NACCDO Emotional Drivers by Collins Hickok Sargent Puskarich Sharpley
Upload
pan-naccdoCategory
view
163download
2description

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
NACCDO 2014
State of the Industry 2013 - 2014Current Challenges to the Case for Support of Hospitals and Health Systems
Michael [email protected]
PhilanthropyLeadership Council
1

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
2
Taking the Donor Perspective
Three Lenses for Evaluating the Philanthropic Environment in Health Care
Source: Philanthropy Leadership Council interviews and analysis.
Donor-Centric Lenses
The Economy and Perception of Personal
Economic Security
Personal Motives and Perception of Value
and Impact
Hospital Performance and Perception of Need
in Health Care
Am I in the financial position to donate?
Is the organization a worthy cause?
Will my gift make a difference?
“MY CHECKBOOK” “THEIR STORY” “OUR IMPACT”

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
3
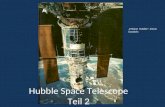
Charities Feeling Bullish About 2013
Source: Flandez R, “70% of Charities Forecast Rise in Donations in 2013,” Chronicle of Philanthropy, April 8, 2013, available at: www.philanthropy.com, accessed June 6, 2013; Philanthropy Leadership Council interviews and analysis.
Lens #1: “My Checkbook”
Anticipated Direction of Change in Charitable Receipts
2013 compared with 2012
Rising Consumer Confidence
“Overall consumer confidence in the economy rose last year and that created a more positive environment for charities to go out in and build relationships [with donors].”
Andrew Watt, PresidentAssociation of Fundraising Professionals
”2%
7%
20%
12%
59% Increase by 1% to 15%
Increase by more than 15%
Stay the same
Decrease by 1% to 15%
Decrease by more than 15%
n=1,167

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
4
Giving Tends to Follow the Economy
Source: Giving USA Foundation™, “GIVING USA 2013,” Lilly Family School of Philanthropy, Indiana University, 2013; Philanthropy Leadership Council interviews and analysis.
2011–2012 Giving Trends
1) Health organizations include: Health care institutions and services; mental health and crisis intervention; diseases, disorders, and medical disciplines; and medical research.
Total Charitable Giving and S&P 500 Index
1972-2012 (in billions of inflation-adjusted dollars)
8.9%Giving to health care organizations as a percent of total
1.5% Total increase in charitable giving
Increase in giving to health organizations12.8%

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
5
Taking the Donor Perspective
Three Lenses for Evaluating the Philanthropic Environment in Health Care
Source: Philanthropy Leadership Council interviews and analysis.
The Economy and Perception of Personal
Economic Security
Personal Motives and Perception of Value
and Impact
Hospital Performance and Perception of Need
in Health Care
Am I in the financial position to donate?
Is the organization a worthy cause?
Will my gift make a difference?
“MY CHECKBOOK” “THEIR STORY” “OUR IMPACT”
Donor-Centric Lenses

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
6
Other Headwinds Challenging Our Case for Support
Health Care Issues at the Forefront
Source: Philanthropy Leadership Council interviews and analysis.
Lens #2: “Their Story”
Increasing Transparency into Hospital Finances1
2
3
Politics of the Affordable Care Act
The Health System “Identity Crisis”
Top Three Case Vulnerabilities

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
7
That’s One Way to Sell Magazines
“Exposé” Shines Spotlight on Hospital Pricing
Issue #1: Increasing Transparency into Hospital Finances
“When you look behind the bills that Sean Recchi and other patients receive, you see nothing rational—no rhyme or reason—about the costs they faced in a marketplace they enter through no choice of their own. The only constant is the sticker shock for the patients who are asked to pay.”
Steven BrillTime Magazine
March 2013
”
Cited Examples of Hospital Pricing
BITTER PILLWHY MEDICAL BILLS
ARE KILLING USBY STEVEN BRILL
$77Box of sterile gauze pads
$1.50Single pill of
acetaminophen
$18One diabetes
test strip
Source: Brill S, “Bitter Pill: Why Medical Bills Are Killing Us,” Time, March 4, 2013; Advisory Board interviews and analysis. The TIME logo is the registered trademark of Time, Inc.

