
Multiple atraumatic osteoporotic vertebral fractures: Unusual cause of pain in adult
6
Multiple atraumatic osteoporotic vertebral fractures: Unusual cause of pain in adult
-
Upload
apollo-hospitals -
Category
Health & Medicine
-
view
25 -
download
2
Transcript of Multiple atraumatic osteoporotic vertebral fractures: Unusual cause of pain in adult
Multiple atraumatic osteoporotic vertebral fractures: Unusual cause of pain in adult
Case Report
Multiple atraumatic osteoporotic vertebral fractures:Unusual cause of pain in adult
Daniel Demesugh Mue, Raju Vaishya *, Amit Kumar Agarwal, Vipul Vijay
Department of Orthopaedics and Joint Replacement Surgery, Indraprastha Apollo Hospitals, Sarita Vihar,New Delhi 110076, India
1. Introduction
Osteoporosis is a progressive metabolic bone disease charac-terized by decrease in bone mineral density and deteriorationin bone structure, leading to an increased risk of fracture.1 Itmay be classified as primary type 1 (postmenopausalosteoporosis), primary type 2 (senile osteoporosis), andsecondary osteoporosis, which accounts for <5% of theosteoporosis cases.2 Secondary osteoporosis may arise atany age and affects both men and women equally; it resultsfrom chronic predisposing medical problems, like hyperpara-thyroidism, renal osteodystrophy, or prolonged use of med-ications including glucocorticoids, thyroxine, etc.3
Osteoporotic vertebral fracture is common in the elderlyand postmenopausal women, but is very uncommon inyoung adults.4 This poses a diagnostic challenge, as only
about one-third are recognized when they become symp-tomatic and they usually present with acute back pain, orwith loss of height and increasing kyphosis. Up to 30% ofwomen and 55% of men with symptomatic vertebral crushfractures have underlying secondary osteoporosis.4 Thesequel to multiple atraumatic osteoporotic vertebral frac-tures may be devastating, especially in the young. Up to 20%patients with an incident vertebral fracture experience afurther vertebral fracture within one year.4,5
We report a case of multiple atraumatic osteoporoticvertebral fractures following prolonged steroid therapy, where11 vertebral bodies were found collapsed in the dorsolumbarregion. This condition is uncommon in young adults, andrequires the clinician to maintain a high index of suspicion inpatientswith back pain, who are on prolonged steroid therapy,to make an early diagnosis and start the treatment, in order tominimize morbidity.
a p o l l o m e d i c i n e 1 2 ( 2 0 1 5 ) 1 4 4 – 1 4 7
a r t i c l e i n f o
Article history:
Received 6 April 2015
Accepted 1 May 2015
Available online 6 June 2015
Keywords:
Osteoporosis
Fractures
Vertebral
Corticosteroid
a b s t r a c t
Secondary osteoporosismay not be detected early, and thus the condition remains clinically
silent until the patient presents with multiple atraumatic compression fractures. It is
devastating for a young patient to develop multiple vertebral fractures in view of the
associatedmorbidity andmortality. To decrease the risk of additional fractures and preserve
the quality of life in these patients, interventions should be initiated early. Hence, it is
important to consider multiple osteoporotic vertebral fractures as a complication in any
patient on prolonged steroid therapy.
# 2015 Indraprastha Medical Corporation Ltd. Published by Elsevier B.V. All rights
reserved.
* Corresponding author at: Sr Consultant Orthopaedic Surgeon, Indraprastha Apollo Hospitals, New Delhi 110076, India.Mobile: +91 9810123331.
E-mail address: [email protected] (R. Vaishya).
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.elsevier.com/locate/apme
http://dx.doi.org/10.1016/j.apme.2015.05.0060976-0016/# 2015 Indraprastha Medical Corporation Ltd. Published by Elsevier B.V. All rights reserved.
