Ms. Pickles & the Meet, Ms. Pickles...
7
6/20/2010 1 Ms. Pickles & the ENTEROCUTANEOUS FISTULA Anna C. Graml April 26, 2010 NUTN 515 Meet, Ms. Pickles A 42 year old, morbidly obese woman, sent from a SNF s/p Small Bowel Obstruction (SBO) & Resection Anastomosis 8 mo ago which was complicated by an Anastomotic Leak, Pelvic Abscess & an Enterocutaneous Fistula (ECF) A Preview A Familiar Face Operations & Complications Management and Treatment Options Nutritional Approaches (as suggested by the literature) Nutritional Assessment Story Time In A Nut Shell References Purple= Associated with Ms. Pickles case A familiar face to the OHSU squad Date Reason for Admit/Procedure Complications/ Action Taken 2000 Large B Cell Lymphoma s/p RCHOP, Cholecystectomy 2005 Ventral Hernia Repair c/b dehiscence Sept 2, 2009 SB Obstruction from phytobezor—impacted pickles SB Resection High-output on POD2. C/b anastomotic leak, fungemia, bacteremia. Candida Parasilosis fungemia. Fluid collections in abdominal cavity. Intra- abdominal abscess. Sept 7 Repair: small bowel anastomosis Sept 19 Ex -Lap TPN. Post-op Ex-Lap c/b ECF Oct 18 Ex-Lap pelvic abscess Anastomatic leak & Pelvic abscess Jan 2010 Intense fevers, chills, sweats, fatigue, malaise, dirty blood/urine Bacteria d/t infected PICC line, line sepsis, ECF, skin infection, malnutrition. Open abd wound surrounding piece of bowel w/ multiple fistulas Feb 2010 N/V/tachycardia, fever Fistula bleeding (1 st time); visible. Peristalsis veg matter found in large ECF. Hct 25.7. March 2010 Fever 102F, Delirium, UTI, Abd pain, N/V. Sepsis Groshong infections, persistent rising of bacterima & fungemia Small Bowel Obstruction & Resection Obstruction- blockage of the bowel Mechanical Something got in the way Resection- removal of small bowel/intestine Anastomosis Normal Bowel Anastomosis