
Ms COPY Form 990 Return of Organization Exempt From Income...
40
Department of the Treasury Sntemal Reveri5e Service A Fps the 2002 caten& B Cneckeappkab4 Please C Address ~aeIR3 change r label or Name ,hang' ant or Initial raNn typ0 . Fmai room See Specific Amended return 1114t1UC- AGChcallon Uons. pending I I& City or town, state or country, and ZIP + 4 mkno0: " Cash LJ Accrual I I Other(specdy) 1 H and 1 are not applicable to section 527 organizations H(a) Is this a group return for affiliates? F1 Yes 0 No H(b) If "Yes," enter number of affiliates 1 N A H(c) Are all affiliates included Yes No (If "Na," attach a list See instructionsg H(d) Is this a separate return filed by an I~ organization covered by a group rullng~ I I Yes n Ho I Enter 4-digd GEN 1 N/ A M Check 1 d the organization is not required to attach Sch 8 (Form 990, 990-EZ, or 990-PF) G Web site : 1WW , GBMC . ORG J Organization type (check only one) 1 g 501(c) ( 0 3 ) ~ (insert no ) 4947(a)(1) or 527 K Check here 1 if the organization's gross receipts are normally not more than $25,000 The organization need not file a return with the IRS, but if the organization received a Form 990 Package in the mad, it should file a return without financial data Some states require a complete return . L Gross receipts Add lines 6b, 8b, 9b, and 10b to line 12 0' l Revenue . Expenses, and Chances in Net Assets or Fund Balances (See oaae 17 of the instructions. 572,918 . 537 7 5 . 489 . Form 990 (2002) 9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1 Form 990 Ms COPY Return of Organization Exempt From Income Tax Under section 501(c), 527, or 4947(a)(1) of the Internal Revenue Code (except black lung benefit trust or private foundation) " The organization may have to use a copy of this return to satisfy state reporting requirements ear or tax ear be g innin g 07/01 2002 and ending 06 / 30 / 2003 Name of organization D Employer Identification number Number and street (or P O box if mad is not delivered to street address) I Room/suite I E Telephone number 0 Section 601(c)(3) organizations and 4947(a)(1) nonexempt charitable trusts must attach a completed Schedule A (Form 990 or 990-EZ) . 1 Contributions, gifts, grants, and similar amounts received a Direct public support , , , , , , , , , , , , , , , , , , , , , , , , 1 a 8 , 017 , 884 . b Indirect public support , 1 b c Government contributions (grants) , , , , , , , , , , , , , , , , , 1 c 555 , 034 . d Total (add lines 1a through 1c) (cash S 8 , 411 , 643 . noneash E 161 , 275 . ) 1 d 2 Program service revenue including government fees a o-{i a ine 93) , , , , , , 2 3 Membership dues and assessments , , , , REr% .E~ 3 4 Interest on savings and temporary cash investments , , " , " , , , , , , , , , , , , " C/3 " , , , , , , , 4 5 Dividends and interest from securities ~ 5 6a Gross rents . . . . . . . . . . . . . . . . . . . 0 . 2's~'2~~~ . N . . . . . . . b Less rental expenses ~C c Net rental income or (loss) (subtract line 6b from fine 6 ) , O ~4D ~ C I~ l~.1 I . . . . . . . 6c ~~ 03 7 Other investment income (describe " ~'d 7 8 a Gross amount from sales of assets other (A) Securities (B) other than inventory , 40 , 599 . 8a 33 , 470 . b Less cost or other basis and sales expenses , 39 , 961 . 8 b 33 , 470 . c Gain or (loss) (attach schedule) 5^~T .2A 638 . 8c d Net gain or (loss) (combine line 8c, columns (A) and (B)) , , , , , , , , , , , , , , , , , , , , , , , , 8d 9 Special events and activities (attach schedule) a Gross revenue (not including $ 75 , 511 . of contributions reported on line 1a), , , , ,STM ,z , , , $TW, 3 9a 68 , 004 . b less' direct expenses other than fundraising expenses , , , , , , , , 9 b 56 , 385 . c Net income or (loss) from special events (subtract line 9b from line 9a) . . . . . . . . . . . . . . 9c 10a Gross sales of inventory, less returns and allowances , , , , , , , , oa b Less cost of goods sold , , , , , , , , , , , , , , , , , , , , , , ob c Gross profit or (loss) from sales of inventory (attach schedule) (subtract line 10b from line 10a) , , , , , 1 Oc 11 Other revenue (from Part VII, line 103) , 11 12 Total revenue (add lines 1d . 2 . 3 . 4 . 5 . 6c . 7 . 8d . 9c . 10c . and 11) " " " " " " " " " " " " " . " . " . 12 13 Program services (from line 44, column (B)) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . v 0 14 Management and general (from line 44, column (C)) , , , , , , , , , , , , , , , , , , , , , , , , , , 15 Fundraising (from line 44, column (D)) , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 16 Payments to affiliates (attach schedule) , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 17 Total ex p enses add lines 16 and 44 column A 18 Excess or (deficit) for the year (subtract line 17 from line 12) , , 19 Net assets or fund balances at beginning of year (from line 73, column (A)) , 20 Other changes in net assets or fund balances (attach explanation) , , , , , S =A , , $TI4T, S , C7 21 Net assets or fund balances at end of ear combine lines 18 19 and 20 JSA For Paperwork Reduction Act Notice, see the separate instructions . 2E1010 7 000 -16 .64
Transcript of Ms COPY Form 990 Return of Organization Exempt From Income...

Department of the Treasury Sntemal Reveri5e Service
A Fps the 2002 caten& B Cneckeappkab4 Please C
Address ~aeIR3 change r
label or Name ,hang' ant or
Initial raNn typ0.
Fmai room See
Specific Amended return 1114t1UC-AGChcallon Uons. pending I I&
City or town, state or country, and ZIP + 4 mkno0: " Cash LJ Accrual
I I Other(specdy) 1
H and 1 are not applicable to section 527 organizations
H(a) Is this a group return for affiliates? F1 Yes 0 No H(b) If "Yes," enter number of affiliates 1 N A H(c) Are all affiliates included Yes No
(If "Na," attach a list See instructionsg H(d) Is this a separate return filed by an I~
organization covered by a group rullng~ I I Yes n Ho
I Enter 4-digd GEN 1 N/A
M Check 1 d the organization is not required
to attach Sch 8 (Form 990, 990-EZ, or 990-PF)
G Web site : 1WW , GBMC . ORG J Organization type (check only one) 1 g 501(c) ( 0 3 ) ~ (insert no ) 4947(a)(1) or 527
K Check here 1 if the organization's gross receipts are normally not more than $25,000 The
organization need not file a return with the IRS, but if the organization received a Form 990 Package
in the mad, it should file a return without financial data Some states require a complete return .
L Gross receipts Add lines 6b, 8b, 9b, and 10b to line 12 0'
l Revenue . Expenses, and Chances in Net Assets or Fund Balances (See oaae 17 of the instructions.
572,918 .
537
7 5 .
489 .
Form 990 (2002)
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
Form 990 Ms COPY
Return of Organization Exempt From Income Tax Under section 501(c), 527, or 4947(a)(1) of the Internal Revenue Code (except black lung
benefit trust or private foundation) " The organization may have to use a copy of this return to satisfy state reporting requirements
ear or tax ear beginning 07/01 2002 and ending 06/30 /2003 Name of organization D Employer Identification number
Number and street (or P O box if mad is not delivered to street address) I Room/suite I E Telephone number
0 Section 601(c)(3) organizations and 4947(a)(1) nonexempt charitable trusts must attach a completed Schedule A (Form 990 or 990-EZ) .
1 Contributions, gifts, grants, and similar amounts received a Direct public support , , , , , , , , , , , , , , , , , , , , , , , , 1 a 8 , 017 , 884 . b Indirect public support � � � � � � � � � � � , 1 b c Government contributions (grants) , , , , , , , , , , , , , , , , , 1 c 555 , 034 . d Total (add lines 1a through 1c) (cash S 8 , 411 , 643 . noneash E 161 , 275 . ) 1 d
2 Program service revenue including government fees a o-{i a ine 93) , , , , , , 2 3 Membership dues and assessments , , , , REr%.E~ 3 4 Interest on savings and temporary cash investments , ,
" , " , , , , , , , , , , , , " C/3 " , , , , , , , 4
5 Dividends and interest from securities ~ 5 6a Gross rents . . . . . . . . . . . . . . . . . . . 0 . 2's~'2~~~ . N . . . . . . .
b Less rental expenses � � � � � � � ~C c Net rental income or (loss) (subtract line 6b from fine 6 ) , O ~4D ~ C I~ l~.1 I .
. . . . . . 6c
~~ 03 7 Other investment income (describe " ~'d 7 8 a Gross amount from sales of assets other (A) Securities (B) other
than inventory � � � � � � � , 40 , 599 . 8a 33 , 470 . b Less cost or other basis and sales expenses , 39 , 961 . 8 b 33 , 470 . c Gain or (loss) (attach schedule) 5^~T .2A 638 . 8c d Net gain or (loss) (combine line 8c, columns (A) and (B)) , , , , , , , , , , , , , , , , , , , , , , , , 8d
9 Special events and activities (attach schedule) a Gross revenue (not including $ 75 , 511 . of
contributions reported on line 1a), , , , ,STM ,z , , , $TW, 3 9a 68 , 004 . b less' direct expenses other than fundraising expenses , , , , , , , , 9 b 56 , 385 . c Net income or (loss) from special events (subtract line 9b from line 9a) . . . . . . . . . . . . . . 9c
10a Gross sales of inventory, less returns and allowances , , , , , , , , oa b Less cost of goods sold , , , , , , , , , , , , , , , , , , , , , , ob c Gross profit or (loss) from sales of inventory (attach schedule) (subtract line 10b from line 10a) , , , , , 1 Oc
11 Other revenue (from Part VII, line 103) � � � � � � � � � � � � � � � , 11 12 Total revenue (add lines 1d . 2 . 3 . 4 . 5 . 6c . 7 . 8d . 9c . 10c . and 11) " " " " " " " " " " " " " . " . " . 12 13 Program services (from line 44, column (B)) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
v 0 14 Management and general (from line 44, column (C)) , , , , , , , , , , , , , , , , , , , , , , , , , , 15 Fundraising (from line 44, column (D)) , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 16 Payments to affiliates (attach schedule) , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 17 Total expenses add lines 16 and 44 column A 18 Excess or (deficit) for the year (subtract line 17 from line 12) , , 19 Net assets or fund balances at beginning of year (from line 73, column (A)) , 20 Other changes in net assets or fund balances (attach explanation) , , , , , S =A , , $TI4T, S , C7 21 Net assets or fund balances at end of ear combine lines 18 19 and 20
JSA For Paperwork Reduction Act Notice, see the separate instructions . 2E1010 7 000
-16 .64