2. Case report
A 32-year-old male patient presented with an 18-monthhistory of non-radiating back pain, which progressivelyworsened over a period of time. His pain got aggravated byactivity and was relieved by taking rest and using analgesics.The pain was severe enough to interfere with his activities ofdaily living and necessitated the use of a walking stick forambulation. He has been on steroid therapy for the last 6months for his back pain. There was no history of any trauma.
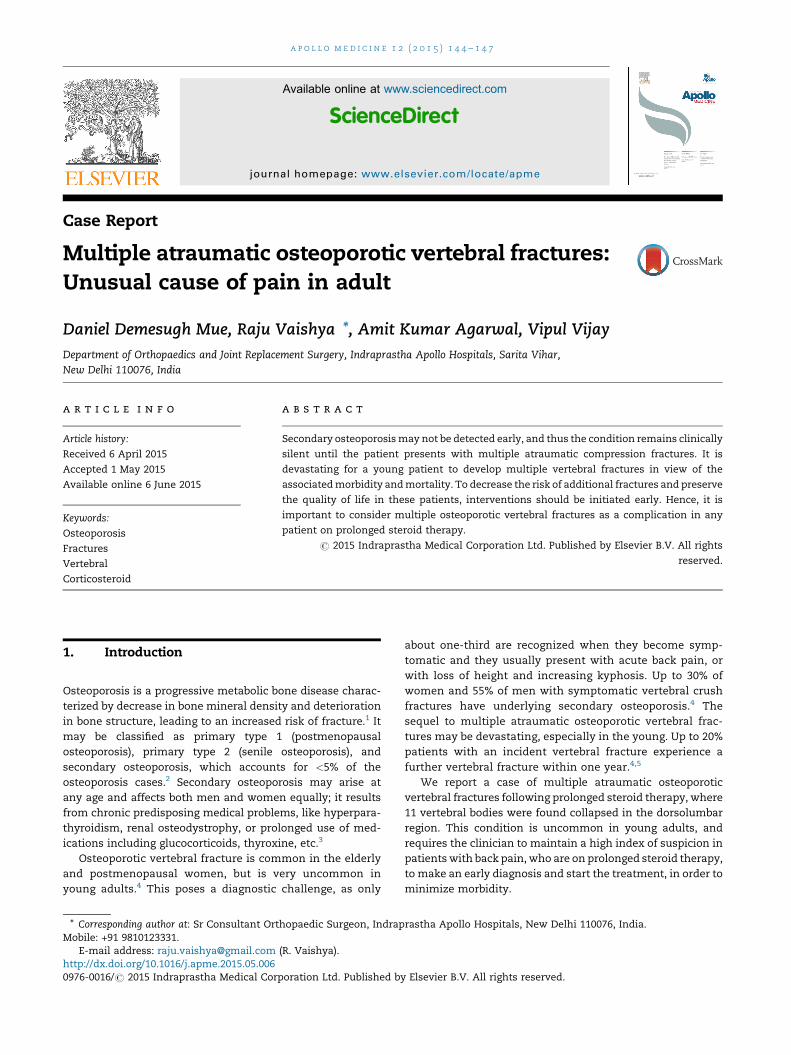
Physical examination revealed a morbidly obese youngmale with Body Mass Index (BMI) of 40. He had cushingoidfacies (Fig. 1), withmultiple striae all over the abdomenand theaxillary folds (Fig. 2). The back revealed a buffalo hump, with[(Fig._1)TD$FIG]
Fig. 1 – Typical cushingoid facies of the patient.[(Fig._2)TD$FIG]
Fig. 2 – Multiple striae over the anterior abdominal wall.
