Myelodysplastic Syndromes: Review of Pathophysiology · PDF fileMyelodysplastic Syndromes:...
18
Current Cancer Drug Targets, 2007, 7, 541-558 541 1568-0096/07 $50.00+.00 © 2007 Bentham Science Publishers Ltd. Myelodysplastic Syndromes: Review of Pathophysiology and Current Novel Treatment Approaches E.D. Warlick* and B.D. Smith Hematologic Malignancies Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins 1650 Orleans Street, room 246 Baltimore, MD 21231, USA Abstract: Myelodysplastic syndromes (MDS) are a heterogeneous group of clonal disorders of hematopoietic progenitors manifest by cytopenias, bleeding, infection, and potential for progression to acute myelogenous leukemia. The wide spectrum of clinical manifestations, including variability in illness severity and potential for progression, suggest that myelodysplastic syndromes encompass a multitude of disorders, likely involving numerous pathologic pathways. In fact, it is the effort to understand the underlying biology of these syndromes that has led to recent advances in treatment approaches, including the FDA approval of three new agents (5-azacitidine, decitabine, and lenalidomide) for the treatment of MDS. This review will present data supporting each of the current pathophysiologic pathways implicated in the development and progression of MDS; summarize the emerging clinical paradigms for treating patients with MDS; and offer insights into several novel approaches attempting to improve treatment options for future MDS patients. Keywords: Myelodysplastic syndrome, pathophysiology, differentiation therapy, epigenetic therapy, bone marrow transplantation, immunomodulation. INTRODUCTION Myelodysplastic syndromes (MDS) are a complex and heterogeneous group of bone marrow failure disorders characterized by ineffective hematopoiesis. This dysfunctional blood cell production is manifest by peripheral cytopenias, marked morphologic dysplasia, and cellular dysfunction resulting in an increased risk of infection and need for transfusions in most MDS patients. In the general population, the incidence of MDS is approximately 2-10 cases per 100,000 people with the incidence rising to approximately 50 cases per 100,000 people over age 70 [1]. The median age at presentation approaches 70 with a slight male predominance of unknown clinical significance. Traditionally, MDS is characterized as either primary (idiopathic) or secondary with exposure to benzene [2], occupational chemicals [3], or prior treatment with radiation [4] or chemotherapy agents [5] well documented secondary causes. Additional data implicates exposure to tobacco [6], excessive alcohol [7], viral infections [8], or autoimmune disorders [9] as potential associations with MDS. Alterations in many individual biologic pathways have been implicated in MDS pathophysiology. However, the generally accepted primary hypothesizes involves an initial deleterious genetic event within a hematopoietic stem cell, subsequent development of excessive cytokines/inflammatory response leading to a pro- apoptotic/proliferative state, and resultant peripheral cytopenias despite a hypercellular bone marrow. The presence of detectable cytogenetic abnormalities in approximately 40-70% of patients with primary MDS and over 80% with secondary MDS [10] as well as the validated prognostic value of cytogenetic data in MDS supports the theory of an incident genetic event. Specifically, good prognostic cytogenetic groups (“5q minus syndrome” or deletion of the long arm of chromosome 20 (20q)) are typically associated with more indolent MDS that requires less intensive therapy while poor prognostic cytogenetic groups (loss of chromosome 5 or 7 or complex abnormalities) have a more aggressive course and are often poorly responsive even to aggressive treatments [11]. The variable response to treatment and course of disease correlating with cytogenetic findings suggests likely differential behavior of the MDS clone: differentiation arrest and a pro-apoptotic cytokine state in low risk cytogenetic cohorts versus a state of proliferative advantage, possibly due to underlying genomic instability or via altered gene expression silencing of DNA repair or tumor suppressor genes, in high risk *Address correspondence to this author at the Hematologic Malignancies Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins 1650 Orleans Street, room 246 Baltimore, MD 21231, USA; Tel: (410) 614-5068; Fax: (410) 614-7437; E-mail: [email protected] cohorts [12-14]. Additionally, altered immune surveillance potentially creates an environment where the transformation to acute leukemia becomes possible [15]. The pathophysiology of “low” and “high” grade MDS is slowly being incorporated into the evolving classification hierarchies as well as treatment paradigms. CLASSIFICATION SYSTEMS Throughout the years, various classification systems have been developed to describe myelodysplastic syndromes. There is no clear “best” schema, yet the numerous revisions and expansions based on the ongoing understanding of MDS pathophysiology and clinical outcomes are notable improvements. FAB Morphologic Classification The initial FAB (French-American British) system was developed by an international group of clinicians and pathologists in the mid 1970’s, refined in 1982, and primarily used cellular morphology to define the MDS subgroups focusing on bone marrow blast percentage, the presence or absence of monocytosis, and the presence or absence of ringed sideroblasts. These morphologic findings, aligned with important prognostic outcomes, were eventually divided into four groups:1) Lower-risk MDS (RA and RARS) with a median survival of 4-5 years and low risk of AML transformation; 2) Intermediate-risk MDS (RAEB) with a median survival close to 1 year; 3) Higher-risk MDS (RAEBt) with a median survival measured in months and a very high risk of AML transformation; and 4) CMML associated with a wildly variable risk [16,17]. The FAB classification served as the first framework to systematically identify and describe the different clinical entities of MDS. However, the FAB system was limited by lack of cytogenetic and molecular information now commonly available, and did not adequately accommodate hypoplastic MDS, MDS with myelofibrosis, and other overlap syndromes [18, 19]. WHO Classification More recently, in 1999, the World Health Organization (WHO) proposed a newer classification system attempting to address some of the limitations of the FAB system [20]. The main goal of this schema was to formally incorporate biologic data, specifically cytogenetic and molecular findings, clinical outcomes, and number of dysplastic lineages involved, in order to better separate subgroups and delineate syndromes within the previous FAB classification. Notably, the WHO classification recognized the unique “5q- syndrome” and CMML within their own categories, lowered the blast percentage defining AML to 20% and eliminated the RAEBt category, assigned
-
Upload
nguyenngoc -
Category
Documents
-
view
216 -
download
0
Transcript of Myelodysplastic Syndromes: Review of Pathophysiology · PDF fileMyelodysplastic Syndromes:...

Current Cancer Drug Targets, 2007, 7, 541-558 541
1568-0096/07 $50.00+.00 © 2007 Bentham Science Publishers Ltd.
Myelodysplastic Syndromes: Review of Pathophysiology and Current Novel Treatment Approaches E.D. Warlick* and B.D. Smith
Hematologic Malignancies Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins 1650 Orleans Street, room 246 Baltimore, MD 21231, USA
Abstract: Myelodysplastic syndromes (MDS) are a heterogeneous group of clonal disorders of hematopoietic progenitors manifest by cytopenias, bleeding, infection, and potential for progression to acute myelogenous leukemia. The wide spectrum of clinical manifestations, including variability in illness severity and potential for progression, suggest that myelodysplastic syndromes encompass a multitude of disorders, likely involving numerous pathologic pathways. In fact, it is the effort to understand the underlying biology of these syndromes that has led to recent advances in treatment approaches, including the FDA approval of three new agents (5-azacitidine, decitabine, and lenalidomide) for the treatment of MDS. This review will present data supporting each of the current pathophysiologic pathways implicated in the development and progression of MDS; summarize the emerging clinical paradigms for treating patients with MDS; and offer insights into several novel approaches attempting to improve treatment options for future MDS patients.
Keywords: Myelodysplastic syndrome, pathophysiology, differentiation therapy, epigenetic therapy, bone marrow transplantation, immunomodulation.
INTRODUCTION Myelodysplastic syndromes (MDS) are a complex and heterogeneous group of bone marrow failure disorders characterized by ineffective hematopoiesis. This dysfunctional blood cell production is manifest by peripheral cytopenias, marked morphologic dysplasia, and cellular dysfunction resulting in an increased risk of infection and need for transfusions in most MDS patients. In the general population, the incidence of MDS is approximately 2-10 cases per 100,000 people with the incidence rising to approximately 50 cases per 100,000 people over age 70 [1]. The median age at presentation approaches 70 with a slight male predominance of unknown clinical significance. Traditionally, MDS is characterized as either primary (idiopathic) or secondary with exposure to benzene [2], occupational chemicals [3], or prior treatment with radiation [4] or chemotherapy agents [5] well documented secondary causes. Additional data implicates exposure to tobacco [6], excessive alcohol [7], viral infections [8], or autoimmune disorders [9] as potential associations with MDS. Alterations in many individual biologic pathways have been implicated in MDS pathophysiology. However, the generally accepted primary hypothesizes involves an initial deleterious genetic event within a hematopoietic stem cell, subsequent development of excessive cytokines/inflammatory response leading to a pro-apoptotic/proliferative state, and resultant peripheral cytopenias despite a hypercellular bone marrow. The presence of detectable cytogenetic abnormalities in approximately 40-70% of patients with primary MDS and over 80% with secondary MDS [10] as well as the validated prognostic value of cytogenetic data in MDS supports the theory of an incident genetic event. Specifically, good prognostic cytogenetic groups (“5q minus syndrome” or deletion of the long arm of chromosome 20 (20q)) are typically associated with more indolent MDS that requires less intensive therapy while poor prognostic cytogenetic groups (loss of chromosome 5 or 7 or complex abnormalities) have a more aggressive course and are often poorly responsive even to aggressive treatments [11]. The variable response to treatment and course of disease correlating with cytogenetic findings suggests likely differential behavior of the MDS clone: differentiation arrest and a pro-apoptotic cytokine state in low risk cytogenetic cohorts versus a state of proliferative advantage, possibly due to underlying genomic instability or via altered gene expression silencing of DNA repair or tumor suppressor genes, in high risk
*Address correspondence to this author at the Hematologic Malignancies Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins 1650 Orleans Street, room 246 Baltimore, MD 21231, USA; Tel: (410) 614-5068; Fax: (410) 614-7437; E-mail: [email protected]
cohorts [12-14]. Additionally, altered immune surveillance potentially creates an environment where the transformation to acute leukemia becomes possible [15]. The pathophysiology of “low” and “high” grade MDS is slowly being incorporated into the evolving classification hierarchies as well as treatment paradigms.
CLASSIFICATION SYSTEMS Throughout the years, various classification systems have been developed to describe myelodysplastic syndromes. There is no clear “best” schema, yet the numerous revisions and expansions based on the ongoing understanding of MDS pathophysiology and clinical outcomes are notable improvements.
FAB Morphologic Classification The initial FAB (French-American British) system was developed by an international group of clinicians and pathologists in the mid 1970’s, refined in 1982, and primarily used cellular morphology to define the MDS subgroups focusing on bone marrow blast percentage, the presence or absence of monocytosis, and the presence or absence of ringed sideroblasts. These morphologic findings, aligned with important prognostic outcomes, were eventually divided into four groups:1) Lower-risk MDS (RA and RARS) with a median survival of 4-5 years and low risk of AML transformation; 2) Intermediate-risk MDS (RAEB) with a median survival close to 1 year; 3) Higher-risk MDS (RAEBt) with a median survival measured in months and a very high risk of AML transformation; and 4) CMML associated with a wildly variable risk [16,17]. The FAB classification served as the first framework to systematically identify and describe the different clinical entities of MDS. However, the FAB system was limited by lack of cytogenetic and molecular information now commonly available, and did not adequately accommodate hypoplastic MDS, MDS with myelofibrosis, and other overlap syndromes [18, 19].
WHO Classification More recently, in 1999, the World Health Organization (WHO) proposed a newer classification system attempting to address some of the limitations of the FAB system [20]. The main goal of this schema was to formally incorporate biologic data, specifically cytogenetic and molecular findings, clinical outcomes, and number of dysplastic lineages involved, in order to better separate subgroups and delineate syndromes within the previous FAB classification. Notably, the WHO classification recognized the unique “5q- syndrome” and CMML within their own categories, lowered the blast percentage defining AML to 20% and eliminated the RAEBt category, assigned

542 Current Cancer Drug Targets, 2007, Vol. 7, No. 6 Warlick and Smith
patients with characteristic AML-associated chromosomal abnormalities to AML regardless of blast percentage, and used the percentage of marrow blasts to divide RAEB into two groups noting that patients with >10% blasts had a shorter survival and increased transformation to acute leukemia compared to patients with <10% [20]. The WHO system also distinguished MDS patients with <5% marrow blasts between those with multilineage dysplasia (worse outcome) and those with erythroid-only dysplasia (better outcome), and added an “unclassifiable MDS” category [19-21]. Although the WHO classification system built on the FAB foundation by including important biologic and clinical data, there remained some obvious shortcomings such as the “MDS-unclassifiable” category and controversies such as the elimination of RAEBt [18]. These concerns epitomize the larger problem that “MDS” is truly a pleomorphic “grab bag” term for multiple disorders that offer significant challenges to both physicians treating patients as well as scientists studying these disorders.
IPSS Prognostic Classification In 1997, Peter Greenberg and colleagues proposed a plan to combine known prognostic variables with outcomes data from seven large, risk-based studies in an effort to determine the most important variables for assigning prognosis to MDS patients. The International Prognostic Scoring System (IPSS) emerged from the analysis of this data from nearly 900 MDS patients and represents the best effort to date for prediction of prognosis and outcome. The variables most predictive of prognosis included percentage bone marrow blasts, cytogenetic abnormalities, and number of peripheral cytopenias. Subsequent IPSS score calculation then assigns patients to one of four risk groups: Low, Intermediate-1 (INT-1), Intermediate-2 (INT-2), and High risk with decreasing survival and increasing risk of AML progression as the score increases [22]. Like each of the classification schemas, the IPSS also has limitations including failure to offer prognostic points for treatment-related MDS (t-MDS) or CMML, and lack of scoring for most of the cytogenetic abnormalities commonly found in MDS. These limitations aside, the IPSS remains a paramount tool in predicting prognosis, categorizing patients for studies, and analyzing treatment outcomes. In combination with the other classification systems, it represents the most quantitative assignment of MDS risk available.
THEORIES IN MDS PATHOPHYSIOLOGY Better understanding of the underlying MDS biology is crucial for the development of better treatments for individual patients. It is commonly accepted that MDS develops through a multi-step process encompassing changes within the hematopoietic stem cell, the bone marrow microenvironment, and the complex interactions between the two [1, 15, 18, 23, 24]. Below we survey specific theories and pathways implicated in the pathogenesis and progression of MDS divided into five major categories: 1) cellular damage related to toxic environmental exposures and cellular aging; 2) genetic alterations including loss or gain of function due to both cytogenetic and epigenetic abnormalities (Table I); 3) changes in the bone marrow microenvironment; 4) dysregulation of the immune system; and 5) altered cell cycle regulation and blocked differentiation. (Theories Summarized in Table II)
Cellular Damage: Toxic Environmental Exposures and Cellular Aging The epidemiology of MDS has offered pivotal links between various environmental exposures, aging, and the development of disease, namely the accumulation of DNA damage. Numerous environmental exposures have been associated with the development of MDS including tobacco [6] and alcohol use [7], infections [8], or auto-immune disorders [9]; however, the classic example linking an environmental toxin exposure to MDS development is highlighted
from the observational case control studies involving benzene, an aromatic hydrocarbon and organic solvent derived from petroleum-refining, used in many occupational compounds [25]. The association, first described in Turkish shoe workers who developed bone marrow failure/pancytopenia states, [26] lead to further prospective cohort studies involving 74,828 benzene exposed subjects in China and revealed a significantly increased relative risk of MDS development approaching infinity [2]. The potential mechanisms of MDS development in benzene-exposed individuals have been described in two contexts: genotoxic and non-genotoxic. Genotoxic mechanisms are characterized by the generation of oxygen free radicals from benzene metabolites with subsequent DNA damage and apoptosis [27, 28]. Support for this mechanism includes the findings of chromosomal abnormalities (trisomy (+9), deletions (-5 or -7) and translocations [t (8, 21)]), oncogene mutations, and somatic mutations in benzene-exposed MDS patients [29-31]. Additionally, as increasing somatic mutations may occur with aging, exposure to benzene and other directly genotoxic agents could lead to more significant damage that progresses to clonal expansion and MDS [31]. Suggested non-genotoxic mechanisms include alteration of the bone marrow microenvironment and immune function through reduced immunoglobulin and complement levels [31]. Radiation and prior chemotherapy are other well documented exposures that can lead to the development of MDS [24, 23, 31]. Specifically, chemotherapy-associated MDS has been associated with treatment using Topoisomerase II inhibitors, anthracyclines, and alkylating agents. MDS from exposure to Topoisomerase II inhibitors and anthracyclines typically has an early onset within 1-3 years and causes balanced genetic alterations typically involving 11q23 (Mixed Lineage leukemia, MLL gene) [5] while exposure to alkylating agents results in a later onset within 5-10 years and yields unbalanced chromosomal alterations often involving chromosomes 5 and 7 [10, 32]. With regard to radiation, epidemiologic studies of atomic bomb survivors have illustrated the connection between previous radiation exposure and leukemia/MDS development, [33] and have characterized the importance of exposure dose and duration [34]. Specific effects and chromosomal abnormalities, additionally, seem to be similar to those seen with exposure to alkylating agents [4]. With a median age of newly diagnosed MDS patients nearing 70, the importance of aging in MDS is clear, yet the specific role it plays biologically remains under investigation [1]. It is theorized that aging itself may produce increased genetic mutations and alterations that result in MDS. Comparing bone marrow from normal controls and older patients is one approach to highlighting potential similarities and differences that could explain the increased incidence of MDS in the elderly. Ogawa et al. evaluated the bone marrows of 100 normal controls of a variety of ages [35] and found increased apoptosis and decreased cellularity in patients of advanced age [36] with apoptosis levels similar in degree to MDS patients. Other studies describing MDS marrows detail a skew in specific TNF-alpha receptor expression leading to increased rates of apoptosis comparable to that seen in normal elderly marrows. While the increased apoptosis in both normal elderly marrows and MDS patients may have distinct biologic causes, the finding may also suggest a reason for the preponderance of increased MDS in the elderly [37]. Another biologic link between aging, stem cell damage, and cancers such as MDS includes the study of telomeres and telomerase activity. Telomeres are simple tandem repeats at the ends of chromosomes in somatic cells that shorten with age and are also found to be shortened in many cancers [38-40]. The shortening is theorized to result from incomplete DNA replication leading to genomic instability, subsequent chromosomal abnormalities, and eventual mutations impacting disease progression once a certain threshold is breeched. Telomerase is the enzyme required for the replication of telomeres, and although not typically found in most somatic cells, has been found in over 85% of primary malignancies [41]. Telomerase may not be required for initiation of malignancy but