------------------------------------------------------------------------------------------------------------------------------------------------------
(Grants and allocations $ )
---------------------------------------------------------------------------(Grants and allocations $ 250 .
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
s2-soassse Form 990 (2002) Page 2
Statement of All organizations must complete column (A) Columns (B), (C), and (D) are required for section 501(c)(3) and (4) organizations Functional Expenses and section 4947(a)(1) nonexempt charitable trusts but optional for others (See page 21 of the instructions )
Do not include amounts reported on line p Total (e) Program (c) Management a _9 of P"rt 1. services and eneral (D) Fundraising 6b . b A . 1016
22 grants and allocations (attach schedule)
(cash S nanash S ) 22
23 Specific assistance to individuals (attach schedule) 23
24 Benefits paid to or for members (attach schedule) 24
25 Compensation of officers, directors, etc . 25 1 , 612 , 640 . 1 , 612 , 640 . 28 Other salaries and wages , , , , , , , 26 133 575 107 . 105 , 18"4 , 895 . 28 , 390 , 212 . 27 Pension plan contributions 27 4 , 611 , 293 . 4 , 611 , 293 . 28 Other employee benefits , , , 28 13 , 929 , 359 . 290 186 . 13 639 173 . 29 Payroll taxes , , , , , , , , , , , , , , 29 8 , 338 , 667 . -178 , 989 . 8 1 517 , 656 . 30 Professional fundraising fees , , , , , 30 31 Accounting fees , , , , , , , , , , , , 31 117 381 . -34 , 779 . 152 , 160 . 32 Legal fees , , , , , , , , , , , , , , , 32 422 , 014 . 1 , 641 . 420 373 . 33 Supplies , , , , , , , , , , , , , , , , 33 59 286 163 . 53 358 506 . 5 1 927 , 657 . 34 Telephone , , , , , , , , , , , , , , , 34 1 , 065 , 611 . 189 772 . 875 839 . 35 Postage and shipping , , , , 35 436 , 348 . 312 243 . 124 105 . 38 Occupancy 36 2 , 651 , 543 . 1 , 823 , 202 . 828 341 . 37 Equipment rental and maintenance . , 37 3 , 520 , 085 . 2 257 101 . 1 1 262 , 984 . 38 Printing and publications , , , , , , , 38 2 , 713 , 739 . 2 , 340 044 . 373 695 . 39 Travel� � � � � � � � � 39 318 , 181 . 184 123 . 134 058 . 40 Conferences, conventions, and meetings , 40 395 , 537 . 151 164 . 244 , 373 . 41 Interest, ,
. e ~,41 4 04 , 273 . 4 , 2--9-5 , 481 . 8 792 .
42 Depreciation, depletion, etc (attach scdr'ulej,~ 42 17 346 185 . 14 818 220 . 2 .527 965 . 43 other expenses not covered above ortemize) STMT 6 3a 31 , 142 , 670 . 15 , 870 , 193 . 15 , 272 , 477 .
b 3b c 43c d 3d
3e 44 Total functional expenses (add lines 22 through e3)
Organizations a eM eolumt -- time totals rounes 13~s , , 44 285 786 796 . 200 863 003 . 84 923 793 .
Joint Costs. Check " if you are following SOP 98-2 Are any point costs from a combined educational campaign and fundraising solicitation reported in (B) Program services? , , , , , " 7 Yes aX No If "Yes," enter (i) the aggregate amount of these joint costs $ , (ii) the amount allocated to Program services $ (ii) the amount allocated to Management and general $ , and (iv) the amount allocated to Fundraising $
_ e~ ..~,. . . ..,. . .a ,.s o. . . .. . .. ..., e .. .. . : ..,, n.. . . .. .. . ..r. ..ti .., . . ..a~ lees .. .,..e ')A ,.s 4ti- ; .,~~.. �.~c . . .. .. N
What is the organization's primary exempt purpose? " STMT 7 r~vy~am ~ervIca
Expenses All organizations must describe their exempt purpose achievements in a clear and concise manner. State the number (Required for 501 (c)(3) and of clients served, publications issued, etc Discuss achievements that are not measurable (Section 501(c)(3) and (4) (4) orgs , and a9a7(a)(t)
organizations and 4947(a)(1) nonexempt charitable trusts must also enter the amount of grants and allocations to others ) trusts, but optional for
others )
a DAILY HOSPITAL-SERVICE-PROVIDED-90,752 DAYS OF CARE_______________________
----------------------------------------------------------------------------------------------------------------------------------------------
(Grants and allocations $ - ) I 57 b OPERATING ROOM_PERFORMED_40,175_SURGICAL PROCEDURES_______________________
c CLINIC-TREATED-81,808-PATIENTS EMERGENCY ROOMS TREATED_49~735_PATIENTS ___________________
d LABORATORY_SERVICE_PERFORN4:D_965f312_ LAB TESTS____________________________
---------------------------------------------------------------------------MEDICAL CENTER_PROVIDED_$2,,9241614_OF CHARITY -CARE ________________________
Grants and allocations $ 13 , 528 , 264 e Other program services attach schedule STMT B Grants and allocations $ 43 144 , 967 .
JSA f Total of Program Service Expenses (should equal line 44, column (B), Program services) . , . . " 200,863,003 . 2e1o2o,ooo Form 990 (2002)

JSA 2E7030 7 000
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
52-6049658 Form 990 (2002) Page 3
" Balance Sheets See page 24 of the instructions . Note: Where required, attached schedules and amounts within the description (A) (B)
column should be for end-of-year amounts only. Beginning of year End of year 45 Cash - non-interest-bearing . . . . . . . . . . . . . . . . . . . . . , , , , , . 18 , 728 . 45 NONE 46 Savings and temporary cash investments . . . . . . . . . . . . , . , . , , , , 25 96,721 . 46 36 871 064 .
47a Accounts receivable , , , , , , , , , , , , , , , , 47a 44 193 193 . b Less . allowance for doubtful accounts , , , , , , 47b 4 , 484 , 519 . 44 , 048 , 268 . 47c 39 708 674 .
48a Pledges receivable , , , , , , , , , , , , , , , , , 48a 9 , 026 , 833 . b Less' allowance for doubtful accounts, , , , , , , 48b NO 48c 9 , 02 6 833 .
49 Grants receivable ���������������� 49 50 Recervables from officers, directors, trustees, and key employees
(attach schedule) ���������������� , 50 51a Other notes and loans receivable (attach
schedule) , , , , , , , , , , , , , , , , , , , , , , 51a b Less allowance for doubtful accounts , , , , , , 51 b SIC
Q 52 inventories for sale or use , , , , , , , , , , , , , , , , , , , , , , , , , , , , 3 , 245 , 290 . 52 3 , 690 , 983 . 53 Prepaid expenses and deferred charges . . . . . . . . . . . . . . . . . . . . . 1 , 875 , 494 . 53 3 532 724 . 54 Investments - securities (attach schedule) $T= ,9, " 0 Cost J] FMV 60 , 014 , 447 . 54 59 , 191 , 669 . 5Sa Investments - land, buildings, and
equipment basis � � � � � � � � � 55a b Less accumulated deprecation (attach
schedule ) , , , , , , , , , , , , , , , , , , , , , , 55b 55c 56 Investments - other (attach schedule) . , . . . . . . . . . , , , , , , , , , 56 57a Land, buildings, and equipment' basis 57a 319 , 169 , 780 .
b Less accumulated deprecation (attach schedule) , , , , , , , , , , , , , , 3?r!'~T 57b 165 442 894 . 153 401 122 . 57c 153 726 886 .
58 Other assets (describe " STMT 10 ) 25 341 985 . 58 18 589 880 .
59 Total assets add lines 45 throw h 58 must equal line 74 ~ ~ ~ " ~ " " - - - " 313 , 642 , 055 . 59 324 338 713 . 60 Accounts payable and accrued expenses , , , , , , , , , , , , , , , , , , , , 30 , 924 : 313 . 60 31 151 191 . 61 Grants payable ����������������� 81 62 Deferred revenue � . . ., . . � ., ., . . . . . . . . . . . ., . � . . . 62
d 63 Loans from officers, directors, trustees, and key employees (attach schedule) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
j 64a Tax-exempt bond liabilities (attach schedule) . . . . . . . . . . . STMT. 11 . 124 807 631 . 84a 122 , 246 , 866 . b Mortgages and other notes payable (attach schedule) , , , , , , , , , , , , , 64b
65 Other liabilities (describe " STMT 12 ) 20 967 913 . 65 41 , 31 6 566 .
66 Total liabilities add lines 60 through 65 . . . . . . . . . . . . . . . . . . . . 176 , 699 , 857 . 66 194 714 623 . Organizations that follow SFAS 117, check here " U and complete lines
67 through 69 and lines 73 and 74 w 67 Unrestr i cted 116 , 666 , 669 . 67 105 , 536 , 372
68 Temporarily restricted , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 18 , 221 , 358 . 68 20 220 923 . m 69 Permanently restricted . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 , 054 , 171 . 69 3 , 866 , 795 .
Organizations that do not follow SFAS 117, check here 10, 0 and complete lines 70 through 74 .
0 70 Capital stock, trust principal, or current funds 70 71 Paid-in or capital surplus, or land, budding, and equipment fund 71
~; 72 Retained earnings, endowment, accumulated income, or other funds , , , , , 72 N a 73 Total net assets or fund balances (add lines 67 through 69 or lines
70 through 72, column (A) must equal line 19 ; column (B) must equal line 21) , , , , , , , , 136 942 198 . 73 129 624 090 .
74 Total liabilities and net assets I fund balances add lines 66 and 73 . 313 642 055 . 74 324 , 338 , 713 .
Form 990 is available for public inspection and, for some people, serves as the primary or sole source of information about a particular organization How the public perceives an organization in such cases may be determined by the information presented on its return Therefore, please make sure the return is complete and accurate and fully describes, m Part III, the organization's programs and accomplishments.

