Hardware and measurement Abstraction l ayers · Hardware and measurement Abstraction l ayers

Name, Title, Affiliation Phil Ayers, PharmD, BCNSP, FASHP Chief, Clinical Pharmacy Services, Mississippi Baptist Medical Center Associate Clinical Professor, University of Mississippi School of Pharmacy Presentation Title Lipid Injectable Emulsions (ILE) Do’s and Don’ts Disclosures Speakers Bureau: Fresenius Kabi, Janssen Presentation Overview/Summary • In 2017, the ASPEN Parenteral Nutrition Safety Committee conducted a ILE Survey with Gap
Analysis. The survey revealed a number of institutions do not filter their ILE’s and infusion times vary from published recommendations.
Learning Objectives • Learning objectives for the presentation. At the conclusion of the presentation, the learner will be able to:
1. Summarize the 2017 ASPEN ILE survey and gap analysis. Key Takeaways/Fast Facts • The results of this survey conducted in late 2016 found a wide variation in practice, particularly
across patient age groups. Conclusion: These findings demonstrate the need for ongoing dissemination and education on standardized safe practices for ILE use.
Learning Assessment Questions
1. Question 2: 2-in-1 PN will have intravenous lipid emulsion (ILE) piggybacked along with the PN. What is the appropriate hang time for ILE when piggybacked with a 2-in-1 PN?
A. 8 hours B. 12 hours C. 18 hours D. 24 hours
Learning Assessment Answers:
1. Answer = B; Rationale: Current recommendations state that ILE within a TNA should have a maximum hang time of 24 hours. Recommendations also state than ILE piggybacked into a 2-in-1 PN solution should have a maximum hang time of 12 hours. Tubing should also be changed every 12 hours when ILE is piggybacked with 2-in-1 PN. These recommendations also state that if ILE is to be infused separately over > 12 hours, the dose should be divided into two parts with a new container and tubing every 12 hours.
References: 1. Christensen ML, Ayers P, Boullata. at.el. Lipid injectable emulsion survey with gap analysis.
NCP. 2017;32(5):694-702.

2017 ASPEN ILE Survey With Gap Analysis
ASPEN 2019 Nutrition Science & Practice Conference
Phil Ayers, PharmD, BCNSP, FASHPChief, Clinical Pharmacy ServicesMississippi Baptist Medical Center
Clinical Associate ProfessorUniversity of Mississippi School of Pharmacy
Jackson, MS
© 2
019
ASPE
N | A
mer
ican
Soc
iety
for
Pare
nter
al a
nd E
nter
al N
utrit
ion.
All R
ight
s R
eser
ved.
Disclosures
• Fresenius Kabi Speakers Bureau
© 2
019
ASPE
N | A
mer
ican
Soc
iety
for
Pare
nter
al a
nd E
nter
al N
utrit
ion.
All R
ight
s R
eser
ved.
Learning Objectives
Upon completion of this session, the learner will be able to….
1. Summarize the 2017 ASPEN Lipid Survey and Gap Analysis.
Lipid Injectable Emulsion Survey With Gap Analysis


ASPEN EDUCATION PROGRAM OUTLINE TEMPLATE Kathleen M Gura, PharmD, BCNSP, Manager Pharmacy Clinical Research Program, Boston Children’s Hospital, Boston MA The Use of Alternative ILEs in the Pediatric Population Disclosures Pharmaceutical advisory board
B Braun Baxter
Consultant B Braun Fresenius Kabi Pfizer Pediatric Center of Excellence Xellia Pharmaceuticals Northsea Therapeutics Alcresta Otsuka Pharmaceutical Factory
Patents/royalties for use of Omegaven Presentation Overview/Summary
For more than 50 years, soybean oil lipid emulsions were the mainstay of therapy in the pediatric patient. In 2016 a mixed oil emulsion was approved for use in adults and 2018 a pure fish oil emulsion became available for pediatric patients with PN associated liver disease. This session will discuss the approved and unapproved uses of these ILEs in pediatric patients and discuss potential the pros and cons of each product.
Learning Objectives At the conclusion of the presentation, the learner will be able to:
1. Understand when lipid restriction protocols can be safely used 2. Discuss the concerns of using a mixed oil IVLE in a pediatric patient 3. List which patients should not receive fish oil monotherapy
Key Takeaways/Fast Facts
1. Pure soybean oil emulsions may be an appropriate alternative to the newer lipid emulsions in certain patients with limited venous access and multiple intravenous medications.
2. Monitoring essential fatty acid status is important in patients receiving an alternative IVLE. 3. Lipid restriction protocols should not be used with alternative IVLEs.
Learning Assessment Questions
Question 1: (True/false) Pure fish oil lipid emulsions contain only omega-3 fatty acids.
A. True B. False
Question 2: According to the Holman Index, biochemical essential fatty acid deficiency occurs then the triene;tetrane ratio is:
A. > 0.05 B. < 0.05 C. >0.2

ASPEN EDUCATION PROGRAM OUTLINE TEMPLATE
D. >0.4
Question 3: (true/false) Pure fish oil emulsions are FDA approved for use in preventing PN associated cholestasis in children.
A. True B. False
Question 4: (true/false) Under the right circumstances, soy/MCT/olive/fish oil lipid emulsions can cause EFAD.
A. True B. False
Question 5: (true/false) Fish oil monotherapy has been shown to be ineffective as a treatment of acetaminophen toxicity.
A. True B. False
Learning Assessment Answers:
1. Answer: B (false). Fish oil contains both omega-3 and omega-6 fatty acids and when dosed appropriately, can provide sufficient essential fatty acids to prevent deficiency.
2. Answer: C. According to the Holman Index, biochemical evidence of EFAD occurs when the triene:tetraene ratio is greater than 0.2. Physical signs occur when the ratio is greater than 0.4. Other laboratory ranges have been used to describe what is observed in healthy individuals eating a typical Western diet.
3. Answer: B (false). Pure fish oil emulsions are only FDA approved as a source of essential fatty acids and calories in children with PN associated cholestasis. It is not approved for preventing PNAC.
4. Answer: A (true). In patients who are totally PN dependent, lower doses of these mixed oil emulsions have been associated with EFAD. Monitoring of EFA status is necessary to ensuring adequate doses are being provided.
5. Answer: A (true) In animal models, fish oil monotherapy has been shown not to be effective in treating the hepatic damage seen with acetaminophen toxicity.
References 1.de Meijer VE, Le HD, Meisel JA, Gura KM, Puder M. Parenteral fish oil as monotherapy prevents essential fatty acid deficiency in parenteral nutrition–dependent patients. J Pediatr Gastroenterol Nutr. 2010;50:212-218. 2.Puder M, Valim C, Meisel JA, et al. Parenteral fish oil improves outcomes in patients with parenteral nutrition–associated liver injury. Ann Surg. 2009;250:395-402. Lee SI, Valim C, Johnston P, et al. Impact of fish oil–based lipid emulsion on serum triglyceride, bilirubin, and albumin levels in children with parenteral nutrition–associated liver disease. Pediatr Res. 2009;66(6):698-703.

ASPEN EDUCATION PROGRAM OUTLINE TEMPLATE 3.Diamond IR, Sterescu A, Pencharz PB, Kim JH, Wales PW. Changing the paradigm: omegaven for the treatment of liver failure in pediatric short bowel syndrome. J Pediatr Gastroenterol Nutr. 2009;48:209-215. 4.de Meijer VE, Gura KM, Meisel JA, Le HD, Puder M. Parenteral fish oil monotherapy in the management of patients with parenteral nutrition– associated liver disease. Arch Surg. 2010;145:547-551. 5.Vanek VW, Seidner DL, Allen P, Bistrian B, Collier S, Gura K, Miles JM, Valentine CJ, Kochevar M; Novel Nutrient Task Force, Intravenous Fat Emulsions Workgroup; American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.) Board of Directors .A.S.P.E.N. position paper: Clinical role for alternative intravenous fat emulsions. Nutr Clin Pract. 2012 Apr;27(2):150-92. 6.Nehra D, Fallon EM, Carlson SJ, Potemkin AK, Hevelone ND, Mitchell PD, Gura KM Puder M. Provision of a Soy-Based Intravenous Lipid Emulsion at 1 g/kg/d Does Not Prevent Cholestasis in Neonates. JPEN J Parenter Enteral Nutr. 2012 Jul 5.

