
Multiple sclerosis - med.swu.ac.th fileOutline • Epidemiology • Pathology & pathogenesis •...
60
Multiple sclerosis Monton Wongwandee, M.D. Division of Neurology Faculty of Medicine Srinakharinwirot University
Transcript of Multiple sclerosis - med.swu.ac.th fileOutline • Epidemiology • Pathology & pathogenesis •...
Multiple sclerosis
Monton Wongwandee, M.D.Division of NeurologyFaculty of Medicine
Srinakharinwirot University
MS
• Inflammatory demyelination of CNS neurons• Relapsing‐remitting or progressive course• Dissemination in time & space
Outline
• Epidemiology• Pathology & pathogenesis• Etiology• Clinical manifestations• Clinical course and prognosis• Diagnosis• Treatment• Neuromyelitis optica (Devic’s disease)
Outline
• Epidemiology• Pathology & pathogenesis• Etiology• Clinical manifestations• Clinical course and prognosis• Diagnosis• Treatment• Neuromyelitis optica (Devic’s disease)
Epidemiology
• Female: male = 3:1 (6:1 in Thai)• Age of onset: typically 20‐40 years• Prevalence: increasing at higher latitudes
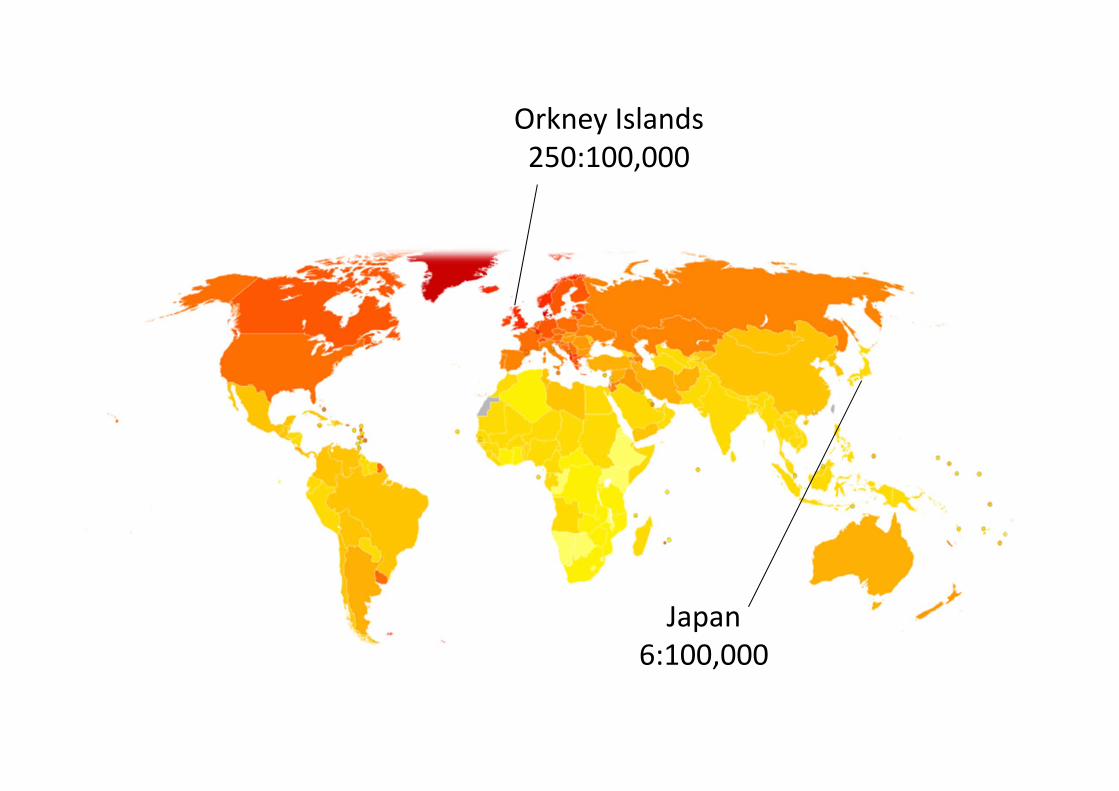
Orkney Islands250:100,000
Japan6:100,000
Outline
• Epidemiology• Pathology & pathogenesis• Etiology• Clinical manifestations• Clinical course and prognosis• Diagnosis• Treatment• Neuromyelitis optica (Devic’s disease)

Pathology