Form 990 52-6049658
4
per
8
4 , 301 , 680 . STMT 14 i 4,194,818 . Add amounts on lines (1) through (4) , , " b
5 , 111 , 285 . c Line a minus line b , , , , , , , , , t c d Amounts included on line 17,
Form 990 but not on line a : (1) Investment expenses
not included on line 6b, Form 990 , , , S
(2) Other (specify)
c Line a minus line b t d Amounts included on line 12,
Form 990 but not on line a: (1) Investment expenses
not included on line 6b, Form 990 , ,
(2) Other (specify) .
$ s Add amounts on lines (1) and (2) , , " d Add amounts on lines (1) and (2) , , " d
e Total revenue per line 12, Form 990 e Total expenses per line 17, Form 990 line c plus line d . . . . . . . . . . " e 295 111 285 . line c plus line d ~ ~ " " " " " ~ ~ ~ " e 285 . 786 . 796 .
List of Officers, Directors, Trustees, and Key Employees (List each one even if not compensated, see page 26 of
75 Did any officer, director, trustee, or key employee receive aggregate compensation of more than $100,000 from your organization and all related organizations, of which more than $10,000 was provided by the related organizations? " a Yes aX No If "Yes," attach schedule - see page 26 of the instructions
Fog 990 (2002)
JSA 2 E 10 d0 1 000
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
a Total revenue, gains, and other support per audited financial statements , , " a
b Amounts included on line a but not on line 12, Form 990:
(1) Net unrealized gains on investments , , $
(2) Donated services and use of facilities $
(3) Recoveries of prior year grants , , , , S
(4) Other (specify)-
STMT 13 $ 4,301,680 . Add amounts on lines (1) through (4) "~
a Total expenses and losses per 412 , 965 . audited financial statements " a
b Amounts included on line a but not on line 17, Form 990'
(1) Donated services and use of facilities $
(2) Prior year adjustments reported on line 20, Form 990 , , , , , $
(3) Losses reported on line 20, Form 990 $
(4) Other (specify),

9NGOGM 2536 05/13/2004 12 :29 :19 V02-8 .1
rorm uav cwc ~~-ovy~v~o raea Other Information See page 27 of the instructions . Yes No
76 Did the organization engage in any activity not previously reported to the IRS? If "Yes," attach a detailed description of each activity , , 76 X 77 Were any changes made in the organizing or governing documents but not reported to the IRS? , , , , , , , , , , , , , , , , , , , 77 X
If "Yes," attach a conformed copy of the changes 78a Did the organization have unrelated business gross income of $1,000 or more during the year covered by this return? , , , , , , , , , 78a X
b If "Yes," has it filed a tax return on Form 990-T for this year? , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 78b X 79 Was there a liquidation, dissolution, termination, or substantial contraction during the year? If "Yes ;" attach a statement , , , , 79 X 80a Is the organization related (other than by association with a statewide or nationwide organization) through common
membership, governing bodies, trustees, officers, etc , to any other exempt or nonexempt organization? . , . . . . . . . . STMT. 16 80a X b If "Yes," enter the name of the organizationt
and check whether d is X exempt or nonexempt. 81 a Enter direct or indirect political expenditures See line 81 instructions , , , , , , , , , , , , , , , , 81a NO
b Did the organization file Form 1120-POL for this year? , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 81b N 82a Did the organization receive donated services or the use of materials, equipment, or facilities at no charge
or at substantially less than fair rental value? 82a X b If "Yes," you may indicate the value of these items here Do not include this amount as revenue in Part I or as an expense in Part II (See instructions in Part III ) , , , , , , , , , , , , , , 82b 10 , 594 .
83a Did the organization comply with the public inspection requirements for returns and exemption applications? , , , , , , , 83a X b Did the organization comply with the disclosure requirements relating to quid pro quo contributions? , , , , , , , , , , , , , , , , , 83b X
84a Did the organization solicit any contributions or gifts that were not tax deductible? , , , , , , , , , , , , , , , , . , , , , , , , . . 84a X b If "Yes," did the organization include with every solicitation an express statement that such contributions
or gifts were not tax deductible? , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , . . . , , , , , , , , , , , . 84b N 85 501(c)(4), (5), or (6) organizations a Were substantially all dues nondeductible by members? . . . . . . . . . . . . . . . . . . . . . 85a N
b Did the organization make only in-house lobbying expenditures of $2,000 or less? , . . , . , . . . . . . . . . . . . . . . . . . , . 85b N If "Yes" was answered to either 85a or 85b, do not complete 85c through 85h below unless the organization received a waiver for proxy tax owed for the prior year
c Dues, assessments, and similar amounts from members . . . . . . . . . . . . . . . . . . . . . . . 85c N/A d Section 162(e) lobbying and political expenditures , , , , , , , , , , , , , , , , , , , , , , , , , 85d N/A e Aggregate nondeductible amount of section 6033(e)(1)(A) dues notices , , , , , , , , , , , , , , , 85e N/A f Taxable amount of lobbying and political expenditures (line 85d less 85e) , , . . . . . , . , , , , . 86( N/A g Does the organization elect to pay the section 6033(e) tax on the amount on line 85f9 , , , . . . 85 N h If section 6033(e)(1)(A) dues notices were sent, does the organization agree to add the amount on line SSf to it reasonable estimate of dues allocable to nondeductible lobbying and political expenditures for the following tax year? , , , , . , , . , , , , , , 85h N
86 501(c)(7) orgs Enter' a Initiation fees and capital contributions included on line 12 , , , , , 86a N/A b Gross receipts, included on line 12, for public use of club facilities , , , , , , 86b N/A
87 501(c)(12) orgs. Enter a Gross income from members or shareholders , . , . , , , , , , , 87a N/A b Gross income from other sources . (Do not net amounts due or paid to other
sources against amounts due or received from them ) , , , , , , , , , , , , , . . . _ . . . . . . , 87b N/A 88 At any time during the year, did the organization own a 50% or greater interest in a taxable corporation or
partnership, or an entity disregarded as separate from the organization under Regulations sections 301 7701-2 and 301 7701-37 If "Yes ;" complete Part IX 88 X
89a 501(c)(3) organizations Enter Amount of tax imposed on the organization during the year under. section 4911 jo- NONE , section 4912 " NONE ; section 4955 lo- NONE
b 50 1(c)(3) and 501(c)(4) orgs. Did the organization engage in any section 4958 excess benefit transaction during the year or did it become aware of an excess benefit transaction from a prior year? If "Yes," attach a statement explaining each transaction , , . , , . . , . . , , , , . . . . , , . , . . . . . . . . . . . , , , , . . . . . . . , . 89b X
c Enter . Amount of tax imposed on the organization managers or disqualified persons during the year under sections 4912,4955,and4958
**''''''****''''*''**''''*'***'***' . . . . . . . . , , , , " NONE
d Enter' Amount of tax on line 89c, above, reimbursed by the organization . , . . . . . . . . . . . . . . . , . . . . . . . , , , ~ NONE 90a List the states with which a copy of this return is filed jMARYLAND
b Number of employees employed in the pay period that includes March 12, 2002 (See instructions) , , , , , , , , , , , , , , , , , , 1 90b 1 2940
91 The books are in care of 1 DANIEL E'EELEY Telephone no 01 443-204-8121
Located at 1 10085 RED RUN BLVD , OWINGS MILLS , I1D ZIP +4 1 21117
92 Section 4947(a)(1) nonexempt charitable trusts filing Form 990 in lieu of Form 1041-Check here , . . , , , , , "
, . , . . . . , 10.0 and enter the amount of tax-exempt interest received or accrued during the tax year . 92 ~ N/A
Form 990 (2002)
JSA 2E1041 1 000

s Note: Enter graze amounts unless otherwise Unrelated business inc indicated.
Business Amount 93 Program service revenue. code
4 PATIENT SERVICE b OTHER OPERATING c d
e
f Medicare/Medicaid payments , , , , ,
g Fees and contracts from government agendas , 94 Membership dues and assessments . ,
95 Interest an savings and temporary cash investments
96 Dividends and interest from securities
97 Net rental income or (loss) from real estate .
a debt-financed property . . . . . . . .
b not debt-financed property . . . . . . . 98 Net rental income or (loss) tram personal property
99 Other investment income . . . . . . .
100 Gam or (doss) from saes of asset other than inventory 101 Net income or (loss) from special events .
102 Gross profit or (loss) ham sales of inventory ,
103 Other revenue a
b STMT 17 43 , 90! c d e
104 Subtotal (add columns (B), (D), and (E)) . . ~ ~ 4 . 105 Total (add line 104, columns (B), (D), and (E)) . . . . . . . . . . . . . Note: Line 105 plus line 1d, Part l, should equal the amount on line 12, Part l.
638 .
,905 .1 1 2,902,307 .1 283,592,155 . " . . . . . . . . " " " " " . " 286 , 538 , 367 .
Line No . Explain how each activity for which income is reported in column (E) of Part VII contributed importantly to the accomplishment of the oraamzation's exempt ouroases (other than by orovidina funds for such ourooses) .
(A) I (B~ I (C) I (D) I (Ef Name, address, and EIN of corporation, Percentage or Nature of activities Total income End -o -year partnership, or disregarded entity ownership interest assets
2E1050 1 000
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
:luded b section 512 513 or 514 Related or
;c usion Amount exempt function code inrnma
7 .
Information Regarding Transfers Associated with Personal Benefit Contracts See page 33 of the instructions (a) Did the organization, during the year, receive any funds, directly or indirectly, to pay premiums on a personal benefit contracts Yes X No (b) Did the organization, during the year, pay premiums, directly or indirectly, on a personal benefit contracts Yes g No Note : If "Yes" to l61 . file Form 8870 and Form 4720 (see instnic6
Under enalties of penury, I declare that I have examined this and be Pef, it zee, correct an om to Declaration of pry
Please Sign I Signature of officer Here ' .t, k / e ,C ~
Type r ~ c,yre2
Type or print name and tale
Preparers Paid signature' PreParer's Firm's mama (or yours ~ PRIcEWATERHOUSECOC Use Only if self-employed), ' 1301 R STREET NW,
address, and ZIP + 4 WASHINGTON DC JS/1
SCHEDULER Organization Exempt Under Section 501(c)(3) (Form 990 or 990-EZ)
(Except Private Foundation) and Section b01(e), 5010, 501(k), 501(n), or Section 4947(a)(1) Nonexempt Charitable Trust
Department of the Treasury Supplementary Information - (See separate instructions .) Internal Revenue Service " MUST be completed by the above organizations and attached to their Form 990 or S
OMB No 1545-0047
LSOoO2 Name of the organization
GREATER INC .
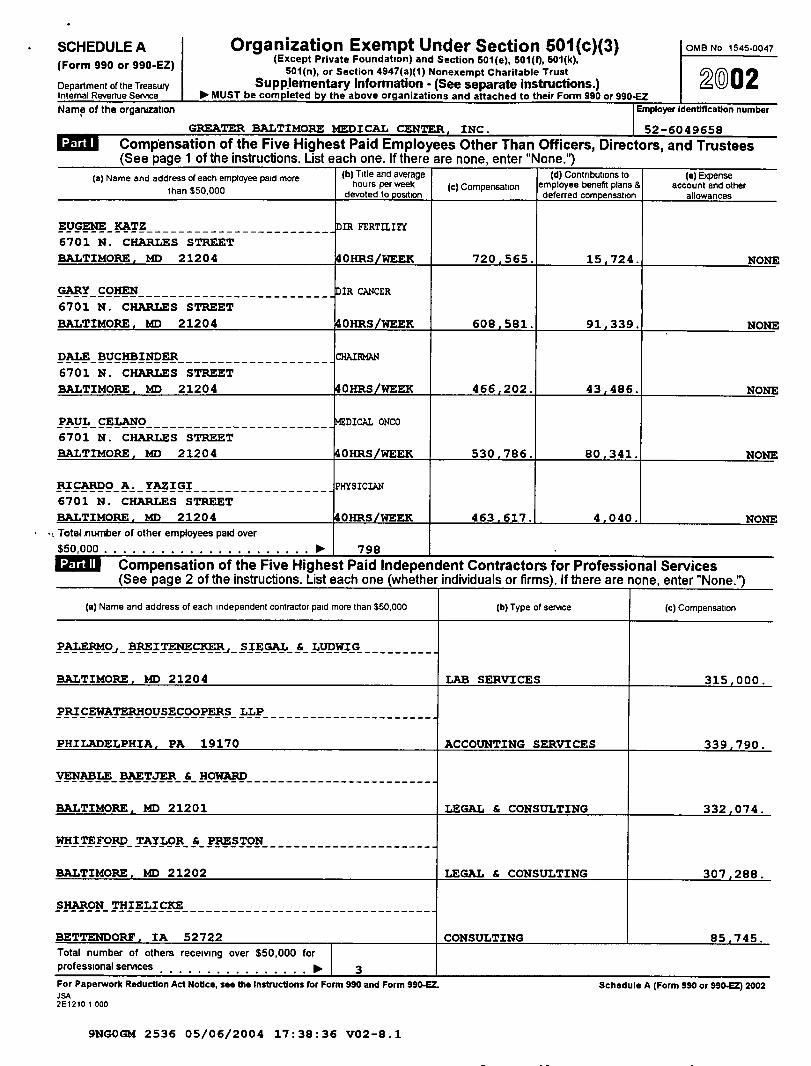
- ; Totel .number of other employees paid over $50,000 .
. " 798
97 Mit Compensation of the Five Highest Paid Independent Contractors for Professional Services (See page 2 of the instructions . List each one (whether individuals or firms) . If there are none, enter "None .
6
Schedule A (Form 990 or 990-Q) 2002
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
Compensation of the Five Highest Paid Employees Other Than Officers, Directors, and Trustees (See page 1 of the instructions . List each one . If there are none, enter "None.")
(a) Name and address of each employee paid more (b) Title and average (d) Contributions to (e) Eipense
than $50,000 hours per week (c) Compensation employee benefit plans 8 account and other
H.-roi r~ --a-
EUGENE KATZ IR FERTII.ITY 6701 N . CHARLES STREET BALTIMORE, MD 21204 ~ OHRS/WEEK 720,565 . 15,724 .
GARY- COFIEN------------------------ fIR CANCER 6701 N . CHARLES STREET
91,339 .
DALE BUCFBINDER 6701 N . CHARLES STREET
PAUL CELANO DICAL ONCO
6701 N. CHARLES STREET
BALTIMORE . I~ 21204 OHRS/WEl
RZCARDO A . YAZIGI 6701 N . CHARLES STREET
(a) Name and address of each independent contractor paid more than $50,000
PALERMO~_ BREZTENECKER~_ SIEGAL 6_ LLTDWZG ---------
204
PRICEWATERHOUSECOOPERS LLP
VENASLE HAETJER & - HOWARD
BALTIMORE, MEI 2120
WHITEFORD TAYLOR & - PRESTON
M1D 21202
SFIARON THIELICRE
Total number of others receiving over $50,000 for professional services For Paperwork Reduction Ad Nonce, see the Instructions for Form 990 and Form 990-Q . .1 SA 2E1210 1 000
(b) Type of service
ACCOUNTING SERVICES
(e) Compensation
5,000 .
332,074 .
288 .
745

