
Multi-Modal Quantitative Analysis of Pediatric Focal Epilepsy Andy Eow Medical Vision Group CSAIL,...
14
Multi-Modal Quantitative Analysis of Pediatric Focal Epilepsy Andy Eow Medical Vision Group CSAIL, MIT
-
Upload
bryan-little -
Category
Documents
-
view
216 -
download
0
Transcript of Multi-Modal Quantitative Analysis of Pediatric Focal Epilepsy Andy Eow Medical Vision Group CSAIL,...

Multi-Modal Quantitative Analysis of
Pediatric Focal EpilepsyAndy Eow
Medical Vision GroupCSAIL, MIT

Project Background
Focal Epilepsy
• 2.5 million Americans suffer from some form of epilepsy.A large percentage being symptomatic partial epilepsy / focal epilepsy.
• 25% of these people are unresponsive to anti-epileptic medication and surgery is the last alternative.
• Success of surgery is highly dependent on the surgeon’s ability to locate the epileptic foci.
EEG Techniques
• Sub-dural EEG (Gold Standard)
• 32-channel Surface EEG
• 128-channel Surface EEG
Sub-dural EEG
32-channel EEG128-channel EEG

Project Background
EEG Source Localization
• Repeatedly solving the forward problem to obtain a set of dipole parameters that produces electrical potential that matches observed EEG data.
• Ill-posed inverse problem where multiple solutions can generate similar scalp potentials.
• Source localization with scalp EEG and visual correlation with imaging modalities guide placement of subdural grid.
Goal
• Improve EEG source localization with:
Patient-specific Head Model (Accuracy of forward solution)
Hotspots Prior Probability Map (Constraint on inverse solution)
• Focal cortical dysplasia (FCD) is one of the most epileptogenic lesions associated with early onset medically refractive focal epilepsy. These are the cases which I focused on.
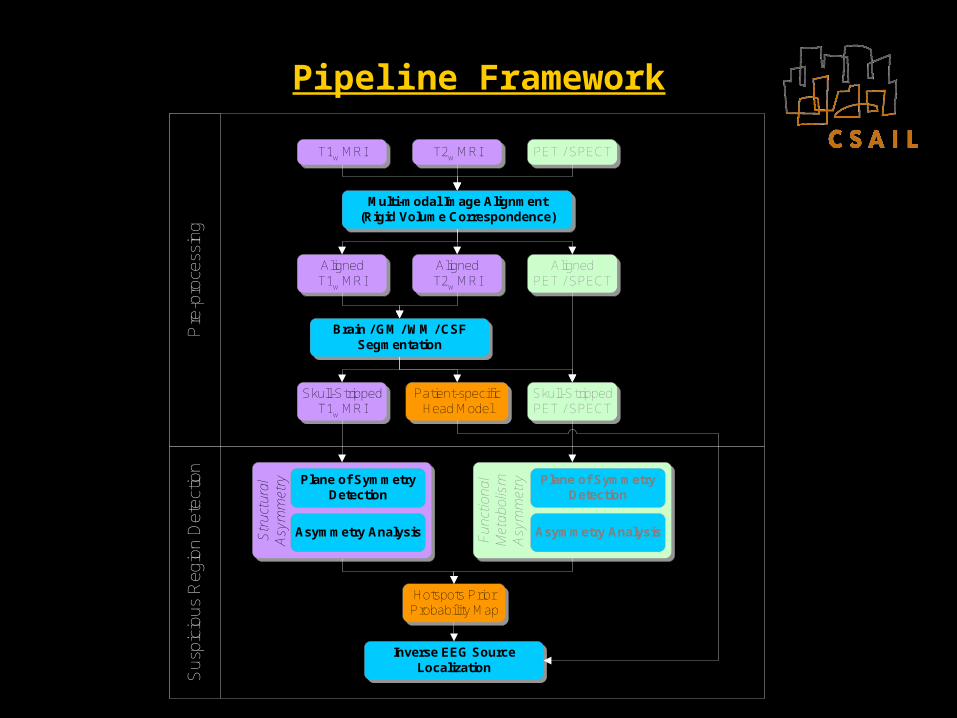
Pipeline Framework
Sus
pici
ous
Reg
ion
Det
ectio
nP
re-p
roce
ssin
g
AlignedPET / SPECT
AlignedT2w MRI
Fun
ctio
nal
Met
abol
ism
Asy
mm
etry
Hotspots PriorProbability Map
T2w MRI PET / SPECT
Skull-StrippedT1w MRI
Patient-specificHead Model
T1w MRI
Str
uctu
ral
Asy
mm
etry
Inverse EEG SourceLocalization
Multi-modal Image Alignment(Rigid Volume Correspondence)
Skull-StrippedPET / SPECT
AlignedT1w MRI
Brain / GM / WM / CSFSegmentation
Fun
ctio
nal
Met
abol
ism
Asy
mm
etry
PET / SPECT
AlignedPET / SPECT
T1w MRI
AlignedT2w MRI
Multi-modal Image Alignment(Rigid Volume Correspondence)
Skull-StrippedT1w MRI
Brain / GM / WM / CSFSegmentation
AlignedT1w MRI
T2w MRI
Patient-specificHead Model
Skull-StrippedPET / SPECT
Str
uctu
ral
Asy
mm
etry
Asymmetry Analysis
Plane of SymmetryDetection
Asymmetry Analysis
Plane of SymmetryDetection
Hotspots PriorProbability Map
Inverse EEG SourceLocalization