• Lesions vary in size (1‐2mm to cms)• Triad
– Inflammation• Perivenular cuffing with T‐cells & MØ
• BBB breakdown– Demyelination– Gliosis (astrocytic proliferation)
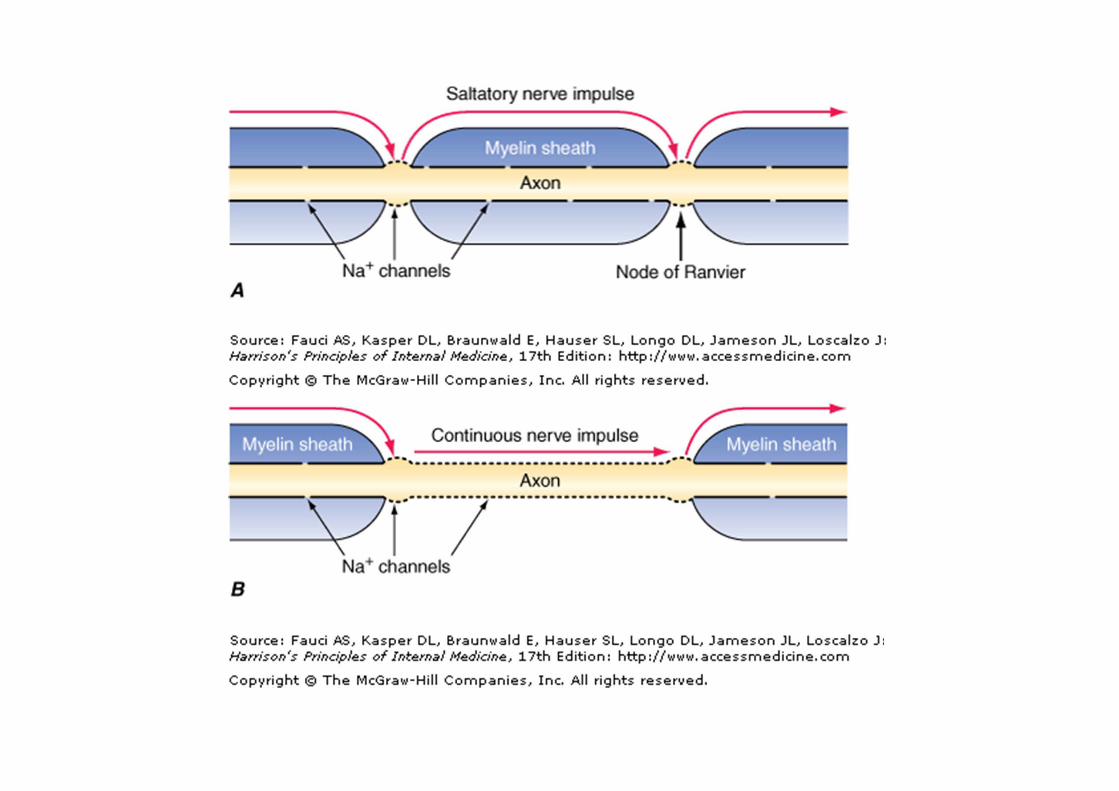
• Axonal loss– Major contributor to irreversible neurologic disability
• Heterogeneity
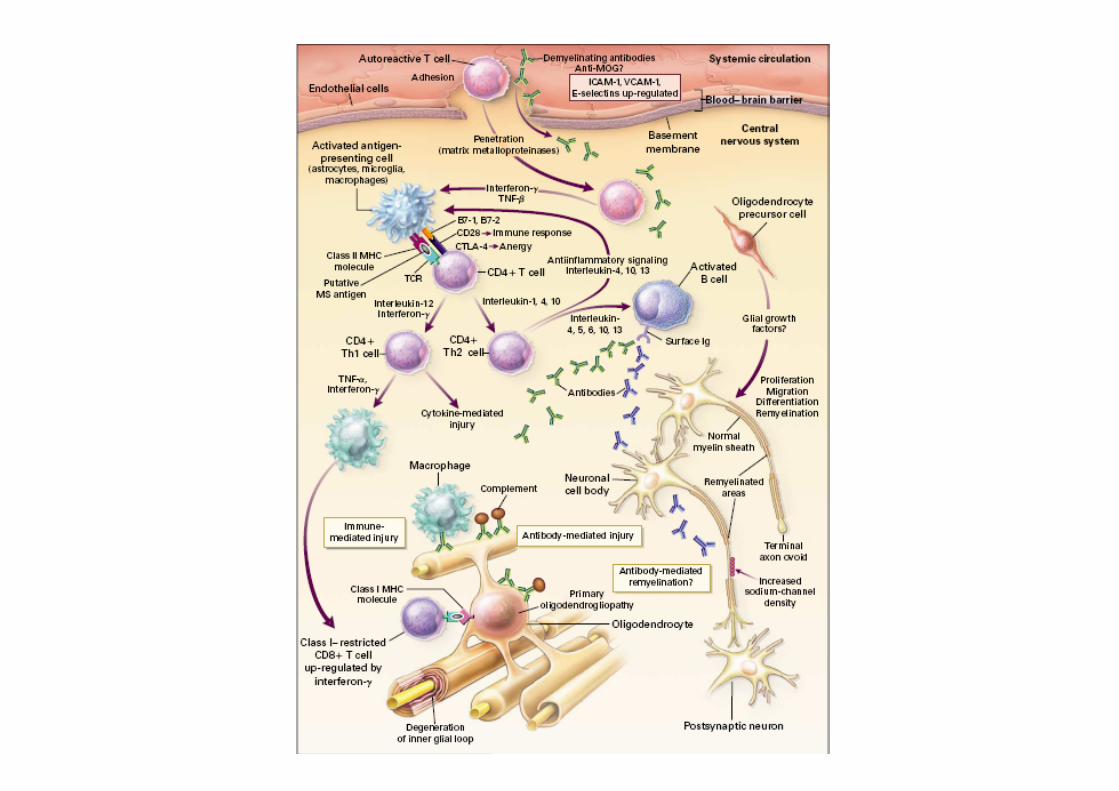
Immunology• Antigen
– Myelin basic protein (MBP)– Myelin oligodendrocyte glycoprotein (MOG)
• Autoreactive T lymphocytes• Humoral autoAb
– B cells– Oligoclonal Ab (intrathecal synthesis)
• Cytokines– IL‐2– TNF‐– IFN‐
• Triggers– URTI (viral)

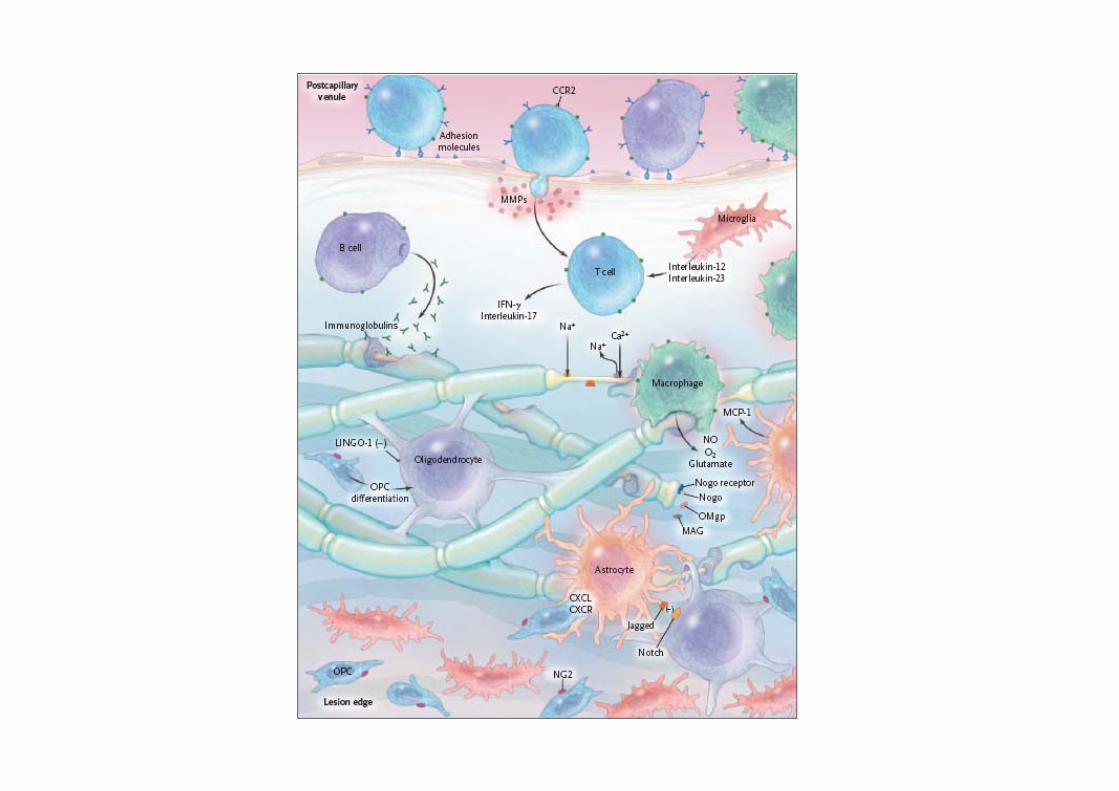
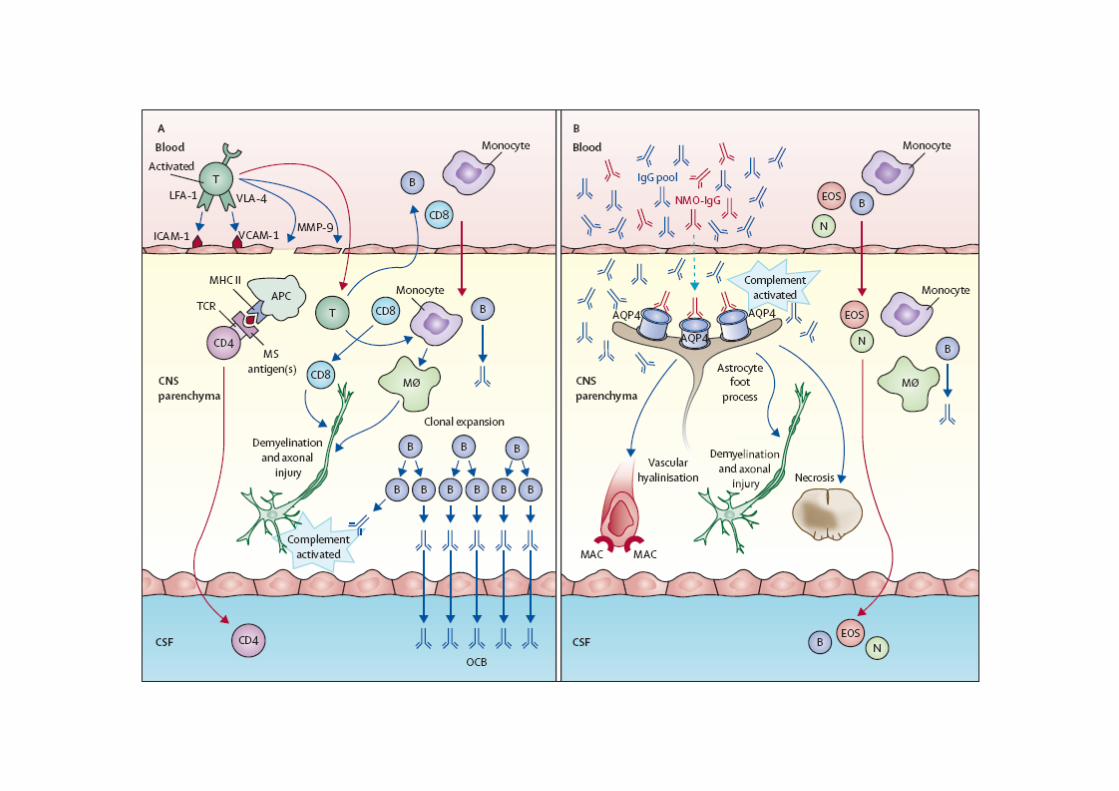
Pathogenesis
• T lymphocyte activation• BBB breakdown• Lymphocytes infiltration
– T cells (CD4,CD8) macrophage– B cells antibodies, compliments
• Oligodendrocytes & myeline destruction• Gray matter involvement

Outline
• Epidemiology• Pathology & pathogenesis• Etiology• Clinical manifestations• Clinical course and prognosis• Diagnosis• Treatment• Neuromyelitis optica (Devic’s disease)
Etiology
• Unknown– Genetic– Environment
Genetic
• Caucasians > africans, asians• Polygene• Genetic heterogeneity
Environment
• Geographic– Higher latitudes, sun exposure– Vitamin D deficiency– Immunoregulatory effect
• High socioeconomic status– Delayed initial exposures to infectious agents?
