Mucocutaneous Hemorrhage
47
Mucocutaneous Hemorrha ge
-
Upload
anastasia-combs -
Category
Documents
-
view
63 -
download
0
description
Mucocutaneous Hemorrhage. Definition. Mucocutaneous hemorrhage is caused by the abnormalities of hemostasis( 止血 ) and /or coagulation( 凝血 ) , characterized by local or extensive mucocutaneous hemorrhage derived from capillary. The bleeding is usually spontaneous or from slight trauma. - PowerPoint PPT Presentation
Transcript of Mucocutaneous Hemorrhage
Mucocutaneous Hemorrhage
Definition
Mucocutaneous hemorrhage is caused by the abnormalities of hemostasis( 止血 ) and /or coagulation( 凝血 ), characterized by local or extensive mucocutaneous hemorrhage derived from capillary. The bleeding is usually spontaneous or from slight trauma.
Hemostasis/coagulationHemostasis/coagulation is the body's norm
al physiological response for the prevention and stopping of bleeding/hemorrhage.
Hemotasis Primary hemostasis---platelet plug formation at sites of injury Secondary hemostasis---plasma coagulation system reaction resu
lting in fibrin formation
Primary and secondary hemostasis are closely linked
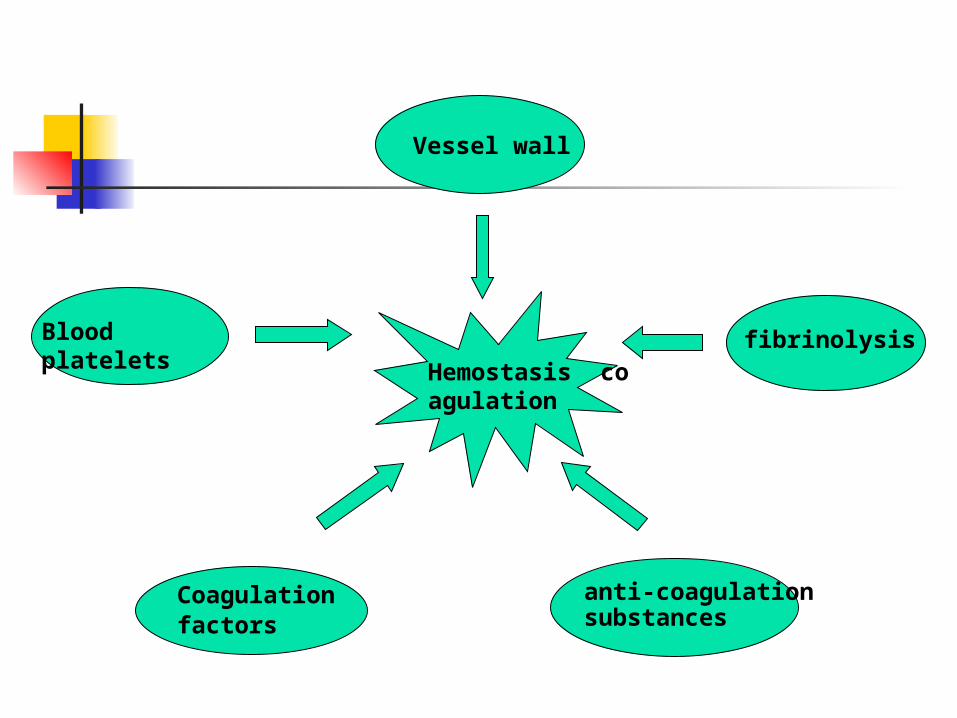
Vessel wall
Blood platelets
Coagulation factors
anti-coagulation substances
fibrinolysisHemostasis coagulation
Etiology & Pathogenesis
Vessel wall disorders Abnormalities of blood platelets — Quantitative platelets defects — Qualitative platelets defects Disturbance of coagulation in circula
tion — Deficiency of coagulation factors Increase of anti-coagulation substances Hyperfunction of fibrinolysis( 纤维蛋白溶解 )
Defects on the vessel wall
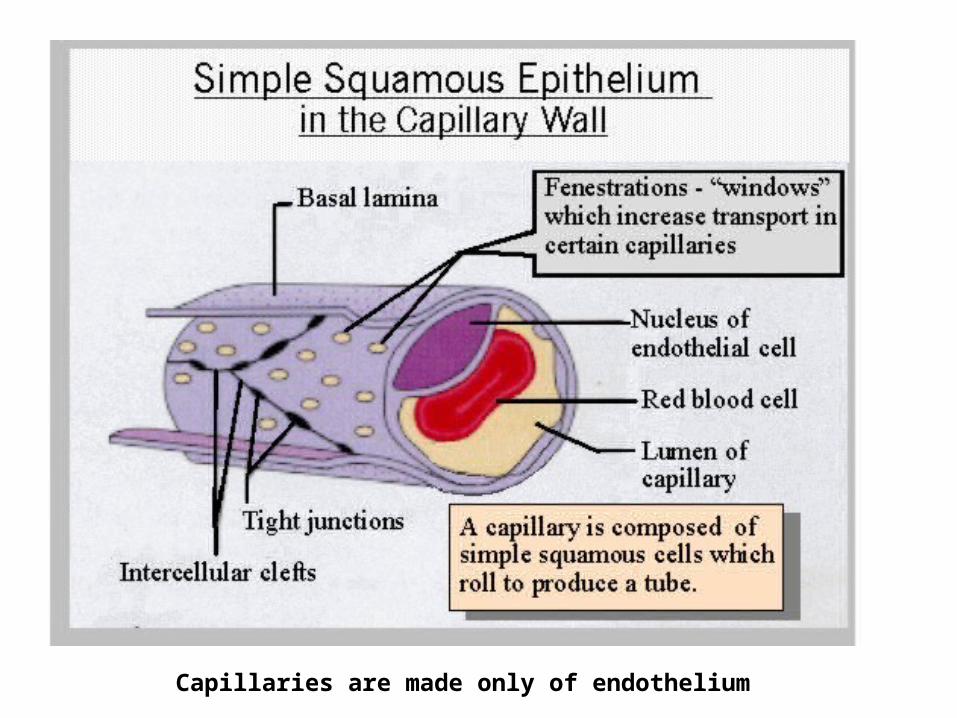
Capillaries are made only of endothelium
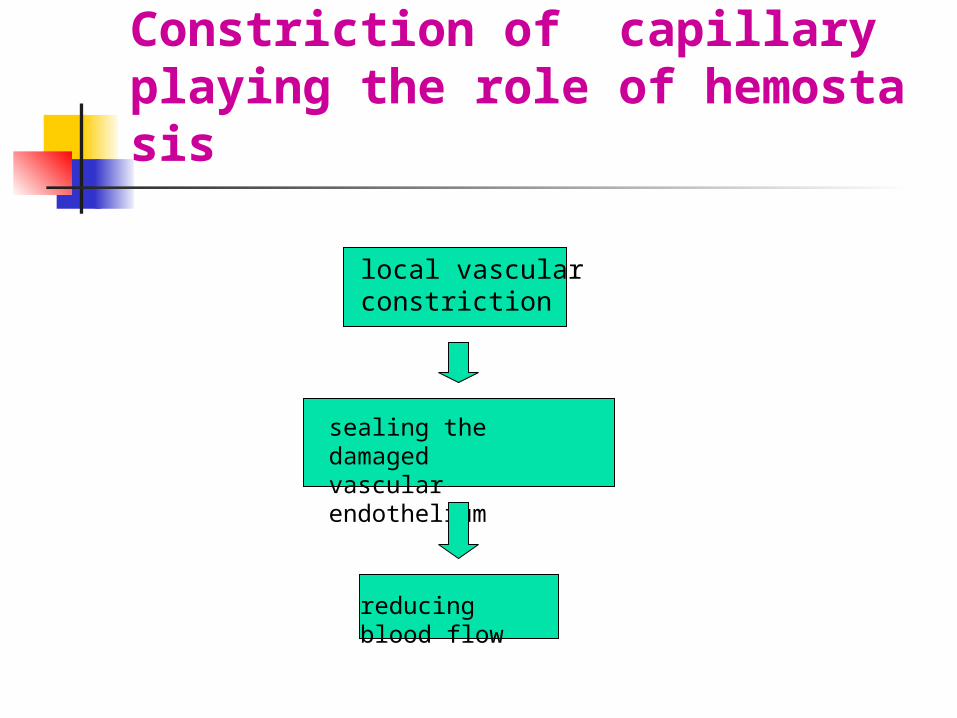
Constriction of capillary playing the role of hemostasis
local vascular constriction
sealing the damaged vascular endothelium
reducing blood flow
Vascular wall disorders Damage to capillary endothelium Abnormalities in the vascular subendotheli
al matrix Defect of extravascular connective tissues t
hat support blood vessels Formation of abnormal blood vessels.
