Ms Miriam Mullard Dr Alasdair Patrick - gpcme.co.nz North/Sat_room7_0830 -The weight loss m… ·...
77
Ms Miriam Mullard Lead Dietitian MacMurray Centre Auckland 8:30 - 9:25 WS #95: The Weight Loss Menu 9:35 - 10:30 WS #107: The Weight Loss Menu (Repeated) Dr Alasdair Patrick Gastroenterologist and General Physician Middlemore Hospital Auckland
Transcript of Ms Miriam Mullard Dr Alasdair Patrick - gpcme.co.nz North/Sat_room7_0830 -The weight loss m… ·...
Ms Miriam MullardLead Dietitian
MacMurray Centre
Auckland
8:30 - 9:25 WS #95: The Weight Loss Menu
9:35 - 10:30 WS #107: The Weight Loss Menu (Repeated)
Dr Alasdair PatrickGastroenterologist and General Physician
Middlemore Hospital
Auckland

The only fully comprehensive
Gastroenterology center in Auckland
Opened in 2009
Largest Gastro practice in NZ
12 Gastroenterologists
1 Paediatric Gastroenterologist
1 Hepatologist
4 Surgeons
Dietician
Full diagnostic facilities on site
Dr Alasdair Patrick
Gastroenterologist
The weight loss menu
Dr Alasdair Patrick
MacMurray Centre
Miriam Mullard
MacMurray Centre
The Weight loss menu
Background
Diet and exercise (Miriam)
Behavioural modification
Pharmacological treatments
Endoscopic treatments:
- Overview
- Intra-gastric Balloons
- Endoscopic sleeve gastroplasty
Conclusion
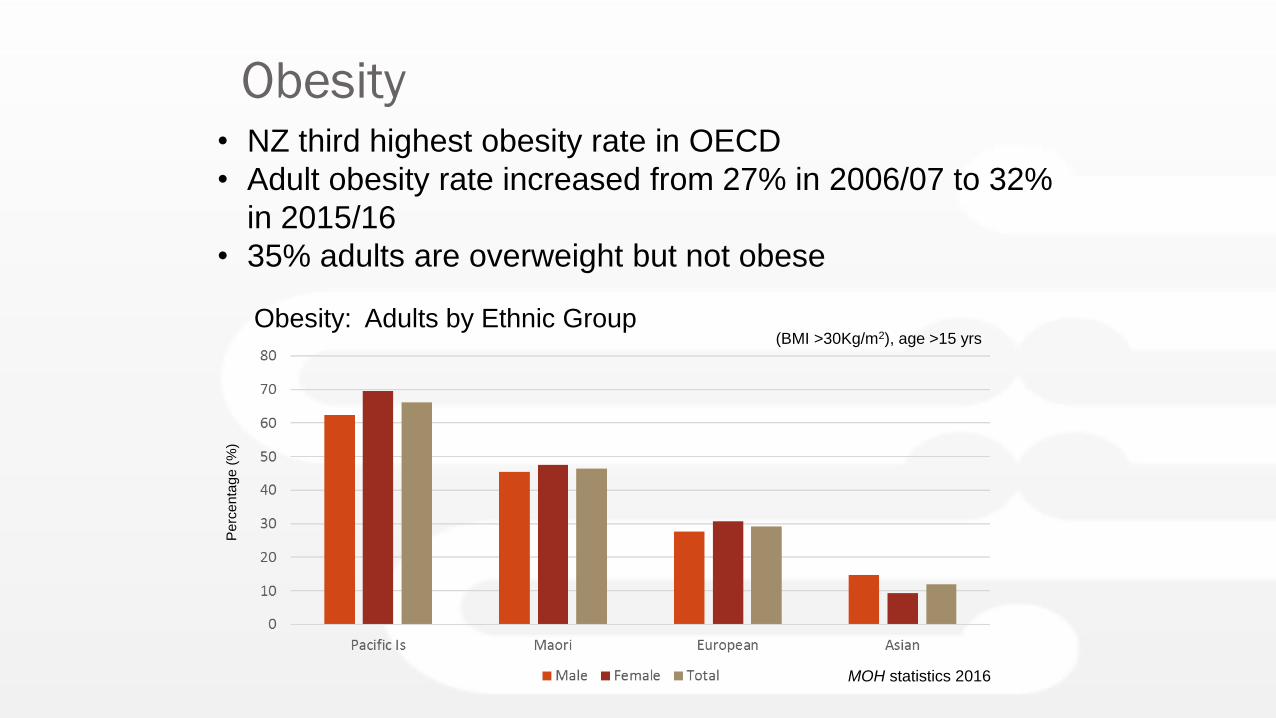
Obesity
Obesity: Adults by Ethnic Group
• NZ third highest obesity rate in OECD
• Adult obesity rate increased from 27% in 2006/07 to 32%
in 2015/16
• 35% adults are overweight but not obeseP
erc
en
tag
e (
%)
(BMI >30Kg/m2), age >15 yrs
MOH statistics 2016
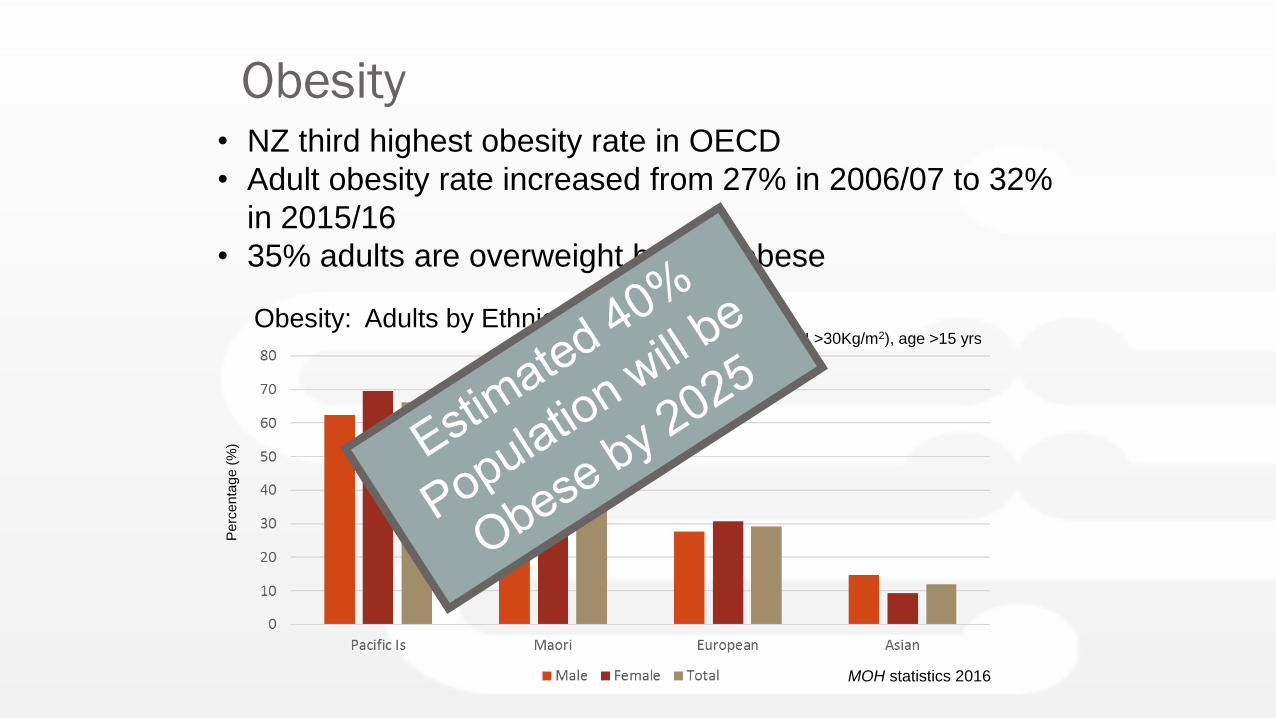
Obesity
Obesity: Adults by Ethnic Group
• NZ third highest obesity rate in OECD
• Adult obesity rate increased from 27% in 2006/07 to 32%
