Establish mechanisms and
processes to increase rural
recruitment, local training and
placement of island-specific
candidates in medical/health
institutes.
1.2.2
Revise and develop incentives
system for health staff working in
islands.
1.2.3 Effectively implement and
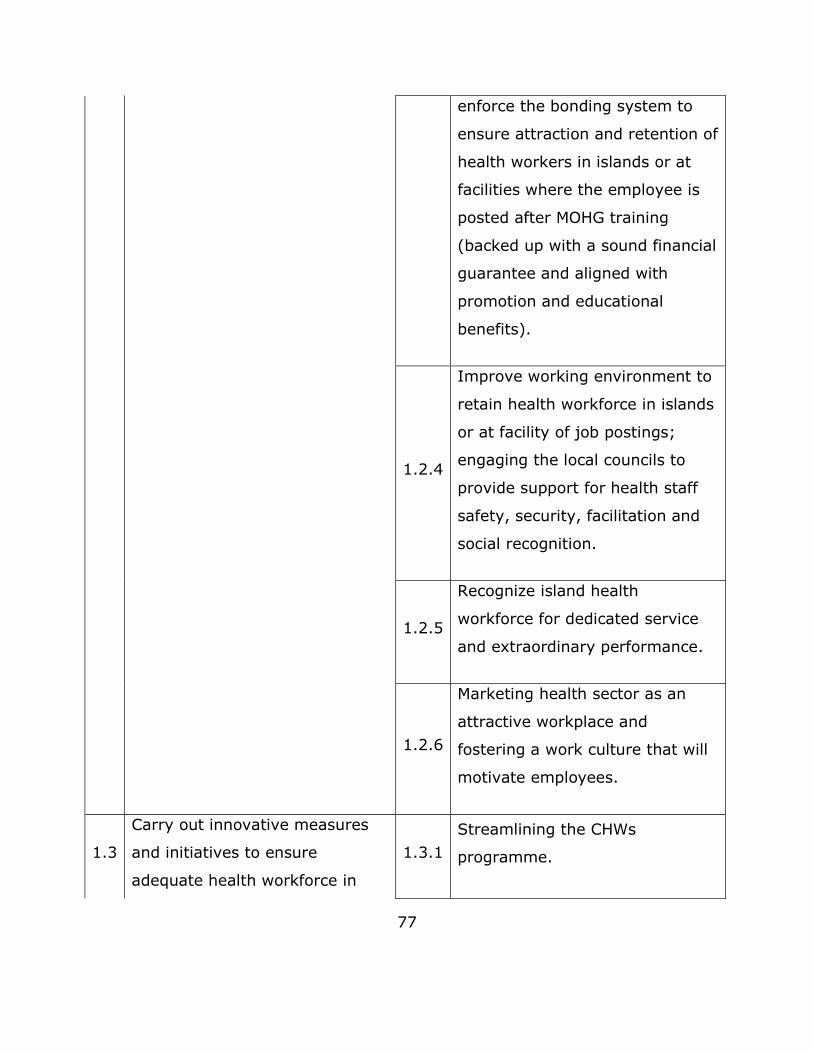
77
enforce the bonding system to
ensure attraction and retention of
health workers in islands or at
facilities where the employee is
posted after MOHG training
(backed up with a sound financial
guarantee and aligned with
promotion and educational
benefits).
1.2.4
Improve working environment to
retain health workforce in islands
or at facility of job postings;
engaging the local councils to
provide support for health staff
safety, security, facilitation and
social recognition.
1.2.5
Recognize island health
workforce for dedicated service
and extraordinary performance.
1.2.6
Marketing health sector as an
attractive workplace and
fostering a work culture that will
motivate employees.
1.3
Carry out innovative measures
and initiatives to ensure
adequate health workforce in
1.3.1
Streamlining the CHWs
programme.