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
8
The PR Bombardment Continues
Health Care Costs Making National Headlines
Source: Clune S and Kane J, “Why Does Health Care Cost So Much in the United States?” PBS Newshour, November 25, 2011; Doyle J, “Hospital CEOs See Double-Digit Pay Hikes,” St. Louis Post-Dispatch, June 2, 2013; Evans M, “Use of CEO Compensation Comparisons Draws Heightened Scrutiny,” Modern Healthcare, May 11, 2013; Kavilanz P, “6 Reasons Health Care Costs Keep Going Up,” CNN Money, July 12, 2012; Kliff S, “Here’s Why Hospitals Set High Prices,” Washington Post, May 19, 2013; “Why Health Care Costs Are So High,” New York Times, June 3, 2013; Philanthropy Leadership Council interviews and analysis.
“Here’s Why Hospitals Set High Prices”Washington Post, 05/19/13“Use of CEO Compensation
Comparisons Draws Heightened Scrutiny”Modern Healthcare, 05/11/13
“Why Health Care Costs Are So High”New York Times, 06/03/13
“Why Does Health Care Cost So Much in the United States?”PBS Newshour, 11/25/11
“6 Reasons Health Care Costs Keep Going Up”CNN Money, 07/12/12
“Hospital CEOs See Double-Digit Pay Hikes”St. Louis Post-Dispatch, 06/02/13

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
9
COPD
Simpl
e Pne
umon
ia
Maj
or Jo
int R
epla
cem
ent
Minimum Maximum
1
2
CMS Fans the Flames on Hospital Pricing
New Database Profiles Charges for Most Frequent Discharges
Source: CMS, Medicare Provider Charge Data, May 2013, available at: www.cms.gov; Young J and Kirkham C, “Hospital Prices No Longer Secret As New Data Reveals Bewildering System, Staggering Cost Differences,” Huffington Post, May 8, 2013; Advisory Board interviews and analysis.
1) Chronic obstructive pulmonary disease.2) Simple Pneumonia and Pleurisy with complications and comorbidities.
“Our purpose for posting this information is to shine a much stronger light on these practices. What drives some hospitals to have significantly higher charges than their geographic peers? I don't think anyone here has come up with a good economic argument.”
Jonathan BlumDeputy Administrator, CMS
”Key Database Features
100 Most frequent discharges
163K Individual charges
3,337 Hospitals
Hospital Charge Variation
Chicago Hospital Referral Regionn=27
$5.8K
$28.3K
$12.7K
$39.4K $36.1K
$74.4K

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
10
Charges a Far Cry from Paid Prices
Most Pay Less than Fifty Cents on the Dollar
Source: 2012 Almanac of Hospital Financial and Operating Indicators , Optuminsight Inc, 2011; CDC, “National Hospital Discharge Survey,” 2010, available at: www.cdc.gov/nchs; Melnick GA and Fonkych K, “Hospital Pricing and the Uninsured: Do the Uninsured Pay Higher Prices?” Health Affairs, 2008, 27: w116-22; AHA, “Uncompensated Care Cost Fact Sheet,” January 2013, available at: http://www.aha.org; Advisory Board interviews and analysis.
The Rest of the Story
Hospital Revenue Received as Percentage of Charges
All Payers, 2010Discounts for Uninsured Patients
35.2%
43.6%
51.8% 5% Self-pay percent ofU.S. discharges, 2010
(28%)Median difference in collected price between uninsured, commercially-insured patients
$39.3B Uncompensated care provided by U.S. hospitals, 2010

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
11
Cross-Subsidy Economics on the Brink of Failure
Source: Advisory Board interviews and analysis.
1) Projected results for health care industry if hospitals do nothing to alter current course, based on the Health Care Advisory Board’s Margin Improvement Intensive that projects margin performance based on key financial and operational metrics from 158 hospitals.
Margin Improvement Analysis Results1
Five-Year Margin Projections Ten-Year Margin Projections
Greater than 10% Decline
5-10% Decline
Improvement
3%
13%
84%
Improvement
0-5% Decline
5-10% Decline
Greater than 10% Decline
15%
36% 36%
13%
Four Forces Eroding Future Margins
0-5% Decline
• Shifting payer mix: most demand growth over the next decade comes from publicly insured patients
• Continuing cost pressure: projected annualized commercial price growth half of historical norms
• Decelerating growth in reimbursement rates: commercial cost shifting stretched to the limit
• Deteriorating case mix: medical demand from aging population threatens to crowd out profitable procedures
!