• Remote infection– EBV?
Outline
• Epidemiology• Pathology & pathogenesis• Etiology• Clinical manifestations• Clinical course and prognosis• Diagnosis• Treatment• Neuromyelitis optica (Devic’s disease)
Clinical manifestations
• Extremely vary – Location: optic n., brain, spinal cord– Onset: abrupt – insidious– Severity: trivial – severe
• Attack from RRMS generally evolve over days to weeks
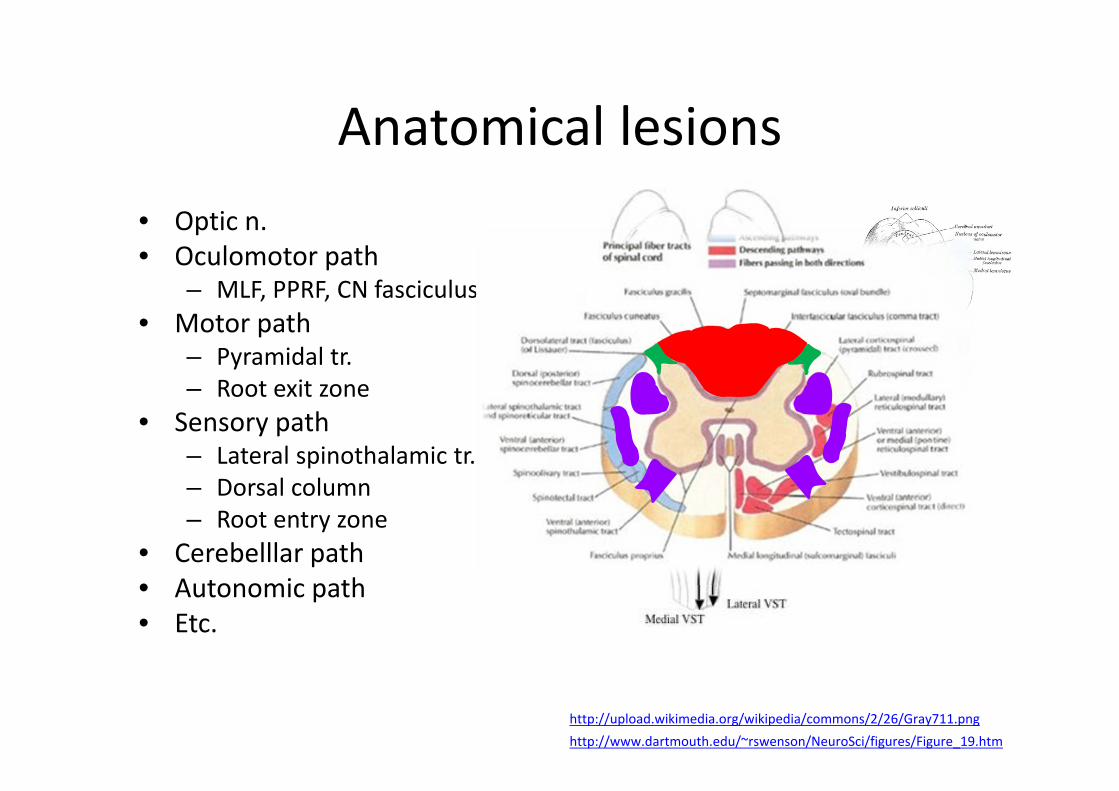
Anatomical lesions• Optic n.• Oculomotor path
– MLF, PPRF, CN fasciculus• Motor path
– Pyramidal tr.– Root exit zone
• Sensory path– Lateral spinothalamic tr.– Dorsal column– Root entry zone
• Cerebelllar path• Autonomic path• Etc.
http://www.dartmouth.edu/~rswenson/NeuroSci/figures/Figure_19.htmhttp://upload.wikimedia.org/wikipedia/commons/2/26/Gray711.png

Clinical manifestationsSymptom Percent of Cases Symptom Percent of Cases
Sensory loss 37 Lhermitte 3
Optic neuritis 36 Pain 3
Weakness 35 Dementia 2
Paresthesias 24 Visual loss 2