3/8/2019
1
The Use of Alternative ILEs in the Pediatric Population
Kathleen M. Gura Pharm.D., BCNSP, FASHP, FPPAG FASPENCenter for Advanced Intestinal Rehabilitation (CAIR)
Boston Children’s HospitalAssistant Professor of Pediatrics, Harvard Medical School
Disclosures• Pharmaceutical advisory board
– B Braun– Baxter
• Consultant– B Braun– Fresenius Kabi– Pfizer Pediatric Center of Excellence– Xellia Pharmaceuticals– Northsea Therapeutics– Alcresta– Otsuka Pharmaceutical Factory
• Patents/royalties for use of Omegaven
2
Disclosures
A licensing agreement exists between Boston Children’s Hospital & Fresenius Kabi for the use
of Omegaven in PNALD.
I will be discussing off labeled indications and products that are currently not FDA approved.
Learning Objectives
At the end of this session, participants will be able to:
• Understand when lipid restriction protocols can be safely used
• Discuss the concerns of using a mixed oil IVLE in a pediatric patient
• List which patients should not receive fish oil monotherapy
Deciding When to Use Which Lipid Emulsion When…..
Soybean Oils
Recommendation: Based on 2 level 2 studies, in critically ill patients who are not malnourished, are tolerating some EN, or when parenteral nutrition is indicated for short term use (< 10 days), withholding lipids high in soybean oil should be considered.
– insufficient data to make a recommendation about withholding lipids high in soybean oil in critically ill patients who are malnourished or those requiring PN for long term (> 10 days)
www.criticalcarenutrition.com 10.2 Strategies to Optimize Parenteral Nutrition and Minimize Risks: Use of lipids March 2013

3/8/2019
2
Intestinal Failure (IF) • Definition:
– PN dependence > 3 mo. • Over 60% of infants with IF develop
cholestasis (direct Bilirubin > 2 mg/dL)– Before 2004:mortality was 37.5% due
to liver failure and or sepsis (Boston Children’s Hospital)
– 78% mortality if bilirubin >3 mg/dL for 3 months
– Approach 90% mortality if cholestasis and remain on PN for > 1 year
– 1.4% of all deaths of children 4 years of age and under
Prevention of IFALD
Impact of Soybean Lipid Dose
Lipid Restriction 1g/kg/dayRollins et al J Pediatr Surg. 2013 Jun;48(6):1348-56
• Pilot study n=28• Prospective RCT• Infants > 26 weeks GA on >50%
total calories from PN• Compared 1g/kg/d to 3g/kg/d • Results:
– Ave PN duration 5.4 weeks– Tot increase in dbili from baseline
less in low dose group (p=0.04)– Weight z-score increased more in
3g/kg/d group– No EFAD
• CONCLUSION:– Markers of cholestasis rose at a
slower rate using 1g/kg/d IFE
Prophylactic Lipid Restriction 1g/kg/day
Sanchez et al J Pediatr Surg. 2013 Mar;48(3):573-8
• Surgical neonates (n=82) receiving 1g/kg/d retrospectively compared to control cohort (2g/kg/d) (n=132)
• Results: PNLAD less in 1g/kg/d group (22% vs. 43% p=0.003)
• Omegaven rescue used in 4 infants in standard dose vs. 2 infants in low dose group
Severe Lipid RestrictionCurrent Opinion in Organ Transplantation 2010,
15:330–333
• Protocol:– 1 g/kg/d twice weekly
– If EFAD develops: 1g/kg/day 3x/week
• If the EFAD persists: 2g/kg/day 3x/week
• Preliminary results indicate IFE restriction resulted in a statistical significant reduction in total bilirubin without impacting growth or causing EFAD

3/8/2019
3
• Multicenter study RCT
• 136 neonates <48 hrs of age randomized to low (1 g/kg/d, n=67) or high dose (~3g/kg/d n=69) SO
• Results– no difference in PNALD (69% vs 63%; 95% confidence interval, -
0.1 to 0.22; P = 0.45)
– weight, length, and head circumference at 28 DOL, discharge, and over time were not different (P > 0.2 for all)
• Conclusion: Compared with the control dose, low-dose SO was not associated with a reduction in PNALD or growth
BCH Experience:Intralipid Dose and Cholestasis
• Retrospective chart review: All patients who received PN/IL in the NICU at BCH between January 2007 – June 2011
• Inclusion Criteria– Age <2months at PN/IL initiation– On IL for at least 3 weeks at CHB– No PN/IL prior to transfer to CHB– Gastrointestinal surgical condition as indication for PN/IL
• Exclusion Criteria– Multisystem organ failure– Inconsistent IL dosing
1g/kg/day IL group
2-3 g/kg/day IL group
Nehra et al JPEN 2013 Jul;37(4):498-505
Patient characteristics while on parenteral nutrition
What About Switching the ILE Type?
16
Safety and efficacy of Fish Oil Based Lipid Emulsion in the Prevention of PNALD
a double-blind randomized controlled clinical trial to compare Soybean oil to Fish oil at 1g/kg/day
• Primary outcome:– Incidence PNLAD
• Secondary outcomes:
– Safety
- Growth
- Infection risk
- EFA status
- Neurodevelopment
• Inclusion Criteria:– <3mo at enrollment
– Baseline d bili <1
– Expected PN > 21 days
• Exclusion criteria:– Shock
– Severe hemolytic disorder
– Baseline triglyceride >400 mg/dL
– Prior exposure to intravenous fat emulsion
Primary Outcome:Incidence of cholestasis
Median Weekly Direct BilirubinOM group
Week
Dir
ect
bili
rub
in
(mg
/dL
)
0 1 2 3 4 5 6 7 8 9 100
2
4
6
8
10
Median Weekly Direct BilirubinIL group
Week
Dir
ect
bili
rub
in
(mg
/dL
)
0 1 2 3 4 5 6 7 8 9 100
2
4
6
8
10
Soybean Oil Fish Oil
No difference in weekly median bilirubin values between groups
Nehra, et al.JPEN J Parenter Enteral Nutr June 14, 2013

3/8/2019
4
Secondary Outcomes:Growth
-2.5
-2
-1.5
-1
-0.5
0
0 1 2 3 4 5 6
Week
Me
dia
n W
eig
ht-
for-
ag
e Z
-sc
ore
Fish Oil
Soybean Oil
P=0.72
Secondary Outcomes:Infection rate
Soybean Oil(n=10)
Fish Oil (n=9)
Total # positive blood cultures
5 7
Total # positive stool cultures
2 2
Total # positive sputum cultures
1 0
Secondary Outcomes:Neurodevelopment
Soybean Oil Fish Oil P-value24 month Bayley
Cognitive
Language
Motor
95
106
99
93
111
101
0.76
0.56
0.76
24 month PARCA-R*
Cognition
Linguistic skills
Composite Score
26
33
59
29
77
98
1.00
0.30
0.30
*PARCA-R: Parent Reports of Child’s Abilities
Conclusions from the pilot study . . .
No adverse effects:
‐Growth‐Infection rate‐Fatty acid profiles‐Neurodevelopment
No difference in the incidence of cholestasis
Treatment of IFALD
Fish Oil Monotherapy
• Dose: 1g -1.5 g/kg/day
• All soy containing IFE discontinued
• Efficacy:– Boston (historical controls)
– LA (historical controls)
– Texas (historical controls)
– Hong Kong (prospective RCT)

3/8/2019
5
Direct Bilirubin
0 4 8 12 16 20 24 28 32 36
05
1015
05
Weeks from Baseline
Dir
ect
Bili
rubi
n (m
g/dL
) P < 0.0001
Soybean oil
Fish oil
•Parameter # 1: direct bilirubin; 80-125% of the value of the potential pair was tolerated
•Parameter # 2: Age at baseline; ± 28-day range was accepted for the potential pair
•Parameter # 3: Gestational age; 90-110% of the value of the potential pair was accepted
31 patients were included in the analysis and matched according to the above mentioned criteria
Boston ExperiencePair-Matching Analysis
Methodology
Results of Pair Matching
Hong Kong RCTNeonatology 2014;105:290-296
• 1.5 g/kg/day for both IFE
• 16 infants (FO n=9, SO n=7)
• no significant difference in reversal of IFALD at 4 months between groups– Rates of increase of Dbili &
ALT in SO group > FO group
• 13.5 vs.0.6 µmol/l/wk and 9.1 vs. 1.1 IU/l/wk (p = 0.03)
– ↑ EN associated with significant improvement of IFALD in FO group compared to SO
• Rate of increase of direct bilirubin in the SO group significantly higher than in the FO group (p = 0.03)
• ALT significantly worsened, increasing by 9.1 IU/l per week in the SO group (p < 0.01) but not in the FO group (1.1 IU/l per week, p = 0.71)
• Rate of increase of ALT in the SO group significantly greater than in the FO group (p = 0.02).
How long should you remain on fish oil monotherapy?