78
remote areas to cope with
emerging health needs.
1.4
Strengthening capacity of the
HRD at central and peripheral
levels.
1.4.1 Capacity-building at all levels.
1.5
Strengthen national capacity for
health system management and
leadership development at the
national level.
1.5.1
Develop and provide executive
managerial training courses for
health managers, including
MOHG to excel their
management skills and
leadership capacities, as well as
improve health service
management for all those
working as managers at facility
level.
1.5.2
Develop a competency-based
model for health management at
all levels of service, including
MOHG, to carry out periodic
results-based assessment of all
management staff linked to their
promotions.
1.5.3
Introduce a health service
performance appraisal system for
health facilities.
1.5.4
Strengthen capacity for local
planning at subnational level.
1.5.5 Introduce workload criteria using
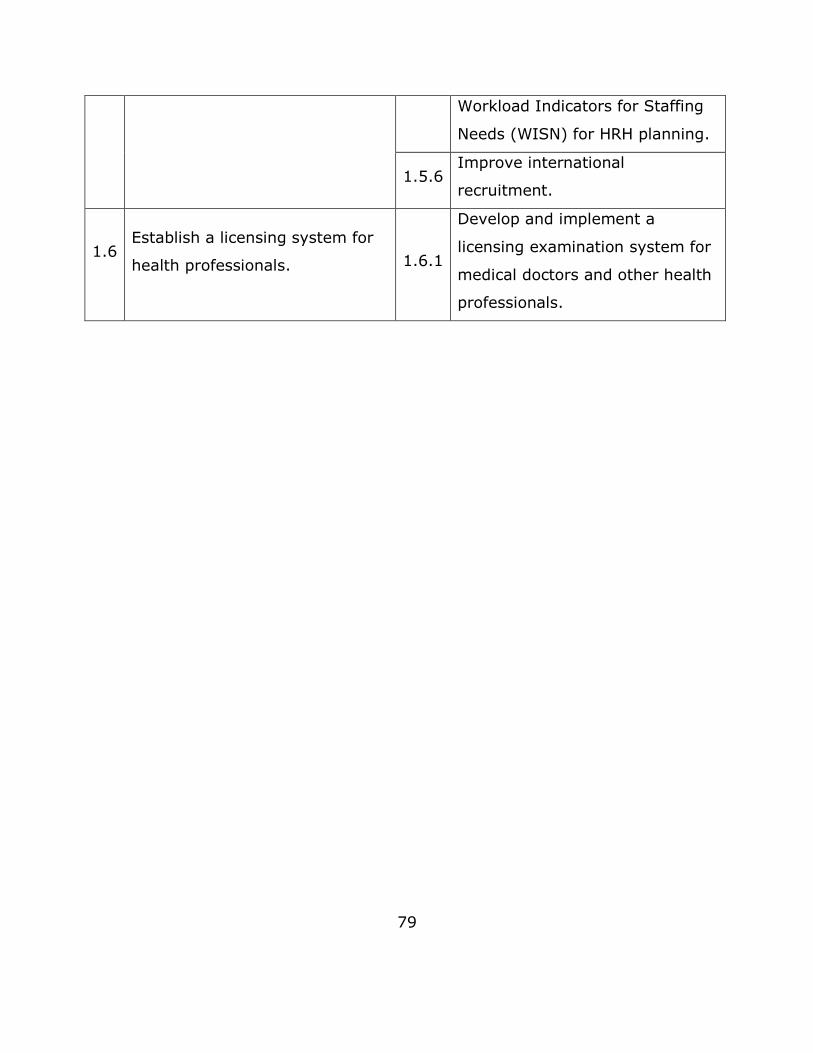
79
Workload Indicators for Staffing
Needs (WISN) for HRH planning.
1.5.6 Improve international
recruitment.
1.6 Establish a licensing system for
health professionals. 1.6.1
Develop and implement a
licensing examination system for
medical doctors and other health
professionals.
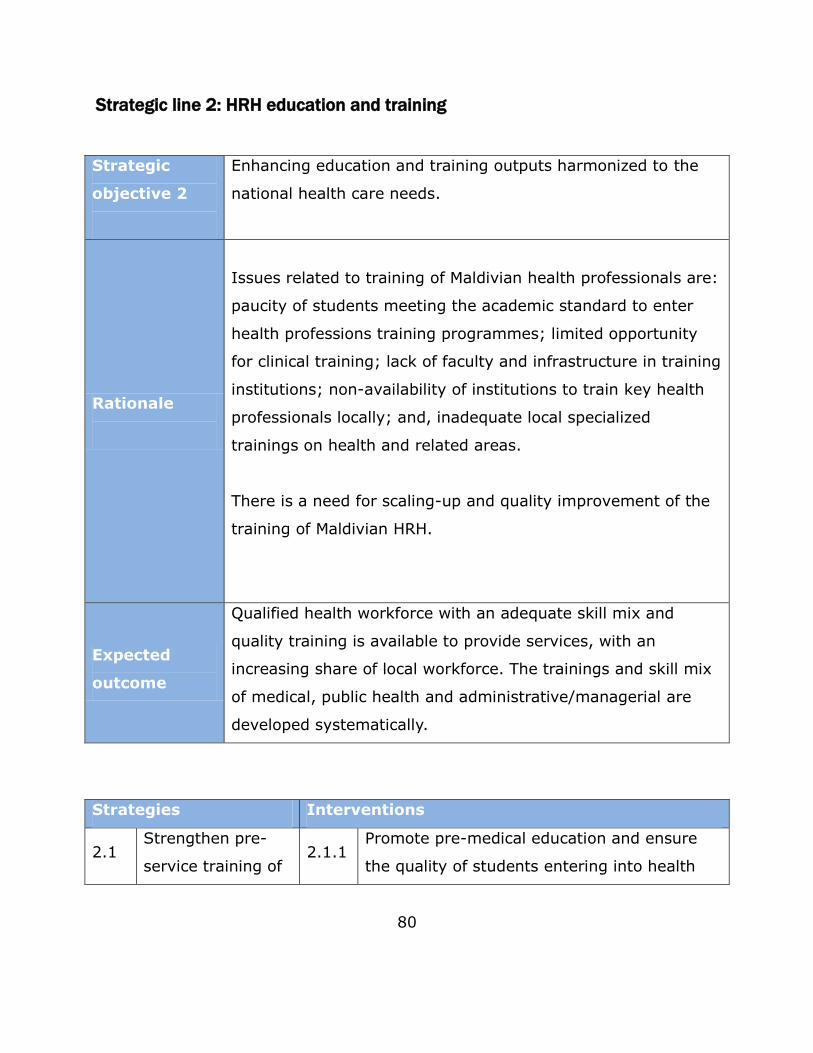
80
Strategic line 2: HRH education and training
Strategic
objective 2
Enhancing education and training outputs harmonized to the
national health care needs.
Rationale
Issues related to training of Maldivian health professionals are:
paucity of students meeting the academic standard to enter
health professions training programmes; limited opportunity
for clinical training; lack of faculty and infrastructure in training
institutions; non-availability of institutions to train key health
professionals locally; and, inadequate local specialized
trainings on health and related areas.
There is a need for scaling-up and quality improvement of the
training of Maldivian HRH.
Expected
outcome
Qualified health workforce with an adequate skill mix and
quality training is available to provide services, with an
increasing share of local workforce. The trainings and skill mix
of medical, public health and administrative/managerial are
developed systematically.
Strategies Interventions
2.1 Strengthen pre-
service training of 2.1.1
Promote pre-medical education and ensure
the quality of students entering into health

81
health
professionals and
scale up training of
local health
professionals.
professions education, through adequate
marketing and policy support by Ministry of
Education.
2.1.2
Establish a mechanism for regular monitoring
and review of quality of health professions
training programmes through an
institutionalized process.
2.1.3
Expand clinical training opportunities through
innovative approaches.
2.1.4
Strengthening the capacity of FHS in training,
research and development. The training
conducted should cater for the needs of the
national health sector and trainees should be
bonded to the public health sector.
2.1.5
Increasing uptake of public services staff with
training bonds or subsidized rates at
government training institutions, including
FHS.
2.1.6
Establishing the foundations to develop a
medical school through public–private
partnership, initially inviting faculty from
outside on a term-by-term basis and
gradually developing national faculty.
2.2 Expand
opportunities for 2.2.1
Negotiate to increase the number of overseas
training slots for training of specialists and

82
specialized
postgraduate
training of health
professionals.
strengthen the bonding system.
2.2.2
Develop IGMH as an accredited training
centre affiliated to overseas degree-awarding
organization/s.
2.2.3
Bilateral arrangement with international
institutes for training in Maldives through
faculty exchange.
2.2.4
Identify and facilitate scholarships and loan
schemes for overseas training.
2.2.5
Expand or plan training opportunities in
administrative/managerial and technical areas
for medical, nursing and public health staff.
2.3
Institutionalize
quality assured
health
professionals’
education for all
cadres.
2.3.1
Establish quality assurance standards and
processes for health professionals’ education
and training.
3.3.2
Introduce an internship and residency
programme for doctors, with at least 20%
service in islands.
2.3.3
Develop an induction programme for new
recruits in all cadres, for orientation at the
time of joining service or a new position in
the health system.

83
2.4
Establish a
comprehensive
and structured
CPD programme
for health
professionals.
2.4.1
Develop and implement a national CPD
strategy for workers to achieve the
competencies required for optimal job
performance.
2.4.2
Provide telemedicine, distance and online
learning opportunities through developing
knowledge centres in hospitals and guidance
services under the CPD secretariat.