Obstruction Phytobezoar Anastomotic Leak Ruptured intestinal anastomosis 5-7 days post-op Anemia, malnutrition, & vit deficiencies Sepsis, UTI, wound infection, excessive wound drainage, tachycardia, respiratory infections Ms. Pickles started on TPN for the 1 st time Results with sepsis, intra-abdominal infection, abscess, fistula, wound dehiscence, reoperation
Transcript of Ms. Pickles & the Meet, Ms. Pickles...
6/20/2010
1
Ms. Pickles & the ENTEROCUTANEOUS
FISTULA
Anna C. GramlApril 26, 2010NUTN 515
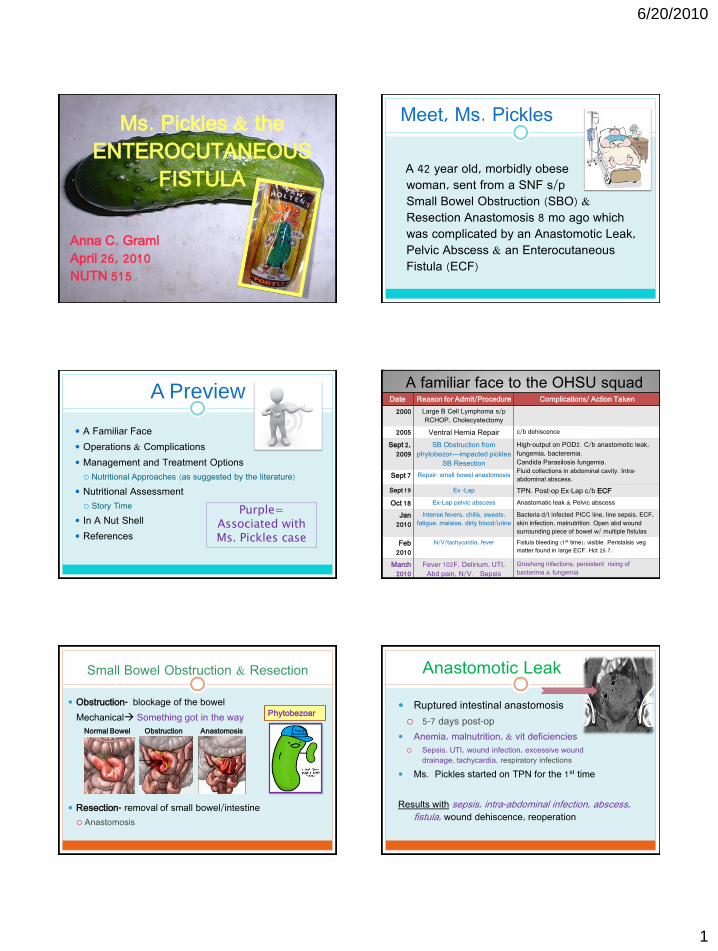
Meet, Ms. Pickles
A 42 year old, morbidly obese woman, sent from a SNF s/p Small Bowel Obstruction (SBO) & Resection Anastomosis 8 mo ago which was complicated by an Anastomotic Leak, Pelvic Abscess & an Enterocutaneous Fistula (ECF)
A Preview
A Familiar Face
Operations & Complications
Management and Treatment Options
Nutritional Approaches (as suggested by the literature)
Nutritional Assessment
Story Time
In A Nut Shell
References
Purple= Associated withMs. Pickles case
A familiar face to the OHSU squadDate Reason for Admit/Procedure Complications/ Action Taken
2000 Large B Cell Lymphoma s/p RCHOP, Cholecystectomy
2005 Ventral Hernia Repair c/b dehiscence
Sept 2, 2009
SB Obstruction from phytobezor—impacted pickles
SB Resection
High-output on POD2. C/b anastomotic leak, fungemia, bacteremia. Candida Parasilosis fungemia. Fluid collections in abdominal cavity. Intra-abdominal abscess. Sept 7 Repair: small bowel anastomosis
Sept 19 Ex -Lap TPN. Post-op Ex-Lap c/b ECF
Oct 18 Ex-Lap pelvic abscess Anastomatic leak & Pelvic abscess
Jan 2010
Intense fevers, chills, sweats, fatigue, malaise, dirty blood/urine
Bacteria d/t infected PICC line, line sepsis, ECF, skin infection, malnutrition. Open abd wound surrounding piece of bowel w/ multiple fistulas
Feb 2010
