MSK Imaging_4.Imaging of muscle china_by Dr. Jim Wu
86
Imaging of Imaging of Muscle Muscle Jim Wu, MD Jim Wu, MD Beth Israel Deaconess Medical Center Beth Israel Deaconess Medical Center Harvard Medical School Harvard Medical School
-
Upload
wanfang-radiology -
Category
Health & Medicine
-
view
317 -
download
1
Transcript of MSK Imaging_4.Imaging of muscle china_by Dr. Jim Wu

Imaging of MuscleImaging of Muscle
Jim Wu, MDJim Wu, MDBeth Israel Deaconess Medical CenterBeth Israel Deaconess Medical Center
Harvard Medical SchoolHarvard Medical School

DisclosuresDisclosures
Kaneka Corp - research funding supportKaneka Corp - research funding support Boehringer Ingelheim - research funding Boehringer Ingelheim - research funding
supportsupport PharmaMar - imaging consultantPharmaMar - imaging consultant

Learning ObjectivesLearning Objectives
Understand skeletal muscle anatomy and Understand skeletal muscle anatomy and physiologyphysiology
Be able to recognize the imaging Be able to recognize the imaging appearance of various muscle injuriesappearance of various muscle injuries
Learn advanced imaging techniques to Learn advanced imaging techniques to study muscle study muscle

Skeletal MuscleSkeletal Muscle
((Garrett & Best. Ortho Basic Science AAOS 1994: 89-126)Garrett & Best. Ortho Basic Science AAOS 1994: 89-126)
More than 400 muscles in More than 400 muscles in the human bodythe human body
Constitutes 40-45% of Constitutes 40-45% of total body weighttotal body weight
Muscle injury is a leading Muscle injury is a leading cause of loss time from cause of loss time from workwork
https://www.bayesianbodybuiding.com

Skeletal Muscle AnatomySkeletal Muscle Anatomy
Muscle fiber is basic unit of Muscle fiber is basic unit of skeletal muscleskeletal muscle Capable only of contractingCapable only of contracting
Single nerve axon controls Single nerve axon controls one or more muscle fibers one or more muscle fibers to form motor unitto form motor unit
Site of connection between Site of connection between muscle fiber and tendon is muscle fiber and tendon is the myotendinous junctionthe myotendinous junction Weakest part of muscleWeakest part of muscle
Muscle fiber
Huard et al JBJS[Am] 2002; 84-A: 822

Types of Muscle ContractionTypes of Muscle Contraction ConcentricConcentric
Muscle force > resisting load Muscle force > resisting load Muscle shortens (contracts)Muscle shortens (contracts) Ex: biceps curlsEx: biceps curls
IsometricIsometric Muscle force = resisting loadMuscle force = resisting load Muscle length does not changeMuscle length does not change Ex: trying to lift a huge rockEx: trying to lift a huge rock
EccentricEccentric Muscle force < resisting loadMuscle force < resisting load Muscle lengthensMuscle lengthens Ex: jumping from a heightEx: jumping from a height

Types of Muscle ContractionTypes of Muscle Contraction
Movement is combination of concentric, Movement is combination of concentric, isometric, and eccentric muscle contractionisometric, and eccentric muscle contraction
More tension generated during eccentric More tension generated during eccentric contraction rendering the muscle more contraction rendering the muscle more susceptible to injurysusceptible to injury
Muscle tears occur during powerful Muscle tears occur during powerful eccentric contractioneccentric contraction
Garrett. Med Sci Sports Exerc 1990; 22: 436-443

Imaging of Muscle InjuryImaging of Muscle Injury
MRI is the best imaging testMRI is the best imaging test Allows for localization and Allows for localization and
characterization of injurycharacterization of injury ProtocolProtocol
T1 to assess for hemorrhage T1 to assess for hemorrhage and fatty atrophyand fatty atrophy
T2/STIR to assess for edemaT2/STIR to assess for edema Contrast not needed if tumor Contrast not needed if tumor
not suspectednot suspected
T1
STIR

Sites of Muscle InjurySites of Muscle Injury Tendon – boneTendon – bone
Apophyseal (growth plate)Apophyseal (growth plate) AvulsionAvulsion
Tendon Tendon TendinopathyTendinopathy Partial tearPartial tear Complete tearComplete tear
Myotendinous junctionMyotendinous junction Partial tear (strain)Partial tear (strain) RuptureRupture Delayed Onset Muscle Soreness Delayed Onset Muscle Soreness
(DOMS)(DOMS) Muscle bellyMuscle belly
Contusion/hematomaContusion/hematoma MyositisMyositis DenervationDenervation