Defects on Capillary Wall
Hereditary Telangioectasia( 毛细血管扩张 );
Acquired Allergic purpura( 过敏性紫癜 ); Senile purpura Non- thrombocytopenic purpura — Severe infection — Vitamin C deficiency — Uremia
Vitamin C is needed to synthesize hydroxyproline( 羟脯氨酸 ), an essential
constituent of collagen
excess production of glucocorticoids
develop generalized protein wasting
atrophy of the supporting connective tissue around blood vessels
skin bleeding or easy bruising
Cushing's syndrome
Senile purpura
Ageing causes a similar atrophy of perivascular connective tissues
In this situation,BT and CT are normal,but capillary fragility
test is positive.
Abnormalities of blood platelets
Blood platelets function in primary hemostasis platelet adhesion and aggregation
Platelet activation from thromboxane A 2 fur
ther aggregates platelets (to form the white thrombus ) and enhances vasoconstriction
platelet secretion activated platelets secrete platelet agents, 5-HT and coagulators participating in the coagulation process and facilitate the clot constriction.
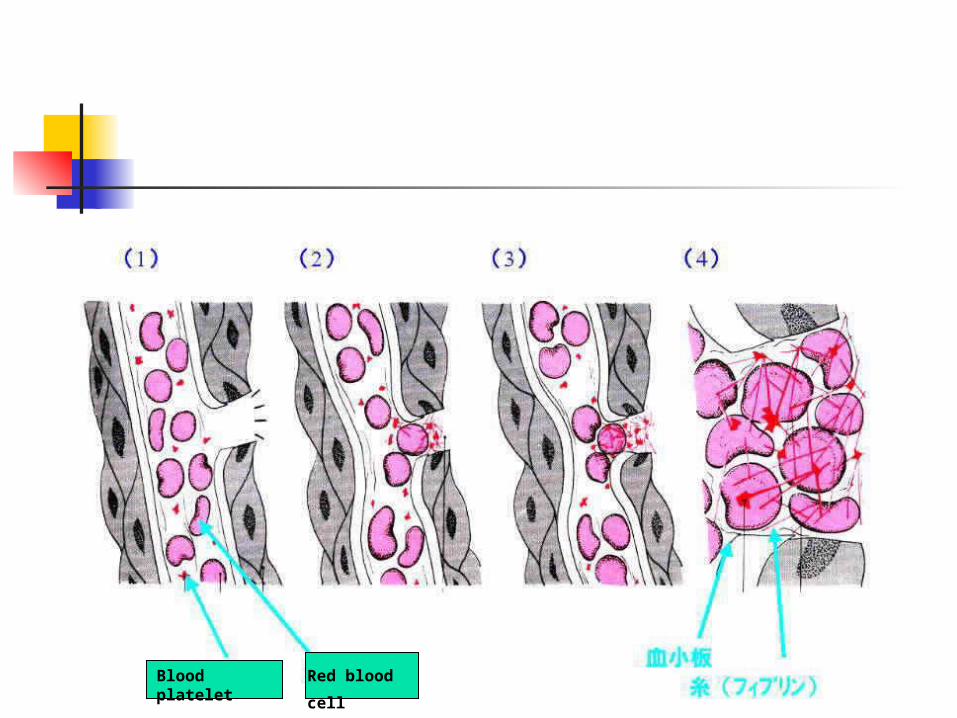
Red blood
cell Blood platelet
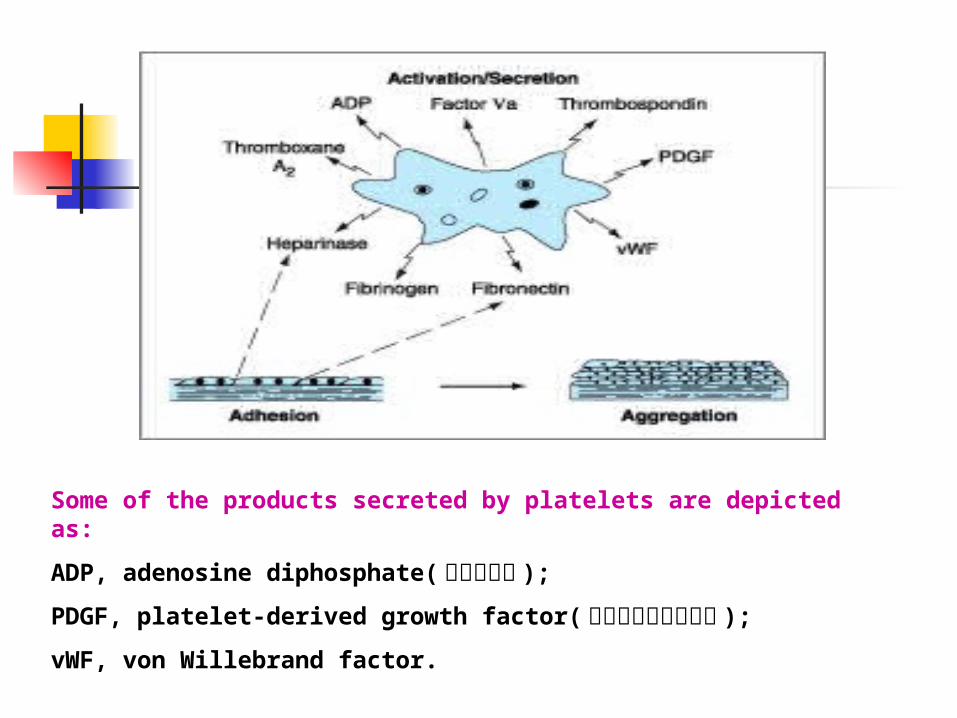
Some of the products secreted by platelets are depicted as:
ADP, adenosine diphosphate( 腺苷二磷酸 );
PDGF, platelet-derived growth factor( 血小板源性生长因子 );
vWF, von Willebrand factor.
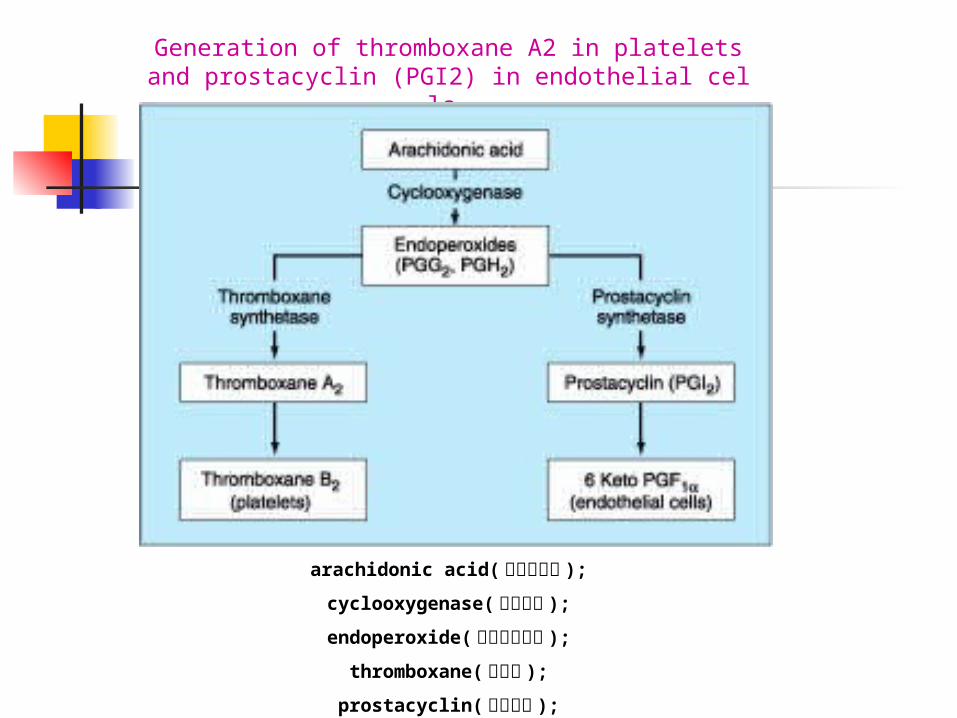
Generation of thromboxane A2 in platelets and prostacyclin (PGI2) in endothelial cells.
