My crook back
22
“My Crook Back” Dr Adrian Nowitzke Acknowledgement: Dr Paul Licina as creator of original slides
-
Upload
spineplus -
Category
Health & Medicine
-
view
75 -
download
0
Transcript of My crook back
“My Crook Back”
Dr Adrian Nowitzke
Acknowledgement: Dr Paul Licina as creator of original slides

Graphic from www.hibiscusflowershop.blogspot.com
Today is not about:
the statistics of back pain
the “blah blah blah” of back pain
management of “garden variety” conditions
being “talked at”
The purpose of today:
To dissect the pot-pourri of back pain byexploring the evidence, techniques and strategies
ofexaminationinvestigation
non-operative treatmentoperative treatment
To provide practical tips and tricks to managing this group of patients
CHRONICSPECIFIC
ACUTESPECIFIC
CHRONICNON
SPECIFIC
ACUTENONSPECIFIC
CHRONICSPECIFIC
ACUTESPECIFIC
CHRONICNON
SPECIFIC
ACUTENONSPECIFIC
Resolves < 3 monthsSurgery rarely indicated w/o neurological change
CHRONICSPECIFIC
ACUTESPECIFIC
CHRONICNON
SPECIFICACUTENONSPECIFIC
Surgeryhas a role
ChronicNon-specific
Low BackPain
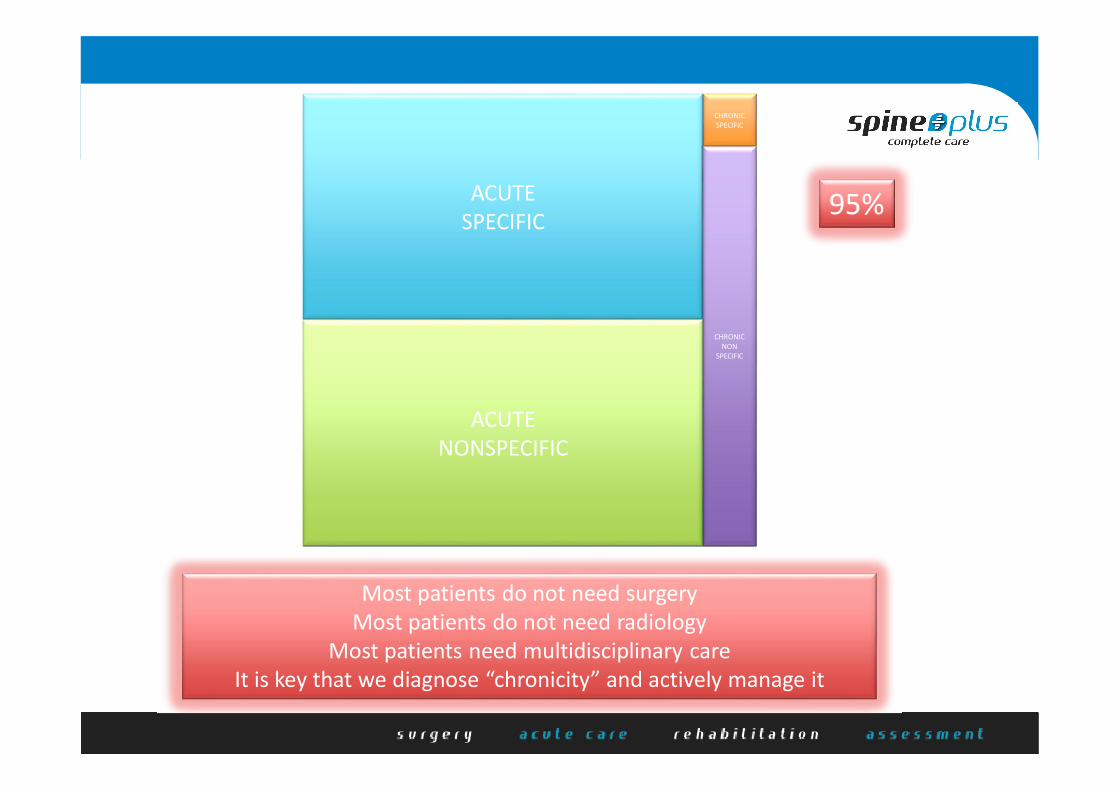
CHRONICSPECIFIC
ACUTESPECIFIC
CHRONICNON
SPECIFIC
ACUTENONSPECIFIC
95%
Most patients do not need surgeryMost patients do not need radiology
Most patients need multidisciplinary careIt is key that we diagnose “chronicity” and actively manage it

http://www.biomedcentral.com/1471-2474/9/11
Chronic non-specific low back painsub-groups or a single mechanism?
