
Multiple Myeloma - UnityPoint Health · Labs – CBC, Calcium, Creatinine, SPEP, UPEP, Serum free...
61
Multiple Myeloma Solving a growing puzzle
Transcript of Multiple Myeloma - UnityPoint Health · Labs – CBC, Calcium, Creatinine, SPEP, UPEP, Serum free...
Multiple Myeloma Solving a growing puzzle
Disclosures
• Financial – I wish.
• I eat too much.
• I did ask who the audience would be.
Nurses and Doctors
Goals
• 1. Understand the incidence, symptoms, and pathophysiology of myeloma.
• 2. Understand the past and current therapies of myeloma.
• 3. Have an understanding of the multiple treatment decisions in patients with myeloma.
• 4. Insight to developing therapies for myeloma.
Outline
• Introduction / Statistics
• Presentation / Diagnosis / Staging
• Treatments – Past and Present
• Guidelines / Biomarkers
• Promising Future Treatments
• Conclusions
Trying to figure out Myeloma
Outline
• Introduction / Statistics
• Physiology / Presentation
• Diagnosis / Staging
• Treatments – Past and Present
• Promising Future Treatments
• Conclusions
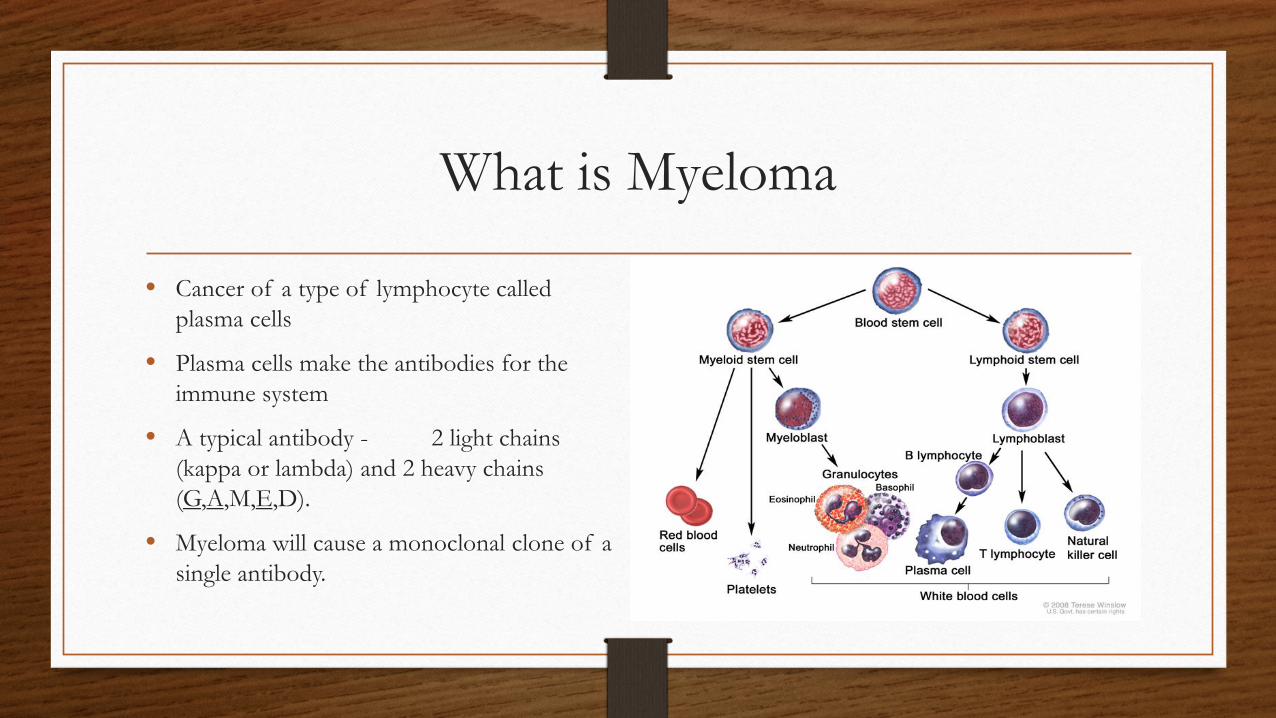
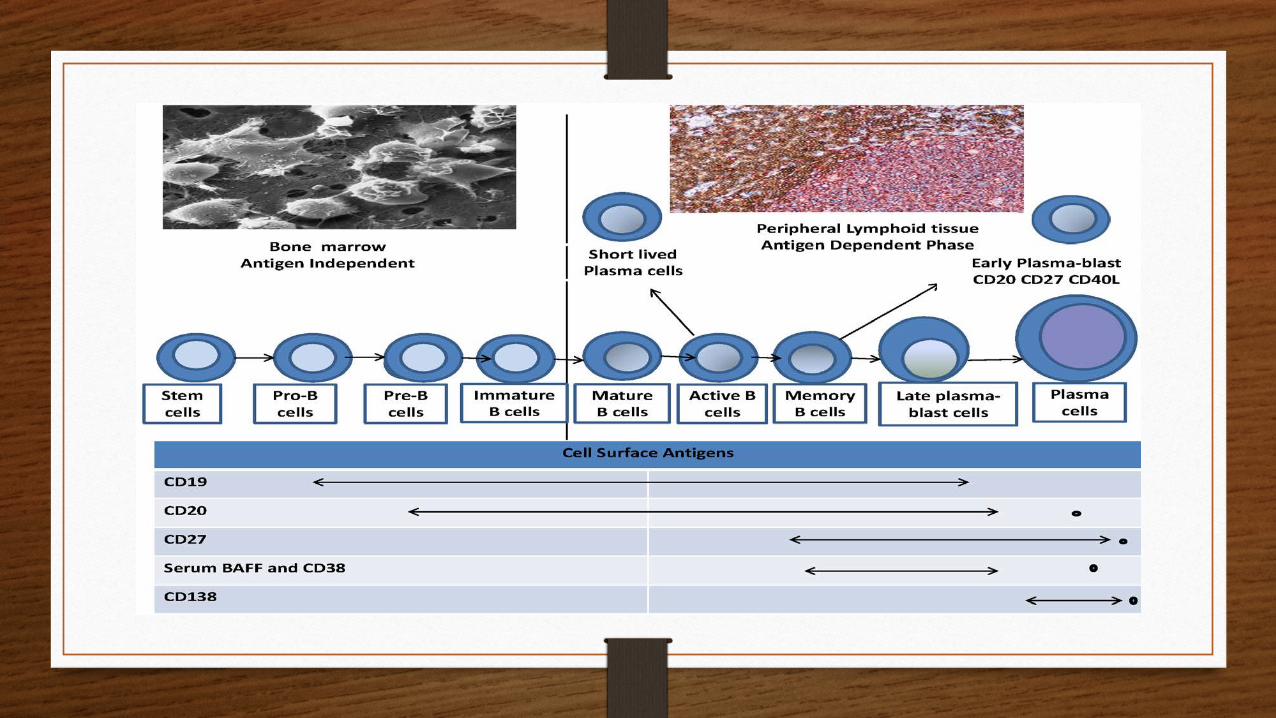
What is Myeloma
• Cancer of a type of lymphocyte called plasma cells
• Plasma cells make the antibodies for the immune system
• A typical antibody - 2 light chains (kappa or lambda) and 2 heavy chains (G,A,M,E,D).
• Myeloma will cause a monoclonal clone of a single antibody.

The Antibodies
Lets start with what we know
• 24,050 new cases in 2014.
• 11,090 estimated deaths from myeloma in 2014 (14th).
• 1.4% of all cancers.
• Incidence is estimated to increase 77% by 2030, due to aging population.
• Myeloma is not curable.
