Mucosal proliferation characteristics in ureterosigmoidostomy: Effect of calcium supplement
4
Mucosal Proliferation Characteristics in Ureterosigmoidostomy: Effect of Calcium Supplement By Thomas Weber, Robert Connors, Thomas Tracy, Jr, Patrick V. Bailey, George Steinhardt, and Cirilo Sotelo-Avila St Louis, MO Ureterosigmoidostomy, frequently performed in chil- dren for urinary diversion, is a known premalignant condi- tion. Dietary calcium supplements have been shown to normalize mucosal proliferative patterns in other human premalignant colonic conditions, which might decrease the risk of cancer. However, calcium supplementation has not been investigated in ureterosigmoidostomy. We used a rat model to study the effects of increased dietary calcium on the progression to carcinoma in ureterosigmoidostomy. Twenty-five Wister rats underwent ureterosigmoidostomy by anastomosis of bladder trigone and ureters to sigmoid, and were divided into two groups: group 1, regular diet (14); and group 2, calcium supplemented (2%) diet (11 ). All animals received the diet for 9 months. At death the anastomosis was weighed and examined histologically. In addition, ornithine decarboxylase (ODC), an enzyme involved in polyamine synthesis that becomes elevated in neoplastic and proliferative disorders, was determined at the anastomosis and 8 cm proximal (normal colon). All animals developed proliferative metaplastic polyposis at the anastomosis. Tumor weights were 2.6 _+ 1.1 g for group 1 and 4.8 _+ 1.2 g for group 2 (P < .05). The ODe levels were: group 1, normal colon 78.2 _+ 15.6 and tumor 321.3 + 58.8 (P < .002); and group 2, normal colon 426.8 _+ 65.4 and tumor 568.0 _+ 40.9 (P = NS). The difference between group 1 normal colon and group 2 normal colon was significant (P < .001 ), as was group I tumor and group 2 tumor (P < .02). These data show that dietary calcium supplementation in this ureterosigmoidostomy-carcinoma model stimulates cell proliferation (ODe levels) in normal colon, and causes significant increases in tumor size end tumor ODe levels at ureterosigmoidostomy sites. Calcium- supplemented diets should be used cautiously in children with ureterosigmoidostomy. 1990 by W,B. Saunders Company. INDEX WORDS: Ureterosigmoidostomy; ornithine decar- boxylase. U RETEROSIGMOIDOSTOMY has been a use- ful means of urinary diversion, most often used in children born with exstrophy of cloaca or bladder. A persistent concern of ureterosigmoidostomy has been a significantly increased risk of the development of colon carcinoma at or adjacent to the ureter-colon anasto- From the Division of Pediatric Surgery, Department of Surgery, St Louis University and Cardinal Glennon Children's Hospital, St Louis, MO. Presented at the 20th Annual Meeting of the American Pediatric Surgical Association, Baltimore, Maryland, May 28-31, 1989. Address reprint requests to Thomas R. Weber, MD, Department of Pediatric Surgery, 1465 S Grand Blvd, St Louis, MO 63104. ~) 1990 by W.B. Saunders Company. 0022-3468/90/2501-0024503.00/0 motic site. Carcinoma related to ureterosigmoidos- tomy develops years after the original operative procedure, and has been reported to occur even after takedown of the ureterostomy, if the remnants of ureter are left in place. The carcinoma is frequently fatal, and early detection has been difficult. The rote of dietary factors in the development of colon carcinoma has received recent emphasis. Cancer promoters, such as high dietary fat, certain bile acids, and other carcinogens have been identified, and are used to explain geographic differences in the incidence of colon carcinoma. Likewise, dietary additives, such as oral calcium supplements, have been investigated as agents that may lower the risk of colonic neoplasia. However, there is little information available regard- ing the use of dietary supplements to decrease the risk of cancer related to ureterosigmoidostomy. Ornithine decarboxylase (ODC), a rate-limiting enzyme involved in polyamine synthesis, is elevated in rapidly growing and neoplastic colonic mucosa) Previ- ous studies from our laboratory have established ele- vated ODC levels in experimental neoplastic uretero- sigmoidostomy,2 but the effects of increased dietary calcium in this model are unknown. To further investi- gate these relationships, a rat model of ureterosig- moidostomy was used to evaluate the effects of a high calcium diet on ODC levels and the development of carcinoma at the anastomotic site. MATERIALS AND METHODS Twenty-five male Wister