Myelodysplastic Syndromes Current Cancer Drug Targets, 2007, Vol. 7, No. 6 543
Table I. Cytogenetic Abnormalities in MDS
Chromosomal Alteration
Incidence (Approximate)
Associations: Exposures / Other Disorders
Classic Clinical or Morphologic Description
Prognostic Impact Research
Chromosome 5 Abnormalities
- 10-20% de novo MDS cases - Tx-related in 40% of cases [31]
-Chemical Exposure -Chemotherapy [49]
Clinical: -5q Minus Syndrome = macrocytic anemia, nl platelet count, female predominance [50]
- 5q alone/5q syndrome = good/low risk of AML transformation [47, 50, 51] - Complex / other abn of 5 / t-MDS = poor prognosis
- 5q CDS: genes for cell cycle & cellular cytokine receptors - No specific gene loss yet identified [52-57]
Deletion 20q
- 5% de novo MDS cases - Tx-related in 7% of cases [11]
Polycythemia Vera [58]
Morphologic: Dyserythropoiesis [58] Clinical: ! freq. in low-risk dz, longer survival: low progression to AML [59]
- Isolated 20q = good outcomes - 20q del + complex = poor outcome [22]
- CDS (20q11.2-q12) contains numerous tumor suppressor genes [11, 58, 60, 61] - No specific gene loss yet identified
Loss of Y
Associated w/ not diagnostic of MDS [58]
- Numerous cancers - Normal Aging population [11, 58]
Favorable prognosis if isolated abn [22]
Chromosome 7 abnormalities
-5% de novo MDS cases - Tx-related in 55% of cases [11]
Associated w/ AML, MDS, NF-1, Fanconi’s anemia, Down’s Syndrome [62]
Poor risk dz w/ high progression to AML [63, 58]
- Monosomy 7 uniformly bad regardless of dz - CDS (7q22 and 7q32-33) found but often full 7 loss so difficult to study [64, 62]
17p Syndrome
- 5% of MDS cases [58] - Tx-related in 33% of cases [65]
Morphologic: Dysgranulopoiesis, pseudo-pelger huet cells, hypogranularity [48]
- Often tx related = poor prognosis - Often seen w/ other abn (5 and 7) = poorer prognosis [11, 58, 65]
- Loss of p53 function - Due to point mutation in p53 at 17p13 in 70% pts [58]
Trisomy 8
- 10-15% of MDS cases [58] - Sole abn. in 10% of cases [49]
- AML/MDS - Linked to Benzene exposure - Solid Tumors: Breast, Colon, Sarcoma [66]
Morphologic: MDS with monocytic component [58]
- Isolated = Intermediate Prognosis [22] - Not specifically linked with FAB class/ AML progression [11]
-High incidence in MDS but not sufficient for leukemogenesis alone [49]
3q Abnormalities
-2% of MDS cases [58] - Typically tx-related [58]
Morphologic: Abn megakaryocytic development Clinical: Retained platelet count
-EVI-1 gene (3q26) alterations: - Interference w/ 3q26 transcription linked w/ abnormal differentiation: may interfere w/ GATA-1, (erythrocyte differentiation) [58]
Complex Cytogenetics
- 10-20% of de novo MDS cases - Tx-related in 90% [67]
Only partial correlation w/ outcome: poor prognosis [67]
Oncogene/Tumor Suppressor
Abnormalities
Oncogene/Tumor Suppressor Function
Frequency of Abnormality in MDS
Patients Specifics of Abnormality Prognostic Implications Research
11q23/MLL Gene
Abnormality
MLL fusion products involved in numerous cell functions: precise oncogenic mechanism still poorly understood [68]
- 5% of MDS cases [58] - often tx-related [32]
Clinical: Typically later stage dz, high AML transformation, shorter survival [69,11] - Forms numerous fusion protein pairs
Assoc. w/ other abn: Complex, 5 and 7 [69]
- MLL Amplification: role in oncogenic changes -Gain of function via HOX9A expression found [70] - absent in de novo MDS [71]
Ras Family of genes encoding GTP-binding proteins: role in signal transduction
-Paquette Study of 220 MDS Pts – 9% w/ n-ras mutations [72]
- Point Mutations [73]
-N-ras mutations assoc. w/ shorter survival and increased progression to AML [72]
-Study showing 70% of pts w/ mutation progressed to AML w/i 2 yrs compared to control [72]
p53 Control of DNA replication repair: crucial for maintaining genome [74]
- In 69% of pts w/ 17p deletion [75] - ! p53 mutations in 17p + complex cytogenetics [76]
-In t-MDS often found w/ chromosome 5 abn and complex cytogenetics [65] - Not usually assoc. w/ chromosome 7 abn [32]
-Resistance to chemo: shorter survival: Shorter time to leukemia development [76, 77]
Legend: MDS = Myelodysplastic Syndrome; Tx = treatment; Nl = normal; AML = Acute Myelogenous Leukemia; t-MDS = treatment related MDS; CDS = Commonly Deleted Segment; w/ = with; Freq. = frequency; Del = deletion; Abn = abnormality; NF-1 = neurofibromatosis 1; Dz = Disease; FAB = French American British; Assoc. = Associated; MLL = multi-lineage leukemia; Pts = patients; w/i - within

544 Current Cancer Drug Targets, 2007, Vol. 7, No. 6 Warlick and Smith
\may be important in tumor propagation [42]. Interestingly, telomerase activity is found in cell populations with high renewal requirements such as hematopoietic stem cells [43]. In MDS, studies evaluating telomeres and telomerase activity show loss of the typical correlation between telomere length and age: specifically, decreasing telomere length with increasing age [44]. Further studies have found an association between shortened telomeres and abnormal cytogenetics, where progressively shortening telomeres correlated with worsening IPSS risk group [44]. Telomerase activity has also been assessed in MDS: high levels of activity have not commonly been found. The culmination of this data may suggest that the hematopoietic stem cells in MDS patients have insufficient telomerase to adequately restore cellular telomeres to their normal lengths subsequently resulting in increased genetic instability [44].
Gain or Loss of Gene Expression: Cytogenetic and Epigenetic Alterations One of the common end results of exposure to environmental toxins is DNA damage and the loss or alteration of gene expression. Yet, chromosomal abnormalities are often detected in MDS that are not associated with such exposures. In addition, newer techniques, including comparative genomic hybridization (CGH) and single nucleotide polymorphisms (SNP) arrays, now allow the detection of even microscopic deletions of genes and continue to fuel the understanding of MDS and its pathophysiology. Finally, it is now clear that epigenetic gene silencing plays a role in loss or gain of gene expression even when the DNA sequence is completely intact. Clonal cytogenetic abnormalities (Table I) are found in 30-70% of patients with primary myelodysplastic syndrome and in over 80% of treatment-related MDS and remain the most important individual prognostic tool [11, 45-47]. The majority of the chromosomal abnormalities in primary MDS involve unbalanced losses: entire chromosomal loss or point mutations [11, 45]. Consequently, it is easy to invoke such abnormalities resulting in the loss or inactivation of a critical tumor suppressor protein; however, efforts to determine a culprit gene or cluster of genes have been much more difficult. Characteristic chromosomal abnormalities in MDS include alterations of chromosomes 5, 7, 8, 11, 17, 20 and Y or complex karyotypes involving multiple abnormalities within individual clonal populations [45, 46]. Several of these abnormalities are shared with AML (e.g., deletions of chromosomes 5 or 7, trisomy 8, and complex cytogenetics), while others appear almost exclusively in AML (e.g., t (15; 17), t (8; 21), and inversion 16) [22]. Although specific cytogenetic abnormalities within MDS do not typically correlate with WHO or FAB classifications, it is now clear that there are characteristic syndromes within MDS, namely 5q- and 17p- syndromes [47, 48] that have unique clinical and prognostic outcomes. Additionally, evidence suggests a correlation with increasing frequency of cytogenetic abnormalities and severity of disease. The traditional cytogenetic alterations noted above are typically evaluated using conventional cytogenetic (CC) techniques that require adequate metaphase chromosomes for analysis. The development of newer techniques has allowed investigators to uncover more subtle genetic alterations that help to reveal further components of MDS pathophysiology. Comparative genomic hybridization (CGH) is a useful tool that can uncover genomic imbalances without the requirement for quality mitoses or dividing cells. Specifically, it allows for detection of changes in chromosome copy number by hybridization techniques between normal and tumor cells [78]. Studies comparing information obtained through CC, FISH analysis, and CGH, showed close correlation between the three techniques with CGH providing additional information on the abnormalities identified by CC as well as uncovering unbalanced genetic alterations not described by CC [79, 80]. CGH continues to add valuable information to many common cytogenetic findings [81, 82].
Identifying alterations of single nucleotide polymorphism (SNPs) arrays have also been used to help investigators study and explain the heterogeneity of MDS. Moreover, this technique has led to insights on genetic predispositions for these diseases. SNPs are the most common form of genetic variation between individuals, and recent reports have investigated the possibility that genetic polymorphisms in genes required for proliferation and differentiation may play a role in MDS development. Specifically, a GLU785Lys polymorphism in the G-CSF receptor was described and demonstrated functional alterations in growth factor responsiveness in high risk MDS patients suggesting a potential role in MDS pathophysiology [83]. It is likely that further investigations will reveal pathways impacted by these subtle changes in gene expression. SNP techniques have also looked at the possibility that polymorphisms create a genetic predisposition to MDS. Based on evidence of defective DNA mismatch repair enzymes in patients with t-MDS and mitochondrial/genetic instability in patients with primary MDS [84], obvious implicated pathways could include those involving metabolic activation or detoxification enzymes. Utilizing both specific and non-specific probes, polymorphisms in detoxification enzymes such as glutathione S-transferase [85] as well as in quinone oxidoreductase have been found, where the presence of NQO1 quinone oxidoreductase polymorphisms correlated with an increased risk of benzene-related and treatment-related MDS [86, 87]. Additional investigation has also shown microsatellite instability (MSI) in treatment-related MDS, a hallmark of defective DNA mismatch repair [88]. In addition to these structural alternations in DNA, another mechanism for altered gene expression leading to gain or loss of function involves the silencing of genes through epigenetic modifications. The two most intensely studied alterations include DNA methylation and histone acetylation. Both of these genetic alterations can affect chromatin packing and create a DNA / histone complex that is not able to be transcribed. The result is silencing of the noted gene despite its non-mutated presence. Although any gene can be affected by these epigenetic phenomena, many of the genes implicated in cancer development involve tumor suppression, cell cycle control, cell death, cell growth, and differentiation. The silencing of gene expression secondary to DNA methylation is responsible for a variety of normal, physiologic functions including X-chromosome inactivation, facilitation of DNA imprinting, and protection against insertion of viral DNA into the genome [89]. DNA methyltransferase is the key enzyme that methylates CpG islands in the promoter region of genes leading to hypermethylation and silencing of gene transcription [90]. Many cancers appear to have extensive regional hypermethylation as well as aberrant gene expression leading researchers to explore the role of hypermethylation in tumor development and progression: AML and MDS lead the way in being the best studied diseases. There are numerous genes that are implicated in MDS/AML pathophysiology with p15INK4B being one of the most studied. Specifically, hypermethylation of p15INK4B, a known tumor suppressor and cell cycle regulatory gene, has been associated with progression of MDS to AML [91, 92]. Functionally, CDK4 and CDK6 allow cell cycle progression from G1 to S phase. p15INK4B can act as a tumor suppressor and inhibit cell cycle progression by inhibiting the function of CDK4 and 6. Hypermethylation of p15INK4B prevents this suppressive function and allows uncontrolled progression through the cell cycle and resultant uncontrolled proliferation [93]. p15INK4B hypermethylation has been seen in up to 50% of patients with MDS; specifically in higher risk MDS, where the uncontrolled proliferation has shown increased progression to AML and portends a worse prognosis [92, 94, 95]. Hypermethylation of the calcitonin gene has also been described and can be found in 65% of MDS cases. Its presence spans all morphologic subtypes and is commonly found in patients with normal cytogenetics [96]. Numerous studies now suggest that hypermethylation of the calcitonin gene may be an important marker of transformation from MDS to AML [97-99].

Myelodysplastic Syndromes Current Cancer Drug Targets, 2007, Vol. 7, No. 6 545
Other commonly reported hypermethylated genes in implicated in MDS include E-Cadherin (CDH1), HIC1, and ER [94]. Similarly, conformational alterations of the DNA histone complex also play an important role in the abnormal gene silencing seen in many cancers. Acetylation of lysine residues on the N-terminus of core histones creates an open and readily transcribable chromatin structure while deacetylation creates a tightly coiled and non-transcribable chromatin structure [100]. Acetylation status can also alter transcription factors (GATA-1), nuclear import proteins, signal transduction proteins, DNA repair enzymes, heat shock proteins, and numerous other cellular proteins [101-106]. The epigenetic modulation of these proteins leads to altered expression of pro-apoptotic and cell cycle proteins (ex. FAS/FAS ligand, Bcl2, p53, caspases, Bax, and p21WAF1/Cip1) [106] and can result in multiple cellular effects including growth arrest in G1 or G2/M, differentiation, and preferential apoptosis of cancer cells [100, 107].
Altered Bone Marrow Microenvironment: Apoptosis, Cytokines and Angiogenesis The bone marrow microenvironment has also been implicated in the development and progression of MDS with numerous studies showing altered cytokine milieu and apoptosis rates as well as changes in vascular microdensity. These alterations produce a common pathway of increased apoptosis of early, CD34+ progenitors in early-stage MDS and a relative reversal of this ratio in later-stage disease. As MDS progresses towards AML, these pathways become less well defined and additional factors, including proliferative genetic events, may play a more important role [12-14]. Each of these processes may offer scientists numerous targets upon which to focus new therapies. Bone marrow samples from MDS patients traditionally reveal a hypercellular marrow in the context of increased cytokines, such as TNF-alpha and IFN-gamma, and persistent peripheral cytopenias. Interestingly, data support both increased and decreased programmed cell death within MDS marrows, yet careful analysis suggests that increased apoptosis is more often associated with early stage MDS (RA/RARS) while decreased apoptosis is more characteristic of advanced disease (RAEB2/AML) [13, 14]. Cytokine dynamics offer one explanation for such cycles of altered apoptosis within the malignant clones. Elevations of TNF-alpha and IFN-gamma are consistently described in the MDS bone marrow microenvironment [37, 108, 109] with additional reports suggesting TGF-beta elevations as well [110, 111] highlighting the important role cytokines play in MDS pathogenesis and maintenance. The role of increased TNF-alpha has been well studied in its involvement in promoting apoptosis in MDS, particularly early stage disease [14, 37, 108]. TNF-alpha promotes apoptosis by engaging with the tumor necrosis factor receptor I and II (TNFRI or TNFRII) and via TNFRI mediates programmed cell death by direct binding with TNF Receptor 1 associated protein with a death domain (TRADD), subsequent indirect binding with FAS-associated protein with a death domain (FADD), and eventual activation of the caspase cascade. TNF-alpha can also interact with TNFRII, which lacks a death domain, but interacts directly with TNF receptor-associated factor 2 (TRAF-2), activating NF-!B and JNK, and ultimately promoting anti-apoptotic effects [37, 112, 113]. The ratio of these receptors impacts the rates of apoptosis in MDS with increased TNFRI documented in low-risk disease and increased TNFRII in high risk disease illustrating, again, the inverse correlation between rates of apoptosis and potential for proliferation and disease progression [37]. Raza et al. have suggested that increased levels of TNF-alpha have a dual impact on MDS development through contrary stimulatory and inhibitory effects: stimulation of primitive progenitor cells, yielding the classic hypercellularity of MDS, while exertion of apoptotic influence on more mature cells, correlating with the peripheral cytopenias [111]. The etiology of these cytokine alterations
and definition of the cells from which they originate (macrophages, fibroblasts, or other) remain unanswered questions [114-117]. In addition to TNF-alpha’s impact on apoptosis in MDS, abnormalities in FAS and bcl-2 pathways have also been implicated. FAS is a transmembrane receptor belonging to the same superfamily as the TNF-alpha receptor and its stimulation follows a similar path to apoptosis that terminates with caspase cascade stimulation and degradation of “death substrates” [14]. Abnormal FAS-signaling has also been implicated in other bone marrow failure states such as aplastic anemia as well as in other malignancies with specific studies in MDS illustrating increased FAS expression and apoptosis in low-risk disease and decreased FAS expression in high-risk disease. Interestingly, although increased FAS expression has been seen, no statistically significant correlation between FAS expression and degree of apoptosis has been shown [118]. Thus, while increased apoptosis is an important component in MDS pathophysiology and is seen more in early stage disease, the mechanism for which this occurs is not explained by one pathway alone and may involve FAS signaling either via direct or indirect pathways [14, 118, 119]. While the TNF-alpha and FAS signaling has supported the increased rates of apoptosis in early stage disease, decreased apoptosis rates have also been implicated in the progression from MDS to AML and has been documented to occur via alterations in anti-apoptotic bcl-2 and bcl-x expression [14]. Changes in vascular microdensity are another component of the marrow environment identified as contributing to the development and sustenance of MDS clones [120]. Originally a focus of research in solid tumors, increased angiogenesis also appears to play a role in hematologic malignancies. In solid tumors new blood vessels are formed to sustain growth of the tumor by supplying blood and nutrients. The role of angiogenesis in hematologic malignancies is slowly being unveiled, and early findings suggest not only its importance but also its varied character among different cancers. New blood vessel growth can drive cytokine production, but may also be a byproduct of excessive cytokines. As described above, the milieu in MDS provides many cytokines capable of influencing new vessel growth. In addition to increased TNF-alpha and INF-gamma in the marrow of MDS patients, varying levels of angiogenic factors including VEGF (vascular endothelial growth factor), bFGF (fibroblast growth factor), angiogenin, HGF (hepatic growth factor), EGF (epidermal growth factor), and TGF-beta (transforming growth factor) have been noted in the plasma of MDS patients. These findings, coupled with direct evidence of increased microvascular density (MVD) on marrow biopsies, support the development of early blood vessels in MDS [120-123]. Both plasma VEGF levels and increased MVD correlate with advanced MDS FAB class [124-126] and imply that increased VEGF may drive increased MVD eventually stimulating MDS progression to AML.
Immune System Dysregulation Dysregulated immunity has been implicated in the development of all cancers, including MDS [127], but direct evidence in MDS has been difficult to uncover. The successful use of immunosuppressive therapies (i.e., cyclosporine-A, anti-thymocyte globulin), the potentially curative role of allogeneic stem cell transplant, and the more recent data showing improved peripheral cytopenias and elimination of certain common cytogenetic abnormalities with immunomodulatory agents (i.e., thalidomide and lenalidomide) highlight the role immune dysregulation plays in the development of MDS. Changes in both B and T cell dynamics have been implicated in MDS development. Studies have substantiated an autoimmune-type T cell attack in MDS pathogenesis. Specific in vitro work by Smith et al. investigated the possibility of auto-reactive T cells and noted the presence of inhibitory T cells in patients with MDS [128] with subsequent clinical studies showing in vivo success using anti T-cell therapies (anti-thymocyte globulin (ATG) [129] and cyclosporine-A (CSA)) [130]. Investigation revealed an abnormal T