Lets start with what we know
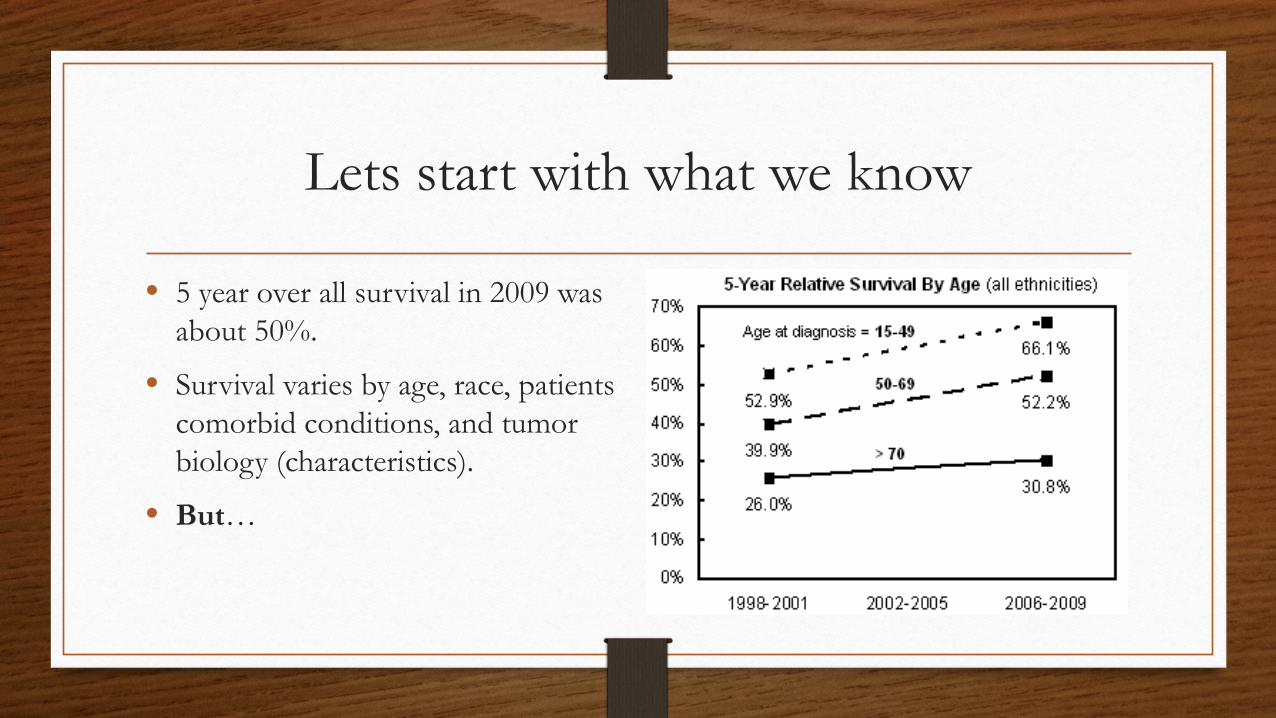
• 5 year over all survival in 2009 was about 50%.
• Survival varies by age, race, patients comorbid conditions, and tumor biology (characteristics).
• But…
The outlook is improving for patients with myeloma
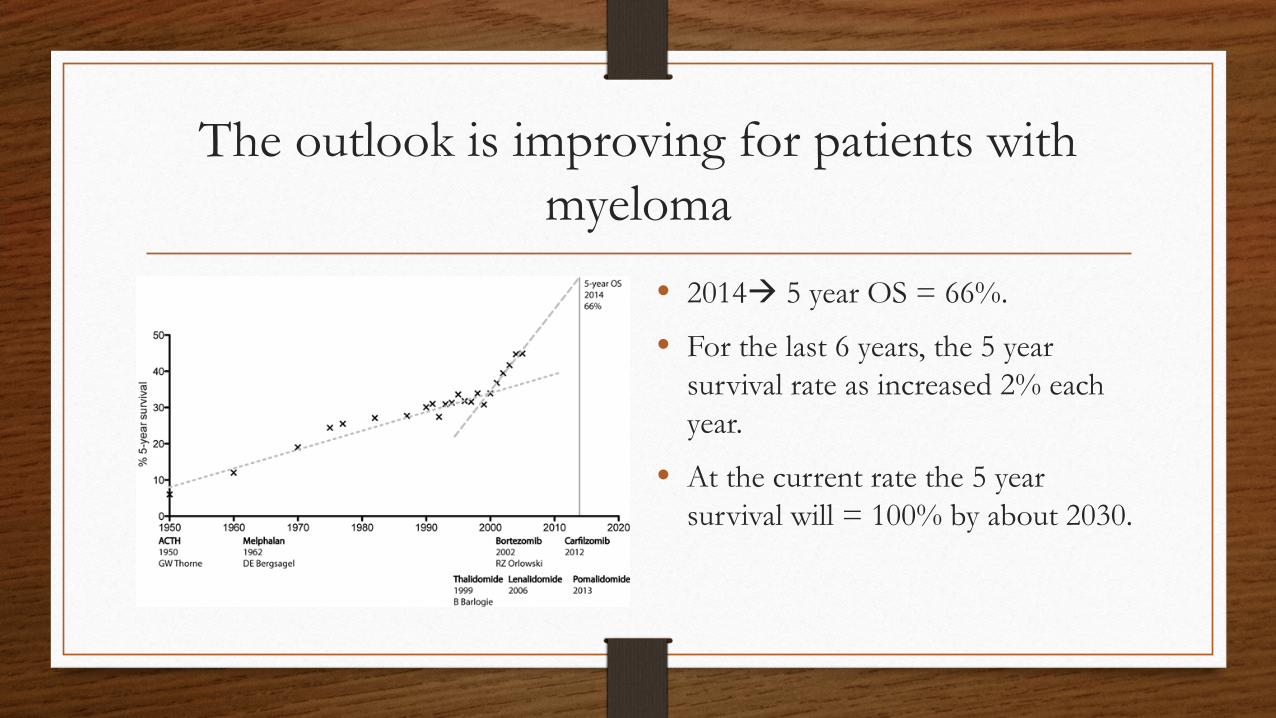
• 2014 5 year OS = 66%.
• For the last 6 years, the 5 year survival rate as increased 2% each year.
• At the current rate the 5 year survival will = 100% by about 2030.

Who gets myeloma
• Elderly: median =70 y/o.
• Overall Woman > men
• But African American men have the highest risk %. (For both diagnosis and death)
• IgG = 52%, IgA = 21%, IgD = 2%, bi-clonal = 2% light chain only = 16%,
From SEER data base.
Outline
• Introduction / Statistics
• Presentation / Diagnosis / Staging
• Treatments – Past and Present
• Guidelines / Biomarkers
• Promising Future Treatments
• Conclusions
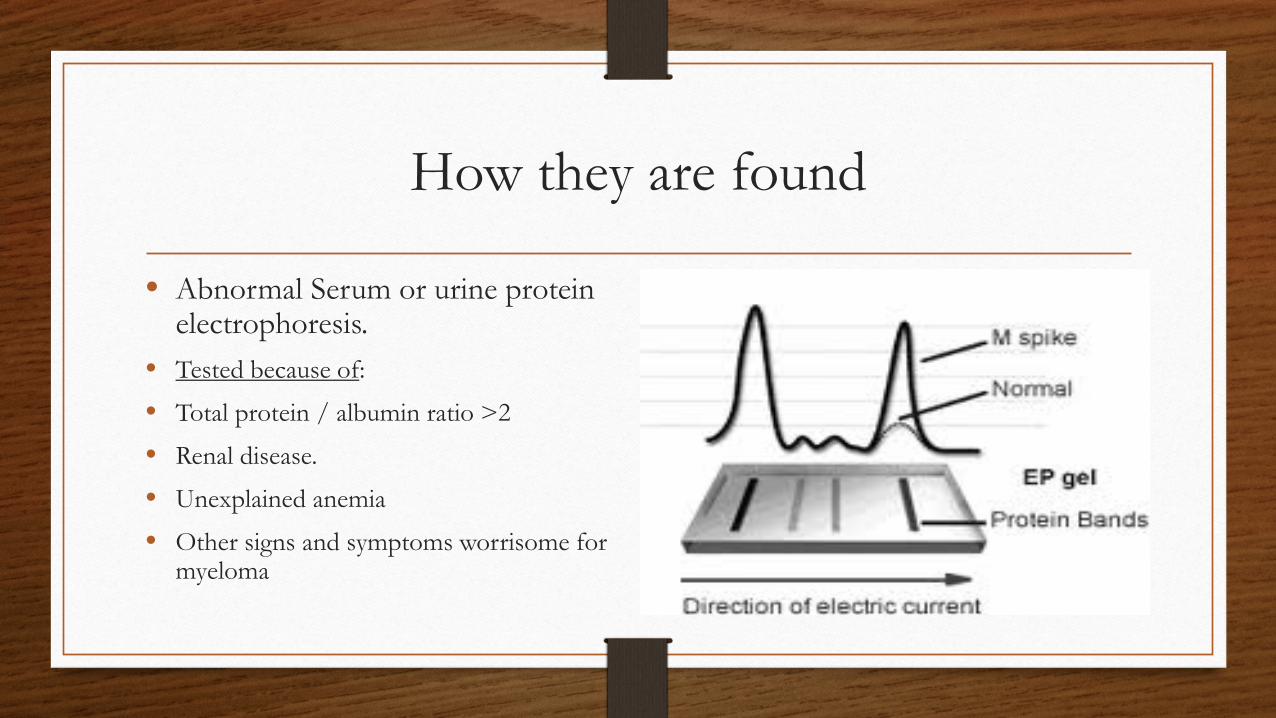
How they are found
• Abnormal Serum or urine protein electrophoresis.