e Transfer of any part of its income or assets? , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 2e' X
3 Does the organization make grants for scholarships, fellowships, student loans, etc ? (See Note below ) , , , , , , , , , , , , , 3 X 4 Do you have a section 403(b) annuity plan for your employees . . . . . . . . . . . . . . . . . . . . . . . . . . . . . , . . 4 X Note : Attach a statement to explain how the organization determines that individuals or organizations receiving grants
(a) Name(s) of supported organizations) I (b) Line number from above
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
52-6049658 Schedule A (Form 990 or 990-EZ) 2002 Page Z
Statements About Activities See a e 2 of the instructions . Yes No 1 During the year, has the organization attempted to influence national, state, or local legislation, including any
attempt to influence public opinion on a legislative matter or referendum? If "Yes," enter the total expenses paid .or incurred in connection with the lobbying activities 10- $ 89 , 350 . (Must equal amounts online 38,
Part VI-A, or line i or Part VI-B ) 1 X Organizations that made an election under section 501(h) by (ding Form 5768 must complete Part VI-A. Other organizations checking "Yes," must complete Part VI-B AND attach a statement giving a detailed description of the lobbying activities
2 During the year, has the organization, either directly or indirectly, engaged in any of the following acts with any substantial contributors, trustees, directors, officers, creators, key employees, or members of their families, or with any taxable organization with which any such person is affiliated as an officer, director, trustee, majority owner, or principal beneficiary? (If the answer to any question is 'Yes,' attach a detailed statement explaining the transactions )
a Sale, exchange, or leasing of property? , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 2a X
b Lending of money or other extension of credit? , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , STMT 19
c Furnishing of goods, services, or facilities? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
d Payment of compensation (or payment or reimbursement of expenses d more than $1,000)? , ,FQRkS .9.9 .0 . , pAR.T, y, , , L2dI X
17 M& Reason for Non-Private Foundation Status (See pages 3 through 5roftheanstructions) I "
The or anization is not a private foundation because it is: (Please check only ONE applicable box .) 5 A church, convention of churches, or association of churches Section 1y0(b)(1)(A)(i) 6 A school Section 170(b)(1)(A)(u). (Also complete Part V ) 7 X A hospital or a cooperative hospital service organization Section 170(b)(1)(A)(w) 8 A Federal, state, or local government or governmental unit . Section 170(b)(1)(A)(v) . 9 u A medical research organization operated m conjunction with a hospital Section 170(b)(1)(A)(nQ. Enter the hospital's name, city,
and state
10 El An organization operated for the benefit of a college or university owned or operated by a governmental unit Section 170(b)(1)(A)(iv)
(Also complete the Support Schedule in Part IV-A )
11 a E1 An organization that normally receives a substantial part of its support from a governmental and or from the general public Section 170(b)(1)(A)(vi) (Also complete the Support Schedule m Part IV-A .)
11 b 8 A community trust Section 170(b)(1)(A)(vi) (Also complete the Support Schedule m Part IV-A ) 12 An organization that normally receives. (1) more than 33 1/3% of it support from contributions, membership fees, and gross
receipts from activities related to its charitable, etc ., functions - subject to certain exceptions, and (2) no more than 33 1/3% of its support from gross investment income and unrelated business taxable income (less section 511 tax) from businesses acquired by the organization after June 30, 1975 See section 509(a)(2) (Also complete the Support Schedule in Part IV-A )
13 a An organization that is not controlled by any disqualified persons (other than foundation managers) and supports organizations described in (1) lines 5 through 12 above ; or (2) section 501(c)(4), (5), or (6), ii they meet the test of section 509(a)(2) . (See section 509(a)(3)
14 17 An organization organized and operated to test for public safety Section 509(a)(4) (See page 5 of the instructions ) JSA Schedule A (Form 990 or 980-EZ) 2002 ze,2zo i o00

Schedule A Form 990 or 990-EZ 2002 52-6049659 e 3 Support Schedule (Complete only if you checked a box online 10, 11, or 12 .) Use cash method of acaWtIMOPLI CABLE
Note: You me use the worksheet in the instructions for converting from the accrual to the cash method of accounting Calendar year (or fiscal year beginning in) . a 2001 b 2000 c 1999 d 1998 e Total 15 Gifts, grants, and contributions received (Do
net .nclude unusual grants See line 28 1 " " . . .
16 Membership fees received . . 17 Gross receipts from admissions, merchandise
sold or services performed, or furnishing of
facilities in any activity that is related to the
organization's charitable, etc , purpose .
18 Gross income from interest, dividends,
amounts received from payments on securities
loans (section 512(a)(5)), rents, royalties, and
unrelated business taxable income (less
section 511 taxes) from businesses acquired
by the organization after June 30, 1975
19 Net income from unrelated business activities not included in line 18
20 Tax revenues levied for the organization's benefit and either paid to it or expended on its behalf . . . . . . . . . . . . . . . . . . . .
22 Other income . Attach a schedule Do not include gam or (loss) from sale of capital assets
otal of lines 15
25 Enter 1%of line 23 26 Organizations described on lines 10 or 11 : a Enter 2% of amount in column (e), line 24 VQT AVPIr7,CjkPZ4 , , , jo. 26a
b Prepare a list for your records to show the name of and amount contributed by each person (other than a
governmental unit or publicly supported organization) whose total gifts for 1998 through 2001 exceeded the
amount shown in line 26a Do not file this list with your return . Enter the total of all these excess amounts " 26b c Total support for section 509(a)(1) test' Enter line 24, column (e) . , , . . . . . . . . . . . . , . . . , , . . . . , . , . Po- 26c d Add' Amounts from column (e) for lines 18 19
22 26b � � � � � � " 26d e Public support (line 26c minus line 26d total) , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 1 26e f Public support percentage line 26e numerator divided b line 26c denominator . " 26f °.6
27 Organizations described on line 12 : a For amounts included in lines 15, 16, and 17 that were received from a "disqualified person," prepare a list for your records to show the name of, and total amounts received in each year from, each "disqualified person" Do not file this list with your return. Enter the sum of such amounts for each year :
(2001) ________________ (2000) ___________________ (1999) ___NOT APPLICABLE _ (1998) ______________ b For any amount included in line 17 that was received from each person (other than "disqualified persons', prepare a list for your records to
show the name of, and amount received for each year, that was more than the larger of (1) the amount on line 25 for the year or (2) $5,000 (Include in the list organizations described in lines 5 through 11, as well as individuals ) Do not fife this list with your return . After computing the difference between the amount received and the larger amount described in (1) or (2), enter the sum of these differences (the excess amounts) for each year' (2001) ---------------- (2000) ------------------- (1999) ------------------- (1998)---------------
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
21 The value of services or facilities furnished to the organization by a governmental unit without charge Do not include the value of services or facilities generally furnished to the
c Add Amounts from column (e) for lines 15 16 17 20 21 . . . . . . . . . . . . Po- 27c
d Add. Line 27a total and line 27b total , , . . . . . . . . . . . . " 27d e Public support (line 27c total minus line 27d total) " " " " " " " " " " " " " " " " " " " " " " " " " " " " " " " " 27e t Total support for section 509(a)(2) test: Enter amount from line 23, column (e) . . . . . . . . . . 110-27( g Public support percentage (line 27e (numerator) divided by line 27t (denominator)) . . . . , . . . . . . . . . . . . . " 27
h investment income percentage (line 18, column (e) (numerator) divided by line 271 (denominator)) . . . . . . . . . . 00- 27h 28 Unusual Grants : For an organization described in line 10, 11, or 12 that received any unusual grants during 1998 through 2001,
prepare a list for your records to show, for each year, the name of the contributor, the date and amount of the grant, and a brief description of the nature of the grant Do not file this list with your return . Do not include these grants in line 15 .
Jsu Schedule A (Foam 990 or 990-Q) 2002 2E1221 7 000