Diplopia 15 Facial palsy 1
Ataxia 11 Impotence 1
Vertigo 6 Myokymia 1
Paroxysmal attacks
4 Epilepsy 1
Bladder 4 Falling 1
Characteristic manifestations
• Intractable hiccup• Intractable vomiting• Intractable itching• Bilateral INO• Bilateral trigeminal neuralgia• Painful tonic spasm• Uhthoff’s symptom (heat sensitivity)
Uhthoff's Phenomenon
• Pseudoexacerbation• Increase in ambient temperature• Fever• Infection• Metabolic abnormalities
Outline
• Epidemiology• Pathology & pathogenesis• Etiology• Clinical manifestations• Clinical course and prognosis• Diagnosis• Treatment• Neuromyelitis optica (Devic’s disease)
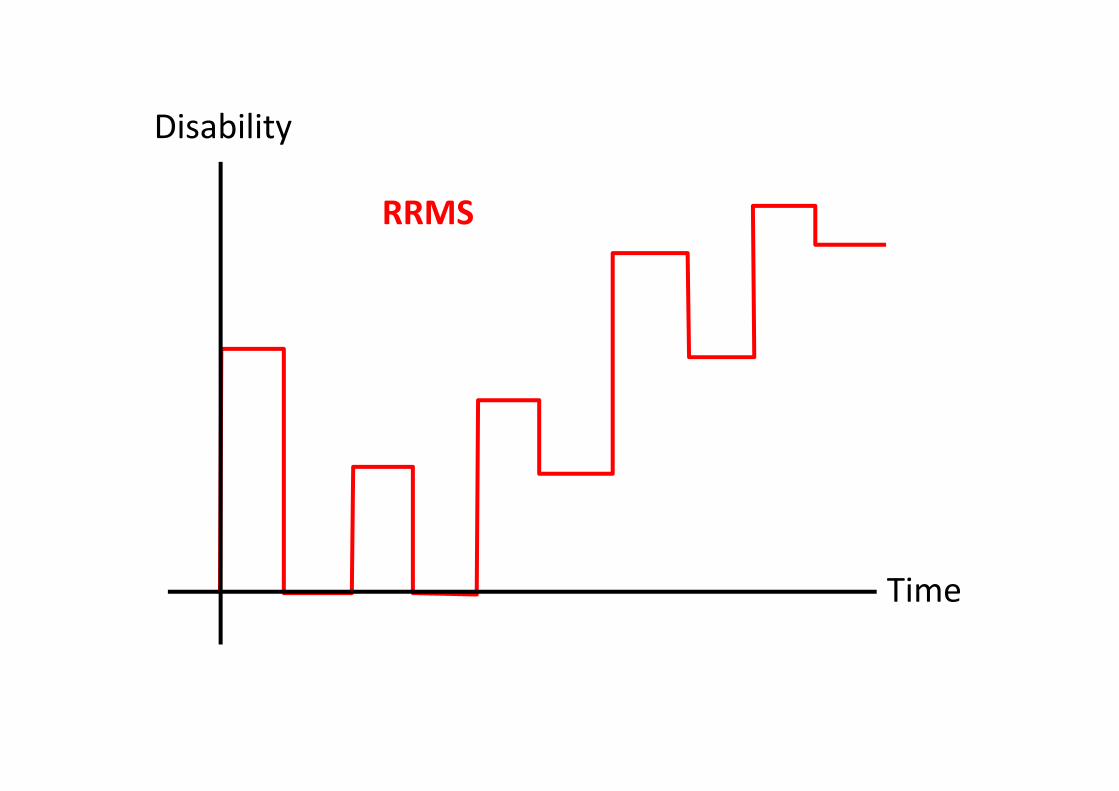
Disability
Time
RRMS
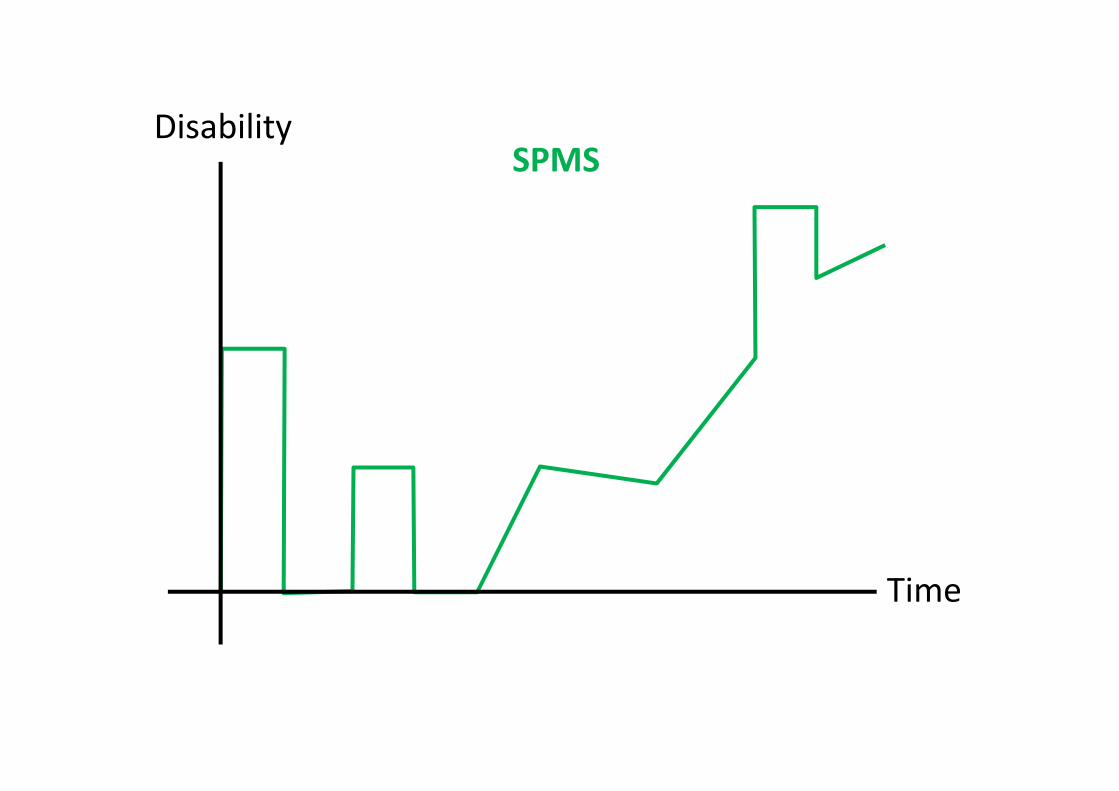
Disability
Time
SPMS
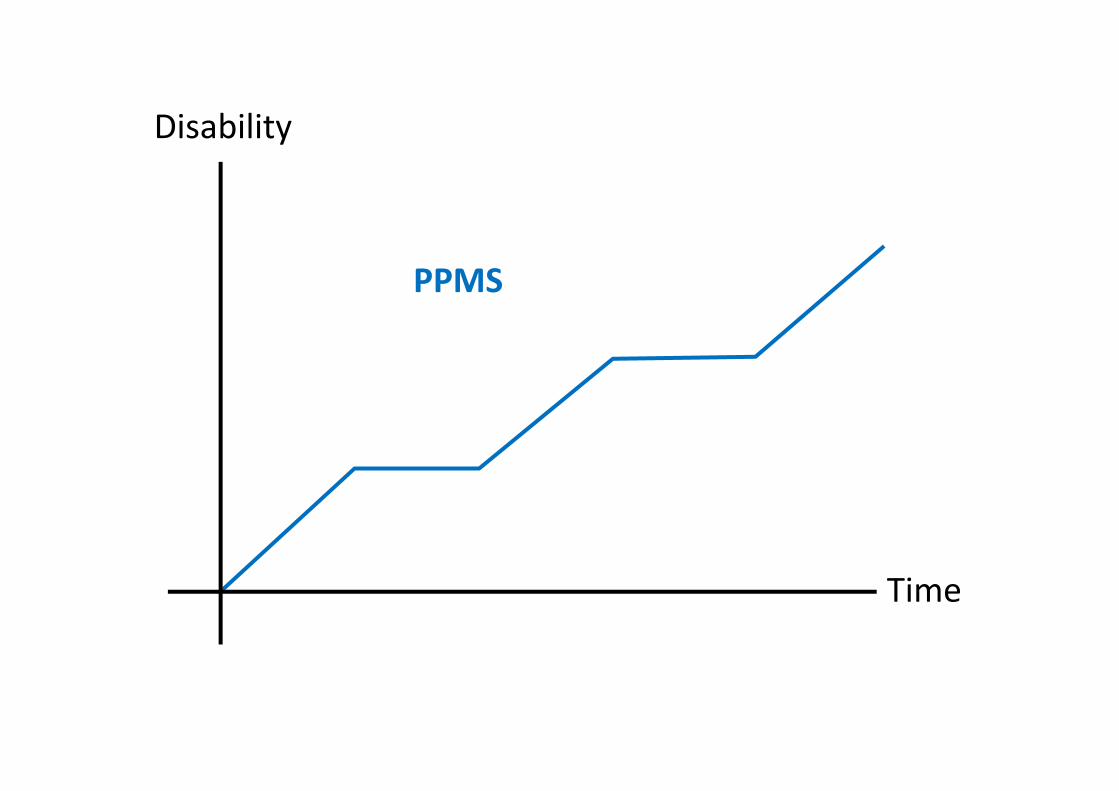
Disability
Time
PPMS
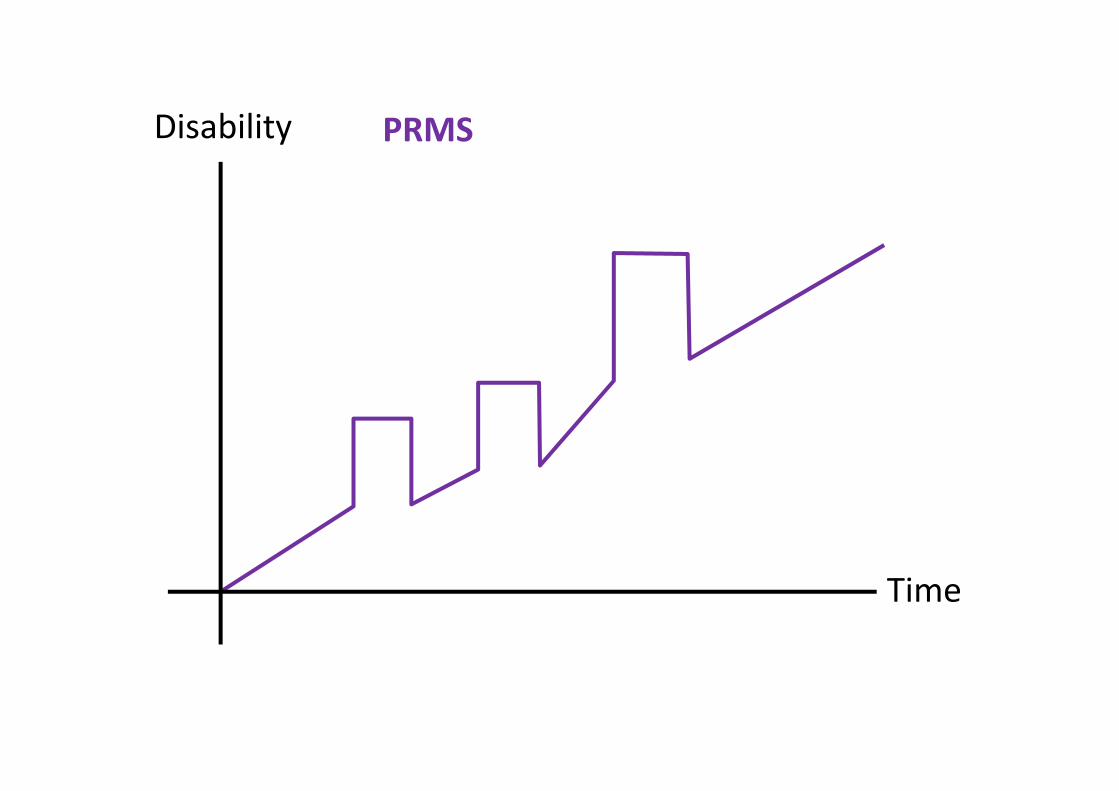
Disability
Time
PRMS
Prognosis• Overall,
– ambulation require assistance in most cases • 80% at 25 years after onset