N/V/tachycardia, fever Fistula bleeding (1st time); visible. Peristalsis vegmatter found in large ECF. Hct 25.7.
March 2010
Fever 102F, Delirium, UTI, Abd pain, N/V. Sepsis
Groshong infections, persistent rising of bacterima & fungemia
Small Bowel Obstruction & Resection
Obstruction- blockage of the bowel
Mechanical Something got in the way
Resection- removal of small bowel/intestine
Anastomosis
Normal Bowel AnastomosisObstruction
Phytobezoar
Anastomotic Leak
Ruptured intestinal anastomosis
5-7 days post-op
Anemia, malnutrition, & vit deficiencies Sepsis, UTI, wound infection, excessive wound
drainage, tachycardia, respiratory infections
Ms. Pickles started on TPN for the 1st time
Results with sepsis, intra-abdominal infection, abscess, fistula, wound dehiscence, reoperation
6/20/2010
2
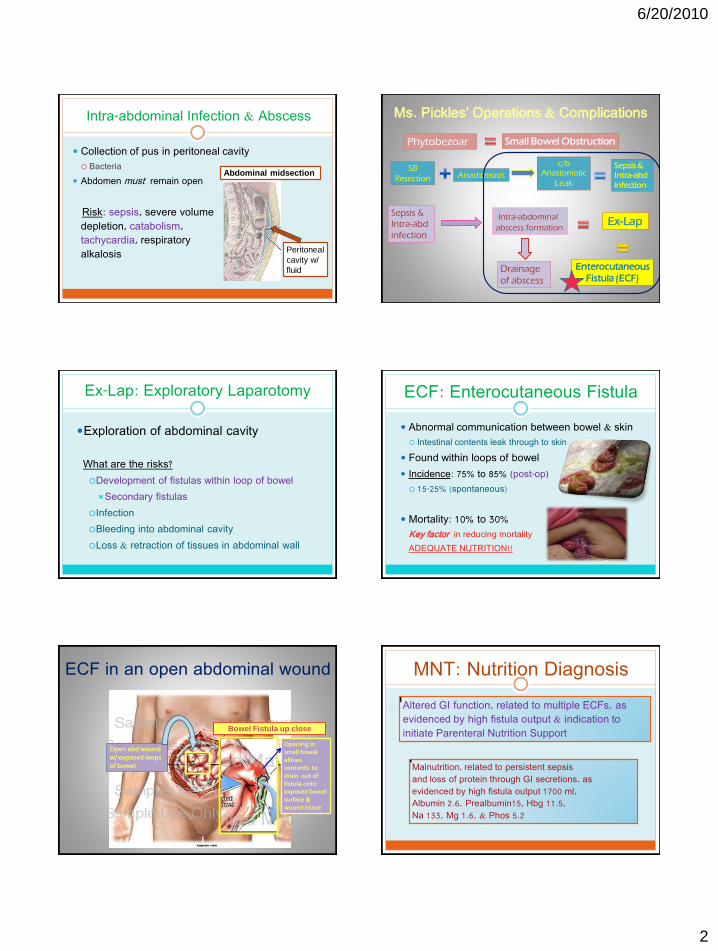
Intra-abdominal Infection & Abscess
Collection of pus in peritoneal cavity Bacteria
Abdomen must remain open
Risk: sepsis, severe volume depletion, catabolism, tachycardia, respiratory alkalosis Peritoneal
cavity w/
fluid
Abdominal midsection
Ms. Pickles’ Operations & Complications
Phytobezoar
SB
Resection
Small Bowel Obstruction
c/b
Anastomotic
Leak
Sepsis &
Intra-abd
infection
Sepsis &
Intra-abd
infection
Ex-LapIntra-abdominal
abscess formation
Drainage
of abscess
Enterocutaneous
Fistula (ECF)
Anastomosis
Ex-Lap: Exploratory Laparotomy
Exploration of abdominal cavity
What are the risks?
Development of fistulas within loop of bowel
Secondary fistulas
Infection
Bleeding into abdominal cavity
Loss & retraction of tissues in abdominal wall
ECF: Enterocutaneous Fistula
Abnormal communication between bowel & skin Intestinal contents leak through to skin
Found within loops of bowel
Incidence: 75% to 85% (post-op)
15-25% (spontaneous)
Mortality: 10% to 30%Key factor in reducing mortality
ADEQUATE NUTRITION!!