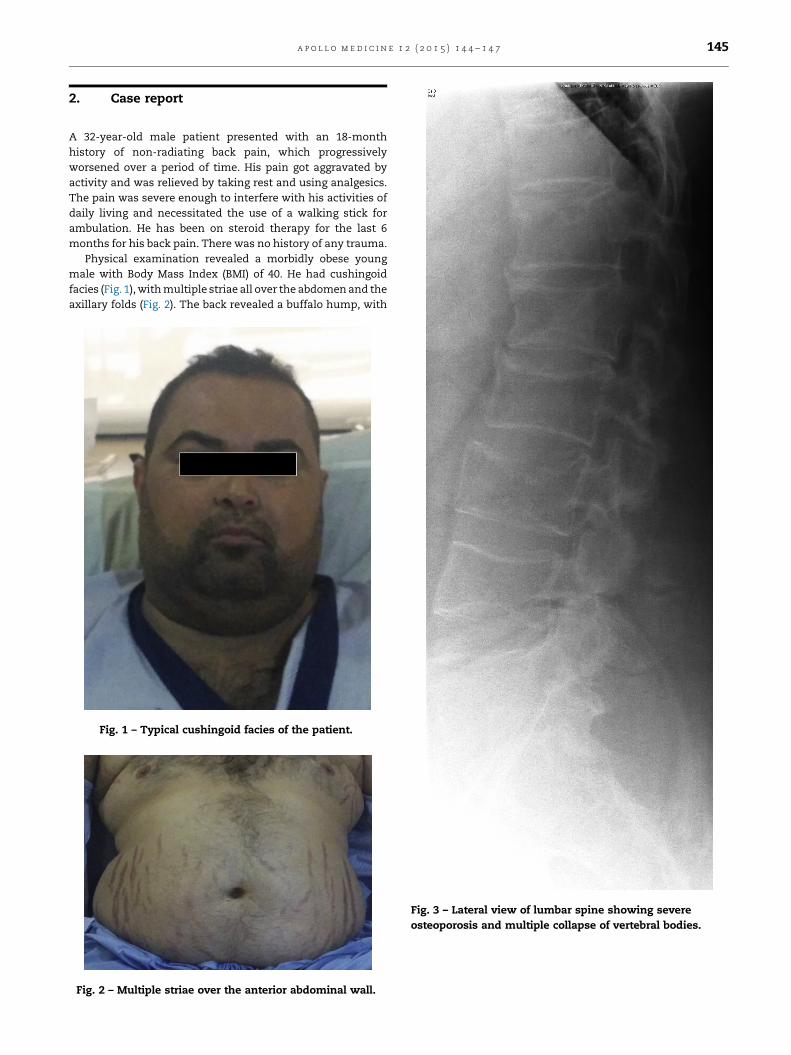
[(Fig._3)TD$FIG]
Fig. 3 – Lateral view of lumbar spine showing severeosteoporosis and multiple collapse of vertebral bodies.
a p o l l o m e d i c i n e 1 2 ( 2 0 1 5 ) 1 4 4 – 1 4 7 145
multiple tender areas over the lower thoracic and lumbarspine. Straight leg raising test was negative. There was noneurological deficit in the lower limbs. Other physicalexamination findings were unremarkable.