in 2015/16
• 35% adults are overweight but not obeseP
erc
en
tag
e (
%)
(BMI >30Kg/m2), age >15 yrs
MOH statistics 2016
Diabetes
>35% rise in prevalence of Type II DM over the last
decade
Prevalence in Maori and Pacific Is 3x higher, increasing at
a faster rate than Europeans
Increasing burden due to obesity epidemic, aging
population and ethnic mix
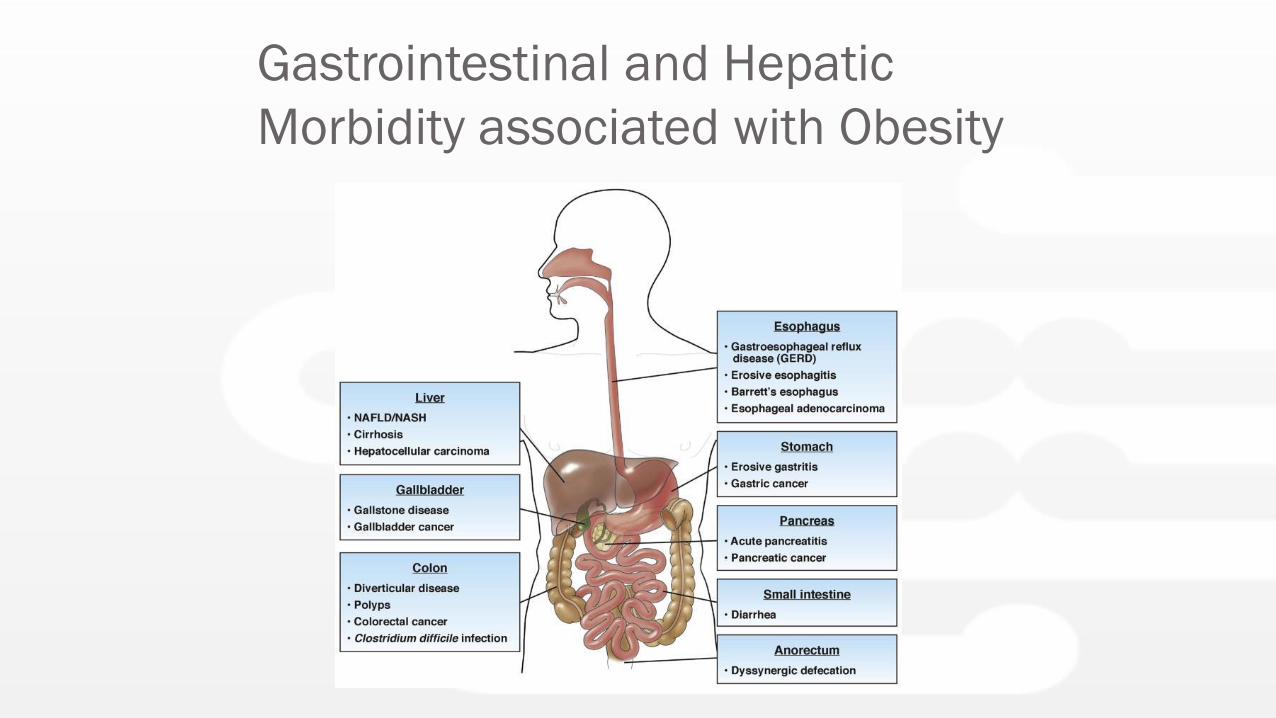
Gastrointestinal and Hepatic
Morbidity associated with Obesity
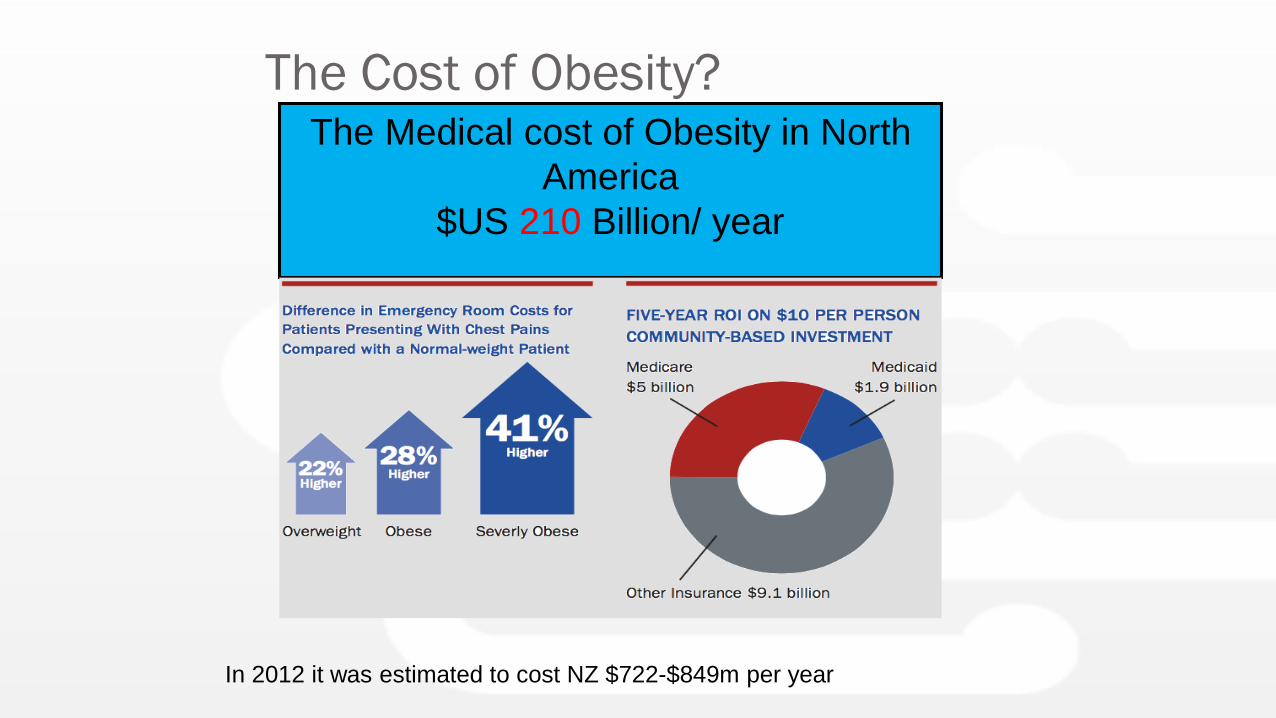
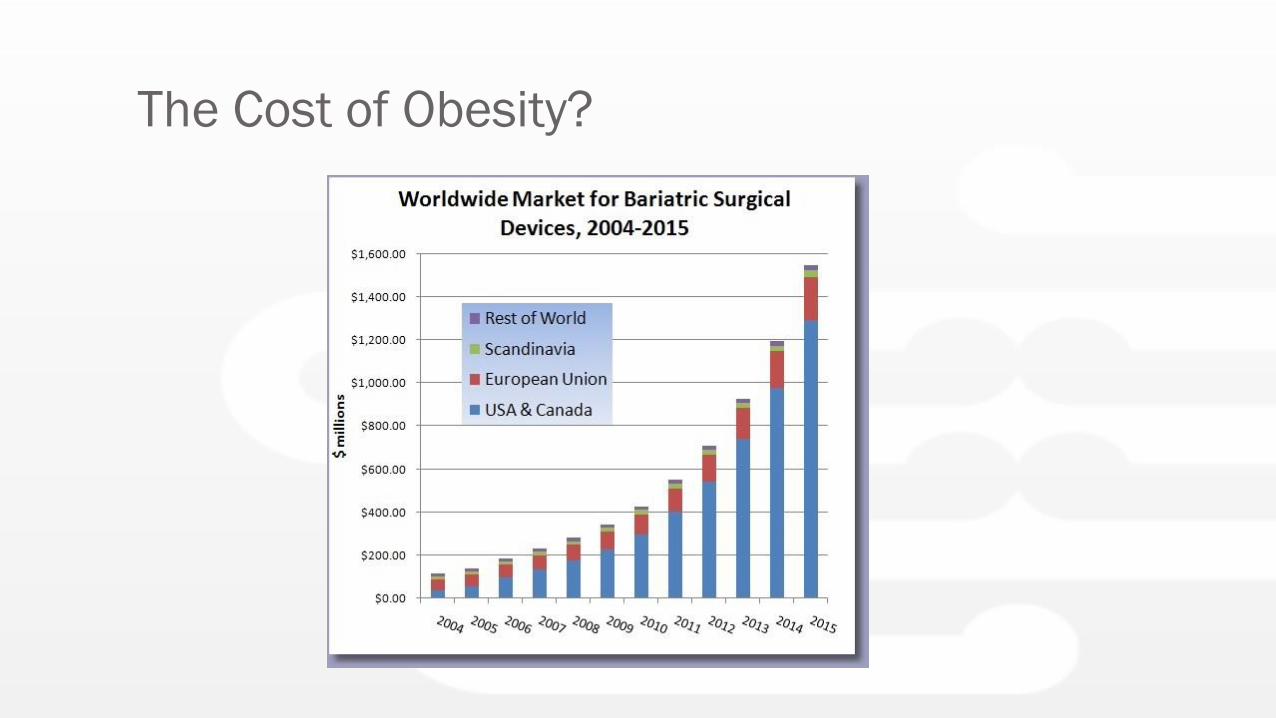
The Cost of Obesity?The Medical cost of Obesity in North
America
$US 210 Billion/ year
In 2012 it was estimated to cost NZ $722-$849m per year
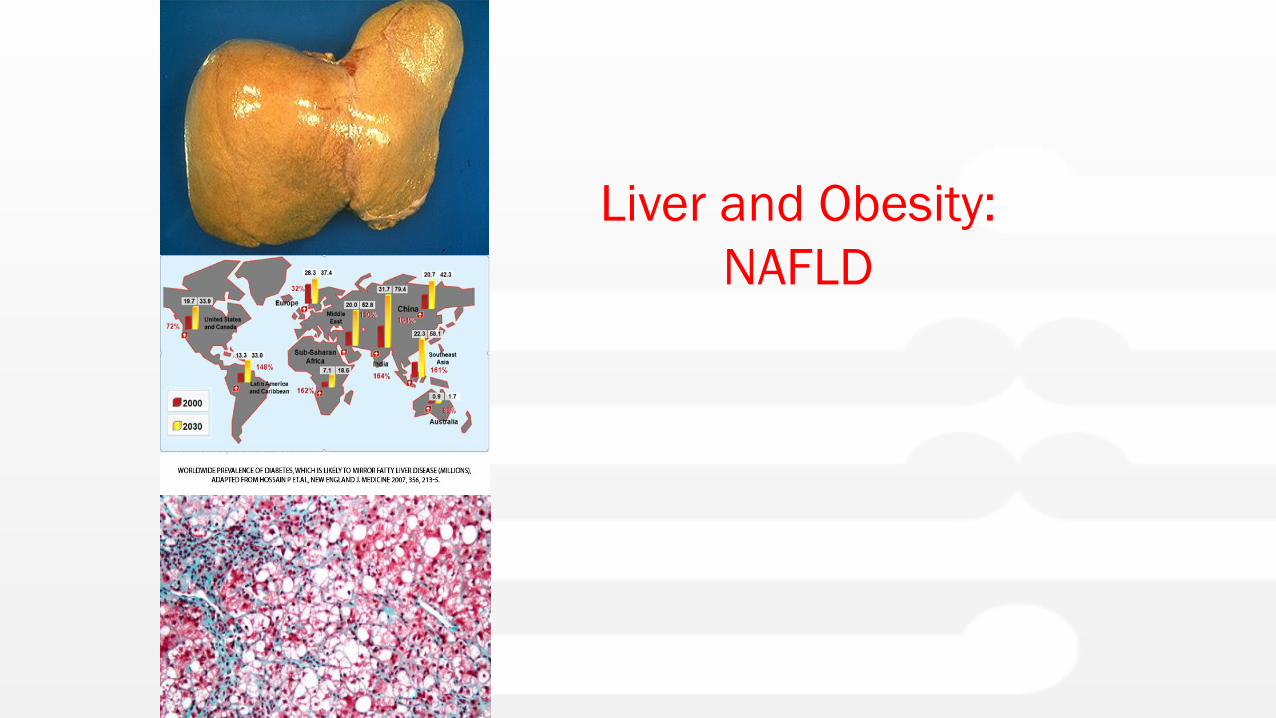
Liver and Obesity:
NAFLD
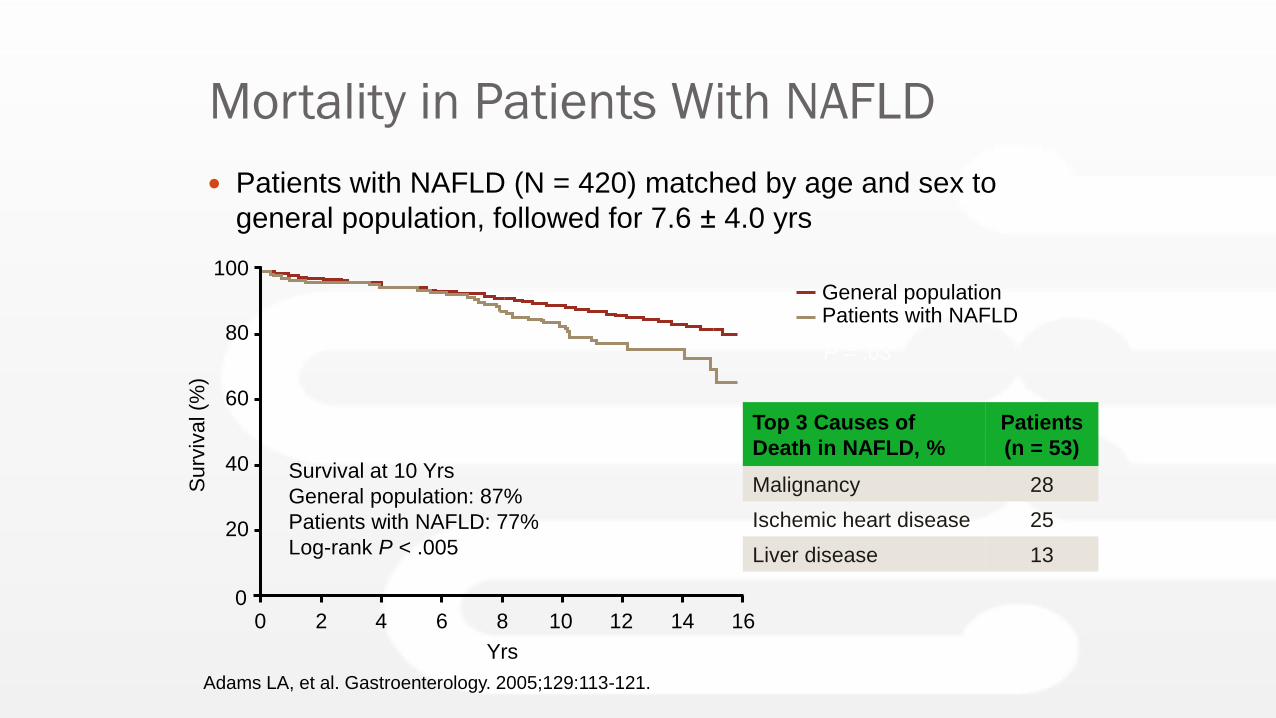
Mortality in Patients With NAFLD
Patients with NAFLD (N = 420) matched by age and sex to
general population, followed for 7.6 ± 4.0 yrs
Adams LA, et al. Gastroenterology. 2005;129:113-121.
Top 3 Causes of
Death in NAFLD, %
Patients
(n = 53)
Malignancy 28
Ischemic heart disease 25
Liver disease 13
Survival at 10 Yrs
General population: 87%
Patients with NAFLD: 77%
Log-rank P < .005
0
20
40
60
80
100
0 4
Surv
ival (%
)
62 10
General populationPatients with NAFLD
P = .03
Yrs
8 12 14 16
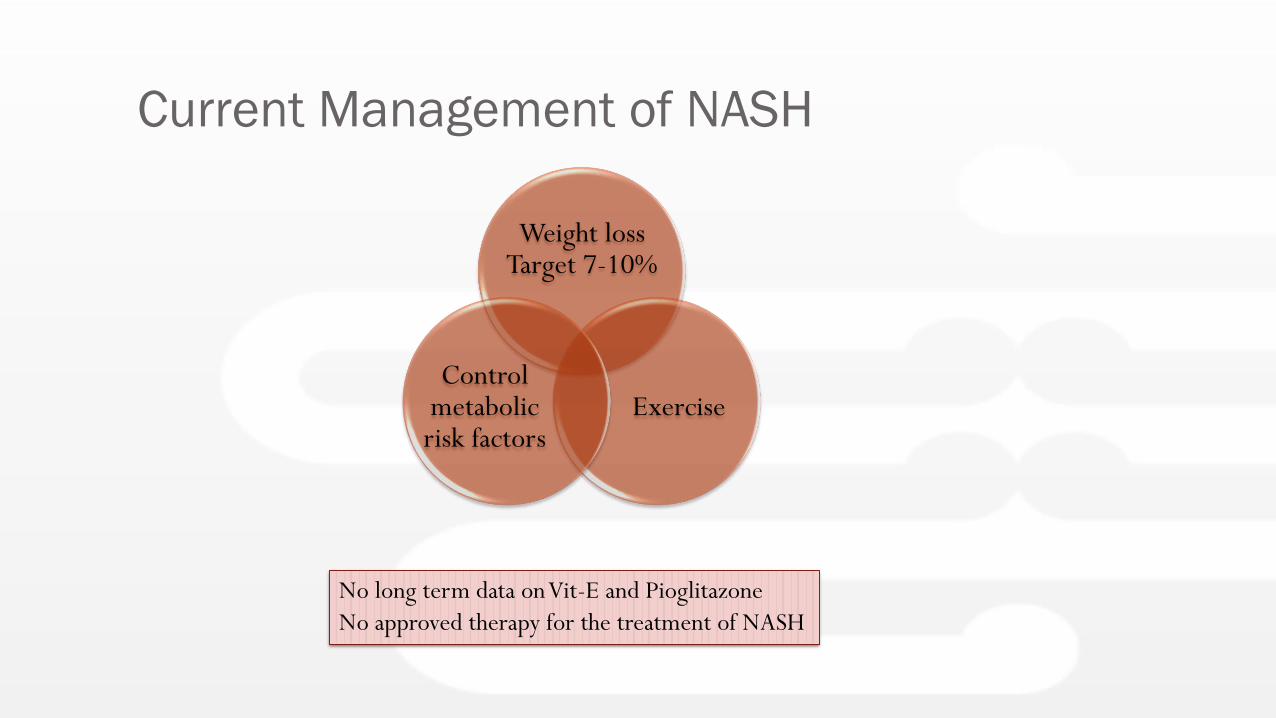
Current Management of NASH
Weight loss Target 7-10%
ExerciseControl
metabolic risk factors
No long term data on Vit-E and Pioglitazone
No approved therapy for the treatment of NASH
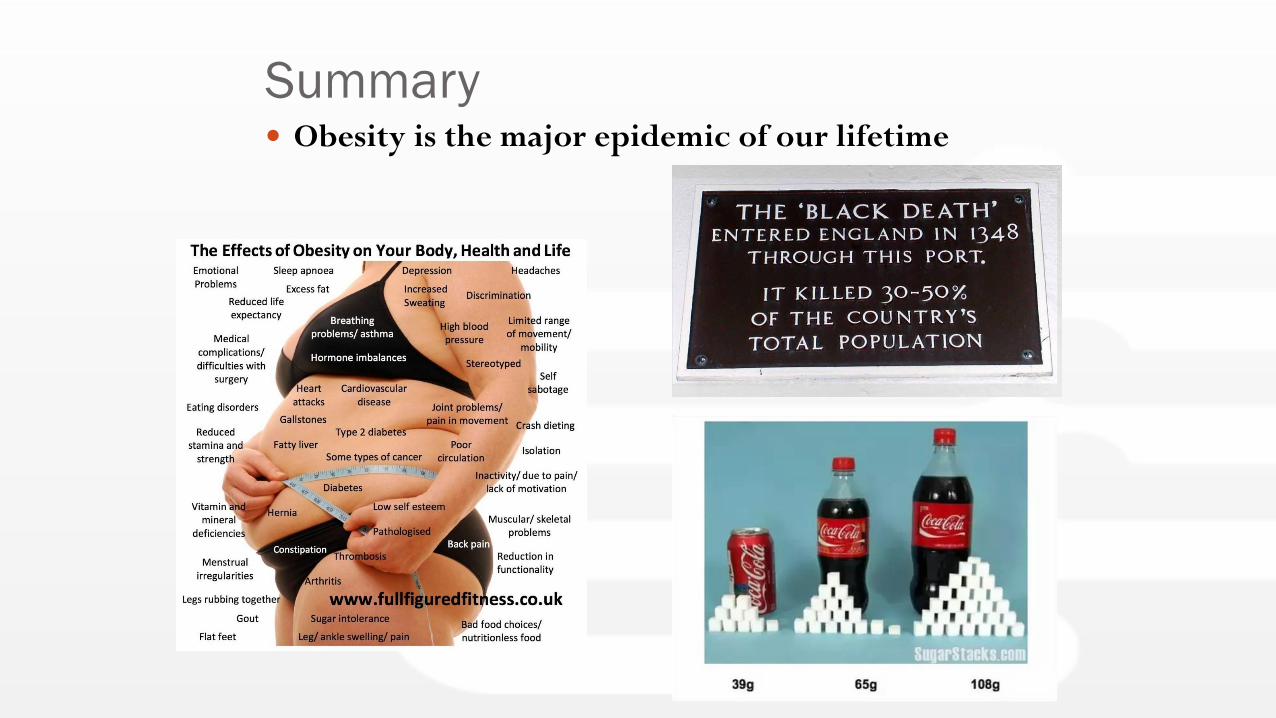
Summary Obesity is the major epidemic of our lifetime
Diet and Exercise
Miriam Mullard
NZ Registered Dietitian
MacMurray Centre
It’s not enough to tell them what to do,
we need to show them how to do it.