ECF in an open abdominal wound
Open abd wound w/ exposed loops of bowel
Opening in small bowel allows contents to drain out of fistula onto exposed bowel surface & wound tissue
Bowel Fistula up close
MNT: Nutrition Diagnosis
Altered GI function, related to multiple ECFs, as evidenced by high fistula output & indication to initiate Parenteral Nutrition Support
Malnutrition, related to persistent sepsisand loss of protein through GI secretions, asevidenced by high fistula output 1700 ml, Albumin 2.6, Prealbumin15, Hbg 11.5, Na 133, Mg 1.6, & Phos 5.2
6/20/2010
3
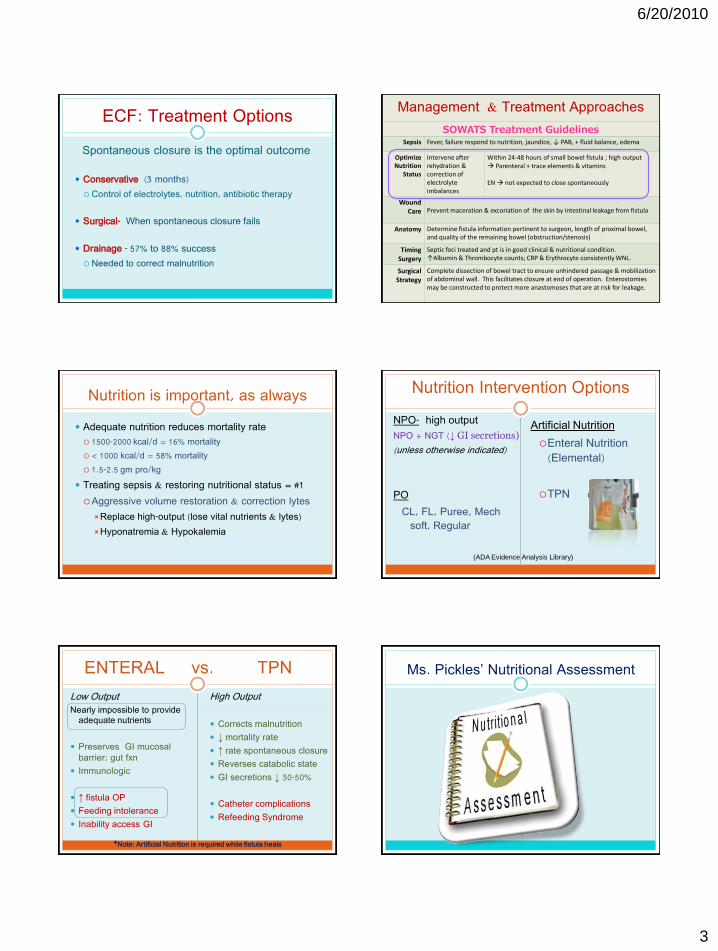
ECF: Treatment Options
Spontaneous closure is the optimal outcome
Conservative (3 months)
Control of electrolytes, nutrition, antibiotic therapy
Surgical- When spontaneous closure fails
Drainage - 57% to 88% success
Needed to correct malnutrition
Management & Treatment Approaches
SOWATS Treatment GuidelinesSepsis Fever, failure respond to nutrition, jaundice, ↓ PAB, + fluid balance, edema
Optimize Nutrition
Status
Intervene after rehydration & correction of electrolyte imbalances
Within 24-48 hours of small bowel fistula ; high output Parenteral + trace elements & vitamins
EN not expected to close spontaneously
Wound Care Prevent maceration & excoriation of the skin by intestinal leakage from fistula
Anatomy Determine fistula information pertinent to surgeon, length of proximal bowel, and quality of the remaining bowel (obstruction/stenosis)
Timing Surgery
Septic foci treated and pt is in good clinical & nutritional condition.↑Albumin & Thrombocyte counts; CRP & Erythrocyte consistently WNL.
Surgical Strategy
Complete dissection of bowel tract to ensure unhindered passage & mobilization of abdominal wall. This facilitates closure at end of operation. Enterostomies may be constructed to protect more anastomoses that are at risk for leakage.
