N2100 renal lecture spring 2014 voice over
42
RENAL FAILURE: Prevention, Chronic, Acute
-
Upload
robinaustin12 -
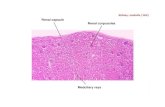
Category
Health & Medicine
-
view
311 -
download
0
description
Nursing Lecture N2100 Renal Unit
Transcript of N2100 renal lecture spring 2014 voice over
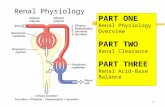
- 1. Homeostasis: acidbase, BP Excrete urea, toxins, water Produce Erythropoetin (hormone that stimulates RBC production) Produce Renin (reninangiotensin system regulates BP) Convert Vitamin D into useable form Think about the nursing implications of each!
2. Two thirds of all chronic kidney disease is related to other chronic illnesses. Diabetes (43%) Hypertension (23%) 1)Why and how do each of these conditions damage the kidney?2) What can be done to prevent or manage these underlying conditions? 3. Nephrotoxic Drugs: -Aminoglycosides: Ex. gentamycin, tobramycin, amikacin, neomycin -Amphotericin B -VancomycinChronic use of NSAIDS (especially cardiac patients and patients with cirrhosis) Patients with Creat > 2.0 who receive radiopaque contrast dye 4. Glomerular filtration rate (GFR) is a test used to check how well the kidneys are working.Specifically, it estimates how much blood passes through the tiny filters in the kidneys, called glomeruli, each minute. The GFR test measures how well your kidneys are filtering a waste called creatinine, which is produced by the muscles.When the kidneys aren't working well, creatinine builds up in the blood.Normal results range from 90 - 120 mL/min/1.73 m2 5. Lab values Measuring kidney functionSerum Creatinine Creatinine is a product of creatine metabolism from muscle dependent of muscle mass Creatinine is eliminated primarily by glomerular filtration (GFR). As GFR , serum creatinine . Doubling of creatinine suggests a 50% drop in GFR (estimated). 6. Acute/Chronic Postinfection causes - Group A betahemolytic strep infection of throat Nursing Management 7. Characteristic of glomerular injury from diabetets, infections, renal toxins, immune disorders. Excretion of 3.5 g or more of protein in the urine per day. Loss of serum proteins and sodium retention 8. Glomerular capillaries are damaged Leads to increased permeability to proteins Decreased osmotic pressure leads to proteinuria, hypoalbuminemia, and edema. MAY LEAD TO RENAL FAILURE..PREVENTION OF CAUSES IS CRITICAL!!! 9. Progressive loss of renal function Associated with systemic disease such as hypertension, diabetes mellitus, intrinsic kidney disease.Diabetes (40%), Hypertension (25%), and Glomerulonephritis (10%)Kidney damage as GFR less than 60 ml/min/1.73m2 for 3 months or more. 10. Altered fluid status and electrolytes Nutritional abnormalities Anemia Secondary hyperparathyroidism 11. Management and goals: Restrict dietary protein Intensive insulin therapy if needed Optimize BP control (tight regulation) Goal for CKD BP 130/85 Goal for Proteinuria BP 125/75Manage hyperlipidemia Goal of LDL - 90), At risk Stage 2: Kidney damage with mild decrease in GFR (60-89), Chronic Renal Insufficiency or CRI Stage 3: Moderate decrease in GFR (30-59), CRI or CRF (Chronic Renal Failure) Stage 4: Severe decrease in GFR (15-29), CHF Stage 5: Kidney Failure, GFR < 15, more than 90% of nephrons have lost function, ESRDEnd Stage Renal Disease, dialysis or transplant required to survive. 13. Rapid loss of renal function, progressive azotemia (accumulation of nitrogenous waste products such as BUN) and increasing serum creatinine. Uremia (literally urine in the blood) is a condition in which renal function declines to the point that symptoms develop in multiple body systems. Often associated with Oliguria (output less than 400 ml/day) In 30% of cases there is a normal or increased urinary output Oliguric patients have a higher mortality rate Develops over hours or days with progressive elevation of BUN, creatinine, and K+. ARF follows severe, prolonged hypotension or hypovolemia or exposure to a nephrotoxic agent, also can be due to obstruction of urine outflow.THINK PREVENTION!!! 14. 