3/8/2019
6
Long-Term Outcomes in Children With Intestinal Failure-Associated Liver Disease Treated With 6
Months of Intravenous Fish Oil Followed by Resumption of Intravenous Soybean Oil
(JPEN J Parenter Enteral Nutr. 2018 Nov 8)
• Children treated who resumed SO after FO; prospectively followed for 4.5 years or until death, transplant, or PN stop
• 1°outcome cumulative incidence rate IFALD return
• 48 subjects
– 71% IFALD resolution after 6 mo.
– 27 resumed SO
• IFALD 26%
• Transplant 6% 31
Omegaven isn’t a wonder drug…..
Predictors of Intravenous Fish Oil (Omegaven®) Failure in the
Treatment of Parenteral Nutrition-Associated Liver Disease
Am J Clin Nutr. 2016 Sep;104(3):663-70.
Study Design
Retrospective review of prospectively collected data for patients started on FO (Omegaven®) therapy at BCH from January 2004 to December 2014.
• Inclusion criteria: – All patients with PNALD who received at least 1 dose of FO
therapy from January 1, 2004 to December 31, 2014
• Exclusion criteria:– Patients who started FO at outside institution
– Patients who are still cholestatic (only included patients who have either failed or reversed)
• 85.7% cholestasis reversed (156/182)
• 14.3% failed FO therapy (26/182)– 8 transplants (6 multivisceral, 2 liver)
– 18 deaths
• 16.9% of pts transferred from OSH with PNALD vs. 9.4% of pts who developed PNALD at BCH failed FO therapy.– 20/118 [16.9%] vs. 6/64 [9.4%], P=0.16
35
Results
Am J Clin Nutr. 2016 Sep;104(3):663-70.
Results
• Patients who failed therapy had more advanced biochemical liver disease at time of FO initiation:– Lower GGT, platelets; Higher DB, INR, PELD
• Patients who failed therapy had higher rates (than
patients whose cholestasis resolved) of:– History of GI bleeding
– Mechanical ventilation &/or sepsis at time of FO initiation
– Neurologic, genetic/chromosomal, or endocrine comorbidity at FO initiation
36
Am J Clin Nutr. 2016 Sep;104(3):663-70.

3/8/2019
7
Independent Predictors of Treatment Failure
37
PELD = 4.8[ln(TB)] + 18.57[ln(INR)] – 6.87[ln(albumin)] + 4.36 (if age <1 yr) + 6.67 (if growth failure)
Reversed(n=128)
Treatment failure(n=20)
P OR (95% CI)
Baseline PELD score ≥ 15
30 (23%) 13 (65%) 0.005 4.7 (1.6, 13.9)
History of GI bleed 22 (17%) 9 (45%) 0.006 4.6 (1.5, 13.8)
Patient age ≥16 weeks at FO initiation
47 (37%) 14 (70%) 0.004 5.5 (1.7, 17.5)
Ventilator at FO initiation
16 (13%) 7 (35%) 0.002 6.8 (2.1, 22.5)
Am J Clin Nutr. 2016 Sep;104(3):663-70.
Lessons learned…• Patients who failed therapy were older and
had more advanced biochemical and clinical liver disease at FO initiation.– However, many patients with similar labs and
acuity responded to FO therapy.
• Early initiation of FO therapy once biochemical cholestasis is detected in PN-dependent patients is recommended. – 85 pts since 2011: 3 deaths, 1 LTx
• Reversibility of PNALD cannot be reliably determined.
38
Patients who shouldn’t be treated with Omegaven….
39
Acetaminophen Toxicity
Animals fed a fish oil-based diet were more susceptible, rather than resistant, to APAP-induced hepatotoxicity
40
JPEN J Parenter Enteral Nutr. 2013 Mar;37 (2):268-73.
Other Approaches
• SMOFlipid
• 50/50 blend FO + SO
• Reduced dose SO
SMOFlipid• Birmingham Children’s
• Case series infants/ children with PNALD while on SO & switched to SMOFlipid (n=8)
• 1 patient died, 1 listed for transplant
• Remaining 6: “sudden, often dramatic and sustained fall in bilirubin 1-3 months after switching to SMOFlipid”
Source:Protheroe/Murphy

3/8/2019
8
Concerns with SMOFlipid
• Not FDA approved in children
• Dosing important
• Low doses– Cause EFAD
• Higher doses– no hepatoprotective
benefits
43
Authors Study Design Cohort Lipid dose Length of time
Outcomes
Goulet et al (2010)
Single-center, prospective, randomized, double-blind study comparing SMOFlipid to SOLE
28 children (5 month - 11 years) on home PN at least 4 weeks with short bowel syndrome, chronicintestinal pseudo-obstruction, or congenital disease of GI mucosa
2 g/kg/day 29 d • Total bilirubin• ω-3 fatty acids• Lipid peroxidation• Plasma α-tocopherol
*Safe and well tolerated, decreased liver
enzymes/bilirubin
Tomsits et al(2010)
Prospective, randomized, double-blind trial comparing SMOFlipid to SOLE
60 premature neonates (age 3-7 days, gestational age ≤ 34 weeks, birth weights 1000-2500 g) on PN for minimum 7 -14 days.
0.5 g/kg/day day 1Increased by
0.5 g/kg/day up to 2 g/kg/day
7-14 d • Triglyceride levels• GGT levels• ω-6 to ω-3 ratio• Plasma α-tocopherol• Liver enzymes
*Safe and well tolerated, decreased GGT, consistent with
maintained liver fxn
Rayyan et al(2012)
Prospective, double blind, randomized trial comparing SMOFlipid to SOLE
53 neonates (<34 week gestation, birth weight 500-2000g) on PN x 7 days minimum
1 g/kg/day days 1-32 g/kg/day day 43 g/kg/day day 53.5 g/kg/day day 6-14
7-14 d • Total and direct bilirubin• Triglyceride levels• ω-6 to ω-3 ratio
*Safe and well tolerated, increase EPA & DHA, decreased GGT & DB
Diamond et al(2017)
Pilot, multicenter, prospective, randomized, blinded trial comparing SMOFlipid to SOLE
24 infants (<24 months) with short bowel syndrome or intestinal failure with hyperbilirubinemia on PN
1-3 g/kg/day 8 wks • Serum conjugated bilirubinSMOFlipid reduces the risk
of progressive IFALD in children with intestinal
failure
Repa et al(2017)
Prospective, single-center, double-blind randomized control trial comparing SMOFlipid to SOLE
230 ELBW infants (birth weight <1000g) on PN
3 g/kg/day 15-35 d • Serum conjugated bilirubin• Triglyceride levels • Liver enzymes
*Incidence of IFALD not decreased, no effect on ROP, no difference in hypertriglyceridemia
Authors Study Design Cohort Lipid dose Length of time
Outcomes
Goulet et al (2010)
Single-center, prospective, randomized, double-blind study comparing SMOFlipid to SOLE
28 children (5 month - 11 years) on home PN at least 4 weeks with short bowel syndrome, chronicintestinal pseudo-obstruction, or congenital disease of GI mucosa
2 g/kg/day 29 d • Total bilirubin• ω-3 fatty acids• Lipid peroxidation• Plasma α-tocopherol
*Safe and well tolerated, decreased liver
enzymes/bilirubin
Tomsits et al(2010)
Prospective, randomized, double-blind trial comparing SMOFlipid to SOLE
60 premature neonates (age 3-7 days, gestational age ≤ 34 weeks, birth weights 1000-2500 g) on PN for minimum 7 -14 days.
0.5 g/kg/day day 1Increased by
0.5 g/kg/day up to 2 g/kg/day
7-14 d • Triglyceride levels• GGT levels• ω-6 to ω-3 ratio• Plasma α-tocopherol• Liver enzymes
*Safe and well tolerated, decreased GGT, consistent with
maintained liver fxn
Rayyan et al(2012)
Prospective, double blind, randomized trial comparing SMOFlipid to SOLE
53 neonates (<34 week gestation, birth weight 500-2000g) on PN x 7 days minimum
1 g/kg/day days 1-32 g/kg/day day 43 g/kg/day day 53.5 g/kg/day day 6-14
7-14 d • Total and direct bilirubin• Triglyceride levels• ω-6 to ω-3 ratio
*Safe and well tolerated, increase EPA & DHA, decreased GGT & DB
Diamond et al(2017)
Pilot, multicenter, prospective, randomized, blinded trial comparing SMOFlipid to SOLE
24 infants (<24 months) with short bowel syndrome or intestinal failure with hyperbilirubinemia on PN
1-3 g/kg/day 8 wks • Serum conjugated bilirubinSMOFlipid reduces the risk
of progressive IFALD in children with intestinal
failure
Repa et al(2017)
Prospective, single-center, double-blind randomized control trial comparing SMOFlipid to SOLE
230 ELBW infants (birth weight <1000g) on PN
3 g/kg/day 15-35 d • Serum conjugated bilirubin• Triglyceride levels • Liver enzymes
*Incidence of IFALD not decreased, no effect on ROP, no difference in hypertriglyceridemia
SMOFlipid failed to reverse IFALD
• Korea
• Case reports (n=2)– Received 2-3 g/kg/d
SMOFlipid
– IFALD developed
• IFALD reversed upon discontinuing SMOFlipid and switching to Omegaven monotherapy
46
Essential Fatty Acid Status in Surgical Infants Receiving Parenteral Nutrition With a Composite
Lipid Emulsion: A Case Series(JPEN J Parenter Enteral Nutr. 2018 May 30)
• 4 infants receiving SMOFlipid® as their IV lipid source
– essential fatty-acid status, triglycerides, and dosing strategy reviewed
• Conclusions– May render infants at risk for EFAD.
• Should be dosed appropriately to prevent EFAD
– Hypertriglyceridemia and cholestasis are known adverse effects and require monitoring
47
Essential Fatty Acid Status in Surgical Infants Receiving Parenteral Nutrition With a Composite Lipid Emulsion: A Case Series
Essential Fatty Acid Status in Surgical Infants Receiving Parenteral Nutrition With a Composite Lipid Emulsion: A Case Series, First published: 30 May 2018, DOI: (10.1002/jpen.1311)