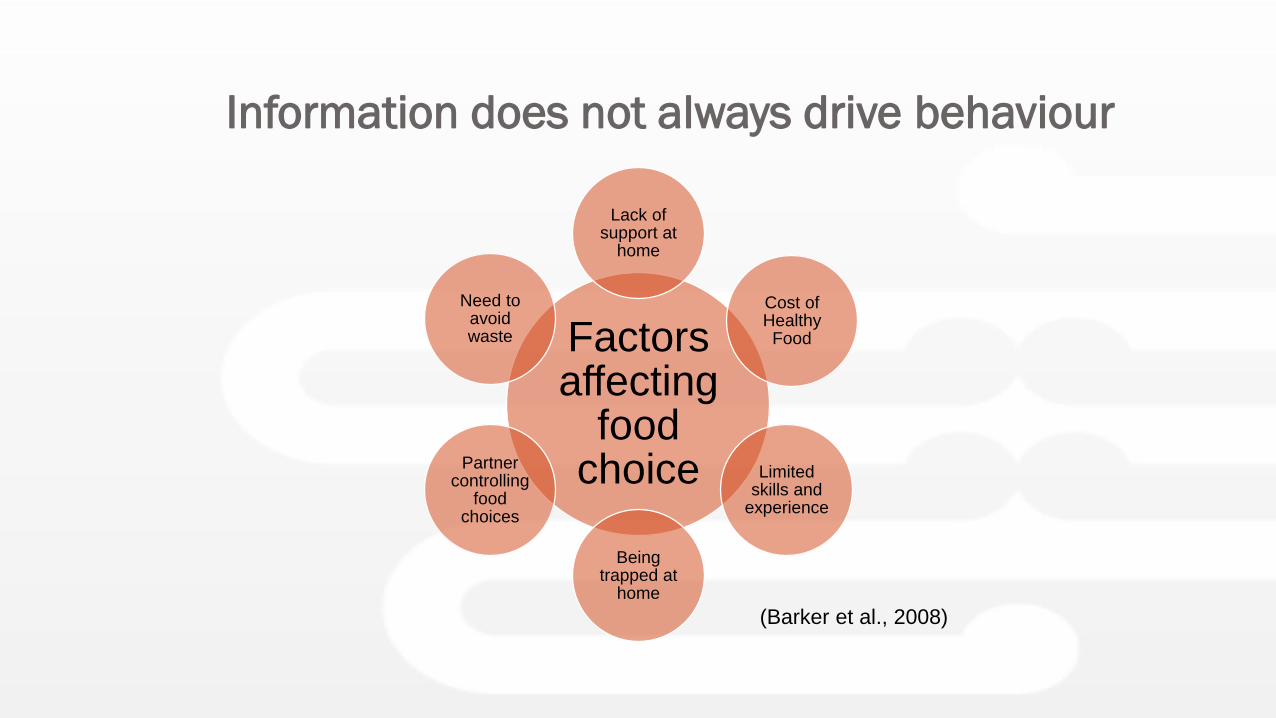
Information does not always drive behaviour
Factors affecting
food choice
Lack of support at
home
Cost of Healthy Food
Limited skills and
experience
Being trapped at
home
Partner controlling
food choices
Need to avoid waste
(Barker et al., 2008)
Motivate patients to find their own solutions
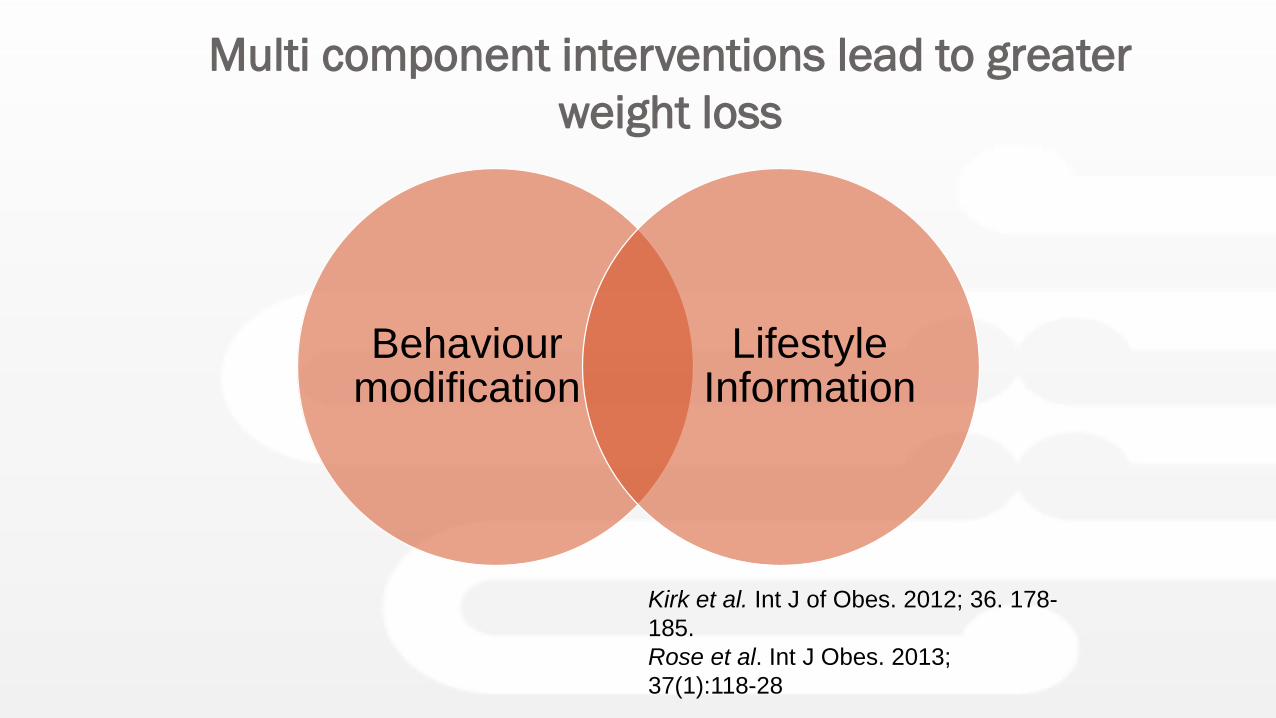
Multi component interventions lead to greater
weight loss
Behaviourmodification
Lifestyle Information
Kirk et al. Int J of Obes. 2012; 36. 178-
185.
Rose et al. Int J Obes. 2013;
37(1):118-28
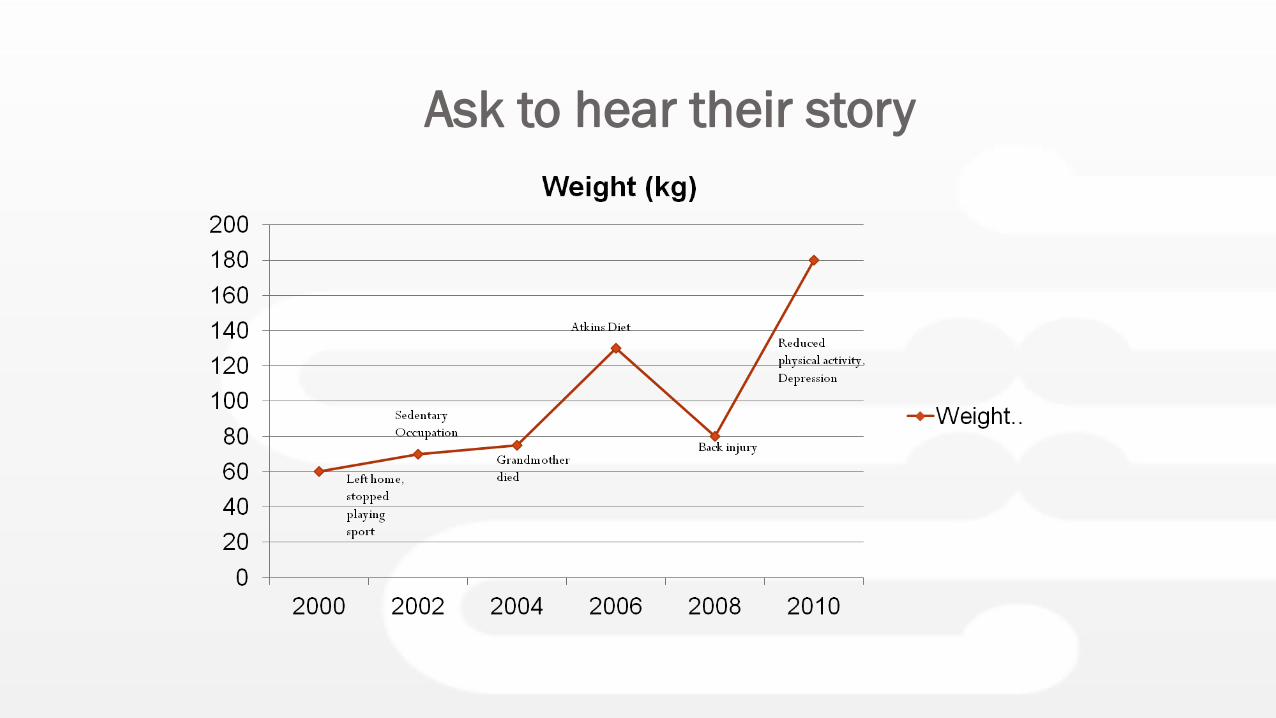
Ask to hear their story
Tailor interventions to your patient
Improve dietary quality
Regulate meal
frequency and
pattern
Reduce portion Sizes
Eat Mindfully
Monitor Diet
Ask clients to name one
thing they can change
Encourage your clients to take control
•Plan meals ahead of
time
•Eat regular meals and
snacks
•Plan ahead for busy
times
•Identify ‘danger’ times
when likely to overeat
Promote regular self monitoring
Apps for self monitoring
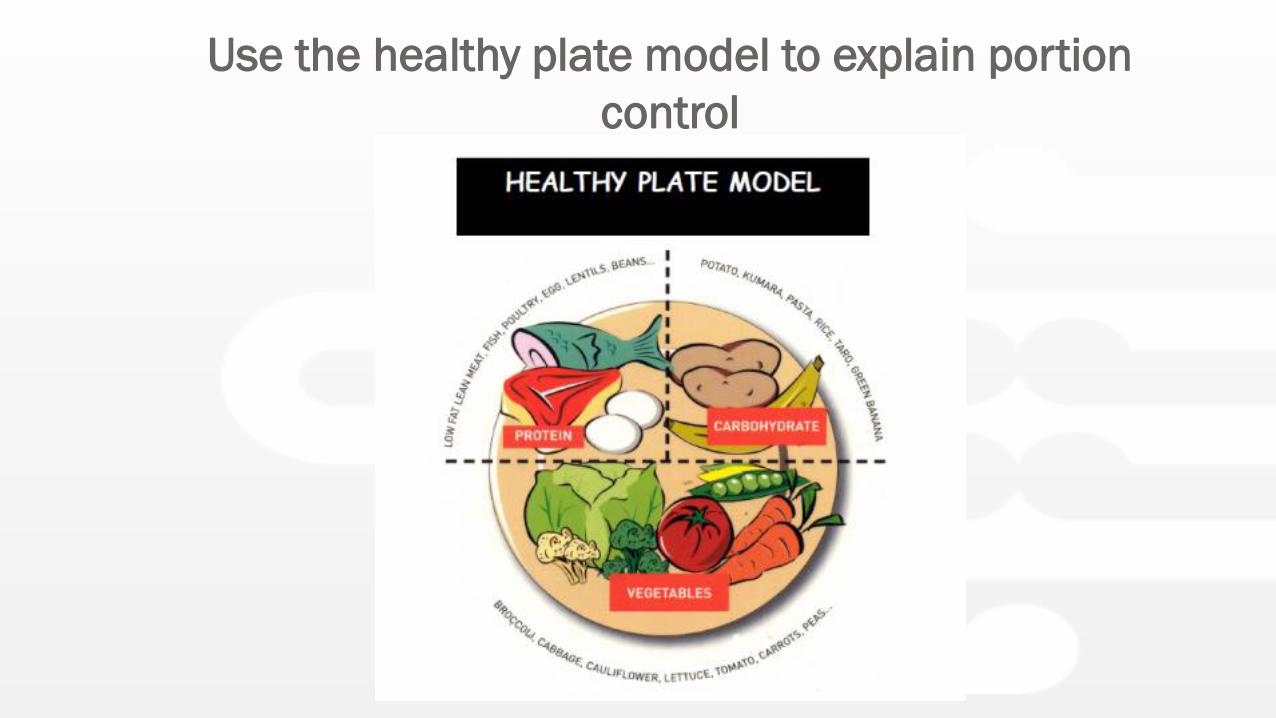
Use the healthy plate model to explain portion
control
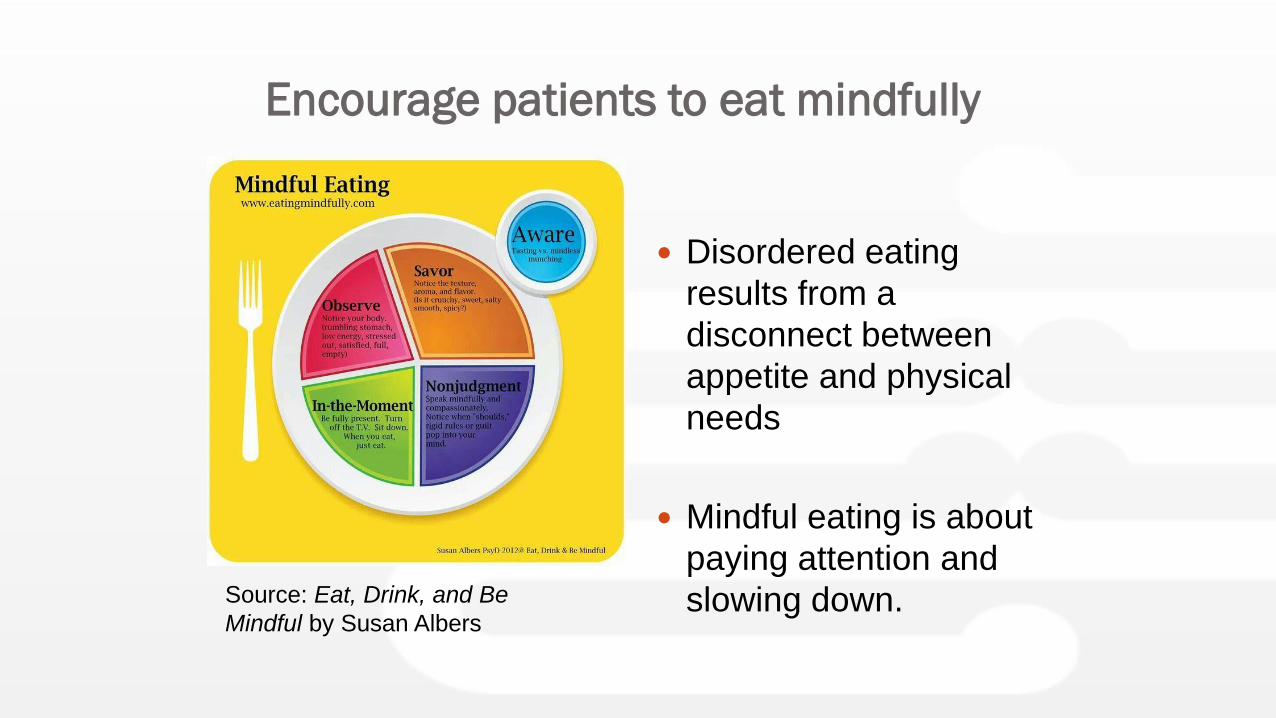
Encourage patients to eat mindfully
Disordered eating
results from a
disconnect between
appetite and physical
needs
Mindful eating is about
paying attention and
slowing down. Source: Eat, Drink, and Be
Mindful by Susan Albers
Mindfulness Apps
Calorie restriction is more important than exercise
for weight loss
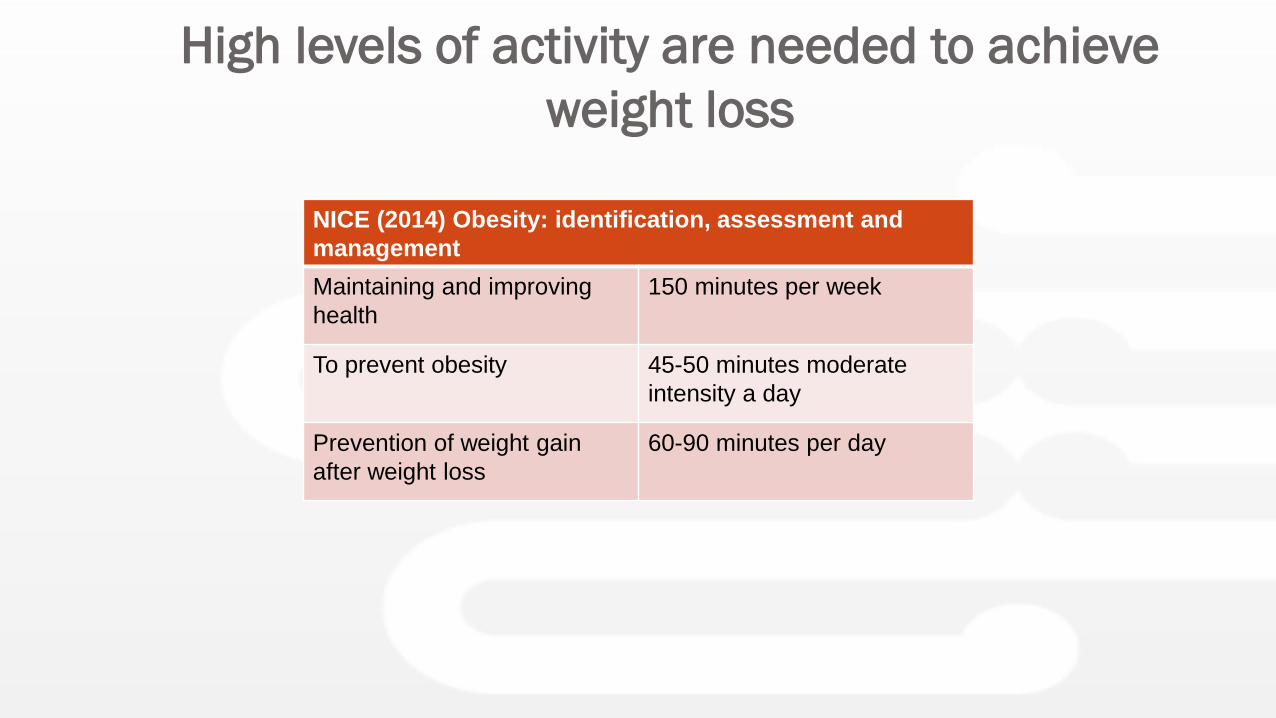
High levels of activity are needed to achieve
weight loss
NICE (2014) Obesity: identification, assessment and
management
Maintaining and improving
health
150 minutes per week
To prevent obesity 45-50 minutes moderate
intensity a day
Prevention of weight gain
after weight loss
60-90 minutes per day
Exercise
improves
health
even
without
weight
loss
Make sure that goals ARE achievable
Reduce Sedentary Behaviours
Encourage Self
Monitoring
Suggest Apps
Exercise on Referral
It’s not enough to tell them what to do,
we need to show them how to do it.
Thanks Miriam
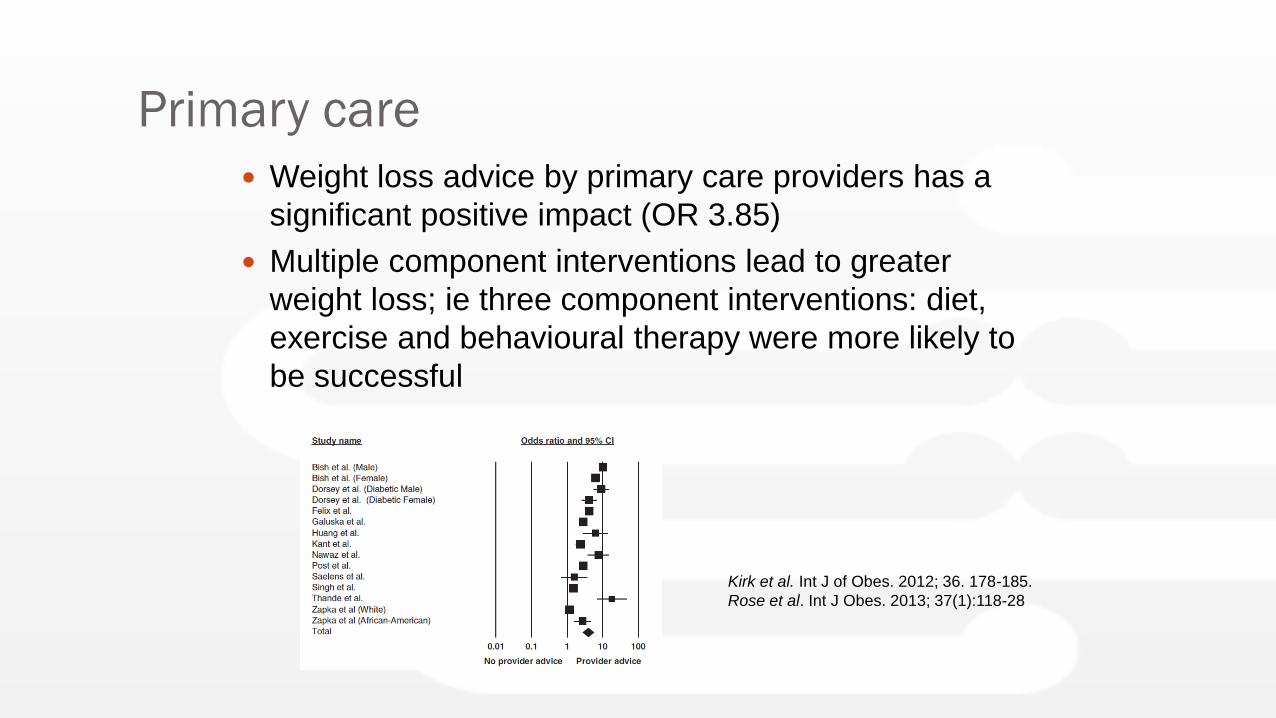
Primary care
Weight loss advice by primary care providers has a
significant positive impact (OR 3.85)
Multiple component interventions lead to greater
weight loss; ie three component interventions: diet,
exercise and behavioural therapy were more likely to
be successful
Kirk et al. Int J of Obes. 2012; 36. 178-185.
Rose et al. Int J Obes. 2013; 37(1):118-28
Diet
Low energy, VLCD, low glycaemic index diets all
achieve similar weight loss ~4kg at 1yr