1. PRERENALImpaired renal perfusion(shock, hypovolemia, volume shifts, CO, PVR, renal artery obstruction)2. INTRARENALInvolves parenchymal changes (renal trauma,acute tubular necrosis, infectious diseases, glomerulonephritis)3. POSTRENALObstruction to urinary tractprostate disease, obstruction, spinal cord injury, pelvic trauma) 15. 1. INITIATING PHASE Begins at time of insult until S&S seen (hours to days) 2. OLIGURIC or ANURIC PHASE Oliguria caused by GFR decrease Begins 1-7 days after insult depending on cause Usually lasts usually 10-14 days (may last up to 8 weeks) Longer the phase, poorer prognosis of renal recovery Manifestations are changes in UOP, fluid & electrolyte balances, & uremia in serum levels of urea, creatinine, uric acid, K+ & Mg 16. Acute Renal Failure Stages 3. DIURETIC PHASE -Gradual increase of UOP can reach 1-2 (or more) L per day. Nephrons are still not fully functional -Caused by osmotic diuresis and inability of tubules to concentrate. -Recovered ability to excrete wastes, but not concentrate. -Monitor for hypokalemia, hyponatremia & dehydration -Hypovolemia and hypotension can occur Lasts 1-3 weeks -Acid-base, electrolyte and waste product levels begin to normalize. 17. 4. RECOVERY PHASE Begins when GFR increases allowing BUN and creatinine to reach a plateau and decrease May still have glycosuria and decreased ability to concentrate urine Major improvements first 1-2 weeks but may take 12 months to stabilize. 18. May excrete as much as 2L/day Urine dilute and iso-osmolar Hypertension and tachypnea and symptoms of fluid overload are usually seen Can see orthostatic hypotension and dry mucous membranes Associated with less morbidity and mortality 19. Urinalysis hemoglobin + in pylonephritis, protein + in diabetic nephropathy, glomerulonephritis, WBC (pyuria) + in infectionSpecific gravity of urine 1.001-1.035 Sodium levels -serum: 135-145 mmol/L -urine (usually 24 hour collection): 27-287mmol/dHematocrit Serum Creatinine .6-1.2 mg/dL BUN 8-21, 10-31 if older than 90 Urine Creatinine & Creatinine Clearance: Determines extent of nephron damage (decreased when 50% of nephrons lost) 20. -Treat cause -Maintain fluid and electrolyte balance -Prevent infection -Monitor for arrhythmias (related to K+and other electrolyte imbalances) -Maintain nutritional status Adequate protein (or restriction) depending oncatabolism Restriction of K+, phosphate, magnesium, and/or sodium Dietary fat 30-40% total calories If necessary, use TPN and/or Ca supplements, phosphate-binders 21. Protein: limit protein pre-dialysis (this slows progression of renal failure). During dialysis, protein is lost so patient will require more protein. Concentrate on high value protein (dairy and meat). Potassium: limit due to hyperkalemia, especially if on dialysis. Salt: restrict use of salt due to renal damage from ongoing hypertension. (canned goods, processed foods, fast foods,, table salt). Make sure salt substitute does not contain potassium. Phosphorus: elevated in patients with renal disease. (dairy products, yogurt, eggs) Fluid restriction: carefully follow restrictions 22. Fluid and electrolyte imbalance Susceptibility to secondary infections Anemia Platelet dysfunction Gastrointestinal (GI) complications Uremic encephalopathy Impaired wound healing Alteration in urine outputConsider the role of the nurse in the prevention and management of each of these! 23. Fluid volume deficit r/t (name cause or causes) Fluid volume excess r/t inability of kidneys to produce urineRisk for infection Disturbed thought processes Fatigue Anxiety 24. Monitor intake & output Assess vital signs Daily weights Evaluate skin turgor, mucous membranes Monitor dialysis site Monitor lab values (UA, Specific gravity, Sodium levels, BUN, & Serum creatinine*)(*best indicator of renal function, not altered by other temporary factors) Monitor urine (amount,color, specific gravity, glucose, protein, sediment, blood) Monitor for pain, bleeding, and neuro status/seizures Monitor for murmurs & dysrhythmias Prevent infection Frequent oral care Monitor lung sounds, pulmonary toilet Restrict fluids Education! 25. The last stage of kidney failure where GFR is