arachidonic acid( 花生四烯酸 );
cyclooxygenase( 环氧合酶 );
endoperoxide( 内皮过氧化酶 );
thromboxane( 血栓素 );
prostacyclin( 前列环素 );
Abnormalities of Blood Platelets
Quantitative platelets defects — BPC is low, as thrombocytopeni
a( 血小板减少症 ) with various causes
Qualitative platelets defects — Platelets dysfunction, as thromba
sthenia( 血小板无力 )
Causes of thrombocytopenia
Primary thrombocytopenia Immunologic thrombocytopenia(vir
al or bacterial infections) Drug-induced thrombocytopenia Hypersplenia( 脾功能亢进 ) Aplastic anemia( 再生障碍性贫血 ), le
ukemia( 白血病 )
Functional platelet disorders
Congenital : Thrombasthenia Giant platelet syndrome( 巨大血小板综合
征 )Acquired : Liver disease Uremia Drug-induced
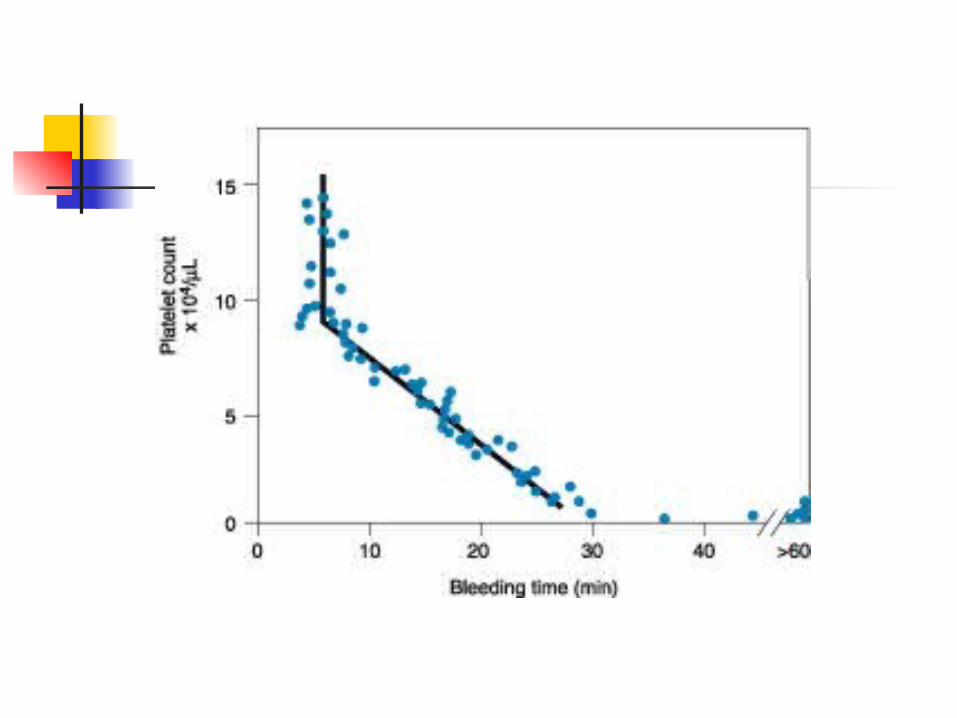
In platelet defects,bleeding time is prolonged and clot retraction is
poor.