rats, 150 to 250 g, were anesthetized with ether and underwent laparotomy using aseptic technique. The bladder trigone, with both ureters attached, was separated from the remainder of the bladder and sutured as a patch into the colon, using 5-0 absorbable suture. The remainder of the bladder was closed using similar suture. After recovery, the animals were housed in standard rodent cages, and allowed water ad lib to which carbenicil- lin was added. The animals were divided into two groups: group I (14 rats), received a regular diet for 9 months; and group 2 (11 rats) were fed a calcium-supplemented (2%) diet for 9 months. No other medications or known carcinogens were given to the animals. All animals were killed at 9 months. At death, the entire colon was removed and placed immediately on ice. The site of the bladder-colonic anastomosis was identified, and resected and weighed. A small portion was fixed in formalin, stained with hematoxylin and eosin, and examined histologically. The mucosa of the remainder of the anastomosis was dissected free from the muscular layers, homogenized, and placed in iced buffer. In addition, mucosa from normal-appearing colon 8 cm proximal to the anastomosis was dissected and homogenized. Mucosa ODC levels were determined by the method of Stanley and Kazarinoff) Briefly, after homogenization, the supernatant was 130 Journal of Pediatric Surgery, Vo125, No 1 (January), 1990: pp 130-133
-
Upload
thomas-weber -
Category
Documents
-
view
212 -
download
0
Transcript of Mucosal proliferation characteristics in ureterosigmoidostomy: Effect of calcium supplement

Mucosal Proliferation Characteristics in Ureterosigmoidostomy: Effect of Calcium Supplement
By Thomas Weber, Robert Connors, Thomas Tracy, Jr, Patrick V. Bailey, George Steinhardt, and Cirilo Sotelo-Avi la
St Louis, MO
�9 Ureterosigmoidostomy, frequently performed in chil- dren for ur inary diversion, is a known premal ignant condi- t ion. Dietary calcium supplements have been shown to normalize mucosal proliferative patterns in o ther human premal ignant colonic condit ions, which might decrease the risk of cancer. However, calcium supplementation has not been invest igated in ureterosigmoidostomy. We used a rat model to study the effects of increased dietary calcium on the progression to carcinoma in ureterosigmoidostomy. Twenty- f ive Wister rats underwent ureteros igmoidostomy by anastomosis of bladder trigone and ureters to sigmoid, and were divided into t w o groups: group 1, regular diet (14); and group 2, calcium supplemented (2%) diet (11 ). All animals received the diet for 9 months. A t death the anastomosis was weighed and examined histologically. In addit ion, orn i th ine decarboxylase (ODC), an enzyme involved in polyamine synthesis that becomes elevated in neoplastic and proliferative disorders, was determined at the anastomosis and 8 cm proximal (normal colon). All animals developed proliferative metaplastic polyposis at the anastomosis. Tumor weights were 2.6 _+ 1.1 g for group 1 and 4.8 _+ 1.2 g for group 2 (P < .05). The ODe levels were: group 1, normal colon 78.2 _+ 15.6 and tumor 321.3 + 58.8 (P < .002); and group 2, normal colon 426.8 _+ 65.4 and tumor 568.0 _+ 40.9 (P = NS). The difference between group 1 normal colon and group 2 normal colon was significant (P < .001 ), as was group I tumor and group 2 tumor (P < .02). These data show that dietary calcium supplementat ion in this ureterosigmoidostomy-carcinoma model stimulates cell proliferation (ODe levels) in normal colon, and causes significant increases in tumor size end tumor ODe levels at ureterosigmoidostomy sites. Calcium- supplemented diets should be used cautiously in children wi th ureterosigmoidostomy. �9 1990 by W,B. Saunders Company.
INDEX WORDS: Ureterosigmoidostomy; ornithine decar- boxylase.
U R E T E R O S I G M O I D O S T O M Y has been a use- ful means of urinary diversion, most often used
in children born with exstrophy of cloaca or bladder. A persistent concern of ureterosigmoidostomy has been a significantly increased risk of the development of colon carcinoma at or adjacent to the ureter-colon anasto-
From the Division of Pediatric Surgery, Department o f Surgery, St Louis University and Cardinal Glennon Children's Hospital, St Louis, MO.
Presented at the 20th Annual Meeting of the American Pediatric Surgical Association, Baltimore, Maryland, May 28-31, 1989.
Address reprint requests to Thomas R. Weber, MD, Department of Pediatric Surgery, 1465 S Grand Blvd, St Louis, MO 63104.