If you answered "No" to any of the above, please explain (If you need more space, attach a separate statement ) -----------------------------------------------------------------------------
- ---------------------------------------------------------------------------33 Does the organization discriminate by race in any way with respect to
a Students'rights orpnvdeges? ��������� , . � , . ������� , . � , . � 33a
b Admissions policies 33b
c Employment of faculty or administrative staff? , , , , , , , , , , . . , . . , , , , , , . . . . . , . . . , , . . _ . , 33c
d Scholarships or other financial assistance 33d
e Educational polices? 33e
f Use of facilities? 33f
g Athletic programs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
h Other extracurricular activities? 33h
If you answered "Yes" to any of the above, please explain (If you need more space, attach a separate statement )
---------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
34a Does the organization receive any financial aid or assistance from a governmental agency . . . . . , . . . , , , . 34a
b Has the organization's right to such aid ever been revoked or suspended , , , . , , . , , . , , , . . , , . , . . . 34b If you answered "Yes" to either 34a or b, please explain using an attached statement.
35 Does the organization certify that it has complied with the applicable requirements of sections 4 01 through 4 OS of Rev Proc 75-50 1975-2 C B 587 covering racial nondiscrimination If "No " attach an explanation .
" "
35 JSA
Schedule AForm 990 or 990-EZ 2002 2E1230 7 000
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
52-6049658
Schedule A (Form 990 or 990-EZ) 2002 NOT APPLICABLE Page 4
Private School Questionnaire (See page 7 of the instructions) (To be completed ONLY by schools that checked the box on line 6 in Part IV)
29 Does the organization have a racially nondiscriminatory policy toward students by statement in its charter, bylaws, Yes No other governing instrument, or in a resolution of its governing body , . , , . . . , . . . . . . . . . . . , . 29
30 Does the organization include a statement of its racially nondiscriminatory policy toward students in all its brochures, catalogues, and other written communications with the public dealing with student admissions, programs, and scholarships . . . . . , , . , , , . . . , . . . . . . . . , , _ . . . . , . . . . 30
31 Has the organization publicized its racially nondiscriminatory policy through newspaper or broadcast media during the period of solicitation for students, or during the registration period if it has no solicitation program, m a way that makes the policy known to all parts of the general community it serves , , , , . . _ . . , . . . . . . . , , . 31 If "Yes," please describe, if "No," please explain (If you need more space, attach a separate statement.) ---------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
32 Does the organization maintain the following. - --------------------------------------------------------------------------- a Records indicating the racial composition of the student body, faculty, and administrative staffs . . _ . . . , . . . 32a b Records documenting that scholarships and other financial assistance are awarded on a racially nondiscriminatory
basis? 32b c Copies of all catalogues, brochures, announcements, and other written communications to the public dealing
with student admissions, programs, and scholarships? . . . . . . , . . . . . . . . . . , . . . 32c d Copies of all material used by the organization or on its behalf to solicit contributions? . . . . , . . . . . . . . , . . 32d

Schedule A Form 990 or 990-EZ 2002 52-6049658 Page 5 Lobbying Expenditures by Electing Public Charities (See page 9 of the instructions) (To be completed ONLY by an eligible organization that filed Form 5768) NOT APPLICABLE
Check t a if the organization belongs to an affiliated group Check " ' b if you checked "a" and "limited control" provisions apply
Affiliated group I To be completed totals for ALL electing
organizations
Not over $500,000 , , , , , , , , , , , , 20% of the amount on line 40 ,
Over $500,000 but not over $1,000,000 , , , $100,000 plus 15°h of the excess over $500,000
Over $1,000,000 but not over $1,500,000 , , $175,000 plus 10% of the excess over $1,000,000
Over $1,500,000 but not over $17,000,000 , , $225,000 plus 5°h of the excess over $1,500,000
Over $17,000,000 , , , , , . , , , . , . $1,000,000 . , , , . , . , . . . , , . . ,
42 Grassroots nontaxable amount (enter 25% of line 41) . . . . . , . . . . . . . . . , 43 Subtract line 42 from line 36 Enter -0- if line 42 is more than line 36 44 Subtract line 41 from line 38 Enter -0- if line 41 is more than line 38
Lobbying Expenditures During 4-Year Averaging Period
(b) I (c) I (d) I (e) 2001 2000 1999 Total
Grassroots lobbying
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
Limits on Lobbying Expenditures
(The term "expenditures" means amounts paid or incurred .) 38 Total lobbying expenditures to influence public opinion (grassroots lobbying) . . , 36 37 Total lobbying expenditures to influence a legislative body (direct lobbying) , , . . 37 38 Total lobbying expenditures (add lines 36 and 37). , , , , . . . . . , . . . . . . . 38 39 Other exempt purpose expenditures � � � � � � � � � � � � , 39 40 Total exempt purpose expenditures (add lines 38 and 39) 40 41 Lobbying nontaxable amount . Enter the amount from the following table
If the amount on line 40 Is - The lobbying nontaxable amount is - F
Caution: If there is an amount on ether line 43 or line 44, you must 61e Form 4720 1 4-Year Averaging Period Under Section 501(h)
(Some organizations that made a section 501(h) election do not have to complete all of the five columns below See the instructions for fines 45 through 50 on page 11 of the instructions )
Calendar year (or fiscal (a) ear beginning In " 2002 Lobbying nontaxable amount Lobbying ceding amount (150% of line 45(e)1 . .
Grassroots nontaxable . . . . . . . .
Grassroots ceding amount
11 snoc M I..,. etiio11 . .
MUM Lobbying Activity by Nonelecting Public Charities For reporting only b organizations that did not complete Part VI-A) See page 11 of the instructions .
During the year, did the organization attempt to influence national, state or local legislation, including any Yes NO Amount attempt to influence public opinion on a legislative matter or referendum, through the use of :
a Volunteers X b Paid staff or management (Include compensation in expenses reported on lines c through h X c Media advertisements x d Mailings to members, legislators, or the public, , , , , , , , , , , , , , , , , , , , , , , , , , X e Publications, or published or broadcast statements , , , , , , , , , , , , , , , , , , , , , , , , , , X f Grants to other organizations for lobbying purposes , , , , , , , , , , , , , , , , , , , , , , , , , X g Direct contact with legislators, their staffs, government officials, or a legislative body . STMT ,20, X 89 , 350 . h Rallies, demonstrations, seminars, conventions, speeches, lectures, or any other means , , , , , , X I Total lobbying expenditures (Add lines c through h ), , , , , , , , , , , , , 89 , 350 .
If "Yes" to any of the above, also attach a statement giving a detailed description of the lobbying acbvrhes JSA Schedule A (Form 990 or 990-EZ) 2002 2E1240 7 000

Schedule A Form 990 or 990-EZ 2002 52-6049658 Page 8 Information Regarding Transfers To and Transactions and Relationships With Noncharitable Exempt Organizations (See page 12 of the instructions .)
51 Did the reporting organization directly or indirectly engage in any of the following with any other organization described m section 501(c) of the Code (other than section 501(c)(3) organizations) or m section 527, relating to political organizations?
a ,Transfers from the reporting organization to a nonchantable exempt organization of. 0 (I) Cash . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . (II) Other assets . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
b Other transactions : (I) Sales or exchanges of assets with a nonchantable exempt organization , . . , , . . , , . . . , . . , (II) Purchases of assets from a nonchardable exempt organization (III) Rental of facilities, equipment, or other assets , , , , , . , . . . . . . . . . . . . . . . . . , . . . . . , (Iv) Reimbursement arrangements ���������������� . . . ., . �� (v) Loans or loan guarantees ������� , ., . . . . ., . . ., . . . . . . ., . . . ., . � . . b(v) X
(v1) Performance of services or membership or fundraising solicitations , , , , , , , , , , , , , , , , , , , , , , c Sharing of facilities, equipment, mailing lists, other assets, or paid employees , , , , , , . . . . . . . , d Ii the answer to any of the above is "Yes," complete the following schedule . Column (b) should always show the fair market value of the
goods, other assets, or services given by the reporting organization If the organization received less than fair market value in any
52a Is the organization directly or indirectly affiliated with, or related to, one or more tax-exempt organizations described in section 501(c) of the Code (other than section 501(c)(3)) or in section 527 , , , , , , , , , , " ~ Yes X No
2E7250 1 000 Jcneaule A (rorm yyu or yyu-tL) LUUl
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1

9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
GREATER BALTIMORE MEDICAL CENTER, INC . 52-6049658
FORM 990, PART I - EXCLUDED CONTRIBUTIONS
DESCRIPTION AMOUNT ----------- ------
GOLF & TENNIS CLASSIC 42,466 . FATHER'S DAY 5K 33,045 .
------------ TOTAL 75,511 .
STATEMENT 2

EIN : 52-6049658
FORM 990, PART I, LINE 8(B) - GAIN ON SALE OF OTHER ASSETS
TOTALS : 33,470 33,470 -
STATEMENT 2A
GREATER BALTIMORE MEDICAL CENTER, INC .
FORM 990 , PART I , LINE 8(A) - GAIN ON SALE OF SECURITIES
PROCEEDS FROM SALES OF SECURITIES 40,599 LESS : BASIS (39,961)
NET GAIN ON SALE OF SECURITIES 638
ASSET PROCEEDS BASIS GAIN / (LOSS)
DIVERSIFIED HEALTH SERVICES 3,909 3,909 - DIVERSIFIED HEALTH ENTERPRISES 29,561 29,561 -

FORM 990, PART I - SPECIAL FUNDRAISING EVENTS AND ACTIVITIES
DIRECT EXPENSES
51,774 . 16,230 .
------------68,004 .
42,034 . 14,351 .
------------56,385 .
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1 STATEMENT 3
GREATER BALTIMORE MEDICAL CENTER, INC .
DESCRIPTION
GOLF & TENNIS CLASSIC FATHER'S DAY 5K
TOTALS
GROSS REVENUE
52-6049658
NET INCOME
9,740 . 1,879 .
------------------------11,61-9 .