Muscle Injury – Key pointsMuscle Injury – Key points Normal tendons do not ruptureNormal tendons do not rupture
Injuries often occur in muscles that cross 2 Injuries often occur in muscles that cross 2 jointsjoints Increase stress on muscleIncrease stress on muscle Rectus femoris, biceps, gastrocnemius, Rectus femoris, biceps, gastrocnemius,
hamstringshamstrings

Tendon-Bone Injury Tendon-Bone Injury
Common in kidsCommon in kids ClassificationClassification
AcuteAcute – violent muscle – violent muscle contraction contraction
ChronicChronic – repetitive – repetitive microtrauma (overuse)microtrauma (overuse)
Pelvic muscle insertions Pelvic muscle insertions most commonly injuredmost commonly injured
Can have aggressive Can have aggressive appearance mimicking appearance mimicking tumortumor

Tendon-Bone Injury (bony avulsion)Tendon-Bone Injury (bony avulsion)
Extensor tendon avulsion Peroneus brevis avulsion

Tendon-Bone Injury (bony avulsion):Tendon-Bone Injury (bony avulsion): Biceps femorisBiceps femoris
PD

Tendon-Bone Injury (apophyseal): Tendon-Bone Injury (apophyseal): Osgood SchlattersOsgood Schlatters
PD

Tendon-Bone Injury: Tendon-Bone Injury: Quadriceps tendon avulsionQuadriceps tendon avulsion
Normal PD T2 fat sat

Tendon-Bone Injury: Tendon-Bone Injury: Hamstrings avulsionHamstrings avulsion
STIR STIR

Tendon-Bone Injury: Tendon-Bone Injury: Pectoralis major tendon avulsionPectoralis major tendon avulsion
STIR T2 fat sat

Tendon-Bone Injury: Tendon-Bone Injury: Biceps tendon avulsionBiceps tendon avulsion
STIR STIR

Types of Muscle InjuryTypes of Muscle Injury Tendon – boneTendon – bone
Apophyseal (growth plate)Apophyseal (growth plate) AvulsionAvulsion
Tendon Tendon TendinopathyTendinopathy Partial tearPartial tear Complete tearComplete tear
Myotendinous junctionMyotendinous junction Partial tear (strain)Partial tear (strain) RuptureRupture Delayed Onset Muscle Soreness Delayed Onset Muscle Soreness
(DOMS)(DOMS) Muscle bellyMuscle belly
Contusion/hematomaContusion/hematoma MyositisMyositis DenervationDenervation

Tendon InjuryTendon Injury
Tendons are relatively avascular structures Tendons are relatively avascular structures which attach muscles to bonewhich attach muscles to bone
Made of dense collagen fibers which Made of dense collagen fibers which interdigitate to form extremely tight bondsinterdigitate to form extremely tight bonds
Dark on all sequences due to few mobile protonsDark on all sequences due to few mobile protons
Normal tendons do not tear!Normal tendons do not tear!
Several conditions can weaken and predispose Several conditions can weaken and predispose tendons to injurytendons to injury

Tendon InjuryTendon Injury
Predisposing conditions:Predisposing conditions: Chronic repetitive stresses (microtears)Chronic repetitive stresses (microtears) Tendon degeneration (age-related)Tendon degeneration (age-related) Inflammatory processesInflammatory processes
Rheumatoid arthritisRheumatoid arthritis SLESLE
InfectionInfection DiabetesDiabetes Drugs (steroids, ciprofloxacin)Drugs (steroids, ciprofloxacin)

Tendon Injury (tendinosis):Tendon Injury (tendinosis):Achilles tendonAchilles tendon
PD STIR

Tendon Injury (partial tear):Tendon Injury (partial tear):AchillesAchilles
T2 fat satPD

Tendon Injury (complete rupture):Tendon Injury (complete rupture):AchillesAchilles
T2 fat satPD

Tendon Injury (complete rupture):Tendon Injury (complete rupture):SupraspinatusSupraspinatus
Normal T1 fat sat

Types of Muscle InjuryTypes of Muscle Injury Tendon – boneTendon – bone
Apophyseal (growth plate)Apophyseal (growth plate) AvulsionAvulsion
Tendon Tendon TendinopathyTendinopathy Partial tearPartial tear Complete tearComplete tear
Myotendinous junctionMyotendinous junction Partial tear (strain)Partial tear (strain) RuptureRupture Delayed Onset Muscle Soreness Delayed Onset Muscle Soreness
(DOMS)(DOMS) Muscle bellyMuscle belly
Contusion/hematomaContusion/hematoma MyositisMyositis DenervationDenervation