84
Strategic line 3: HRH Financing and partnerships
Strategic
objective 3
Improving financial inputs from public, private and
international sources; streamlining the multi-stakeholder
coordination processes, and fostering bilateral partnerships
with organizations, entities, institutions and countries.
Rationale
HRH absorbs a considerable share of the health budget. Total
spending on health workforce is approximately 79% of the
recurrent health budget, which is higher than other countries
in the region. However, Maldives currently faces an alarming
escalation in health care costs together with a vulnerable fiscal
position, which is a burden on the Government.
Appropriate opportunities and methods should be made
available to enable and empower all stakeholders, including
intersectoral partners, to participate in decision-making and
work in honest and open partnership.
Expected
outcomes
Increased financial input from the Government and other
stakeholders, with better accountability mechanisms and
synergic partnerships.
Strategies Interventions
3.1
Develop national
policy and plan for
enhancing the
HRH resources
from the national
budget as well as
3.1.1 Develop HRH resource mobilization
strategy.
3.1.2
Advocating for a greater share and
allocation of public sector financial
resources.
3.1.3 Allocate resources under each programme
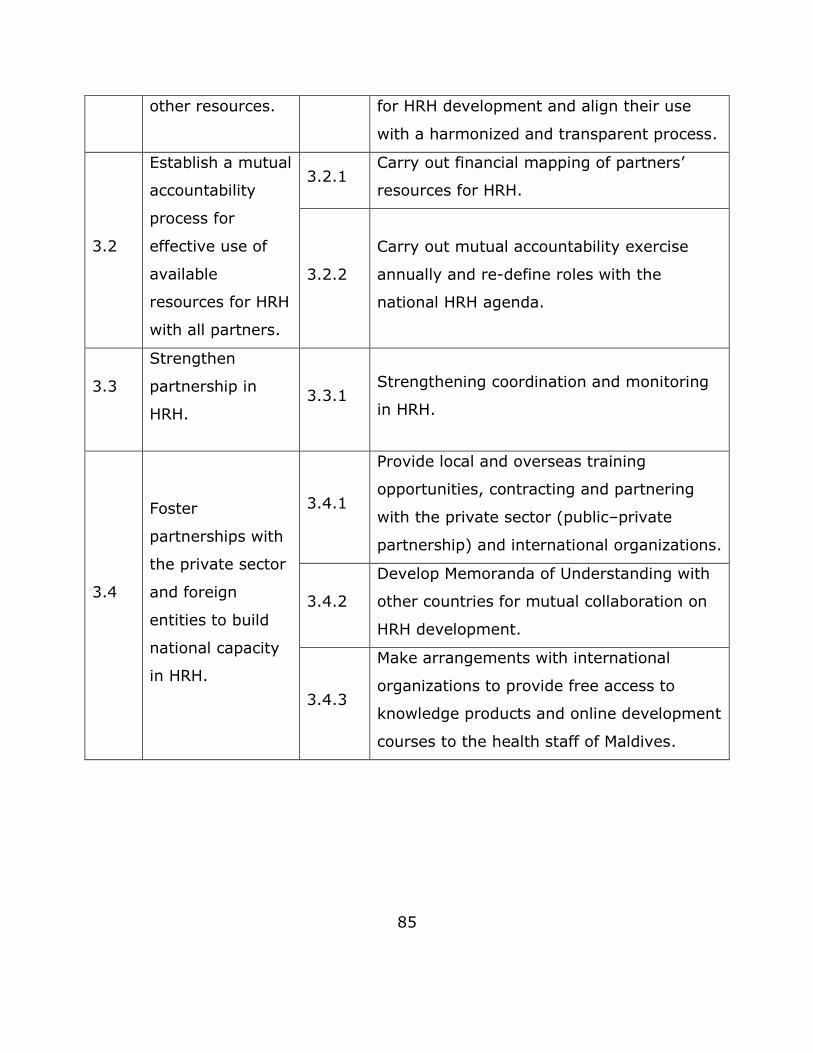
85
other resources. for HRH development and align their use
with a harmonized and transparent process.
3.2
Establish a mutual
accountability
process for
effective use of
available
resources for HRH
with all partners.
3.2.1 Carry out financial mapping of partners’
resources for HRH.
3.2.2
Carry out mutual accountability exercise
annually and re-define roles with the
national HRH agenda.
3.3
Strengthen
partnership in
HRH. 3.3.1
Strengthening coordination and monitoring
in HRH.
3.4
Foster
partnerships with
the private sector
and foreign
entities to build
national capacity
in HRH.
3.4.1
Provide local and overseas training
opportunities, contracting and partnering
with the private sector (public–private
partnership) and international organizations.
3.4.2
Develop Memoranda of Understanding with
other countries for mutual collaboration on
HRH development.
3.4.3
Make arrangements with international
organizations to provide free access to
knowledge products and online development
courses to the health staff of Maldives.

86
Section D: The way forward Based on findings highlighted in this report and several stakeholder
consultations, the HRH strategic plan proposed in Section C addresses HRH
challenges in Maldives. The three strategic objectives will serve as guidelines to
implement plans to solve HRH problems. Detailed steps required to ensure
appropriate implementation of the strategic plan are provided in Table 25.
Table 22. Forward plan
Objectives Activities Sub-activities Process Roles
Developing a
detailed
operational
plan to
implement the
planned
strategies and
interventions.
Operational
plan
Development
of draft plan
Hire a consultant
to develop initial
draft based upon
the agreed
operational plan
WHO
Inputs from all
concerned and
revision
Consultation
with
stakeholders
through
individual and
group meetings
Consultant
Validation
Face to face/
online
consultation
Consultant
Approval Agreement WHO, MOHG
Estimating the
cost of the
planned
activities,
interventions
and strategies,
indicating each
partner’s share
and timeframe.
Costing
Costing draft
based upon
operational
plan
Hire a consultant
to make costing
the agreed
operational plan
(activity-wise,
intervention-
wise and
strategy-wise,
and then total)
WHO
Consultation
and revision
Review by
stakeholders Consultant
Validation
Face to face/
online
consultation
Consultant
Approval Agreement WHO, MOHG

87
Preparing a
monitoring and
evaluation plan
to ensure the
set objectives
are met.
Monitoring
and
evaluation
plan
Monitoring and
evaluation plan
draft
The consultant
hired for
operational
planning will
develop
monitoring and
evaluation plan,
along with the
indicators and
implementation
framework
Consultant
Validation
Face to face/
online
consultation
Consultant
Approval Agreement WHO, MOHG
Developing a
resource
mobilization
plan to guide
HRH financing
efforts.
Resource
mobilization
plan
Resource
mobilization
policy and plan
draft
The consultant
hired for costing
will develop the
resource
mobilization plan
Consultant
Validation
Face to face/
online
consultation
Consultant
Approval Agreement WHO, MOHG