Patient Example
Details
• 16 years when image acquisition was done.
• Focal cortical dysplasia in the right inferior frontal lobe
• T1-weighted & T2-weighted structural MRI volumes
T1-weighted MRI T2-weighted MRI
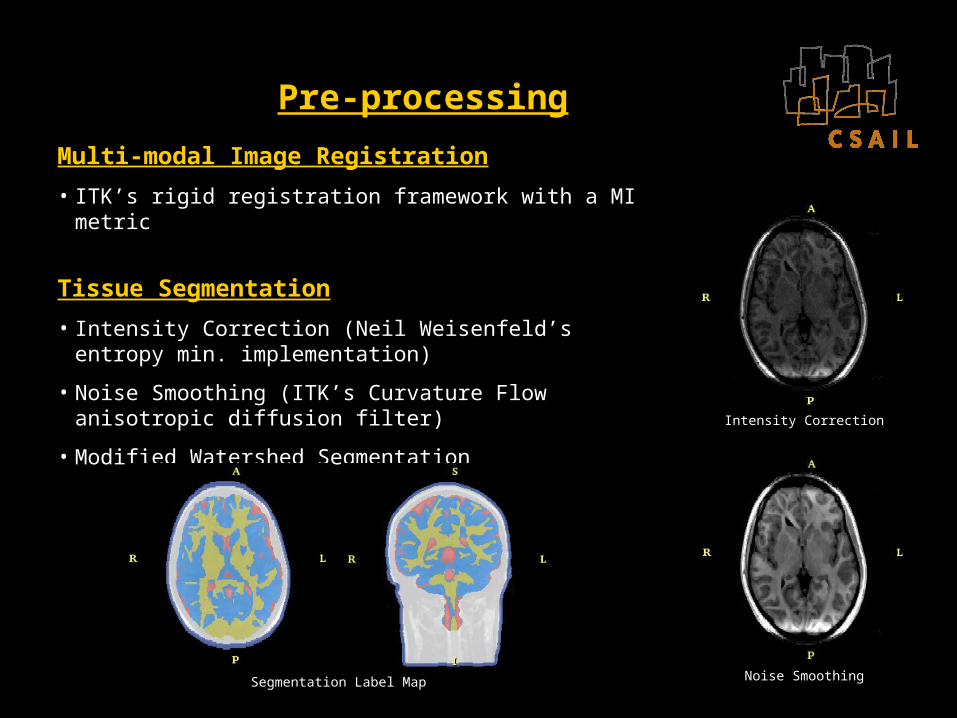
Pre-processing
Multi-modal Image Registration
• ITK’s rigid registration framework with a MI metric
Tissue Segmentation
• Intensity Correction (Neil Weisenfeld’s entropy min. implementation)
• Noise Smoothing (ITK’s Curvature Flow anisotropic diffusion filter)
• Modified Watershed Segmentation
Intensity Correction
Noise SmoothingSegmentation Label Map

Symmetry Plane Detector
*RT 2
1*RT
cII scI
H
• Choose arbitrary target symmetry plane. Obtain chiral, Ic, from reflection about this plane.
• Find optimal rigid transformation, TR*, that maps Ic to I.
• “Half” the transform TR* and apply to Ic to obtain
symmetrically aligned chiral.
• Aligns plane of maximal inter-hemispheric similarity with target symmetry plane.

Symmetry Plane Robustness
Assumption
• In the absence of large pathologies, plane of maximal inter-hemispheric similarity matches the anatomical mid-sagittal plane.
MCA Infarction (Worst Case)
• Left hemisphere largely absent.
• Left shifting of mid-line structures.
• Plane of maximal inter-hemispheric similarity no longer coincides well with the mid-sagittal plane.
• Matches remaining cortical tissues and other major structural features such as the skull, ocular cavities etc.
• Holistically, symmetry plane detected still reasonable.
• Unlikely for FCD cases to present with such large pathologies.