9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
GREATER BALTIMORE MEDICAL CENTER, INC . 52-6049658
FORM 990, PART I - OTHER INCREASES IN FUND BALANCES
DESCRIPTION AMOUNT ----------- ------
EQUITY INTEREST IN AFFILIATE 418,700 . UNREALIZED GAIN ON INVESTMENT 2,838,542 .
------------ TOTAL 3,257,242 .
STATEMENT 4

9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
GREATER BALTIMORE MEDICAL CENTER, INC . 52-6049658
FORM 990, PART I - OTHER DECREASES IN FUND BALANCES
DESCRIPTION AMOUNT ----------- ------
ADDITIONAL PENSION LIABILITY 18,874,913 . TRANSFER TO AFFILIATES 913,961 . PRIOR PERIOD ADJUSTMENT 110 , 965 .
------------ TOTAL 19,899,839 .
STATEMENT 5

CURRENT YEAR DEPRECIATION EXPENSE :
STATEMENT SA
GREATER BALTIMORE MEDICAL CENTER, INC .
FORM 990 .LINE 42 AND 57
LAND AND LAND IMPROVEMENTS BUILDING & BUILDING SERVICE EQUIPMENT MOVABLE EQUIPMENT CONSTRUCTION IN PROGRESS
LESS : ACCUMULATED DEPRECIATION
NET PROPERTY AND EQUIPMENT
95-3930725
22,416,816 146,886,771 134,648,858 15,217,335
319,169,780 (165,442,894) 153,726,886
17,346,185

16081115 . -210,922 .
15870193 .
23424514 . 7,718,156 .
31142670 .
9NGOCM 2536 05/06/2004 17 :38 :36 V02-8 .1 STATEMENT 6
GREATER BALTIMORE MEDICAL CENTER, INC .
FORM 990, PART II - OTHER EXPENSES
DESCRIPTION
PURCHASED SERVICES UNCOLLECTIBLE ACCOUNTS
TOTALS
TOTAL
52-6049658
PROGRAM SERVICES
MANAGEMENT AND GENERAL
7,343,399 . 7,929,078 .
15272477 .

9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
GREATER BALTIMORE MEDICAL CENTER, INC . 52-6049658
FORM 990, PART III - ORGANIZATION'S PRIMARY EXEMPT PURPOSE
GREATER BALTIMORE MEDICAL CENTER'S PRIMARY EXEMPT PURPOSE IS AS FOLLOWS : (1) TO ORGANIZE, BUILD, ERECT, EQUIP, MANAGE AND OPERATE EXCLUSIVELY FOR CHARITABLE PURPOSES A NON-PROFIT GENERAL HOSPITAL AND MEDICAL CENTER FOR THE CARE OF THE SICK, AND TO FURNISH MEDICAL AND SURGICAL ATTENDANCE THEREIN IN ANY FORM IN THE CARE OF SICK, AFFLICTED, INFIRM OR INJURED PERSONS ; PROVIDED, HOWEVER, THE OPERATIONS ARE NOT TO BE EXCLUSIVELY FOR THOSE WHO ARE ABLE AND EXPECTED TO PAY BUT TO THE EXTENT OF FINANCIAL ABILITY ARE TO BE FOR THOSE NOT ABLE TO PAY FOR THE SERVICES RENDERED, AND THE FACILITIES ARE NOT TO BE RESTRICTED TO A PARTICULAR GROUP OF PHYSICIANS AND SURGEONS EXCEPT TO THE EXTENT THAT DISCRETIONARY AUTHORITY IN THE MANAGEMENT MAY IMPOSE LIMITATIONS BASED UPON THE QUALIFICATIONS OF THOSE APPLYING OR UPON THE SIZE AND NATURE OF THE FACILITIES, AND NO PART OF ITS NET EARNINGS ARE TO INURE DIRECTLY OR INDIRECTLY TO THE BENEFIT OF ANY PRIVATE SHAREHOLDER OR INDIVIDUAL . (2) TO ORGANIZE, BUILD, ERECT, EQUIP, MANAGE AND OPERATE A SCHOOL OR SCHOOLS FOR TRAINING PHYSICIANS, SURGEONS, NURSES AND OTHERS, AND TO EDUCATE AND TRAIN ANY SUCH PERSONS IN THE CARE OF SICK, AFFLICTED, INFIRM, OR INJURED PERSONS BY TEACHING MEDICINE, HYGIENE, SURGERY AND EVERYTHING HAVING TO DO WITH THE PHYSICAL WELL-BEING OF INDIVIDUALS . (3) TO ENGAGE IN ANY ACTIVITY AND TO DO ANYTHING AND EVERYTHING THAT MAY BE NECESSARY, EXPEDIENT OR INCIDENTAL TO THE PURPOSES STATED IN PARAGRAPHS (1) AND (2) . (4) TO HAVE AND TO EXERCISE TO THE EXTENT NECESSARY OR DESIRABLE FOR THE ACCOMPLISHMENT OF ANY OF THE AFORESAID PURPOSES, AND TO THE EXTENT THAT THEY ARE NOT INCONSISTENT WITH THE CHARITABLE PURPOSES OF THE CORPORATION, AND THE LIMITATIONS IMPOSED BY SECTION 501(C)(3) OF THE INTERNAL REVENUE CODE, ANY AND ALL POWERS CONFERRED UPON CORPORATIONS BY THE MARYLAND GENERAL CORPORATION LAW .
STATEMENT 7

GRANTS AND ALLOCATIONS
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1 STATEMENT 8
GREATER BALTIMORE MEDICAL CENTER, INC .
FORM 990, PART III - OTHER PROGRAM SERVICES
DESCRIPTION
DELIVERY ROOM AND LABOR ROOM ANESTHESIOLOGY RADIOLOGY - DIAGNOSTIC RADIOLOGY - THERAPEUTIC RADIOSOTOPE RESPIRATORY THERAPY PHYSICAL THERAPY ELECTROCARDIOLOGY ELECTROENCEPHALOGRAPHY RESIDENCY PROGRAM MEDICAL SUPPLIES DRUGS PARENTAL EDUCATION MISCELLANEOUS
TOTALS
52-6049658
EXPENSES
4,635,158 . 386,816 .
4,643,346 . 3,727,474 . 2,108,998 . 1,816,705 . 1,864,542 . 3,675,546 .
307,071 . 5,308,098 .
903,210 . 12,879,300 .
471,278 . 417,425 .
--------------43,144,967 .

9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
GREATER BALTIMORE MEDICAL CENTER, INC . 52-6049658
FORM 990, PART IV - INVESTMENTS - SECURITIES
ENDING DESCRIPTION BOOK VALUE ----------- ----------
BOND PROCEEDS HELD BY MHHEFA TREASURY RESERVES 35,386,252 .
DEBT RESERVE- US OBLIGATIONS 9,156,597 . COMMON STOCK 13 , 739 , 591 . BONDS 404,361 . OTHER SECURITIES 335,407 . OTHER EQUITY INVESTMENTS 169,461 .
--------------- TOTALS 59,191,669 .
STATEMENT 9

9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
GREATER BALTIMORE MEDICAL CENTER, INC . 52-6049658
FORM 990, PART IV - OTHER ASSETS
ENDING DESCRIPTION BOOK VALUE ----------- ----------
OTHER ASSETS 161,926 . INVESTMENT IN SUBSIDARY 8,138,439 . A/R - AFFILIATE 7,891,395 . DEFERRED COSTS 1,648,210 . INTANGIBLE ASSETS 749,910 .
--------------- TOTALS 18,589,880 .
STATEMENT 10

52-6049658
2003
MHHCFA project and refunding revenue bonds Serves 2001 Bonds 5% term bonds $ 52,830,000
Series 1995 Bonds Variable rate serial bonds 8,945,000
Series 1993 Bonds 3 .80% - 5 .38% sepal bonds 17,345,000 5 .00% term bonds 48,980,000
Capital leases 1,078,801 Charitable gift annuity 630,703 Unamortized bond discount (3,869,307) Unamortized charitable gift annuity discount (185,777)
125,754,420 Less current portion of lams-trrm debt (3,507,5 54)
S 122,24G .8GG
19,765,000 48,980,000 1,683,456
53,960 (4,076,274)
(14,778) 128,396,364 (3,88,73?)
S 124,807,G32
2536 02/05/2004 09 :04 :39 V02-8 .1
GREATER BALTIMORE MEDICAL CENTER, INC .
FORM 990, PART IV - TAX-EXEMPT BOND LIABILITIES
Long-Term Debt
Lung-term debt at June 30, consisted of the following-
2002
5 52,830,000
9,175,000
On \o% ember 1 . 2001 . the Medical Center issued S52.830,000 principal amount of Re, enue Bonds, Series 2001 ;1 puition of the proceeds was used to refund in advance of their maturities the G°./o Series 1991 bonds that mature on July 1 . 2021 The bonds are collateralized by a first lien on all (Tross receipts of the Medical Center The Serves 2001 Bonds 5% term bonds are due July 1, 2020, 202 and 203=1 in the amount of X6,155,000, S 14,590,000 and S3?,OS5,000, respectively
The Serves 199 Bonds are due in annual installments ranging from S235,000 in 2003 to X590,000 in 202 The bonds bear interest at a variable rate which is determined on a weekly basis by Legg Mason, the underwriter of the issue . The rate at June 30 . 2003 and 2002 vas 1 25% and 2 80%, respectively The bonds are collateralired by a first lien on all gross receipts of the Medical Center
Yile Series 1993 Sepal Bonds are due in annual installments ranging from 52,540,000 in 2003 to S3,275,000 in 2008 . The 5 00% term bonds are due . $19,045,000 on July l, 2013, and S29,935,000 on July 1, 2019 The bonds are collateralized by a first lien on all gross receipts of the Medical Center
The Series 1991 Serial Bonds' last installment was $725,000 due on July 1, 2001 . The 6% term bonds due to mature on July 1, 2021 were refunded with proceeds of the Series 2001 bond issuance
Unexpended bond proceeds and approximately one year's debt service of the Series 2001 and 1993 Serial Bonds have been deposited with a trustee and are classified as limited use funds . Interest income, net of the amount capitalized, earned on these funds of approximately $1,838,000 and 5446,000 was included in other operating revenue for 2003 and 2002, respectively .
STATEMENT 11

STATEMENT 11
2536 02/04/2004 18 :13 :07 V02-8 .1
GREATER BALTIMORE MEDICAL CENTER, INC .
FORM 990, PART IV - TAX-EXEMPT BOND LIABILITIES
The aggregate future matunties oflong-term debt at June 30, 2002 was .
Capital Charitable Long-Term Lease Gift
Debt Obligations Annuity
2004 S 2,775,000 $ 694,541 $ 38,013 2005 2,915,000 332,086 38,013 2006 3,065,000 43,639 38,013 2007 3,215,000 5,070 38,013 2008 3,390,000 3,465 38,013 Thereafter 112,740,000 - 440,638
128,100,000 1,078,801 630,703 Less unamortized bond discount (3,869,307) - (185,777)
124,230,693 S 1,078,801 $ 444,926
The fair value of the Medical Center's long-term debt, which is estimated based on quotes from underwriters, vas approximately S 127,6 16,000 and S 123.228.000 at June 30, 2003 and 2002, respectively .
During the year ended June 30, 2003, the Medical Center obtained a S 10 .000,000 line of credit which expires on March 31, 2004, bearing interest at the LI130R Daily Floating Rate No amounts %%crc drawn on this line during fiscal year 2003
52-6049658

9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
GREATER BALTIMORE MEDICAL CENTER, INC . 52-6049658
FORM 990, PART IV - OTHER LIABILITIES
ENDING DESCRIPTION BOOK VALUE ----------- ----------
CURRENT PORTION OF LT DEBT 3,157,554 . THIRD PARTY ADVANCES 10,737,889 . INSURANCE RESERVES 6,969,242 . MINORITY INTEREST 177,089 . PENSIONS LIABILITY 19,521,992 . OTHER 752,800 .
--------------- TOTALS 41,316,566 .
STATEMENT 12

52-6049658
FORM 990, PART IV-A - OTHER REVENUE ON BOOKS BUT NOT ON RETURN
INCOME OF SUBSIDIARY-5EPERATELY REPORTED
STATEMENT 13
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
GREATER BALTIMORE MEDICAL CENTER, INC .
DESCRIPTION
TOTAL
AMOUNT
4,301,680 . ---------------
4,301,680 .