88
Annexes
Annex 1. Technical working group
Name Designation Organization
Dr Sheeza Ali Director General of Health
Services Ministry of Health and Gender
Dr Akjemal
Magtymova WHO Representative WHO Country Office, Maldives
Dr Igor Pokanevych Medical Officer WHO Country Office, Maldives
Ms Asma Ibrahim Director Health Protection Agency, Ministry of
Health and Gender
Ms Aisath
Mohammed Director
Maldives Food and Drugs Agency,
Ministry of Health and Gender
Ms Sofeenaz
Hassan Director
Human Resource Division, Ministry of
Health and Gender
Ms Aminath Shaina Assistant Director Policy Planning Division, Ministry of
Health and Gender
Ms Aminath Nashia Assistant Director Ministry of Health and Gender
Mr Ahmed Shakir Director Health Service Division, Ministry of
Health and Gender
Dr Mohamed
Habeeb Chief Civil Servant Indira Gandhi Memorial Hospital
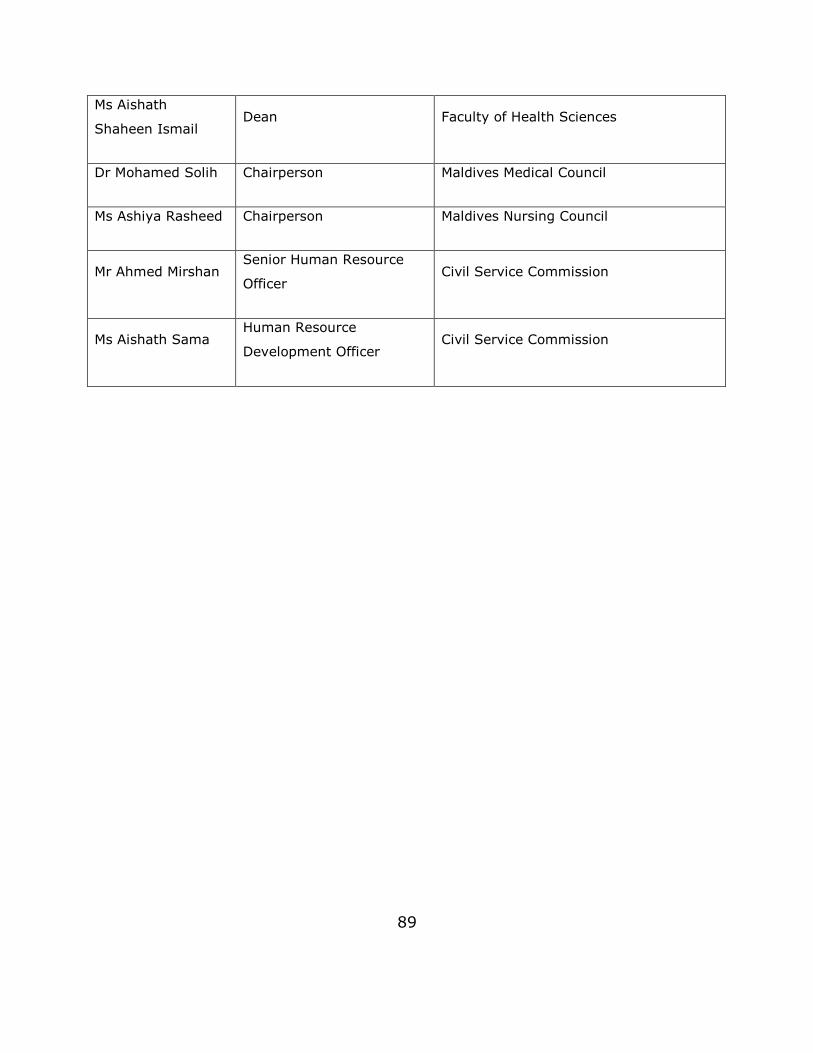
89
Ms Aishath
Shaheen Ismail Dean Faculty of Health Sciences
Dr Mohamed Solih Chairperson Maldives Medical Council
Ms Ashiya Rasheed Chairperson Maldives Nursing Council
Mr Ahmed Mirshan Senior Human Resource
Officer Civil Service Commission
Ms Aishath Sama Human Resource
Development Officer Civil Service Commission

90
Annex 2. Stakeholders engaged in development and validation
Name Designation Organization
Ms Geela Ali Permanent Secretary Ministry of Health and Gender
Dr Sheeza Ali Director General of Health Services
Ministry of Health and Gender
Dr Akjemal
Magtymova
WHO Representative to the
Republic of Maldives WHO
Ms Shareefa Adam Manik
Director General Maldives Food and Drugs Authority
Ms Asma Ibrahim Director Health Protection Agency, Ministry of Health and Gender
Ms Aishath Samiya Director Policy Planning Division, Ministry of
Health and Gender
Ms Sofeenaz Hassan
Director Human Resource Division, Ministry of Health and Gender
Ms Aminath Shaina Assistant Director Policy Planning Division, Ministry of Health and Gender
Ms Aminath Nashia Assistant Director Training Section, Ministry of Health and Gender
Mr. Ahmed Shakir Director Health Service Division, Ministry of Health and Gender
Dr Mohamed
Habeeb CEO Indira Gandhi Memorial Hospital
Mr Abdulla Shinah Chief Operating Officer ADK Hospital
Ms Aishath Shaheen Ismail
Dean Faculty of Health Sciences
Dr Mohamed Solih Chairperson Maldives Medical Council
Ms Ashiya Rasheed Chairperson Maldives Nursing Council

91
Ms Aishatt Mahfoosa
Chairperson Maldives Board of Health Sciences
Mr Yoosuf Naeem Assistant Director Ministry of Finance and Treasury
Mr Ahmed Mirshan Senior Human Resource Officer Civil Service Commission
Ms Aishath Sama Human Resource Development Officer
Civil Service Commission
Ms Zeba Tanvir Bukhari
UNICEF Representative to Maldives
UNICEF
Ms Azusa Kuboto Programme Operation Coordinator
UNDP
Mr Alejandro Ruiz-Acevedo
Project Centre Manager UNOPS
Ms Athifa Ibrahim Programme Analyst UNDP
Mr Murthada Sessay
Project Manager UNOPS
Ms Jeehan Saleem National Programme Officer UNFPA
Mr Mohamed Faisal Coordination Specialist Resident Coordinator’s Office, UN Maldives
Mr Mohamed
Hunaif Under Secretary President’s Office

92
Annex 3. HRH positions approved by the CSC for health-care facilities under the MOHG
(staffing standards)
Medical workforce
IGMH TH CTR
# Fclts. # Fclts. # Fclts. # Fclts. # Fclts. # Fclts. # Fclts. # Fclts.
5 5 7 3 20 41 33 27
1 Cardiologist 1 5 0 0 0 0 0 0 0 2 7
2 Urologist 1 5 0 0 0 0 0 0 0 1 6
3 Pulomonologist 0 0 0 0 0 0 0 0 2 2
4 Physician 2 10 1 5 1 7 0 0 0 0 0 11 33
5 Orthopaedic Surgeon 1 5 1 5 0 0 0 0 0 0 7 17
6 Gastroenterologist 0 0 0 0 0 0 0 0 1 1
7 Neurologist 0 0 0 0 0 0 0 0 3 3
8 Emergency Medicine 0 0 0 0 0 0 0 0 2 2
9 Radiology 0 0 0 0 0 0 0 0 5 5
10 Pathology 0 0 0 0 0 0 0 0 5 1 7
11 Maxillofacial Surgery 0 0 0 0 0 0 0 0 1 1
12 Orthodontics 0 0 0 0 0 0 0 0 1 1
13 Ophthalmologist 1 5 1 5 0 0 0 0 0 0 6 16
14 Gynaecologist 2 10 2 10 2 14 1 3 0 0 0 0 12 49
15 Anaesthesiologist 2 10 2 10 1 7 1 3 0 0 0 0 10 40
16 Surgeon 2 10 1 5 1 7 0 0 0 0 0 10 32
17 Paediatrician 2 10 1 5 1 7 1 3 0 0 0 0 10 35
18 Dermatologist 1 5 0 0 0 0 0 0 0 4 9
19 Cardio surgeon 0 0 0 0 0 0 0 0 1 1
20 ENT Surgeon 1 5 0 0 0 0 0 0 0 4 9
21 Psychiatrist /Clinical Physiologist 1 5 1 5 0 0 0 0 0 0 3 13
22General Practitioner (Senior Medical
Officer/Medical Officer /Registrar)7 35 5 25 4 28 4 12 2 40 1 41 1 33 0 91 3 308
TOTAL
STANDARDSS
HOSP 1 HOSP 2 HOSP 3 HOSP 4 HC 1 HC 2 HC 3 HC 4
SS SS SS SS SSSS SS SS SS# Posts