Asymmetry Analysis
Deformation Field, F
• Find optimal deformation that best matches symmetrically aligned volume and its chiral (about the target symmetry plane)
• ITK’s non-rigid registration framework with a SSD metric
Asymmetry
• |F|(1 + .F)
• Emphasis is placed on |F|.
Deformation Magnitude, |F|
Modified Deformation Divergence, 1+.F
Asymmetry, |F|(1+.F)
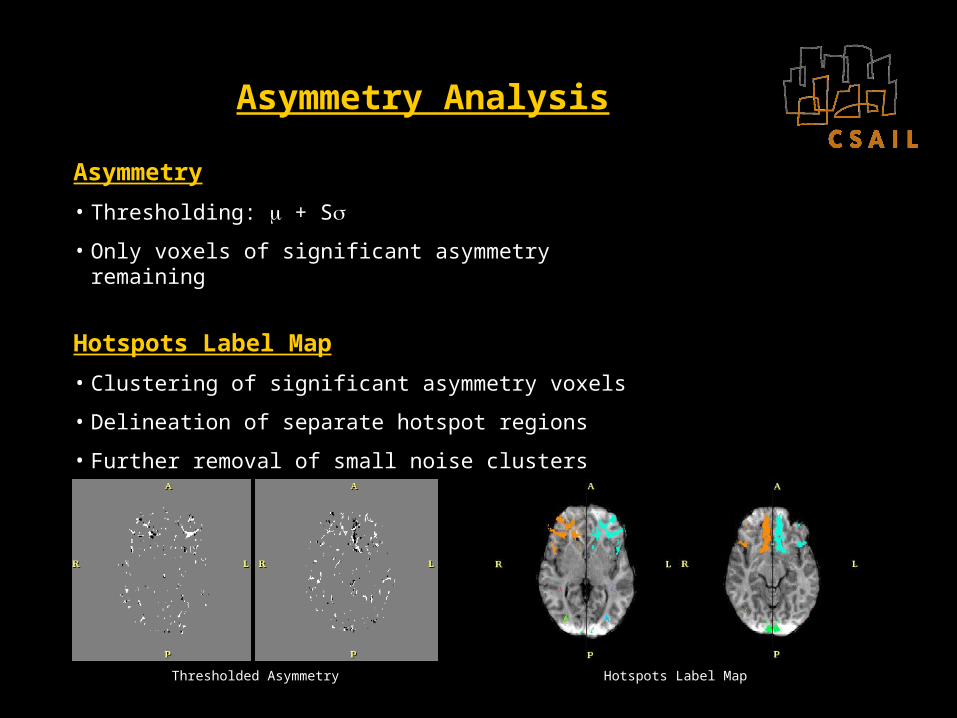
Asymmetry Analysis
Asymmetry
• Thresholding: + S
• Only voxels of significant asymmetry remaining
Hotspots Label Map
• Clustering of significant asymmetry voxels
• Delineation of separate hotspot regions
• Further removal of small noise clusters
Thresholded Asymmetry Hotspots Label Map

Hotspots Prior Probability Map
Building the Probability Map …
• Assigning probability values
• Photspot = 0.9
• PGM = 0.2
• PWM = 0.1
• PCSF = 0.01
• Poutside = 0
• Gaussian smoothing
Prior Probability Map
Hotspots Label Map

EEG Source Localization
Experiments
• Simulate dipole within detected hotspot to obtain EEG measurements.
• Perturbations:
EEG voltage noise, v
Electrode location noise, e
Tissue conductivity, c
Results
Simulated Noise
v / V e / mm c / %Location Error / mm
NeuroFEM Prior
Zero Noise NA NA NA 0.07 Not necessary
Low Noise 5 x 10-4 3 5 2 Not necessary
Medium Noise 1 x 10-3 4 7.5 4.9 0.5
High Noise 5 x 10-3 5 10 14.6 0.5

Future Work
Functional Neuroimaging
• PET / SPECT
• Detect functional asymmetries such as regions of decreased glucose metabolism for PET and cerebral blood flow for SPECT etc.
• Complements structural asymmetries provided by MRI.
Diffusion-Tensor Imaging
• Anisotropic patient-specific head model
• Reduced FA in dysplastic neurons within white-matter tissue structures. Complements structural and functional asymmetries to generate a more comprehensive prior probability map.
• Detects cortical abnormalities at an earlier stage.
• Analyze neural connectivity between potential surgical sites and eloquent

Thank you!













![EOW LU Tax 2013 Payrolls 1.3.13[1]](https://static.fdocuments.net/doc/165x107/577ce37b1a28abf1038c3c61/eow-lu-tax-2013-payrolls-13131.jpg)