• Tested because of:
• Total protein / albumin ratio >2
• Renal disease.
• Unexplained anemia
• Other signs and symptoms worrisome for myeloma
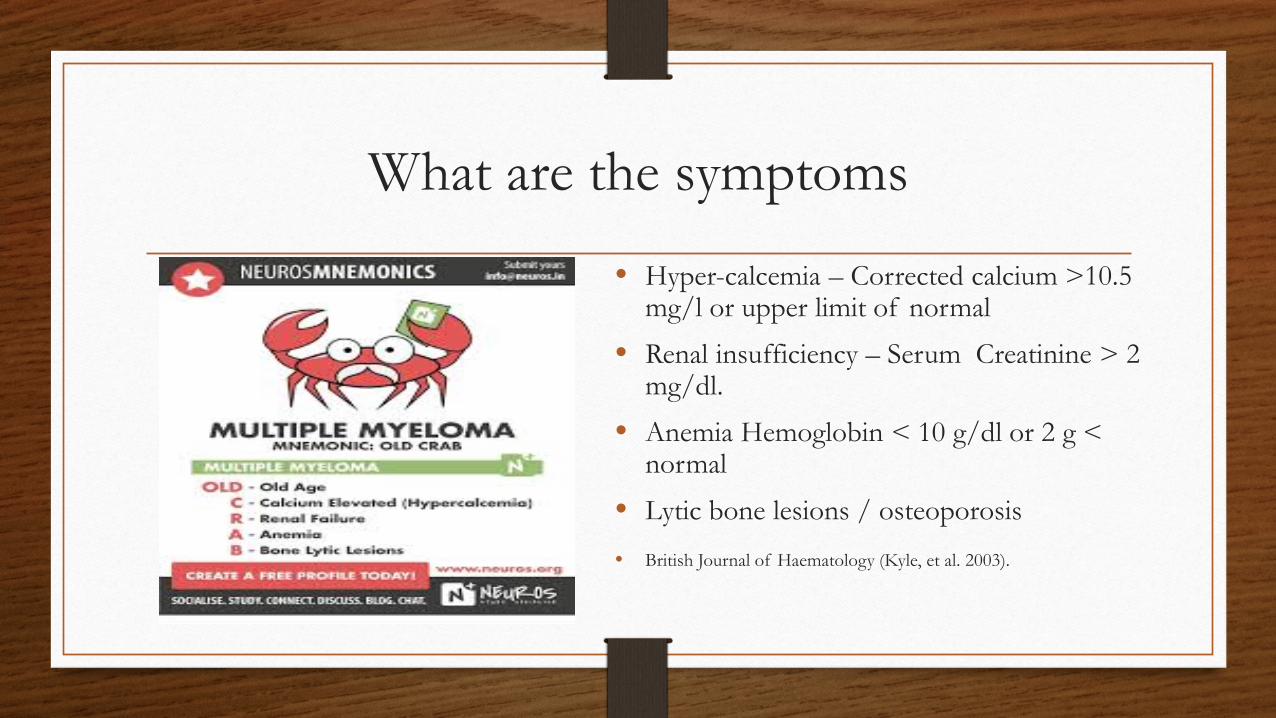
What are the symptoms
• Hyper-calcemia – Corrected calcium >10.5 mg/l or upper limit of normal
• Renal insufficiency – Serum Creatinine > 2 mg/dl.
• Anemia Hemoglobin < 10 g/dl or 2 g < normal
• Lytic bone lesions / osteoporosis
• British Journal of Haematology (Kyle, et al. 2003).
Diagnostic work up
• History and physical • Labs – CBC, Calcium, Creatinine, SPEP, UPEP, Serum free
light chains, B2 macroglobulin, Total protein, Albumin, LDH • Bone marrow biopsy – with Fluorescence in situ hybridization for
chromosomal abnormalities and cytogenetic analysis • Scans – Bone survey (consider MRI or PET)

Staging
• International Staging System • Stage I = B2-macroglobulin <3.5 and
Albumin at least 3.5g/dL.
• Stage II = B2-macroglobulin <3.5 but Albumin < 3.5gm/dL. or B2-macroglobulin 3.5 to </=5.5
• Stage III = B2-macroglobulin >5.5
• Chromosomal abnormalities • High risk = t(14;16) 17p-
t(14;16) • Intermediate = t(4;14) • Standard = trisomies
t(11;14) t(6;14)
Outline
• Introduction / Statistics
• Presentation / Diagnosis / Staging
• Treatments – Past and Present
• Guidelines / Biomarkers
• Promising Future Treatments
• Conclusions
Current Treatment Options Drugs
• Alkylating agents melphalan, cyclophosphamide, bendamustine.
• Steroids dexamethasone, prednisone
• Interferon
• Other chemotherapy cisplatin, liposomal doxorubicin, vincristine, etoposide
• Immune modulators thalidomide, lenalidomide, pomalidomide
• Proteasome inhibitors bortezomib, carfilzomib
• Stem cell transplant
• Histone deacetylase inhibitor vorinostat
Treatment Option Combinations basically any 1, 2, 3, or >3 drug combinations
• RVd
• Cybord
• DCEP
• DT-PACE
• VDT-PACE
• Rd, Thal/dex, Pom/dex
• Vd
• MP
• MPB, MPL, MPT
• VAD, DVD
The main question for induction therapy transplant or no?
Rules of thumb
• 1. Currently if patient is eligible for an auto-transplant they should have one (or at least the discussion).
• 2. Radiation is only used for palliation of symptomatic bone lesions.
• 3. Bisphosphonate agents should be used in patients with known lytic bone lesions and considered in all myeloma patients.
Older Regimens (historical) no transplant
• Melphalan / Prednisone (mp) (i.e. IFM-9906… mp vs. mtp vs. vad…mel100)
• M= 0.25mg/kg D1-4 + P= 2mg/kg D1-4 (q6wk x 12)
• RR= 35%, >/=VGPR= 7%
• PFS= 17.8m, OS= 33m
• Note – all arms lived about 12-14m after progression. • T. Facon. Lancet, Oct.6,2007; vol.370; p.1209-1218.
Induction Older Regimens (historical) transplant eligible
• VAD (data from the HOVON-65 trial) VAD vs. PAD then Auto-T, then Thalidomide 50mg/d vs. (P) 1.3mg/n2 q2wk x 2yrs.
• Vincristine= 0.4mg/m2/d, A= 9mg/m2/d, D= 40mg/d (D1-4, 9-12, 17-20 q4wk) x 3 cycles was the VAD induction.
• 827 patients with follow up = 41m.