93
Paramedical workforce
IGMH TH CTR
# Fclts. # Fclts. # Fclts. # Fclts. # Fclts. # Fclts. # Fclts. # Fclts.
5 5 7 3 20 41 33 27
23 Dentist 1 5 1 5 0 0 0 0 0 0 8 18
24 Dental Hygienist /Dental Assistant 2 10 1 5 0 0 0 0 0 0 16 31
25 Pharmacist 0 0 0 0 0 0 0 0 2 2
26 Radiographer 2 10 2 10 1 7 1 3 0 0 0 0 14 44
27 Radiographer Assistant 0 0 0 0 0 0 0 0 6 6
28 Radiographer Trainee 1 5 1 5 1 7 1 3 0 0 0 0 20
29 Optometrist 0 0 0 0 0 0 0 0 1 1
30 Physiotherapist 2 10 1 5 0 0 0 0 0 0 12 27
31 Physiotherapist Assistant 0 0 0 0 0 0 0 0 10 10
32 Physiotherpaist Trainee 1 5 1 5 0 0 0 0 0 0 10
33 Labortaory Technologist 6 30 4 20 3 21 2 6 2 40 1 41 1 33 0 60 12 263
34 Labortatory Assistant 2 10 1 5 1 7 1 3 0 0 0 0 10 35
35 EEG/EMG Technician 0 0 0 0 0 0 0 0 2 2
36 Speech Therapist 0 0 0 0 0 0 0 0 1 1
37 Nurses 86 430 60 300 36 252 23 69 18 360 10 410 4 132 2 54 619 16 2642
38 Nurse Midwife 0 0 0 0 2 40 1 41 1 33 1 27 8 149
39 Dietician 0 0 0 0 0 0 0 0 1 1
40 Councellors 1 5 1 5 1 7 1 3 0 0 0 0 3 23
41Regional Health Administrator/ Director/
Manager1 5 1 5 1 7 1 3 0 0 0 0
14 2 36
42 Assistant Manager / Deputy Manager 2 10 1 5 1 7 1 3 0 0 0 0 13 38
43 Administrative Officer 0 0 0 0 0 0 0 0 67 11 77
44
Senior Health Cordinator / Community
Health Cordinator / Community Health
Supervisor/ Community Health Worker
4 20 4 20 3 21 3 9 2 40 2 82 1 33 1 27
1 253
45 Family Health Officer 0 0 0 0 1 20 1 41 1 33 1 27 121
TOTAL
STANDARDSS
HOSP 1 HOSP 2 HOSP 3 HOSP 4 HC 1 HC 2 HC 3 HC 4
SS SS SS SS SSSS SS SS SS# Posts

94
Support workforce
IGMH TH CTR
# Fclts. # Fclts. # Fclts. # Fclts. # Fclts. # Fclts. # Fclts. # Fclts.
5 5 7 3 20 41 33 27
46 Secretary 5 25 4 20 3 21 2 6 3 60 3 123 3 99 2 54 7 415
47 Budjet Officer 3 15 2 10 2 14 2 6 1 20 0 0 0 10 75
48 Maintenance Officer 2 10 1 5 1 7 1 3 0 0 0 0 25
49 Medical Record Officer 4 20 3 15 2 14 1 3 1 20 0 0 0 3 75
50 IT Officer 2 10 2 10 1 7 1 3 0 0 0 0 10 40
51 Cashier 8 40 6 30 5 35 4 12 2 40 1 41 1 33 0 34 265
52 Public Realation Officer 6 30 4 20 3 21 3 9 1 20 0 0 0 24 124
53 Clinical assistant 0 0 0 0 0 0 0 0 69 2 71
54 Translator 18 90 12 60 8 56 5 15 2 40 1 41 1 33 0 335
55 Reception Clark 8 40 6 30 6 42 5 15 3 60 3 123 3 99 0 6 415
56 Store Keeper 3 15 2 10 2 14 1 3 1 20 0 0 0 5 67
57 House Keeper 2 10 1 5 1 7 1 3 1 20 0 0 0 28 73
58 Sarudhaaru 1 5 0 0 0 0 0 0 0 5
59 Messenger 1 5 1 5 1 7 1 3 0 0 0 0 20
60 Masakkathu (Support Staffs) 4 20 2 10 2 14 2 6 4 80 3 123 3 99 1 27 9 388
61 Masakkathu (staff Accomodation) 4 20 4 20 3 21 3 9 0 0 0 0 70
62 Attendent / Health Auxiliary 16 80 12 60 10 70 8 24 9 180 7 287 4 132 2 54 9 5 901
63 Security Officer /Watcher 10 50 6 30 6 42 4 12 2 40 2 82 1 33 0 43 332
64 Mechanic 4 20 4 20 2 14 2 6 1 20 0 0 0 27 107
65 Electrician 2 10 1 5 1 7 1 3 1 20 0 0 0 12 57
66 Bio Medical Technician 1 5 1 5 1 7 1 3 0 0 0 0 3 23
67 Ambulance Driver / Attanedent 10 50 8 40 6 42 5 15 3 60 2 82 2 66 0 146 501
68 Dhonna (Laundry Assistants) 6 30 6 30 4 28 4 12 2 40 2 82 1 33 1 27 282
69 Nevi/Captain/Driver 2 10 2 10 1 7 1 3 0 0 0 0 22 52
70 Mechanic Driver 2 10 2 10 1 7 1 3 0 0 0 0 30
71 Falhuveri 4 20 4 20 2 14 2 6 0 0 0 0 60
263 1315 190 950 132 924 102 306 64 1280 40 1640 28 924 11 297 1526 53 9215
TOTAL
STANDARDSS
HOSP 1 HOSP 2 HOSP 3 HOSP 4 HC 1 HC 2 HC 3 HC 4
SS SS SS SS
Grand Total
SSSS SS SS SS# Posts