– Benign variant < 20% (no disability)• Individual,
– Favorable outcome• ON or sensory symptoms at onset• < 2 relapses in the 1st year• Minimal impairment after 5 years
– Poor prognosis• Truncal ataxia• Action tremor• Pyramidal symptoms• Progressive course
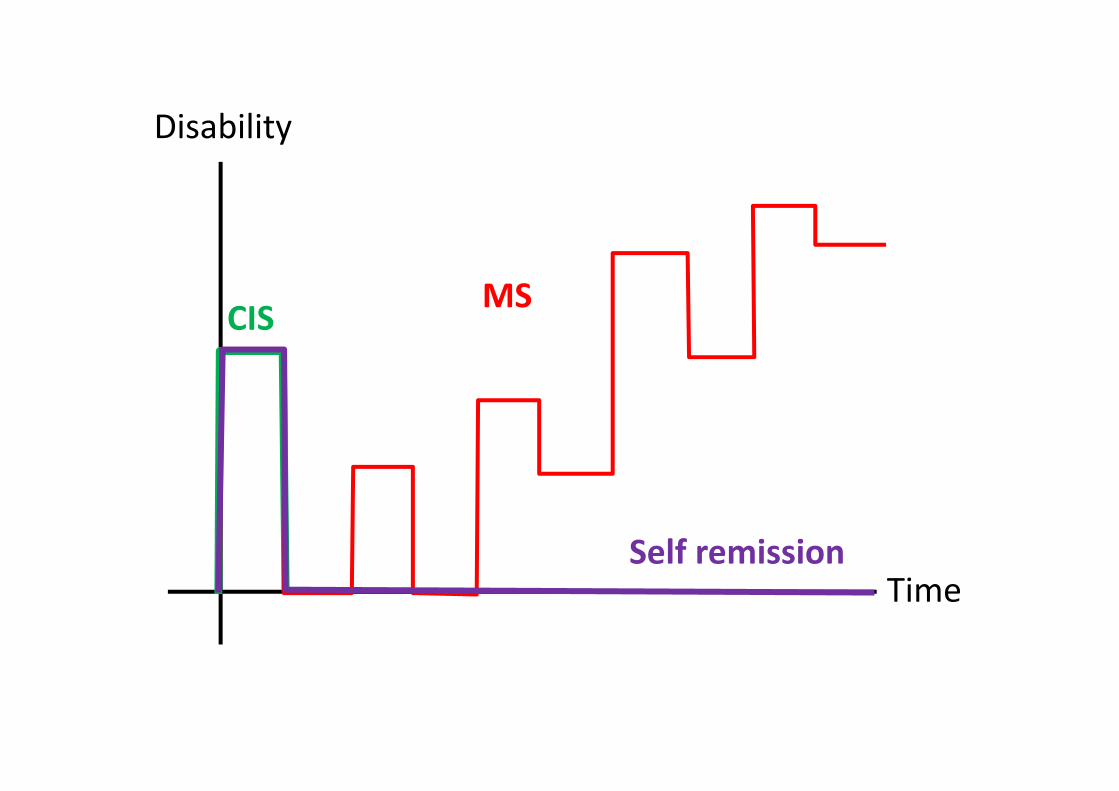
Disability
Time
MSCIS
Self remission
Clinically isolated syndrome (CIS)
• Single attack compatible with MS (first demyelinating event)
• Most common: ON, transverse myelitis• Prognosis
– Abnormal brain MRI 10 yr risk ̴ 60%– Normal brain MRI 10 yr risk ̴ 20%
Outline
• Epidemiology• Pathology & pathogenesis• Etiology• Clinical manifestations• Clinical course and prognosis• Diagnosis• Treatment• Neuromyelitis optica (Devic’s disease)
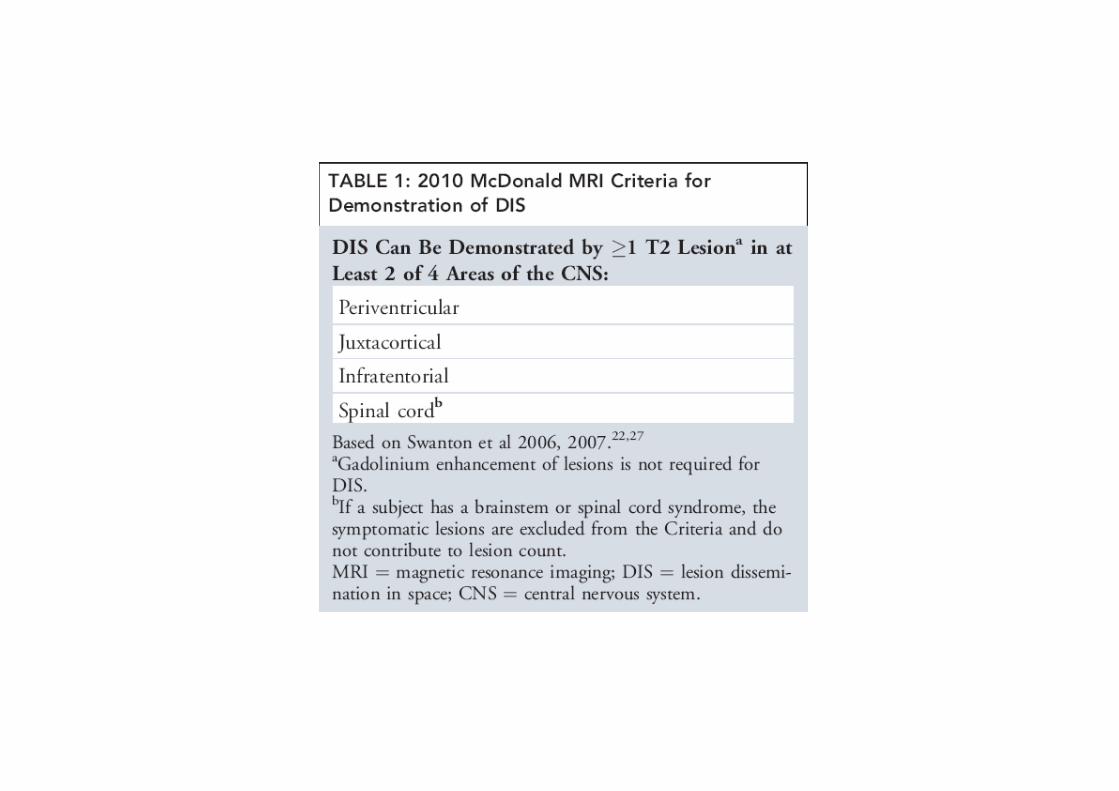
Dissemination in time and space
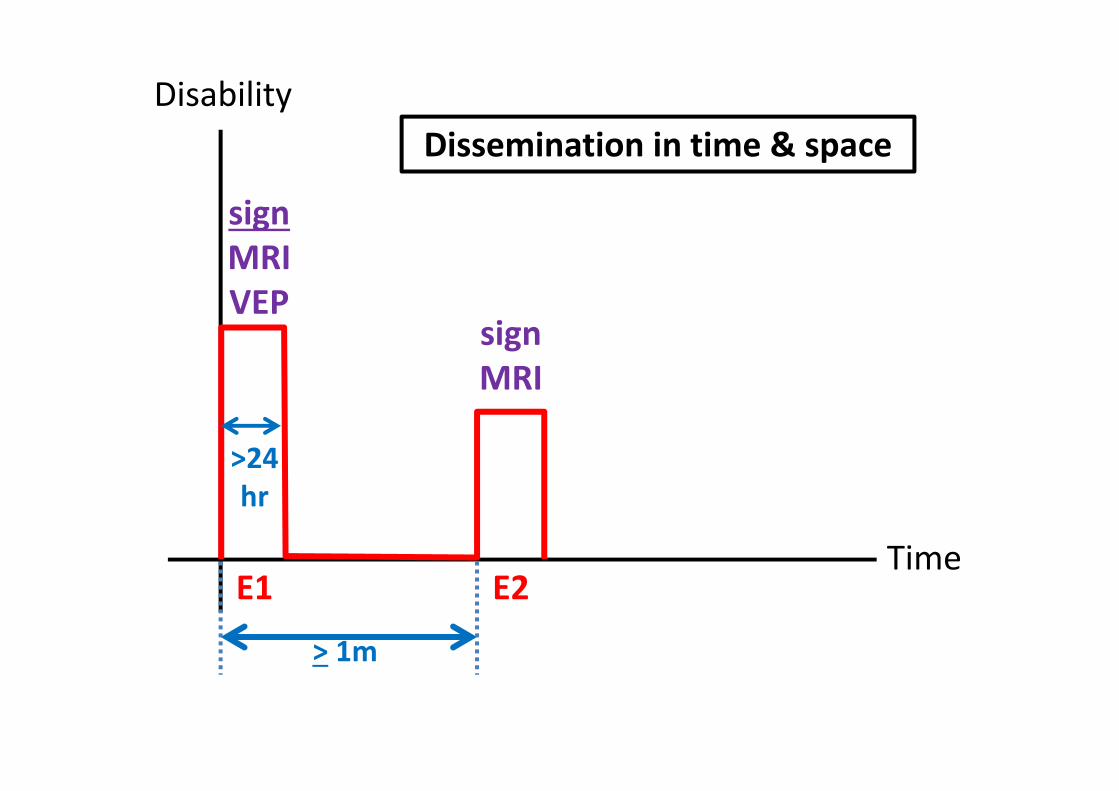
Disability
TimeE1 E2
> 1m
signMRIVEP
signMRI
>24hr
Dissemination in time & space

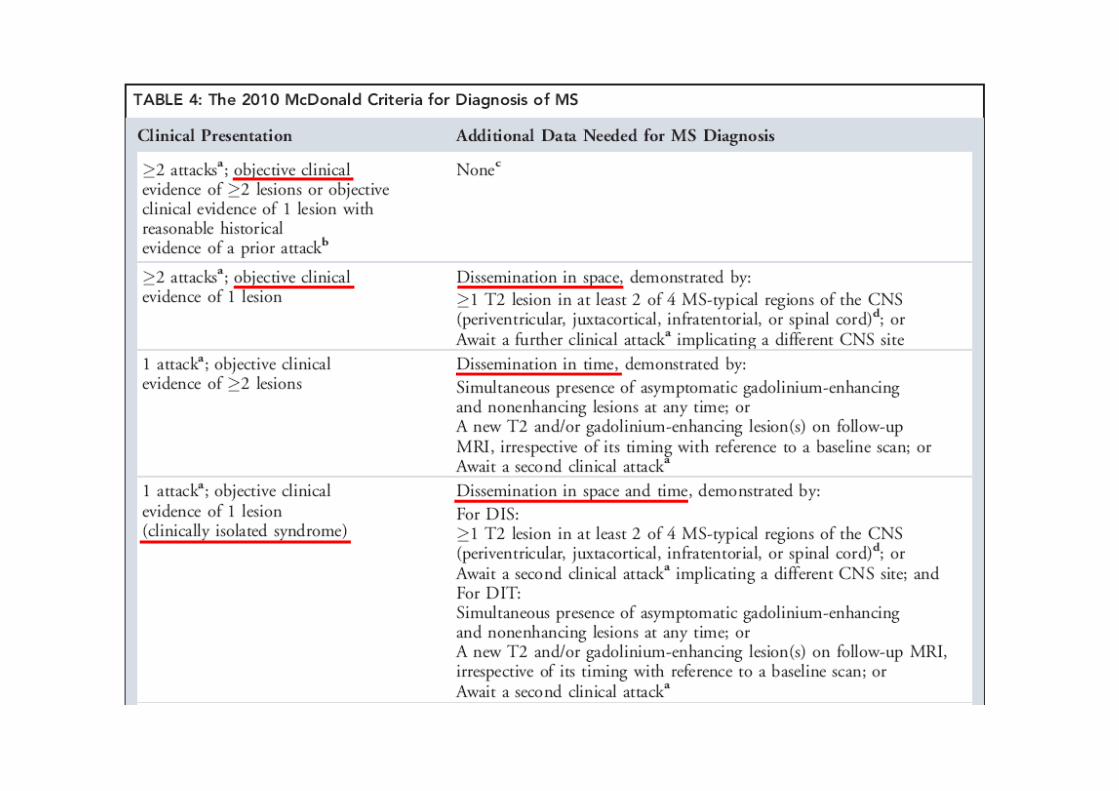
Diagnostic tests