Myotendinous Junction InjuryMyotendinous Junction Injury
Highly folded membrane at muscle-tendon Highly folded membrane at muscle-tendon interfaceinterface
Increases muscle-tendon contact by 15-20 timesIncreases muscle-tendon contact by 15-20 times
Majority of partial tears (strains) occur hereMajority of partial tears (strains) occur here
Due to eccentric contractionDue to eccentric contraction
Typically in muscles crossing 2 joints: Typically in muscles crossing 2 joints: biceps femoris, rectus femoris, gastrocnemiusbiceps femoris, rectus femoris, gastrocnemius Type II muscle fibersType II muscle fibers
(Garrett & Best. Ortho Basic Science AAOS 1994: 89-126Noonan & Garrett. Clin Sports Med 1992; 11:783-806)

Grading of Muscle StrainsGrading of Muscle Strains
Grade 1Grade 1: Edema in muscle and myotendinous : Edema in muscle and myotendinous junction without disruption of muscle fibers. No or junction without disruption of muscle fibers. No or minimal perifascial fluidminimal perifascial fluid
Grade 2Grade 2: Partial tear. Irregular fibers and associated : Partial tear. Irregular fibers and associated muscle edema. muscle edema. Hematoma (pathognomonic) Hematoma (pathognomonic) and and moderate perifascial fluidmoderate perifascial fluid
Low – less than 1/3 of area involvedLow – less than 1/3 of area involved Moderate – 1/3 to 2/3 Moderate – 1/3 to 2/3 High – greater than 2/3High – greater than 2/3
Grade 3Grade 3: Rupture of the myotendinous junction: Rupture of the myotendinous junction

Myotendinous Junction Injury: Myotendinous Junction Injury: Grade 1 muscle strainGrade 1 muscle strain
Key Point: Myotendinous junction is weakest part of skeletal muscle

Myotendinous Junction Myotendinous Junction Injury: Grade 2 (Partial tear)Injury: Grade 2 (Partial tear)
T1 STIR
STIR
Hemorrhage indicates at least a Grade 2 injury

Myotendinous Junction Myotendinous Junction Injury: Grade 2 (Partial tear)Injury: Grade 2 (Partial tear)
STIRT1

Myotendinous Junction Injury – Myotendinous Junction Injury – Grade 3 (Complete Tear)Grade 3 (Complete Tear)
STIR STIR

Myotendinous Junction Injury – Myotendinous Junction Injury – Grade 3 (Complete Tear)Grade 3 (Complete Tear)
STIR T2 fat sat

Delayed Onset Muscle Soreness Delayed Onset Muscle Soreness (DOMS)(DOMS)
Muscle pain and soreness following renewed or Muscle pain and soreness following renewed or unaccustomed exerciseunaccustomed exercise
Pain peaks after 12-48 hours following exercise eventPain peaks after 12-48 hours following exercise event
Symptoms depend on:Symptoms depend on: Exercise durationExercise duration Exercise intensityExercise intensity
Stretching prior to exercise has not been shown to Stretching prior to exercise has not been shown to reduce symptomsreduce symptoms
Stretching and massage does not shorten recovery timeStretching and massage does not shorten recovery time But feels GOOD!But feels GOOD!

Delayed Onset Muscle Soreness Delayed Onset Muscle Soreness (DOMS)(DOMS)
Normal response by muscle which will lead to Normal response by muscle which will lead to increase muscle strength and staminaincrease muscle strength and stamina
Grade 1 muscle strain due to microscopic tears Grade 1 muscle strain due to microscopic tears at the myotendinous junctionat the myotendinous junction
Can be associated with increase in serum Can be associated with increase in serum creatine kinase levelscreatine kinase levels
Rhabdomyolysis in rare severe casesRhabdomyolysis in rare severe cases

Delayed Onset Muscle Soreness Delayed Onset Muscle Soreness (DOMS)(DOMS)
CPK >7000 IU/L (nl range <150 IU/L)CPK >7000 IU/L (nl range <150 IU/L)
STIRSTIR

Delayed Onset Muscle Delayed Onset Muscle Soreness (DOMS)Soreness (DOMS)
STIR

Types of Muscle InjuryTypes of Muscle Injury Tendon – boneTendon – bone
Apophyseal (growth plate)Apophyseal (growth plate) AvulsionAvulsion
Tendon Tendon TendinopathyTendinopathy Partial tearPartial tear Complete tearComplete tear
Myotendinous junctionMyotendinous junction Partial tear (strain)Partial tear (strain) RuptureRupture Delayed Onset Muscle Soreness Delayed Onset Muscle Soreness
(DOMS)(DOMS) Muscle bellyMuscle belly
Contusion/hematomaContusion/hematoma MyositisMyositis DenervationDenervation

Muscle Belly Injury - ContusionMuscle Belly Injury - Contusion
Result of blunt traumaResult of blunt trauma Edema and Edema and
hemorrhage seen as hemorrhage seen as high T2 signal in the high T2 signal in the musclemuscle
Hemorrhage as high Hemorrhage as high T1 signalT1 signal
Often adjacent to Often adjacent to bonebone
STIR