52-6049658
FORM 990, PART IV-B - OTHER EXPENSES ON BOOKS BUT NOT ON RETURN
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
GREATER BALTIMORE MEDICAL CENTER, INC .
DESCRIPTION AMOUNT ----------- ------
EXPENSE OF SUBSIDIARY- SEPERATELY REPORTED 4,194,818 .
--------------- TOTAL 4,194,818 .
STATEMENT 14

GREATER BALTIMORE MEDICAL CENTER, INC . 52-6049658
FORM 990, PART V - LIST OF OFFICERS, DIRECTORS, AND TRUSTEES
CONTRIBUTIONS EXPENSE ACCT TO EMPLOYEE AND OTHER
BENEFIT PLANS ALLOWANCES ------------- ----------
202,877 . 36,000 .
TITLE AND TIME DEVOTED TO POSITION COMPENSATION ------------------- ------------
PRESIDENT 547,317 . 40 HRS/WK
NAME AND ADDRESS ----------------
LA(TRENCE MERLIS 6701 N . CHARLES STREET BALTIMORE, MD 21204
CHARLES A. HAILE, MD 6701 N . CHARLES STREET BALTIMORE, MD 21204
JOHN R. SAUNDERS, MD 6701 N . CHARLES STREET BALTIMORE, MD 21204
ERIC MELCHIOR 6701 N. CHARLES STREET BALTIMORE, MD 21204
RODNEY WILLIAMS 6701 N . CHARLES STREET BALTIMORE, MD 21204
MICHAEL HEBRANK 6701 N . CHARLES STREET BALTIMORE, MD 21204
GRAND TOTALS
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1 STATEMENT 15
CHIEF OF STAFF 40 HRS/WK
VICE CHIEF OF STAFF 40 HRS/WK
EXECUTIVE VP/CFO 40 HRS/WK
EXEC .VP/CHF .MED .OFFC 40 HRS/WK
VP / CIO 40 HRS/WK
127,510 . 27,182 . NONE
106,648 . 21,642 . NONE
313,320 . 123,335 . 8,400 .
324,306 . 134,794 . 8,900 .
193,539 . 66,874 . NONE
-------------- -------------- --------------1,612,640 . 576,704 . 52,800 .

I
STATEMENT 15
GREATER BALTIMORE MEDICAL CENTER, INC .
F%,"M 990, PART V - LIST OF OFFICERS, DIRECTORS, AND TRUSTEES
NAME BUSINESS ADDRESS
Mr. Kenneth P. Barksdale 20501 Bordly Court Brookeville, MD 20833
Mr. Mark S. Bartlett Ernst 8 Young, LLP One N . Charles Street Baltimore, MD 21201
Mr. Herbert J. Belgrad Partner (VICE CHAIRMAN) Tydings 8 Rosenberg, LLP
100 E. Pratt St. 26' Fir. Baltimore, MD 21202
Albert L. Biumberg, M.D. Physician Dept. of Radiation Oncology 6701 N. Charles Street Baltimore, MD 21204
Mr. Raymond J . Brusca Vice President-Benefits The Black 8 Decker Corp. 701 E. Joppa Road, TVN170 Towson, MD 21286
Mr. William H. Conkling, Jr . Senior Vice President (VICE CHAIRMAN) Trammel) Crow Co.
1055 Thomas Jefferson St., NW #650 Washington, D.C. 20007
52-604965 "

Mr. Michael H. Davis Attorney Venable, Baetjer 8 Howard 210 Allegheny Avenue Towson, MD 21204
Mr. J. William Knott- Regional Vice President (TREASURER) First Union National Bank
7 SL Paul Street Baltimore, MD 21202
Mr. Charles C. Fenwick, Jr. President 8 General Manager Valley Motors, Inc. 9800 York Road Cockeysville, MD 21030
Ms. Dorothy Hamill P. O. Box 16286 Baltimore, MD 21210
Mr. Harry S. Johnson Whiteford, Taylor S Preston L.L.P . 7 St Paul Street Baltimore, MD 21202-1626

Ms. Patricia J. Mitchell Vice . Pres.-Global Sales 8 Operations IBM Global Services 100 E. Putt Street, 3`° Floor Baltimore, MD 21202
Mr. William A. Kroh Retired Executive 2401 Still Forest Road Baltimore, MD 21208
Mrs. Barbara Lucas Senior Vice President-Public Affairs (CHAIRMAN) The Black & Decker Corp.
701 E. Joppa Road, TYV245 Towson, MD 21286
Mr. Thomas H. Maddux Schenuit Investments, Inc. 102 W. Pennsylvania Ave. Suite 300 Towson. MD 21204
Ms. Sayra Wells Meyerhoff Community Leader Nine Meadow Road Baltimore, MD 21212

Unless otherwise noted, directors receive no compensation or benefits . Hours are less than
one per week
Mr. Ackneil M. Muldrow, II President 8 CEO Development Credit Fund, Inc. 2530 N. Charles St., Suite 200 Baltimore, MD 21218
Mrs. Margaret V. Preston Sr. VP for Private Wealth Mgmt. Mercantile Safe Deposit & Trust Co Sun Life Bldg., 5' Fir. 20 S. Charles Street Baltimore, MD 21201
Mr. Stephen T. Scott Investment Counselors of MD 803 Cathedral Street Baltimore, MD 21201
Mrs. Karen D. Weatherholtz Sr. Vice President-Human Relations (SECRETARY) McCormick & Co., Inc.
18 Loveton Circle Sparks, MD 21152

UtCt.~"~1ZK CSNL11MVttZ Mt.LlUL1L l:t.N'1't;K, 1N(...
FORM 990, PART VI - NAMES OF RELATED ORGANIZATIONS
DOES GBMC FOR-PROFIT ENTITY OWNERSHIP % PREPARE fIS9 CONSOLi0ATE7 OR NON-PROFIT TYPE ROTES
10091 YES YES FOR PROFIT CORPORATION SHELL COMPANY FOR GBMC AGENCY 50% NO YES FOR PROFIT PARTNERSHIP ADVANCED RADIOLOGY PREPARES THE FINANCULS (50/50 OWNERSHIP) 100% YES YES FOR PROFIT CORPORATION FORMERLY GBMD. ORGANIZED TO FACILITATE PROCESSING OF MANAGED CARE CONTRACTS SOX NO YES FOR PROFIT PARTNERSHIP NEIGHBORCARE PREPARES F/S (60160 OWNERSHIP) 100% YES YES FOR PROFIT CORPORATION MEDICAL OFFICE BUILDING IN OWINGS MILLS 88% YES YES FOR PROFIT PARTNERSHIP PARTNERSHIP, AGENCY OWNS 52% . HOSPITAL OWNS 38%
100% YES YES FOR PROFIT CORPORATION EAST PAVILION MEDICAL OFFICE BUILDING MGMT CO 100% YES YES FOR PROFIT CORPORATION EAST PAVILION MEDICAL OFFICE BUILDING LP
100% YES YES
100% YES YES 50°K KO YES 100% YES YES 100% YES YES 100% YES YES 100% YES YES 100'K YES YES 100% YES YES 100% NO NO 100% NO NO 100% NO NO 10016 YES YES
NONE
ONSOL E1LL COMPANY NAME
1 EMC AGENCY & SUBSIDIARIES
ADMIN GREATER 6ALT)MORE DIAGNOSTIC IMAGING GREATER BALTIMORE MEDICAL ASSOCIATES NEiGHBORCARE PHARMACY OYVINGS MILLS PAVILION GBMC PAVILION WEST MEDICAL ARTS, LP
2 GBMC AGENCY " SUBStDWt1ES GBMC MANAGEMENT. INC
(G9MC MK" Am Ltd ParoarsluP)
3 aBYC AGENCY l SUBSIDIARIES GBMC MANAGEMENT (EAST PAVILION LP) GSMC INVESTMENTS
t OBMC AGENCY i SUBSIDIARIES GBMC MANAGEMENT (EAST PAVILION LP) GBMC INVESTMENTS, INC i SUBSIDUIRIEB GBMC HOSPITAL
PARTNERS IN RECOVERY DIVERSIFIED HEALTH ENTERPRISES DIVERSIFIED HEALTH SERVICES DIVERSIFIED NURSES GBMC FOUNDATION HOSPICE OF BALTIMORE GBMC HEALTMCARE INC GBMC FINANCE GBMC FINANCE II GBMIC FINANCE //I G8MC LAND. INC
:J4 G-OVti _IV VJO
NON-PROFIT CORPORATION RESTRICTED 6 UNRESTRICTED INVESTMENTS
1 ;
NON-PROFIT CORPORATION NON-PROFIT CORPORATION NON-PROFIT CORPORATION HOME HEALTH SVCS PARENT COMPANY NON-PROFIT CORPORATION HOME HEALTH $VCS NON-PROFIT CORPORATION HOME HEALTH SYCS NON-PROFIT CORPORATION NON-PROFIT CORPORATION NON-PROFIT CORPORATION PARENT CO , FORMERLY KNOWN AS MD HEALTHCORP FOR PROFIT CORPORATION SHELL COMPANY TO HOUSE PAVILION DEBT SERVICE (EAST PAVILION) FOR PROFIT CORPORATION SHELL COMPANY TO HOUSE PAVILION DE9T SERVICE (OWWGS HILLS PAVILION) FOR PROFIT CORPORATION SHELL COMPANY 70 HOUSE PAVILION DEBT SERVICE (WEST PAVILION) FOR PROFIT CORPORATION SMELL COMPANY ONLY, NO ACTIVITY SINCE FY 1987
STATEMENT 16