• MRI• Evoked potentials• CSF
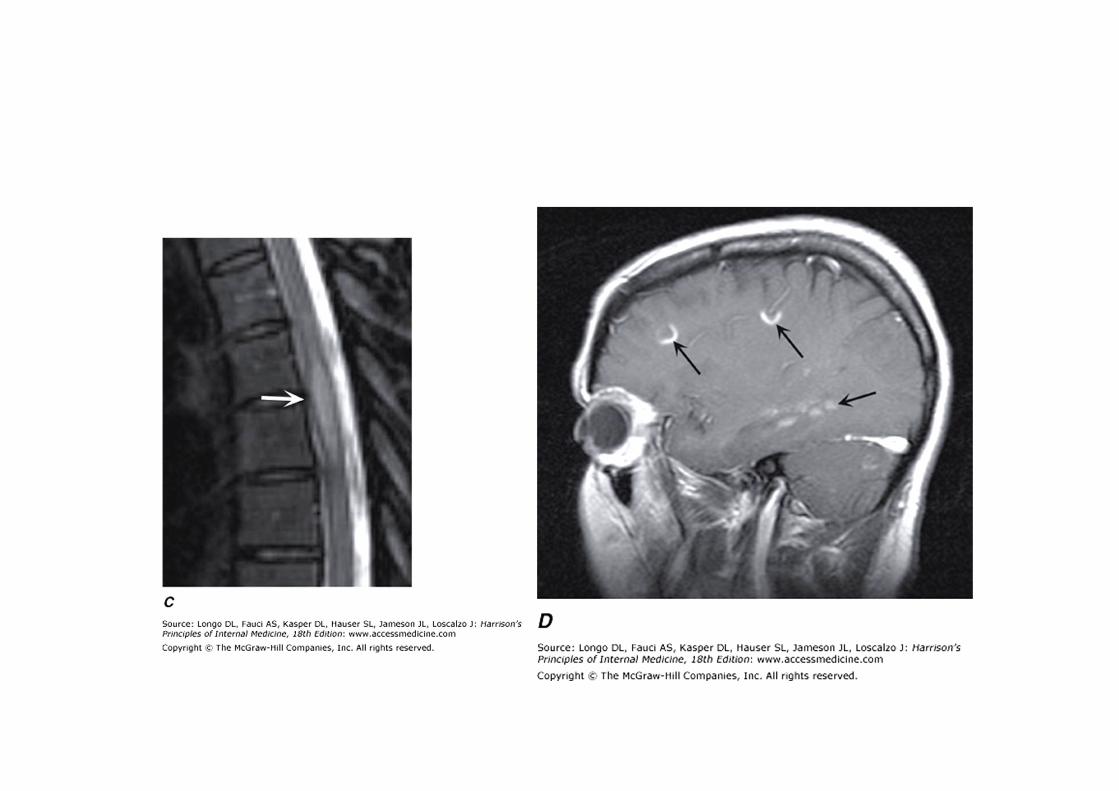
MRI
• Characteristics of lesions– Hypersignality in T2,FLAIR image– Gadolinium enhancement (BBB breakdown)– Hyposignality in T1 image (black holes)
• Distribution– White matter, usually no edema– Multifocal lesions involved brain, brain stem, spinal cord
• Periventricular area• Corpus collosum
• Other technic– MTR (magnitization transfer ratio)– MRS (magnetic resonance spectroscopy)
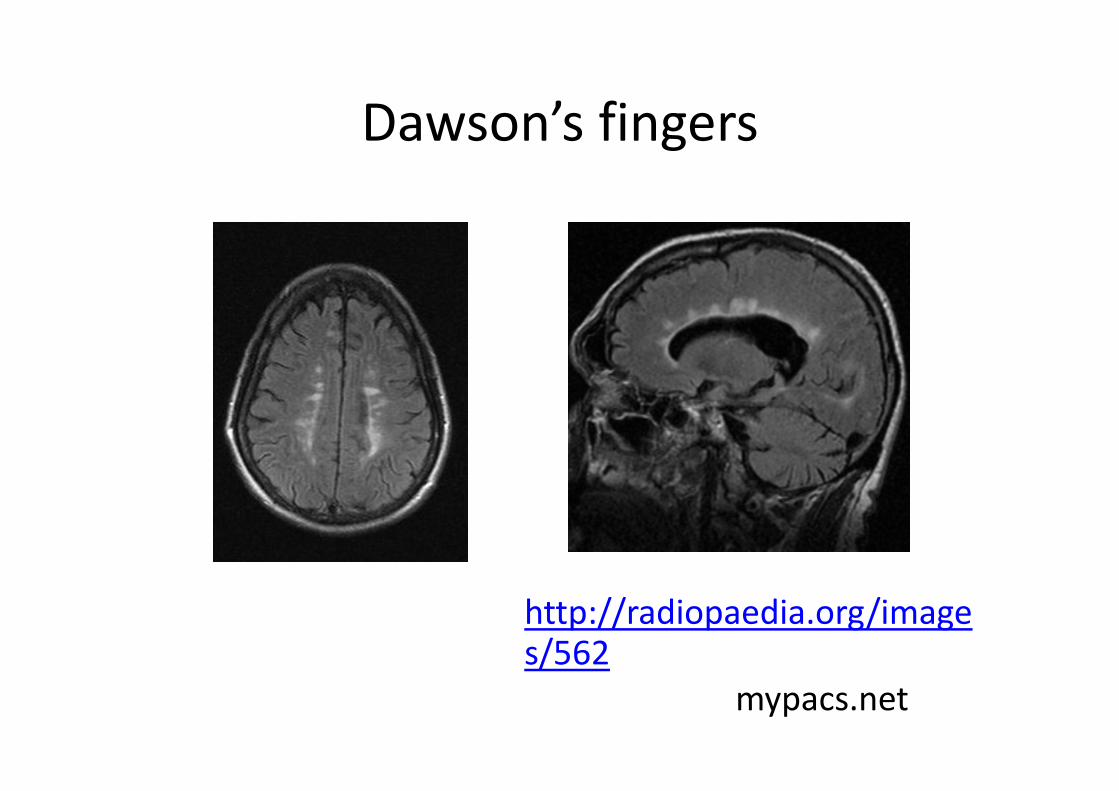
Dawson’s fingers
mypacs.net
http://radiopaedia.org/images/562
Evoked potentials
• Test of function in CNS pathways– Afferent : VEP,BAEP,SSEP– Efferent: motor
• Non‐specific etiology

CSF
• Most are normal• Mild MNC pleocytosis (WBC > 5cells/µL)• CSF total protein normal or slightly increase• Red flags
– WBC > 75 cells/µL– PMN predominate– Protein > 100 mg/dL
Outline
• Epidemiology• Pathology & pathogenesis• Etiology• Clinical manifestations• Clinical course and prognosis• Diagnosis• Treatment• Neuromyelitis optica (Devic’s disease)
Treatment
• Acute attack• Disease modifying therapy
Acute attack
• Shortening the symptom• Long term effect?• High dose steroid
– Methylprednisolone 500‐1,000 mg/day x 3‐5 days with/without tapering in 2 weeks
• Plasma exchange in selected case that not responding to corticosteroid (no clear benefit)
Disease modifying therapy
• Slow the disease but not stop it!• First choice
– Interferon beta‐1a,1b– Glatiramer acetate
• Natalizumab• Mitoxantrone• Fingolimod
Outline
• Epidemiology• Pathology & pathogenesis• Etiology• Clinical manifestations• Clinical course and prognosis• Diagnosis• Treatment• Neuromyelitis optica (Devic’s disease)
Neuromyelitis optica(NMO)
Devic’s disease
Clinical manifestations
• ON (unilateral or bilateral)• Myelitis• Days, months or years between attack• Usually not brain stem, cerebellar, cognitive involvement
• Brain MRI is typically normal• OSMS (Optico‐spinal MS) or Asian type MS ?
