NADIA DI MUZIO IRCCS OSPEDALE S. RAFFAELE … - Dott.ssa... · varese 3 luglio 2012 basi...
54
VARESE 3 LUGLIO 2012 BASI SCIENTIFICHE PER LA DEFINIZIONE DI LINEE GUIDA DIAGNOSTICO-TERAPEUTICHE PER IL CARCINOMA DEL PANCREAS NADIA DI MUZIO IRCCS OSPEDALE S. RAFFAELE MILANO
Transcript of NADIA DI MUZIO IRCCS OSPEDALE S. RAFFAELE … - Dott.ssa... · varese 3 luglio 2012 basi...

VARESE 3 LUGLIO 2012
BASI SCIENTIFICHE PER LA DEFINIZIONE DI LINEE GUIDA DIAGNOSTICO-TERAPEUTICHE PER IL
CARCINOMA DEL PANCREAS
NADIA DI MUZIO
IRCCS OSPEDALE S. RAFFAELE MILANO
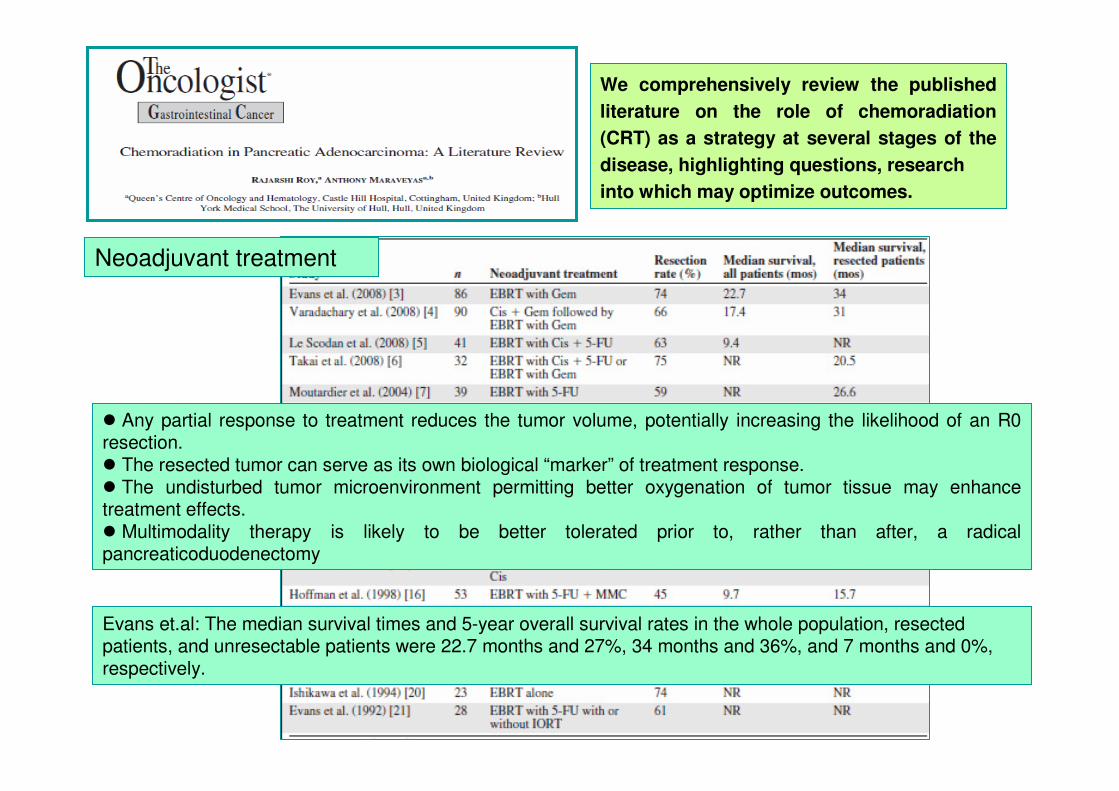
We comprehensively review the published
literature on the role of chemoradiation
(CRT) as a strategy at several stages of the
disease, highlighting questions, research
into which may optimize outcomes.
� Any partial response to treatment reduces the tumor volume, potentially increasing the likelihood of an R0 resection. � The resected tumor can serve as its own biological “marker” of treatment response. � The undisturbed tumor microenvironment permitting better oxygenation of tumor tissue may enhance treatment effects.� Multimodality therapy is likely to be better tolerated prior to, rather than after, a radical pancreaticoduodenectomy
Neoadjuvant treatment
Evans et.al: The median survival times and 5-year overall survival rates in the whole population, resected patients, and unresectable patients were 22.7 months and 27%, 34 months and 36%, and 7 months and 0%, respectively.