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
12
Responding to “Sticker Shock”
Source: Philanthropy Leadership Council interviews and insights.
Talking Points for Donor Conversations
Emphasize that philanthropy has essential role to play in ensuring that hospitals can continue to serve their communities, especially as pressure increases on operating margins; know your institution’s operating margin
Be equipped to discuss the “community benefit” the institution provides, whether that is charity care for low-income patients, free wellness services and diagnostic screenings, or something else; know how much charity care and community benefit your institution provides each year
Explain that hospitals and health systems are facing more financial pressures than they ever have; be prepared to talk about cuts to Medicare, Medicaid payments and that the population is becoming more expensive to care for
If your operating margin is particularly healthy, reinforce the concept that, as not-for-profit institutions, hospitals reinvest profits into providing services rather than pay them out to shareholders; position philanthropic opportunities as sound financial investments

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
13
Other Headwinds Challenging Our Case for Support
Health Care Issues at the Forefront
Source: Philanthropy Leadership Council interviews and analysis.
Lens #2: “Their Story”
Increasing Transparency into Hospital Finances1
2
3
Politics of the Affordable Care Act
The Health System “Identity Crisis”
Top Three Case Vulnerabilities

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
274
97A
Not the Smoothest of Starts
Federal Exchange Slow to Answer the Bell

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
274
97A
Some State Exchanges Faring Better
15
Enrollment Slow, But Most Websites Working
Source: Kaiser Family Foundation, “State Decisions for Creating Health Insurance Exchanges, as of May 28, 2013,” available at: www.kff.org; CNBC, “One Washington gets Obamacare Right,” available at: http://www.cnbc.com/id/101096445, Kentucky Governor’s Office, “2.6 Million Page Views on Kynect for Affordable Health Insurance,” available at: http://migration.kentucky.gov/newsroom/governor/20131005kynect.htm; Health Care Advisory Board interviews and analysis.
State Decisions on Exchange Participation
16 States, District of Columbia Running Own Exchanges
27
17
7
State-Based ExchangeFederal
Exchange
Partnership Exchange
State Exchange Enrollment Within First Week of Launch
>40,000 Completed applications in New York
16,311 Completed applications in California
326 Completed applications in Maryland
12,955 Completed applications in Kentucky

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
274
97A
Post-Subsidy Premiums Within Reach for Many
16
But Penalties Still Smaller than Cost of Coverage
Observation #1: Affordable Premiums
Year Annual Penalty
2014 $95 or 1% of income
2015 $325 or 2% of income
2016 $695 or 2.5% of income
Penalties for Non-compliance
Annual Penalty
Income: $30,000
2014 2015 2016
$300
$600
$750
Source: Kaiser Family Foundation, “Kaiser Health Tracking Poll,” March 2013, available at: kff.org; PwC, “Health Insurance Exchanges: Long on Options, Short on Time,” October 2012, available at: www.pwc.com; Health Care Advisory Board interviews and analysis.
Weighted Average Monthly Premiums for Adult Individual Aged 27
For Second Cheapest Silver Plan, by State, 2014, Pre and Post subsidy1 for Income of $30,000
Tennessee Florida Mississippi Alaska
$154
$255 $286
$344
$154
$214 $214 $214
Before Subsidy After Subsidy

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
274
97A
Trading Price for Volume on the Public Exchanges
17
Reimbursement Information Still Anecdotal , but Rates Not Generous
Source: Mathews AW and Kamp J, “Another Big Step in Reshaping HealthCare,” Wall Street Journal, February 28, 2013, available at: www.online.wsj.com;; Health Care Advisory Board interviews and analysis.
Observation #2: Low Reimbursement
1) Pseudonym.
Anticipated Provider Reimbursement Rates for Exchange Plans
Catholic Health Initiatives
Modest discounts from commercial rates
Tenet Healthcare Up to 10% below commercial rates
Meriwether Hospital1
5% below commercial rates
WellPoint Inc.Between Medicare
and Medicaid rates
Meyers Health1
10% above Medicare rates
Millern Medical Center1
20% below commercial rates