~) 1990 by W.B. Saunders Company. 0022-3468/90/2501-0024503.00/0
motic site. Carcinoma related to ureterosigmoidos- tomy develops years after the original operative procedure, and has been reported to occur even after takedown of the ureterostomy, if the remnants of ureter are left in place. The carcinoma is frequently fatal, and early detection has been difficult.
The rote of dietary factors in the development of colon carcinoma has received recent emphasis. Cancer promoters, such as high dietary fat, certain bile acids, and other carcinogens have been identified, and are used to explain geographic differences in the incidence of colon carcinoma. Likewise, dietary additives, such as oral calcium supplements, have been investigated as agents that may lower the risk of colonic neoplasia. However, there is little information available regard- ing the use of dietary supplements to decrease the risk of cancer related to ureterosigmoidostomy.
Ornithine decarboxylase (ODC), a rate-limiting enzyme involved in polyamine synthesis, is elevated in rapidly growing and neoplastic colonic mucosa) Previ- ous studies from our laboratory have established ele- vated ODC levels in experimental neoplastic uretero- sigmoidostomy, 2 but the effects of increased dietary calcium in this model are unknown. To further investi- gate these relationships, a rat model of ureterosig- moidostomy was used to evaluate the effects of a high calcium diet on ODC levels and the development of carcinoma at the anastomotic site.
MATERIALS AND METHODS
Twenty-five male Wister rats, 150 to 250 g, were anesthetized with ether and underwent laparotomy using aseptic technique. The bladder trigone, with both ureters attached, was separated from t h e remainder of the bladder and sutured as a patch into the colon, using 5-0 absorbable suture. The remainder of the bladder was closed using similar suture. After recovery, the animals were housed in standard rodent cages, and allowed water ad lib to which carbenicil- lin was added. The animals were divided into two groups: group I (14 rats), received a regular diet for 9 months; and group 2 (11 rats) were fed a calcium-supplemented (2%) diet for 9 months. No other medications or known carcinogens were given to the animals. All animals were killed at 9 months.
At death, the entire colon was removed and placed immediately on ice. The site of the bladder-colonic anastomosis was identified, and resected and weighed. A small portion was fixed in formalin, stained with hematoxylin and eosin, and examined histologically. The mucosa of the remainder of the anastomosis was dissected free from the muscular layers, homogenized, and placed in iced buffer. In addition, mucosa from normal-appearing colon 8 cm proximal to the anastomosis was dissected and homogenized.
Mucosa ODC levels were determined by the method of Stanley and Kazarinoff) Briefly, after homogenization, the supernatant was
130 Journal of Pediatric Surgery, Vo125, No 1 (January), 1990: pp 130-133

MUCOSAL PROLIFERATION IN URETEROSIGMOIDOSTOMY 131
mixed with buffer and 14C-ornithine added and incubated at 37~ The resultant '4CO2 was collected in hyamine hydrochloride, and counted in a scintillation counter. Activity was expressed as micro- moles of ]4CO2 per milligram protein per hour.
Group 1 and 2 animals were compared for mean tumor weights, ODC levels at the anastomosis, and ODC levels in normal colon, using Students t test for statistical analysis.
RESULTS
All 25 rats survived the 9-month period, and appeared healthy at the time of death. The bladder- bowel anastomosis was grossly abnormal in each case, with multiple polypoid lesions covering both bowel and bladder mucosa. Histologically, florid squamous meta- plasia was seen. These changes were identical to those reported previously. = No invasive or metastatic tumor was present grossly in the remainder of the abdominal cavity, land each animal had two intact, normal- appearing kidneys with patent ureters.
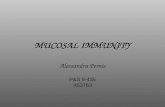
The tumor weights for each group are shown in Fig 1. There was a statistically significant difference in the weights, with group 2 rats having larger tumors. However, histologically the two groups appeared iden- tical.
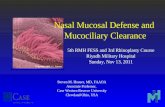
The ODC levels for normal and tumor tissue in animals fed a regular diet are shown in Fig 2. There was a significant increase in ODC levels in tumor compared with normal colonic mucosa indicating florid mucosa proliferation at the anastomotic site. This finding is similar to that previously published. 2
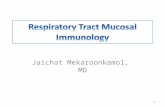
The ODC levels for normal and tumor colonic mucosa in the animals fed a calcium-supplemented diet are shown in Fig 3. The high calcium diet stimu- lated mucosa proliferation in both normal and tumor mucosa. In addition, ODC levels in both tumor and colonic mucosa in calcium-supplemented rats were significantly higher than levels in regular diet rats (Fig 2); P < .001 normal colon, and P < .02 tumor mucosa. These data again confirm a proliferation-stimulatory effect of calcium on both normal and tumor mucosa.