Low carbohydrate vs low fat diets, no significant
difference in weight loss. (7.25Kg vs 7.27Kg, p=ns).
Meta-analysis; no specific diet identified for healthy
obese patients
Vink et al. Obesity. 2016 Feb;24(2):321-7.
Johnston et al. JAMA. 2014; 312(9):923-33
Stelmach-Mardas et al. Nutrients. 2016; 28; 8(8).
Exercise
150-250 mins/week moderate intensity exercise will
only produce modest weight loss
>250mins/week associated with clinically significant
weight loss
BUT: health status is improved even in the absence of
weight loss (improved BP, lipids, insulin resistance).
Exercise results in improved weight loss maintenance
at 1 yr.
Weight Loss in NASH
Randomized 2:1 ratio to receive intensive lifestyle intervention (LS) or structured education (control) for 48 weeks.
LS group lost an average of 9.3% TBW versus 0.2% in the control group (p=0.003).
LS group reduction of NAS of at least 3 points or had post treatment NAS ≤ 2 compared with the control group (72% versus 30%, p=0.03).
Participants who achieved the study weight loss goal (>7%), had significant improvements in NAS (P < 0.001).
Pomrat et al. Hepatology 2010
Pharmacologic Management
of Obesity
Weight loss drugs
Only recommend if:
- No significant improvement with >6-months
lifestyle changes
- BMI >30kg/m2. (or >27Kg/m2 with at least one
weight related disease)
FDA approved five ‘long-term’ weight loss drugs:
- Orlistat, Lorcaserin, Naltrexone-bupropion,
Phenteramine-topiramate, Liraglutide.
Orlistat
FDA approved 1999
Gastrointestinal lipase inhibitor; preventing dietary fat
(`30%) from being metabolized and absorbed
Continue >3-months only if >5% TBW loss
Adverse effects; oily stool, faecal urgency, increased
flatus
Outcome
Meta-analysis: 1-year weight loss ~3.4Kg
Associated reduction in lipids, BP, fasting glucose
<10% patients will take for a year due to GI
side effects
Phentermine (Duromine)
FDA approved 1959
Sympathomimetic amine, a stimulant that acts on the
CNS and suppresses appetite.
(Combined with low-dose topiramate; associated with
increased appetite suppression; off-label use in NZ)
Starting dose 15mg, maintenance 30mg mane
Adverse effects: tachycardia, HT, insomnia, irritability,
headache, nausea, altered bowel
Outcome
6-months; wt loss 4.5kg (>placebo), 46% lost >5%
TBW
Topiramate
FDA approved 1996 for epilepsy
Used in combination with phentermine (3.75/23mg, 7.5/46mg,
11.25/69mg, 15/92mg).
Adverse effects: paresthesia, insomnia, constipation, impaired taste
Outcome: Phentermine-topiramate over 1yr
6.6- 8.6kg (>placebo)
Reduction in progression to DM
Use of Topiramate in NZ would be off label.