Deficiency of coagulation factors
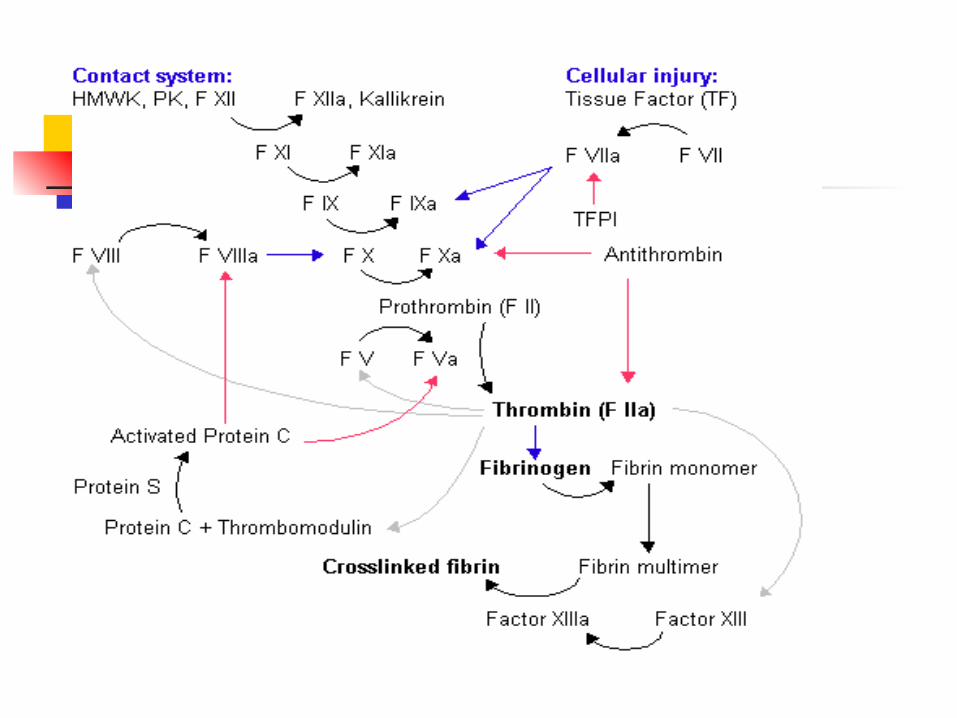
Coagulation process
First stage :the formation of activated thrombokinase( 凝血酶原激酶 ).
Second stage:thrombokinase converts prothrombin( 凝血酶原 ) into thrombin( 凝血酶 ).
Final stage: thrombin in turn converts fibrinogen( 纤维蛋白原 ) into fibrin( 纤维蛋白 ).
Congenital plasma coagulation
defects
Hemophilia A-dificiency of factor VIII
Hemophilia B-dificiency of factor IX
Hemophilia C-dificiency of factor XI
Deficiencies in factors V, VII, X, and prothrombin (factor II)
Acquired coagulation disorders Vitamin K deficiency(II, VII,IX, X) Liver disease Disseminated intravascular coagulation
(DIC) Complications of anticoagulant therapy
Vitamin K deficiency
Serves as a cofactor in the enzymatic carboxylation of glutamic acid( 谷氨酸 ) residues on prothrombin complex proteins (factors II, VII, IX, X; proteins C and S)
Plasma levels of all the prothrombin complex proteins decrease.
Vitamin K Deficiency
Inadequate dietary intake Intestinal mal-absorption Loss of storage sites due to hepatocellula
r disease
Coagulation Disorders in Liver Disease
Decreased production of coagulation proteins(II,VII,IX,X), and fibrinogen(factor I) and factor V
Some degree of vitamin K deficiency “Hypercoagulable" and predisposed to
developing DIC or systemic fibrinolysis.