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
274
97A
Lower Prices through Narrower Networks
18
Source: Covered California, “Health Plans & Rates for 2014: Making the Individual Market in California Affordable, May 23, 2013, available at: www.coveredca.com; Kliff S, “California Obamacare premiums: No ‘rate shock’ here,” Washington Post, May 23, 2013, available at: www.washingtonpost.com; Terhune C, “Insurers limit doctors, hospitals in state-run exchange plans,” LA Times, May 24, 2013, available at: www.articles.latimes.com; Health Care Advisory Board interviews and analysis.
Observation #3: Narrow Networks
1) Silver plan premiums for 40-year old individual, before subsidy; actual rates represent HMO plans in Northern Los Angeles.
Monthly Health Insurance Premiums
Cedars-Sinai Medical Center not participating in any exchange plan networks
UCLA Health System participating in only one exchange plan network
Prominent Health Systems Largely on the Sidelines
36% 80%13Blue Shield of
California network physicians in payer’s
exchange plans
California physicians, hospitals participating
in at least one exchange plan
Insurers offering plans on Covered
California exchange
5MIndividuals expected
to be eligible for Covered California
exchange, 2014
$450
$222 $254 $294
Actual Premiums
Select California Exchange Plans, 20141

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
274
97A
19
Employer-Sponsored Coverage at a Crossroads
Employers Choosing Between Abdication, Activation
“Activation”“Abdication”
Self-Funded Benefits
No Health Benefits
Pros:
• Full control over networks
• Exemption from minimum benefits requirements
Cons:
• Greater exposure to unexpected expenditures
• Complex network negotiations
Defined Contribution/Private Exchange
Pros:
• Health benefits still part of compensation package
• Predictable, controllable cost growth
Cons:
• Fundamental disruption in benefit design
• Employees may under-insure
Pros:
• Total escape from cycle of rising premium costs
Cons:
• Fine for violating employer mandate
• Loss of important labor market differentiator
Spectrum of Options for Controlling Health Benefits Expense
Source: Health Care Advisory Board interviews and analysis.

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
274
97A
20
Employers Already Scaling Back Coverage
Erosion of Employer-Sponsored Coverage Well Underway
Sources: Sonier J, et al., “State-Level Trends in Employer-Sponsored Health Insurance,” Robert Wood Johnson Foundation, April 2013, available at: www.rwjf.org; Collins R, et al., “Insuring the Future,” The Commonwealth Fund, April 2013, available at: www.commonwealthfund.org; Towers Watson, “Reshaping Health Care,” 2013, available at: www.towerswatson.com; Health Care Advisory Board interviews and analysis.
Individuals Covered by ESI1
23%Employers planning
to offer CDHP2 as only plan option, 2014
25%Insured non-elderly adults with deductibles $1,000
or higher, 2012
Non-elderly Population
2000 2011
69.7%
59.5%
11.5M fewer individuals
Contribution to Insurance Premiums
1) Employer-sponsored insurance.2) Consumer-directed health plan.
Coverage for Family of Four
$5,866
$2,137
$11,429
$4,316
2002 2012
Employer
2002 2012
Worker
95% growth
102% growth

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
274
97A
21
Some Employers Dodging Their Mandate
Despite Delay, Employers Finding Ways to Avoid Insurance Requirement
Source: Reynolds J and Merin J, “Business Leaders Give 2013 Outlook Mixed Reviews,” International Franchise Association, January 2013, available at: www.franchise.org; Mercer, “Health Reform Poses Biggest Challenges to Companies with the Most Part-Time and Low-Paid Employees,” August 8, 2012, available at: www.mercer.com; “Regal Entertainment Group Cuts Employee Hours, Explicitly Blames Obamacare in Memo: Report,” The Huffington Post, April 17, 2013, available at: www.huffingtonpost.com; Health Care Advisory Board interviews and analysis.
1) Full-time equivalents.2) n=72 franchisees, all industries.3) n=1,203 employers.
Case in Brief: Regal Entertainment Group
• In March 2013, reduced number of work shifts for non-salaried employees to ensure part-time status
• First public company to institute policy
31%Franchisees that plan to cut jobs to stay under 50-employee threshold2
32%Retail and hospitality companies that plan to “change workforce strategy” to avoid penalties3
Strategies to Avoid ACA Penalties
Cut jobs to remain under 50 FTEs1
Convert full-time employees to part-time status
Hire all new employees at part-time status
Split into smaller companies with fewer than 50 FTEs
Memo to Managers
To comply with the Affordable Care Act, Regal had to increase our health care budget to cover those newly deemed eligible based on the law's definition of a full time employee. To manage this budget, all other employees will be scheduled in accord with business needs and in a manner that will not negatively impact our health care budget…