3/8/2019
9
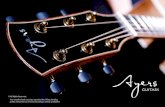
Triglyceride and Direct Bilirubin Levels
Essential Fatty Acid Status in Surgical Infants Receiving Parenteral Nutrition With a Composite Lipid Emulsion: A Case Series, First published: 30 May 2018, DOI: (10.1002/jpen.1311)
50/50 FO + SOJ Pediatr Gastroenterol Nutr. 2009 Feb;48(2):209-15
• Canada
• 12 patients with PNALD
• 1g/kg/d SO + 1g/kg/d FO
• 5 cases, hepatic dysfunction while on the blended regimen progressed until Intralipid® stopped and Omegaven® was given alone
• Complete resolution of PNALD occurred in 9 patients (75%)
Control: 3 g/kg/d, Intervention: 1 g/kg twice weekly, n = 31 each group
Results:
42% resolution (fat reduction)
10% resolution control group
Cober et al, J Pediatr 2012;160:421-7
SOY LIPID RESTRICTIONJ Pediatr. 2012 Mar;160(3):421-7.
Putting it all together….
52
Pros and Cons Soybean Oil ILE
• Pros– 50+ years of experience
– 1g/kg/day does not cause EFAD
– Lots of compatibility information
• Cons– High risk of IFALD
– Rich in phytosterols, omega-6 fatty acids
– Low in alpha-tocopherol
53
Pros and ConsFish Oil ILE
• Pros– Improves hepatic function in IFALD
– Rich in omega-3 fatty acids, alpha-tocopherol
– Low in phytosterol content
• Cons– Need at least 1g/kg/day to prevent EFAD
– 10% emulsion
– Little compatibility information
54

3/8/2019
10
Pros and ConsSoy-MCT-Olive-Fish ILE
Pros
-20% emulsion
-can use to reduce GIR
-contains MCT – more stable TNAs
Cons
-3g/kg/d = 1g/kg/day soybean ILE
-not approved for use in pediatric patients
-limited compatibility data
-dose low: EFAD, dose high: IFALD
55
Gura’s Thoughts
• New start – Intralipid or SMOFlipid at age appropriate
doses (i.e., 3g/kg/day if neonate)
• Limited vascular access/lots of IV meds– Intralipid 1g/kg/day
• Need to reduce GIR, no IFALD present– SMOFlipid
• IFALD – Omegaven
56
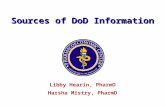
4 Lipid Emulsions Oil Red-O
CHOW PN + IL
PN + SMOF PN + OM
PN +ClinOleic ®
Meisel JA et al Journal of Pediatric Surgery 2011; 46:666-673
There is no ideal ILEMonitoring is essential!
58
Never assume….
59 60

3/8/2019
11
61
References• Waitzberg DL, Torrinhas RS, Jacintho TM. New parenteral lipid emulsions for
clinical use. JPEN J Parenter Enteral Nutr. 2006;30:351-367.
• Le HD, Meisel JA, de Meijer VE, Gura KM, Puder M. The essentiality of arachidonic acid and docosahexaenoic acid. Prostaglandins Leukot Essent Fatty Acids. 2009;81:165-170.
• Serhan CN. Controlling the resolution of acute inflammation: a new genus of dual anti-inflammatory and proresolving mediators. J Periodontol. 2008;79(8)(suppl):1520-1526.
• Serhan CN, Chiang N, Van Dyke TE. Resolving inflammation: dual anti-inflammatory and pro-resolution lipid mediators. Nat Rev Immunol. 2008;8:349-361.
• Serhan CN, Yacoubian S, Yang R. Anti-inflammatory and pro-resolving lipid mediators. Annu Rev Pathol. 2008;3:279-312.
• Driscoll DF. Lipid injectable emulsions: 2006. Nutr Clin Pract. 2006;21: 381-386.
• Bach AC, Frey A, Lutz O. Clinical and experimental effects of medium chain-triglyceride-based fat emulsions—a review. Clin Nutr. 1989;8: 223-235.
• Bockus HL, Sarett HP, Hashim SA, Anderson CM, Isselbacher KJ, Jeffries
• GH. Panel discussion of practical problems in usage of medium chain triglycerides. In: Senior JR ed. Medium Chain Triglycerides. Philadelphia:University of Pennsylvania Press, 1968:193.
References• Pianese P, Salvia G, Campanozzi A, et al. Sterol profiling in red blood cell
membranes and plasma of newborns receiving total parenteral nutrition. J Pediatr Gastroenterol Nutr. 2008;47:645-651.
• Ling WH, Jones PJ. Dietary phytosterols: a review of metabolism, benefits and side effects. Life Sci. 1995;57:195-206.
• Ostlund RE Jr, McGill JB, Zeng CM, et al. Gastrointestinal absorption and plasma kinetics of soy Delta(5)-phytosterols and phytostanols in humans. Am J Physiol Endocrinol Metab. 2002;282:E911-E916.
• Ball MJ. Parenteral nutrition in the critically ill: use of a medium chain triglyceride emulsion. Intensive Care Med. 1993;19:89-95.
• Jiang ZM, Zhang SY, Wang XR, Yang NF, Zhu Y, Wilmore D. A comparison of medium-chain and long-chain triglycerides in surgical patients. Ann Surg. 1993;217:175-184.
• Socha P, Koletzko B, Demmelmair H, et al. Short-term effects of parenteral nutrition of cholestatic infants with lipid emulsions based on medium chain and long-chain triacylglycerols. Nutrition. 2007;23:121-126.
• Lehner F, Demmelmair H, Röschinger W, et al. Metabolic effects of intravenous LCT or MCT/LCT lipid emulsions in preterm infants. J Lipid Res. 2006;47:404-411.
References• de Meijer VE, Le HD, Meisel JA, Gura KM, Puder M. Parenteral fish oil as
monotherapy prevents essential fatty acid deficiency in parenteral nutrition–dependent patients. J Pediatr Gastroenterol Nutr. 2010;50:212-218.
• Puder M, Valim C, Meisel JA, et al. Parenteral fish oil improves outcomes in patients with parenteral nutrition–associated liver injury. Ann Surg. 2009;250:395-402.
• Lee SI, Valim C, Johnston P, et al. Impact of fish oil–based lipid emulsion on serum triglyceride, bilirubin, and albumin levels in children with parenteral nutrition–associated liver disease. Pediatr Res. 2009;66(6):698-703.
• Diamond IR, Sterescu A, Pencharz PB, Kim JH, Wales PW. Changing the paradigm: omegaven for the treatment of liver failure in pediatric short bowel syndrome. J Pediatr Gastroenterol Nutr. 2009;48:209-215.
• de Meijer VE, Gura KM, Meisel JA, Le HD, Puder M. Parenteral fish oil monotherapy in the management of patients with parenteral nutrition– associated liver disease. Arch Surg. 2010;145:547-551.
• Vanek VW, Seidner DL, Allen P, Bistrian B, Collier S, Gura K, Miles JM, Valentine CJ, Kochevar M; Novel Nutrient Task Force, Intravenous Fat Emulsions Workgroup; American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.) Board of Directors .A.S.P.E.N. position paper: Clinical role for alternative intravenous fat emulsions. NutrClin Pract. 2012 Apr;27(2):150-92.
• Nehra D, Fallon EM, Carlson SJ, Potemkin AK, Hevelone ND, Mitchell PD, Gura KM
Puder M. Provision of a Soy-Based Intravenous Lipid Emulsion at 1 g/kg/d Does Not
Prevent Cholestasis in Neonates. JPEN J Parenter Enteral Nutr. 2012 Jul 5.