Muscle Belly Injury - ContusionMuscle Belly Injury - Contusion
STIRT1

Muscle Belly Injury - ContusionMuscle Belly Injury - Contusion
STIR

Muscle Belly Injury - MyositisMuscle Belly Injury - Myositis
Inflammation of skeletal muscleInflammation of skeletal muscle Many causesMany causes Associated with pain and muscle weaknessAssociated with pain and muscle weakness Elevated serum creatine kinase and other Elevated serum creatine kinase and other
markers of muscle damagemarkers of muscle damage Imaging findings are non-specificImaging findings are non-specific
High signal on edema-sensitive MR sequencesHigh signal on edema-sensitive MR sequences

Autoimmune diseaseAutoimmune disease PolymyositisPolymyositis DermatomyositisDermatomyositis Inclusion bodyInclusion body
InfectionInfection HIVHIV LymeLyme ParasitesParasites
Trauma Trauma MedicationsMedications
StatinsStatins AlcoholAlcohol SteroidsSteroids
IdiopathicIdiopathic
Muscle Belly Injury - CausesMuscle Belly Injury - Causes

PolymyositisPolymyositis
STIRSTIR
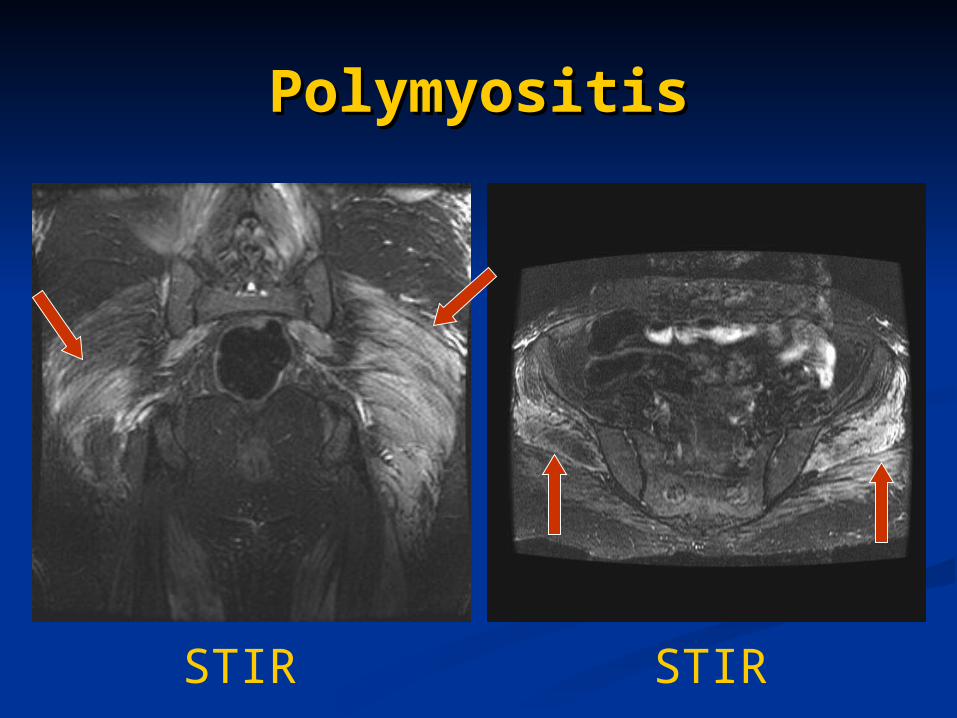
PolymyositisPolymyositis
STIRSTIR

Statin MyopathyStatin Myopathy
STIRSTIR

Muscle Belly Injury: DenervationMuscle Belly Injury: Denervation
Loss of stimulus to muscleLoss of stimulus to muscle Nerve/muscle interfaceNerve/muscle interface Secondary to myotendinous Secondary to myotendinous
unit ruptureunit rupture
Imaging findings in Imaging findings in denervationdenervation Early: normal signal, normal Early: normal signal, normal
bulkbulk Subacute: high signal on T2 Subacute: high signal on T2
(edema), normal/decrease (edema), normal/decrease bulkbulk
Chronic: high signal on T1 Chronic: high signal on T1 (fatty atrophy), decrease bulk(fatty atrophy), decrease bulk

Deltoid Muscle Denervation Following Deltoid Muscle Denervation Following Rotator Cuff RepairRotator Cuff Repair
PD STIR