546 Current Cancer Drug Targets, 2007, Vol. 7, No. 6 Warlick and Smith
cell repertoire and T cell-mediated inhibition of bone marrow CFU-GM [131] as a potential mechanism to the response to ATG. Further characterization of the T cell repertoire in MDS patients demonstrated T cell expansion with recurrent patterns of V-Beta and J region skewing suggestive of unknown chronic antigenic stimulation [127] while other studies identified high percentages of cytotoxic T cells (CD8+, CD28-, CD57+) [132]. In aggregate, these findings indicate an activated immune environment [133]. Irregularities in B cell function have also been implicated in MDS based upon epidemiologic data revealing increased frequency of autoimmune disorders and immune-mediated complications in these patients [134, 135]. Studies evaluating this correlation revealed the presence of either clinical or serologic manifestation of auto-immunity in 10-12% of MDS patients with a higher prevalence in younger patients, those with treatment-related MDS, or those with cytogenetic abnormalities [135, 134]. Just as T cell repertoire skewing has been noted, clonality of B cells within MDS is also under investigation. The presence or absence of such clonality may lend insight to the cell of disease origin. Using cytogenetic abnormalities as a marker to trace lineage, various progenitor and terminally differentiated populations in MDS samples have been studied with seemingly discrepant findings. Using Trisomy 8 as the tracing abnormality in their MDS samples, Saitoh’s group found the additional 8th chromosome in granulocytes, monocytes, and erythroblasts but not in lymphocytes in the BM or in B, T, or NK cells of the peripheral blood. Additional analysis found Trisomy 8 in the level of the CFU-GEMM stem cell (CD34+, CD33+) but not in the pluripotent stem cells (CD34+, Thy1+) indicating absence of B cell clonality and instead a myeloid progenitor as the neoplastic clone [136]. Other groups have shown the presence of specific cytogenetic abnormalities in both myeloid and lymphoid lineages indicting a
more pluripotent stem cell of origin. Specifically, White’s group showed the presence of deletion 20q in Epstein Barr Virus (EBV) immortalized lymphoid cell lines derived from an MDS patient [137] while Nilsson’s group has shown interesting findings with both 5q deletion and Trisomy 8 [138, 139]. Specific studies with 5q deletion documented its presence in the majority of pluripotent (CD34+, CD38-) stem cells with both myeloid and lymphoid differentiation; however, transfer of this cell population to SCID mice showed inability to reconstitute hematopoiesis indicating absence of 5q in the most primitive progenitors [138]. Interestingly, in cases with both Trisomy 8 and del 5q, it was evident that Trisomy 8 was a secondary genetic event potentially explaining the discrepancy by suggesting that the additional Trisomy 8 event developed in the progeny of the CD34+CD38- del 5q containing stem cells [139]. The quest to document the potential clonality of B cells involved in MDS pathogenesis has led to the deeper discovery that different cytogenetic abnormalities may originate in different cells of origin in MDS which could have substantial implications on treatment strategies.
Cell Cycle Dysregulation, Abnormal Differentiation, and Transcription Factor Alterations Abnormal differentiation and growth represents the most dominant morphologic feature of MDS. Although there has been an exhaustive analysis of cellular signaling pathways in an effort to define the main problems with differentiation, our best understanding of this problem is linked to studies of the cell cycle: the cell’s ability to initiate normal cellular division, speed of the cell cycle, and regulation of cell cycle checkpoints. The speed of the cycle plays an important role in assuring balanced homeostasis between self-renewal and progenitor expansion with natural aging and cellular death of each cell type required to maintain an adequate blood supply [140].
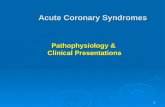
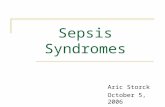
Transplant Candidate?
Yes NO
INT-2/HIGH LOW/INT-2 INT-2/HIGH
AlloBMT# Growth Factors**CSA/ATG~DMTIs @
Lenalidomide if 5q-
DMTIs
No Response? CLINICAL TRIAL +
# Controversies in BMT for MDS: Approaches to Consider
Timing of transplantation:Low/INT-1: Delay BMT until progression but prior toleukemic transformation INT-2/High: Proceed towards BMT from diagnosis
Treatment Pre-BMT:Low/INT-1: Consider BMT as 1o TherapyINT-2/High: Consider alternative 1o Therapy piror to BMT
** If EPO level <500 considerErythropoietin. Consider addition of G-CSFif no response to erythropoietin alone ! Improved response rates seen in hypoplastic MDS, PNH clone, HLA-DR15positivity
@ 5-azacitidine or decitabine
+ Participation in clinical trials encouraged
Fig. (1). Hopkins approach to MDS treatment.

Myelodysplastic Syndromes Current Cancer Drug Targets, 2007, Vol. 7, No. 6 547
Detailed molecular work has shown characteristic lineage specific cell cycle changes required for normal differentiation: 1) up-regulation of cdc2 and cyclin A in erythroid lines; 2) induction of cyclin D1 and p15 in myeloid lines; and 3) selective upregulation of cyclin D3 and induction of p21 in megakaryocyte differentiation [141]. Alterations in any of these normal differentiation pathways could thus lead to maturation arrests. Specific blocks in differentiation in MDS and AML have been linked to abnormalities such as constitutive activation of CDK inhibitor p16 leading to G0/G1 arrest and subsequent maturation arrest [141]. Additionally, cell cycle specific changes, such as alterations to the CDK inhibitor and tumor suppressor p15INK4B, have been closely linked to uncontrolled cell cycling and proliferation leading to progression from MDS to AML [93]. Resultant aberrant cell cycle function in MDS has been the common final pathway for a number of genetic, epigenetic,
micronenvironmental, and common transcription factor alterations. The GATA transcription factor family (GATA-1, 2, and 3) is of interest with alterations implicated in MDS pathogenesis. Normal GATA-1 is involved in control of erythroid cells, megakaryocytes, eosinophils, and mast cells while GATA-2 is expressed in more immature progenitors including hematopoietic stem cells [142]. Abnormalities or increased levels of GATA-1 have previously been described to affect cell cycle regulation [143], proliferation, differentiation, and regulation of apoptosis [144] of both erythroid and megakaryocytic progenitors. Studies show that normal GATA-2 expression is increased in hematopoietic stem cells and its expression inhibits terminal differentiation thus playing more of a role in proliferation and self-renewal capacity of the stem cells [145]. Consequently, imbalances of GATA-1 and GATA-2 could skew the progenitor population contributing to abnormal differentiation [146], the development of MDS [147], and in the setting of an additional genetic hit may contribute to the progression to acute leukemia [142].
Table II. Theories of Pathophysiology involved in MDS Development
Theories of Pathophysiology involved
in MDS Development Potential Targets/Components Involved Overall Result of Abnormality
Current Directed Therapies, Potential Directed Therapies,
and Investigatory Treatments for MDS
Environmental/Aging
Aging Increased BM apoptosis Decreased hematopoietic stem cell pool
Environmental Exposures
! Smoking ! Radiation ! Benzene ! Viral Infections ! Chemotherapy
! Direct Toxicity to hematopoietic stem cells ! Genotoxic: O2 free radicals, DNA
damage ! Non-Genotoxic: Immune
modulation (Immunoglobulin/complement alterations) and altered BM microenvironment
Telomere Abnormalities ! Potential decreased telomerase and subsequent telomere shortening
! Impaired ability to renew stem cell pool ! Genetic Instability
Genetic Alterations
Cytogenetic Abnormalities
Common Abnormalities: ! 5q- ! 20q- ! Y- ! Trisomy 8 ! 7q-/Monosomy7 ! 17p Syndrome ! 11q23 ! 3q ! P53 mutations ! Ras mutations ! Complex Cytogenetics
! Abnormalities: typically unbalanced genetic loss
! Numerous theories of tumor suppressor loss
! Multi-Hit progression from low risk MDS to AML
! Genetic Instability
! Lenalidomide:* 5q- syndrome ! Ph III Lenalidomide in del 5q- pts @
NCT00179621
Epigenetic Modulation
! Hypermethylation: ! Calcitonin gene ! p15INK4B ! ER ! E-Cadherin ! Acetylation Alterations: ! Cell cycle components: p21WAF1 ! Alteration of differentiation and apoptotic machinery ! Alterations of angiogenesis
! Methylation and acetylation abnormalities lead to silencing of genes important in cell cycle, differentiation, apoptosis, angiogenesis
! DNA Methyltransferase Inhibitors: (DMTIs)# ! 5 Azacitidine*
! Ph I Aza maintenance post AlloBMT @ NCT00350818
! Decitabine* ! Ph I/II Decitabine + Tretinoin @
NCT00382200 ! Ph II Decitabine post Aza failure @
NCT00113321 ! Histone Deacetylase Inhibitors (HDIs)
! Ph I MS-275 + Aza @ NCT00101179 ! Ph II Aza,VPA, ATRA @NCT00339196 ! Ph II Aza vs. VPA vs. Ara-C @
NCT00382590 ! Ph II Decitabine +/- VPA @ NCT00414310 ! Ph II MGCD0103 @ NCT00374296 ! Ph I Vorinistat + Ara-C + VP-16 @
NCT00357305
Microscopic Genetic Alterations
! Comparative Genomic Hybridization: ! Single Nucleotide Polymorphisms (SNPs): ! NQO1 ! Glutathione S-transferase ! G-CSF Receptor ! Microsatellite instability
! Dysfunction of enzymes required for detoxification, DNA mismatch repair, or differentiation

548 Current Cancer Drug Targets, 2007, Vol. 7, No. 6 Warlick and Smith
Given the complexity of the cell cycle control in hematopoiesis, alterations of any key component could lead to abnormal differentiation and the potential for MDS.
STANDARD TREATMENT FOR MDS Until the recent past, treatment for MDS was limited to best supportive care (growth factors and transfusion support) for the
(Table II). Contd…..
Theories of
Pathophysiology involved in MDS Development
Potential Targets/Components Involved Overall Result of Abnormality Current Directed Therapies, Potential Directed Therapies,
and Investigatory Treatments for MDS
Altered Bone Marrow Microenvironment
Altered Bone Marrow Microenvironment Cytokines
! Upregulation of: ! TNF-" ! IFN-gamma ! TGF-Beta ! IL-1B ! IL-6 ! Il-11
! Alteration of growth, differentiation, angiogenesis ! Immune modulation
Anti-TNF-" Trials: ! Ph I/II Aza + Etanercept: INT-2 / High Risk @
NCT00118287 ! Ph II ATG + Etanercept: low / INT-1 @
NCT00217386 ! Ph II Infliximab: Low / INT-1 @ NCT00074074 ! SCIO-469 Open Label Study: Inhibitor of
p38MAPK (TNF-"/other cytokine/Fas blocker) @ NCT00113893
Alterations in Apoptosis via Signaling
Increased TNF-! levels: ! Increased Apoptosis: Low Risk MDS
! Binding to TNFRI – oligomerization – TRADD/FAD association -- activation of Caspase cascade -- increased apoptosis
! Decreased Apoptosis: High Risk MDS ! Binding to TNFRII -- TRAF-2
interaction -- activation of NFkB – apoptosis inhibition
FAS: Increased Apoptosis ! Increased FAS binds to FAS-Ligand --
trimerization -- activation of FADD -- association with Caspase 8 -- triggering protease/caspase cascade cleaving DNA repair proteins
BCL-2 alterations: ! Oncogene Interactions:
! Inhibits c-myc: required for progression from G1/S
! Interacts with Raf-1 ! Interacts with Ras
! Increased apoptosis and proliferation in early stage MDS leading to hypercellular marrow with peripheral cytopenias
! Decreased apoptosis and increased proliferation in later stage MDS leading to progression to AML
Anti-TNF-" Trials: direct blockage see above ! Bortezamib @ NCT00440076 (indirect NFkB
inhibitor: implicated in TNF-" production) Arsenic Trials: (Target TNF-", increase susceptibility to apoptosis, suppress VEG-F, induce differentiation via p21/p27 activation) ! Ph II Arsenic Trioxide @ NCT00225992 ! Ph I/II Arsenic+ Ara-C @ NCT00195104 ! Ph II Arsenic + Gemtuzimab @NCT00274781 ! Ph I/II Aza + Arsenic @ NCT00234000 FAS Target: ! See above SCIO-469 trial ( FAS blocker) BCL-2 Target: Ph II BCL- 2 inhibitor GX15-070MS @ NCT00413114 Oncogene Targets: ! Ph I Sorafenib (Sorafenib: raf kinase/VEGF
inhibitor) @ NCT00217646 ! Ph III Lonafarnib vs Placebo (farnesyl
transferase inhibitor: inhibits RAS) @ NCT00109538
Increased Angiogenesis
! Increased VEG-F ! Possible Increase:
! gFGF and EGF ! Angiogenin
! Increased Microvessel Density (MVD): role in pathogenesis not clearly elucidated but associated with progression to AML
! Ph II Vatalanib (anti-angiogenesis/ VEGF inhibitor) @ NCT000072475
! See above Sorafenib trial (VEGF inhibitor) ! See Arsenic Trioxide Trials
Immune Dysregulation
! T cell Expansion ! Skewed V# and J regions ! Increased Cytotoxic T cells CD8+,
CD28-, CD57+ ! B cell alterations
! Clonal B cell expansion/connection with increased frequency of autoimmune phenomena in MDS
! Increased T cells leading to potential attack on hematopoietic stem cells
! Etiology: Possible chronic antigenic stimulation
IMIDs: ! Ph I Bortezomib + Thalidomide* @
NCT00271804 ! Ph I Lenolidamide* + Aza @
NCT00326846 Other Immune Modulation: ! Ph III ATG + CSA vs. Best Supportive Care @
NCT00004208 ! Ph I/II Campath +CSA @ NCT00217594 ! WT-1/PR-1 Peptide Vaccine + GM-CSF @
NCT00313638 ! K562/GM-CSF Vaccine @NCT00361296 ! Alloreactive NK Infusion + AlloBMT : Ph I/II
@ NCT00402558 and Ph II @ NCT00303667 ! Cytoxan + DLI @ NCT00356928
Abnormal Differentiation ! Cell Cycle Maturation arrest: Ex: p16 alt. ! Altered Proliferation: Ex. p15INK4B ! Transcription Factors alt: GATA-1/GATA-2
! Impaired maturation ! Cytopenias ! Progression to leukemia
! Ph II Calcitriol + Dex @ NCT00030069 Growth Factors + Differentiating Agents: ! Ph II Bexarotene+GM-CSF@NCT00425477
Legend: *-FDA-Approved for MDS; @- clinical trials from clinicaltrials.gov; # = Numerous epigenetic trial combinations active: representative sample included.
BM = bone marrow; DMTIs = DNA Methyltransferase inhibitors; HDIs = Histone deacetylase inhibitors, MDS = myelodysplastic syndrome; AML = acute myelogenous leukemia; ER = Estrogen receptor; Aza =5-Azacitidine; Ph = Phase; VPA = valproic acid; ATRA= all-trans retinoic acid; CSA = cyclosporine A; gFGF = fibroblast growth factor; EGF = epidermal growth factor; ATG = anti-thymocyte globulin; NK = natural killer; AlloBMT = allogeneic bone marrow transplant; DLI = donor lymphocyte infusion; dex = decadron; GM-CSF = granulocyte macrophage colony stimulating factor; alt = alterations

Myelodysplastic Syndromes Current Cancer Drug Targets, 2007, Vol. 7, No. 6 549
majority of patients and allogeneic stem cell transplant for the small minority of patients eligible for the procedure. Of these treatments, only transplant offered an approach that changed the natural history of the disease and offered a cure. More recently, newer agents, such as azacitidine and decitabine, have been FDA approved to treat MDS based on their impact on the natural history of disease through decreasing the rate of transformation from MDS to AML. Formal evaluation of response to treatment has been described by International Working Group (IWG) criteria, which has recently been modified and described in Table III [148]. We review current standard treatments (Table IV), describe future directions and novel treatment approaches, and conclude with a treatment algorithm for MDS patients (Fig. (1)).
Supportive Care Based on concerns of poor tolerance to traditional cytotoxic agents in patients with advanced age, poor performance status, or medical co-morbidities, supportive care has been the longstanding
approach to MDS patients. Unfortunately, these criteria of concern are common in the MDS population. Traditionally, supportive care has taken the form of close blood count monitoring, blood product transfusions, systemically administered lineage-directed growth factors, and often prophylactic antibiotics with the sole intent of improving marrow function and minimizing the impact of the bone marrow failure on the patients’ lives. While somewhat effective, each of these approaches is relatively limited. Close monitoring of blood counts requires a compliant and diligent patient and takes time each week for testing and follow-up. Use of transfusions is ultimately limited by the development of alloimmunization and the resultant antibodies that effectively reduce the impact of both red cell and platelet transfusions. Myeloid growth factors are generally only recommended in patients plagued by recurrent neutropenic fevers, severe systemic infections, or in combination with erythropoietin. Erythropoietin is generally considered the most effective supportive approach yet yields an overall response of approximately 16% as a single agent [149, 150] and up to 36-50% in combination with G-CSF
Table III. Modified IWG Response Criteria
Response Category Response Criteria ( must last minimum of 4 weeks)
Complete Remission BM: < 5% blasts with normal trilineage maturation Any persistent dysplasia PB: Hgb> 11g/dl Neutrophils > 1 X 109/L Blasts 0%
Partial Remission If abnormal before treatment, all CR criteria except: BM blasts decreased by >50% but still greater than 5%
Marrow CR BM: < 5% blasts and greater than 50% decrease over pre-treatment PB: HI responses will be described in addition to marrow CR
Stable Disease PR not achieved but no progression for >8 weeks
Failure Death or disease progression
Relapse post CR/PR 1+ of the following: Recurrence of pre-treatment BM blast % > 50% Decrease from greatest response in neutrophils or platelets Hgb reduced by greater than 1.5 g/dl or transfusion dependence
Cytogenetic Response Complete: Resolution of all cytogenetic abnormalities Partial: 50%+ reduction of cytogenetic abnormality
Disease Progression For patients with: 1) < 5% BM blasts: > 50% increase in blasts to >5% 2) 5-10% BM blasts: > 50% increase in blasts to >10% 3) 10-20% BM blasts: > 50% increase in blasts to >20% 4) 20-30% BM blasts: > 50% increase in blasts to >30%
Any of: 1) 50%+ decrease in maximum neutrophil or platelet response 2) Hgb reduction by > 2g/dl 3) Transfusion Dependence
Survival Endpoints: OS: Death by any cause EFS: Treatment failure or death by any cause PFS: progressive disease or death from MDS DFS: time to relapse Cause-specific death: any death related to MDS
Hematologic Improvement (HI)
Responses must be sustained for at least 8 weeks: Erythroid Responses (pre-treatment <11 gm/dl):
• Hgb increase by > 1.5 g/dl • Reduced PRBC transfusions by at least 4 per 8 week period compared to pre-treatment transfusion requirements (only those
given for Hgb < 9 g/dl counted) Platelet Responses (pre-treatment < 100 X 109 /L)
• Absolute increase of > 30 X 109 /L for pts starting with > 20 X 109/L • Increase from < 20 X 109/L to > 20 X 109/L by > 100%
Neutrophil Response (pre-treatment < 1 X 109/L) • > 100% increase and final count > 0.5 X 109/L
Progression or relapse after HI: At least one of the following:
• 50%+ decrease from maximum response in neutrophils or platelets • Hgb reduction by > 1.5 g/dl • Transfusion dependence
Legend: BM = Bone marrow; PB = peripheral blood; g/dl = grams per deciliter; CR = Complete Remission; PR = Partial Remission; HI = Hematologic Response; Hgb = Hemoglobin; OS = Overall Survival; EFS = Event-free survival; PFS = Progression Free Survival; DFS = Disease-Free Survival Adapted from [148]