• RR= 54% with >/= nCR= 7% (induction part only included)
• PFS= 28m. (all), if cr.>2 PFS= 13m. • P. Somneveld. JCO. 8/20/2012; v.30(24) p.2946-2955
Newer Single Agents Immune Modulator Drugs (IMID’s)
• Rd vs. RD (E4A03) • 445pts. Phase III, (median age = 65 y/o), Follow up = 17m. • Dexamethasone 40mg. weekly vs. D1-4,9-12,17-20 q4wk. Both arms received
Lenalidomide 25mg. D1-21 q4wk. • RR= 68%(d) vs. 79%(D), >/=VGPR = 24%(d) vs. 42%(D). • 1yr. OS = 96%(d) vs. 87%(D). • 3yr. OS = 74%(d) vs. 75%(D) (all patients crossed over), 3yr. OS if Auto-T = 93%. • Rajkumar SV, et al. Lancet Oncol. 2010;11:29-37
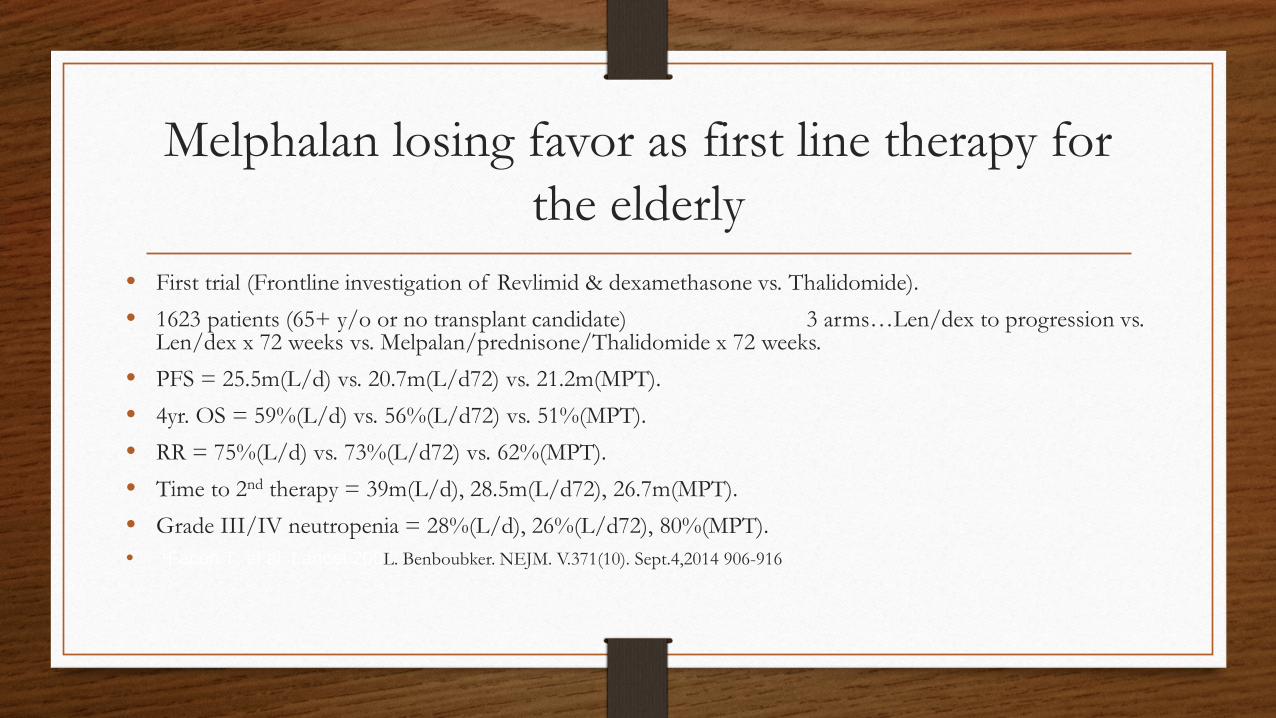
Melphalan losing favor as first line therapy for the elderly
• First trial (Frontline investigation of Revlimid & dexamethasone vs. Thalidomide). • 1623 patients (65+ y/o or no transplant candidate) 3 arms…Len/dex to progression vs.
Len/dex x 72 weeks vs. Melpalan/prednisone/Thalidomide x 72 weeks. • PFS = 25.5m(L/d) vs. 20.7m(L/d72) vs. 21.2m(MPT). • 4yr. OS = 59%(L/d) vs. 56%(L/d72) vs. 51%(MPT). • RR = 75%(L/d) vs. 73%(L/d72) vs. 62%(MPT). • Time to 2nd therapy = 39m(L/d), 28.5m(L/d72), 26.7m(MPT). • Grade III/IV neutropenia = 28%(L/d), 26%(L/d72), 80%(MPT). • 1Facon T, et al. Lancet 200L. Benboubker. NEJM. V.371(10). Sept.4,2014 906-916
RA
ND
OM
IZA
TIO
N 1
:1:1
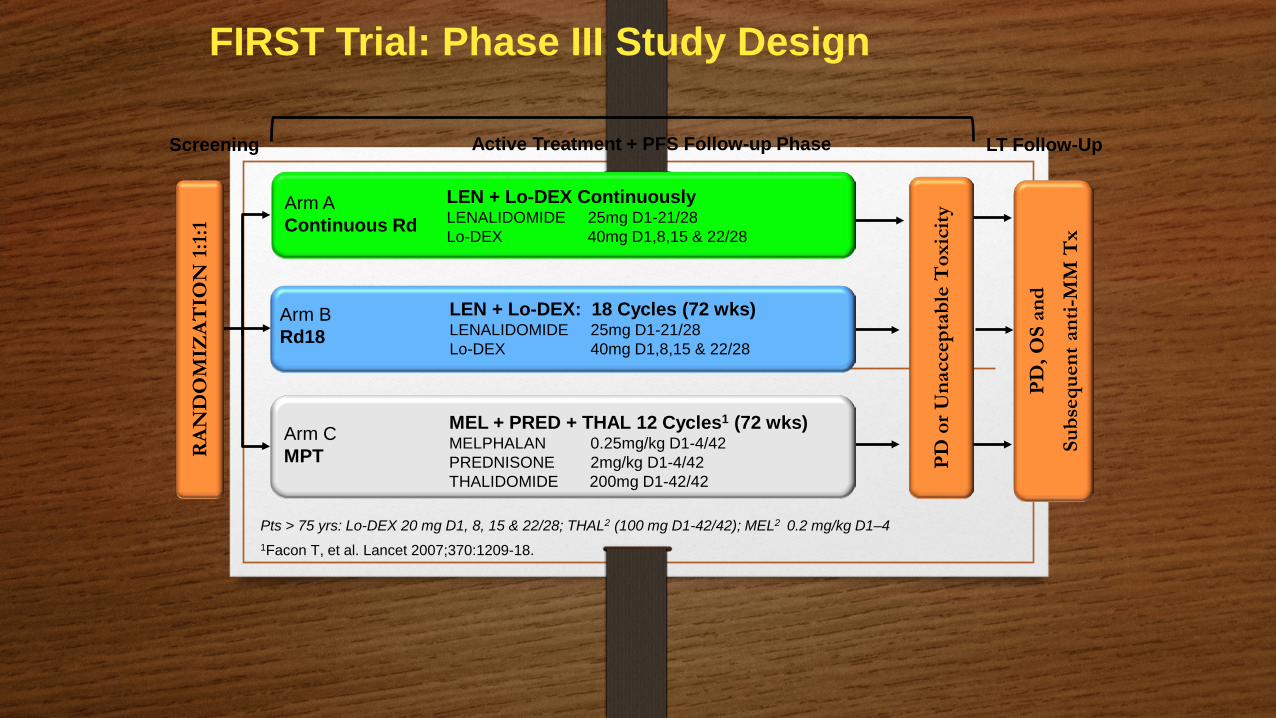
Arm B Rd18
Arm C MPT
LEN + Lo-DEX: 18 Cycles (72 wks) LENALIDOMIDE 25mg D1-21/28 Lo-DEX 40mg D1,8,15 & 22/28
MEL + PRED + THAL 12 Cycles1 (72 wks) MELPHALAN 0.25mg/kg D1-4/42 PREDNISONE 2mg/kg D1-4/42 THALIDOMIDE 200mg D1-42/42
PD, O
S an
d
Subs
eque
nt a
nti-M
M T
x
PD o
r Una
ccep
tabl
e T
oxic
ity
Active Treatment + PFS Follow-up Phase Screening LT Follow-Up
Pts > 75 yrs: Lo-DEX 20 mg D1, 8, 15 & 22/28; THAL2 (100 mg D1-42/42); MEL2 0.2 mg/kg D1–4 1Facon T, et al. Lancet 2007;370:1209-18.