Chemoradiation in locally advanced nonresectable pancreatic cancer
The GITSG demonstrated the superiority of 5-FU– based CRT over radiotherapy alone in locally advanced unresectable disease. The median survival time was 5.7 months in the 60-Gy radiotherapy alone arm, compared with 10 months in the arms receiving bolus 5-FU with 40 Gy and 60 Gy of radiation. That trial also raised the possibility that, with chemotherapy, a higher dose of radiation is perhaps not necessary because the 1-year survival rates in the 60-Gy arm and 40-Gy arm with concurrent 5-FU were similar.
the Eastern Cooperative Oncology Group recently reported on a trial comparing CRT with concurrent gemcitabine followed by maintenance gemcitabine with gemcitabine alone; it still showed a significant median survival advantage in favor of the radiotherapy arm; the rates of grade 3 and 4 toxicities were low and these were manageable.
IORTIORTIORT included either implantation of iodine-125 seeds or intraoperative electron beam radiotherapy (IOERT).IOERT has been the favored approach in most studies. The National Cancer Institute showed better local control with 20 Gy of IORT following surgical therapy than with observation.
Although most have shown better local control, survival was not shown to be superior to that seen with EBRT alone.

Adjuvant chemoradiation
GITSG (1985 the first trial) � Resected pancreatic cancer patients with R0 margins were assigned to receive split-course radiotherapy over 6 weeks with a 2-week gap in between, with concurrent 5-FU, followed by maintenance 5-FU for 2 years or until progression or no active treatment. At an interim analysis, patients in the CRT arm had a significantly longer median survival time (21 months versus 11 months).The final analysis showed a median survival time of 18 months with 2- and 5-year survival rates of 46% and 17%, respectively. Following that trial, adjuvant CRT became the standard of care in the U.S
The European Study Group for Pancreatic Cancer (ESPAC) conducted the largest phase III RCT in this setting between 1994 and 2000. Five hundred forty-one patients were randomized (a) chemotherapy versus observation,(b) CRT versus observation, and (c) a 2x2 factorial design of observation versus chemotherapy versus CRT versus CRT plus maintenance chemotherapy. The conclusion from that trial was that adjuvant chemotherapy significantly improved survival, whereas CRT had a detrimental effect on survival because it delayed systemic chemotherapy. The results generated substantial controversy and the trial was criticized.
The latest trial of CRT (Radiation Therapy Oncology Group trial 97–04) was conducted between 1998 and 2002; 381 patients with pancreatic head tumors only had a significant benefit from gemcitabine in terms of the median survival time and 3-year survival rate (20.6 months versus 16.9 months and 32% versus 21%, respectively).
It is difficult to formulate a “one-size-fits-all” strategy in the adjuvant setting for pancreatic cancer. Good quality trials are still needed, targeting surgical subgroups, especially because more aggressive surgery of “borderline”cases will lead to a greater number of R1 resections. The advent of biologicals is interesting