Plain radiographs of lumbar spine revealed anterior wedgecollapse, loss of vertebral height, and biconcave-shaped bodies
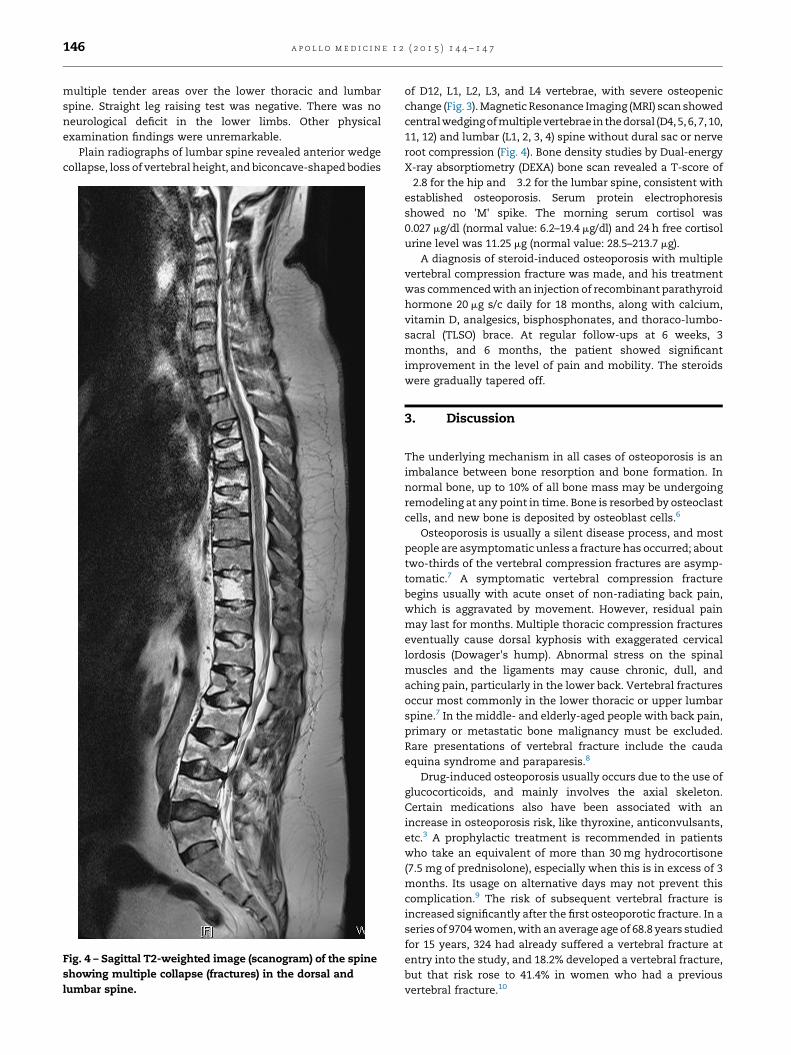
of D12, L1, L2, L3, and L4 vertebrae, with severe osteopenicchange (Fig. 3).Magnetic Resonance Imaging (MRI) scan showedcentralwedgingofmultiplevertebrae in thedorsal (D4, 5, 6, 7, 10,11, 12) and lumbar (L1, 2, 3, 4) spine without dural sac or nerveroot compression (Fig. 4). Bone density studies by Dual-energyX-ray absorptiometry (DEXA) bone scan revealed a T-score of�2.8 for the hip and �3.2 for the lumbar spine, consistent withestablished osteoporosis. Serum protein electrophoresisshowed no 'M' spike. The morning serum cortisol was0.027 mg/dl (normal value: 6.2–19.4 mg/dl) and 24 h free cortisolurine level was 11.25 mg (normal value: 28.5–213.7 mg).
A diagnosis of steroid-induced osteoporosis with multiplevertebral compression fracture was made, and his treatmentwas commencedwith an injection of recombinant parathyroidhormone 20 mg s/c daily for 18 months, along with calcium,vitamin D, analgesics, bisphosphonates, and thoraco-lumbo-sacral (TLSO) brace. At regular follow-ups at 6 weeks, 3months, and 6 months, the patient showed significantimprovement in the level of pain and mobility. The steroidswere gradually tapered off.