Lab test of coagulation defect
PT PTT CT platelet count fibrinogen determination
Fibrinolytic system
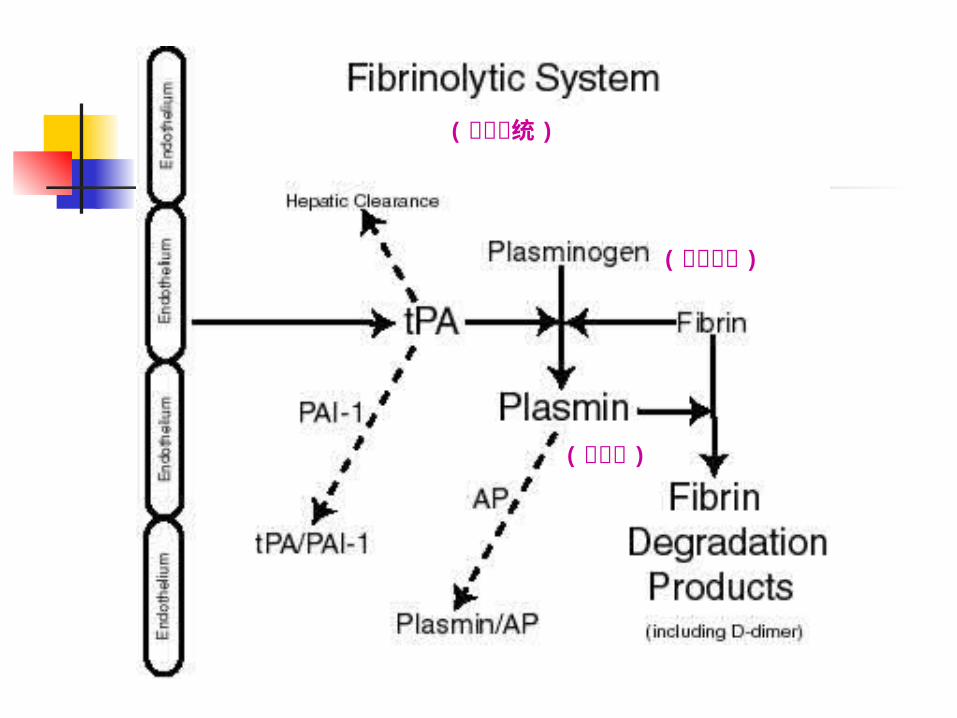
( 纤溶酶原 )
( 纤溶酶 )
( 纤溶系统 )
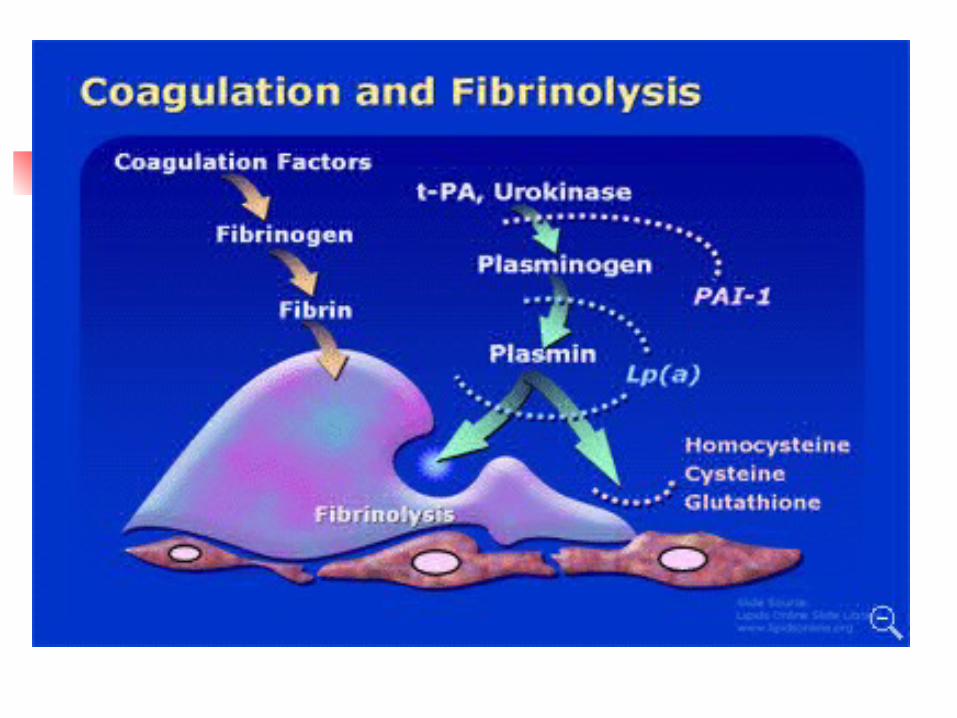
Defects in the fibrinolytic system a2 plasmin inhibitor deficiency or plasmi
nogen activator inhibitor (PAI) 1 Secondary fibrinolysis accompanying DIC
Increase of anti-coagulation substances
the increase of heparan anticogulants or the over-dosage of anticoagulants.