(dose available 25, 50 and 100mg)
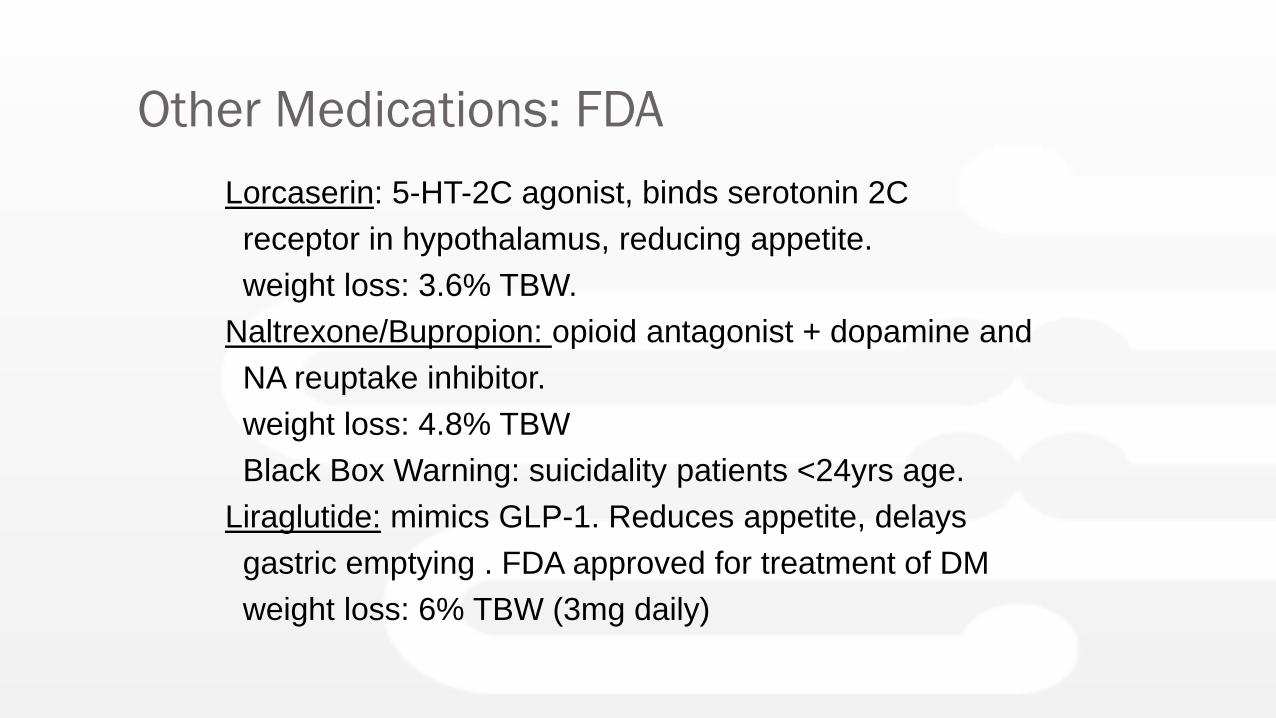
Other Medications: FDA
Lorcaserin: 5-HT-2C agonist, binds serotonin 2C
receptor in hypothalamus, reducing appetite.
weight loss: 3.6% TBW.
Naltrexone/Bupropion: opioid antagonist + dopamine and
NA reuptake inhibitor.
weight loss: 4.8% TBW
Black Box Warning: suicidality patients <24yrs age.
Liraglutide: mimics GLP-1. Reduces appetite, delays
gastric emptying . FDA approved for treatment of DM
weight loss: 6% TBW (3mg daily)
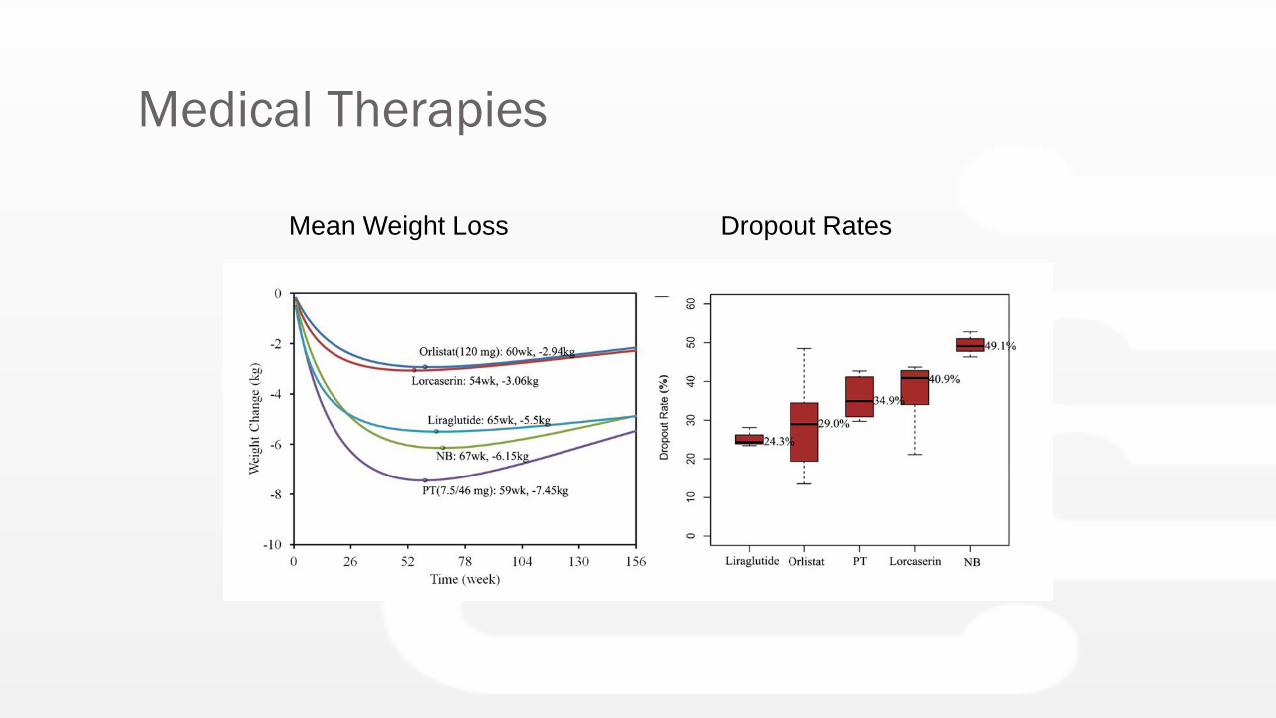
Medical Therapies
Mean Weight Loss Dropout Rates
Endoscopic Management of Obesity
The Cost of Obesity?
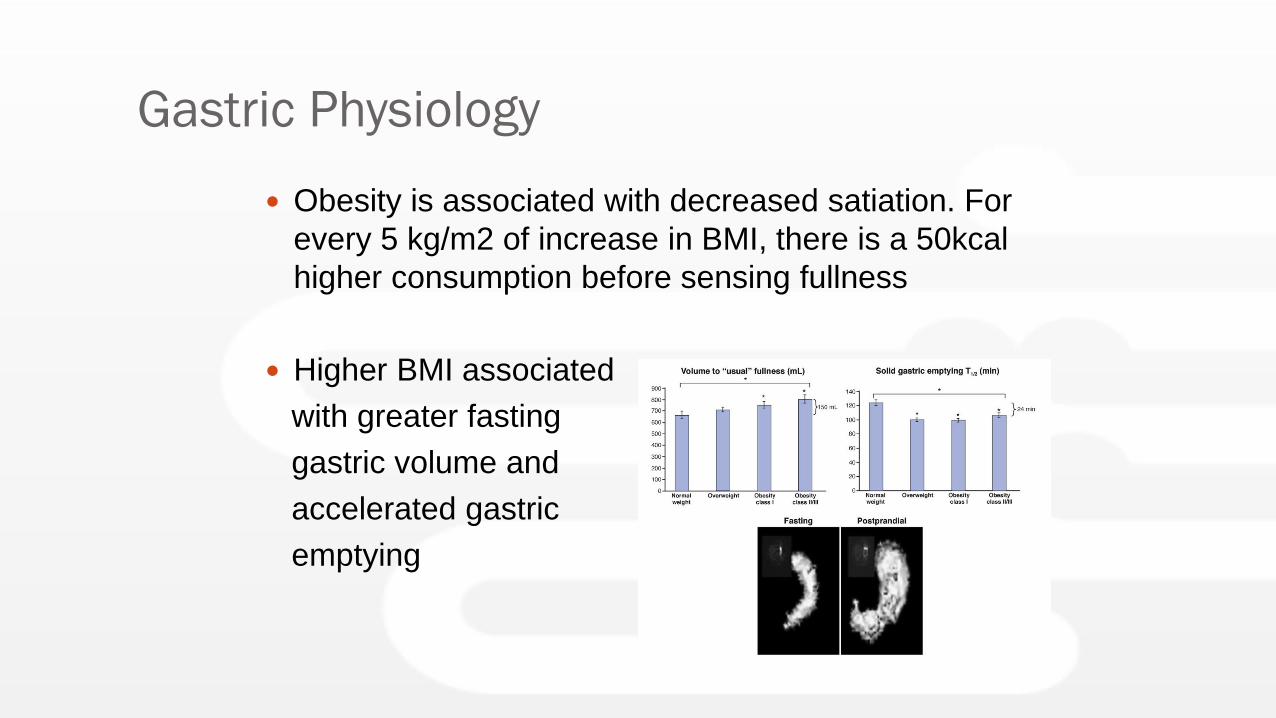
Gastric Physiology
Obesity is associated with decreased satiation. For
every 5 kg/m2 of increase in BMI, there is a 50kcal
higher consumption before sensing fullness
Higher BMI associated
with greater fasting
gastric volume and
accelerated gastric
emptying
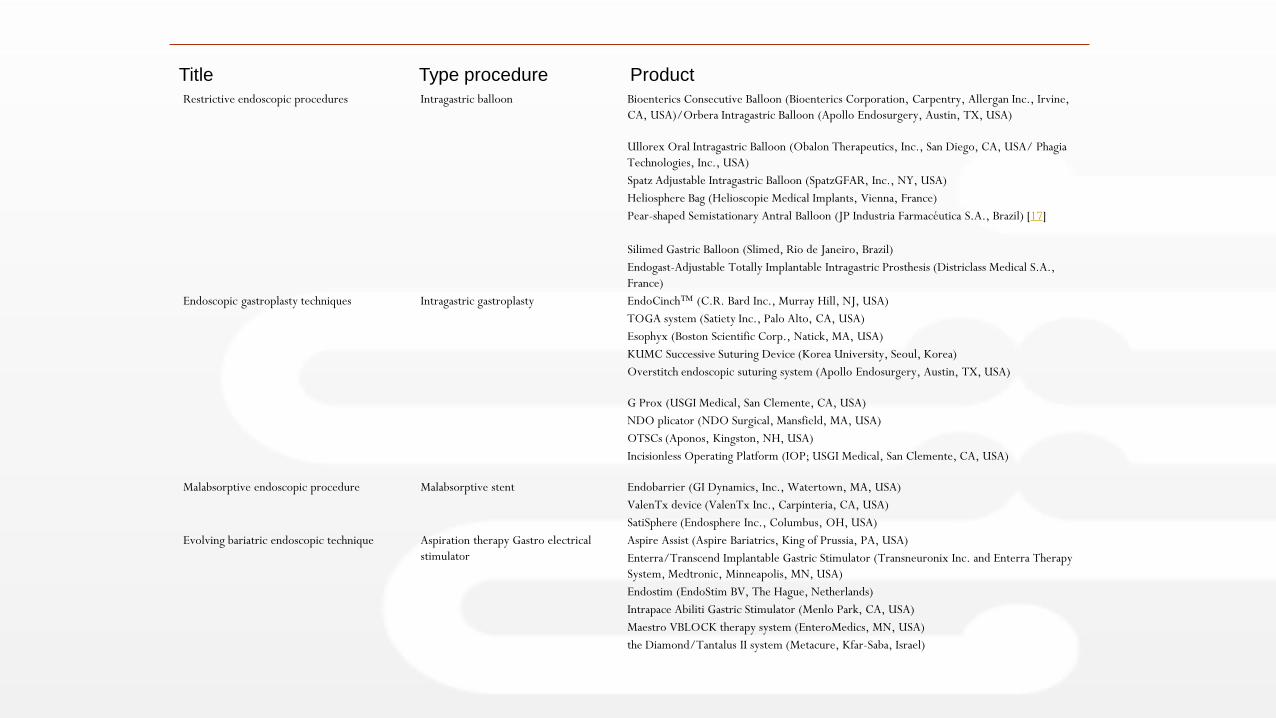
Restrictive endoscopic procedures Intragastric balloon Bioenterics Consecutive Balloon (Bioenterics Corporation, Carpentry, Allergan Inc., Irvine,
CA, USA)/Orbera Intragastric Balloon (Apollo Endosurgery, Austin, TX, USA)
Ullorex Oral Intragastric Balloon (Obalon Therapeutics, Inc., San Diego, CA, USA/ Phagia
Technologies, Inc., USA)
Spatz Adjustable Intragastric Balloon (SpatzGFAR, Inc., NY, USA)
Heliosphere Bag (Helioscopie Medical Implants, Vienna, France)
Pear-shaped Semistationary Antral Balloon (JP Industria Farmacéutica S.A., Brazil) [17]
Silimed Gastric Balloon (Slimed, Rio de Janeiro, Brazil)
Endogast-Adjustable Totally Implantable Intragastric Prosthesis (Districlass Medical S.A.,
France)
Endoscopic gastroplasty techniques Intragastric gastroplasty EndoCinch™ (C.R. Bard Inc., Murray Hill, NJ, USA)
TOGA system (Satiety Inc., Palo Alto, CA, USA)
Esophyx (Boston Scientific Corp., Natick, MA, USA)
KUMC Successive Suturing Device (Korea University, Seoul, Korea)
Overstitch endoscopic suturing system (Apollo Endosurgery, Austin, TX, USA)
G Prox (USGI Medical, San Clemente, CA, USA)