FIRST Trial: Phase III Study Design
LEN + Lo-DEX Continuously LENALIDOMIDE 25mg D1-21/28 Lo-DEX 40mg D1,8,15 & 22/28
Arm A Continuous Rd
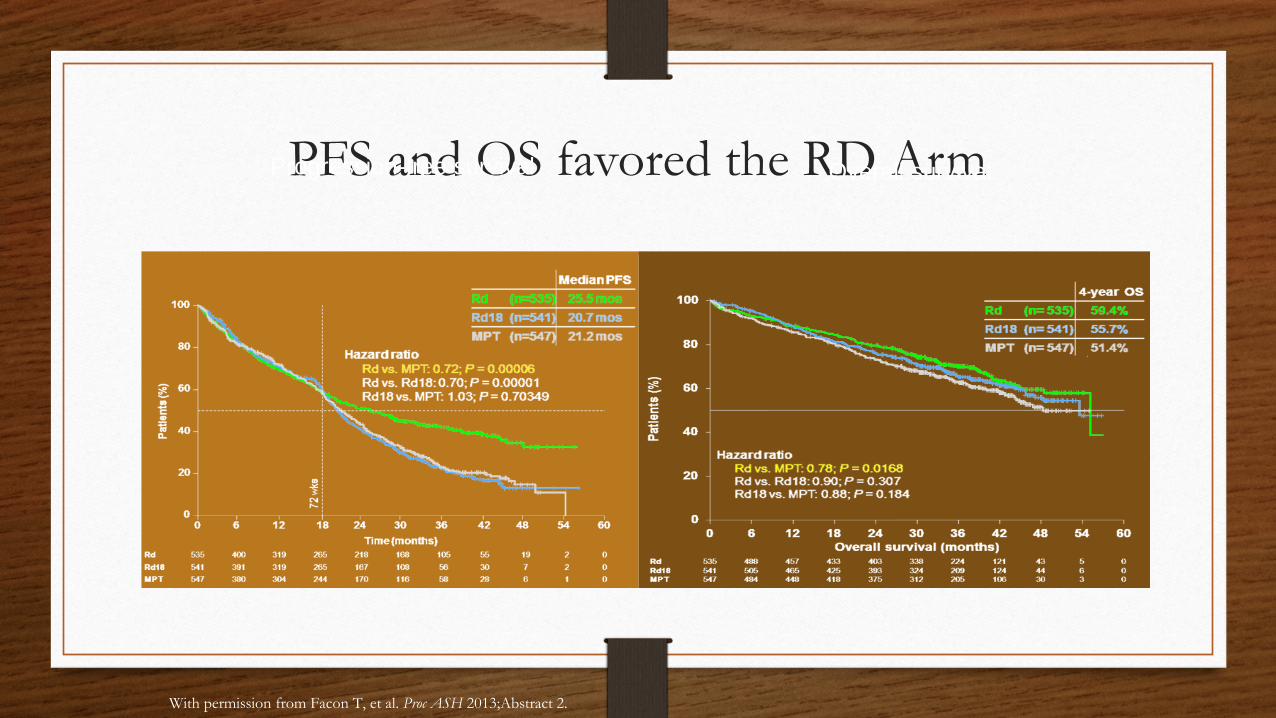
PFS and OS favored the RD Arm Progression-free survival Overall survival
With permission from Facon T, et al. Proc ASH 2013;Abstract 2.
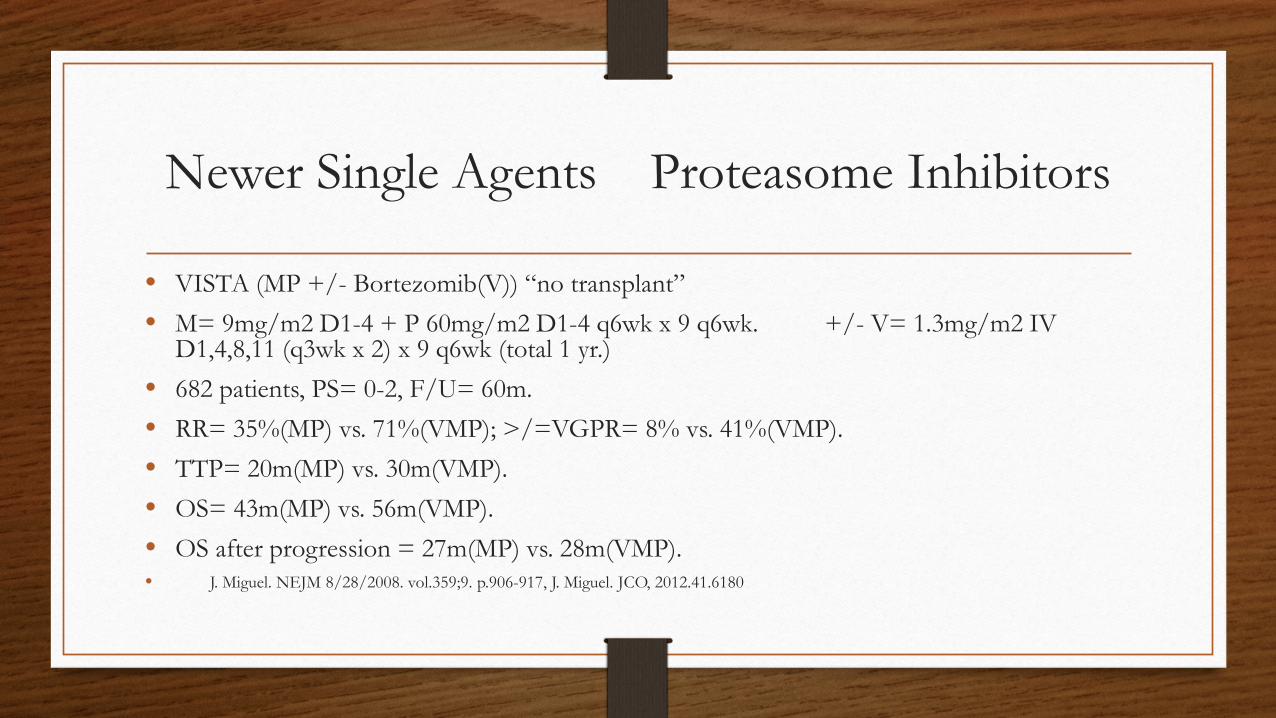
Newer Single Agents Proteasome Inhibitors
• VISTA (MP +/- Bortezomib(V)) “no transplant” • M= 9mg/m2 D1-4 + P 60mg/m2 D1-4 q6wk x 9 q6wk. +/- V= 1.3mg/m2 IV
D1,4,8,11 (q3wk x 2) x 9 q6wk (total 1 yr.) • 682 patients, PS= 0-2, F/U= 60m. • RR= 35%(MP) vs. 71%(VMP); >/=VGPR= 8% vs. 41%(VMP). • TTP= 20m(MP) vs. 30m(VMP). • OS= 43m(MP) vs. 56m(VMP). • OS after progression = 27m(MP) vs. 28m(VMP). • J. Miguel. NEJM 8/28/2008. vol.359;9. p.906-917, J. Miguel. JCO, 2012.41.6180
RVD
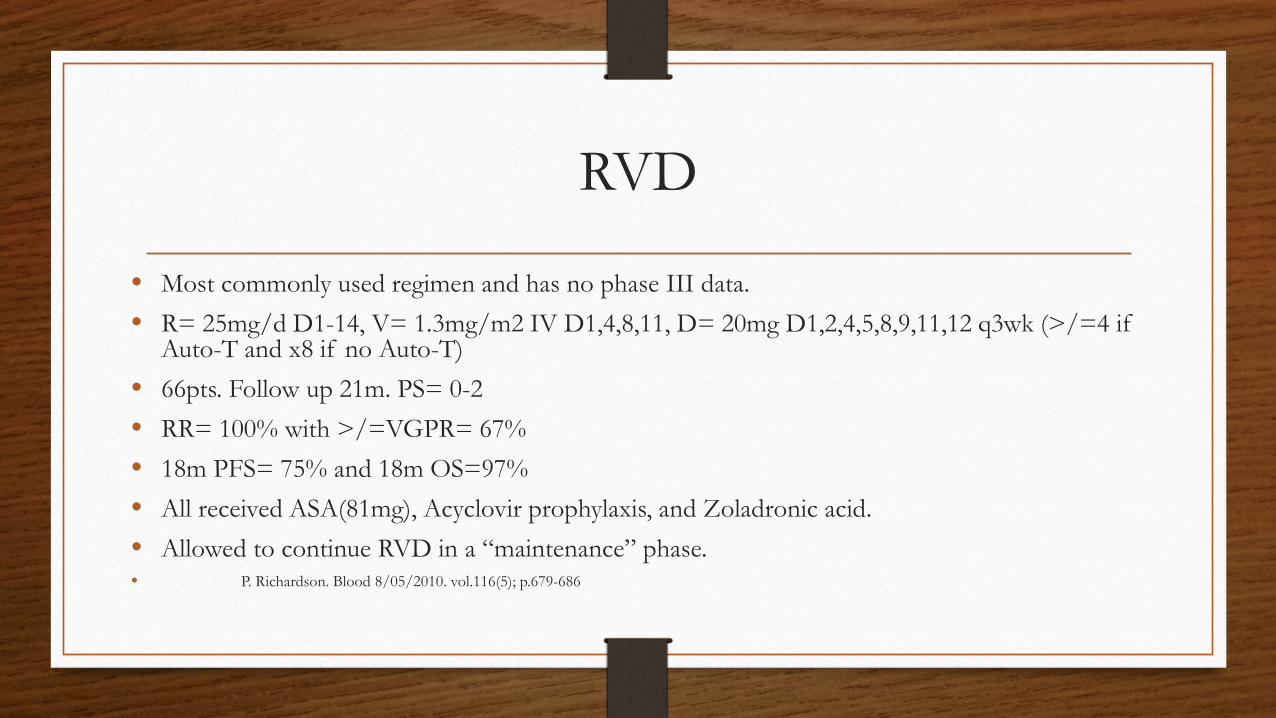
• Most commonly used regimen and has no phase III data. • R= 25mg/d D1-14, V= 1.3mg/m2 IV D1,4,8,11, D= 20mg D1,2,4,5,8,9,11,12 q3wk (>/=4 if
Auto-T and x8 if no Auto-T) • 66pts. Follow up 21m. PS= 0-2 • RR= 100% with >/=VGPR= 67% • 18m PFS= 75% and 18m OS=97% • All received ASA(81mg), Acyclovir prophylaxis, and Zoladronic acid. • Allowed to continue RVD in a “maintenance” phase. • P. Richardson. Blood 8/05/2010. vol.116(5); p.679-686

Evolution trials
• Also large phase II study. • 4 arms – RVD, R-CyborD, CyborD, (mod)CyborD. • D= 40mg/wk., C= 500mg/m2 D1,8 or D1.8,15(mod) q3wk. R and V same dosing as RVD. • 145pts. Follow up= 20m. • RR= 85-100% with >/= VGPR= 51-58% • 1yr. PFS= 83-100% • 1yr. OS= 93%(4 drug) & 100%(all other regimens) • S. Kumar; Blood. vol.119(19); p.4375-94
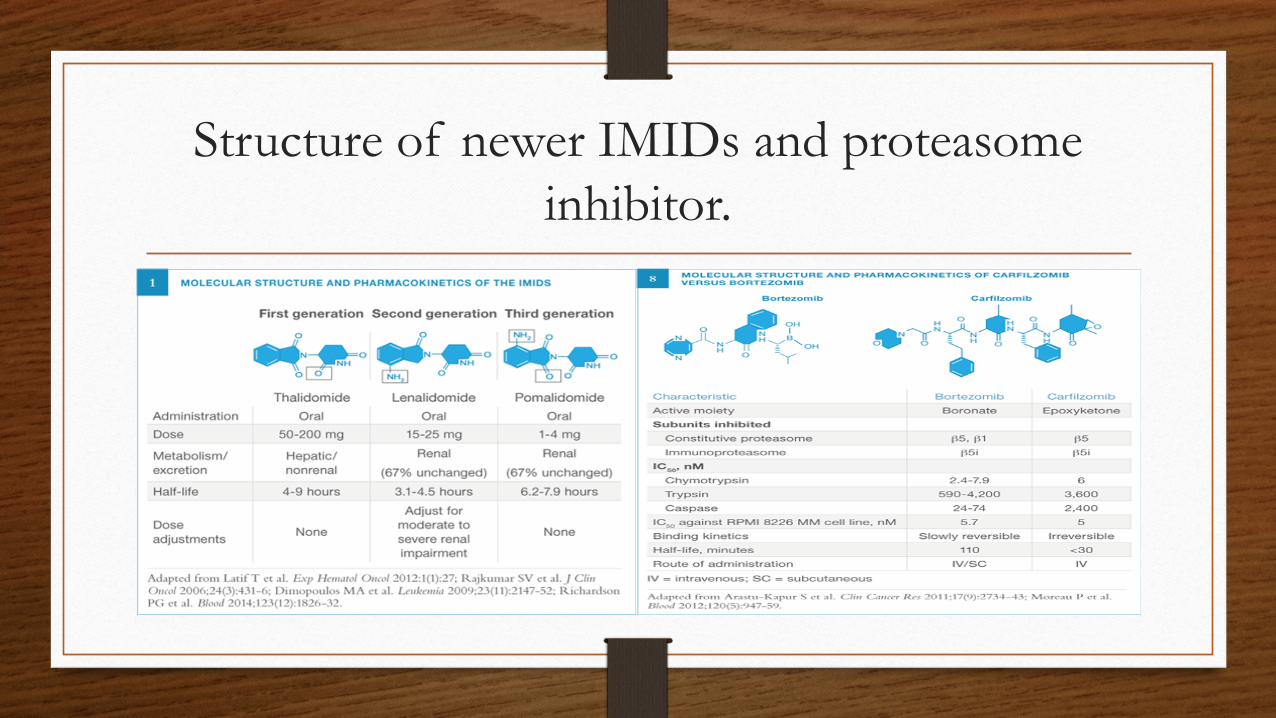
Structure of newer IMIDs and proteasome inhibitor.
How long do we go? Maintenance or Consolidation
Maintenance Lenalidomide (no transplant)
• MM-015 • MPR-R vs. MPR vs. MP • R= 10mg/d D1-21 q4wk. (until progression) • 300pts with Follow up 30m. • RR= 77%(R) vs, 50% with >/= VGPR= 33%(R) vs. 12%. • PFS= 31m(R) vs. 13m (65-75 y/o greatest benefit) • 3yr. OS= 70% vs. 66% • 2nd malignancies 7% vs. 3% • A. Palumbo. NEJM. Vol.366(19). P1759-68.