550 Current Cancer Drug Targets, 2007, Vol. 7, No. 6 Warlick and Smith
[150-154]. Prolonged administration may yield higher responses with Terpos et al. showing response rates approximating 50% in patients with a low blast percentage [155]. Responders are typically limited to patients with significant anemia, transfusion independence, and low endogenous EPO levels [155, 149]. Newer studies using darbepoetin in MDS patients have reported erythroid response rates ranging from 26% in previous erythropoietin failures [156] to rates as high as 71% [157]. Interestingly, new reports have highlighted adverse outcomes in patients receiving high doses of erythropoietin or darbepoetin to achieve a hemoglobin level greater than 12. While tumor progression and decreased survival were the adverse outcomes in head and neck and breast cancer patients respectively, general adverse events included increased venous and arterial thrombosis, strokes, myocardial infarction, and congestive heart failure. Given the increased concern, the FDA has altered its safety information to recommend using the lowest dose of the agent needed to decrease transfusion requirements, increasing the hemoglobin gradually, and not exceeding a hemoglobin level of 12mg/dl.1 While these studies prompt caution in the extended use of erythropoietin growth factors in MDS patients, reaching a hemoglobin level greater than 12 is unusual, and consequently the degree to which these findings will affect this patient population is yet to be determined.
Allogeneic Stem Cell Transplantation Allogeneic stem cell transplant, the only known curative treatment option for MDS patients, lies at the other treatment extreme. Unfortunately, several factors limit its application for most patients and include advanced age, poor performance status, limited access to an HLA matched sibling or matched un-related donor (MUD), and significant potential for treatment related morbidity and mortality. Despite these problems, allogeneic transplants are commonly recommended for younger patients. Transplant outcomes for more than 452 MDS patients conducted and reported by the IBMTR from 1989 through 1997 were recently presented. The median age of the group undergoing the transplant was 38 years with an overall disease free survival of 53% at 1 year and 40% at 3 years and cumulative incidences of relapse of 17% at 1 year and 23% at 3 years [158]. The most important predictor of survival was the blast percentage prior to transplant with increased relapse correlating with increasing blast percentage and higher IPSS scores. Transplant-related mortality was 32% at 1 year and 37% at 3 years. Generally, most data cite improved transplant outcomes in patients treated both early in their disease course and with low level disease [158]. Alternative reports indicate that some pause should be taken when making decisions regarding allogeneic BMT in younger or low risk MDS patients. Kuendgen et al. reported their series following over 200 untreated MDS patients younger than 50 years of age in an attempt to establish a more accurate natural history of disease and compared their outcomes to a registry of over 2000 MDS patients older than 50. In IPSS low risk or INT-1 disease, untreated patients less than 50 years of age had an overall survival nearing 80% (median still not reached at 360 months) compared to an overall survival less than 20% with a median of 45 months in the untreated older cohort [159]. In IPSS INT-2 or high risk disease, there appeared to be no difference in survival between the two age groups thus indicating that age was an important predictor for survival particularly in IPSS early stage disease, while treatment more a predictor of outcome in advanced stage disease. The study also evaluated outcomes comparing treatment versus best supportive care and showed no improvement in survival in low risk and INT-1 disease but superior outcomes in treated INT-2 and high risk IPSS disease [159]. Additionally, Cutler et al. contributed to decision analysis for use of alloBMT in MDS patients and showed improved outcomes when transplant was delayed from diagnosis but completed prior to leukemic transformation in low risk MDS [160]. With previous
1www.FDA-news.com. 3/1/2007 report: FDA Warnings Regarding High Dose Erythropoietin Products.
reports recommending allogeneic BMT for young patients with low grade, early stage disease, these data provide an updated perspective and would suggest that in young, low risk and INT-1 IPSS MDS patients, transplant should be delayed until IPSS progression or progression of cytogenetic abnormalities. Most patients will not be considered medical candidates for myeloablative preparative regimens, and many of those who are candidates will not have a matched sibling donor. Strategies have evolved to make allogeneic treatments more broadly available by developing approaches that adjust for each of the limiting factors. Reduced intensity conditioning (RIC) and non-myeloablative regimens have successfully minimized the preparative regimen toxicities to make older patients and those with mild to moderate end-organ dysfunction eligible. Graft manipulation methods have focused on decreasing the rates and severity of the most lethal complication of allogeneic transplants, graft versus host disease. In addition, alternative stem cell sources, including the use of cord blood stem cells and haploidentical stem cells, have been developed to expand the donor pool. Recent retrospective analysis of 993 MDS patients undergoing allogeneic transplant comparing myeloablative and reduced intensity conditioning (RIC) regimens showed improvements in favor of RIC in terms of non-relapse mortality at 3 years (22% vs. 32%) and rates of acute GVHD (43% vs. 58%); however, these “improvements” were offset by a higher rate of relapse at 3 years (45% vs. 27%) [161]. Not surprisingly, relapse rates were higher in individual risk groups of older age (>50 years), poor risk cytogenetics, and in those undergoing transplant greater than 6 month from diagnosis. Interestingly, the overall survival and progression free survival rates were not statistically different between the two groups with 3 year OS of 41% and 45% in RIC and myeloablative regimens respectively and a 3 year PFS of 33% and 39% [161]. Reduced intensity regimens, or non-myeloablative regiments, have thus been successful with regards to decreasing transplant-related toxicity in terms of end organ toxicity; however, this proposed benefit has been offset by the higher incidence of relapse, mixed chimerism, and similar or higher rates of GVHD [162-165]. One proposed mechanism for the increased relapse, or decreased graft versus leukemia effect, is the loss of direct cytoreduction and increased occurrence of mixed chimerism from reduced intensity preparative regimens [162]. Despite the fact that RIC regimens allow for use of alloBMT in the older MDS population, several reports now suggest the importance of preparative regimen dose intensity for allogeneic BMT in MDS, particularly due to its ability to control active disease [162-165]. Unfortunately, better disease control with intensity comes at the expense of increased mortality, particularly in elderly patients. Given these issues, an alternative method of transplant maintaining conditioning intensity while decreasing treatment related toxicity and adequately dealing with relapse is needed. The use of T cell depleted allografts following a myeloablative preparative regimen could reduce the toxicity of alloBMT while maintaining dose intensity; however, the success of TCD has also been limited due to increased relapse [166, 158] suggesting that in such settings additional post-BMT interventions are needed. Efforts are also underway to expand the potential source of donors for MDS patients requiring bone marrow transplantation by using alternative stem cell sources such as cord blood and haploidentical transplants. A recent analysis of 22 MDS patients undergoing unrelated cord blood transplants showed a four year disease free survival of 76% with relatively low severe acute GVHD and a moderate degree of extensive stage chronic GVHD [167] showing feasibility of this alternative source of bone marrow for patients without a suitable matched unrelated donor. Additionally, recent studies with haploidentical donors have shown similar outcomes to fully-matched transplants in terms of GVHD and morbidity and mortality in myeloid malignancies with only advanced acute leukemia associated with higher rates of relapse and mortality

Myelodysplastic Syndromes Current Cancer Drug Targets, 2007, Vol. 7, No. 6 551
[168]. Efforts continue to expand the potential alternative donor source and improve upon outcomes. Targeting Epigenetic Changes Within the past 3 years, options for the medical management of MDS has evolved from the limited supportive care approach of careful count monitoring, transfusions, and growth factors to now having 3 FDA-approved agents indicated for the treatment of patients with MDS. This progress has led to enthusiasm among physicians and their patients and families. However, the availability of these drugs has raised many important questions including how to best use each of the drugs including when to initiate therapy, which agent to use, and how to best administer each of the drugs. There is also intensive ongoing investigation to better understand the mechanism of action of each of the drugs. The data supporting the close relationship between epigenetic modifications and the biology of MDS grows almost daily. Importantly, 5-azacitidine and decitabine, two newly FDA approved DNA methyltransferase inhibitors, are clinically effective in high risk MDS and appear to work at least in part, by reversing these epigenetic changes. The agents cause demethylation of commonly involved promoter regions by incorporation into DNA as nucleoside analogues resulting in inhibition of the methyltransferase activity responsible for maintaining these hyper-methylated regions [169]. A phase III CALGB trial comparing 5-azacitidine versus best supportive care showed an overall response rate of 60% (7% CR, 16 % PR, and 37% improved) compared to only 5% in the supportive care only arm [170]. The responses also appeared to confer a survival advantage and a decrease in the risk of AML transformation (21 months versus 13 months) in the 5-azacitidine treated group [170]. Retrospective analysis of several 5-azacitidine trials done in the CALGB (trials 8421, 8921, and 9221) incorporated the new IWG [171] response criteria (Table III) and confirmed its effectiveness but showed lower complete response rates (10-17%) and increased hematologic responses (23-26%) with most responses being seen by the sixth cycle [171]. Similar response data also exists for a second, FDA-approve DNA methyltransferase inhibitor, decitabine. Early studies with varying treatment schedules showed hematopoietic responses nearing 50% [172, 173] and lead to further Phase III trials randomizing patients to decitabine versus best supportive care. In this Phase III study, the decitabine treatment resulted in a complete response rate of 9%, a hematologic improvement rate of 13%, and median response duration of 10 months [174]. Although no survival benefit was seen, most patients became transfusion independent and there was a trend towards a delay to AML transformation or death [174]. Retrospective subset review suggested that responses were associated with cytogenetic complete remissions in 35% of patients [174]. More recent studies have focused on improving dosing schedules of decitabine (namely lower dosing over increased days) for higher risk MDS patients and show higher CR rates (21-30%) and overall responses of up to 73% noting a median of 3 cycles needed to obtain CR [175]. Chromatin remodeling via histone acetylation status is a second epigenetic target [176] with histone deacetylase inhibitors (HDIs) another group of agents used to modify epigenetic changes. Acetylation of lysine residues on the N-terminus of core histones creates an open and readily transcribable chromatin structure. HDIs function to reverse the gene silencing caused by deacetylation and maintain the histones in an acetylated and transcribable state [100] and exist as several different classes of drugs including hydroximates (trichostatin A and SAHA), cyclic peptides (cyclic tetrapeptides), aliphatic acids (phenylbutyrate and valproic acid), and benzamides (MS-275) [177]. A variety of clinical trials have shown both single agent clinical and biologic activity. For example, the use of valproic acid either alone or in combination with all-trans-retinoic acid (ATRA) in MDS patients has shown an overall hematologic response rate of 24%. Interestingly, response rate correlated inversely with
bone marrow blast percentage and those with a normal blast count had a greater than 50% response rate while those with > 10% blasts (RAEB I or II) had only a 6% response rate [178, 179]. Additional studies with various HDIs such as MS-275, valproic acid, and SAHA are ongoing.
Use of IMIDS as Immune Therapy Cyclosporine and ATG were among the first immunomodulatory agents used in the treatment of MDS and showed partial success in producing transfusion independence [129, 130]. The mechanism of action of these agents remained unclear, but investigators identified a small subset of patients, typically RA patients with less than 5% blasts, with the following associations that responded with transfusion independence: HLA-DR15 or HLA-DR2 association, younger age, and shorter duration of red cell transfusion dependence [180]. Efforts to study agents that had immunomodulatory impact in MDS were undertaken and thalidomide emerged as having mild clinical activity with very interesting potential mechanisms of action, including: 1) immunomodulatory effects related to a shift of T cell response from Th1 to a Th2 [181], partial T cell activation via alteration of secondary T cell signals, and increased NK cell number and cellular lytic activity [182]; 2) anti-angiogenic properties through possible mechanisms such as nitric oxide inhibition and blockage of endothelial cell migration [183], inhibition of VEG-F and bFGF [120], inhibition of TNF-alpha-induced upregulation of cell adhesion markers, [184] and additional TNF-alpha independent mechanisms [185]; 3) alterations of the bone marrow microenvironment through the impact of cytokines and augmentation of stromal cell growth [120]; 4) alterations of apoptosis [182, 186]; and 5) alterations of adhesion molecule expression [187, 182]. Early studies of thalidomide’s effectiveness in patients with MDS reported 31% hematologic responses after twelve weeks of therapy [188]. Subsequent studies revealed response rates from minimal to nearly 50% with partial success inducing transfusion independence seen in a subset of patients [189-192]. Unfortunately, the side effect profile of hypotension, neuropathy, constipation, and drowsiness makes the drug poorly tolerated, especially in elderly patients [190]. Consequently, based on the clinical activity of thalidomide, newer analogues have been developed to try to minimize side effects. Lenalidomide is the only currently clinically available thalidomide analogue for treatment of patients with MDS. It is reported to share many of the same mechanisms of action with thalidomide; however, lenalidomide has not shown the same effect on endothelial cell proliferation [193-195]. Given the better toxicity profile and similar mechanism of action, clinical investigation by List et al. began with early phase I/II trials showing extraordinary clinical response specifically in a subset of MDS patients who either hadn’t responded to EPO therapy or had high endogenous levels, had low risk IPSS, or had cytogenetic abnormalities involving chromosome 5 [196]. The study boasted a 56% overall hematologic response rate across all cytogenetic abnormalities; in predominantly low risk IPSS, with 63% of previously transfusion-dependant patients achieving transfusion independence. Median time to hematologic response ranged from 9 to 11.5 weeks depending on the dose of lenalidomide. Hematologic effects, primarily erythroid, were the most notable in patients with deletion 5q31. Additionally, complete cytogenetic responses were seen in 50% with a median time to response of 8 weeks. Toxicities included significant neutropenia and thrombocytopenia in greater than half the patients [196]. Further larger scale trials are ongoing to study the effects of lenalidomide in specific subsets of MDS and have substantiated the early success [197]. Additionally, trials investigating the combination of lenalidomide with other agents are ongoing.
NEW THERAPEUTIC APPROACHES UNDER DEVELOP-MENT FOR MDS The incredibly complex pathophysiology intrinsic to MDS provides many targets and fertile ground for investigators to develop

552 Current Cancer Drug Targets, 2007, Vol. 7, No. 6 Warlick and Smith
new treatment approaches. A very well done recent review captured many of these approaches [199]. We focus our new therapeutic discussion on three areas under development at our own institution:
epigenetics, immune modulation, and differentiation-based approaches.
Table IV. Standard Treatments for MDS
Treatment Categories Drugs Dose Expected Response Studies
Erythropoietin Standard Starting Dose: • 150 IU/kg SQ 3 times weekly
(Micromedix) vs.
• 40,000-60,000 IU 2-3 times a week for 2-3 months (NCCN Guidelines)
• Prolonged EPO administration
(minimum 26 weeks) using 150 IU/kg 3 times weekly dose
Overall HR: 16% [149] RR by certain characteristics: • Trans. Indep. vs. Dep. (44% vs. 10%) • Mode using FAB group (RARS vs. other)
+ Epo level + trans. status predicts response to EPO
• MDS (not RARS) + Trans. Indep. RR >50%
• RARS + EPO>200U/l RR=0% Overall RR: 45% Better RR if: • low blast % • Good Cytogenetics • EPO<150U/l
Hellstrom-Linberg et al. Meta-analysis [149] Terpos et al. [155]
Darbepoetin ** under investigation for MDS
• 300mcg SQ weekly then 300mcg SQ q2weeks maintenance
• Transition from EPO to Dar:
Darbepoetin dose 200mcg q2weeks
Tx for 12 wks: ER: 71% • 8/13 patients previous EPO non-
responders Tx. Naive Patients: • Epo: MR 35% • Dar: MR 46% Prev EPO: • Epo: MR 17% • Dar: MR 26%
Mannone et al. [157]
Patton et al. [156]
Growth Factors
Erythropoietin + G-CSF
Varied Schedules • EPO 5000-10,000 IU/day SQ + G-
CSF 30-75-150mcg/day SQ • EPO 300U/kg 3 times weekly for
8 weeks + G-CSF 1mcg/kg/day SQ
• G-CSF 1mcg/kg daily X 2 weeks then EPO 300U /Kg per day for minimum 8 weeks combined then G-CSF stopped
• Review of studies
Results: Overall ER: 38% ER: 50% Combined treatment: • Neutrophil response 96% and ER 48% After G-CSF Cessation: • All neutrophil responses lost and 8/55
continued ER
Hellstrom-Lindberg et al. [198]
Remacha et al. [152] Negrin et al.[153] Kasper et al. [154]
5-Azacitidine 75mg/m2 SQ qd X 7 days q4 weeks Response Typically Seen after 4 cycles: Phase III CALGB: OR: 60% CR: 7% + PR: 16% + Improved: 37% CALGB Reanalysis: CR: 10-17% HR: 23-26% Majority of Responses seen by 6th cycle
Silverman et al. [170] Silverman et al. [171]
Epigenetic Modulators DNA Methyltransferase Inhibitors (DMTIs)
Decitabine 15mg/m2 IV q8hours times 3 days q6 wks Alternative Treatment Schedules: Total Dose: 100mg/m2 20mg/m2 IV qd X 5d 20mg/m2 SQ qd X 5d 10mg/m2 IV qd X 10d
Phase III Trial: OR: 30% CR: 9% + PR: 8% + HR: 13% • All responders gained trans. indep. • Majority of Responders: cytogenetic
response Overall Response: 73% CR: 34% + PR: 1% + Marrow CR: 11% + Marrow CR + HI: 14% + HI: 13% CR % per dosing schedule: 20mg/m2 IV: 39% 20mg/m2 SQ: 21% 10mg/ms IV: 24%
Kantarjian et al. [174] Kantarjian et al. [175]
Standard Myeloablative Conditioning
Per specific regimens 3 yr DFS: 40% 3 yr Relapse Rate: 23% 3 yr TRM: 37%
IBMTR Data/ Sierra et al. [158]
Reduced Intensity Conditioning
Per specific Regimens 3 yr PFS: 33% 3 yr Relapse Rates: 45% 3 year NRM: 22%
Martino et al. [161]
Bone Marrow Transplant
T Cell Depletion (TCD)
Per specific regimen Entire Group: 2 yr DFS: 39% 2 yr Relapse: 34% RA Pts: DFS: 73% Relapse: 11% Advanced MDS: (in CRI) DFS: 42% Relapse: 34% IBMTR Data: TCD Relative Risk of TRM: 0.6 Relative Risk of Relapse: 1.8
Mattijssen et al. [166] Sierra et al. [158]
Thalidomide 100mg titrated to 400mg/day for 12 wks Survey of studies
ER: 31% Varied Response: • 0 – 50%
Raza et al. [188] Numerous Studies [189-192]
Immunotherapy
Lenalidomide 10mg po qday 10mg/day for 21 days
ER: 54%
ER: 65% Improved Response: Low IPSS/FAB class and highest in del5q-83%
List et al. [196]
Legend: Trans. = Transfusion; Indep. = Independence; Dep.= Dependence; kg = kilogram; mcg = microgram; OR = Overall response; MR = Major Response; Epo = Erythropoietin; CR = Complete response; ER = Erythroid Response; Dar = Darbepoetin; PR = Partial response; RARS = Refractory Anemia w/ Ringed Sideroblasts; HR = Hematologic Response; RR = Response Rate; mg/m2 = milligrams per meters squared; CALGB = The Cancer and Leukemia Group B; NRM = Non-relapse mortality; TRM = Treatment-related mortality; DFS = Disease Free Survival; PFS = Progression Free Survival; Pts = patients, TCD = T Cell Depletion.