Nutrition is important, as always
Adequate nutrition reduces mortality rate
1500-2000 kcal/d = 16% mortality
< 1000 kcal/d = 58% mortality
1.5-2.5 gm pro/kg
Treating sepsis & restoring nutritional status = #1
Aggressive volume restoration & correction lytes
Replace high-output (lose vital nutrients & lytes)
Hyponatremia & Hypokalemia
Nutrition Intervention Options
NPO- high output
NPO + NGT (↓ GI secretions)
(unless otherwise indicated)
PO
CL, FL, Puree, Mechsoft, Regular
Artificial Nutrition
Enteral Nutrition (Elemental)
TPN
(ADA Evidence Analysis Library)
ENTERAL vs. TPN
Low OutputNearly impossible to provide
adequate nutrients
Preserves GI mucosal barrier; gut fxn
Immunologic
↑ fistula OP
Feeding intolerance
Inability access GI
High Output
Corrects malnutrition
↓ mortality rate
↑ rate spontaneous closure
Reverses catabolic state
GI secretions ↓ 30-50%
Catheter complications
Refeeding Syndrome
*Note: Artificial Nutrition is required while fistula heals
Ms. Pickles’ Nutritional Assessment
6/20/2010
4
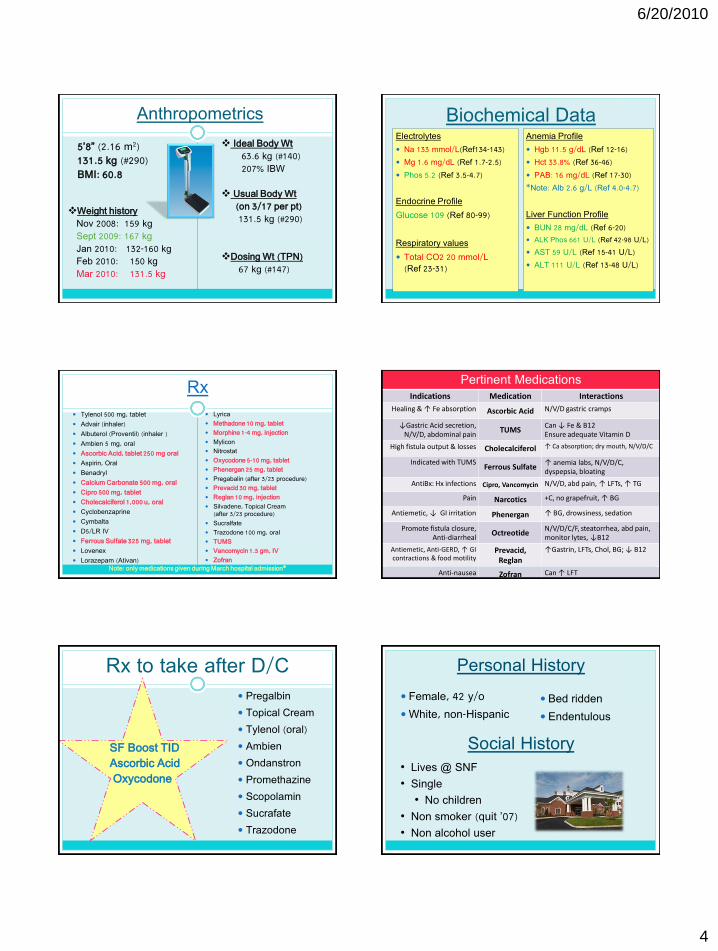
Anthropometrics
5’8” (2.16 m2)131.5 kg (#290)BMI: 60.8
Weight historyNov 2008: 159 kgSept 2009: 167 kgJan 2010: 132-160 kgFeb 2010: 150 kgMar 2010: 131.5 kg
Ideal Body Wt63.6 kg (#140)207% IBW
Usual Body Wt (on 3/17 per pt)131.5 kg (#290)
Dosing Wt (TPN)67 kg (#147)
Biochemical DataElectrolytes
Na 133 mmol/L(Ref134-143)
Mg 1.6 mg/dL (Ref 1.7-2.5)
Phos 5.2 (Ref 3.5-4.7)
Endocrine Profile
Glucose 109 (Ref 80-99)
Respiratory values
Total CO2 20 mmol/L(Ref 23-31)
Anemia Profile
Hgb 11.5 g/dL (Ref 12-16)
Hct 33.8% (Ref 36-46)
PAB: 16 mg/dL (Ref 17-30)
*Note: Alb 2.6 g/L (Ref 4.0-4.7)
Liver Function Profile
BUN 28 mg/dL (Ref 6-20)
ALK Phos 661 U/L (Ref 42-98 U/L)
AST 59 U/L (Ref 15-41 U/L)
ALT 111 U/L (Ref 13-48 U/L)
Rx Tylenol 500 mg, tablet
Advair (inhaler)
Albuterol (Proventil) (inhaler )
Ambien 5 mg, oral
Ascorbic Acid, tablet 250 mg oral
Aspirin, Oral
Benadryl
Calcium Carbonate 500 mg, oral
Cipro 500 mg, tablet
Cholecalciferol 1,000 u, oral
Cyclobenzaprine
Cymbalta
D5/LR IV
Ferrous Sulfate 325 mg, tablet
Lovenex
Lorazepam (Ativan)
Lyrica
Methadone 10 mg, tablet
Morphine 1-4 mg, injection
Mylicon
Nitrostat
Oxycodone 5-10 mg, tablet
Phenergan 25 mg, tablet
Pregabalin (after 3/23 procedure)
Prevacid 30 mg, tablet
Reglan 10 mg, injection
Silvadene, Topical Cream (after 3/23 procedure)
Sucralfate