NDO plicator (NDO Surgical, Mansfield, MA, USA)
OTSCs (Aponos, Kingston, NH, USA)
Incisionless Operating Platform (IOP; USGI Medical, San Clemente, CA, USA)
Malabsorptive endoscopic procedure Malabsorptive stent Endobarrier (GI Dynamics, Inc., Watertown, MA, USA)
ValenTx device (ValenTx Inc., Carpinteria, CA, USA)
SatiSphere (Endosphere Inc., Columbus, OH, USA)
Evolving bariatric endoscopic technique Aspiration therapy Gastro electrical
stimulator
Aspire Assist (Aspire Bariatrics, King of Prussia, PA, USA)
Enterra/Transcend Implantable Gastric Stimulator (Transneuronix Inc. and Enterra Therapy
System, Medtronic, Minneapolis, MN, USA)
Endostim (EndoStim BV, The Hague, Netherlands)
Intrapace Abiliti Gastric Stimulator (Menlo Park, CA, USA)
Maestro VBLOCK therapy system (EnteroMedics, MN, USA)
the Diamond/Tantalus II system (Metacure, Kfar-Saba, Israel)
Title Type procedure Product
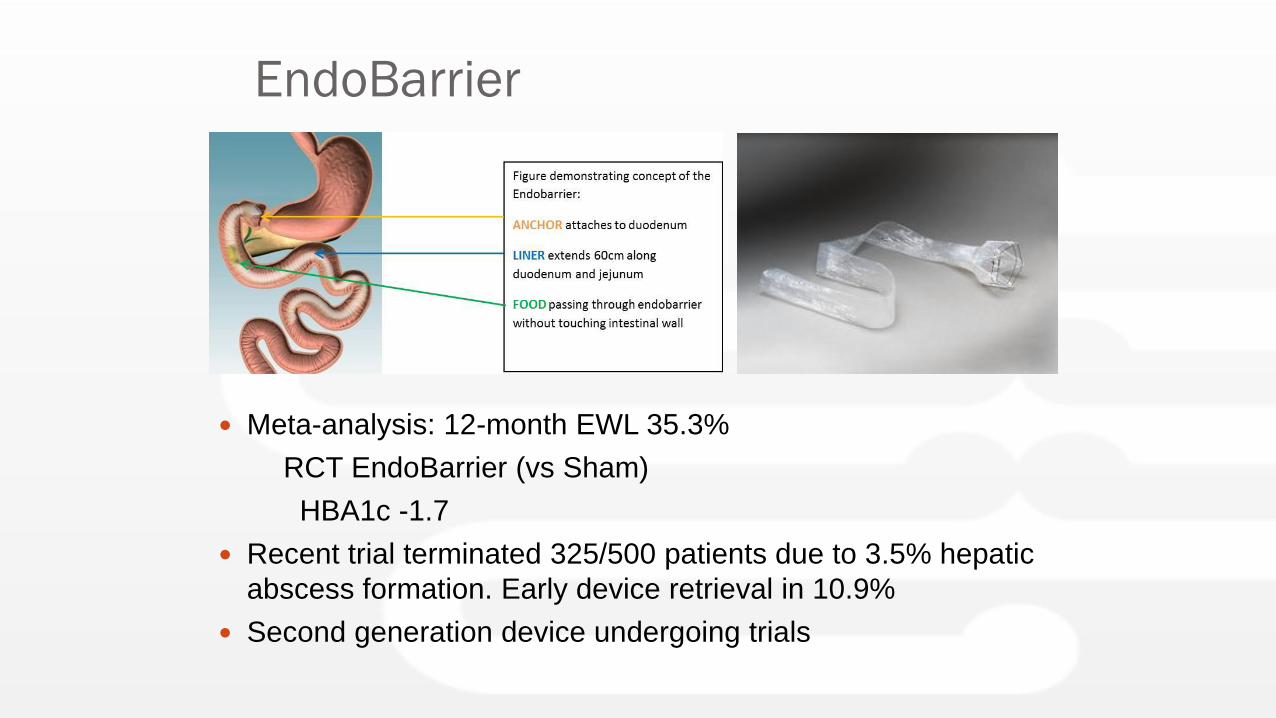
EndoBarrier
Meta-analysis: 12-month EWL 35.3%
RCT EndoBarrier (vs Sham)
HBA1c -1.7
Recent trial terminated 325/500 patients due to 3.5% hepatic
abscess formation. Early device retrieval in 10.9%
Second generation device undergoing trials
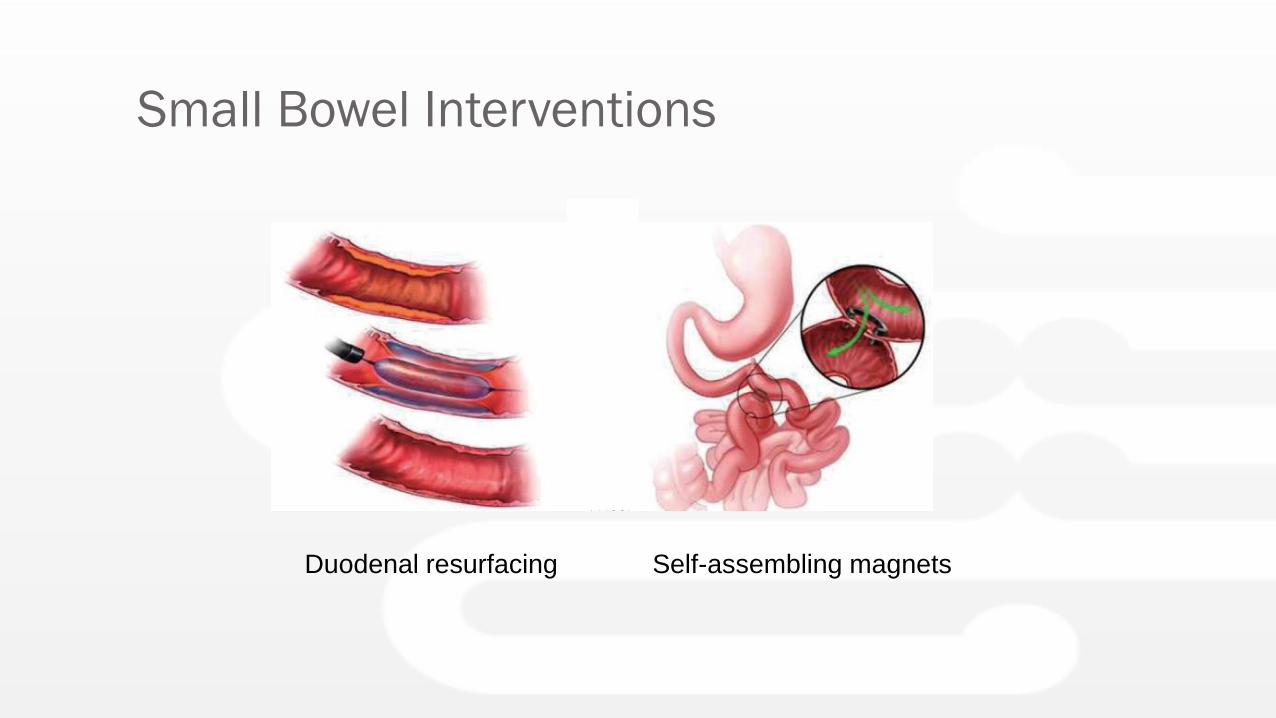
Small Bowel Interventions
Duodenal resurfacing Self-assembling magnets
Intragastric Balloons
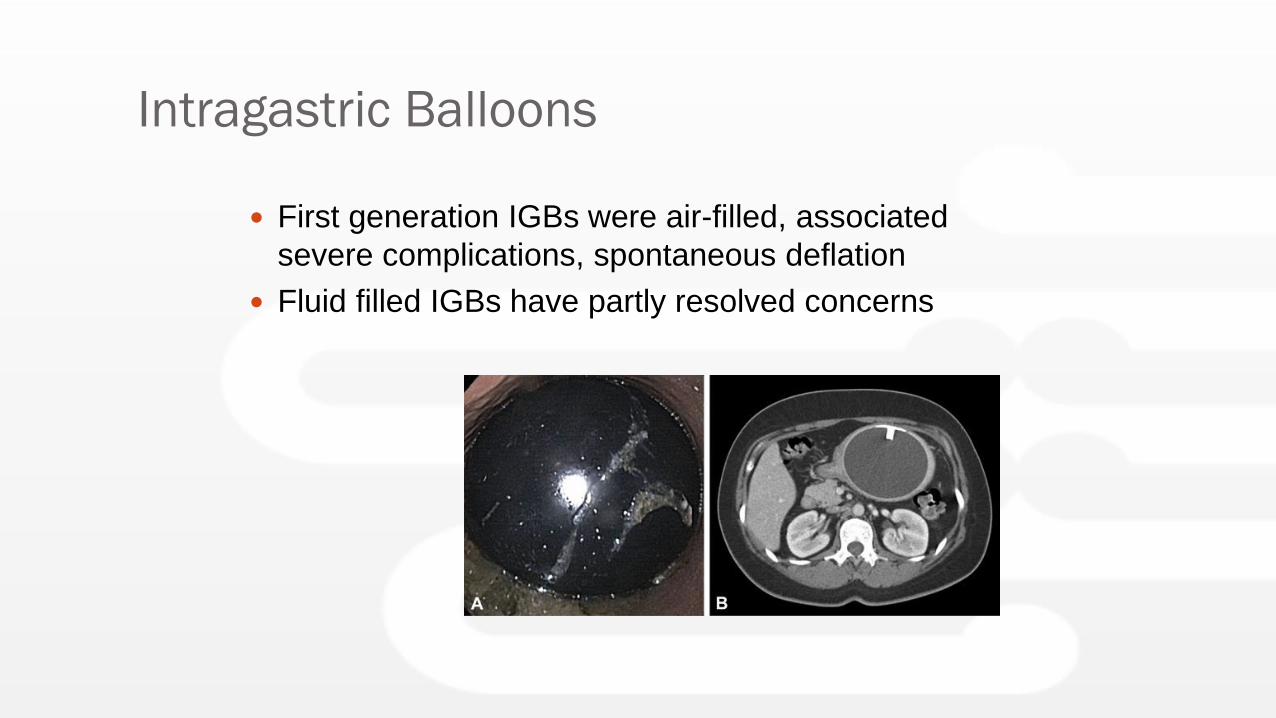
Intragastric Balloons
First generation IGBs were air-filled, associated
severe complications, spontaneous deflation
Fluid filled IGBs have partly resolved concerns
IGB RCT: Meta-analysis
20 RCTs, 1195 patients (Saber et al)
- 3-month effect: BMI reduction 1.59kg/m2, or
14.25% EWL, or 4.6Kg weight loss (compared to
control group- behavioural modification, and sham
procedure)
16 Studies; 3068 patients (Imaz et al)
- Overall Weight loss: 14.7Kg, reduction BMI
5.7Kg/m2 and 32.1 %EWL at 6-months
Saber et al. Obes Surg 2017; 27: 277-87
Imaz et al. Obes Surg 2008; 18 (7): 841-6
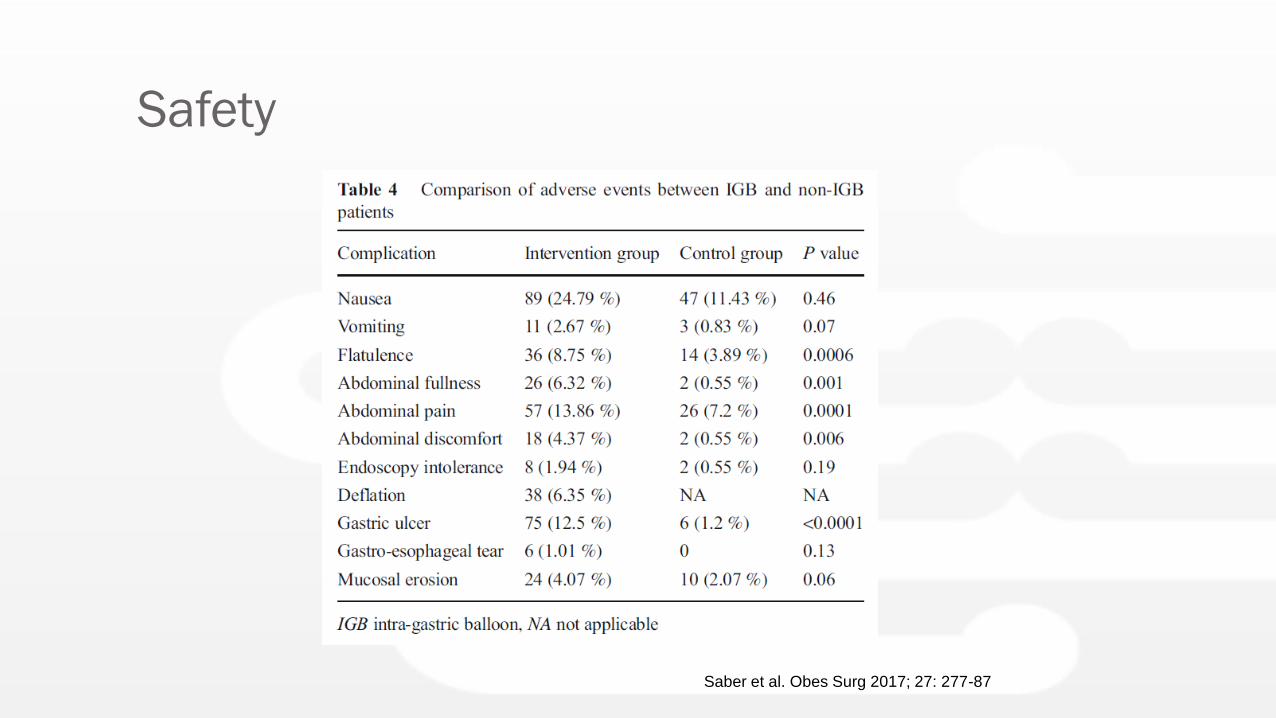
Safety
Saber et al. Obes Surg 2017; 27: 277-87
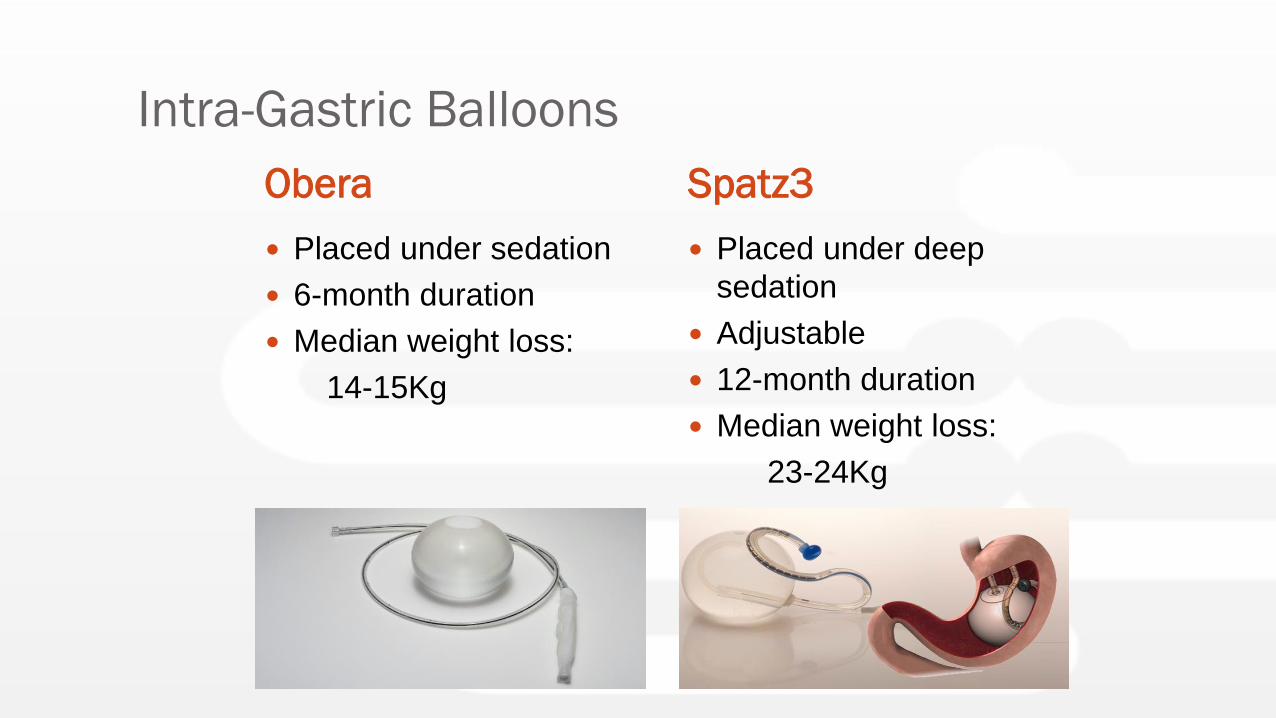