95
Annex 4. Distribution of expatriate/local HRH, standards and
vacancy rates in hospitals level 1–4 (regional/atoll) (Source:
MOHG)
Loca l Expa t Loca l Expa t Loca l Expa t Loca l Expa t
1 Cardiologis t 1 0 0 0 0 0 0 05
1 1 0 -480%
2 Urologis t 0 0 0 0 0 0 0 05
0 0 0 -5100%
3 Phys ician 0 4 0 3 0 0 0 022
7 0 7 -1568%
4 Orthopaedic Surgeon 0 3 0 1 0 0 0 010
4 0 4 -660%
5 Ophthalmologis t 0 3 0 0 0 0 0 010
3 0 3 -770%
6 Gynaecologis t 0 7 0 3 0 6 0 137
17 0 17 -2054%
7 Anaes thes iologis t 0 4 0 5 0 7 0 230
18 0 18 -1240%
8 Surgeon 0 5 0 3 0 1 0 022
9 0 9 -1359%
9 Paediatrician 0 5 0 3 0 5 0 225
15 0 15 -1040%
10 Dermatologis t 0 0 0 0 0 0 0 05
0 0 0 -5100%
11 ENT Surgeon 0 2 0 0 0 0 0 05
2 0 2 -360%
12 Ps ychiatris t /Clinical Phys iologis t 0 0 0 1 0 0 0 010
1 0 1 -990%
13 General P ractitioner (Senior Medical Officer/Medical Officer /Regis trar) 3 31 0 19 1 30 0 10 100 94 4 90 -6 6%
14 Dentis t 1 2 0 3 0 0 0 010
6 1 5 -440%
15 Radiographer 0 10 0 5 0 7 0 330
25 0 25 -517%
16 Phys iotherapis t 0 5 0 1 0 0 0 015
6 0 6 -960%
17 Laboratory Technologis t 11 21 10 9 4 17 0 677
78 25 53 1-1%
18 Dental Hygienis t /Dental As s is tant 0 0 0 0 0 0 0 015
0 0 0 -15100%
19 Radiographer Trainee 2 0 3 0 7 0 1 020
13 13 0 -735%
20 Phys iotherapis t Trainee 3 0 0 0 0 0 0 010
3 3 0 -770%
21 Laboratory As s is tant 2 0 2 0 2 0 0 025
6 6 0 -1976%
22 Nurs es 176 126 68 87 90 73 16 30 1051 666 350 316 -38537%
23 Couns ellors 0 0 0 0 0 0 0 020
0 0 0 -20100%
24 Regional Health Adminis trator/ Director/ Manager 2 0 1 0 3 0 2 0
208 8 0 -12
60%
25 As s is tant Manager / Deputy Manager 5 0 2 0 4 0 0 025
11 11 0 -1456%
26Senior Health Coordinator / Community Health Coordinator / Community Health Supervis or/ Community Health Worker
3 0 0 0 1 0 1 0 70 5 5 0 -6593%
Ga p Va ca ncy ra te
Tota l (sta nda rd) OCCUPIED EXPATLOCAL# POSTS
Hosp L1 Hosp L2 Hosp L3 Hosp L4

96
(Contd.)
Loca l Expa t Loca l Expa t Loca l Expa t Loca l Expa t
27 Secretary 31 5 20 2 28 0 5 072
91 84 7 19-26%
28 Budget Officer 9 0 12 2 15 0 3 045
41 39 2 -49%
29 Maintenance Officer 3 0 3 0 2 0 0 025
8 8 0 -1768%
30 Medical Record Officer 5 0 3 1 6 0 3 052
18 17 1 -3465%
31 IT Officer 2 0 2 0 3 0 0 030
7 7 0 -2377%
32 Cas hier 16 0 3 4 17 0 6 0117
46 42 4 -7161%
33 Public Relations Officer 17 0 8 1 15 0 5 080
46 45 1 -3443%
34 Trans lator 47 0 26 4 29 0 9 0221
115 111 4 -10648%
35 Reception Clark 28 0 15 4 25 0 7 0127
79 75 4 -4838%
36 S tore Keeper 3 0 3 1 8 0 2 042
17 16 1 -2560%
37 Hous e Keeper 6 0 4 0 4 0 3 025
17 17 0 -832%
38 Sarudhaaru 1 0 0 0 0 0 0 05
1 1 0 -480%
39 Mes s enger 2 0 0 0 2 0 2 020
6 6 0 -1470%
40 Mas akkathu 13 0 10 2 13 0 6 050
44 42 2 -612%
41 Mas akkathu (s taff Accommodation) 13 0 12 1 21 0 7 070
54 53 1 -1623%
42 Attendant / Health Auxiliary 50 0 24 7 45 0 13 0234
139 132 7 -9541%
43 Security Officer /Watcher 28 0 18 3 22 0 8 0134
79 76 3 -5541%
44 Mechanic 9 0 3 2 10 0 1 060
25 23 2 -3558%
45 Electrician 8 0 1 0 3 0 2 025
14 14 0 -1144%
46 Bio Medical Technician 0 1 1 0 0 0 0 020
2 1 1 -1890%
47 Ambulance Driver / Attendant 38 0 21 2 29 0 6 0147
96 94 2 -5135%
48 Dhonna 29 0 18 3 26 0 11 0100
87 84 3 -1313%
49 Nevi/Captain/Driver 3 0 4 1 7 0 3 030
18 17 1 -1240%
50 Mechanic Driver 3 0 3 1 8 0 1 030
16 15 1 -1447%
51 Falhuveri 9 0 5 2 14 0 6 060
36 34 2 -2440%
582 234 305 186 464 146 129 54 3495 2100 1480 620 -1395 40%TOTAL
Ga p Va ca ncy ra te
Tota l (sta nda rd) OCCUPIED EXPATLOCAL# POSTS
Hosp L1 Hosp L2 Hosp L3 Hosp L4