6
5
Gins
4
3 T 2"
Regular Diet Calcium Diet
Fig 1. Tumor weights for each group (regular diet and calci- um-supplemented diet) (P < .05). Note: Statistically significant increase in tumor weight with high-calcium diet.
400
350 T 30O
ODC 250 p moles/hr
200
150
100
50 ~ ~ t ~ o Normal Colon Tumor
Fig 2. ODC levels in animals fed a regular diet. There was a statist ical ly significant increase in ODC levels wi th in tumor tissue (P < .002).
DISCUSSION
Although ureterosigmoidostomy has been a useful technique for urinary diversion in patients of all ages, its use in children has become the subject of increasing concern because of the known significant risk of carci- nogenesis. In several carefully examined series, 4'5 up to 40% of patients with ureterosigmoidostomy had pre- malignant (adenomatous) polyps or adenocarcinoma at the ureteral anastomosis site, with an estimated risk for eventual development of cancer 7,000 times that for the general population under 25 years of age. The carcinomas that develop in association with ureterosig- moidostomy are highly malignant, with over half of the patients having metastatic disease at the time of dis- covery of the tumor. 6
Because of these significant risks, early discovery of malignant change associated with ureterosigmoidos- tomy through regular surveillance has been advocated. Frequent contrast enemas, colonoscopy, testing of stool for occult blood, and similar techniques have been used to detect established tumors, but fail to detect prema- lignant changes. In a previous study, 2 we proposed mucosa ODC levels as a measure of premalignancy in a rat model of ureterosigmoidostomy, but the useful-
70C
60C
50C
ODC 40C. . p moles/hr
30C.
20C. .
10C.
I
Normal Colon Tumor
Fig 3. ODC levels in animals fed a calcium-supplemented diet. There was no significant difference in normal and tumor tissue, in contrast to animals fed a regular diet (Fig 2).

132 WEBER ET AL
ness of this technique has yet to be tested in the clinical setting. Although early diagnosis of cancer associated with ureterosigmoidostomy is valuable, the ultimate control of this frequently lethal disease rests with a more complete understanding of the factors associated with its cellular carcinogenesis.
It is now generally accepted that most colonic can- cers arise as a result of classic two-stage carcinogene- sis. 7 Although Berenblum's concepts of initiation fol- lowed by promotion are still widely accepted, most carcinomas are probably the result of a more complex interaction of initiators, promoters, cofactors, and inhibitors. 8 Initiators and promoters have received the majority of emphasis in most published experimental and epidemiologic studies of colonic carcinoma, but it has only been recently that inhibitors have been actively investigated.
Colon carcinoma can develop in a number of set- tings. Inflammatory bowel disease, familial polyposis, ureterosigmoidostomy, other familial factors, and dietary carcinogens are but a few of the known or suspected factors that may initiate carcinogenesis. In addition, there is an emerging list of cancer promoters that may actively participate in the mucosal prolifera- tive sequence that ends in carcinogenesis. The most widely studied of these promoters are dietary fat and fiber content. 8
Recently, several studies have investigated the role of dietary calcium in the prevention of colonic carci- noma. In a prospective epidemiologic study, Garland et al 9 found a significantly lower colorectal cancer rate in men with a higher calcium intake. N e w m a r k e t al, I~ based on experimental studies, felt that a high calcium diet would bind bile acids that are known carcinoma promoters, thus decreasing the risk of carcinoma development in populations that consume a high fat diet. Lipkin and Newmark H found that calcium sup- plementation normalized mucosal proliferative rates, as measured by tritiated-thymidine labeling, in a popu- lation at increased risk for colon carcinoma on a
familial basis. The latter study is not sufficiently long-term to assess whether increased calcium will in fact decrease cancer incidence in this group, but sug- gests that calcium supplementation might decrease colon cancer incidence in other patients with known high risk factors. To our knowledge, calcium supple- mentation has not been used in patients with uretero- sigmoidostomy.
The present experiments a t tempt to evaluate whether dietary calcium supplements will decrease mucosal proliferation at a ureterosigmoidostomy site. A previous study demonstrated very active mucosal proliferation at ureterosigmoidostomy, measured both histologically and by mucosa ornithine decarboxylase levels. 2 The present study shows that added dietary calcium in this same model increases the metaplasic proliferation at the ureterosigmoidostomy, in both size (weight) and biochemically (ODC levels). Other stud- ies of carcinogens and promoters ~ suggest that an increase in cell proliferation, such as that seen here, might result in an increased development of tumors.