Trazodone 100 mg, oral
TUMS
Vancomycin 1.5 gm, IV
ZofranNote: only medications given during March hospital admission*
Pertinent MedicationsIndications Medication Interactions
Healing & ↑ Fe absorption Ascorbic Acid N/V/D gastric cramps
↓Gastric Acid secretion, N/V/D, abdominal pain
TUMSCan ↓ Fe & B12Ensure adequate Vitamin D
High fistula output & losses Cholecalciferol ↑ Ca absorption; dry mouth, N/V/D/C
Indicated with TUMSFerrous Sulfate
↑ anemia labs, N/V/D/C, dyspepsia, bloating
AntiBx: Hx infections Cipro, Vancomycin N/V/D, abd pain, ↑ LFTs, ↑ TG
Pain Narcotics +C, no grapefruit, ↑ BG
Antiemetic, ↓ GI irritation Phenergan ↑ BG, drowsiness, sedation
Promote fistula closure, Anti-diarrheal
OctreotideN/V/D/C/F, steatorrhea, abd pain, monitor lytes, ↓B12
Antiemetic, Anti-GERD, ↑ GI contractions & food motility
Prevacid, Reglan
↑Gastrin, LFTs, Chol, BG; ↓ B12
Anti-nausea Zofran Can ↑ LFT
Rx to take after D/C Pregalbin
Topical Cream
Tylenol (oral)
Ambien
Ondanstron
Promethazine
Scopolamin
Sucrafate
Trazodone
SF Boost TID Ascorbic AcidOxycodone
Bed ridden
Endentulous
Personal History
Female, 42 y/o
White, non-Hispanic
Social History• Lives @ SNF
• Single
• No children
• Non smoker (quit ’07)
• Non alcohol user

6/20/2010
5
1. Trichorhinophlangel Syndrome- TRPS 2. Pyelonephritis3. Asthma4. GERD5. Morbid Obesity (BMI > 60)6. Diverticulitis 7. Polysubstance abuse8. Large B Cell Lymphoma s/p RCHOP (2000)9. Cholecystectomy (2000)10. Ventral Hernia Repair- VHR (2005)11. Small Bowel Obstruction12. Small Bowel Resection & Anastomosis13. Ex Lap14. Enterocutaneous Fistula15. UTI16. Bacteremia & Fungemia 17. Dental Caries18. Malnutrition
Past Medical History Food/Nutrition Related History
NPO, CL, FL, Puree, Mech Soft, Reg, PPN, TPN
“Subjective Global Assessment” obtained 3/17/10
Decreased appetite
FL diet past 2 weeks at SNF
+N/V/D for past 2 weeks
Last BM: “months ago”
Bed ridden (doesn’t walk SNF)
Edentulous (4 teeth)
Muscle wasting
Nutrition education - Amy Dorman, RD High protein foods allowed with a Pureed diet
Score: CSeverely
Malnourished
Day 1: Admit & Physical Exam
Fevers (102*), hypotension, delirium, RLQ pain, +N/V few days, ↑ ECF size, diaphoretic
-BP: 113/54 mmHG -Respiratory: 30
-Temp: 37°C (98.6°F)* -Sp02: 98% Open abd wound w/ visible viscera, yellow d/c, wound has
mild erythema. Abd tender. No signs of anasarca or peripheral edema.