Intra-Gastric Balloons
Obera Spatz3
Placed under sedation
6-month duration
Median weight loss:
14-15Kg
Placed under deep
sedation
Adjustable
12-month duration
Median weight loss:
23-24Kg
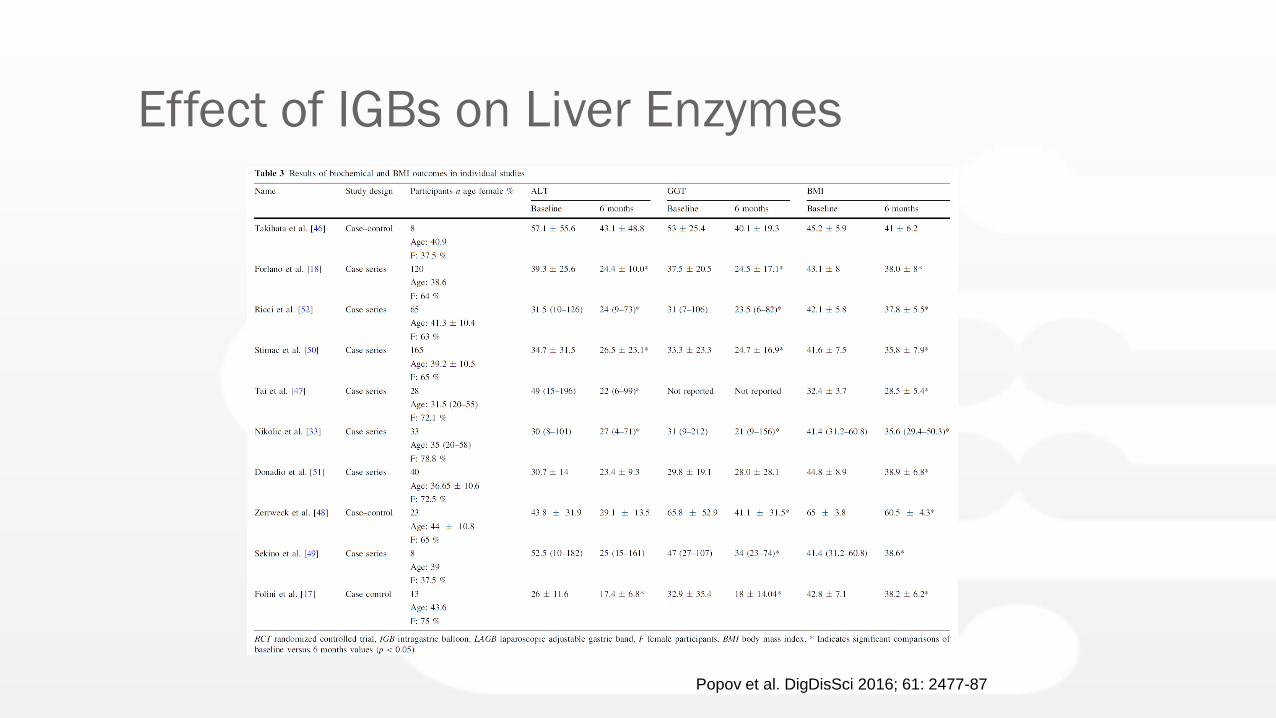
Effect of IGBs on Liver Enzymes
Popov et al. DigDisSci 2016; 61: 2477-87
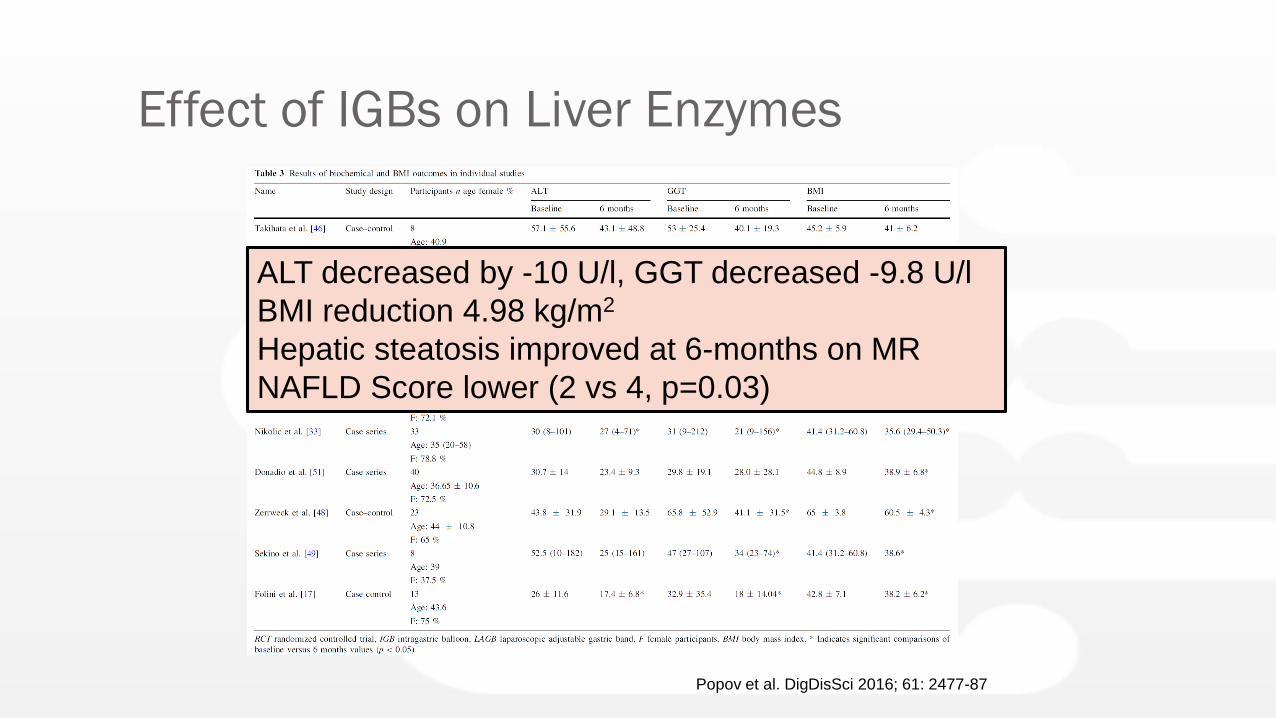
Effect of IGBs on Liver Enzymes
Popov et al. DigDisSci 2016; 61: 2477-87
ALT decreased by -10 U/l, GGT decreased -9.8 U/l
BMI reduction 4.98 kg/m2
Hepatic steatosis improved at 6-months on MR
NAFLD Score lower (2 vs 4, p=0.03)

Endoscopic Sleeve Gastroplasty
(ESG)
Background
• Bariatric interventions offer a more efficacious and
durable weight loss than non-surgical approaches
• Surgical weight loss procedures are limited by
appeal, availability, cost and short and long term
risks
• Endoscopic Sleeve Gastroplasty is an incisionless,
minimally invasive technique
• Clinically significant improvements in obesity related
co-morbidities are higher when %TBWL exceeds
10%.
(lifestyle intervention typically results in 3-5% TBWL)
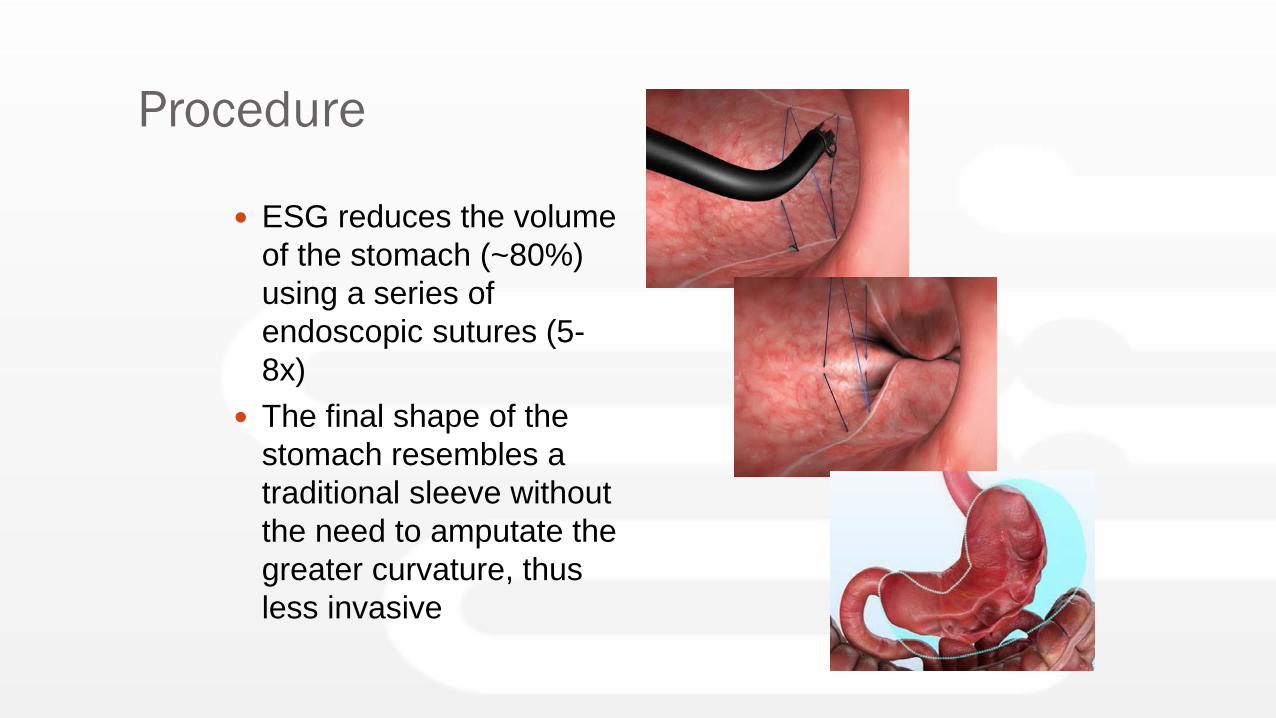
Procedure
ESG reduces the volume
of the stomach (~80%)
using a series of
endoscopic sutures (5-
8x)
The final shape of the
stomach resembles a
traditional sleeve without
the need to amputate the
greater curvature, thus
less invasive
Patient Selection and Exclusion
Recommendations
Age: 18-65+
BMI: 30-40 (BMI is not limited to 40. The IFSO/OSSANZ bariatric guidelines are followed)
Compliant with prescribed diet, aftercare instructions
Exclusion RecommendationFamily history of Stomach Cancer
Hiatus hernia >5cm
Previous gastric surgery
Gastric ulceration
Cirrhosis
Pregnancy or plans of pregnancy in the next 12 months
Coagulation disorders or chronic use of anticoagulants***
Any active medical condition that would preclude a safe endoscopic suturing repair
***at the discretion of the treating physician
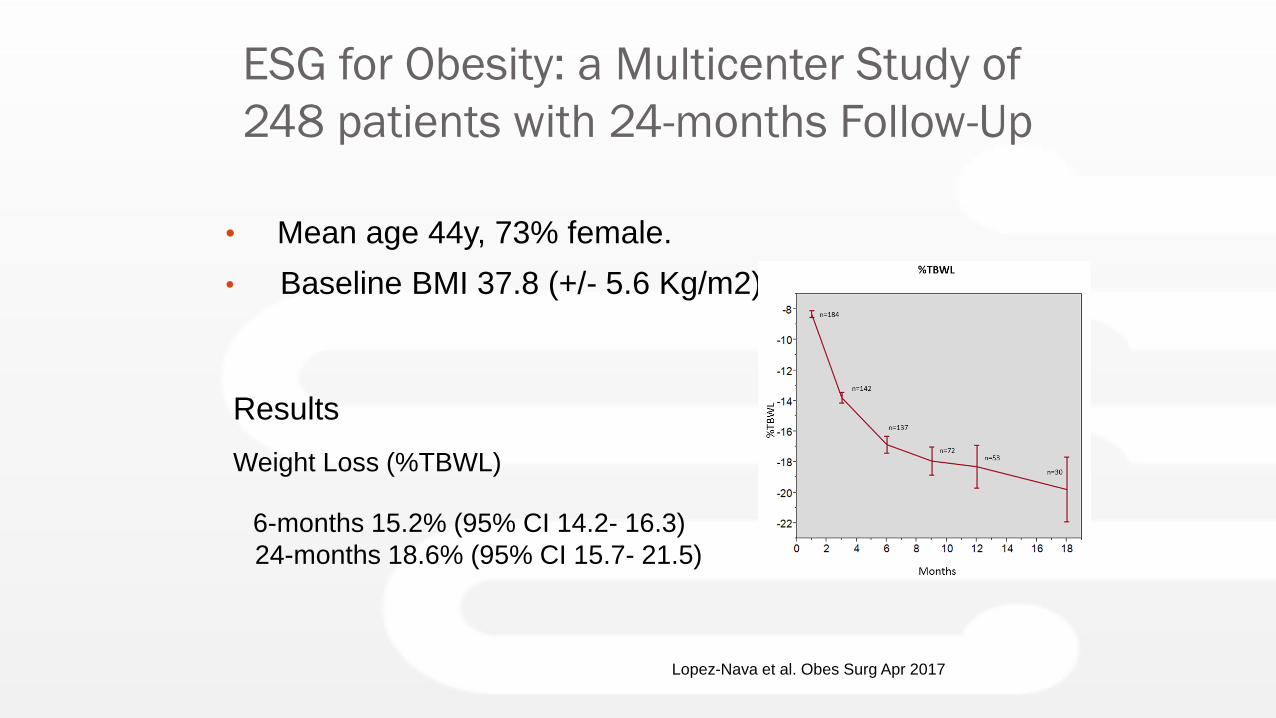
ESG for Obesity: a Multicenter Study of
248 patients with 24-months Follow-Up
• Mean age 44y, 73% female.