GREATER BALTIMORE MEDICAL CENTER, INC .
FORM 990, PART VII - OTHER REVENUE
52-6049658
BUSINESS EXCLUSION RELATED OR EXEMPT CODE AMOUNT CODE AMOUNT FUNCTION INCOME ---- ------ ---- ------ ---------------
O1 -46,580 . 01 -53,432 . 03 1,543,172 . 03 546, 498 .
561000 43,905 . 03 220 .
------------ ------------ ------------ 43,905 . 1,989,878 . TOTALS
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1 STATEMENT 17
DESCRIPTION
EQUITY IN EARNINGS MINORITY INTEREST CAFETERIA PARKING BILLING FEES

52-6049658
EXPLANATION OF HOW EACH ACTIVITY FOR WHICH INCOME LINE IS REPORTED IN COLUMN (E) OF PART VII CONTRIBUTED NO . IMPORTANTLY TO THE ACCOMPLISHMENT OF EXEMPT PURPOSES --- ----------------------------------------------------
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
GREATER BALTIMORE MEDICAL CENTER, INC .
FORM 990, PART VIII - ACCOMPLISHMENT OF EXEMPT PURPOSES
93A DAILY HOSPITAL SERVICES REV RUL 69-545 TO LABORATORY TAM 8246018 93B OPERATING ROOM REV RUL 69-545
RADIOLOGY PLR 8305115 CLINIC & ER REV RUL 83-157 MEDICAL SUPPLIES REV RUL 68-376 DELIVERY & LABOR RMS REV RUL 69-545 DRUGS REV RUL 69-545 RESPIRATORY THERAPY PLR 7843128 ANESTHESIOLOGY REV RUL 69-545 ELECTROENCEPfiALOGRAPHY PLR 7843128 PHYSICAL THERAPY TAM 8013052 ELECTROCARDIOLOGY PLR 8736046 OTHER HOSPITAL RELATED INC. REV RUL 69-545
101 NET REVENUE FROM SPECIAL EVENTS HELD TO RAISE MONEY FOR THE HOSPITAL AND SUPPORT ITS CHARITABLE CAUSE .
STATEMENT 18

9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
GREATER BALTIMORE MEDICAL CENTER, INC . 52-6049658
SCHEDULE A, PART III - EXPLANATION FOR LINE 2C
GBMC PURCHASES SERVICES FROM FIRMS WITH WHICH CERTAIN MEMBERS OF ITS BOARD OF DIRECTORS ARE AFFILIATED . ALL TRANSACTIONS ARE CONDUCTED AT ARMS-LENGTH AND AT FAIR MARKET VALUE .
STATEMENT 19

52-6049658
SCHEDULE A, PART VI-B - DIRECT CONTACT WITH LEGISLATORS ------ -------
9NGOGM 2536 05/06/2004 17 :38 :36 V02-8 .1
r GREATER BALTIMORE MEDICAL CENTER, INC .
THE LOBBYING EXPENSES ARE RELATED TO DIRECT CONTACT WITH THE LEGISLATIVE BODIES REGARDING LEGISLATION THAT IMPACTED HEALTH SYSTEM & HOSPITAL ISSUES .
STATEMENT 20

" It you arZ filing for an Automatic 3-Month Extension, complete only Part 1 and check this box . . . . . . . . . . . . . " If you are filing for an Additional (not automatic) 3-Month Extension, complete only Part II (on page 2 of this form). Note : Do riot complete Part 11 unless you have already been granted an automatic 3-month extension on a previously filed Form 8868 . Part I Automatic 3-Month Extension of Time - Only submit original (no copies needed) Note: Form 990-T corporations requesting an automatic 6-month extension - check this box and complete Part I only . . . " [] All other corporations (including Form 990-C filers) must use Form 7004 to request an extension of time to file income tax returns Partnerships, REMICs and trusts must use Form 8736 to request an extension of time to file Form 1065, 1066, or 1041 . Type or Name of Exempt Organization Employer identification number print GREATER BALTIMORE MEDICAL CENTER, INC . 152-6049658
Number, street, and room a suite no It a P 0 box, see instructions File by the
SW FEneoser t
F,;r�, $$6$ Application for Extension of Time To File an (December 2000) Exempt Organization Return OMB No 15d5-1709 Dsprtrnanl d the 7roasuy rx .R,.i rtwexr s«wca f File a separate application for each velum
tor auedate filing your 6701 NORTH CHARLES STREET velum See City, faun or post office, state, and ZIP code For a foreign address, see instructions instructions
BALTIMORE, MD 21204 Check type of return to be filed (file a separate application for each return) : OX Form 990 0 Form 990-T (corporation) ~ Form 4720
Form 990-BL F] Form 990-T (sec . 401(a) or 408(a) trust) E] Form 5227 [] Form 990-EZ 0 Form 990-T (trust other than above) 0 Form 6069
Form 990-PF ~ Form 1041-A 0 Form 8870 " If the organization does not have an office or place of business m the United States, check this box ~ 0 " If this is for a Group Return, enter the organization's four digit Group Exemption Number (GEN) If this is for the whole group, check this box jo. 0 If it is for part of the group, check this box " hand attach a list with the names and EINs of all members the extension will cover
1 I request an automatic 3-month (6-month, for 990-T corporation) extension of time until FEBRUARY 17 , 20 .L4_, to file the exempt organization return for the organization named above The extension is for the organization's return for o. ~ calendar year 20 - or
t ~X tax year beginning JULY Ol , 20 Q -2, and ending JUNE 30 , 20 03
2 If this tax year is for less than 12 months, check reason' 0 initial return [] Final return 0 Change in accounting period
3a If this application is for Form 990-BL, 990-PF, 990-T, 4720, or 6069, enter the tentative tax, less any nonrefundable credits See instructions . . . . . . . . . . . $ NONE
b If this application is for Form 990-PF or 990-T, enter any refundable credits and estimated tax payments made include any prior year overpayment allowed as a credit $ NONE
c Balance Due. Subtract line 3b from line 3a Include your payment with this form, or, if required, deposit with FTD coupon or, if required, by using EFTPS (Electronic Federal Tax Payment System) See instructions . . . $ NONE
Signature and Verification Under penalties of penury, I declare that l have examined this form, including accompanying schedules and statements, and to the best of my knowledge and belief, it is true, correct, and complete, and that I am authorized to prepare this form
r signature t ~ ~-A TiOe lp. TAX PRE PARER Date lo- 11/10/03
For Paperwork Reduction Act N", see Instruction Form 8868 ('12-2000)

Form 8868(12-2000) Page 2 e If you are filing for an Additional (not automatic) 3-Month Extension, complete only Part II and check this box . . . . . . . 10. 0 Note: Only complete Part h ~ you have already been granted an automatic 3-month extension on a previously filed Form 8868. 0 If you are fil ;lng for an Autqlinatic 3-Month Extension, complete only Part 1 (on page 1) .
r, Part II, Additional (not automatic) 3-Month Extension of Time - Must File Original and One Copy. Type or Name off Exempt Organization print GRF&TER BALTIMORE MEDICAL CENTER,' I'NC . File by the Number, street, and room or suite no. If a P O box, see instructions . extended due date for 6701 NORTH CHARLES STREET
o° sing the City, fawn or post office, state, and ZIP code For a foreign address, see instructions
Employer identification number 52-6049658 For IRS use only
" If the organization does not have an office or place of business in the United States, check this box . . . . . . . . . . . . . . . . . . 11. " If this is for a Group Return, enter the organization's four digit Group Exemption Number (GEN) If this is for the whole group, check this box " E] If it is for part of the group, check this box lo. [] and attach a list with the names and EINs of all members the extension is for. ,i
v v v L_ ] 'I , y I j Signature and Verification Under penalties of penury, I declare that I have examined this form, including accompanying schedules and statements, and to the best of my knowledge and belief, it is true, correct and complete, and that I am authorized to prepare this form
Datepi. 2/12/2004 reed TAX PREPARER Signature
STF FED9056F 2
>~ return See
BALTIMORE, MD 21204 io :~ Check type of return to be filed (File a separate application for each return) :
Form 990 0 Form 990-EZ ~ Form 990-T (sec . 401(a) or 408(a) trot) 0 Form 1041-A E] Form 5227 [:] Form 8870 0 Form 990-BL Ej Form 990-PF ~ Form 990-T (trust other than above) E] Form 4720 Ej Form 6069
STOP: Do not complete Part II if you were not already granted an automatic 3-month extension on a previously filed Form 8868.
4 I request an additional 3-month extension of time until - - MAY- ,~j~ / _-~> , 20 .24- 5 For calendar year-, or other tax year beginning JULY 1 ` , 2002 and ending JUNE 30 .20 03 6 If this tax year is for less than 12 months, check reason' 0 Initial return 0 Final return [:] Change in accounting period 7 State in detail why you need the extension AWAITING INFORMATION FROM THIRD PARTIES WHICH
IS NECESSARY TO PREPARE A COMPLETE AND ACCURATE RETURN . ADDITIONAL TIME TO FILE IS REQUESTED .
8a If this application is for Form 990-BL, 990-PF, 990-T, 4720, or 6069, enter the tentative tax, less any r,opri-f1inrjahIPrrp.d*ts See instructions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $ N/A
i rm 9 0-PF, 990-T, 4720, or 6069, enter any refundable credits and estimated b I this = t
ix
prior year overpayment allowed as a credit and any amount paid I:
I
iously with Form 8868 (n . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $ N/A n e
JS 4ne
f; u
or o f ui c I@ ncP%e.jSt8)t?"4ne 'rorn line 8a . Include your payment with this form, or, if required, deposit
,it FT3Dcoupon or, if requi @ by using EFTPS (Electronic Federal Tax Payment System). See I StfU~~Sr~r� . ., ., . .- . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $ N/A
Notice to Applicant - To Be Completed by the IRS [~ We have approved this application Please attach this form to the organization's return 0 1 We have not approved this application However, we have granted a 10-day grace period from the later of the date thavn below or the due date of the
organization's return (including any prior extensions) . This grace period is considered to he a valid extension of time for elections otherwise required to be made on a Limey return Please attach this form to the organization's return. We have not approved this application After considering the reasons stated in item 7, we cannel grant your request for an extension of time to file We are not granting a 10-day grace period. We cannot consider this application because d was filed after the due date of the return for which an extension was requested . Other t _ f 7;;a":
+N
Director
Alternate Mailing Address - Enter the address if you want the copy of this application returned to an address different than the one entered above.
Name PRICEWATERHOUSECOOPERS LLP, ATTN : DAVID T
Type or Number and street (include suite, room, or apt no.) a a P.O. box number print 1301 K STREET NW, SUITE 800W
City or town, province or state, and country (including postal or ZIP code) WASHINGTON, DC 20005-3333
form 8868 (12-2000)


