3. Discussion
The underlying mechanism in all cases of osteoporosis is animbalance between bone resorption and bone formation. Innormal bone, up to 10% of all bone mass may be undergoingremodeling at any point in time. Bone is resorbed by osteoclastcells, and new bone is deposited by osteoblast cells.6
Osteoporosis is usually a silent disease process, and mostpeople are asymptomatic unless a fracture has occurred; abouttwo-thirds of the vertebral compression fractures are asymp-tomatic.7 A symptomatic vertebral compression fracturebegins usually with acute onset of non-radiating back pain,which is aggravated by movement. However, residual painmay last for months. Multiple thoracic compression fractureseventually cause dorsal kyphosis with exaggerated cervicallordosis (Dowager's hump). Abnormal stress on the spinalmuscles and the ligaments may cause chronic, dull, andaching pain, particularly in the lower back. Vertebral fracturesoccur most commonly in the lower thoracic or upper lumbarspine.7 In the middle- and elderly-aged people with back pain,primary or metastatic bone malignancy must be excluded.Rare presentations of vertebral fracture include the caudaequina syndrome and paraparesis.8
Drug-induced osteoporosis usually occurs due to the use ofglucocorticoids, and mainly involves the axial skeleton.Certain medications also have been associated with anincrease in osteoporosis risk, like thyroxine, anticonvulsants,etc.3 A prophylactic treatment is recommended in patientswho take an equivalent of more than 30 mg hydrocortisone(7.5 mg of prednisolone), especially when this is in excess of 3months. Its usage on alternative days may not prevent thiscomplication.9 The risk of subsequent vertebral fracture isincreased significantly after the first osteoporotic fracture. In aseries of 9704women,with an average age of 68.8 years studiedfor 15 years, 324 had already suffered a vertebral fracture atentry into the study, and 18.2% developed a vertebral fracture,but that risk rose to 41.4% in women who had a previousvertebral fracture.10
[(Fig._4)TD$FIG]
Fig. 4 – Sagittal T2-weighted image (scanogram) of the spineshowing multiple collapse (fractures) in the dorsal andlumbar spine.
a p o l l o m e d i c i n e 1 2 ( 2 0 1 5 ) 1 4 4 – 1 4 7146

For early diagnosis of osteoporosis, plain radiographs maynot be useful, as decreased radiodensity and loss of trabecularstructuremay not be apparent until about 30% of the bone hasbeen lost. In established osteoporosis, vertebral fractures arecharacterized by decrease in posterior vertebral height(compression), decrease in mid-vertebral height (biconcavity),and decrease in anterior vertebral height (anteriorwedging). Inlong bones, although the cortices may be thin, the periostealsurface remains smooth. Glucocorticoid-induced osteoporosisis likely to cause rib fractures, aswell as fractures at other sites,where osteoporotic fractures are common and there isexuberant callus formation at sites of healing fractures.11
Dual-energy X-ray absorptiometry is considered as the goldstandard for the diagnosis of osteoporosis. Osteoporosis isdiagnosed when the bonemineral density is less than or equalto 2.5 standard deviations, below that of a young (30–40-year-old), healthy adult women reference population. This istranslated as a T-score.11
The goals of treatment in fractures related to osteoporosisare topreservebonemass, prevent fractures,decreasepain, andmaintain function. Risk factor modification can includeincreasing weight-bearing exercise, minimizing caffeine, alco-hol intake, and smoking cessation. The optimal amount ofweight-bearing exercise is not established, but an average of30 min/day is recommended. It is recommended that at least1000mg of elemental Ca be taken daily. Vitamin D supplemen-tation is recommendedwith a dose of 800–1000 IU/day. Bispho-sphonates are the first-line drug therapy. By inhibiting boneresorption, bisphosphonates preserve bone mass and candecrease vertebral and hip fractures by 50%.12 They can begiven orally or by IV. Intranasal salmon calcitonin can be usedfor treating osteoporosis, usually for patients who hadosteoporotic fractures. Salmon calcitonin may provide short-term analgesia after an acute fracture, such as a painfulvertebral fracture, due to an endorphin effect. Teriparatide (arecombinant parathyroid hormone) is an anabolic agent, whichstimulates new bone formation, and is generally reserved forpatients who cannot tolerate antiresorptive drugs, or havecontraindications to their use, or fail to respond (i.e., developnew fractures or lose bone mineral density), or possibly havesevere osteoporosis (e.g., T-score >�3.5), or have multiplevertebral fragility fractures.When given daily by injection in anaverage of 20 mg, synthetic parathyroid hormone (PTH 1-34;teriparatide) increases bone mass and reduces risk of frac-tures.13 Educating patients about the risks of falls and fractures,modifying the home environment for safety, and developingindividualized programs to increase physical stability andattenuate risk is also very important for preventing fractures.