Newer techniques
Stereotactic RadiotherapyHoyer et al., used 45 Gy in three fractions in 5–10 days in 22 patients with locally advanced pancreatic cancer. There were unacceptable acute gastrointestinal toxicities, with 4.5% of patients experiencing gastric perforation.
The Stanford group used a single fraction of SRT delivering 25 Gy; demonstrating an 81% local control rate. The same group studied the effect of SRT as a boost to EBRT, yielding a very impressive 94% local control rate. Gastrointestinal toxicity remained a significant issue: 12.5% rate of late duodenal ulceration.
Despite a major improvement in local control, no difference in the median survival time was noted in these studies.
IMRTIMRTMilano et al., treated 25 patients with IMRT and concurrent 5-FU. IMRT was well tolerated and reduced the mean dose to the liver, kidneys, stomach, and small bowel, with 80% of patients experiencing G2 toxicity only. Ben-Josef et al., treated 15 patients with adenocarcinoma of the pancreas with IMRT and concomitant capecitabine. The IMRT was delivered to a dose of 54 Gy to the gross tumor and 45 Gy to the draining lymph nodes in a simultaneous boost method. The study reported a 7% grade 3 toxicity and 0% grade 4 toxicity rate.
With superior planning techniques and better and effective monitoring of toxicities, IMRT is likely to be safelydelivered to patients with pancreatic cancer concurrently with systemic chemotherapy.
Induction ChemotherapyInduction ChemotherapyMD Anderson Cancer Center, in a retrospective analysis of 318 patients, 73 patients receiving a median of 2.5 months of induction chemotherapy before proceeding to CRT with a significantly longer overall time to local and distant progression than patients receiving CRT as their first treatment.Brade et al. used induction chemotherapy with gemcitabine followed by concurrent gemcitabine and radiotherapy showed that 22% of patients (six of 27) had disease progression on induction chemotherapy.In a recently published nonrandomized series, 181 patients were treated with gemcitabine-based chemotherapyfor 3 months, and those with stable disease (128 patients) were treated with CRT or chemotherapy alone.The median survival time was significantly longer in patients receiving CRT (15 months versus 11.7 months). This shows a probable benefit of CRT in patients who have achieved stable disease with induction chemotherapy.
Conclusions:
the quality assurance of delivered radiotherapy and agreement on similar standards of what constitutes a radical treatment field in the two settings of an in situ primary and a resected primary are seen as a sine qua non for the success of any trial in this area.
the position of CRT in patients with initially resectable disease on first intent ending up with R1 margins needs further study,
the “neoadjuvant” approach using CRT for patients with a borderline resectable primary given the high likelihood of R1 or R2 margins would also benefit from an RCT.
for locally advanced nonresecatable cancer, the two most promising strategies of gemcitabine-based CRT followed by gemcitabine or the reverse need further study in a head-to-head RCT.
the position of IMRT and that of SRT need RCT approaches with conventional comparators
Conclusions: Conclusions:
the quality assurance of delivered radiotherapy and agreement on similar standards of what constitutes a radical treatment field in the two settings of an in situ primary and a resected primary are seen as a sine qua non for the success of any trial in this area.
the position of CRT in patients with initially resectable disease on first intent ending up with R1 margins needs further study,
the “neoadjuvant” approach using CRT for patients with a borderline resectable primary given the high likelihood of R1 or R2 margins would also benefit from an RCT.
for locally advanced nonresecatable cancer, the two most promising strategies of gemcitabine-based CRT followed by gemcitabine or the reverse need further study in a head-to-head RCT.
the position of IMRT and that of SRT need RCT approaches with conventional comparators

Purpose: This analysis evaluates acute/late toxicity outcomes and compares these data with toxicity results from RTOG-97.04 trial (pts treated with 3D-CRT).
.
Methods and Materials: 46 patients with pancreatic/ampullary cancer; 67% (n = 31) of patients were treated after undergoing definitive surgical resection; the remainder had non-metastatic but locally advanced disease.All patients received 5-fluorouracil (5-FU)–based concurrent CRT therapy with either capecitabine; the majority of patients received one to two cycles of gemcitabine before beginning concurrent CRT.
RT volumes: The initial treatment field was based on gross tumor volume (unresectable patients) or clinical tumor volume (postoperative patients), including the celiac, peripancreatic, pancreatico-duodenal, portahepatic, and para-aortic lymph node basins extending from approximately T10 through L3. Margins of 1 to 1.5 centimeters were added in all dimensions, with the final planning target volume (PTV). This volume was prescribed 45 Gy.Small field boosts included gross tumor volume or tumor bed plus a 1- to 1.5-cm margin; were treated to an additional 5.4–14.4 Gy. Inverse-planned IMRT was used to generate optimized treatment plans for each patient.
One of the major challenges of administering radiation to the upper abdomen in either the postoperative or neoadjuvant setting is the presence of multiple critical structures in the immediate vicinity of the pancreas. Intensity-modulated radiation therapy (IMRT) has been shown to reduce dose to critical dose-limiting structures in the upper abdomen.

RESULTS ACUTE TOXICITYACUTE TOXICITY: Median weight loss among IMRT patients 3% (range, 0–10%).Grade 3–4 nausea-vomiting 0% vs. 11%
Grade 3–4 diarrhea 3% vs 18%
Grade 3–4 anorexia <5% in both groups
LATE TOXICITYLATE TOXICITY
Small bowel obstruction in two pts (2 months and 1 year after completion of therapy).
SURVIVALmedian follow-up: 22 months
resectable patients
- median survival 24.8 months
- median progression- free survival 17.5 months.
patients with unresectable disease
- median overall survival 9.7 months.
SURVIVALmedian follow-up: 22 months
resectable patients
- median survival 24.8 months
- median progression- free survival 17.5 months.
patients with unresectable disease
- median overall survival 9.7 months.
CONCLUSIONS- IMRT significantly improve the toxicity of concurrent upper abdominal CRT. - IMRT reduces the acute toxicity of concurrent CRT to the upper abdomen. - IMRT not only can improve patients’ quality of life but also may allow for radiation dose escalation and intensification of chemotherapy regimens in an attempt to improve the cure rates of this disease.
Axial comparison of IMRT (left) and 3DCRT (right)
treatment plans.