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
274
97A
22
New Path for Employer Cost Shifting
Private Health Insurance Exchanges Open for Business
Source: Towers Watson, “18th Annual Towers Watson Employer Survey on Purchasing Value in Health Care,” 2013, available at: www.towerswatson.com; Wall JK, “Mercer Courts Employers with Private Exchange,” Indianapolis Business Journal, April 22, 2013, available at: www.ibj.com; Health Care Advisory Board interviews and analysis.
Responding to Market Demands
“The high-caliber carrier participation in Mercer’s private benefits exchange matches the increasing interest displayed by our clients and prospects.”
Julio A. Portalatin President and CEO, Mercer
”
15%Employers considering
private exchange model for 2014
Private Health Insurance Exchanges
• Over 100,000 employees enrolled in Aon Hewitt’s private health insurance exchange in fall 2012
• Benefits offered by nine national, regional carriers
• Launching private health insurance exchange in nine states
• Expect to serve employers covering approximately 30,000 individuals
• Offering suite of exchange offerings to employers
• Will include coverage from 10 major insurers

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
274
97A
23
Igniting a Race to the Bottom
Exchange Shoppers Trading Premiums for Deductibles
Source: Mathews AW, “To Save, Workers Take On Health-Cost Risk,” Wall Street Journal, March 17th, 2013, available at: www.wsj.com; Health Care Advisory Board interviews and analysis.
1) Preferred provider organization.2) Health maintenance organization.
Case in Brief: Sears, Darden Restaurants
• For 2013 open enrollment, self-insured large employers redesigned benefits to reduce health spend through defined contribution model
• Employers offered employees lump sum credit to choose coverage in Aon Hewitt’s online marketplace
2013
2012
47%
70%
14%
18%
39%
12%
PPO HMO
High-Deductible Plan1 2
42%Employees on Aon Hewitt health
insurance exchanges selecting plans less rich than the previous year
Results of Open Enrollment Process

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
274
97A
24
The Future of Employer-Sponsored Insurance?
Private Exchanges Poised For Rapid Growth
2014 2015 2016 2017 2018
1M
9M
19M
30M
40M
Projected Private Exchange Enrollment
27%Percentage of consumers receiving
employer-sponsored coverage today projected to receive benefits through
private exchanges in 2018
Factors Influencing Move to Private Exchange Models
Logistical difficulty of benefit renegotiations
Internal politics of benefit changes
Attractiveness of other options
Source: Accenture, “One-in-Four Consumers Will Receive Employer Health Benefits Through Insurance Exchanges in Five Years, Accenture Research Shows,” available at: http://newsroom.accenture.com/news/one-in-four-consumers-will-receive-employer-health-benefits-through-insurance-exchanges-in-five-years-accenture-research-shows.htm, Health Care Advisory Board interviews and analysis.

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
274
97A
25
Reexamining the ACA “Grand Bargain”
Source: CBO, “Letter to the Honorable John Boehner Providing an Estimate for H.R.6079, The Repeal of Obamacare Act,” July 24, 2012, available at: www.cbo.gov; CBO, “Effects of the Affordable Care Act on Health Insurance Coverage—February 2013 Baseline,” February 5, 2013, available at: www.cbo.gov; Advisory Board interviews and analysis.
1) Non-elderly population.2) Disproportionate Share Hospital.
ACA Hospital Payment Cuts
2013-2023
2013 2014 2015 2016 2017 2018
2M
14M
20M
26M27M 27M
Projected Cumulative Increase in Newly Insured Population1
Provider “Get”: Higher Revenue
• Medicaid expansion• Insurance exchanges • Employer mandate
Provider “Give”: Lower Payment
• Medicare rate cuts• DSH cuts
$260B
$316B
$56B
2DSH2 Payment Cuts