Supraspinatus Muscle AtrophySupraspinatus Muscle Atrophy
T2 fat satNormal

Supraspinatus Muscle AtrophySupraspinatus Muscle Atrophy
Normal T2 FSE

Fatty Atrophy from PolioFatty Atrophy from Polio
T1 T1

Sites of Muscle InjurySites of Muscle Injury Tendon – boneTendon – bone
Apophyseal (growth plate)Apophyseal (growth plate) AvulsionAvulsion
Tendon Tendon TendinopathyTendinopathy Partial tearPartial tear Complete tearComplete tear
Myotendinous junctionMyotendinous junction Partial tear (strain)Partial tear (strain) RuptureRupture Delayed Onset Muscle Soreness Delayed Onset Muscle Soreness
(DOMS)(DOMS) Muscle bellyMuscle belly
Contusion/hematomaContusion/hematoma MyositisMyositis DenervationDenervation

Imaging of Muscle disordersImaging of Muscle disorders
Imaging studies are often normal despite Imaging studies are often normal despite symptomssymptoms
When imaging findings are present, they can be When imaging findings are present, they can be non-specificnon-specific
CK typically normal unless severe disease CK typically normal unless severe disease despite clinical symptomsdespite clinical symptoms
Makes diagnosis of the muscle disease difficultMakes diagnosis of the muscle disease difficult Need for better imaging tests to assess muscle Need for better imaging tests to assess muscle
diseases!!diseases!!

Novel imaging techniques to Novel imaging techniques to evaluate muscle disordersevaluate muscle disorders
Advance MRI techniquesAdvance MRI techniques 3131P MR SpectroscopyP MR Spectroscopy
Quantitative ultrasound (QU)Quantitative ultrasound (QU) Muscle echointensity Muscle echointensity

Advanced MR technique – 31P MR Spectroscopy
Uses Uses 3131Phosphorus Phosphorus imaging instead of imaging instead of 11HH
Many muscle Many muscle metabolites contain metabolites contain phosphorusphosphorus
Concentration of muscle Concentration of muscle metabolites directly metabolites directly related to mitochondrial related to mitochondrial function and muscle function and muscle healthhealth

Advanced MR technique – 31P MR Spectroscopy
ATPATP – energy rich compound – energy rich compound needed for muscle contraction needed for muscle contraction
Phosphocreatine (PCr)Phosphocreatine (PCr) Crucial energy store in skeletal Crucial energy store in skeletal
musclemuscle decreases in exercisedecreases in exercise
Phophosdiesterase (PDE)Phophosdiesterase (PDE) Breakdown product of cell Breakdown product of cell
membranesmembranes increases with high cell turnoverincreases with high cell turnover
Inorganic phosphate (Pi)Inorganic phosphate (Pi) Byproduct of PCr during muscle Byproduct of PCr during muscle
contractioncontraction increases with exerciseincreases with exercise


RestingResting
Peak Peak ExerciseExercise

Time
Pipinos et al J Vasc Surg 2000;31:944-952


Statins are used to lower cholesterol, but associated Statins are used to lower cholesterol, but associated with calf pain in 5-10% of patientswith calf pain in 5-10% of patients
Cause is not fully understoodCause is not fully understood 10 patients given statins for 4 weeks10 patients given statins for 4 weeks Studied the effects of statins on mitochondrial function Studied the effects of statins on mitochondrial function
and phosphocreatine (PCr) recovery with and phosphocreatine (PCr) recovery with 3131P MR P MR spectroscopy (before and after statin use)spectroscopy (before and after statin use)
Significant drop in PCr recovery after 4 weeksSignificant drop in PCr recovery after 4 weeks Conclusion – Statins weaken mitochondrial functionConclusion – Statins weaken mitochondrial function