Aim: to assess feasibility and safety of SBRT in patients with advanced pancreatic adenocarcinoma.
MATERIALS AND METHODS
71 pts with histologically proved pancreatic ADNca; treated with SBRT, between July 2004 and January 2009. - positive surgical margins 12 pts (17%)- locally-advanced unresectable disease 40 pts (56%)- regionally-metastatic disease 11 pts (16%)- metastatic disease 8 pts (11%)
Median tumor volume (range) cc 17 (5.1 – 249)
SBRT was performed with Cyberknife (97%) or Trilogy-IMRS (3%)Single dose SBRT 67 pts (94%)Fractionated SBRT (2 frz) 4 pts (6%)
The choice of prescription doses and fractionation was based on tumor size, prior radiation, and patient’s general condition and tolerability. All patients had 2 to 4 gold fiducials.
Fifteen patients received prior radiotherapy to the pancreas, all via 3DCRT; median dose was 45 Gy (range, 34.4 –52.2 Gy). One patient had previously received 10 Gy of HDR-brachytherapy in 2 fractions.

Results: OUTCOMESOUTCOMESMedian follow-up among surviving patients 12.7 months(4–26 months)Freedom from local progression rates at 6 months/1 year 71.7% / 48.5%
FFLP in pts with macroscopic disease 77.3% of pts with tumor size <15 mL (n 22)
59.5% of pts with tumor size> 15 mL (n 37)
FFLP in 24 to 25 Gy group 73%in 18 to 22 Gy group 45%
Median OS 10.3 months, with 6 month/1 year OS rates of 65.3% / 41%, respectively.
Results: TOXICITYTOXICITYGrade 1–2 acute and late GI toxicity were seen in 39.5% of patients. Acute toxicities were seen in 27 patients (38.1%); 3 patients (4.2%) had G3 toxicity (1 with nausea; 1 with severe abdominal pain secondary to superior mesenteric vein thrombosis; 1 with gastroparesis).No patients experienced bowel perforation secondary to SBRT. Late toxicities were seen in 3 patients (4.2%); 1 with G1 diarrhea and 2 with G1 weight loss.

A, Overall survival for different SBRT subgroups from the time of SBRT. B, Overall survival for different SBRT subgroups from the time of diagnosis for primary disease or time of recurrence for recurrent disease.
A, Overall survival for different SBRT subgroups from the time of SBRT. B, Overall survival for different SBRT subgroups from the time of diagnosis for primary disease or time of recurrence for recurrent disease.
A, Overall survival for adjuvant versus locally-advanced groups from the time of SBRT. B, Overall survival for adjuvant versus locally-advanced groups from the time of diagnosis for primary disease or time of recurrence for recurrent disease.
A, Overall survival for adjuvant versus locally-advanced groups from the time of SBRT. B, Overall survival for adjuvant versus locally-advanced groups from the time of diagnosis for primary disease or time of recurrence for recurrent disease.
CONCLUSIONS
- SBRT is feasible with mostly mild toxicity and offers symptom relief in patients with advanced pancreatic cancer.
- SBRT achieves local control rates comparable to those with conventional EBRT.
- SBRT can be delivered without delay in the initiation of adjuvant chemotherapy, which may lead to improved treatment outcomes.
- Patients with margins of resection within 1.5 mm benefited from Adjuvant SBRT
Further studies are needed to assess the benefit of the early initiation of chemotherapy allowed by the short SBRT course versus the long treatment course of conventional radiotherapy
CONCLUSIONSCONCLUSIONS
- SBRT is feasible with mostly mild toxicity and offers symptom reSBRT is feasible with mostly mild toxicity and offers symptom relief in patients with advanced pancreatic lief in patients with advanced pancreatic cancer. cancer.
-- SBRT achieves local control rates comparable to those with convSBRT achieves local control rates comparable to those with conventional EBRT.entional EBRT.
-- SBRT can be delivered without delay in the initiation of adjuvaSBRT can be delivered without delay in the initiation of adjuvant chemotherapy, which may lead to nt chemotherapy, which may lead to improved treatment outcomes. improved treatment outcomes.
-- Patients with margins of resection within 1.5 mm benefited fromPatients with margins of resection within 1.5 mm benefited from Adjuvant SBRTAdjuvant SBRT
Further studies are needed to assess the benefit of the early inFurther studies are needed to assess the benefit of the early initiation of chemotherapy allowed by the short itiation of chemotherapy allowed by the short SBRT course versus the long treatment course of conventional radSBRT course versus the long treatment course of conventional radiotherapyiotherapy


PET/TC BASED PLANNING OF RT IN LOCALLY ADVANCED PANCREATIC CANCER

Single fraction: 25 Gy

4D-CT CON MDC: qualità di immagine


RPM Respiratory Gating™ System
TM : Varian Medical System Gating School Copenhagen

X-ray ONPET acquisition
CT or PET Images Phases
4D Data Sorting
Patient Breathing Curve

Goal:Define the target volume and the volume of space that
encompasses tumor motion.