Myelodysplastic Syndromes Current Cancer Drug Targets, 2007, Vol. 7, No. 6 553
Epigenetic Treatments – Expanding Targets Epigenetic modulation through a combination of DMTIs and HDIs seemed to be a logical approach noting the responses seen with these individual classes of agents. A pilot study combining phenylbutyrate (HDI) with 5-azacitidine showed that both complete and partial remissions could be achieved in nearly half of the MDS and AML patients and showed a strong association between the clinical responses and changes in hypermethylation and expression of p15 [200]. The clinical responses were supported with findings from a second pilot study of the same combination [201]. Gore et al. combined MS-275 (HDI) with 5-azacitidine (DMTI) in a follow-up pilot study recently presented in abstract form at ASH 20062. Thirty one patients (13 MDS, 4CMMol, and 14 AML 4 of which had multi-lineage dysplasia) were treated with the combination. Azacitidine was given in 3 different doses subcutaneously for 10 days and MS-275 was given orally in 4 different doses on day 3 and 10 of a 28 day cycle. The treatment regimen was based on in vitro studies illustrating the optimal timing for reversal of epigenetic silencing. Of patients with MDS or AML w/ MLD, 50% responded with a median time to best hematologic response of 4 cycles. Of the entire cohort, 6 clinical responses were seen in the 20 patients with cytogenetic abnormalities and included 4 with complete cytogenetic responses. Best cytogenetic responses were seen in a median of 4 cycles. Correlative studies showed increased H3 or H4 acetylation after 5 azacitidine alone in 30% of patients with increase in H3 and H4 acetylation after combination therapy in 25/29 and 28/29 patients respectively. Gore’s study provided additional excitement for the successful combination of DMTIs and HDIs in treating MDS and AML w/ MDL and prompted the current ECOG randomized trial comparing MS-275 + 5-azacitidine to 5-azacitidine alone.
Immune Strategies – Immune System Modulation through Vaccines Vaccine strategies have been employed in many solid tumor malignancies and more recently, hematologic malignancies. Despite the enthusiasm from many clinical immunologists, there is little published clinical efficacy data for these approaches to date. Some strategies are based on targeting tumor antigens preferentially expressed by the cancer cells. Specifically in MDS and AML, much of the vaccines work has been based on overexpressed antigens (WT-1, survivin, and proteinase 3). A peptide vaccine against WT-1 was developed and studied in a phase I trial in Japan [202]. The study treated 12 patients with AML and considered 7 responders based on a decrease in WT-1 serum levels following the vaccines. Of interest, 2 MDS patients receiving the vaccine became markedly cytopenic. Based on concerns that the vaccine may in fact be targeting both normal and MDS stem cells, no further patients with MDS were enrolled [202]. However, this may be the stronger piece of correlative data supporting the activity of such approaches. Currently at the Sidney Kimmel Cancer Center at Johns Hopkins, we have created a pilot study evaluating the use of an institutionally-developed, K562/GM-CSF secreting vaccine in patients with MDS. Given that K562 expresses a number of defined myeloid antigens, such as WT-1, proteinase 3, and survivin, found overexpressed in MDS as well as other myeloid malignancies, it has the potential to generate specific anti-tumor responses to these antigens. Open to 15 MDS patients, our trial will evaluate treatment success based on clinical parameters including resolution of cytogenetic abnormalities or improvement of transfusion requirements with additional investigation of immune correlates.
2 Gore, S. D.; Jiemjit, A.; Silverman, L. B.; Aucott, T.; Baylin, S.; Carraway, H.; Dauses, T.; Fandy, T.; Herman, J.; Karp, J.; Licht, J. D.; Murgo, A. J.; Odchimar-Reissig, R.; Smith, B. D.; Zwiebel, J. A.; Sugar, E. Combined Methyltransferase/Histone Deacetylase Inhibition with 5-Azacitidine and MS-275 in Patients with MDS, CMMoL and AML: Clinical Response, Histone Acetylation and DNA Damage. Blood (ASH Annual Meeting Abstracts) 2006, 108, 517.
Differentiation Therapy – Combinations that Improve Responses The outstanding success of ATRA in the treatment of acute promyelocytic leukemia (APL) is proof of the principle that differentiation therapy has potential to be an important therapy [203]. MDS has also been the target of attempts at utilizing differentiation therapy with the use of agents such as interferon, polar planar compounds, homoharringtonine, 5-azacitidine, ara-c, butyrates, amifostine, retinoids, vitamin D derivatives, growth factors, and/or combinations of the above drugs [204]. Each of these agents has shown glimpses of differentiating activity, including single agent interferon [205-209], demethylating agents [170, 171, 173, 174], vitamin D derivatives [210-212], and retinoids in combination with other compounds [179, 213, 214]. Interestingly, each of these agents appears to have differing mechanisms of action raising the question of how pharmacologic differentiating agents actually work. In vitro studies have shown that lineage-specific growth factors can enhance the activity of many pharmacologic differentiation agents noted above in both AML and MDS cell lines and primary bone marrow cells [215-217]. Further investigation noted that this synergy only occurred with cytostatic doses of the pharmacologic differentiating agents. This supported the hypothesis that pharmacologic differentiating agents functioned primarily through inhibition of cell cycle and could preferentially augment the differentiating capacity of growth factors indicating that the agents were not sufficient in and of themselves for terminal differentiation of malignant cells [217]. Matsui’s group went on to show that growth factors were actually required for substantial in vitro differentiation [215-217]. While growth factors alone are sufficient to induce differentiation, their use as single agents is limited due to their pleiotropic effects of stimulating proliferation and enhancing survival via inhibition of apoptosis [218, 219]. Thus, in theory, preferential enhancement of self-renewal and survival could cause tumor progression while selective induction of differentiation could exhaust the neoplastic clone. This hypothesis was recently tested in a phase I study with the differentiating agent bryostatin in combination with GM-CSF at the Sidney Kimmel Cancer Center at Johns Hopkins. Bryostatin, a protein kinase C agonist, was administered via continuous infusion in a dose escalation fashion. Smith and colleagues3 found that Bryostatin, in conjunction with GM-CSF, had remarkable clinical activity with 1 poor risk AML patient achieving a CR following a single course of the combination therapy and a second MDS patient having a morphologic CR and partial cytogenetics response following 2 cycles. Unfortunately, further development was limited due to an intolerable side effect profile at clinically active doses. Future directions that build upon these principles include agents with in vitro activity in combination with growth factors including the HDI, MS-275, and novel retinoids, like bexarotene.
SUMMARY The myelodysplastic syndromes are an incredibly complex spectrum of hematopoietic stem cell disorders. Their range of severity along with variations in response to multiple treatment approaches suggests that the pathophysiology underpinning these disorders is just as complex. We are only beginning to unravel the biology of MDS. This review hopes to not only provide a broad introduction to the complex pathways involved in the development and progression of these disorders but also to intrigue and challenge both basic and clinical scientists to continue to work towards unlocking the mysteries of MDS.
3 Smith, B. D.; Matsui, W.; Gladstone, D. E.; Karp, J.; Gore, S.; Huff, C. A.; Vala, M.; Baker, S.; Zhao, M.; Piantadosi, S.; Jones, R. J. Differentiation Therapy for Poor Risk Myeloid Malignancies: Results of a Dose Finding Study of Bryostatin-1 (BRYO) + GM-CSF. Blood (ASH Annual Meeting Abstracts) 2005, 106, 2792.

554 Current Cancer Drug Targets, 2007, Vol. 7, No. 6 Warlick and Smith
ACKNOWLEDGEMENTS Special thanks to Dr. Michael Mcdevitt for review of the manuscript and expert advice. Special thanks to Dr. Steven Gore for his instrumental help in development of the Hopkins Treatment Algorithm. Special thanks also to Kimberly Pate for her help in table and manuscript formatting.
REFERENCES [1] Aul, C.; Giagounidis, U.; Germing, U. Epidemiological features of
myelodysplastic syndrome: real or factitious? Int. J. Hematol. 2001, 73(4), 405-410.
[2] Yin, S. N.; Hayes, R. B.; Linet, M. S.; Li, G. L.; Dosemeci, M.; Travis, L. B.; Li, C. Y.; Zhang, Z. N.; Li, D. G.; Chow, W. H.; Wacholder, S.; Wang, Y. Z.; Jiang, Z. L.; Dai, T. R.; Zhang, W. Y.; Chao, X. J.; Ye, P. Z.; Kou, Q. R.; Zhang, X. C.; Lin, X. F.; Meng, J. F.; Ding, C. Y.; Zho, J. S.; Blot, W. J. A cohort study of cancer among benzene-exposed workers in China: overall results. Am. J. Ind. Med. 1996, 29(3), 227-235.
[3] West, R. R.; Stafford, D. A.; Farrow, A.; Jacobs, A. Occupational and environmental exposures and myelodysplasia: a case-control study. Leuk. Res. 1995, 19(2), 127-139.
[4] Moloney, W. C. Radiogenic leukemia revisited. Blood 1987, 70(4), 905-908. [5] Pedersen-Bjergaard, J.; Philip, P.; Larsen, S. O.; Andersson, M.; Daugaard,
G.; Ersboll, J.; Hansen, S. W.; Hou-Jensen, K.; Nielsen, D.; Sigsgaard, T. C. Therapy-related myelodysplasia and acute myeloid leukemia. Cytogenetic characteristics of 115 consecutive cases and risk in seven cohorts of patients treated intensively for malignant diseases in the Copenhagen series. Leukemia 1993, 7(12), 1975-1986.
[6] Pasqualetti, P.; Festuccia, V.; Acitelli, P.; Collacciani, A.; Giusti, A.; Casale, R. Tobacco smoking and risk of haematological malignancies in adults: a case-control study. Br. J. Haematol. 1997, 97(3), 659-662.
[7] Ido, M.; Nagata, C.; Kawakami, N.; Shimizu, H.; Yoshida, Y.; Nomura, T.; Mizoguchi, H. A case-control study of myelodysplastic syndromes among Japanese men and women. Leuk. Res. 1996, 20(9), 727-731.
[8] Mundle, S.; Allampallam, K.; Aftab, R. K.; Dangerfield, B.; Cartlidge, J.; Zeitler, D.; Afenya, E.; Alvi, S.; Shetty, V.; Venugopal, P.; Raza, A. Presence of activation-related m-RNA for EBV and CMV in the bone marrow of patients with myelodysplastic syndromes. Cancer Lett. 2001, 164(2), 197-205.
[9] Dalamaga, M.; Petridou, E.; Cook, F. E.; Trichopoulos, D. Risk factors for myelodysplastic syndromes: a case-control study in Greece. Cancer Causes Control. 2002, 13(7), 603-608.
[10] Rund, D.; Ben Yehuda, D. Therapy-related leukemia and myelodysplasia: evolving concepts of pathogenesis and treatment. Hematology 2004, 9(3), 179-187.
[11] Olney, H. J.; Le Beau, M. M. The cytogenetics of myelodysplastic syndromes. Best. Pract. Res. Clin. Haematol. 2001, 14(3), 479-495.
[12] Parker, J. E.; Mufti, G. J.; Rasool, F.; Mijovic, A.; Devereux, S.; Pagliuca, A. The role of apoptosis, proliferation, and the Bcl-2-related proteins in the myelodysplastic syndromes and acute myeloid leukemia secondary to MDS. Blood 2000, 96(12), 3932-3938.
[13] Rajapaksa, R.; Ginzton, N.; Rott, L. S.; Greenberg, P. L. Altered oncoprotein expression and apoptosis in myelodysplastic syndrome marrow cells. Blood 1996, 88(11), 4275-4287.
[14] Parker, J. E.; Mufti, G. J. Ineffective haemopoiesis and apoptosis in myelodysplastic syndromes. Br. J. Haematol. 1998, 101(2), 220-230.
[15] Rosenfeld, C.; List, A. A hypothesis for the pathogenesis of myelodysplastic syndromes: implications for new therapies. Leukemia 2000, 14(1), 2-8.
[16] Bennett, J. M.; Catovsky, D.; Daniel, M. T.; Flandrin, G.; Galton, D. A.; Gralnick, H. R.; Sultan, C. Proposals for the classification of the acute leukaemias. French-American-British (FAB) co-operative group. Br. J. Haematol. 1976, 33(4), 451-458.
[17] Bennett, J. M.; Catovsky, D.; Daniel, M. T.; Flandrin, G.; Galton, D. A.; Gralnick, H. R.; Sultan, C. Proposals for the classification of the myelodysplastic syndromes. Br. J. Haematol. 1982, 51(2), 189-199.
[18] Steensma, D. P.; Tefferi, A. The myelodysplastic syndrome(s): a perspective and review highlighting current controversies. Leuk. Res. 2003, 27(2), 95-120.
[19] Steensma, D. P.; Bennett, J. M. The myelodysplastic syndromes: diagnosis and treatment. Mayo Clin. Proc. 2006, 81(1), 104-130.
[20] Harris, N. L.; Jaffe, E. S.; Diebold, J.; Flandrin, G.; Muller-Hermelink, H. K.; Vardiman, J.; Lister, T. A.; Bloomfield, C. D. World Health Organization classification of neoplastic diseases of the hematopoietic and lymphoid tissues: report of the Clinical Advisory Committee meeting-Airlie House, Virginia, November 1997. J. Clin. Oncol. 1999, 17(12), 3835-3849.
[21] Vardiman, J. W.; Harris, N. L.; Brunning, R. D. The World Health Organization (WHO) classification of the myeloid neoplasms. Blood 2002, 100(7), 2292-2302.
[22] Greenberg, P.; Cox, C.; LeBeau, M. M.; Fenaux, P.; Morel, P.; Sanz, G.; Sanz, M.; Vallespi, T.; Hamblin, T.; Oscier, D.; Ohyashiki, K.; Toyama, K.; Aul, C.; Mufti, G.; Bennett, J. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood 1997, 89(6), 2079-2088.
[23] Catenacci, D. V.; Schiller, G. J. Myelodysplasic syndromes: A comprehensive review. Blood Rev. 2005, 19(6), 301-319.
[24] Mufti, G. J. Pathobiology, classification, and diagnosis of myelodysplastic syndrome. Best. Pract. Res. Clin. Haematol. 2004, 17(4), 543-557.
[25] Kuang, S.; Liang, W. Clinical analysis of 43 cases of chronic benzene poisoning. Chem. Biol. Interact. 2005, 153-154, 129-135.
[26] Aksoy, M.; Dincol, K.; Erdem, S.; Dincol, G. Acute leukemia due to chronic exposure to benzene. Am. J. Med. 1972, 52(2), 160-166.
[27] Yardley-Jones, A.; Anderson, D.; Parke, D. V. The toxicity of benzene and its metabolism and molecular pathology in human risk assessment. Br. J. Ind. Med. 1991, 48(7), 437-444.
[28] Hiraku, Y.; Kawanishi, S. Oxidative DNA damage and apoptosis induced by benzene metabolites. Cancer Res. 1996, 56(22), 5172-5178.
[29] Smith, M. T. The mechanism of benzene-induced leukemia: a hypothesis and speculations on the causes of leukemia. Environ. Health Perspect. 1996, 104(Suppl. 6), 1219-1225.
[30] Rothman, N.; Haas, R.; Hayes, R. B.; Li, G. L.; Wiemels, J.; Campleman, S.; Quintana, P. J.; Xi, L. J.; Dosemeci, M.; Titenko-Holland, N. Benzene induces gene-duplicating but not gene-inactivating mutations at the glycophorin A locus in exposed humans. Proc. Natl. Acad. Sci. USA 1995, 92(9), 4069-4073.
[31] Aul, C.; Bowen, D. T.; Yoshida, Y. Pathogenesis, etiology and epidemiology of myelodysplastic syndromes. Haematologica 1998, 83(1), 71-86.
[32] Pedersen-Bjergaard, J.; Andersen, M. K.; Christiansen, D. H.; Nerlov, C. Genetic pathways in therapy-related myelodysplasia and acute myeloid leukemia. Blood 2002, 99(6), 1909-1912.
[33] Matsuo, T.; Tomonaga, M.; Bennett, J. M.; Kuriyama, K.; Imanaka, F.; Kuramoto, A.; Kamada, N.; Ichimaru, M.; Finch, S. C.; Pisciotta, A. V. Reclassification of leukemia among A-bomb survivors in Nagasaki using French-American-British (FAB) classification for acute leukemia. Jpn. J. Clin. Oncol. 1988, 18(2), 91-96.
[34] Kadhim, M. A.; Lorimore, S. A.; Hepburn, M. D.; Goodhead, D. T.; Buckle, V. J.; Wright, E. G. Alpha-particle-induced chromosomal instability in human bone marrow cells. Lancet 1994, 344(8928), 987-988.
[35] Kitagawa, M.; Yamaguchi, S.; Takahashi, M.; Tanizawa, T.; Hirokawa, K.; Kamiyama, R. Localization of Fas and Fas ligand in bone marrow cells demonstrating myelodysplasia. Leukemia 1998, 12(4), 486-492.
[36] Ogawa, T.; Kitagawa, M.; Hirokawa, K. Age-related changes of human bone marrow: a histometric estimation of proliferative cells, apoptotic cells, T cells, B cells and macrophages. Mech. Ageing Dev. 2000, 117(1-3), 57-68.
[37] Sawanobori, M.; Yamaguchi, S.; Hasegawa, M.; Inoue, M.; Suzuki, K.; Kamiyama, R.; Hirokawa, K.; Kitagawa, M. Expression of TNF receptors and related signaling molecules in the bone marrow from patients with myelodysplastic syndromes. Leuk. Res. 2003, 27(7), 583-591.
[38] Moyzis, R. K.; Buckingham, J. M.; Cram, L. S.; Dani, M.; Deaven, L. L.; Jones, M. D.; Meyne, J.; Ratliff, R. L.; Wu, J. R. A highly conserved repetitive DNA sequence, (TTAGGG)n, present at the telomeres of human chromosomes. Proc. Natl. Acad. Sci. USA 1988, 85(18), 6622-6626.
[39] Iwama, H.; Ohyashiki, K.; Ohyashiki, J. H.; Hayashi, S.; Yahata, N.; Ando, K.; Toyama, K.; Hoshika, A.; Takasaki, M.; Mori, M.; Shay, J. W. Telomeric length and telomerase activity vary with age in peripheral blood cells obtained from normal individuals. Hum. Genet. 1998, 102(4), 397-402.
[40] Allsopp, R. C.; Vaziri, H.; Patterson, C.; Goldstein, S.; Younglai, E. V.; Futcher, A. B.; Greider, C. W.; Harley, C. B. Telomere length predicts replicative capacity of human fibroblasts. Proc. Natl. Acad. Sci. USA 1992, 89(21), 10114-10118.
[41] Kim, N. W.; Piatyszek, M. A.; Prowse, K. R.; Harley, C. B.; West, M. D.; Ho, P. L.; Coviello, G. M.; Wright, W. E.; Weinrich, S. L.; Shay, J. W. Specific association of human telomerase activity with immortal cells and cancer. Science 1994, 266(5193), 2011-2015.
[42] Shay, J. W.; Bacchetti, S. A survey of telomerase activity in human cancer. Eur. J. Cancer 1997, 33(5), 787-791.
[43] Engelhardt, M.; Kumar, R.; Albanell, J.; Pettengell, R.; Han, W.; Moore, M. A. Telomerase regulation, cell cycle, and telomere stability in primitive hematopoietic cells. Blood 1997, 90(1), 182-193.
[44] Ohyashiki, J. H.; Iwama, H.; Yahata, N.; Ando, K.; Hayashi, S.; Shay, J. W.; Ohyashiki, K. Telomere stability is frequently impaired in high-risk groups of patients with myelodysplastic syndromes. Clin. Cancer Res. 1999, 5(5), 1155-1160.
[45] Hirai, H. Molecular mechanisms of myelodysplastic syndrome. Jpn. J. Clin. Oncol. 2003, 33(4), 153-160.
[46] Look, A. T. Molecular Pathogenesis of MDS. Hematology (Am. Soc. Hematol. Educ. Program) 2005, 156-160.
[47] Nimer, S. D. Clinical management of myelodysplastic syndromes with interstitial deletion of chromosome 5q. J. Clin. Oncol. 2006, 24(16), 2576-2582.
[48] Jary, L.; Mossafa, H.; Fourcade, C.; Genet, P.; Pulik, M.; Flandrin, G. The 17p-syndrome: a distinct myelodysplastic syndrome entity? Leuk. Lymphoma 1997, 25(1-2), 163-168.
[49] Paulsson, K.; Johansson, B. Trisomy 8 as the sole chromosomal aberration in acute myeloid leukemia and myelodysplastic syndromes. Pathol. Biol. (Paris) 2007, 55(1), 37-48.
[50] Boultwood, J.; Lewis, S.; Wainscoat, J. S. The 5q-syndrome. Blood 1994, 84(10), 3253-3260.
[51] Nimer, S. D.; Golde, D. W. The 5q- abnormality. Blood 1987, 70(6), 1705-1712.