Maintenance Lenalidomide (with transplant)
• CALGB100104 • 460pts. Median age=59, PS=0-1, Follow up= 34m. • Any induction with at least stable disease after Auto-T • Lenalidomide (5-15mg/d) • TTP= 46m(L) vs. 27m. (HR=0.48) • 3yr. OS = 88%(L) vs. 80% (HR=0.62) • 2nd malignancies 8%(L) vs. 3% • K. Anderson. NEJM (5/10/2012); VOL.366(19) P.1770-80
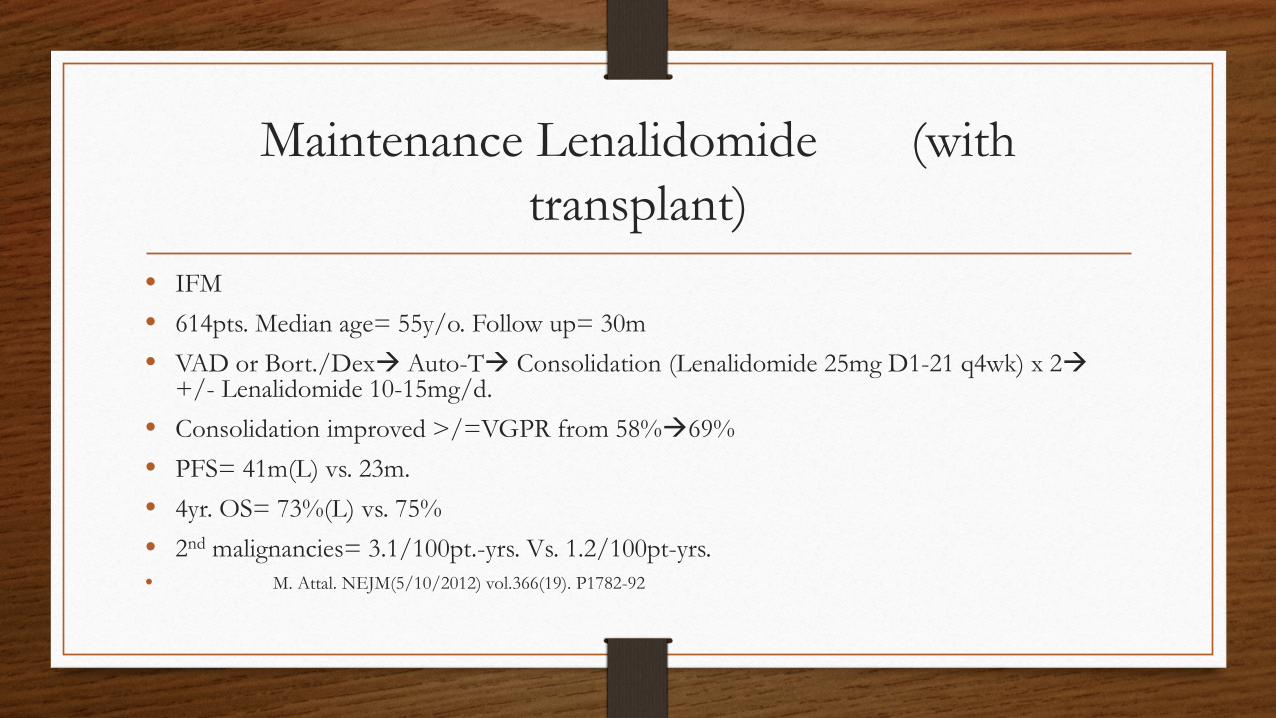
Maintenance Lenalidomide (with transplant)
• IFM • 614pts. Median age= 55y/o. Follow up= 30m • VAD or Bort./Dex Auto-T Consolidation (Lenalidomide 25mg D1-21 q4wk) x 2
+/- Lenalidomide 10-15mg/d. • Consolidation improved >/=VGPR from 58%69% • PFS= 41m(L) vs. 23m. • 4yr. OS= 73%(L) vs. 75% • 2nd malignancies= 3.1/100pt.-yrs. Vs. 1.2/100pt-yrs. • M. Attal. NEJM(5/10/2012) vol.366(19). P1782-92
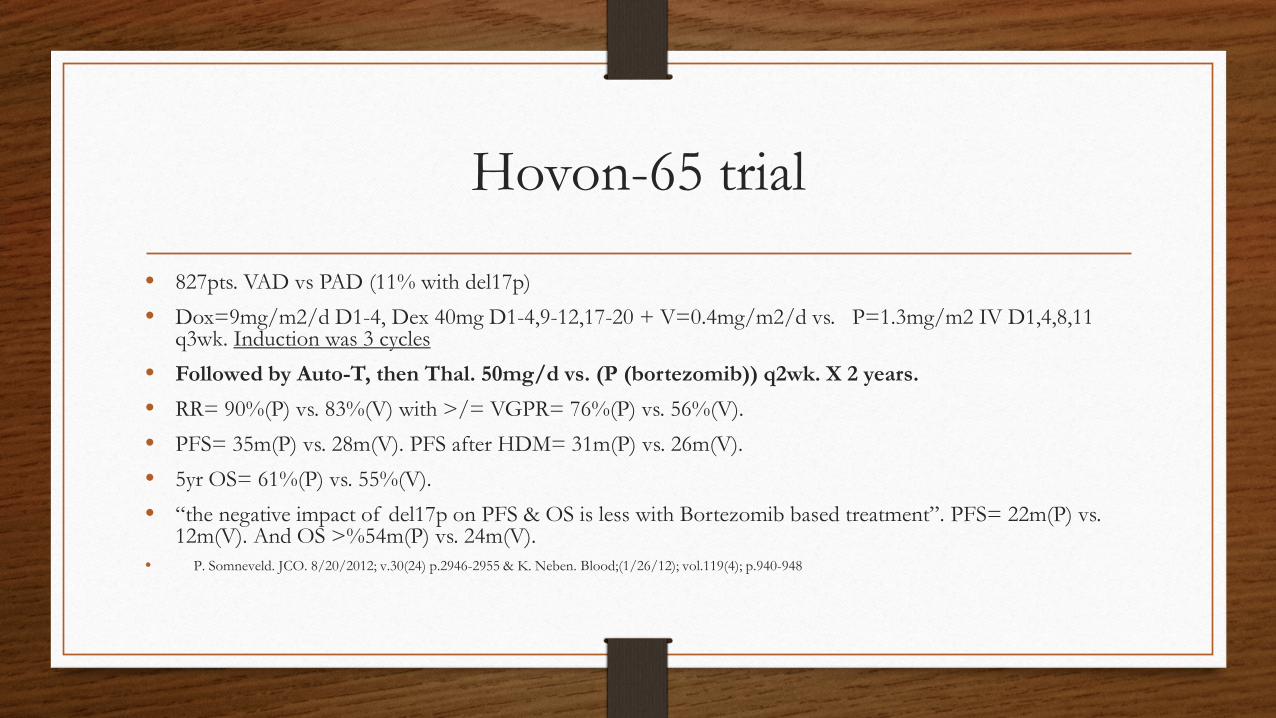
Hovon-65 trial
• 827pts. VAD vs PAD (11% with del17p) • Dox=9mg/m2/d D1-4, Dex 40mg D1-4,9-12,17-20 + V=0.4mg/m2/d vs. P=1.3mg/m2 IV D1,4,8,11
q3wk. Induction was 3 cycles • Followed by Auto-T, then Thal. 50mg/d vs. (P (bortezomib)) q2wk. X 2 years. • RR= 90%(P) vs. 83%(V) with >/= VGPR= 76%(P) vs. 56%(V). • PFS= 35m(P) vs. 28m(V). PFS after HDM= 31m(P) vs. 26m(V). • 5yr OS= 61%(P) vs. 55%(V). • “the negative impact of del17p on PFS & OS is less with Bortezomib based treatment”. PFS= 22m(P) vs.
12m(V). And OS >%54m(P) vs. 24m(V). • P. Somneveld. JCO. 8/20/2012; v.30(24) p.2946-2955 & K. Neben. Blood;(1/26/12); vol.119(4); p.940-948
Outline
• Introduction / Statistics
• Presentation / Diagnosis / Staging
• Treatments – Past and Present
• Guidelines / Biomarkers
• Promising Future Treatments
• Conclusions
Rules to remember
• IMID’s • 1. Need thrombi prophylaxis. • 2. Watch blood counts. • 3. IMID + Melphalan increase risk of
second malignancies. (First trial) • 4. Lenalidomide is excreted mainly via
urine – dose adjustment in renal disease.
• Proteasome inhibitors • 1. Shingle prophylaxis. • 2. Monitor platelet counts. • 3. Monitor peripheral neuropathy • 4. Standard of care in high risk
myeloma initial therapy.
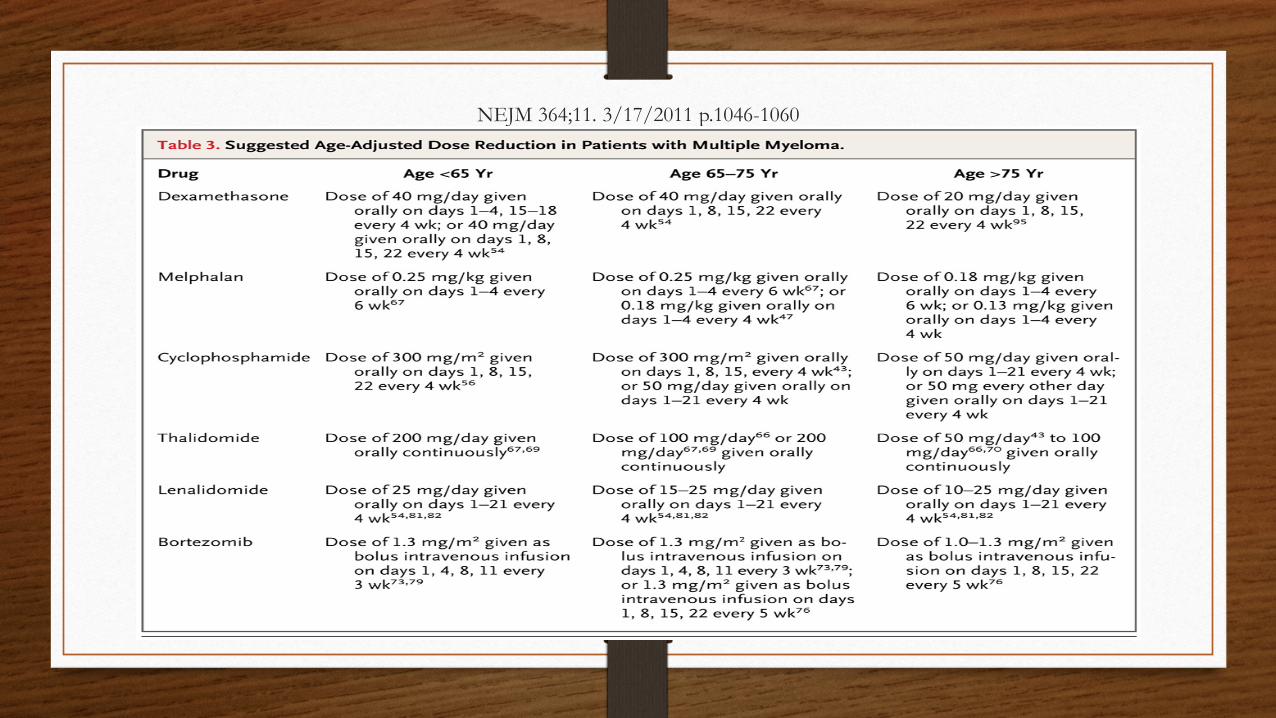
NEJM 364;11. 3/17/2011 p.1046-1060