Goal:Define the target volume and the volume of space that
encompasses tumor motion.

HSR , Milan
4D-PET/CT CONTOURING
exp
insp sum
st
BTV

HSR , Milan
4D-PET/CT CONTOURING
ITV ITV

4D CT
Cine Review
HSR-Milano
ITV

4D CT
Cine Review
HSR-Milano
ITV

4D-PET/CT Gating StudiesRT Application: Pancreas
• Organ and lesions undergo complex movement
• CT based target definition is difficult even with c.m
• Close organs at risk (OARs)
4D-CT + c.m.4D-PET

Pancreatic Tumour
HSR-Milano

4D-CT with c.m.
4D-PET
FusedPET /CT
Pancreatic Tumour

BTV
GTV
4D-PET/CT
BTV
GTV

ITV2
4D-PTV2
STD-PTV2
Target DefinitionPTVs e OAR
PTV1
ITV1 Kidneys
Liver
Duodenum
Spinal cord

SYNTHESIS OF PRESENTATIONSYNTHESIS OF PRESENTATION
To evaluate toxicity and efficacy of hypofractionated image-guided
Tomotherapy concomitant to oral capecitabine in patients with
advanced pancreatic adenocarcinoma.

CHARACTERISTICS OF PATIENTSCHARACTERISTICS OF PATIENTS
● From June 2006 to November 2009
● 33 pts (♀. 19; ♂. 14)
● Median age: 62 ys (46-81)
● Median KPS : 90 (70-100)
● Adenocarcinoma: 33
● 30 pts received induction CHT
● Stage: III 24 pts, IV 9 pts with controlled metastatic diseases

11 pts � contrast-enhanced 4D-CT/PET simulation22 pts� contrast-enhanced CT and CT/PET simulation
MATERIALS AND METHODSMATERIALS AND METHODS
CAPECITABINE CAPECITABINE 1250 mg/m2/day
Tomotherapy treatment
44.25 Gy in 15 fractions

MATERIALS AND METHODSMATERIALS AND METHODS
volume definitions:
GTV in 4 series of 4D-CT
GTV in CT
ITVITV
4D4D--PTVPTV
BTVBTV
PTVPTV
ITVITV
0.5-0.5-0.5 cm
4D4D--CT GROUPCT GROUP NO 4 DNO 4 D--CT GROUPCT GROUP
boolean Union
ITV/BTVITV/BTV
0.50.5--0.50.5--11
ITV/BTVITV/BTV

ST-PTV vs 4D-PTC: GEOMETRIC RESULTS
STST--PTVs 3DCRT vs 4DPTVs 3DCRT vs 4D--PTVs 3DCRTPTVs 3DCRT
4D-PTVs were smaller than ST-PTVs in all pts
4D-PTVs were 36% smaller than ST-PTV (mean value 187 cm3 vs 295
cm3, p=0.0006)
Overlapping volumes between 4D-PTVs and stomach was 59% smaller
than overlapping volumes between ST-PTVs and stomach (mean value 7
vs 18 cm3, P=0.0014)
Overlapping volumes between 4D-PTVs and duodenum was 43%
smaller than overlapping volumes between ST-PTVs and duodenum
(mean value 9 vs 16 cm3, P=0.006)

3DCRT Targets
Organ DVH Parameters
ST-PTV
(Mean
Values)
4D-PTV
(Mean
Values)
Organ
Spared
(%)
P
Stomach D_mean
V20
V50
22.6
48.5
13,9
17.6
39.7
8.3
22%
18%
40%
0.007
0.01
0.004
Duode-
num
D_mean
V20
V50
35.0
69.9
36.1
30.1
63.4
25.3
24%
9%
29%
0.01
0.01
0.01
Kidney D_mean
V20
V30
9.0
18.5
11.2
6.9
13.2
7.7
23%
28%
31%
0.03
0.05
0.06
STST--PTVs 3DCRT vs 4DPTVs 3DCRT vs 4D--PTVs 3DCRTPTVs 3DCRT