Myelodysplastic Syndromes Current Cancer Drug Targets, 2007, Vol. 7, No. 6 555 [52] Fairman, J.; Chumakov, I.; Chinault, A. C.; Nowell, P. C.; Nagarajan, L.
Physical mapping of the minimal region of loss in 5q- chromosome. Proc. Natl. Acad. Sci. USA 1995, 92(16), 7406-7410.
[53] Zhao, N.; Stoffel, A.; Wang, P. W.; Eisenbart, J. D.; Espinosa, R., III; Larson, R. A.; Le Beau, M. M. Molecular delineation of the smallest commonly deleted region of chromosome 5 in malignant myeloid diseases to 1-1.5 Mb and preparation of a PAC-based physical map. Proc. Natl. Acad. Sci. USA 1997, 94(13), 6948-6953.
[54] Jaju, R. J.; Boultwood, J.; Oliver, F. J.; Kostrzewa, M.; Fidler, C.; Parker, N.; McPherson, J. D.; Morris, S. W.; Muller, U.; Wainscoat, J. S.; Kearney, L. Molecular cytogenetic delineation of the critical deleted region in the 5q- syndrome. Genes Chromosomes Cancer 1998, 22(3), 251-256.
[55] Horrigan, S. K.; Arbieva, Z. H.; Xie, H. Y.; Kravarusic, J.; Fulton, N. C.; Naik, H.; Le, T. T.; Westbrook, C. A. Delineation of a minimal interval and identification of 9 candidates for a tumor suppressor gene in malignant myeloid disorders on 5q31. Blood 2000, 95(7), 2372-2377.
[56] Le Beau, M. M.; Espinosa, R., III; Neuman, W. L.; Stock, W.; Roulston, D.; Larson, R. A.; Keinanen, M.; Westbrook, C. A. Cytogenetic and molecular delineation of the smallest commonly deleted region of chromosome 5 in malignant myeloid diseases. Proc. Natl. Acad. Sci. USA 1993, 90(12), 5484-5488.
[57] Boultwood, J.; Fidler, C.; Strickson, A. J.; Watkins, F.; Kostrzewa, M.; Jaju, R. J.; Muller, U.; Wainscoat, J. S. Transcription mapping of the 5q- syndrome critical region: cloning of two novel genes and sequencing, expression, and mapping of a further six novel cDNAs. Genomics 2000, 66(1), 26-34.
[58] Vallespi, T.; Imbert, M.; Mecucci, C.; Preudhomme, C.; Fenaux, P. Diagnosis, classification, and cytogenetics of myelodysplastic syndromes. Haematologica 1998, 83(3), 258-275.
[59] Wattel, E.; Lai, J. L.; Hebbar, M.; Preudhomme, C.; Grahek, D.; Morel, P.; Bauters, F.; Fenaux, P. De novo myelodysplastic syndrome (MDS) with deletion of the long arm of chromosome 20: a subtype of MDS with distinct hematological and prognostic features? Leuk. Res. 1993, 17(11), 921-926.
[60] Davis, M. P.; Dewald, G. W.; Pierre, R. V.; Hoagland, H. C. Hematologic manifestations associated with deletions of the long arm of chromosome 20. Cancer Genet. Cytogenet. 1984, 12(1), 63-71.
[61] Asimakopoulos, F. A.; Green, A. R. Deletions of chromosome 20q and the pathogenesis of myeloproliferative disorders. Br. J. Haematol. 1996, 95(2), 219-226.
[62] Liang, H.; Fairman, J.; Claxton, D. F.; Nowell, P. C.; Green, E. D.; Nagarajan, L. Molecular anatomy of chromosome 7q deletions in myeloid neoplasms: evidence for multiple critical loci. Proc. Natl. Acad. Sci. USA 1998, 95(7), 3781-3785.
[63] Pasquali, F.; Bernasconi, P.; Casalone, R.; Fraccaro, M.; Bernasconi, C.; Lazzarino, M.; Morra, E.; Alessandrino, E. P.; Marchi, M. A.; Sanger, R. Pathogenetic significance of "pure" monosomy 7 in myeloproliferative disorders. Analysis of 14 cases. Hum. Genet. 1982, 62(1), 40-51.
[64] Le Beau, M. M.; Espinosa, R., III; Davis, E. M.; Eisenbart, J. D.; Larson, R. A.; Green, E. D. Cytogenetic and molecular delineation of a region of chromosome 7 commonly deleted in malignant myeloid diseases. Blood 1996, 88(6), 1930-1935.
[65] Merlat, A.; Lai, J. L.; Sterkers, Y.; Demory, J. L.; Bauters, F.; Preudhomme, C.; Fenaux, P. Therapy-related myelodysplastic syndrome and acute myeloid leukemia with 17p deletion. A report on 25 cases. Leukemia 1999, 13(2), 250-257.
[66] Albin, M.; Bjork, J.; Welinder, H.; Tinnerberg, H.; Mauritzson, N.; Johansson, B.; Billstrom, R.; Stromberg, U.; Mikoczy, Z.; Ahlgren, T.; Nilsson, P. G.; Mitelman, F.; Hagmar, L. Acute myeloid leukemia and clonal chromosome aberrations in relation to past exposure to organic solvents. Scand. J. Work Environ. Health 2000, 26(6), 482-491.
[67] Thirman, M. J.; Larson, R. A. Therapy-related myeloid leukemia. Hematol. Oncol. Clin. North Am. 1996, 10(2), 293-320.
[68] Wiederschain, D.; Kawai, H.; Shilatifard, A.; Yuan, Z. M. Multiple mixed lineage leukemia (MLL) fusion proteins suppress p53-mediated response to DNA damage. J. Biol. Chem. 2005, 280(26), 24315-24321.
[69] Papenhausen, P. R.; Griffin, S.; Tepperberg, J. Oncogene amplification in transforming myelodysplasia. Exp. Mol. Pathol. 2005, 79(2), 168-175.
[70] Poppe, B.; Vandesompele, J.; Schoch, C.; Lindvall, C.; Mrozek, K.; Bloomfield, C. D.; Beverloo, H. B.; Michaux, L.; Dastugue, N.; Herens, C.; Yigit, N.; De Paepe, A.; Hagemeijer, A.; Speleman, F. Expression analyses identify MLL as a prominent target of 11q23 amplification and support an etiologic role for MLL gain of function in myeloid malignancies. Blood 2004, 103(1), 229-235.
[71] Pappa, V.; Young, B. D.; Economopoulos, T.; Papageorgiou, E.; Panani, A.; Lilington, D.; Bollas, G.; Stamouli, M.; Kontsioti, F.; Tsiotra, P.; Vessalas, G.; Dervenoulas, J.; Raptis, S. Absence of MLL gene rearrangement in de novo myelodysplastic syndromes (MDS). Ann. Hematol. 2004, 83(3), 170-175.
[72] Paquette, R. L.; Landaw, E. M.; Pierre, R. V.; Kahan, J.; Lubbert, M.; Lazcano, O.; Isaac, G.; McCormick, F.; Koeffler, H. P. N-ras mutations are associated with poor prognosis and increased risk of leukemia in myelodysplastic syndrome. Blood 1993, 82(2), 590-599.
[73] Bos, J. L. ras oncogenes in human cancer: a review. Cancer Res. 1989, 49(17), 4682-4689.
[74] Harris, C. C.; Hollstein, M. Clinical implications of the p53 tumor-suppressor gene. N. Engl. J. Med. 1993, 329(18), 1318-1327.
[75] Lai, J. L.; Preudhomme, C.; Zandecki, M.; Flactif, M.; Vanrumbeke, M.; Lepelley, P.; Wattel, E.; Fenaux, P. Myelodysplastic syndromes and acute myeloid leukemia with 17p deletion. An entity characterized by specific dysgranulopoiesis and a high incidence of P53 mutations. Leukemia 1995, 9(3), 370-381.
[76] Horiike, S.; Kita-Sasai, Y.; Nakao, M.; Taniwaki, M. Configuration of the TP53 gene as an independent prognostic parameter of myelodysplastic syndrome. Leuk. Lymphoma 2003, 44(6), 915-922.
[77] Wattel, E.; Preudhomme, C.; Hecquet, B.; Vanrumbeke, M.; Quesnel, B.; Dervite, I.; Morel, P.; Fenaux, P. p53 mutations are associated with resistance to chemotherapy and short survival in hematologic malignancies. Blood 1994, 84(9), 3148-3157.
[78] Paulsson, K.; Heidenblad, M.; Strombeck, B.; Staaf, J.; Jonsson, G.; Borg, A.; Fioretos, T.; Johansson, B. High-resolution genome-wide array-based comparative genome hybridization reveals cryptic chromosome changes in AML and MDS cases with trisomy 8 as the sole cytogenetic aberration. Leukemia 2006, 20(5), 840-846.
[79] Verdorfer, I.; Brecevic, L.; Saul, W.; Schenker, B.; Kirsch, M.; Trautmann, U.; Helm, G.; Gramatzki, M.; Gebhart, E. Comparative genomic hybridization-aided unraveling of complex karyotypes in human hematopoietic neoplasias. Cancer Genet. Cytogenet. 2001, 124(1), 1-6.
[80] Wilkens, L.; Tchinda, J.; Burkhardt, D.; Nolte, M.; Werner, M.; Georgii, A. Analysis of hematologic diseases using conventional karyotyping, fluorescence in situ hybridization (FISH), and comparative genomic hybridization (CGH). Hum. Pathol. 1998, 29(8), 833-839.
[81] Babicz, M.; Kowalczyk, J. R.; Winnicka, D.; Gaworczyk, A.; Lejman, M.; Dmowski, R.; Kaczanowska, K. The effectiveness of high-resolution-comparative genomic hybridization in detecting the most common chromosomal abnormalities in pediatric myelodysplastic syndromes. Cancer Genet. Cytogenet. 2005, 158(1), 49-54.
[82] Wilkens, L.; Burkhardt, D.; Tchinda, J.; Busche, G.; Werner, M.; Nolte, M.; Ganser, A.; Georgii, A. Cytogenetic aberrations in myelodysplastic syndrome detected by comparative genomic hybridization and fluorescence in situ hybridization. Diagn. Mol. Pathol. 1999, 8(1), 47-53.
[83] Wolfler, A.; Erkeland, S. J.; Bodner, C.; Valkhof, M.; Renner, W.; Leitner, C.; Olipitz, W.; Pfeilstocker, M.; Tinchon, C.; Emberger, W.; Linkesch, W.; Touw, I. P.; Sill, H. A functional single-nucleotide polymorphism of the G-CSF receptor gene predisposes individuals to high-risk myelodysplastic syndrome. Blood 2005, 105(9), 3731-3736.
[84] Willman, C. L. Molecular genetic features of myelodysplastic syndromes (MDS). Leukemia 1998, 12(Suppl. 1), S2-S6.
[85] Chen, H.; Sandler, D. P.; Taylor, J. A.; Shore, D. L.; Liu, E.; Bloomfield, C. D.; Bell, D. A. Increased risk for myelodysplastic syndromes in individuals with glutathione transferase theta 1 (GSTT1) gene defect. Lancet 1996, 347(8997), 295-297.
[86] Rothman, N.; Smith, M. T.; Hayes, R. B.; Traver, R. D.; Hoener, B.; Campleman, S.; Li, G. L.; Dosemeci, M.; Linet, M.; Zhang, L.; Xi, L.; Wacholder, S.; Lu, W.; Meyer, K. B.; Titenko-Holland, N.; Stewart, J. T.; Yin, S.; Ross, D. Benzene poisoning, a risk factor for hematological malignancy, is associated with the NQO1 609C-->T mutation and rapid fractional excretion of chlorzoxazone. Cancer Res. 1997, 57(14), 2839-2842.
[87] Naoe, T.; Takeyama, K.; Yokozawa, T.; Kiyoi, H.; Seto, M.; Uike, N.; Ino, T.; Utsunomiya, A.; Maruta, A.; Jin-nai, I.; Kamada, N.; Kubota, Y.; Nakamura, H.; Shimazaki, C.; Horiike, S.; Kodera, Y.; Saito, H.; Ueda, R.; Wiemels, J.; Ohno, R. Analysis of genetic polymorphism in NQO1, GST-M1, GST-T1, and CYP3A4 in 469 Japanese patients with therapy-related leukemia/ myelodysplastic syndrome and de novo acute myeloid leukemia. Clin. Cancer Res. 2000, 6(10), 4091-4095.
[88] Olipitz, W.; Hopfinger, G.; Aguiar, R. C.; Gunsilius, E.; Girschikofsky, M.; Bodner, C.; Hiden, K.; Linkesch, W.; Hoefler, G.; Sill, H. Defective DNA-mismatch repair: a potential mediator of leukemogenic susceptibility in therapy-related myelodysplasia and leukemia. Genes Chromosomes Cancer 2002, 34(2), 243-248.
[89] Robertson, K. D.; Jones, P. A. DNA methylation: past, present and future directions. Carcinogenesis 2000, 21(3), 461-467.
[90] Singal, R.; Ginder, G. D. DNA methylation. Blood 1999, 93(12), 4059-4070. [91] Herman, J. G.; Civin, C. I.; Issa, J. P.; Collector, M. I.; Sharkis, S. J.; Baylin,
S. B. Distinct patterns of inactivation of p15INK4B and p16INK4A characterize the major types of hematological malignancies. Cancer Res. 1997, 57(5), 837-841.
[92] Quesnel, B.; Guillerm, G.; Vereecque, R.; Wattel, E.; Preudhomme, C.; Bauters, F.; Vanrumbeke, M.; Fenaux, P. Methylation of the p15(INK4b) gene in myelodysplastic syndromes is frequent and acquired during disease progression. Blood 1998, 91(8), 2985-2990.
[93] Leone, G.; Teofili, L.; Voso, M. T.; Lubbert, M. DNA methylation and demethylating drugs in myelodysplastic syndromes and secondary leukemias. Haematologica 2002, 87(12), 1324-1341.
[94] Aggerholm, A.; Holm, M. S.; Guldberg, P.; Olesen, L. H.; Hokland, P. Promoter hypermethylation of p15INK4B, HIC1, CDH1, and ER is frequent in myelodysplastic syndrome and predicts poor prognosis in early-stage patients. Eur. J. Haematol. 2006, 76(1), 23-32.
[95] Christiansen, D. H.; Andersen, M. K.; Pedersen-Bjergaard, J. Methylation of p15INK4B is common, is associated with deletion of genes on chromosome arm 7q and predicts a poor prognosis in therapy-related myelodysplasia and acute myeloid leukemia. Leukemia 2003, 17(9), 1813-1819.