97
Annex 5. Distribution of expatriate/local HRH, standards and
vacancy rates in health centres level 1–4 (Source: MOHG)
loca l expat loca l expat loca l expat loca l expat
1 Community Health Worker 3 0 9 0 8 0 6 0182 26 26 0 -156 86%
7 Administrative Officer /Secretary 53 0 82 0 42 0 20 0 336 197 197 0 -139 41%
3 SMO/MO/Registrar 0 33 0 45 0 32 0 0114 110 0 110 -4 4%
4 Nurses 116 83 111 118 38 58 4 17956 545 269 276 -411 43%
5 Nurse Midwife 0 0 0 0 0 0 0 0141 0 0 0 -141 100%
6 Laboratory Technologist 5 22 3 33 0 5 0 0114 68 8 60 -46 40%
8 Budget Officer 0 0 0 0 0 0 0 020 0 0 0 -20 100%
9 Cashier 15 0 5 0 4 0 0 0114 24 24 0 -90 79%
10 Medical Record Officer 0 0 0 0 0 0 0 020 0 0 0 -20 100%
11 Translator 34 0 38 0 24 0 0 0114 96 96 0 -18 16%
12 Public Relation Officer 0 0 0 0 0 0 0 020 0 0 0 -20 100%
13 Reception Clark 28 0 20 0 10 0 0 0282 58 58 0 -224 79%
14 Store Keeper 0 0 0 0 0 0 0 020 0 0 0 -20 100%
15 Family Health Officer 0 0 0 0 0 0 0 0121 0 0 0 -121 100%
16 House Keeper 0 0 0 0 0 0 0 020 0 0 0 -20 100%
17 Masakkathu 43 0 86 0 42 0 21 0329 192 192 0 -137 42%
18 Attendant /Health Auxiliary 86 0 114 0 47 0 2 0653 249 249 0 -404 62%
20 Ambulance Driver /Attendant 42 0 67 0 37 0 0 0208 146 146 0 -62 30%
21 Mechanic 2 0 0 0 0 0 0 020 2 2 0 -18 90%
22 Electrician 0 0 0 0 0 0 0 020 0 0 0 -20 100%
23 Watcher 28 0 35 0 22 0 0 0155 85 85 0 -70 45%
24 Dhonna 14 0 23 0 17 0 0 0182 54 54 0 -128 70%
469 138 593 196 291 95 53 17 4141 1852 1406 446 -2289 55%TOTAL
HC L1 HC L2 HC L3 Va ca ncy ra tePOSTS#
HC L4OCCUPIED EXPATLOCALTota l
sta nda rd Ga p
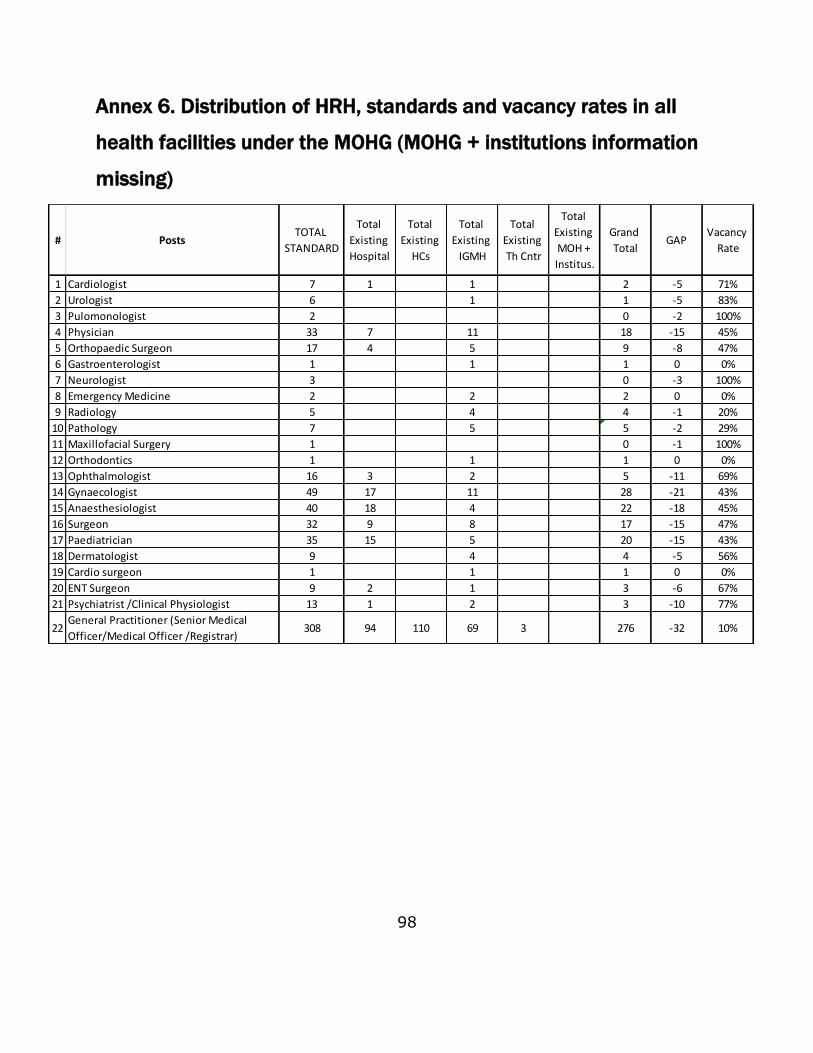
98
Annex 6. Distribution of HRH, standards and vacancy rates in all
health facilities under the MOHG (MOHG + institutions information
missing)
1 Cardiologist 7 1 1 2 -5 71%
2 Urologist 6 1 1 -5 83%
3 Pulomonologist 2 0 -2 100%
4 Physician 33 7 11 18 -15 45%
5 Orthopaedic Surgeon 17 4 5 9 -8 47%
6 Gastroenterologist 1 1 1 0 0%
7 Neurologist 3 0 -3 100%
8 Emergency Medicine 2 2 2 0 0%
9 Radiology 5 4 4 -1 20%
10 Pathology 7 5 5 -2 29%
11 Maxillofacial Surgery 1 0 -1 100%
12 Orthodontics 1 1 1 0 0%
13 Ophthalmologist 16 3 2 5 -11 69%
14 Gynaecologist 49 17 11 28 -21 43%
15 Anaesthesiologist 40 18 4 22 -18 45%
16 Surgeon 32 9 8 17 -15 47%
17 Paediatrician 35 15 5 20 -15 43%
18 Dermatologist 9 4 4 -5 56%
19 Cardio surgeon 1 1 1 0 0%
20 ENT Surgeon 9 2 1 3 -6 67%
21 Psychiatrist /Clinical Physiologist 13 1 2 3 -10 77%
22General Practitioner (Senior Medical
Officer/Medical Officer /Registrar)308 94 110 69 3 276 -32 10%
GAPGrand
Total
Vacancy
Rate
TOTAL
STANDARD
Total
Existing
Hospital
Total
Existing
HCs
Total
Existing
IGMH
Total
Existing
Th Cntr
Total
Existing
MOH +
Institus.
# Posts

99
(Contd.)