• Baseline BMI 37.8 (+/- 5.6 Kg/m2)
Weight Loss (%TBWL)
6-months 15.2% (95% CI 14.2- 16.3)
24-months 18.6% (95% CI 15.7- 21.5)
Results
Lopez-Nava et al. Obes Surg Apr 2017
Endoscopic Sleeve Gastroplasty;
1-year Follow-Up
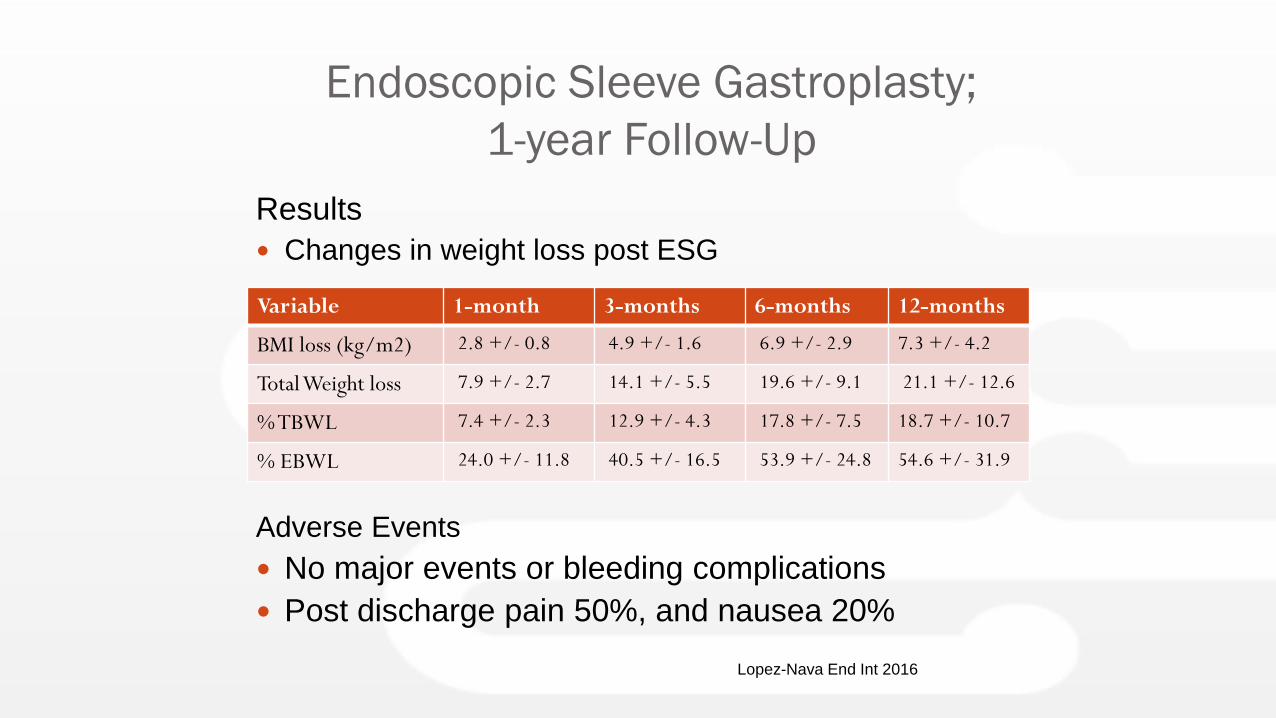
Results
Changes in weight loss post ESG
Adverse Events
No major events or bleeding complications
Post discharge pain 50%, and nausea 20%
Variable 1-month 3-months 6-months 12-months
BMI loss (kg/m2) 2.8 +/- 0.8 4.9 +/- 1.6 6.9 +/- 2.9 7.3 +/- 4.2
Total Weight loss 7.9 +/- 2.7 14.1 +/- 5.5 19.6 +/- 9.1 21.1 +/- 12.6
% TBWL 7.4 +/- 2.3 12.9 +/- 4.3 17.8 +/- 7.5 18.7 +/- 10.7
% EBWL 24.0 +/- 11.8 40.5 +/- 16.5 53.9 +/- 24.8 54.6 +/- 31.9
Lopez-Nava End Int 2016
Endoscopic Sleeve Gastroplasty;
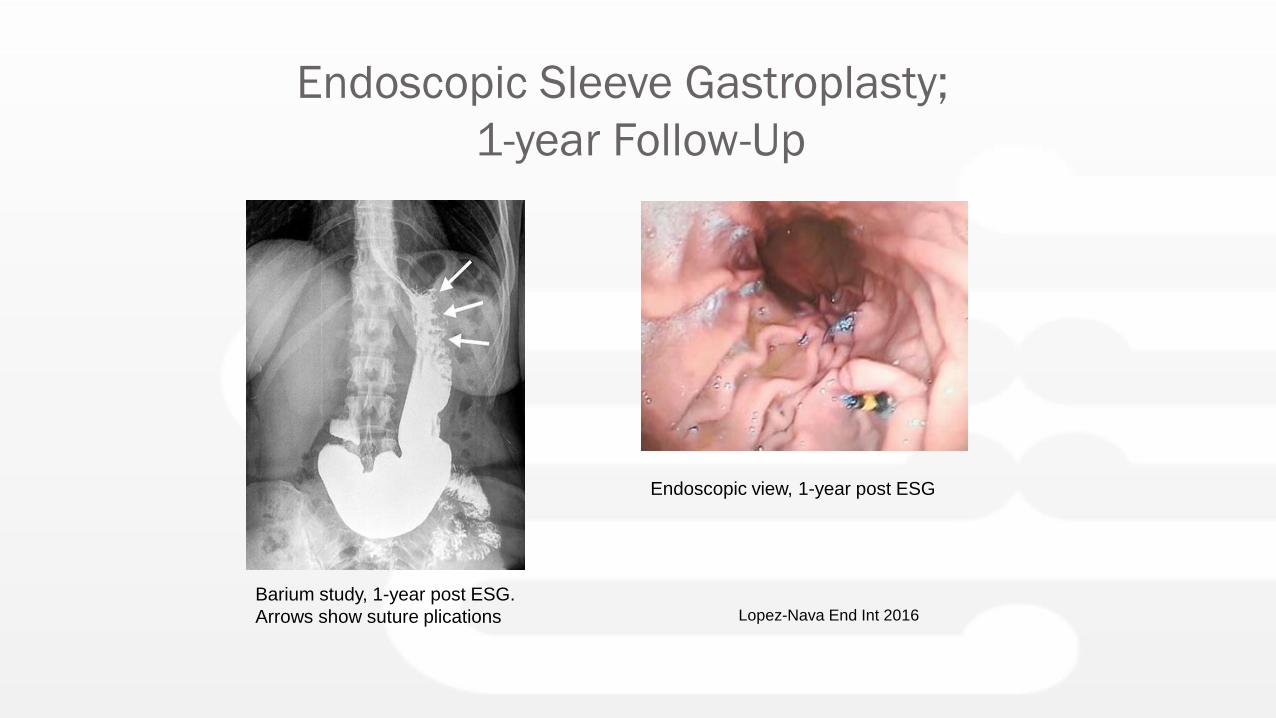
1-year Follow-Up
Barium study, 1-year post ESG.
Arrows show suture plications
Endoscopic view, 1-year post ESG
Lopez-Nava End Int 2016
Endoscopic Sleeve Gastroplasty: Gastric
Physiology
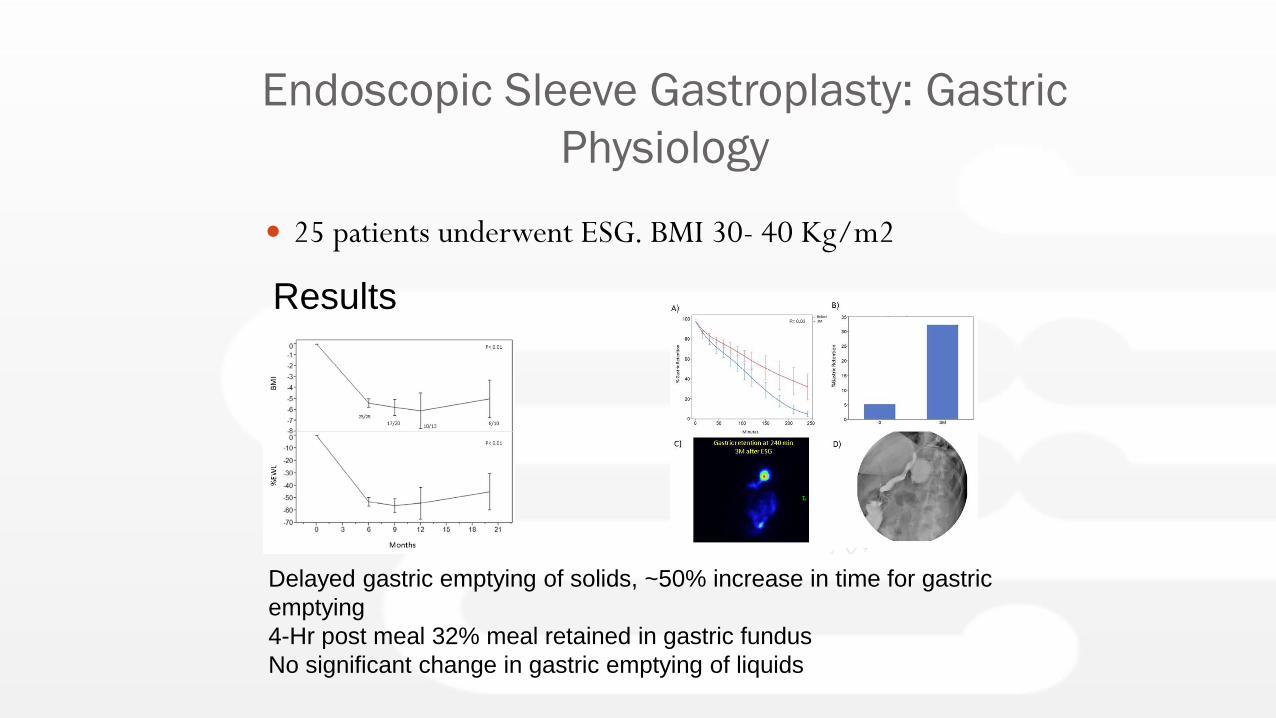
25 patients underwent ESG. BMI 30- 40 Kg/m2
Results
Delayed gastric emptying of solids, ~50% increase in time for gastric
emptying
4-Hr post meal 32% meal retained in gastric fundus
No significant change in gastric emptying of liquids
Endoscopic Sleeve Gastroplasty: Gastric
Physiology
Results
ESG increases satiation with a 59% decrease in
calorie intake to reach maximum fullness (meal
tolerance test)
Postprandial ghrelin levels decreased by 29.4% (no
statistically significant changes in leptin, GLP-1 and
PYY)
Insulin sensitivity improved (HOMA-IR reduced by
>30%)
Endoscopic Sleeve Gastroplasty
ESG is an effective and durable treatment for
weight loss
Weight loss at 2 years ~18-20% TBWL
Low morbidity
Successful weight loss requires a multidisciplinary
approach
Endoscopic Sleeve Gastroplasty
ESG is an effective and durable treatment for
weight loss
Weight loss at 2 years ~18-20% TBWL
Low morbidity
Successful weight loss requires a multidisciplinary
approach
Available at the
MacMurray Centre
Conclusions
Obesity and obesity related complication
prevalence is rapidly increasing.
A multidisciplinary and population based approach
is required.
- Diet, exercise and behavioural management
- ?Pharmacologic treatments
- Endoscopic treatment:
Intra-gastric balloon
Endoscopic sleeve gastroplasty
- Surgical treatment

The only fully comprehensive
Gastroenterology center in Auckland
Opened in 2009
Largest Gastro practice in NZ
12 Gastroenterologists
1 Paediatric Gastroenterologist
1 Hepatologist
4 Surgeons
Dietician
Full diagnostic facilities on site