556 Current Cancer Drug Targets, 2007, Vol. 7, No. 6 Warlick and Smith [96] Dhodapkar, M.; Grill, J.; Lust, J. A. Abnormal regional hypermethylation of
the calcitonin gene in myelodysplastic syndromes. Leuk. Res. 1995, 19(10), 719-726.
[97] Wu, S.; Xie, G.; Bai, R.; Wang, Y.; Zhu, P. Semi-quantitative study of calcitonin gene methylation in myelodysplastic syndrome. Chin. Med. J. (Engl.) 1998, 111(8), 690-693.
[98] Bai, R.; Wu, S.; Zhu, P.; Xue, H.; Xu, Y.; Qin, X. Quantitative study of calcitonin gene methylation in myelodysplastic syndromes. Zhonghua Xue. Ye. Xue. Za Zhi. 1997, 18(1), 17-20.
[99] Li, G.; Zou, D.; Bai, R. Clinical significance of human calcitonin and gene-related peptide in the serum of myelodysplastic syndromes patients. Zhonghua Xue. Ye. Xue. Za Zhi. 1999, 20(2), 79-81.
[100] Marks, P.; Rifkind, R. A.; Richon, V. M.; Breslow, R.; Miller, T.; Kelly, W. K. Histone deacetylases and cancer: causes and therapies. Nat. Rev. Cancer 2001, 1(3), 194-202.
[101] Haggarty, S. J.; Koeller, K. M.; Wong, J. C.; Grozinger, C. M.; Schreiber, S. L. Domain-selective small-molecule inhibitor of histone deacetylase 6 (HDAC6)-mediated tubulin deacetylation. Proc. Natl. Acad. Sci. USA 2003, 100(8), 4389-4394.
[102] Wolf, D.; Rodova, M.; Miska, E. A.; Calvet, J. P.; Kouzarides, T. Acetylation of beta-catenin by CREB-binding protein (CBP). J. Biol. Chem. 2002, 277(28), 25562-25567.
[103] Bannister, A. J.; Miska, E. A.; Gorlich, D.; Kouzarides, T. Acetylation of importin-alpha nuclear import factors by CBP/p300. Curr. Biol. 2000, 10(8), 467-470.
[104] Cohen, H. Y.; Lavu, S.; Bitterman, K. J.; Hekking, B.; Imahiyerobo, T. A.; Miller, C.; Frye, R.; Ploegh, H.; Kessler, B. M.; Sinclair, D. A. Acetylation of the C terminus of Ku70 by CBP and PCAF controls Bax-mediated apoptosis. Mol. Cell 2004, 13(5), 627-638.
[105] Fuino, L.; Bali, P.; Wittmann, S.; Donapaty, S.; Guo, F.; Yamaguchi, H.; Wang, H. G.; Atadja, P.; Bhalla, K. Histone deacetylase inhibitor LAQ824 down-regulates Her-2 and sensitizes human breast cancer cells to trastuzumab, taxotere, gemcitabine, and epothilone B. Mol. Cancer Ther. 2003, 2(10), 971-984.
[106] Morgan, M. A.; Reuter, C. W. Molecularly targeted therapies in myelodysplastic syndromes and acute myeloid leukemias. Ann. Hematol. 2006, 85(3), 139-163.
[107] Johnstone, R. W.; Licht, J. D. Histone deacetylase inhibitors in cancer therapy: is transcription the primary target? Cancer Cell 2003, 4(1), 13-18.
[108] Kitagawa, M.; Saito, I.; Kuwata, T.; Yoshida, S.; Yamaguchi, S.; Takahashi, M.; Tanizawa, T.; Kamiyama, R.; Hirokawa, K. Overexpression of tumor necrosis factor (TNF)-alpha and interferon (IFN)-gamma by bone marrow cells from patients with myelodysplastic syndromes. Leukemia 1997, 11(12), 2049-2054.
[109] Stifter, G.; Heiss, S.; Gastl, G.; Tzankov, A.; Stauder, R. Over-expression of tumor necrosis factor-alpha in bone marrow biopsies from patients with myelodysplastic syndromes: relationship to anemia and prognosis. Eur. J. Haematol. 2005, 75(6), 485-491.
[110] Shetty, V.; Mundle, S.; Alvi, S.; Showel, M.; Broady-Robinson, L.; Dar, S.; Borok, R.; Showel, J.; Gregory, S.; Rifkin, S.; Gezer, S.; Parcharidou, A.; Venugopal, P.; Shah, R.; Hernandez, B.; Klein, M.; Alston, D.; Robin, E.; Dominquez, C.; Raza, A. Measurement of apoptosis, proliferation and three cytokines in 46 patients with myelodysplastic syndromes. Leuk. Res. 1996, 20(11-12), 891-900.
[111] Raza, A.; Mundle, S.; Shetty, V.; Alvi, S.; Chopra, H.; Span, L.; Parcharidou, A.; Dar, S.; Venugopal, P.; Borok, R.; Gezer, S.; Showel, J.; Loew, J.; Robin, E.; Rifkin, S.; Alston, D.; Hernandez, B.; Shah, R.; Kaizer, H.; Gregory, S. Novel insights into the biology of myelodysplastic syndromes: excessive apoptosis and the role of cytokines. Int. J. Hematol. 1996, 63(4), 265-278.
[112] Hsu, H.; Xiong, J.; Goeddel, D. V. The TNF receptor 1-associated protein TRADD signals cell death and NF-kappa B activation. Cell 1995, 81(4), 495-504.
[113] Hsu, H.; Huang, J.; Shu, H. B.; Baichwal, V.; Goeddel, D. V. TNF-dependent recruitment of the protein kinase RIP to the TNF receptor-1 signaling complex. Immunity 1996, 4(4), 387-396.
[114] Flores-Figueroa, E.; Gutierrez-Espindola, G.; Montesinos, J. J.; Arana-Trejo, R. M.; Mayani, H. In vitro characterization of hematopoietic microenvironment cells from patients with myelodysplastic syndrome. Leuk. Res. 2002, 26(7), 677-686.
[115] Wetzler, M.; Kurzrock, R.; Estrov, Z.; Estey, E.; Talpaz, M. Cytokine expression in adherent layers from patients with myelodysplastic syndrome and acute myelogenous leukemia. Leuk. Res. 1995, 19(1), 23-34.
[116] Deeg, H. J.; Beckham, C.; Loken, M. R.; Bryant, E.; Lesnikova, M.; Shulman, H. M.; Gooley, T. Negative regulators of hemopoiesis and stroma function in patients with myelodysplastic syndrome. Leuk. Lymphoma 2000, 37(3-4), 405-414.
[117] Koike, M.; Ishiyama, T.; Tomoyasu, S.; Tsuruoka, N. Spontaneous cytokine overproduction by peripheral blood mononuclear cells from patients with myelodysplastic syndromes and aplastic anemia. Leuk. Res. 1995, 19(9), 639-644.
[118] Bouscary, D.; De Vos, J.; Guesnu, M.; Jondeau, K.; Viguier, F.; Melle, J.; Picard, F.; Dreyfus, F.; Fontenay-Roupie, M. Fas/Apo-1 (CD95) expression and apoptosis in patients with myelodysplastic syndromes. Leukemia 1997, 11(6), 839-845.
[119] Gersuk, G. M.; Lee, J. W.; Beckham, C. A.; Anderson, J.; Deeg, H. J. Fas (CD95) receptor and Fas-ligand expression in bone marrow cells from patients with myelodysplastic syndrome. Blood 1996, 88(3), 1122-1123.
[120] Estey, E. H. Modulation of angiogenesis in patients with myelodysplastic syndrome. Best. Pract. Res. Clin. Haematol. 2004, 17(4), 623-639.
[121] Aguayo, A.; Kantarjian, H.; Manshouri, T.; Gidel, C.; Estey, E.; Thomas, D.; Koller, C.; Estrov, Z.; O'Brien, S.; Keating, M.; Freireich, E.; Albitar, M. Angiogenesis in acute and chronic leukemias and myelodysplastic syndromes. Blood 2000, 96(6), 2240-2245.
[122] Zorat, F.; Shetty, V.; Dutt, D.; Lisak, L.; Nascimben, F.; Allampallam, K.; Dar, S.; York, A.; Gezer, S.; Venugopal, P.; Raza, A. The clinical and biological effects of thalidomide in patients with myelodysplastic syndromes. Br. J. Haematol. 2001, 115(4), 881-894.
[123] Brunner, B.; Gunsilius, E.; Schumacher, P.; Zwierzina, H.; Gastl, G.; Stauder, R. Blood levels of angiogenin and vascular endothelial growth factor are elevated in myelodysplastic syndromes and in acute myeloid leukemia. J. Hematother. Stem Cell Res. 2002, 11(1), 119-125.
[124] Wimazal, F.; Krauth, M. T.; Vales, A.; Bohm, A.; Agis, H.; Sonneck, K.; Aichberger, K. J.; Mayerhofer, M.; Simonitsch-Klupp, I.; Mullauer, L.; Sperr, W. R.; Valent, P. Immunohistochemical detection of vascular endothelial growth factor (VEGF) in the bone marrow in patients with myelodysplastic syndromes: correlation between VEGF expression and the FAB category. Leuk. Lymphoma 2006, 47(3), 451-460.
[125] Pruneri, G.; Bertolini, F.; Soligo, D.; Carboni, N.; Cortelezzi, A.; Ferrucci, P. F.; Buffa, R.; Lambertenghi-Deliliers, G.; Pezzella, F. Angiogenesis in myelodysplastic syndromes. Br. J. Cancer 1999, 81(8), 1398-1401.
[126] Korkolopoulou, P.; Apostolidou, E.; Pavlopoulos, P. M.; Kavantzas, N.; Vyniou, N.; Thymara, I.; Terpos, E.; Patsouris, E.; Yataganas, X.; Davaris, P. Prognostic evaluation of the microvascular network in myelodysplastic syndromes. Leukemia 2001, 15(9), 1369-1376.
[127] Epperson, D. E.; Nakamura, R.; Saunthararajah, Y.; Melenhorst, J.; Barrett, A. J. Oligoclonal T cell expansion in myelodysplastic syndrome: evidence for an autoimmune process. Leuk. Res. 2001, 25(12), 1075-1083.
[128] Smith, M. A.; Smith, J. G. The occurrence subtype and significance of haemopoietic inhibitory T cells (HIT cells) in myelodysplasia: an in vitro study. Leuk. Res. 1991, 15(7), 597-601.
[129] Molldrem, J. J.; Caples, M.; Mavroudis, D.; Plante, M.; Young, N. S.; Barrett, A. J. Antithymocyte globulin for patients with myelodysplastic syndrome. Br. J. Haematol. 1997, 99(3), 699-705.
[130] Jonasova, A.; Neuwirtova, R.; Cermak, J.; Vozobulova, V.; Mocikova, K.; Siskova, M.; Hochova, I. Cyclosporin A therapy in hypoplastic MDS patients and certain refractory anaemias without hypoplastic bone marrow. Br. J. Haematol. 1998, 100(2), 304-309.
[131] Molldrem, J. J.; Jiang, Y. Z.; Stetler-Stevenson, M.; Mavroudis, D.; Hensel, N.; Barrett, A. J. Haematological response of patients with myelodysplastic syndrome to antithymocyte globulin is associated with a loss of lymphocyte-mediated inhibition of CFU-GM and alterations in T-cell receptor Vbeta profiles. Br. J. Haematol. 1998, 102(5), 1314-1322.
[132] Melenhorst, J. J.; Eniafe, R.; Follmann, D.; Nakamura, R.; Kirby, M.; Barrett, A. J. Molecular and flow cytometric characterization of the CD4 and CD8 T-cell repertoire in patients with myelodysplastic syndrome. Br. J. Haematol. 2002, 119(1), 97-105.
[133] Voulgarelis, M.; Giannouli, S.; Ritis, K.; Tzioufas, A. G. Myelodysplasia-associated autoimmunity: clinical and pathophysiologic concepts. Eur. J. Clin. Invest. 2004, 34(10), 690-700.
[134] Marisavljevic, D.; Kraguljac, N.; Rolovic, Z. Immunologic abnormalities in myelodysplastic syndromes: clinical features and characteristics of the lymphoid population. Med. Oncol. 2006, 23(3), 385-392.
[135] Billstrom, R.; Johansson, H.; Johansson, B.; Mitelman, F. Immune-mediated complications in patients with myelodysplastic syndromes--clinical and cytogenetic features. Eur. J. Haematol. 1995, 55(1), 42-48.
[136] Saitoh, K.; Miura, I.; Takahashi, N.; Miura, A. B. Fluorescence in situ hybridization of progenitor cells obtained by fluorescence-activated cell sorting for the detection of cells affected by chromosome abnormality trisomy 8 in patients with myelodysplastic syndromes. Blood 1998, 92(8), 2886-2892.
[137] White, N. J.; Nacheva, E.; Asimakopoulos, F. A.; Bloxham, D.; Paul, B.; Green, A. R. Deletion of chromosome 20q in myelodysplasia can occur in a multipotent precursor of both myeloid cells and B cells. Blood 1994, 83(10), 2809-2816.
[138] Nilsson, L.; Astrand-Grundstrom, I.; Arvidsson, I.; Jacobsson, B.; Hellstrom-Lindberg, E.; Hast, R.; Jacobsen, S. E. Isolation and characterization of hematopoietic progenitor/stem cells in 5q-deleted myelodysplastic syndromes: evidence for involvement at the hematopoietic stem cell level. Blood 2000, 96(6), 2012-2021.
[139] Nilsson, L.; Astrand-Grundstrom, I.; Anderson, K.; Arvidsson, I.; Hokland, P.; Bryder, D.; Kjeldsen, L.; Johansson, B.; Hellstrom-Lindberg, E.; Hast, R.; Jacobsen, S. E. Involvement and functional impairment of the CD34(+)CD38(-)Thy-1(+) hematopoietic stem cell pool in myelodysplastic syndromes with trisomy 8. Blood 2002, 100(1), 259-267.
[140] Furukawa, Y. Cell cycle control during hematopoietic cell differentiation. Hum. Cell 1997, 10(3), 159-164.
[141] Furukawa, Y.; Kikuchi, J.; Nakamura, M.; Iwase, S.; Yamada, H.; Matsuda, M. Lineage-specific regulation of cell cycle control gene expression during haematopoietic cell differentiation. Br. J. Haematol. 2000, 110(3), 663-673.

Myelodysplastic Syndromes Current Cancer Drug Targets, 2007, Vol. 7, No. 6 557 [142] Shimizu, R.; Kuroha, T.; Ohneda, O.; Pan, X.; Ohneda, K.; Takahashi, S.;
Philipsen, S.; Yamamoto, M. Leukemogenesis caused by incapacitated GATA-1 function. Mol. Cell Biol. 2004, 24(24), 10814-10825.
[143] Dubart, A.; Romeo, P. H.; Vainchenker, W.; Dumenil, D. Constitutive expression of GATA-1 interferes with the cell-cycle regulation. Blood 1996, 87(9), 3711-3721.
[144] Weiss, M. J.; Orkin, S. H. Transcription factor GATA-1 permits survival and maturation of erythroid precursors by preventing apoptosis. Proc. Natl. Acad. Sci. USA 1995, 92(21), 9623-9627.
[145] Briegel, K.; Lim, K. C.; Plank, C.; Beug, H.; Engel, J. D.; Zenke, M. Ectopic expression of a conditional GATA-2/estrogen receptor chimera arrests erythroid differentiation in a hormone-dependent manner. Genes Dev. 1993, 7(6), 1097-1109.
[146] McDevitt, M. A.; Shivdasani, R. A.; Fujiwara, Y.; Yang, H.; Orkin, S. H. A "knockdown" mutation created by cis-element gene targeting reveals the dependence of erythroid cell maturation on the level of transcription factor GATA-1. Proc. Natl. Acad. Sci. USA 1997, 94(13), 6781-6785.
[147] Fadilah, S. A.; Cheong, S. K.; Roslan, H.; Rozie-Hanisa, M.; Yen, G. K. GATA-1 and GATA-2 gene expression is related to the severity of dysplasia in myelodysplastic syndrome. Leukemia 2002, 16(8), 1563-1565.
[148] Cheson, B. D.; Greenberg, P. L.; Bennett, J. M.; Lowenberg, B.; Wijermans, P. W.; Nimer, S. D.; Pinto, A.; Beran, M.; de Witte, T. M.; Stone, R. M.; Mittelman, M.; Sanz, G. F.; Gore, S. D.; Schiffer, C. A.; Kantarjian, H. Clinical application and proposal for modification of the International Working Group (IWG) response criteria in myelodysplasia. Blood 2006, 108(2), 419-425.
[149] Hellstrom-Lindberg, E. Efficacy of erythropoietin in the myelodysplastic syndromes: a meta-analysis of 205 patients from 17 studies. Br. J. Haematol. 1995, 89(1), 67-71.
[150] Stein, R. S. The role of erythropoietin in the anemia of myelodysplastic syndrome. Clin. Lymphoma 2003, 4(Suppl. 1), S36-S40.
[151] Hellstrom-Lindberg, E.; Negrin, R.; Stein, R.; Krantz, S.; Lindberg, G.; Vardiman, J.; Ost, A.; Greenberg, P. Erythroid response to treatment with G-CSF plus erythropoietin for the anaemia of patients with myelodysplastic syndromes: proposal for a predictive model. Br. J. Haematol. 1997, 99(2), 344-351.
[152] Remacha, A. F.; Arrizabalaga, B.; Villegas, A.; Manteiga, R.; Calvo, T.; Julia, A.; Fernandez, F., I; Gonzalez, F. A.; Font, L.; Junca, J.; del Arco, A.; Malcorra, J. J.; Equiza, E. P.; de Mendiguren, B. P.; Romero, M. Erythropoietin plus granulocyte colony-stimulating factor in the treatment of myelodysplastic syndromes. Identification of a subgroup of responders. The Spanish Erythropathology Group. Haematologica 1999, 84(12), 1058-1064.
[153] Negrin, R. S.; Stein, R.; Doherty, K.; Cornwell, J.; Vardiman, J.; Krantz, S.; Greenberg, P. L. Maintenance treatment of the anemia of myelodysplastic syndromes with recombinant human granulocyte colony-stimulating factor and erythropoietin: evidence for in vivo synergy. Blood 1996, 87(10), 4076-4081.
[154] Kasper, C.; Zahner, J.; Sayer, H. G. Recombinant human erythropoietin in combined treatment with granulocyte- or granulocyte-macrophage colony-stimulating factor in patients with myelodysplastic syndromes. J. Cancer Res. Clin. Oncol. 2002, 128(9), 497-502.
[155] Terpos, E.; Mougiou, A.; Kouraklis, A.; Chatzivassili, A.; Michalis, E.; Giannakoulas, N.; Manioudaki, E.; Lazaridou, A.; Bakaloudi, V.; Protopappa, M.; Liapi, D.; Grouzi, E.; Parharidou, A.; Symeonidis, A.; Kokkini, G.; Laoutaris, N. P.; Vaipoulos, G.; Anagnostopoulos, N. I.; Christakis, J. I.; Meletis, J.; Bourantas, K. L.; Zoumbos, N. C.; Yataganas, X.; Viniou, N. A. Prolonged administration of erythropoietin increases erythroid response rate in myelodysplastic syndromes: a phase II trial in 281 patients. Br. J. Haematol. 2002, 118(1), 174-180.
[156] Patton, J. F.; Sullivan, T.; Mun, Y.; Reeves, T.; Rossi, G.; Wallace, J. F. A retrospective cohort study to assess the impact of therapeutic substitution of darbepoetin alfa for epoetin alfa in anemic patients with myelodysplastic syndrome. J. Support. Oncol. 2005, 3(6), 419-426.
[157] Mannone, L.; Gardin, C.; Quarre, M. C.; Bernard, J. F.; Vassilieff, D.; Ades, L.; Park, S.; Vaultier, S.; Hamza, F.; Beyne-rauzy, M. O.; Cheze, S.; Giraudier, S.; Agape, P.; Legros, L.; Voillat, L.; Dreyfus, F.; Fenaux, P. High-dose darbepoetin alpha in the treatment of anaemia of lower risk myelodysplastic syndrome results of a phase II study. Br. J. Haematol. 2006, 133(5), 513-519.
[158] Sierra, J.; Perez, W. S.; Rozman, C.; Carreras, E.; Klein, J. P.; Rizzo, J. D.; Davies, S. M.; Lazarus, H. M.; Bredeson, C. N.; Marks, D. I.; Canals, C.; Boogaerts, M. A.; Goldman, J.; Champlin, R. E.; Keating, A.; Weisdorf, D. J.; de Witte, T. M.; Horowitz, M. M. Bone marrow transplantation from HLA-identical siblings as treatment for myelodysplasia. Blood 2002, 100(6), 1997-2004.
[159] Kuendgen, A.; Strupp, C.; Aivado, M.; Hildebrandt, B.; Haas, R.; Gattermann, N.; Germing, U. Myelodysplastic syndromes in patients younger than age 50. J. Clin. Oncol. 2006, 24(34), 5358-5365.
[160] Cutler, C. S.; Lee, S. J.; Greenberg, P.; Deeg, H. J.; Perez, W. S.; Anasetti, C.; Bolwell, B. J.; Cairo, M. S.; Gale, R. P.; Klein, J. P.; Lazarus, H. M.; Liesveld, J. L.; McCarthy, P. L.; Milone, G. A.; Rizzo, J. D.; Schultz, K. R.; Trigg, M. E.; Keating, A.; Weisdorf, D. J.; Antin, J. H.; Horowitz, M. M. A decision analysis of allogeneic bone marrow transplantation for the myelodysplastic syndromes: delayed transplantation for low-risk myelodysplasia is associated with improved outcome. Blood 2004, 104(2), 579-585.
[161] Martino, R.; Iacobelli, S.; Brand, R.; Jansen, T.; van Biezen, A.; Finke, J.; Bacigalupo, A.; Beelen, D.; Reiffers, J.; Devergie, A.; Alessandrino, E.; Mufti, G. J.; Barge, R.; Sierra, J.; Ruutu, T.; Boogaerts, M.; Falda, M.; Jouet, J. P.; Niederwieser, D.; De Witte, T. Retrospective comparison of reduced intensity conditioning and conventional high dose conditioning for allogeneic hematopoietic stem cell transplantation using HLA identical sibling donors in myelodysplastic syndromes. Blood 2006, 108(3), 836-846.
[162] de Lima, M.; Anagnostopoulos, A.; Munsell, M.; Shahjahan, M.; Ueno, N.; Ippoliti, C.; Andersson, B. S.; Gajewski, J.; Couriel, D.; Cortes, J.; Donato, M.; Neumann, J.; Champlin, R.; Giralt, S. Nonablative versus reduced-intensity conditioning regimens in the treatment of acute myeloid leukemia and high-risk myelodysplastic syndrome: dose is relevant for long-term disease control after allogeneic hematopoietic stem cell transplantation. Blood 2004, 104(3), 865-872.
[163] Scott, B. L.; Sandmaier, B. M.; Storer, B.; Maris, M. B.; Sorror, M. L.; Maloney, D. G.; Chauncey, T. R.; Storb, R.; Deeg, H. J. Myeloablative vs nonmyeloablative allogeneic transplantation for patients with myelodysplastic syndrome or acute myelogenous leukemia with multilineage dysplasia: a retrospective analysis. Leukemia 2006, 20(1), 128-135.
[164] Shimoni, A.; Hardan, I.; Shem-Tov, N.; Yeshurun, M.; Yerushalmi, R.; Avigdor, A.; Ben Bassat, I.; Nagler, A. Allogeneic hematopoietic stem-cell transplantation in AML and MDS using myeloablative versus reduced-intensity conditioning: the role of dose intensity. Leukemia 2006, 20(2), 322-328.
[165] Alyea, E. P.; Kim, H. T.; Ho, V.; Cutler, C.; Deangelo, D. J.; Stone, R.; Ritz, J.; Antin, J. H.; Soiffer, R. J. Impact of Conditioning Regimen Intensity on Outcome of Allogeneic Hematopoietic Cell Transplantation for Advanced Acute Myelogenous Leukemia and Myelodysplastic Syndrome. Biol. Blood Marrow Transplant. 2006, 12(10), 1047-1055.
[166] Mattijssen, V.; Schattenberg, A.; Schaap, N.; Preijers, F.; De Witte, T. Outcome of allogeneic bone marrow transplantation with lymphocyte-depleted marrow grafts in adult patients with myelodysplastic syndromes. Bone Marrow Transplant. 1997, 19(8), 791-794.
[167] Ooi, J. The efficacy of unrelated cord blood transplantation for adult myelodysplastic syndrome. Leuk. Lymphoma 2006, 47(4), 599-602.
[168] Lu, D. P.; Dong, L.; Wu, T.; Huang, X. J.; Zhang, M. J.; Han, W.; Chen, H.; Liu, D. H.; Gao, Z. Y.; Chen, Y. H.; Xu, L. P.; Zhang, Y. C.; Ren, H. Y.; Li, D.; Liu, K. Y. Conditioning including antithymocyte globulin followed by unmanipulated HLA-mismatched/haploidentical blood and marrow transplantation can achieve comparable outcomes with HLA-identical sibling transplantation. Blood 2006, 107(8), 3065-3073.
[169] Kizaki, M.; Koeffler, H. P. Differentiation-inducing agents in the treatment of myelodysplastic syndromes. Semin. Oncol. 1992, 19(1), 95-105.
[170] Silverman, L. R.; Demakos, E. P.; Peterson, B. L.; Kornblith, A. B.; Holland, J. C.; Odchimar-Reissig, R.; Stone, R. M.; Nelson, D.; Powell, B. L.; DeCastro, C. M.; Ellerton, J.; Larson, R. A.; Schiffer, C. A.; Holland, J. F. Randomized controlled trial of azacitidine in patients with the myelodysplastic syndrome: a study of the cancer and leukemia group B. J. Clin. Oncol. 2002, 20(10), 2429-2440.
[171] Silverman, L. R.; McKenzie, D. R.; Peterson, B. L.; Holland, J. F.; Backstrom, J. T.; Beach, C. L.; Larson, R. A. Further analysis of trials with azacitidine in patients with myelodysplastic syndrome: studies 8421, 8921, and 9221 by the Cancer and Leukemia Group B. J. Clin. Oncol. 2006, 24(24), 3895-3903.
[172] Zagonel, V.; Lo, R. G.; Marotta, G.; Babare, R.; Sardeo, G.; Gattei, V.; De, A. V.; Monfardini, S.; Pinto, A. 5-Aza-2'-deoxycytidine (Decitabine) induces trilineage response in unfavourable myelodysplastic syndromes. Leukemia 1993, 7(Suppl. 1), 30-35.
[173] Wijermans, P. W.; Krulder, J. W.; Huijgens, P. C.; Neve, P. Continuous infusion of low-dose 5-Aza-2'-deoxycytidine in elderly patients with high-risk myelodysplastic syndrome. Leukemia 1997, 11(Suppl. 1), S19-S23.
[174] Kantarjian, H.; Issa, J. P.; Rosenfeld, C. S.; Bennett, J. M.; Albitar, M.; DiPersio, J.; Klimek, V.; Slack, J.; de Castro, C.; Ravandi, F.; Helmer, R., III; Shen, L.; Nimer, S. D.; Leavitt, R.; Raza, A.; Saba, H. Decitabine improves patient outcomes in myelodysplastic syndromes: results of a phase III randomized study. Cancer 2006, 106(8), 1794-1803.
[175] Kantarjian, H.; Oki, Y.; Garcia-Manero, G.; Huang, X.; O'Brien, S.; Cortes, J.; Faderl, S.; Bueso-Ramos, C.; Ravandi, F.; Estrov, Z.; Ferrajoli, A.; Wierda, W.; Shan, J.; Davis, J.; Giles, F.; Saba, H. I.; Issa, J. P. Results of a randomized study of 3 schedules of low-dose decitabine in higher-risk myelodysplastic syndrome and chronic myelomonocytic leukemia. Blood 2007, 109(1), 52-57.
[176] Schreiber, S. L.; Bernstein, B. E. Signaling network model of chromatin. Cell 2002, 111(6), 771-778.
[177] Dokmanovic, M.; Marks, P. A. Prospects: histone deacetylase inhibitors. J. Cell Biochem. 2005, 96(2), 293-304.
[178] Kuendgen, A.; Strupp, C.; Aivado, M.; Bernhardt, A.; Hildebrandt, B.; Haas, R.; Germing, U.; Gattermann, N. Treatment of myelodysplastic syndromes with valproic acid alone or in combination with all-trans retinoic acid. Blood 2004, 104(5), 1266-1269.
[179] Kuendgen, A.; Knipp, S.; Fox, F.; Strupp, C.; Hildebrandt, B.; Steidl, C.; Germing, U.; Haas, R.; Gattermann, N. Results of a phase 2 study of valproic acid alone or in combination with all-trans retinoic acid in 75 patients with myelodysplastic syndrome and relapsed or refractory acute myeloid leukemia. Ann. Hematol. 2005, 84(Suppl. 13), 61-66.