Tachycardic
MD: Septic & UTI FULL CODE
Day 1: Nutrition Consult (Anna)
TPN Recs: (dosing wt: 67 kg)
18 kcal/kg, 1.6 gm pro/kg, 20% lipids in 1560 ml vol
Cyclic: 16 hrs
45 ml/hr x 1 hr; ↑ to 105 ml/hr x 14 hrs; ↓to 45 ml/hr x 1 hr; off 8 hr
Added: Thiamine (100 mg), Folic Acid (1 mg), Vit C (500 mg), Zinc (5 mg), Selenium (200 mcg)
Diet Rx : Regular Fistula output- “high”
Na 136
↓ K 3.2
↓ Mg 1.6
↑ P 5.2
↑ BUN 21
↓ Ca 8.5
↓ Alb 2.6
↑ LFTs
Glu 95
Estimated Energy Needs
18 kcal/dosing wt kg =1206-1541 kcal/day1.6 gm/IBW kg = 65.4 gm protein/day
22-25 kcal/IBW kg = 900-1020 kcal/day2.5 gm/IBW kg = 102 gm protein/day
Inaccurate ht for first 2 days
Day 2
Day 2: Rounds with Dr. Martindale
Diet recall obtained TPN continues (18 kcal; 1.6 gm)
Removed ALL Phos↑ KCl to 50 mEq/L ↑ MOS4 to 14 mEq/L
Est. Needs to: 900-1020 kcal; 102 gm pro (IBW)
Diet Rx: Pureed Dr. Martindale recommended Mech Soft + Boost TID
Fistula output: 1700 ml/d UTI mgmt- AntiBx Therapy: Cipro
↓ K 3.2
↑ Mg 1.7
↑ P 5.2
↓ Ca 8.3
↓ Hct 26.7

6/20/2010
6
The Infamous Strawberries
Story Time Day 3: TPN Stopped; New recs (Anna)
• Oral feeding trial
• Ck Mg in 2 days
New dosing wt: 40.9 kg (IBW)
22 kcal/IBW kg = 900 calories
2.5 gm pro/IBW kg = 103 g pro
↑ CRP 2.8
↓Ca 8.3
↓PAB 14
Mg: n/a
Day 3: Mg 1.7 (previous lab)
NaCl 70 mEq/L
KCl 50 mEq/L
Kphos 0 mmol/L
MgSO4 14 mEq/LRe-ck 2 days
CaGluconate
5 mEq/L
MVI & TE Standard Amt
Zinc 5 mg
Thiamine 100 mg
Vitamin C 500 mg
Selenium 200 mcg**
Folic Acid 1 mg
Day 1: Na 136, K 3.2, Mg 1.6, P 5.2
NaCl 70 mEq/L
KCl 20 mEq/L
Kphos 15 mmol/L
MgSO4 8 mEq/L
CaGluconate
5 mEq/L
MVI 1 mL
Zinc 5 mg
Copper I mg
Manganese 0.5 mg
Chronium 10 mcg
Selenium 60 mcg
Day 2:
K 3.2, Mg 1.7, P 5.2, Ca 8.3
NaCl 70 mEq/L
KCl ↑ to 50 mEq/L**
Kphos ↓ to 0 mmol/L*
MgSO4 ↑ to 14 mEq/L**
CaGluconate
5 mEq/L
MVI & TE Standard Amt
Zinc 5 mg
Thiamine 100 mg
Vitamin C 500 mg**
Selenium 200 mcg**
Folic Acid 1 mg**
Day 3: No Mg
NaCl 70 mEq/L
KCl 50 mEq/L
Kphos 0 mmol/L
MgSO4 14 mEq/LRe-ck 2 days
CaGluconate
5 mEq/L
MVI & TE Standard Amt
Zinc 5 mg
Thiamine 100 mg
Vitamin C 500 mg
Selenium 200 mcg**
Folic Acid 1 mg
TPN: Electrolytes & Additives Day 4 & 6: No TPN
Day 4: Oral Intake Test
•Severe abd pain; +N•Diet Rx: Mech Soft + Boost TIDoStart Calorie count, per RD
•Fistula Output: 3150 ml
Day 6: BM x 1 (liquid)
↓ Mg 1.6
↑ Ca 8.7
↓ PAB 16
↓ Alb 2.6
↑ Hct 26.7
↑ Alb 2.7
↓ BUN 4
↑ PAB 17-tgt
↑ Hct 29.9
↑ LFTs
Calorie Count
Day 4 1473 calories 57 gm pro
Day 6 2318 calories 103 gm pro
Remember, Ms. Pickles’ estimated needs were…
900-1020 calories; 102 gm pro
Day 7: Nutrition Consult
AEB TPN d/c 3 days ago & calorie count started Tolerating & meeting needs on mechanical soft