ASPEN EDUCATION PROGRAM OUTLINE TEMPLATE Name, Title, Affiliation Todd W Mattox, PharmD, BCNSP; Medicine/Surgery Clinical Pharmacist Moffitt Cancer Center; Tampa, Florida Presentation Title ILE: Does and Don’ts- The Utility of Alternative ILEs in the Adult Population Disclosures I have a commercial relationship with Fresenius Kabi as a consultant. I will not include any practice recommendations and will address only evidence-based science in my presentation Presentation Overview/Summary • Data and recommendations for use of mixed oil intravenous lipid emulsion (IVLE) in adults are not
clear. A large portion of the currently available data is based on investigations of formulations that were previously only available in Europe. In addition, the heterogeneity between published investigations further complicates evaluation of clinical use. Multiple meta-analyses have been conducted to evaluate the clinical utility of mixed oil IVLE and have reported conflicting results. Mixed oil IVLE has been reported to have a positive impact on a variety of important clinical outcomes. This case report will focus on the use of mixed oil IVLE in a critically ill patient with impaired triglyceride clearance.
Learning Objectives At the conclusion of the presentation, the learner will be able to: 1. Summarize current evidenced based considerations for use of alternative IVLE in adult patients
who require PN support 2. Explain the role of a 4-oil IVLE formulation in a critically ill adult patient with hypertriglyceridemia
Key Takeaways/Fast Facts • Data and recommendations for use of mixed oil intravenous lipid emulsion (IVLE) in adults are not
clear • Data from previous investigations of alternative IVLE in patients requiring PN support have
demonstrated a positive effect on triglyceride clearance
Learning Assessment Questions
1. Four-oil intravenous lipid emulsions have been investigated for potential clinical advantages including
a. Stabilization of 3-in-1 PN solutions b. Prevention of micronutrient deficiencies associated with injectable soybean emulsions c. Improved triglyceride clearance d. Enhance carnitine metabolism in pediatric patients

ASPEN EDUCATION PROGRAM OUTLINE TEMPLATE
2. Factors contributing to conflicting recommendations for routine clinical use of alternative IVLE in adults include
a. Lack of comparative studies between specific IVLE formulations b. Inconsistent sources & doses of omega-3 fatty acids utilized in investigations c. Lack of heterogeneity between published investigations d. All of the above
Learning Assessment Answers:
1. Answer = C; SMOF lipid has demonstrated improved triglyceride clearance which is thought to be related to the medium chain triglyceride component
2. Answer = D; Clinical use of alternative IVLE in adults is not clear for a variety of reasons but primarily due to lack of heterogeneity between published investigations, lack of comparative studies between specific IVLE formulations and inconsistent sources and doses of omega-3 fatty acids utilized in investigations.
References
1. Kreymann KG, Heyland DK, de Heer G, Elke G. Intravenous fish oil in critically ill and surgical patients-historical remarks and critical appraisal. Clin Nutr 2018; 37:1075-1081
2. Bae HJ, Young G, Seong JM, Gwak HS. Outcomes with perioperative fat emulsions containing omega-3 fatty acid: A meta-analysis of randomized controlled trials Am J Health-Syst Pharm. 2017;74:904-918.
3. Mateu-de Antonio J, Florit-Sureda M. New strategy to reduce hypertriglyceridemia during parenteral nutrition while maintaining energy intake. JPEN J Parenter Enteral Nutr 2016;40:705-712.
4. Zaloga GP. Phytosterols, lipid administration, and liver disease during parenteral nutrition. JPEN J Parenter Enteral Nutr. 2015;39(suppl 1):39S-60S
5. Antébi H, Mansoor O, Ferrier C, et al. Liver function and plasma antioxidant status in intensive care unit patients requiring total parenteral nutrition: comparison of 2 fat emulsions. JPEN J Parenter Enteral Nutr. 2004;28:142-148.

The Utility of Alternative ILEs in the Adult Population
ILE: Does and Don’ts
ASPEN 2019 Nutrition Science & Practice Conference
Todd W Mattox, PharmD, BCNSPMedicine/Surgery Clinical Pharmacist
Moffitt Cancer CenterTampa, Florida
© 2
019
ASPE
N | A
mer
ican
Soc
iety
for
Pare
nter
al a
nd E
nter
al N
utrit
ion.
All R
ight
s R
eser
ved.
Disclosures
• I have a commercial relationship with Fresenius Kabi as a consultant. I will not include any practice recommendations and will address only evidence-based science in my presentation.
© 2
019
ASPE
N | A
mer
ican
Soc
iety
for
Pare
nter
al a
nd E
nter
al N
utrit
ion.
All R
ight
s R
eser
ved.
Learning Objectives
Upon completion of this session, the learner will be able to….
1. Summarize current evidenced based considerations for use ofalternative IVLE in adult patients who require PN support
2. Explain the role of a 4-oil IVLE formulation in a critically ill adult patientwith hypertriglyceridemia
Clinical Use of Mixed IVLE in Adults
• IVLE provide a source of concentrated calories and essential fatty acids (FA)
• The oil source of IVLE influences cellular FA content which impacts a variety of metabolic processes such as essential FA status, cytokine production, triglyceride clearance and liver function in pts receiving PN
• The clinical relevance of oil-dependent metabolic changes associated with IVLE use in adult pts receiving PN is not clear
• Lack of comparative studies between specific formulations
Clinical Use of Mixed IVLE in Adults
• Heterogeneity between published investigations• Patient populations; Small sample sizes• Types of controls• Sources & doses of omega-3 FA• Biochemical and clinical end points
• Conflicting recommendations from a variety of sources• International Professional Nutrition Societies acknowledge a role for
lower ω-6: ω-3 IVLE• ASPEN, ESPEN, Canadian Critical Care Nutrition
Clinical Use of Mixed IVLE in Adults
• Areas Investigated for Clinical Advantages
▪ Mortality & ventilation days in critically-ill▪ Infectious complications▪ ICU length of stay▪ Effect on Markers of Inflammation▪ PN associated liver disease▪ Serum triglyceride clearance

Clinical Use of Mixed IVLE in Adults
• Areas Investigated for Clinical Advantages
▪ Mortality & ventilation days in critically-ill▪ Infectious complications▪ ICU length of stay▪ Effect on Markers of Inflammation▪ PN associated liver disease▪ Serum triglyceride clearance
MCC Criteria for Use: SMOF Lipid
▪ Critically ill patients requiring PN
▪ Patients who require PN support after HSCT
▪ Patients receiving SO-IVLE who develop hypertriglyceridemia
▪ Patients receiving SO IVLE who develop severe liver dysfunction
© 2
019
ASPE
N | A
mer
ican
Soc
iety
for
Pare
nter
al a
nd E
nter
al N
utrit
ion.
All R
ight
s R
eser
ved.
Patient Case Study: Adult Critical Care➢ 52 yo woman with recurrent metastatic mucinous adenocarcinoma of
sigmoid colon cancer with peritoneal involvement admitted for cytoreductivesurgery, hyperthermic intraperitoneal chemotherapy (HIPEC), bilateral ureteral stent placement and hernia repair.
• Pts cytoreductive surgery included greater omenectomy, multiple peritonectomies for tumor removal, splenectomy and distal pancreatectomy, capsular lesion resections, small bowel resection and subsequent heated mitomycin intraperitoneal chemotherapy
➢POD 2 Transfer to ICU for further management of hypoxia requiringheated high flow nasal cannula oxygen
© 2
019
ASPE
N | A
mer
ican
Soc
iety
for
Pare
nter
al a
nd E
nter
al N
utrit
ion.
All R
ight
s R
eser
ved.
Patient Case Study: Adult Critical Care
➢POD 8 Nutrition Intervention• Conservative approach with PN was chosen in view of suspected
pancreatic leak in setting of respiratory instability which was determined to be an unacceptable risk factor for bedside feeding tube placement
Anthropometrics
• Wt: 108 kg• Ht: 160 cm• IBW: 52.2 kg• BMI: 42 kg/m2
Goal PN Regimen
• AA: 130 gm/day• Dex: 300 gm/day
- Electrolytes, MVI, TE• IVLE: SO-IVLE 20% 250 mL/day
Est. Daily Requirements
• Calories: 1700 (approx; Mifflin St Jeor)
• Protein: 105-130 g
© 2
019
ASPE
N | A
mer
ican
Soc
iety
for
Pare
nter
al a
nd E
nter
al N
utrit
ion.
All R
ight
s R
eser
ved.
➢POD 38 Development of intra-abdominal abscesses and peritonitis requiring return to the operating room for exploratory laparotomy, abdominal washout, and adhesiolysis at multiple sites.
• Post operatively, patient developed hypoxia and respiratory failurerequiring mechanical ventilation and hypotension requiring vasopressor support
• Dexmedetomidine was initiated for ICU sedation, which was later changed to propofol
Patient Case Study: Adult Critical Care
© 2
019
ASPE
N | A
mer
ican
Soc
iety
for
Pare
nter
al a
nd E
nter
al N
utrit
ion.
All R
ight
s R
eser
ved.
Days of PN Therapy
Triglyceride Levelmg/dL
ILE Source Notes
1 292 SO-IVLE4 18411 16218 29725 21539 288 SO-IVLE Return to OR;
dexmedetomidine46 352 SO-IVLE + propofol Dexmedetomidine changed
to Propofol48 311 Propofol
Receiving approx. 70 gm/day SO-IVLE
SO-IVLE held
50 Propofol Dc’d; SMOFlipid 20% 250 mL added to PN regimen
53 230 SMOFlipid60 16267 243