558 Current Cancer Drug Targets, 2007, Vol. 7, No. 6 Warlick and Smith [180] Saunthararajah, Y.; Nakamura, R.; Nam, J. M.; Robyn, J.; Loberiza, F.;
Maciejewski, J. P.; Simonis, T.; Molldrem, J.; Young, N. S.; Barrett, A. J. HLA-DR15 (DR2) is overrepresented in myelodysplastic syndrome and aplastic anemia and predicts a response to immunosuppression in myelodysplastic syndrome. Blood 2002, 100(5), 1570-1574.
[181] Candoni, A.; Silvestri, F.; Buonamici, S.; Li, D.; Reddy, P.; Galili, N.; Nucifora, G.; Raza, A. Targeted therapies in myelodysplastic syndromes: ASH 2003 review. Semin. Hematol. 2004, 41(2 Suppl. 4), 13-20.
[182] Galili, N.; Raza, A. Immunomodulatory drugs in myelodysplastic syndromes. Expert Opin. Investig. Drugs 2006, 15(7), 805-813.
[183] Tamilarasan, K. P.; Kolluru, G. K.; Rajaram, M.; Indhumathy, M.; Saranya, R.; Chatterjee, S. Thalidomide attenuates nitric oxide mediated angiogenesis by blocking migration of endothelial cells. BMC Cell Biol. 2006, 7, 17-29.
[184] Geitz, H.; Handt, S.; Zwingenberger, K. Thalidomide selectively modulates the density of cell surface molecules involved in the adhesion cascade. Immunopharmacology 1996, 31(2-3), 213-221.
[185] D'Amato, R. J.; Loughnan, M. S.; Flynn, E.; Folkman, J. Thalidomide is an inhibitor of angiogenesis. Proc. Natl. Acad. Sci. USA 1994, 91(9), 4082-4085.
[186] Mitsiades, N.; Mitsiades, C. S.; Poulaki, V.; Chauhan, D.; Richardson, P. G.; Hideshima, T.; Munshi, N. C.; Treon, S. P.; Anderson, K. C. Apoptotic signaling induced by immunomodulatory thalidomide analogs in human multiple myeloma cells: therapeutic implications. Blood 2002, 99(12), 4525-4530.
[187] Mitsuyasu, R. T.; Champlin, R. E.; Gale, R. P.; Ho, W. G.; Lenarsky, C.; Winston, D.; Selch, M.; Elashoff, R.; Giorgi, J. V.; Wells, J. Treatment of donor bone marrow with monoclonal anti-T-cell antibody and complement for the prevention of graft-versus-host disease. A prospective, randomized, double-blind trial. Ann. Intern. Med. 1986, 105(1), 20-26.
[188] Raza, A.; Meyer, P.; Dutt, D.; Zorat, F.; Lisak, L.; Nascimben, F.; du, R. M.; Kaspar, C.; Goldberg, C.; Loew, J.; Dar, S.; Gezer, S.; Venugopal, P.; Zeldis, J. Thalidomide produces transfusion independence in long-standing refractory anemias of patients with myelodysplastic syndromes. Blood 2001, 98(4), 958-965.
[189] Strupp, C.; Germing, U.; Aivado, M.; Misgeld, E.; Haas, R.; Gattermann, N. Thalidomide for the treatment of patients with myelodysplastic syndromes. Leukemia 2002, 16(1), 1-6.
[190] Musto, P.; Falcone, A.; Sanpaolo, G.; Bisceglia, M.; Matera, R.; Carella, A. M. Thalidomide abolishes transfusion-dependence in selected patients with myelodysplastic syndromes. Haematologica 2002, 87(8), 884-886.
[191] Bowen, D.; MacIlwaine, L.; Cavanagh, J.; Killick, S.; Culligan, D.; Thomson, E.; Mufti, G. Thalidomide therapy for low-risk Myelodysplasia. Leuk. Res. 2005, 29(2), 235-236.
[192] Bouscary, D.; Legros, L.; Tulliez, M.; Dubois, S.; Mahe, B.; Beyne-Rauzy, O.; Quarre, M. C.; Vassilief, D.; Varet, B.; Aouba, A.; Gardembas, M.; Giraudier, S.; Guerci, A.; Rousselot, P.; Gaillard, F.; Moreau, A.; Rousselet, M. C.; Ifrah, N.; Fenaux, P.; Dreyfus, F. A non-randomised dose-escalating phase II study of thalidomide for the treatment of patients with low-risk myelodysplastic syndromes: the Thal-SMD-2000 trial of the Groupe Francais des Myelodysplasies. Br. J. Haematol. 2005, 131(5), 609-618.
[193] Corral, L. G.; Haslett, P. A.; Muller, G. W.; Chen, R.; Wong, L. M.; Ocampo, C. J.; Patterson, R. T.; Stirling, D. I.; Kaplan, G. Differential cytokine modulation and T cell activation by two distinct classes of thalidomide analogues that are potent inhibitors of TNF-alpha. J. Immunol. 1999, 163(1), 380-386.
[194] Davies, F. E.; Raje, N.; Hideshima, T.; Lentzsch, S.; Young, G.; Tai, Y. T.; Lin, B.; Podar, K.; Gupta, D.; Chauhan, D.; Treon, S. P.; Richardson, P. G.; Schlossman, R. L.; Morgan, G. J.; Muller, G. W.; Stirling, D. I.; Anderson, K. C. Thalidomide and immunomodulatory derivatives augment natural killer cell cytotoxicity in multiple myeloma. Blood 2001, 98(1), 210-216.
[195] Maier, S. K.; Hammond, J. M. Role of lenalidomide in the treatment of multiple myeloma and myelodysplastic syndrome. Ann. Pharmacother. 2006, 40(2), 286-289.
[196] List, A.; Kurtin, S.; Roe, D. J.; Buresh, A.; Mahadevan, D.; Fuchs, D.; Rimsza, L.; Heaton, R.; Knight, R.; Zeldis, J. B. Efficacy of lenalidomide in myelodysplastic syndromes. N. Engl. J. Med. 2005, 352(6), 549-557.
[197] Sekeres, M. A.; List, A. Immunomodulation in myelodysplastic syndromes. Best. Pract. Res. Clin. Haematol. 2006, 19(4), 757-767.
[198] Hellstrom-Lindberg, E.; Ahlgren, T.; Beguin, Y.; Carlsson, M.; Carneskog, J.; Dahl, I. M.; Dybedal, I.; Grimfors, G.; Kanter-Lewensohn, L.; Linder, O.; Luthman, M.; Lofvenberg, E.; Nilsson-Ehle, H.; Samuelsson, J.; Tangen, J. M.; Winqvist, I.; Oberg, G.; Osterborg, A.; Ost, A. Treatment of anemia in myelodysplastic syndromes with granulocyte colony-stimulating factor plus erythropoietin: results from a randomized phase II study and long-term follow-up of 71 patients. Blood 1998, 92(1), 68-75.
[199] Meletis, J.; Viniou, N.; Terpos, E. Novel agents for the management of myelodysplastic syndromes. Med. Sci. Monit. 2006, 12(9), RA194-RA206.
[200] Gore, S. D.; Baylin, S.; Sugar, E.; Carraway, H.; Miller, C. B.; Carducci, M.; Grever, M.; Galm, O.; Dauses, T.; Karp, J. E.; Rudek, M. A.; Zhao, M.; Smith, B. D.; Manning, J.; Jiemjit, A.; Dover, G.; Mays, A.; Zwiebel, J.; Murgo, A.; Weng, L. J.; Herman, J. G. Combined DNA methyltransferase and histone deacetylase inhibition in the treatment of myeloid neoplasms. Cancer Res. 2006, 66(12), 6361-6369.
[201] Maslak, P.; Chanel, S.; Camacho, L. H.; Soignet, S.; Pandolfi, P. P.; Guernah, I.; Warrell, R.; Nimer, S. Pilot study of combination transcriptional modulation therapy with sodium phenylbutyrate and 5-azacitidine in patients with acute myeloid leukemia or myelodysplastic syndrome. Leukemia 2006, 20(2), 212-217.
[202] Oka, Y.; Tsuboi, A.; Taguchi, T.; Osaki, T.; Kyo, T.; Nakajima, H.; Elisseeva, O. A.; Oji, Y.; Kawakami, M.; Ikegame, K.; Hosen, N.; Yoshihara, S.; Wu, F.; Fujiki, F.; Murakami, M.; Masuda, T.; Nishida, S.; Shirakata, T.; Nakatsuka, S.; Sasaki, A.; Udaka, K.; Dohy, H.; Aozasa, K.; Noguchi, S.; Kawase, I.; Sugiyama, H. Induction of WT1 (Wilms' tumor gene)-specific cytotoxic T lymphocytes by WT1 peptide vaccine and the resultant cancer regression. Proc. Natl. Acad. Sci. USA 2004, 101(38), 13885-13890.
[203] Tallman, M. S.; Andersen, J. W.; Schiffer, C. A.; Appelbaum, F. R.; Feusner, J. H.; Ogden, A.; Shepherd, L.; Willman, C.; Bloomfield, C. D.; Rowe, J. M.; Wiernik, P. H. All-trans-retinoic acid in acute promyelocytic leukemia. N. Engl. J. Med. 1997, 337(15), 1021-1028.
[204] Santini, V.; Ferrini, P. R. Differentiation therapy of myelodysplastic syndromes: fact or fiction? Br. J. Haematol. 1998, 102(5), 1124-1138.
[205] Nand, S.; Ellis, T.; Messmore, H.; Fisher, S. G.; Gaynor, E.; Fisher, R. I. Phase II trial of recombinant human interferon alpha in myelodysplastic syndromes. Leukemia 1992, 6(3), 220-223.
[206] Maerevoet, M.; Van Den, N. E.; Delannoy, A.; Ferrant, A.; Martiat, P.; Bosly, A.; Fauchet, M.; Michaux, J. L. Limited activity of mini-dose interferon alpha-2a in the treatment of myelodysplastic syndrome. Leuk. Lymphoma 1996, 21(5-6), 519-520.
[207] Holcombe, R. F. Mini-dose interferon alpha-2a in the treatment of myelodysplasia. Leukemia 1993, 7(2), 192-195.
[208] Elias, L.; Hoffman, R.; Boswell, S.; Tensen, L.; Bonnem, E. M. A trial of recombinant alpha 2 interferon in the myelodysplastic syndromes: I. Clinical results. Leukemia 1987, 1(2), 105-110.
[209] Gisslinger, H.; Chott, A.; Linkesch, W.; Fritz, E.; Ludwig, H. Long-term alpha-interferon therapy in myelodysplastic syndromes. Leukemia 1990, 4(2), 91-94.
[210] Motomura, S.; Kanamori, H.; Maruta, A.; Kodama, F.; Ohkubo, T. The effect of 1-hydroxyvitamin D3 for prolongation of leukemic transformation-free survival in myelodysplastic syndromes. Am. J. Hematol. 1991, 38(1), 67-68.
[211] Koeffler, H. P.; Aslanian, N.; O'Kelly, J. Vitamin D(2) analog (Paricalcitol; Zemplar) for treatment of myelodysplastic syndrome. Leuk. Res. 2005, 29(11), 1259-1262.
[212] Mellibovsky, L.; Diez, A.; Perez-Vila, E.; Serrano, S.; Nacher, M.; Aubia, J.; Supervia, A.; Recker, R. R. Vitamin D treatment in myelodysplastic syndromes. Br. J. Haematol. 1998, 100(3), 516-520.
[213] Ganser, A.; Seipelt, G.; Verbeek, W.; Ottmann, O. G.; Maurer, A.; Kolbe, K.; Hess, U.; Elsner, S.; Reutzel, R.; Wormann, B. Effect of combination therapy with all-trans-retinoic acid and recombinant human granulocyte colony-stimulating factor in patients with myelodysplastic syndromes. Leukemia 1994, 8(3), 369-375.
[214] Hofmann, W. K.; Ganser, A.; Seipelt, G.; Ottmann, O. G.; Zander, C.; Geissler, G.; Hoffmann, K.; Hoffken, K.; Fischer, J. T.; Isele, G.; Hoelzer, D. Treatment of patients with low-risk myelodysplastic syndromes using a combination of all-trans retinoic acid, interferon alpha, and granulocyte colony-stimulating factor. Ann. Hematol. 1999, 78(3), 125-130.
[215] Matsui, W. H.; Gladstone, D. E.; Vala, M. S.; Barber, J. P.; Brodsky, R. A.; Smith, B. D.; Jones, R. J. The role of growth factors in the activity of pharmacological differentiation agents. Cell Growth Differ. 2002, 13(6), 275-283.
[216] Matsui, W.; Huff, C. A.; Vala, M.; Barber, J.; Smith, B. D.; Jones, R. J. Anti-tumour activity of interferon-alpha in multiple myeloma: role of interleukin 6 and tumor cell differentiation. Br. J. Haematol. 2003, 121(2), 251-258.
[217] Matsui, W.; Smith, B. D.; Vala, M.; Beal, N.; Huff, C. A.; Diehl, L. F.; Jones, R. J. Requirement for myeloid growth factors in the differentiation of acute promyelocytic leukaemia. Br. J. Haematol. 2005, 128(6), 853-862.
[218] Williams, C. D.; Linch, D. C.; Watts, M. J.; Thomas, N. S. Characterization of cell cycle status and E2F complexes in mobilized CD34+ cells before and after cytokine stimulation. Blood 1997, 90(1), 194-203.
[219] Williams, G. T.; Smith, C. A.; Spooncer, E.; Dexter, T. M.; Taylor, D. R. Haemopoietic colony stimulating factors promote cell survival by suppressing apoptosis. Nature 1990, 343(6253), 76-79.
Received: November 08, 2006 Revised: April 03, 2007 Accepted: April 09, 2007