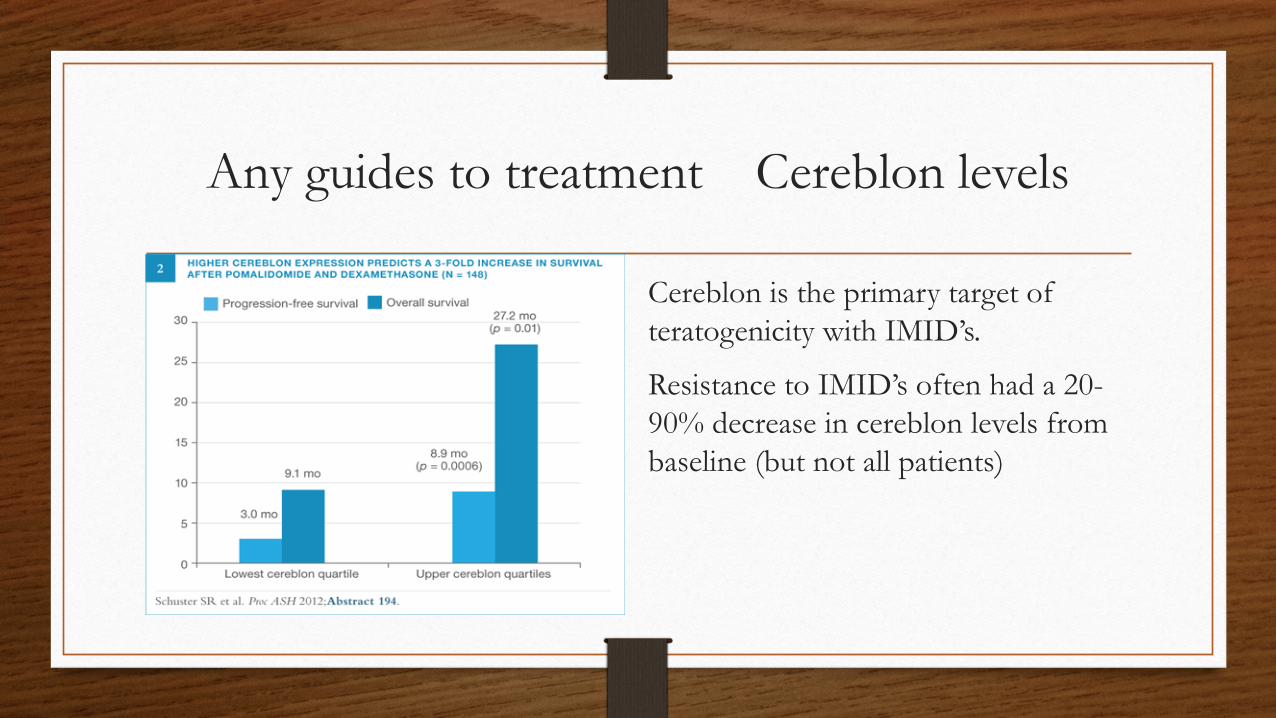
Any guides to treatment Cereblon levels
Cereblon is the primary target of teratogenicity with IMID’s.
Resistance to IMID’s often had a 20-90% decrease in cereblon levels from baseline (but not all patients)
Any guides to treatment NRAS mutation
• RAS family (KRAS, HRAS, NRAS). Mutations are mutually exclusive. • In most tumors one subtype is predominately mutated In solid cancers usually KRAS, in
Hem cancers usually NRAS • Myeloma has about 20% KRAS and 20% NRAS mutations • Tissue from 133pts in Bortezomib trials (APEX & 2 phase II) • 71/133 had mutations (20% had NRAS mutation) • RR to Bortezomib 7%(NRAS) vs. 53% and shorter TTP • No OS difference and NRAS mutation did not effect steroid activity. • G. Mulligan Blood (1/30/14). Vol.123(5); p632-638.
Is there a subtype where standard treatment is not good enough?
• Patients with the combination of: • 1. Stage III • 2. t(4;14) or 17p- • 3. High LDH • Accounts for 5-8% of myeloma patients. • 50% 2yr. failure rate of standard induction and auto-T. • P. Moreau. JCO. V.32(20); 7/10/14. p.2173-2180
Outline
• Introduction / Statistics
• Presentation / Diagnosis / Staging
• Treatments – Past and Present
• Guidelines / Biomarkers
• Promising Future Treatments
• Conclusions
Antibodies
• Anti-CS1(Elotuzumab) + Lenalidomide / Dexamethasone • E= 20mg/kg IV Elotuzumab weekly + D= 40mg/wk. + L= 25mg/d D1-21 q4wk.
• Single agent Elotuzumab has no activity.
• Phase I; 29pts. Age= 60. Follow up= 16.4m.
• Median 3 prior regimens and >5yrs.from diagnosis.
• Combination RR=82% and TTP= not reached. • S. Lonial JCO. Vol.30(16); 6/1/2012.
Antibodies
• Anti-CD38 Daratumumab. • Novel, high-affinity, human mAb against a unique CD38 epitope induced potent
Ab-dependent cellular cytotoxicity. • A response was seen 67% patients receiving more than 4 mg/kg. (42%= PR and
25%= minimal) • Approximately 80% of patients were double-refractory. • 1st monoclonal antibody to receive breakthrough therapy designation by the FDA. • 18th Congress of the European Hematology Association (EHA): Abstract S576. Presented June 15, 2013