Target = 4DPTVs
Organ DVH
Parameters
3DCRT
(Mean values)
TOMO
(Mean values)
Organ
Spared
(%)
P
Stomach D_mean
V20
V50
17.6
39.7
8.3
16.5
29.2
4.3
8%
29%
48%
0.36
0.004
0.001
Duode-
num
D_mean
V20
V50
30.1
63.4
25.3
24.6
50.5
12.7
17%
20%
49%
0.003
0.001
0.001
Kidney D_mean
V20
V30
6.9
13.2
7.7
13.3
18.0
1.2
-48%
-26%
84%
0.0006
0.16
0.01
3DCRT vs TOMOTHERAPY

●● Early Toxicity G3: gastric ulcer : 1pts (3%); diarrhoea: 1pts (3%)
●● No LateNo LateToxicity
RESULTS:TOXICITYRESULTS:TOXICITY
“Common Terminology Criteria for Adverse Events (CTCAE)” v 3.0-NCI- 2003.
Early toxicity G1-G2 33pts/33
Nausea e vomiting 15 ( 45%)
Abdominal pain 9 ( 27%)
Diarrhoea 3 (9% )
trombocitopenia 7 (21%)
Anemia 6 (18%)
Neutropenia 2 (6%)
Hepatotoxicity 3
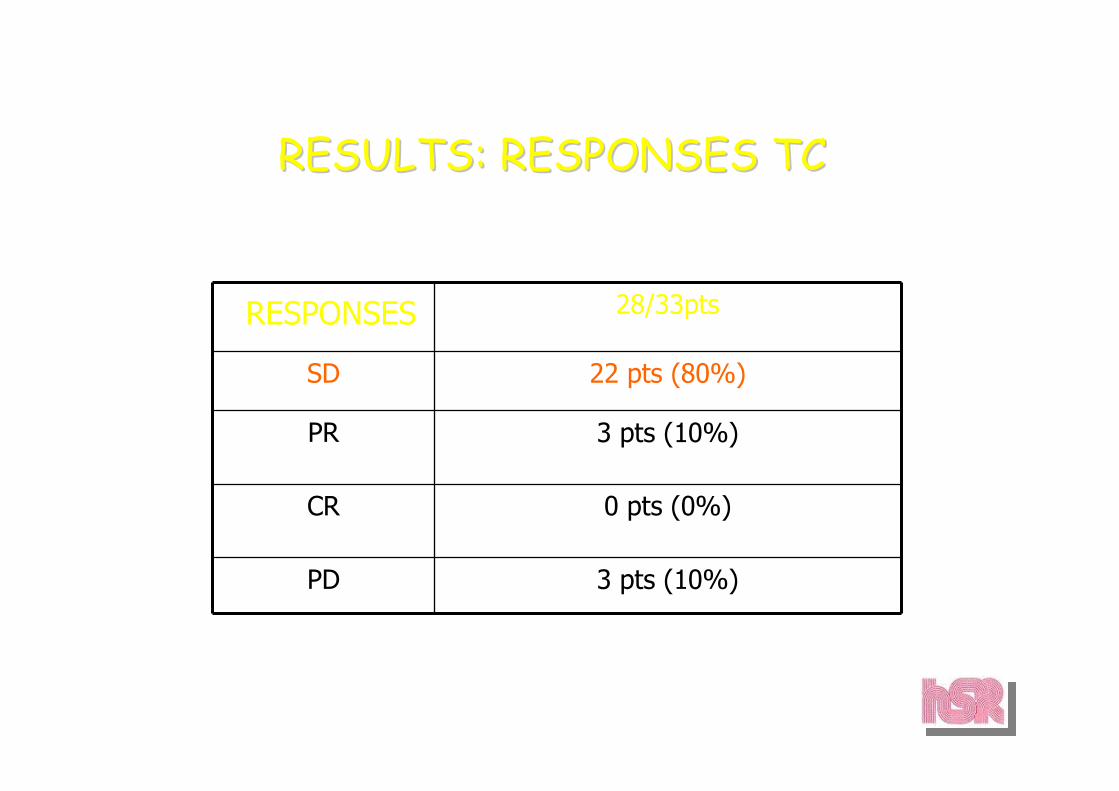
RESULTS: RESPONSES TCRESULTS: RESPONSES TC
RESPONSES 28/33pts
SD 22 pts (80%)
PR 3 pts (10%)
CR 0 pts (0%)
PD 3 pts (10%)

RESULTSRESULTS
Median FU: 34.5 m.Median FU: 34.5 m.
Median TTP: 12 m. Median TTP: 12 m.
Median TTLP: 17.5 m. Median TTLP: 17.5 m.
25 m. OS : 63%.25 m. OS : 63%.