The reasons for the difference in the response to calcium in our study, compared with the previous studies, suggest a different mode of tumor promotion in ureterosigmoidostomy that may not involve dietary fat or bile acids. These relationships are the object of continuing studies.
Although the present studies are somewhat prelimi- nary, several important implications are nevertheless suggested. The mechanism of carcinogenesis asso- ciated with ureterosigmoidostomy needs further inves- tigation. The role of dietary factors, both promotional and inhibitory, needs extensive study. The role of urine in the carcinogenesis process is also poorly under- stood.
Until further studies are performed, calcium supple- ments should be used with caution in patients with ureterosigmoidostomy, as they may increase the risk of the development of carcinoma.
REFERENCES
1. Pegg AE, McMann PP: Polyamine metabolism and function. Am J Physiol 243:C212-221, 1982
2. Weber TR, Westfall SH, Steinhardt GF, et al: Malignancy associated with ureterosigmoidostomy: Detection by mucosa orni- thine decarboxylase. J Pediatr Snrg 23:1091-1094, 1988
3. Stanley BA, Kazarinoff MN: Induction of ornithine decarbox- ylase in colon and liver by starvation and refeeding: A comparison of effects on total and holoenzyme. Biochem Biophys Res Commun 105:773-777, 1982
4. Starling JR, Uehling DT, Gildrist KW: Value of colonoscopy after ureterosigmoidostomy. Surgery 96:784-789, 1984
5. Eraklis A J, Folkman M J: Adenocarcinoma at the site of ureterosigmoidostomies for exstrophy of the bladder. J Pediatr Surg 13:730-734, 1978
6. Gittes RF: Carcinogenesis in ureterosigmoidostomy. Urol Clin North Am 13:201-205, 1986
7. Berenblum I: Sequential aspects of chemical carcinogenesis: Skin, in Becker FF (ed): Cancer, a Comprehensive Treatise. Etiolo- gy: Chemical and Physical Carcinogenesis, vol 1. New York, NY, Plenum, 1975, pp 323-351
8. Zaridze DG: Environmental etiology of large bowel cancer. JNCI 70:389-400, 1983
9. Garland C, Shekell RB, Barrett-Connor E, et al: Dietary vitamin D and calcium and risk of colorectal cancer: A 19-year prospective study in men. Lancet 1:307-309, 1985
10. Newmark HL, Wargovich M J, Bruce WR: Colon cancer and dietary fat, phosphate, and calcium: A hypothesis. JNCI 72:1323- 1325, 1985
11. Lipkin M, Newmark H: Effect of added dietary calcium on colonic epithelial-cell proliferation in subjects at high-risk for famil- ial colonic cancer. N Engl J Med 313:1381-1384, 1985

MUCOSAL PROLIFERATION IN URETEROSlGMOIDOSTOMY 133
Discuss ion
J. Noseworthy (Wilmington, DE): Dr Folkman has thought of more questions in 2 minutes than I did in the 5 days that I had to review the manuscript, but I was still fascinated by this piece of work, despite the fact that the findings fly in the face of the hypothesis. It may simply be that this model system is vastly different in its biochemical control mechanisms from the human colonic carcinoma system. I would like to ask a couple of specific questions that have to do with more carefully dissecting the role of calcium in this system. Is it in fact possible to look at calcium binding or insolubilization of bile acids and ionized fatty acids intraluminally in this model? It has been suggested that it is that specific effect of calcium in the human cancer model that leads to this reduction in prolifera- tive stimulation, and have you the ability to look at those kinds of effects of calcium in your model system?
T.R. Weber (closing): In response to Dr Nose- worthy's question, we have not investigated bile acids.
With the paradoxical response that we observed, I do not think that bile acids are involved in this carcino- genosis process. However, bile acids that are bound by calcium can be examined and that is worthwhile pursuing. In response to Dr Folkman, there is some recent information regarding calcium, growth factors, and oncogene expression, even since the manuscript was written, that might have some bearing on these observations. Calcium is now known to be a secondary messenger associated with a number of growth factors, including epidermal growth factor, platelet derived growth factor, and insulin-like growth factor. All of these have been implicated at one time or another in the carcinogenesis process. In addition, a high calcium diet is known to increase expression of C-RAS onco- gene. We looked for C-MYC oncogene expression in this model and did not find it, but now I think we will go back with our molecular biologists and pursue the oncogene expression and/or growth factor idea fur- ther.