PCR recovery after cessation of exercise
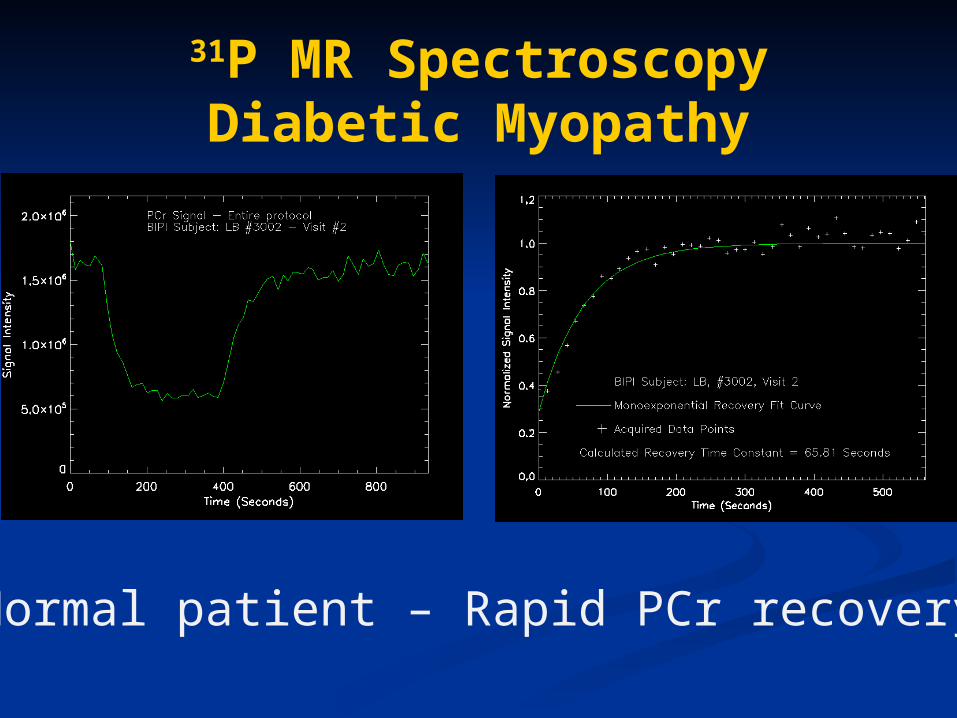
31P MR SpectroscopyDiabetic Myopathy
Normal patient – Rapid PCr recovery

31P MR SpectroscopyDiabetic Myopathy
Diabetic Myopathy – blunted PCr recovery

Quantitative UltrasoundQuantitative Ultrasound
Diseased muscle (especially in neuromuscular Diseased muscle (especially in neuromuscular disorders) is often echogenic due to fibrosis and disorders) is often echogenic due to fibrosis and fatty infiltrationfatty infiltration
Technique assesses muscle health by Technique assesses muscle health by measuring the echointensity of the musclemeasuring the echointensity of the muscle
Easy to use: painless, quick, no radiationEasy to use: painless, quick, no radiation

Neuromuscular disorders (NMD)Neuromuscular disorders (NMD)
Patients with have disruption of normal muscle architecture with infiltration of fat and connective tissue
Have decreased muscle thickness and increased subcutaneous fat thickness when compared to controls
Normal With NMD

Infiltration of fat and connective tissue into muscle increases the number of reflective interfaces
PathophysiologyPathophysiology
a. Normal subject b. Patient with spinal muscular atrophy
Subcutaneous Fat
Fascia
Muscle
Bone
Diseased muscleMore echogenic
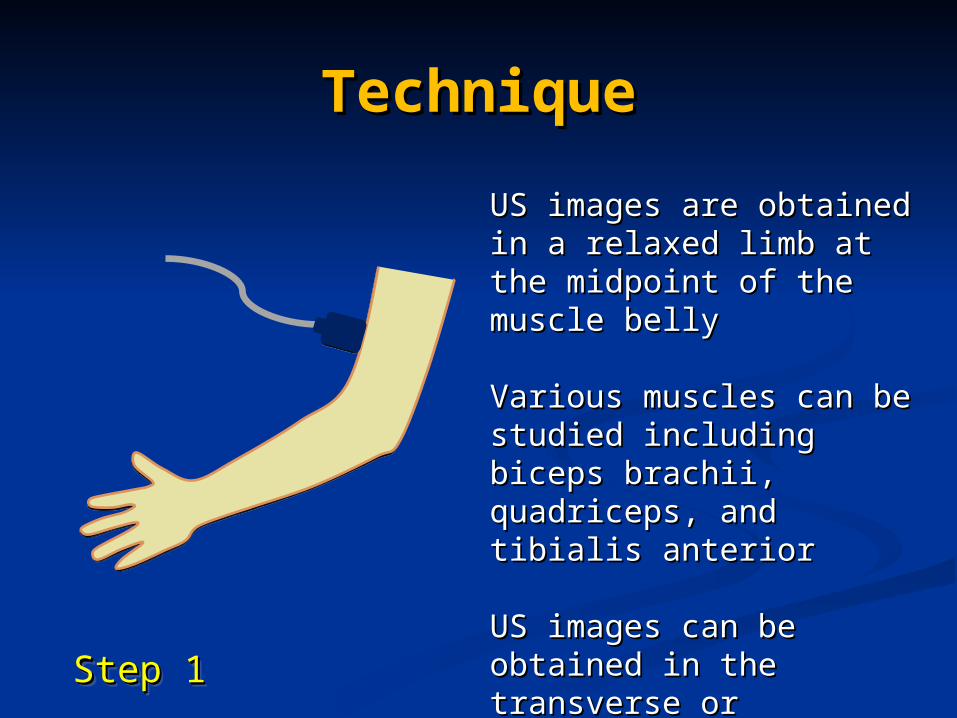
TechniqueTechnique
Step 1Step 1Step 1Step 1
US images are obtained in a US images are obtained in a relaxed limb relaxed limb at the midpoint at the midpoint of the muscle belly of the muscle belly
Various muscles can be Various muscles can be studied including biceps studied including biceps brachii, quadriceps, and brachii, quadriceps, and tibialis anteriortibialis anterior
US images US images can be obtained can be obtained in the transverse or in the transverse or longitudinal positionslongitudinal positions