CONCLUSIONS
A dose of 44.25 Gy in 15 fractions on PTV concomitant to oral capecitabine is feasible, associated with a mild rate of acute toxicity and provides further stabilization or improvement of local disease in heavily pre-treated patients.
Long term local control is still a dream (mirage). Considering the low rate of G3 toxicity, there is probably room for further dose escalation.
The sequence of induction chemotherapy followed by Chemoradiation seems to allow the best long term survival results

PANCREATIC CANCER
Hypofractionated Tomotherapy with concomitant
chemotherapy in advanced pancreatic adenocarcinoma.
Preliminary results of a phase I study.
ENDPOINT
To determine the radiotherapy MTD to a tumor sub-volume infiltrating vessels
METHODS
31 patients in stage III or IV previously CT-treated
Simulation performed with contrast-enhanced 4D-CT/PET
GTV1, the tumor, and
GTV2, a tumor sub-volume 1 cm around infiltrated vessels
were contoured on 4D-CT.

MATERIALS AND METHODSMATERIALS AND METHODS
• ● From June 2005 to November 2008
• ● 32 pts (♀. 18 ♂. 13)
• ● Median age: 60 ys (40-74)
• ● Median KPS : 90 (60-100)
• ● Adenocarcinoma: 32
• ● IInduction CHT 30 pz, mmedian N°of cycles : 6 (2-11)
• (PEXG: 11, PDXG: 8, PEFG: 6, GEM: 3, CDDP+GEM: 1)
• ● Stage: III 26 pts, IV 3 pts (2 pts with CR of hepatic metastases, 1 pt with stable disease 6 months after the end of CHT), local relapse 3 pts
SIB GROUPSIB GROUP: : 19 pts 19 pts
PTV2PTV2 44.25 Gy/15 f. +44.25 Gy/15 f. +
SIB with dose escalation toSIB with dose escalation to PTV1 PTV1
(48 Gy: 4 pts, 50 Gy: 6 pts, (48 Gy: 4 pts, 50 Gy: 6 pts,
52 Gy: 3 pts, 55 Gy: 3 pts 58 Gy: 3 52 Gy: 3 pts, 55 Gy: 3 pts 58 Gy: 3 pts)pts)
No SIB GROUP: 13 pts No SIB GROUP: 13 pts
44.25 Gy /15 f. PTV (44.25 Gy /15 f. PTV (PTV2PTV2))
c.i. 5FU / CAPECITABINE c.i. 5FU / CAPECITABINE 5-FU 250mg/m2/day c.i. in the first 6 pts. 23 remaining pts received capecitabine, 1250 mg/m2/day

MATERIALS AND METHODSMATERIALS AND METHODS
Volume Definitions:
GTV in 4 series of 4D-CT
GTV in 4 series of 4D-CT
GTV2GTV2(tumor)(tumor)
GTV1 GTV1 (infiltrating vessels (infiltrating vessels
+ 5+ 5--10 mm)10 mm)
ITV2ITV2 ITV1ITV1
4D4D--PTV2PTV2 4D4D--PTV1PTV14D4D--PTV=4DPTV=4D--PTV2PTV2
ITV=ITV1ITV=ITV1
0.5-0.5-0.7 cm
SIB GROUPSIB GROUP No SIB GROUPNo SIB GROUP
boolean Union

MATERIALS AND METHODSMATERIALS AND METHODS
IMAGE QUALITY OF CONTRAST-ENHANCED 4DCT
PTV
• Volume definitions:

PANCREATIC CANCER
RESULTS
DOSE LEVELS:
I level, 48 Gy: 4 pts
II level, 50 Gy: 6 pts
III level, 52Gy: 3 pts
IV level, 55 Gy: 6 pts
V level, 58Gy: 3 pts
G3 TOXICITY:
Gastric ulcer: 1 pt at the II level
Gastro-duodenitis: 1 at the IV level
COMMENTS:
The planned final dose to PTV2 is 58 Gy

●● Early Toxicity G3: gastric ulcer in SIB Group : 2/19 patients (11%)
●● LateLateToxicity: emorragic gastro-duodenitis G3 in No SIB Group : 1/13 pz (7%)
RESULTS:TOXICITYRESULTS:TOXICITY
“Common Terminology Criteria for Adverse Events (CTCAE)” v 3.0-NCI- 2003.
Early toxicity
Diarroea G1 3 ( 15%) 1 (7% )
Diarroea G2 2 ( 11%) 2 (15%)
Nausea e vomiting G1 5 ( 23%) 3 ( 23%)
Nausea e vomiting G2 3 ( 15 %) 2 (15%)
Nausea e vomiting G3 0 ( 0%) 1 (7% )
Anorexia G1 3 (11%) 1 (7% )
Anorexia G2: 1 ( 6%) 1 (7% )
Abdominal pain G1 2 (13%) 0 ( 0%)
Abdominal pain G2 3 (20 %) 5 ( 38%)
Weigth loss G1 1 ( 6%) 0 ( 0%)
trombocitopenia G1 1 ( 6%) 1 (7% )
Neutropenia G2 0 (0%) 2 (15%)
Hepatotoxicity G1 2 (13%) 2 ( 15%)
Hepatotoxicity G2 1 (6%) 0 (0%)
SIB Group N°Pts (%) No SIB Group N° Pts(%)