Benedict M Wand and Neil E O'Connell
CNSLBP patients have back pain yet no conservative or surgical pain relieving measures directed at the back appear effective.
• exercise programme• manipulation• massage• acupuncture• cognitive therapy• functional restoration• steroid injection• radiofrequency neurotomy• spinal fusion
similar effectsvariable and modest improvementnot sustained over time
They display a number of biomechanical abnormalities, however treatment directed at normalising lumbar biomechanics has little effect and there is no relationship between changes in outcome and changes in spinal mechanics.
• exercise is beneficial• no evidence that one type better than
another• general physical activity may be better than
specific exercises
They demonstrate some psychological problems but psychologically based treatments offer only partial solution to the problem.
• high levels of distress• presence of depression• fear-avoidance behaviour
A possible explanation for these findings is that they are epiphenomena, features that are incidental to a problem of neurological reorganisation and degeneration.
• is it in the brain vs the back?• much evidence to suggest changes in brain
structure and function• reorganisation of the brain may lead to
sensitisation of nociceptive pathways, central pain memories, sensory-motor conflict
• may lead to changes in back biomechanics• may alter cortical representation of back
and lead to fear-avoidance behaviour• thus biomechanical and psychological
changes may be the compensatory rather than causative
Tools you may find helpful
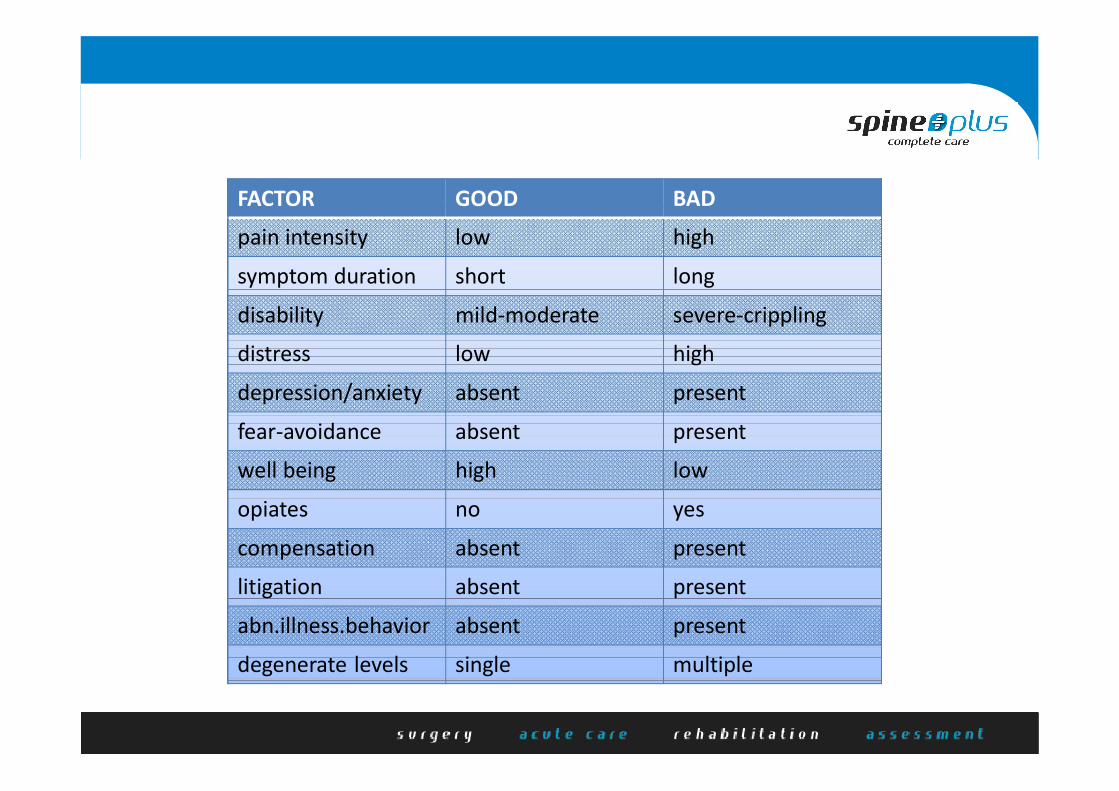
FACTOR GOOD BAD
pain intensity low high
symptom duration short long
disability mild-moderate severe-crippling
distress low high
depression/anxiety absent present
fear-avoidance absent present
well being high low
opiates no yes
compensation absent present
litigation absent present
abn.illness.behavior absent present
degenerate levels single multiple
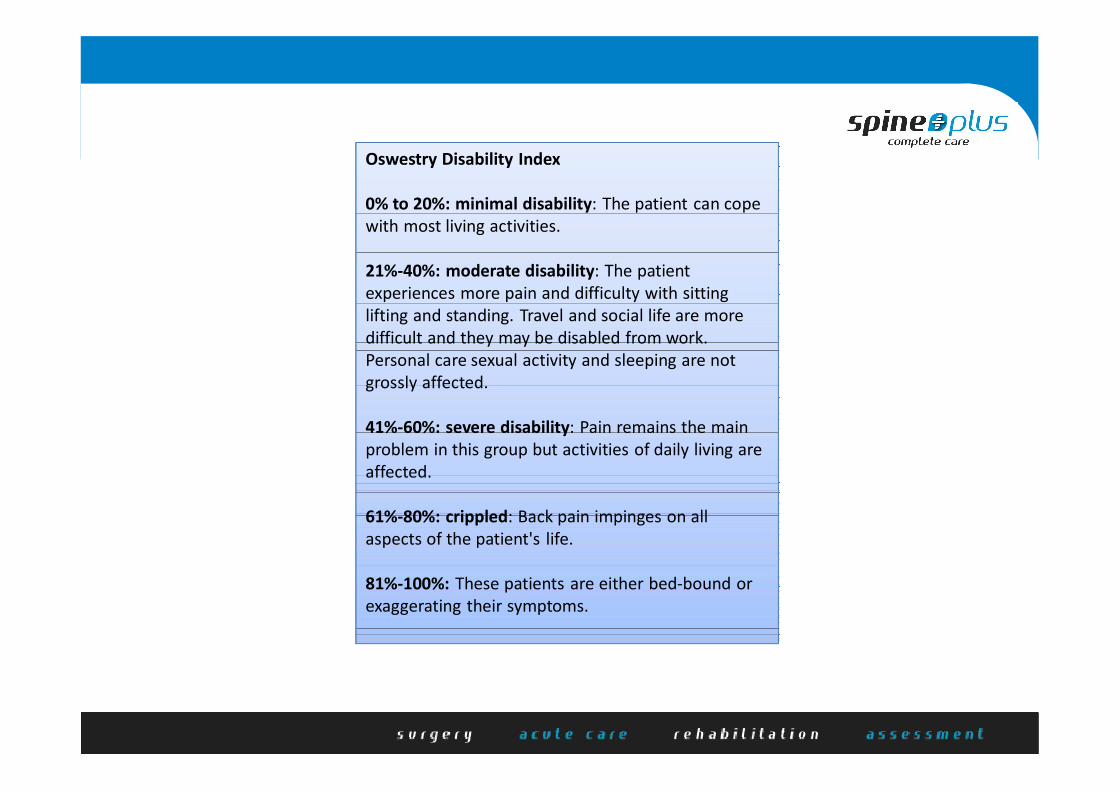
Oswestry Disability Index
0% to 20%: minimal disability: The patient can cope with most living activities.
21%-40%: moderate disability: The patient experiences more pain and difficulty with sitting lifting and standing. Travel and social life are more difficult and they may be disabled from work. Personal care sexual activity and sleeping are not grossly affected.
41%-60%: severe disability: Pain remains the main problem in this group but activities of daily living are affected.
61%-80%: crippled: Back pain impinges on all aspects of the patient's life.
81%-100%: These patients are either bed-bound or exaggerating their symptoms.