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
274
97A
26
Divided Public Opinion of Health Care ReformOpponents Taking Stronger Stance
Source: Ramlet M and Dropp K, “Memo on the Poll Findings – Public Opinion on the Affordable Care Act,” June 12, 2013, available at: www.themorningconsult.com, accessed June 14, 2013; Philanthropy Leadership Council interviews and insights.
Do You Approve or Disapprove of the Affordable Care Act?
8%
20%
23%
41%
Strongly approve
Somewhat approve
Somewhat disapprove
Strongly disapprove 5%
15%
23%
11%
33%
How Do You Think the Affordable Care Act Will Affect You and Your Family?
June 2013
n=1,000
June 2013
n=1,000

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
274
97A
27
Common Sentiments from Million-Dollar Health Care Donors
Many Donors Interested, but Uncertain
Source: Philanthropy Leadership Council interviews and insights.1) Pseudonym.
“Health care has become too political, and I’ll be on the sidelines until things are sorted out.”
“I defy anyone to make sense of the current medical care situation.”
“It’s hard to plan when you don’t know what the future is.”
“We don’t know what’s going to happen. The hospital president went to a meeting [about health care reform], and he came out more confused than before. Nobody has their finger on the pulse.”
Typi
cal S
essio
n
Health
Car
e Ref
orm
Ses
sion
50
220
Attendance at Biannual Donor Educational Sessions at Odair Health System1
”

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
274
97A
28
Coverage Expansion Reducing Perception of NeedLess Charity Care Provided, Less Charity Required
Source: CBO, “Effects of the Affordable Care Act on Health Insurance Coverage—February 2013 Baseline,” February 5, 2013, available at: www.cbo.gov; Philanthropy Leadership Council interviews and analysis.1) Non-elderly population.
A Threat to Giving?
“If everybody would truly be able to receive treatment under ObamaCare, it probably would at that point impact what we may be giving. People will already be covered, and we’re probably going to be taxed a lot more to get to that point anyway.”
Million-dollar health care donor”
Projected Cumulative Increase in Newly Insured Individuals1
2013 2014 2015 2016 2017 2018
2M
14M
20M
26M27M 27M

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
29
Key to Emphasize Local Impact
Most Large Gifts to Health Care Organizations Stay Local
Source: “The Million Dollar Gift Next Door,” Indiana University Lilly Family School of Philanthropy, April 17, 2013; Philanthropy Leadership Council interviews and analysis.1) Geographic regions include Northeast, Midwest, South, and West.
60%
7%
33%
Within the donor’s state or geographic region1
Outside the donor’s geographic region1
Unidentified
Geographic Distribution of $1M+ Gifts
2000–2011
n=20,941 gifts

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
30
Other Headwinds Challenging Our Case for Support
Health Care Issues at the Forefront
Source: Philanthropy Leadership Council interviews and analysis.
Lens #2: “Their Story”
Increasing Transparency into Hospital Finances1
2
3
Politics of the Affordable Care Act
The Health System “Identity Crisis”
Top Three Case Vulnerabilities

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
31
What Business Are We In?
Businesses Displaced by Focusing on the Means Rather than the Ends
Study in Brief: What Business Are We in?
• Explores how Eastman Kodak Company’s camera and film business was displaced by alternate mediums that fulfilled customers’ desires for images
• Draws parallels to the challenges that provider organizations face in shifting activities from delivering health services to a broader spectrum of tactics for health
Providing Health, Not Health Care
“…It's always better to define a business by what consumers want than by what a company can produce…whereas doctors and hospitals focus on producing health care, what people really want is health. Health care is just a means to that end—and an increasingly expensive one.”
Source: Asch D., "What Business Are We In? The Emergence of Health as the Business of Health Care,” NEJM, 367,2012: 888-889; Advisory Board interviews and analysis.
”
197690% market share of commercial film business
1990sDigital cameras enter mainstream market
2012Kodak files for bankruptcy
Timeline for Eastman Kodak Business
Researchers featured in New England Journal of Medicine