RESULTS: RESPONSES TC/RESPONSES PETRESULTS: RESPONSES TC/RESPONSES PET
RESPONSES SIB Group (15/16 pts)
No SIB Group (13/13 pts)
14 /29 pts
PR 4 pts (27%) 4 pts (31%) 10 pts (72%)
CR 0 pts (0%) 1 pts (7%) 2 pts (14%)
SD 8 pts (53%) 4 pts (31%) 0 pts (0%)
PD 3 pts (20%) 4 pts (31%) 2pts (14%)
TC PET

RESULTS: SITES OF FIRST PROGRESSIONRESULTS: SITES OF FIRST PROGRESSION
Local + systemic: 15/32 (45%)
Local only: 3/32 (9%)
Median TTP : 12 m. Median TTP : 12 m.
Median TTLP: 16 m. Median TTLP: 16 m.
Median OS : 20.2 m.Median OS : 20.2 m.

CONCLUSIONSCONCLUSIONS
A dose of 44.25 Gy in 15 fractions on PTV2 concomitant to 5-FU c.i. or oral capecitabine is feasible and effective.
The concomitant boost to infiltrated vessels does not seem to improve the response rate; however, once the maximum tolerated dose to the tumor sub-volume is reached, its efficacy will be tested on potentially operable disease.

PANCREATIC CANCER
FUTURE PERSPECTIVES
Once established the MTD, this SIB approach will be tested in pts with
potentially resectable disease.

Cancer February 15, 2012
BACKGROUNDBACKGROUND: Radiotherapy may improve the outcome of patients with pancreatic cancer but at an
increased cost. In this study, the authors evaluated the cost-effectiveness of modern radiotherapy techniques in the treatment of locally advanced pancreatic cancer
METHODS: A Markov decision-analytic model was constructed to compare the cost-effectiveness of 4 treatment regimens: -Gemcitabine alone-Gemcitabine plus conventional radiotherapy-Gemcitabine plus intensity-modulated radiotherapy (IMRT)-Gemcitabine with stereotactic body radiotherapy (SBRT)
Decision-analytic Markov model
With gem-alone and gem-RT, we used the treatment schema and outcome data from the preliminary report of the clinical trial E4201 � monthly cycles of gem alone (1000 m2 weekly every 3 of 4 weeks), or gem plus radiotherapy (600 mg/m2 weekly with 50.4 Gy in 28 fractions) followed by monthly gem (1000 mg/m2 every 3-4 weeks).
We considered only grade 3 or higher gastrointestinal toxicity attributable to radiation.
To our knowledge, the relative decrease in toxicity from IMRT compared with conventional radiotherapy has not been reported in patients. A dosimetric study estimated that IMRT would reduce small bowel toxicity from 24.4% to 9.3%; therefore, the rate of toxicity for gem-IMRT was assumed to be 38% that of gem-RT.

These charts illustrate model outcome predictions. (A) disease-free survival, (B) Local control, (C) distant-metastases-free survival, (D) overall survival for all 4 treatment groups. Gemcitabine plus radiotherapy (RT) and gemcitabine plus intensity-modulated radiotherapy (IMRT) had
identical outcomes and are plotted as 1 curve. SBRT indicates stereotactic body radiotherapy.
RESULTS: SBRT increased life expectancy by 0.20 quality-adjusted life years (QALY) at anincreased cost of $13,700 compared with gemcitabine alone (incremental cost-effectiveness ratio [ICER] ¼$69,500 per QALY). SBRT was more effective and less costly than conventional radiotherapy and IMRT.
After 1 year, our model predicted that, among patients who received gem-SBRT, 16% would fail with local progression (8% local failure alone and 8% local + distant failure), and 63% would fail with distant progression (55% distant alone and 8% local + distant).
CONCLUSIONS:IMRT in locally advanced pancreatic cancer exceeds what society considers cost-effective. Combining gemcitabine with SBRT increased clinical effectiveness beyond that of gemcitabine alone at a cost potentially acceptable by today’s standards.