Gain, compression, and Gain, compression, and time gain compensation time gain compensation kept constantkept constant
TechniqueTechnique
Step 1 continuedStep 1 continuedStep 1 continuedStep 1 continued

Subcutaneous skin thickness measured using electronic calipers
TechniqueTechnique
Step 1 continuedStep 1 continued
Measurements taken from the interface between the dermis and superficial fascia

US images are transferred to photo analysis software program
TechniqueTechnique
Step 2 continuedStep 2 continued

TechniqueTechnique
Step 2 continuedStep 2 continued
1) Place regions of interest in the subcutaneous fat
2) Apply grayscale histogram function
3) Take median value = 32
Quantify tissue luminosity:
Normal subject

TechniqueTechnique
Step 2 continuedStep 2 continued
1) Repeat steps with muscle. Exclude placing region of interest over fascia and muscle tendon transitions.
2) Apply grayscale histogram function.
3) Take median value = 38
Quantify tissue luminosity:
Normal subject

Calculate luminosity ratio (LR) :Divide muscle luminosity value (LV) by the overlying
subcutaneous fat luminosity value
TechniqueTechnique
Step 3Step 3
Normal subject

TechniqueTechnique
1) Place regions of interest in the subcutaneous fat
2) Apply grayscale histogram function
3) Take median value--36
Quantify tissue luminosity:
Distance 1.50
Patient with spinal muscular atrophy

TechniqueTechnique
1) Place regions of interest in the muscle
2) Apply grayscale histogram function
3) Take median value--88
Quantify tissue luminosity:
Distance 1.50
Patient with spinal muscular atrophy
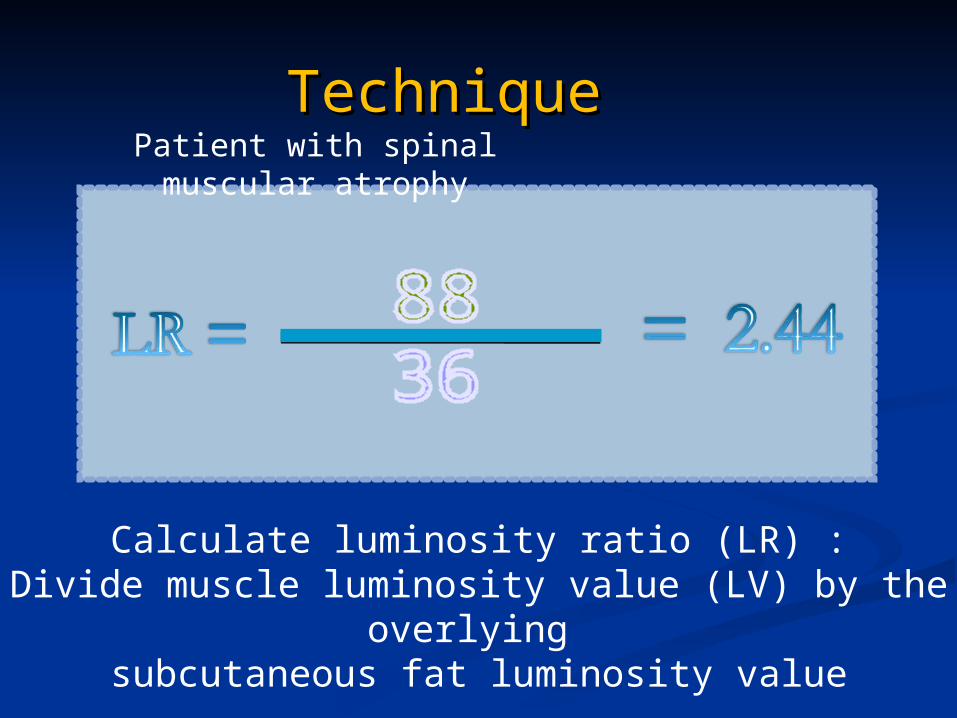
TechniqueTechnique Patient with spinal muscular atrophy
Calculate luminosity ratio (LR) :Divide muscle luminosity value (LV) by the overlying
subcutaneous fat luminosity value