Acute back pain from a vertebral compression fractureshould be treated with an orthotic support and usinganalgesics. Chronic backache may be relieved by exercisesthat help to strengthenparavertebralmuscles, and by avoidingheavy lifting. Bed rest should be minimized, and consistent,carefully designed weight-bearing exercise should be encour-aged. In some cases, vertebroplasty or kyphoplasty can relievesevere pain due to a new vertebral fragility fracture. Invertebroplasty, methyl methacrylate is injected into thevertebral body. In kyphoplasty, the vertebral body is firstexpanded with a balloon and then injected with methylmethacrylate. These procedures may reduce deformity in the
injected vertebrae but do not reduce and may even increasethe risk of fractures in adjacent vertebrae. Other risks mayinclude rib fractures, cement leakage, and rarely pulmonaryedema or myocardial ischemia. A further study to determinethe indications for these procedures is warranted.
4. Conclusion
Secondary osteoporosis may not be detected early and thusthe condition remains clinically silent until the patientpresents with multiple atraumatic compression fractures. Itis devastating for a young patient to developmultiple vertebralfractures in view of the associatedmorbidity andmortality. Todecrease the risk of additional fractures and preserve thequality of life in these patients, interventions should beinitiated early. Hence, it is important to consider multipleosteoporotic vertebral fractures as a complication in anypatient on prolonged steroid therapy.
Conflicts of interest
The authors have none to declare.
r e f e r e n c e s
1. Kado DM, Browner WS, Palermo L, Nevitt MC, Genant HK,Cummings SR. Vertebral fractures and mortality in olderwomen: a prospective study of Osteoporotic FracturesResearch Group. Arch Intern Med. 1999;159:1215–1220.
2. Scane AC, Francis RM. Risk factors for osteoporosis in men.Clin Endocrinol. 1993;38:15–16.
3. Caplan GA, Scane AC, Francis RM. Pathogenesis of vertebralcrush fractures in women. J Royal Soc Med. 1994;87:200–202.
4. Cooper C. Epidemiology and public health impact ofosteoporosis. Baillieres Clin Rheumatol. 1993;7:459–477.
5. Black D, Arden NK, Palermo L, Pearson J, Cummings SR.Prevalent vertebral deformities predict hip fractures andnew vertebral deformities but not wrist fractures. J BoneMiner Res. 1999;14:821–828.
6. Raisz L. Pathogenesis of osteoporosis: concepts, conflicts,and prospects. J Clin Invest. 2005;115(12):3318–3325.
7. Waugh EJ, Lam MA, Hawker GA, et al. Risk factors for lowbone mass in healthy 40–60 year old women: a systematicreview of the literature. Osteoporos Int. 2009;20(1):1–21.
8. Kim DH, Vaccaro AR. Osteoporotic compression fractures ofthe spine; current options and considerations for treatment.Spine J. 2006;6(5):479–487.
9. Gourlay M, Franceschini N, Sheyn Y. Prevention andtreatment strategies for glucocorticoid-induced osteoporoticfractures. Clin Rheumatol. 2007;26(2):144–153.
10. Cauley JA, Hochberg MC, Lui LY, Palermo L, Ensrud KE,Hillier TA. Long-term risk of incident vertebral fractures.JAMA. 2007;298(23):2761–2767.
11. Guglielmi G, Scalzo G. Imaging tools transform diagnosis ofosteoporosis. Diagnostic Imaging Europe. 2010;26:7–11.
12. Body JJ. How to manage postmenopausal osteoporosis? ActaClin Belg. 2011;66(6):443–447.
13. Han SL, Wan SL. Effect of teriparatide on bone mineraldensity and fracture in postmenopausal osteoporosis: meta-analysis of randomised controlled trials. Int J Clin Pract.2012;66(2):199–209.
a p o l l o m e d i c i n e 1 2 ( 2 0 1 5 ) 1 4 4 – 1 4 7 147

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/


