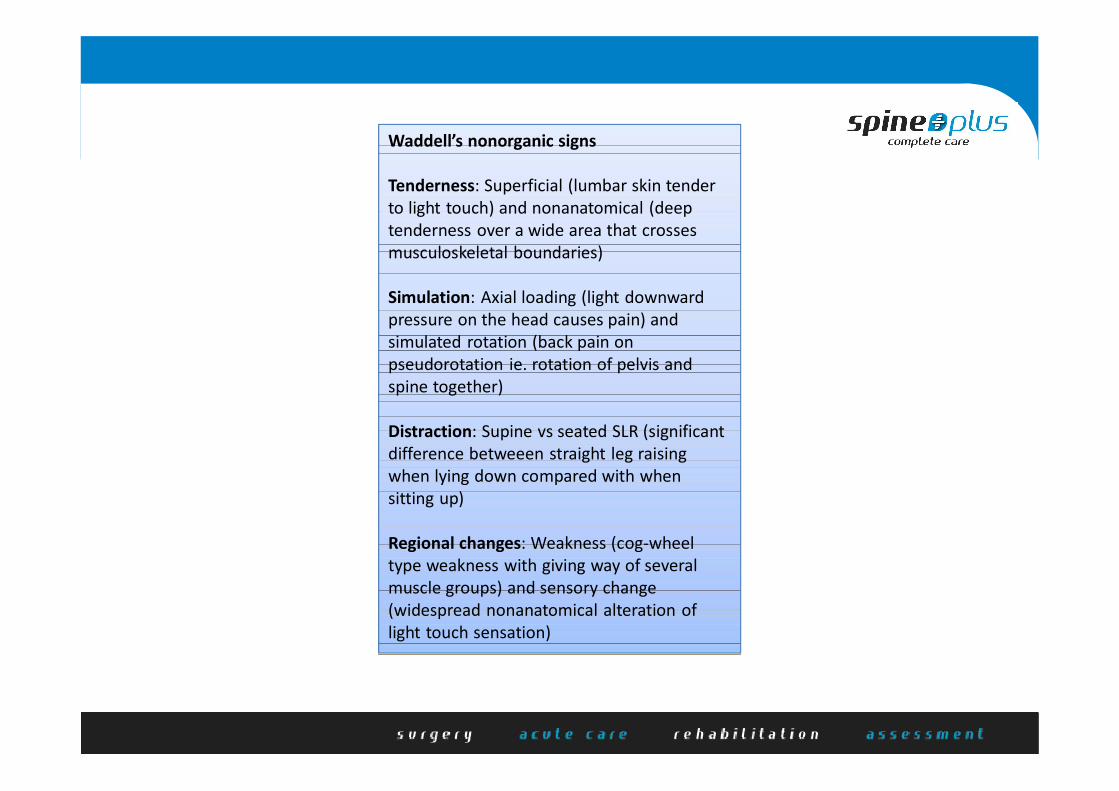
Waddell’s nonorganic signs
Tenderness: Superficial (lumbar skin tender to light touch) and nonanatomical (deep tenderness over a wide area that crosses musculoskeletal boundaries)
Simulation: Axial loading (light downward pressure on the head causes pain) and simulated rotation (back pain on pseudorotation ie. rotation of pelvis and spine together)
Distraction: Supine vs seated SLR (significant difference betweeen straight leg raising when lying down compared with when sitting up)
Regional changes: Weakness (cog-wheel type weakness with giving way of several muscle groups) and sensory change (widespread nonanatomical alteration of light touch sensation)

Three take home strategies
Understand and explain the cause
80% of people get back pain.90% improve within 3 months.For those who do not improve (CNSLBP)
Most people have nothing serious wrong.Multiple investigations and treatments are unhelpful.There is likely to be a central cause that is not well understood.
Provide evidence-based treatment advice
Drug treatment does not cure back pain.Opioids only partially relieve the pain and must be used carefully.Massage and manipulation can help relieve pain.Exercises can be beneficial.Multidisciplinary therapy can help improve function, but will not completely cure pain.Surgery can help some patients to various degrees, but most people are not suitable candidates.
Avoid making things worse
Recognise those at risk of chronicity.Minimise the use of opiates.Discourage prolonged passive treatments.Ensure imaging done with contextual interpretation.Refer judiciously to exclude treatable cause.Facilitate return to activity and work.Try to help in the compensation process.Do not encourage litigation.