© 2
019
ASPE
N | A
mer
ican
Soc
iety
for
Pare
nter
al a
nd E
nter
al N
utrit
ion.
All R
ight
s R
eser
ved.
Days of PN Therapy
Triglyceride Levelmg/dL
ILE Source Notes
1 292 SO-IVLE4 18411 16218 29725 21539 288 SO-IVLE Return to OR;
dexmedetomidine46 352 SO-IVLE + propofol Dexmedetomidine changed
to Propofol48 311 Propofol
Receiving approx. 70 gm/day SO-IVLE
SO-IVLE held
50 Propofol Dc’d; SMOFlipid 20% 250 mL added to PN regimen
53 230 SMOFlipid60 16267 24373 Pt expired
© 2
019
ASPE
N | A
mer
ican
Soc
iety
for
Pare
nter
al a
nd E
nter
al N
utrit
ion.
All R
ight
s R
eser
ved.
Summary
• Data from previous investigations of alternative IVLE in patients requiring PN support have demonstrated a positive effect on triglyceride clearance
• This case illustrates an association with use of an alternative IVLE containing Soybean oil, MCT oil, Olive oil and Fish oil with improvement in triglyceride concentrations in a complicated critically ill patient receiving PN
© 2
019
ASPE
N | A
mer
ican
Soc
iety
for
Pare
nter
al a
nd E
nter
al N
utrit
ion.
All R
ight
s R
eser
ved.
References
1. Kreymann KG, Heyland DK, de Heer G, Elke G. Intravenous fish oil in critically ill and surgical patients-historical remarks and critical appraisal. Clin Nutr 2018; 37:1075-1081
2. Bae HJ, Young G, Seong JM, Gwak HS. Outcomes with perioperative fat emulsions containing omega-3 fatty acid: A meta-analysis of randomized controlled trials Am J Health-Syst Pharm.2017;74:904-918.
3. Mateu-de Antonio J, Florit-Sureda M. New strategy to reduce hypertriglyceridemia during parenteral nutrition while maintaining energy intake. JPEN J Parenter Enteral Nutr2016;40:705-712.
4. Zaloga GP. Phytosterols, lipid administration, and liver disease during parenteral nutrition.JPEN J Parenter Enteral Nutr. 2015;39(suppl 1):39S-60S
5. Antébi H, Mansoor O, Ferrier C, et al. Liver function and plasma antioxidant status in intensive care unit patients requiring total parenteral nutrition: comparison of 2 fat emulsions. JPEN JParenter Enteral Nutr. 2004;28:142-148.
Questions [email protected]

ASPEN EDUCATION PROGRAM OUTLINE TEMPLATE Name, Title, Affiliation Jay M Mirtallo, MS, RPh, BCNSP, FASHP, FASPEN, Clinical Practice Specialist, The American Society for Parenteral and Enteral Nutrition and Professor Emeritus, The Ohio State University, College of Pharmacy Presentation Title Overview and History of ILEs Available in the United States Disclosures I have a commercial relationship with Fresenius Kabi as a member of speaker’s bureau and consultant. I also consult with Coram Home Infusion, MedEdicus and Wolters Kluwer. I will provide practice recommendations that are based on formal structured review of the literature and will state inclusion and exclusion criteria. Presentation Overview/Summary Clinicians have had over 4 decades experience with Soy based ILE. Along this journey, there have been many issues with ILE use that needed to be addressed. ILE is a complex formula that has physico-chemical properties that present issues with stability and compatibility. Although an excellent source of essential fatty acids, Soy ILE is scrutinized for its usefulness as an energy source and its role in physiologic processes related to immunity, infection, coagulation and stress. The safety of Soy ILE is dependent on daily dose, infusion rate, duration of therapy and administration method. This led to the evolution of ILE products not commercially available in the United States until recently. In our quest to find ILE that have a lower content of omega-6 fatty acids, a reliable source of omega-3 fatty acids and an efficient energy source, we now have ‘alternative’ ILE available to consider. Its an exciting time for PN therapy due to the approval of the ‘alternative’ ILEs and the discussion of if, when and how these will be put into use. Learning Objectives At the conclusion of the presentation, the learner will be able to:
1. Discuss the variables to consider when selecting ILE products for use in practice 2. State the advantages of ILE over dextrose as a PN calorie source 3. Describe the characteristics of the various oils used in ILE products 4. Compare the compositional difference in ILE products available in the US
Key Takeaways/Fast Facts Variables to consider when selecting ILE products for use in practice
• Cost • Stability • Compatibility • Metabolism • Oxidized for energy • Free radical production • Triglyceride clearance • Administration: as TNA or separate infusion, multi-chamber product • Physiologic impact on immunity, infection, coagulation and stress response
Learning Assessment Questions 1. is an advantage of ILE use as a calorie source in PN
A. Reduced fluid volume due to caloric density B. Reduced glucose load C. Increased carbon dioxide production D. Decreased in-use contamination
2. The infusion rate of ILE associated with a lower rate of hypertriglyceridemia is
g/kg/d. A. < 1.5 B. 2.0 C. > 1.5

ASPEN EDUCATION PROGRAM OUTLINE TEMPLATE
D. >2.5
3. A characteristic of oil is its reliable triglyceride clearance A. Soy B. Olive C. Medium Chain Triglycerides (MCT) D. Fish
4. An important compositional difference of the new ‘Alternative’ ILE products as compared with
Soy ILE is . A. The inclusion of fish oil B. The particle size of the emulsion C. Reduced omega-6 fatty acid content D. The inclusion of medium chain triglycerides
Learning Assessment Answers: 1. Answer = B: Although oral fat is more calorically dense than dextrose, because the
concentration of lipid in ILE (20%) is lower that dextrose (50-70%) before admixture in PN, it is not always more calorically dense. Fat oxidation has a lower amount of carbon dioxide produced than carbohydrate and ILE. ILE due to its lower osmolality and oil characteristic may support microbial growth better than dextrose based PN if inadvertently contaminated.
2. Answer = A: in the study by Liop, ILE infusion rate was correlated with hypertriglyceridemia with the frequency being lower at a rate of <1.5 g/kg/d (24.9% compared with 54.5% at rates > 1.5 g/kg/d). A rate >2.5 g/kg/d should not be exceeded according to all ILE package inserts.
3. Answer = C: MCT is also efficiently oxidized, soy oil is useful for essential fatty acids, olive oil is not metabolized to active biproducts and fish oil provides a rich source of omega 3 fatty acids
4. Answer = C; Although fish oil and medium chain fatty acids are positive additions to ILE formulations, not all ILEs contain fish oil and/or MCT but the ‘alternatives all have a lower content of omega 6 fatty acids.
References 1. Huschak G, Nieden K, Hoell T, et al. Olive oil based nutrition in multiple trauma patients: a pilot
study. Intens Care Med 31:1202-1208. 2. Mirtallo JM, Powell CR, Campbell S, et al. Invited review: cost effective nutrition support. Nutr Clin
Pract 198;7;2:142-151. 3. Mirtallo J, Canada T, Johnson D, et al.; Task Force for the Revision of Safe Practices for Parenteral
Nutrition. Safe practices for parenteral nutrition. J Parenter Enteral Nutr 2004;28(suppl):S39-70. 4. Mirtallo JM, Dasta JF, Kleinschmidt KC, Varon J. State of the Art Review. Intravenous fat emulsion:
current applications, safety profile and clinical implications. Ann Pharmacother 2010;44:688-700. 5. Llop J, Sabin P, Garau M, et al.; the Hospital Pharmacy Artificial Nutrition Group of Catalonia. The
importance of clinical factors in parenteral nutrition–associated hypertriglyceridemia. Clin Nutr 2003;22:577-83.
6. Salvian AJ, Allardyce DB. Impaired bilirubin secretion during total parenteral nutrition. J Surg Res 1980;28:547-55
7. Pedersen CA, Schneider PJ, Schecklehoff DJ. ASHP national survey of pharmacy practice in hospital settings: dispensing and administration – 2011. Am J Health Syst Pharm 2012;69:768-785.
8. Storey MA, Weber RJ, Besco K, et al. Evaluation of parenteral nutrition errors in an era of drug shortages. Nutr Clin Pract 2015;31:211-217.
9. Mirtallo JM. Parenteral nutrition ordering processes. J Parenter Enter Nutr 2012;36:29S-31S. 10. Grimble R. Fatty acid profile of modern lipid emulsions: scientific consideration for creating the ideal
composition. Clin Nutr 2005 (1,suppl):9-15.