Evaluated 25 pts with SMA and 21 normal controls from the Evaluated 25 pts with SMA and 21 normal controls from the spinal muscular atrophy clinic at Children’s Hospital Bostonspinal muscular atrophy clinic at Children’s Hospital Boston
Luminosity ratio for 4 muscle groups (biceps, wrist extensors, Luminosity ratio for 4 muscle groups (biceps, wrist extensors, quadriceps, and tibialis anterior) had a significant correlation quadriceps, and tibialis anterior) had a significant correlation with worsening diseasewith worsening disease
Able to distinguish between SMA subtypes 3 (walkers) and 2 Able to distinguish between SMA subtypes 3 (walkers) and 2 (sitters) using the luminosity ratio(sitters) using the luminosity ratio

Normal Type 2 SMAType 3 SMA
LR: 1.19 LR: 2.44 LR: 5.31
Spinal Muscular AtrophyQuadriceps muscle
Echointensity increases with worsening muscle disease

Duchenne Muscular DystrophyDuchenne Muscular DystrophyBiceps brachii muscleBiceps brachii muscle
Increased muscle Increased muscle echogenicityechogenicity

Becker Muscular DystrophyBecker Muscular Dystrophy
21 yrs21 yrs 17 yrs17 yrs 15 yrs15 yrs
Quadriceps muscleQuadriceps muscle
Three brothers with Becker Muscular Dystrophy and normal strengthThree brothers with Becker Muscular Dystrophy and normal strength

Amyotrophic Lateral SclerosisAmyotrophic Lateral Sclerosis
72 year-old with ALS72 year-old with ALS
Biceps brachii muscleBiceps brachii muscle
Subcutaneous fatSubcutaneous fat

SummarySummary Skeletal muscle is a unique and dynamic organSkeletal muscle is a unique and dynamic organ Injuries can be classified by their location in the Injuries can be classified by their location in the
muscle-tendon-bone unitmuscle-tendon-bone unit Tendon-bone (weakest in children)Tendon-bone (weakest in children) TendonTendon Myotendinous junction (weakest in adults)Myotendinous junction (weakest in adults) Muscle bellyMuscle belly
Injuries often occur in muscles that cross 2 jointsInjuries often occur in muscles that cross 2 joints MR is the best conventional imaging test to MR is the best conventional imaging test to
localize and characterize muscle injurieslocalize and characterize muscle injuries

SummarySummary
Findings on conventional imaging studies can be Findings on conventional imaging studies can be normal despite clinical symptomsnormal despite clinical symptoms
Advanced imaging techniques can better assess Advanced imaging techniques can better assess skeletal muscle disordersskeletal muscle disorders 31P-MR spectroscopy31P-MR spectroscopy Quantitative ultrasoundQuantitative ultrasound

ReferencesReferences Garrett & Best. Ortho Basic Science AAOS 1994: 89-126)Garrett & Best. Ortho Basic Science AAOS 1994: 89-126) Huard et al JBJS[Am] 2002; 84-A: 822Huard et al JBJS[Am] 2002; 84-A: 822 Zaraiskaya et al. JMRI 2006; 24:402–408 Zaraiskaya et al. JMRI 2006; 24:402–408 Elsayes et al. Curr Prob in Diag Radiol2006;35(5):206-212Elsayes et al. Curr Prob in Diag Radiol2006;35(5):206-212 Noonan & Garrett. Clin Sports Med 1992; 11:783-806)Noonan & Garrett. Clin Sports Med 1992; 11:783-806) Garrett. Med Sci Sports Exerc 1990; 22: 436-443Garrett. Med Sci Sports Exerc 1990; 22: 436-443 Subhawong et al. RadioGraphics 2014; 34:1163–1177Subhawong et al. RadioGraphics 2014; 34:1163–1177 Kuo and Carrino. Curr Opin Rheumatol 19:530–535Kuo and Carrino. Curr Opin Rheumatol 19:530–535 Budzik et al. RadioGraphics 2014; 34:E56–E72Budzik et al. RadioGraphics 2014; 34:E56–E72 Costa et al. Muscle Nerve 46: 465–481, 2012Costa et al. Muscle Nerve 46: 465–481, 2012 Kassarjian et al. European Journal of Radiology 81 (2012) 3763– 3771Kassarjian et al. European Journal of Radiology 81 (2012) 3763– 3771 Shelly et al. Magn Reson Imaging Clin N Am 17 (2009) 757–773Shelly et al. Magn Reson Imaging Clin N Am 17 (2009) 757–773 Olsen et al. Current Rheumatology Reports 2005, 7:106–114Olsen et al. Current Rheumatology Reports 2005, 7:106–114 Wu et al. Neurology. 2010; 75(6):526-31. Wu et al. Neurology. 2010; 75(6):526-31. Wu et al. Muscle and Nerve. 2011; 43:76-81.Wu et al. Muscle and Nerve. 2011; 43:76-81.

謝謝聆聽