Types of Mucocutaneous hemorrhage
Petechia( 出血点 ; 瘀点 ): pinpoint hemorrhage
<2mm in diameter Purpura( 紫癜 ): > 3- 5mm in diameter Ecchymosis( 瘀斑 ): common bruise, >5mm Hematoma( 血肿 ): local elevation and fluct
uation Epistaxis( 鼻出血 ) Bleeding in skin, mucous membrane, joint
cavity and viscera( 内脏 ).
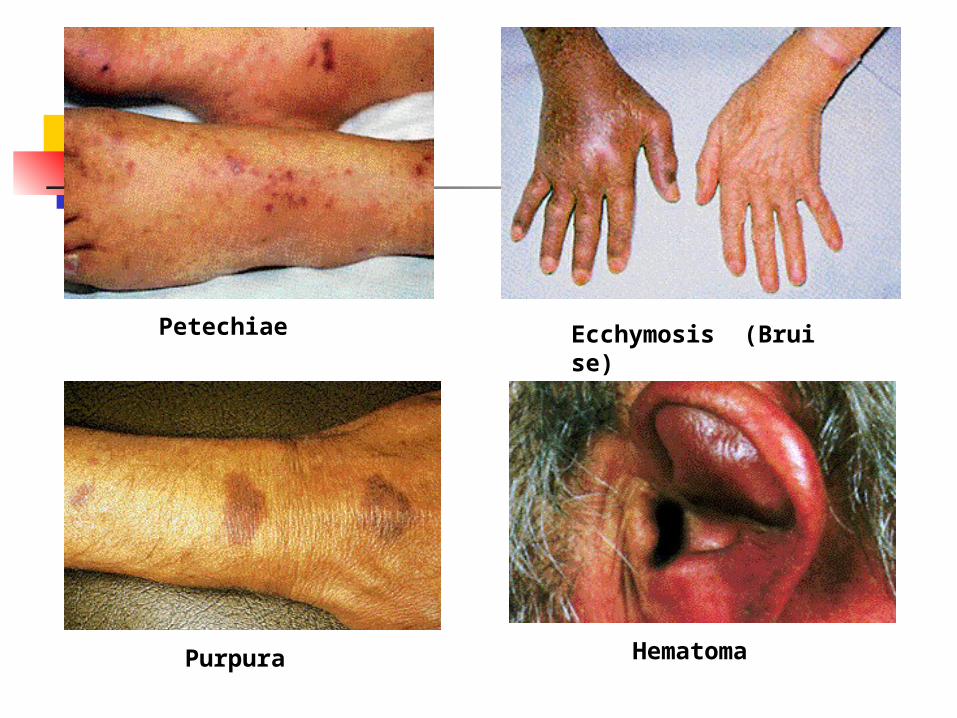
Petechiae
Purpura
Ecchymosis (Bruise)
Hematoma
Approach to patients with mucocutaneous hemorrhag
e
History-taking Age,male or female,onset of the disease Spontaneous or following trauma Past history of bleeding tendency, such
as bleeding after tooth extraction, Liver disease A family history of bleeding and bleedin
g from multiple sites, repeated episodes A record of drug ingestion
Physical examination
Bleeding should be traced over whole body, sometimes including urine and stool.
In addition, the jaundice and the size of liver and spleen should be noted.
Bleeding from a platelet disorder
Bleeding sites localized to superficial sites such as the skin and mucous membranes
Immediately after trauma or surgery
Readily controlled by local measures
Bleeding from plasma coagulation
defects Bleeding sites: in deep subcutaneous tissue
s, muscles, joints, or body cavities
time: hours or days after injury
Unaffected by local therapy
Laboratory routine tests Blood routine Blood platelet count Bleeding time (a sensitive measure of plat
elet function) Prothrombin time (PT, screens the extrin
sic limb of the coagulation system) Coagulation time
Bone marrow studyCoagulation factors determinationFibrinogen determination.
Screening tests
Specific tests