Histone deacetylase inhibitors
• Panorama-1: Bortezomib 1.3mg./m2 IV D1,4,8,11 Dexamethasone 20mg. PO D1,2,4,5,8,9,11,12 +/- Panobinostat 20mg. PO 3x/week. Q3 week x 8
• Relapsed or refractory disease (>1/2 had >2 prior regimens).
• 768 patients
• PFS = 12m (pan) vs. 8m … DOR = 13.1m (pan) vs. 10.9m.
• RR = 61% (pan) vs. 55% … nCR/CR = 28% (pan) vs. 16%
• Toxicity = thrombocytopenia, neutropenia, diarrhea
Rationale for BTK inhibitors
• B cell-activating factor (BAFF) of the TNF family (BAFF-R) is coupled to the NF-κB pathway by Bruton’s tyrosine kinase (BTK).
• BAFF-induced signaling to NF-κB via BTK serves to promote B-cell survival.
• Proteasome inhibitors block NF-kB activity via blocking destruction of the inhibitor protein of NF-kB (IK-B(alpha)).
• S. Rushworth. Abstr.181P Queen Elizabeth II Conference Centre London BPS Meeting 2012.

Activation of Bruton’s Tyrosine Kinase (BTK) pathway
Ibutinib
• Bruton’s tyrosine kinase inhibitor. • Potently enhances Bortezomib and Lenalidomide activities through NF-kB. • Approved in CLL and Mantle cell. • Likely approval in Waldenstrom’s. • Ibutinib blocks phosphorylation of serine-536 resulting in down regulation of BCL-
xL, FLIP, Survivin, and increases caspace-mediated apoptosis. • S. Rushworth. Cellular Signaling. Vol.25(1); 1/2013. p.106-112.
Outline
• Introduction / Statistics
• Presentation / Diagnosis / Staging
• Treatments – Past and Present
• Guidelines / Biomarkers
• Promising Future Treatments
• Conclusions
Conclusion
• Myeloma is still a disease with no cure in 2014. • New medications and how to use those medications most effectively is still a
work in progress. • We are making strides in the management of myeloma. • Soon we may turn myeloma into a chronic disease and away from being a
terminal disease. • Thank You.




![osteoporosispatients2015 [Read-Only] · • SPEP/UPEP • TTGIGA (celiac) • Phosphorus • Magnesium • PTH. 6/11/2015 7 Who do we treat? 6/11/2015 8. 6/11/2015 9 FRAX. 6/11/2015](https://static.fdocuments.net/doc/165x107/5aec58b47f8b9a90318e2a89/osteoporosispatients2015-read-only-spepupep-ttgiga-celiac-phosphorus.jpg)