100
(Contd.)
46 Secretary 415 91 4 95 -320 77%
47 Budjet Officer 75 41 9 50 -25 33%
48 Maintenance Officer 25 8 8 -17 68%
49 Medical Record Officer 75 18 3 21 -54 72%
50 IT Officer 40 7 7 14 -26 65%
51 Cashier 265 46 24 34 104 -161 61%
52 Public Realation Officer 124 46 21 67 -57 46%
53 Clinical assistant 71 30 2 32 -39 55%
54 Translator 335 115 96 211 -124 37%
55 Reception Clark 415 79 58 6 143 -272 66%
56 Store Keeper 67 17 3 20 -47 70%
57 House Keeper 73 17 27 44 -29 40%
58 Sarudhaaru 5 1 1 -4 80%
59 Messenger 20 6 6 -14 70%
60 Masakkathu (Support Staffs) 388 44 192 9 245 -143 37%
61 Masakkathu (staff Accomodation) 70 54 54 -16 23%
62 Attendent / Health Auxiliary 901 139 249 132 4 524 -377 42%
63 Security Officer /Watcher 332 79 85 30 194 -138 42%
64 Mechanic 107 25 2 33 60 -47 44%
65 Electrician 57 14 5 19 -38 67%
66 Bio Medical Technician 23 2 2 4 -19 83%
67 Ambulance Driver / Attanedent 501 96 146 242 -259 52%
68 Dhonna (Laundry Assistants) 282 87 54 141 -141 50%
69 Nevi/Captain/Driver 52 18 20 38 -14 27%
70 Mechanic Driver 30 16 16 -14 47%
71 Falhuveri 60 60 60 0 0%
9215 2124 1852 1276 45 5297 -3918 43%
GAPGrand
Total
Vacancy
Rate
TOTAL
STANDARD
Total
Existing
Hospital
Total
Existing
HCs
Total
Existing
IGMH
Total
Existing
Th Cntr
Total
Existing
MOH +
Institus.
Grand Total
# Posts
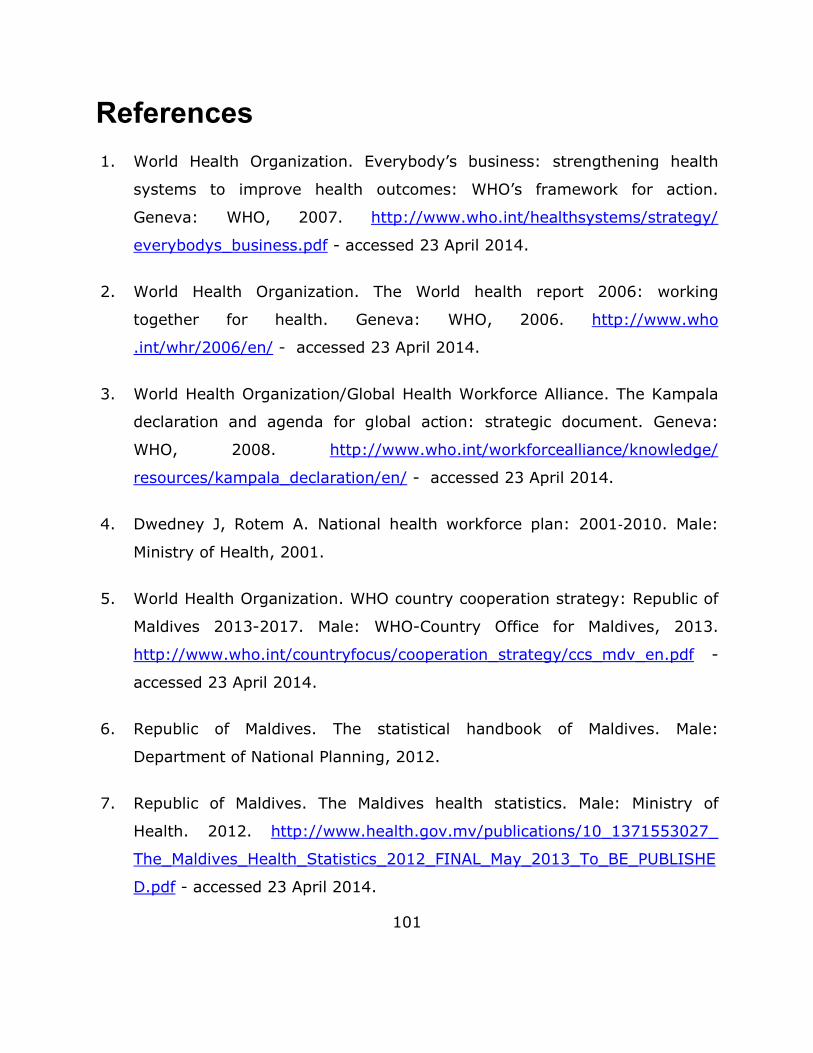
101
References
1. World Health Organization. Everybody’s business: strengthening health
systems to improve health outcomes: WHO’s framework for action.
Geneva: WHO, 2007. http://www.who.int/healthsystems/strategy/
everybodys_business.pdf - accessed 23 April 2014.
2. World Health Organization. The World health report 2006: working
together for health. Geneva: WHO, 2006. http://www.who
.int/whr/2006/en/ - accessed 23 April 2014.
3. World Health Organization/Global Health Workforce Alliance. The Kampala
declaration and agenda for global action: strategic document. Geneva:
WHO, 2008. http://www.who.int/workforcealliance/knowledge/
resources/kampala_declaration/en/ - accessed 23 April 2014.
4. Dwedney J, Rotem A. National health workforce plan: 2001‐2010. Male:
Ministry of Health, 2001.
5. World Health Organization. WHO country cooperation strategy: Republic of
Maldives 2013-2017. Male: WHO-Country Office for Maldives, 2013.
http://www.who.int/countryfocus/cooperation_strategy/ccs_mdv_en.pdf -
accessed 23 April 2014.
6. Republic of Maldives. The statistical handbook of Maldives. Male:
Department of National Planning, 2012.
7. Republic of Maldives. The Maldives health statistics. Male: Ministry of
Health. 2012. http://www.health.gov.mv/publications/10_1371553027_
The_Maldives_Health_Statistics_2012_FINAL_May_2013_To_BE_PUBLISHE
D.pdf - accessed 23 April 2014.
102
8. World Health Organization. Maldives National Health Accounts 2012. Male:
WHO Country Office for Maldives, 2012.
9. International Monetary Fund. Maldives: economic outlook: IMF mission,
April 2012.
10. Azzam O. Cost of running the basic service packages in Maldives. Male:
WHO Country Office for Maldives, 2013.
11. Republic of Maldives. Health master plan 2006-2016. Male: Ministry of
Health, 2006.
12. World Bank. Human capital for a modern society: general education in the
Maldives - an evolving seascape. Washington D.C.: The World Bank 2012.
13. Maldives Medical Council. Maldives Medical Council regulations. Male:
Ministry of Health.
14. Republic of Maldives Ministry of Health. Maldives Nursing Council
regulations. Male: MOH; Maldives Nursing Council.
15. The National University of Maldives. Course handbook-2012. Male: Faculty
of Health Sciences, 2012.
16. World Health Organization. Standards for MBBS education in Maldives:
WHO technical report. Male: WHO Country Office for Maldives, 2013.
17. The Maldives National University. Strategic plan. Male: MNU, 2012.
18. World Health Organization, Regional Office for South-East Asia. Regional
guidelines for continuing medical education (CME)/ continuing professional
development. (CPD) activities. New Delhi: WHO-SEARO, 2010.

103
http://www.searo.who.int/entity/human_resources/documents/Guide_CME
/en/ - accessed 24 April 2014.
19. Shareef AF, Kinshuk. Distance education in small island nations. In:
Encyclopedia of distance learning. 2009. Chapter 94. pp. 661-670.
http://www.igi-global.com/chapter/distance-education-small-island-
nations/11821 - accessed 24 April 2014.
20. Moosa S. Assessment of the human resource management system in the
health services of Maldives. Male: WHO Country Office for Maldives;
Ministry of Health, Maldives, 2012.
21. World Federation of Medical Education. Guidelines for accreditation of basic
medical education. World Federation of Medical Education. Male: WFME,
2012.
22. General Medical Council. Tomorrow’s doctors. London: General Medical
Council, 2003.
23. Harden RM, Gleeson FA. Assessment of clinical competence using an
objective structured clinical examination (OSCE). Medical Education.
1979;13(1):39–54.
24. Gupta SD, Jain NP. Mid-term review of national health workforce plan
2001-2010. Male: Ministry of Health; WHO Country Office for Maldives;
2006.
25. Global Health Workforce Alliance; USAID; World Health Organization. HRH:
Human resources for health action framework (HAF): a guide to develop
and implement strategies to achieve an effective and sustainable health
workforce. Cambridge: Management Sciences for Health, 2009.

104
http://www.msh.org/sites/msh.org/files/hrh_guidelines_final_for_sign-
off1.pdf - accessed 24 April 2014.
26. World Health Organization. Increasing access to health workers in remote
and rural areas through improved retention: global policy
recommendations. Geneva: WHO, 2010. http://whqlibdoc. who. int/
publications/2010/9789241564014_eng.pdf - accessed 24 April 2014.
27. Wiskow C, Aebreht T, Pietro C. How to create an attractive and supportive
working environment for health professionals. Policy brief 15. Copenhagen:
WHO Regional Office of Europe, 2010.


