Overview and History of ILEs Available in the United States
ASPEN 2019 Nutrition Science & Practice Conference
Jay M. Mirtallo, MS, RPh, BCNSP, FASHP, FASPENProfessor Emeritus, The Ohio State University, College of Pharmacy
Clinical Specialist, American Society for Parenteral and Enteral Nutrition
© 2
019
AS
PE
N |
Am
eric
an S
ocie
ty fo
r Par
ente
ral a
nd E
nter
al N
utrit
ion.
All
Rig
hts
Res
erve
d.
Disclosures
• I have a commercial relationship with Fresenius Kabi as a member of speaker’s bureau and consultant. I also consult with Coram Home
Infusion, MedEdicus and Wolters Kluwer. I will provide practice recommendations that are based on formal structured review of the literature and will state inclusion and exclusion criteria.
© 2
019
ASPE
N | A
mer
ican
Soc
iety
for P
aren
tera
l and
Ent
eral
Nut
ritio
n.Al
l Rig
hts
Rese
rved
.
Learning Objectives
Upon completion of this session, the learner will be able to….
• Discuss the variables to consider when selecting ILE products for usein practice
• State the advantages of ILE over dextrose as a PN calorie source
• Describe the characteristics of the various oils used in ILE products
• Compare the compositional difference in ILE products available in theUS
© 2
019
AS
PE
N |
Am
eric
an S
ocie
ty fo
r Par
ente
ral a
nd E
nter
al N
utrit
ion.
All
Rig
hts
Res
erve
d.
Role of Lipid (ILE) in Parenteral Nutrition
Prevention of Essential Fatty Acid (EFA) deficiencyDose:
Linoleic acid 2.5% of caloriesLinolenic acid 0.5% of calories
Energy sourceReduce dextrose load/dose
Precursor to biochemical products of immunity, coagulation and stress response
20% Lipid Emulsion Composition: A Complex Pharmaceutical Formulation
Product Soy ILE
OilSoybean 20%
Egg yolk phosphatide 1.2%
Glycerin 2.25%
Osmolarity 260
pH 6-8.9
Fat particle size 0.5
Size 100, 250, 500, 1000
Lipid Advantage over Glucose as a Calorie Source
• Reduced Glucose from PN for Glucose Control
• Trauma pts (N=33)o ILE group
- Lower blood glucose (133 vs 156 mg/dl)- Lower carbon dioxide production- Decreased minute volume- Shorter duration of mechanical ventilation
Huschak et al. Intensive Care Med 31: 1202-1208, 2005

PN Pulmonary Complications: Hypercapnea
Dextrose dose > 5 mg/kg/min
or
Caloric dose > 150% of Needs
Lungs
Carbon dioxide production
Respiratory failure in Pts
with limited pulmonary reserve
Prolonged mechanical ventilation
• Less CO2 produced per molecule of fat than per molecule of dextrose
• Respiratory quotient (RQ) dextrose = 1
• RQ fat = 0.7
ILE: Limitations to Use
• Limitations to use as a Calorie SourceoCost
oStability
oContamination
oMetabolism more complicated than dextrose
ILE: Cost Effective Nutrition Support
• Lipid emulsions 15 x more expensive than dextrose
• Restricted use: savings of $75,000 per yro Diabetes or diabetes of stress
o Impaired pulmonary function
- CO2 retentiono TPN-induced liver disease
• Hold Lipid for 3 weeks for EFAD prevention
Mirtallo et al. Nutr Clin Pract 1987;12:142
ILE: Stability Concerns
• Emulsion destabilizationo Aggregation
o Creaming - reversible
o Coalescence - irreversible
o ‘Oiling ‘ out
- Excess particle size▪ > 6 microns
IV Lipid Emulsions: Stability Concerns• Adverse effects of Administration
oParticle size > 6
- Fat embolism- Acute reactions
▪ Hypotension
▪ Pulmonary hypertension
▪ Acidosis
- More rapid clearance by RES in liver, spleen andlungs
Mirtallo et al. JPEN 2004;28:S39-S70
ILE: In-Use Contamination
• Microbial growth characteristicso Lipid emulsion alone
- Intermittent infusion separate from PN- Characteristics supporting microbrial growth
▪ Iso-osmotic
▪ High pH
▪ Glycerol
o As TNA
Mirtallo et al. Ann Pharmacother 44:688, 2010

ILE: In-Use Contamination
• Malassezia furfuro Dependent on exogenous fatty acids
- Sebaceous glands and surrounding tissueso Propoful –
- hang time- aseptic technique- contaminated equipment in preparation
Mirtallo et al. Ann Pharmacother 44:688, 2010
ILE: In-Use Contamination• Malassezia furfur
o Nutritional use
- Repackaging for neonatal PN useo CDC limit hang time
- 12 hours separate from PN- 24 hours in PN- Syringe: ? 6 hrs- TNA: 24 hours along with administration set
Mirtallo et al. Ann Pharmacother 44:688, 2010
Soy ILE: Metabolic Fate of IV Lipid
Mirtallo et al. Ann Pharmacother 44:688, 2010
ILE: Factors affecting Clearance
• Phospholipid contento Phospholipid:Tg ratio
- 4 X greater in 10% vs 20% emulsion• Particle size
o Increase size hastens clearance
• Infusion rate o Amount: >1.5 g/kg/d
o Continuous
- Fewer fluctuations in serum Tg- Improved fat oxidation- Immune function
Hypertriglyceridemia• Plasma clearance
o Phospholipid concentration: 10 vs 20%
- Phospholipid:triglyceride ratio• Infusion rate: exceed lipolytic capacity of endothelial lipases
o Influence of critical illness
o Accumulation of TG in RES
o Displacement of bilirubin from albumin by FFA
Hypertriglyceridemia• Side effects of lipids- rapid administration
o Rate not to exceed
- 0.11 g/kg/hr healthcare environment (continuous)- 0.15 g/kg/hr homecare (cyclic)
• Caution to prevento Pancreatitis in adults
o Hyperlipidemia and fat overload in neonates