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
32
Health System Strategy, c. 2003
“Extractive Growth”
Health System Strategy, 2013-2023
“Value-Based Growth”
Grow by being bigger: Leverage market dominance to secure prime pricing, network status
Grow by being better: Leverage cost, quality, service advantage to attract key decision makers
• Expand market share• Strengthen service lines• Exert pricing leverage
• Solidify referrals• Secure physicians• Increase utilization
• Expand covered lives• Compete on outcomes• Minimize total cost
• Assemble network• Offer convenience• Expand access
• Discharges• Service line share• Fee-for-service revenue
• Pricing growth• Occupancy rate• Process quality
• Share of lives• Geographic reach• Risk-based revenue
• Share of wallet• Outcomes quality• Total cost of care
• Inpatient capacity• Outpatient imaging
centers
• Clinical technology• Ambulatory surgery
centers
• Primary care capacity• Care management staff
and systems
• IT analytics• Post-acute care
network
Toward an Economics of Value
Adapting to New Rules of Competition
Source: Advisory Board interviews and analysis.
Description
Key Success Factors
Performance Metrics
Critical Infrastructure

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
33
Carving a New Growth Path
Competing Under Distinct, but Not Mutually Exclusive, Identities
Source: Advisory Board interviews and analysis.
Best-in-Class Acute Care Destination
Consumer-Oriented Ambulatory Network
Full Service Population Health Manager
Integrated Finance and Delivery System
• Assumes full risk by offering health plan to subscribers
• Unifies care financing and delivery into single coordinated care enterprise
• Maintains extensive network of outpatient care sites
• Offers convenient primary care, diagnostic, procedural services at competitive prices
• Assumes delegated risk from payers and/or employers
• Prioritizes care management, coordination to limit avoidable demand
• Consistently delivers efficient, effective acute care episodes
• Ensures reliable coordination, communication, data sharing across the care continuum
Four Emerging Provider Identities

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
34
Fundraising’s Role in Carving a New Growth Path
What Can You Make the Case For?
Source: Philanthropy Leadership Council interviews and analysis.
• Outpatient clinics
• Primary care offices
• Post-acute care facilities
• Outpatient lab, imaging centers
• EMR, meaningful use
• Employee utilization liaisons
• Inpatient care coordinators
Investment Priorities
• Outpatient clinics
• Outpatient care managers
• Clinical patient guides
• Disease management
• Palliative care
• Non-urgent care navigators
• Transition partners
• EMR, meaningful use
• Telemonitoring services
• Home health initiatives
• Primary care offices
• Outpatient lab, imaging centers
• Wellness centers
• EMR, meaningful use
Best-in-Class Acute Care Destination
Consumer-Oriented Ambulatory Network
Full Service Population Health Manager
Integrated Finance and Delivery System
• IT systems
• Cash/unrestricted funds

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
35
Taking the Donor Perspective
Three Lenses for Evaluating the Philanthropic Environment in Health Care
Source: Philanthropy Leadership Council interviews and analysis.
The Economy and Perception of Personal
Economic Security
Personal Motives and Perception of Value
and Impact
Hospital Performance and Perception of Need
in Health Care
Am I in the financial position to donate?
Is the organization a worthy cause?
Will my gift make a difference?
“MY CHECKBOOK” “THEIR STORY” “OUR IMPACT”
Donor-Centric Lenses

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
36
Focusing on What We Can Control
Source: Philanthropy Leadership Council interviews and analysis.
Lens #3: “Our Impact”
“You feel like it’s just not fundraising
as it is solving a problem.”
Underlying Values Desire for Impact
“I do believe that we need to give; those of us that have, we need to help.”
“Charitable giving for us is really from following what the Lord has taught us… where much is given, much is expected.”
“Blaming the government and taxes is just an excuse for not acting.”
“We can afford it, and I’m a great believer in giving while I’m living.”
“We want to give all our money away while we’re still young enough to appreciate the impact … it’s such a joy to see how lives are changed.”

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
37
Revisiting the Conversation About Impact
Source: Philanthropy Leadership Council interviews and analysis.
Donor Comprehension Barriers
Reframed Donor Perspective
A Bridge Too Far
Priorities focused outside hospital sphere
Institutional Priority
Non-traditional but current priorities of broader health system
IntangibleConcept lacks physical manifestation
Concrete Initiative
Easily articulated explanation
Far Removed
Impact several steps away from meaningful donor experience
Direct Impact
Affecting lives of people throughout community

©20
13 T
he A
dvis
ory
Boa
rd C
ompa
ny •
271
03A
38
Elevating Philanthropy’s Strategic Value
Translate Our Relevance and Impact to Key Stakeholders
Source: Philanthropy Leadership Council interviews and analysis.
Providing 360° Value
Clinicians
Donors
Executives
Foundation