Failed oral intake test “miserably” Copious fistula output with PO intake
May need restart TPN; PICC insertion scheduled
Fistula output: 925 ml/d
BM x 1 (liquid)
Recommended
MVI & Zinc Monitor PO, continue Mech Soft + Boost TID

6/20/2010
7
Continue TPN Rx @ SNF & allow for recreational PO with no fluid restriction
Corrected Na, K, Ca, Mg, Phos
Appropriate PAB (17)
Low albumin (2.7), High BUN (4) & LFTs
F/U as an outpatient in few weeks
Ready for fistula take down in 3 weeks
Day 8: Groshong Inserted & Ms. Pickles Discharged
In a Nut Shell
Cyclic TPN maintained without complications Obtained optimal electrolyte levels
Diet Rx changed
Met her needs, PO However, failed oral intake trial
New PICC placed, current TPN regimen to resume @ SNF
Recreational PO & no fluid restriction
A BIG THANKS
Dr. Robert Martindale
Marliese White, MS, RD, CNSD, LD
References
1) ADA Nutrition Care Manual
2) Schecter WP, Hirshberg A, Chang DS, Harris HW, Napolitano LM, Wexner SD, Dudrick SJ. Enteric fistulas: Principles of management. J Am Coll Surg. 2009; 209(4):484-490.
3) Thompson MJ, Epanomeritakis E. An accountable fistula management treatment plan. Br J Nurs. 2008; 17(7): 434-440.
4) Visschers RGJ, Olde Damink SWM, Winkens B, Soeters, van Gemert WG. Treatment strategies in 135 consecutive patients with enterocutaneous fistulas. World J Surg. 2008; 32:445-453
5) Cawich SH, McFarlane ME, Mitchell DIG. Fistuloclysis: A novel approach to the management of enterocutaneous fistulae. The Internet J Surg. 2007; 9(2): 1-5.
6) Kwon SH, Oh JH, Kim HJ, Park SJ, Park HO. Interventional management of gastrointestinal fistulas. Korean J Radiol. 2008; 9(6): 541-549.
References
7) Fekaj E, Salihu L, Morina A. Treatment of enterocutaneous fistula with total parenteral feeding in combination with octreotide: a case report. Cases Journal. 2009; 2(177).
8) Baars JE, Kuipers EJ, van Dekken H, van der Woude CJ. Surgery is indicated for persistent enterocutaneous fistulizing Chron’s disease. Clin Med: Gastroenterology. 2008;1:1-3 (Case Report)
9) Connolly PT, Antje Teubner ChB, Lees NP, Anderson ID, Scott NA, Carlson GL. Outcome of reconstructive surgery for intestinal fistula in the open abdomen. Ann Surg. 2008;247: 440-444.
10) Makhdoom ZA, Komar MJ, Still CD. Nutrition and Enterocutaneous Fistulas. J Clin Gastroenterol. 2000;31(3):195-204.
11) Dudrick SJ, Maharaj AR, McKelvey AA. Artificial nutritional support in patients with gastrointestinal fistulas. World J. Surg. 1999;23:570-576
12) ADA Analysis Library13) OHSU Suggested Guidelines for Nutritional Care14) Pronsky ZA. (2008) Food medication interactions. 15th edition. Burch Runville,
Maryland.