Hypertriglyceridemia (6-30%)
• Infusion rate (g/kg/d)o < 1.5 62/249 24.9%
o > 1.5 6/11 54.5%
• Risk factor 62/215 28.8%o Renal failure
o Gluc > 180
o Prednisone
o Pancreatitis
o sepsis
• No Risk Factor 6/45 13.3%
• Important to monitor triglycerides at baseline and periodically thereafter
Liop et al. Clin Nutr 22:577, 2003
© 2
019
AS
PE
N |
Am
eric
an S
ocie
ty fo
r Par
ente
ral a
nd E
nter
al N
utrit
ion.
All
Rig
hts
Res
erve
d.
Fat Overload Syndrome
Other symptoms
LethargyTachycardiaHeadacheNausea, vomiting, abdominal pain Hepatosplenomegaly Cough with hemoptysis
Excessive accumulation of serum lipids
Acute onset:FeverJaundiceIrritabilitySpontaneous hemorrhageHyperlipidemia
Fat Overload Syndrome
• Childreno 10 month to 9 years
o Large daily doses
- 3.3-5.4 g/kg/dayo Long duration
- 28-114 days
• Extreme effects when administered beyond therecommended daily dose and infusion rates
Mirtallo et al. Ann Pharmacother 44:688, 2010
ILE: Cholestatic Jaundice• Excessive dosage
o 3 g/kg/day
• Long-term useo Mean duration 45 days
• Significant increaseo Alkaline phosphatase
o Bilirubin
o Cholesterol
• Liver biopsyo Periportal, mixed inflammatory infiltrates
o Bile duct proliferation in portal triads
o Canalicular bile plugs
• Improvement with lower dose or PN discontinued
Salvian AJ, Allardyce DB. J Surg Res 28:547, 1980
Parenteral Nutrition Associated Liver Disease (PNALD)
• Prevalence increases with duration of PN therapy
• Role of fat emulsionso Fat source
oPhytosterol content
oDose
- > 1g/kg/day in long term PN patients
Lipid Peroxidation• Alterations in various organs as a result of tissue
peroxidative damageo ‘Free radicals’
-React with all cellular components:▪Proteins
▪Nucleic acids
▪ Lipids
o α-tocopherol inhibits lipid peroxidation

ILE: Systems Issues
• TNA vs separate intermittent infusion
• Look alike-sound alike
• Safetyo Infusion rate
oDuration
oMedication errors
Method of Compounding PN
Pedersen et al Am J Health-Syst Pharm 2012;69:768-85
24 hour nutrient infusion system – transition to automated compounding
Safety of System: Lipid Emulsions
• Medication errors occur with fat emulsionsoSeparate administration from PN
• Nodes involvedoOrder
- Lack of standard method of ordering IVFEo Administration
-Misinterpretation of the rate on the IVFE order- Improper programming of infusion pump
Storey et al. Nutr Clin Pract 2015;31:211
ILE: PN Ordering Practicesg/kg/dg/dg/L of PNVolume of % original concentration% final concentrationg/total volume of PNKcal/dayVolume of % concentration to be added to or infused separate from PNml/dml/L of PNG per total PN volumeNonprotein kcal
Mirtallo JM. J Parenter Enter Nutr 2012;36:29S-31S
ILE: Clinical Implications
Soy IVE are relatively safe when used according to manufacturer best practice recommendations
o Dose < 2.5 g/kg/d
o Infusion rate: < 0.11 g/kg/h
• Tg levels may be improved with use of 20% vs 10% product
• Use of Soy IV ILE require careful monitoring of triglycerides and otherorgan systems affected from long term use.
Evolution of ILE ProductsObjective
• ‘Dilution’ of ω-6 fatty acid contentoOils that are easily metabolizable and do not exacerbate
inflammatory stress
- MCT, Olive OiloAdd ω-3 fatty acids from fish oil
• Ultimately achieve a ratio of ω-6:ω-3 of 2:1-4:!
Grimble. Clin Nutr (Suppl) 2005;1:9-15

Oil Characteristics
• Soybeano Rich source of Essential fatty acids
o Omega 6 fatty acids – more proinflammatory
• Medium chain triglycerideso Efficient energy source
o Reliable triglyceride clearance
• Olive oil (Oleic acid)o Reduce polyunsaturated fatty acid load (peroxides)
o Neutral end product
• Fish oilo Omega 3 fatty acids – less proinflammatory
U.S. Lipid Product Composition
Brand Intralipid®Nutralipid®
Smoflipid® Clinolipid® Omegaven®
Oil Source Soybean 100% Soybean 30%Medium Chain
30%Olive Oil 25%Fish Oil 15%
Soybean 20%Olive Oil 80%
Fish Oil
Fat Composition (% Mean Value(Range)Linoleic acid 53 19.5 13.8-22% 1.5%Linolenic acid 7.5 2.5 0.5-4.2% 1.1%Oleic acid 24.5 (19-30) (23-35) 44.3-79.5% 4-11%Eicosapentanoicacid (EPA)
0 2.3 13-26%
Docosahexaenoic acid (DHA)
0 2.3 14-27%
Package Insert:Intralipid®, Nutralipid®, Smoflipid®, Clinolipid®, Omegaven®
Summary
• Variables to consider when selecting ILE products for use in practiceo Cost
o Stability
o Compatibility
o Metabolism
- Oxidized for energy- Free radical production- Triglyceride clearance
o Administration: as TNA or separate infusion, multi-chamber product
o Physiologic impact on immunity, infection, coagulation and stress response
Conclusion
• Safety and efficacy of Soy ILE has been shown to be dependent oninfusion rate, daily dose (g/kg) and duration.o Current guidelines for use in the US address the problems from Soy ILE that
limits dose and use in particular patient populations
• Issues concerning the efficacy as a calorie source, triglyceride clearance and physiologic effects on immunity, coagulation and stress response ledto an evolution in ILE products not commercially available in the US until recently
• Its an exciting time for PN therapy due the approval of ‘alternative’ ILEs
and the discussion of if, where and how these will be put into use
Learning Assessment Questions
1. is an advantage of ILE use as a calorie source in PNa) Reduced fluid volume due to caloric densityb) Reduced glucose loadc) Increased carbon dioxide productiond) Decreased in-use contamination
Learning Assessment Questions
2. The infusion rate of ILE associated with a lower rate of hypertriglyceridemia is g/kg/d.a) < 1.5b) 2.0c) > 1.5d) >2.5

Learning Assessment Questions
3. A characteristic of oil is its reliable triglyceride clearancea) Soyb) Olivec) Medium Chain Triglycerides (MCT)d) Fish
Learning Assessment Questions
4. An important compositional difference of the new ‘Alternative’ ILE
products as compared with Soy ILE is .a) The inclusion of fish oilb) The particle size of the emulsionc) Reduced omega-6 fatty acid contentd) The inclusion of medium chain triglycerides
© 2
019
ASPE
N | A
mer
ican
Soc
iety
for P
aren
tera
l and
Ent
eral
Nut
ritio
n.Al
l Rig
hts
Rese
rved
.
References
• Huschak G, Nieden K, Hoell T, et al. Olive oil based nutrition in multiple trauma patients: a pilot study. Intens Care Med 31:1202-1208.
• Mirtallo JM, Powell CR, Campbell S, et al. Invited review: cost effective nutrition support. Nutr Clin Pract 198;7;2:142-151.
• Mirtallo J, Canada T, Johnson D, et al.; Task Force for the Revision of Safe Practices for Parenteral Nutrition. Safe practices for parenteral nutrition.JPEN J Parenter Enteral Nutr 2004;28(suppl):S39-70.
• Mirtallo JM, Dasta JF, Kleinschmidt KC, Varon J. State of the Art Review.Intravenous fat emulsion: current applications, safety profile and clinical implications. Ann Pharmacother 2010;44:688-700.
• Llop J, Sabin P, Garau M, et al.; the Hospital Pharmacy Artificial Nutrition Group ofCatalonia. The importance of clinical factors in parenteral nutrition–associated hypertriglyceridemia. Clin Nutr 2003;22:577-83.
© 2
019
ASPE
N | A
mer
ican
Soc
iety
for P
aren
tera
l and
Ent
eral
Nut
ritio
n.Al
l Rig
hts
Rese
rved
.
© 2
019
AS
PE
N |
Am
eric
an S
ocie
ty fo
r Par
ente
ral a
nd E
nter
al N
utrit
ion.
All
Rig
hts
Res
erve
d.
References
• Salvian AJ, Allardyce DB. Impaired bilirubin secretion during total parenteral nutrition. J Surg Res 1980;28:547-55
• Pedersen CA, Schneider PJ, Schecklehoff DJ. ASHP national survey ofpharmacy practice in hospital settings: dispensing and administration –2011. Am J Health Syst Pharm 2012;69:768-785.
• Storey MA, Weber RJ, Besco K, et al. Evaluation of parenteral nutritionerrors in an era of drug shortages. Nutr Clin Pract 2015;31:211-217.
• Mirtallo JM. Parenteral nutrition ordering processes. J Parenter Enter Nutr 2012;36:29S-31S.
• Grimble R. Fatty acid profile of modern lipid emulsions: scientific consideration for creating the ideal composition. Clin Nutr 2005 (1,suppl):9-15.
© 2
019
AS
PE
N |
Am
eric
an S
ocie
ty fo
r Par
ente
ral a
nd E
nter
al N
utrit
ion.
All
Rig
hts
Res
erve
d.