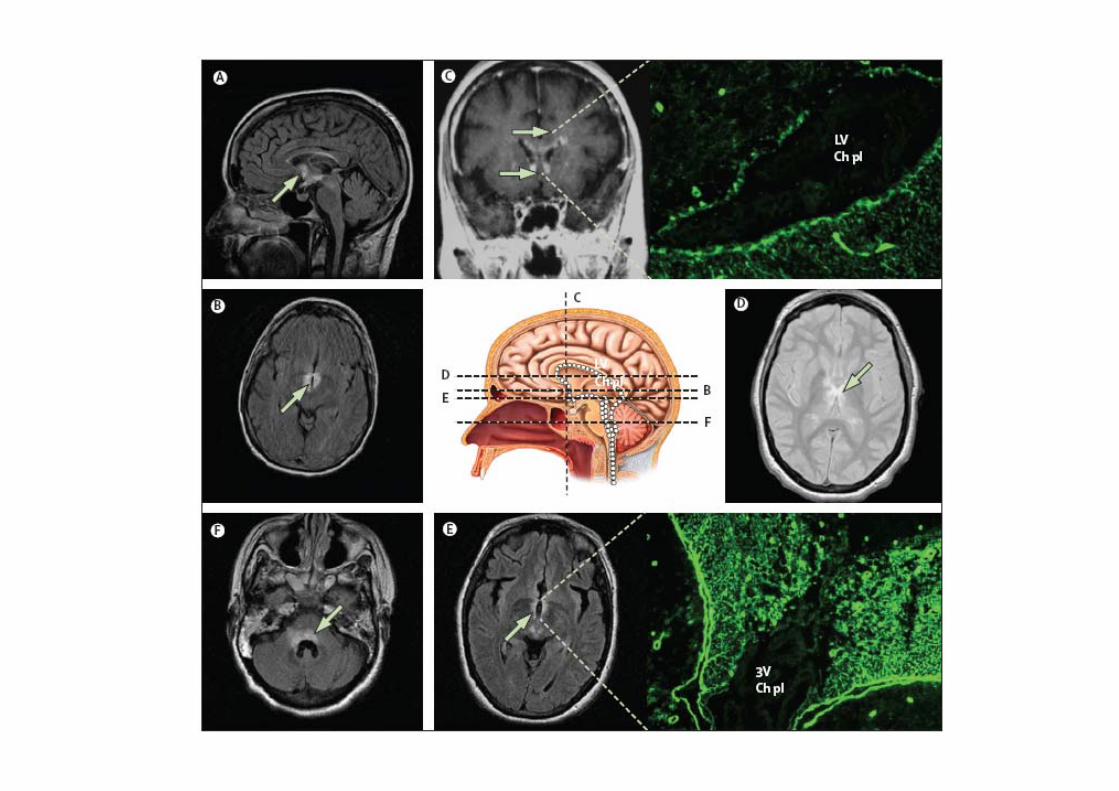
Pathophysiology
• NMO IgG• Aquaporin 4 (AQP4)
– Water channel at foot process of the perivascularastrocyte
• Necrotizing cavitation
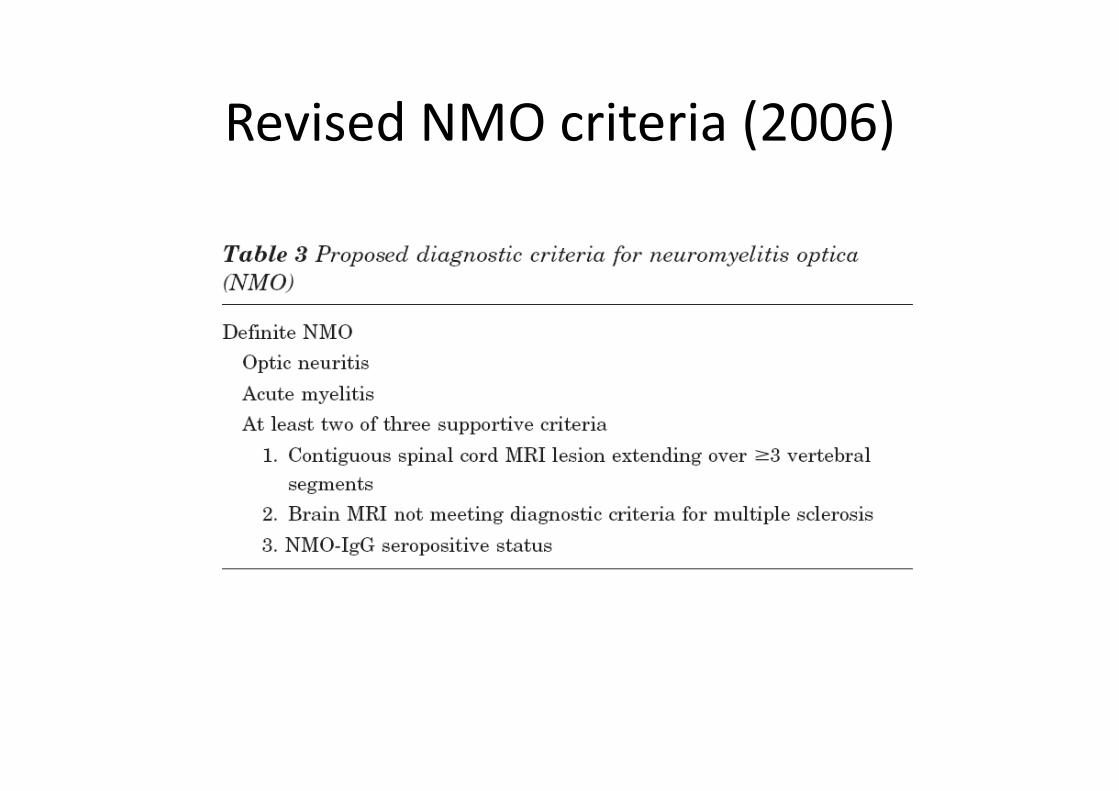
Revised NMO criteria (2006)
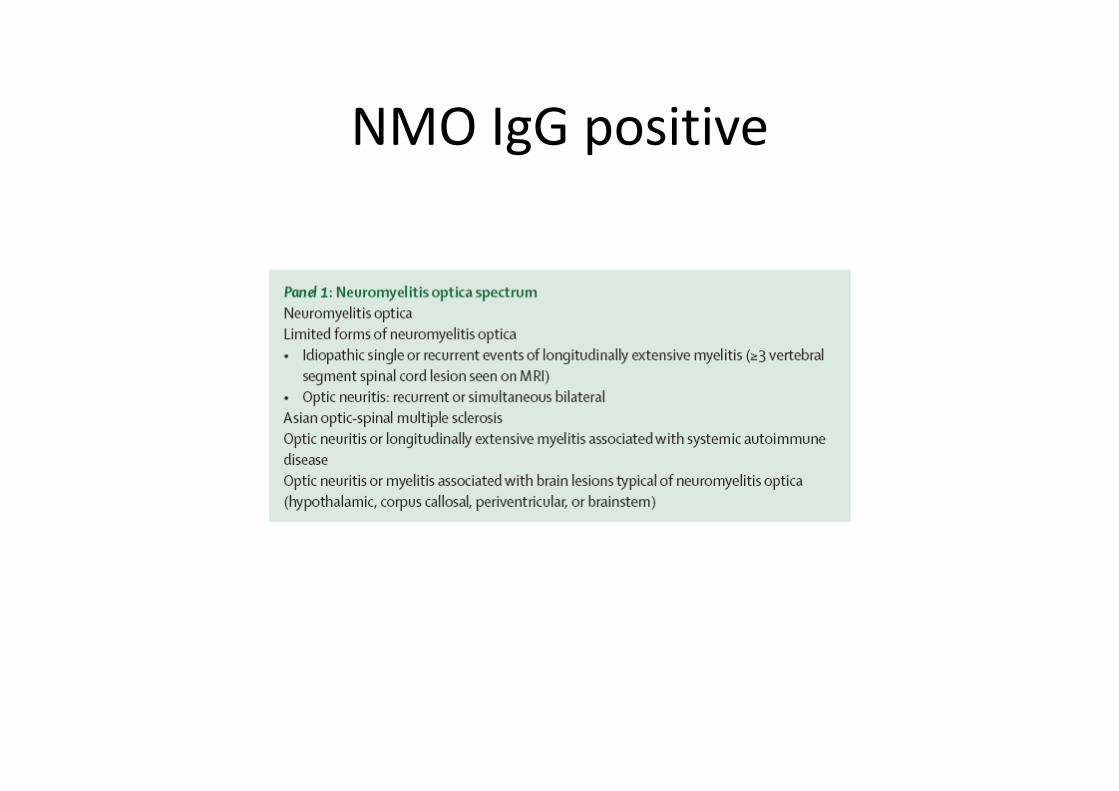
NMO IgG positive

Treatment
• Acute attack– Steroid– PE
• Disease modifying therapy ?


















