Mr. Ryan Sports Medicine. DORSIFLEX Tibialis anterior, Extensor hallucis longus, Extensor Digitorum...
25
Mr. Ryan Sports Medicine
-
Upload
lucas-thornton -
Category
Documents
-
view
238 -
download
4
Transcript of Mr. Ryan Sports Medicine. DORSIFLEX Tibialis anterior, Extensor hallucis longus, Extensor Digitorum...

Mr. Ryan Sports Medicine

DORSIFLEX Tibialis anterior, Extensor hallucis longus,
Extensor Digitorum Longus
PLANTARFLEX (7)- Gastrocnemius, Soleus, Flexor Digitorum Longus, Flexor Hallucis Longus, Tibialis Posterior, Peroneus Longus, Peroneus Brevis
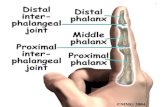
FLEXION & EXTENSION OF THE PHALANGES
INVERSION - tibialis posterior, flexor digitorum, flexor hallucis longus, and the tibialis anterior
EVERSION - Extensor digitorum longus, Peroneus longus, Peroneus brevis
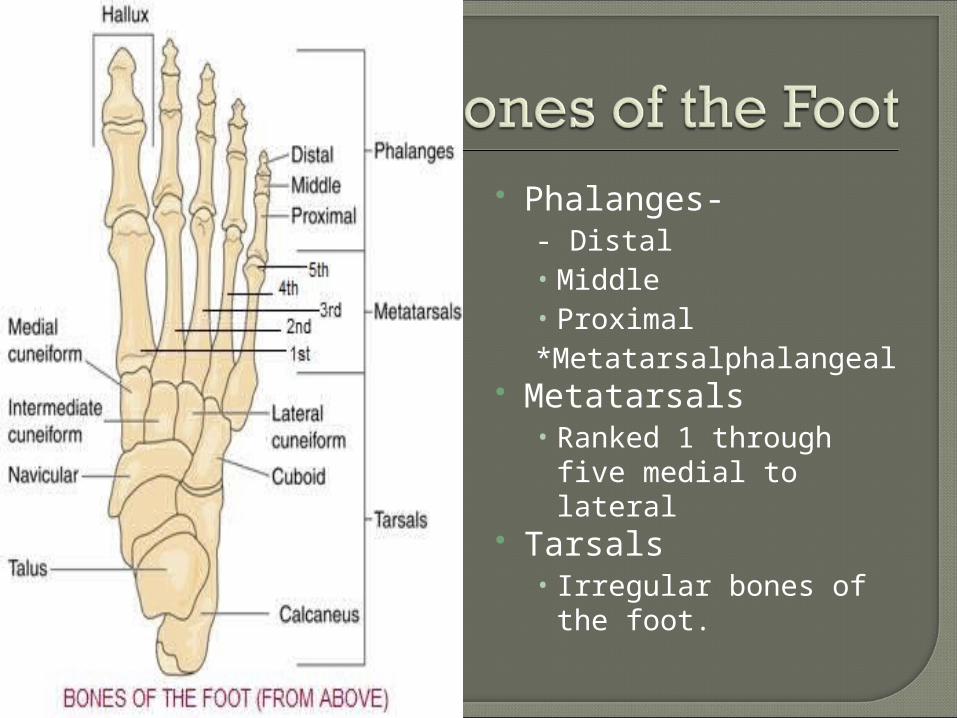
Phalanges-- Distal • Middle• Proximal*Metatarsalphalangeal
Metatarsals• Ranked 1 through
five medial to lateral Tarsals
• Irregular bones of the foot.

Balance and forward body propulsion.
Major Movement bones of the foot –• Flexion, extenstion,
abduction, and adduction.
Hallux – • Big Toe• Has two phalanges,
and all other toes have three phalanges.
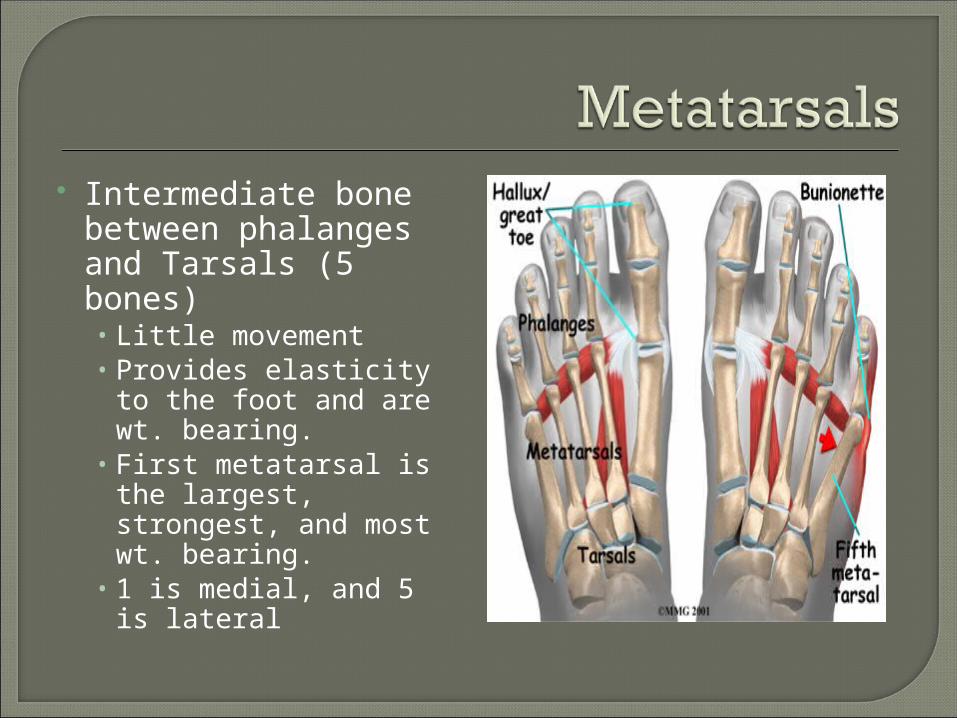
Intermediate bone between phalanges and Tarsals (5 bones)• Little movement• Provides elasticity to
the foot and are wt. bearing.
• First metatarsal is the largest, strongest, and most wt. bearing.
• 1 is medial, and 5 is lateral
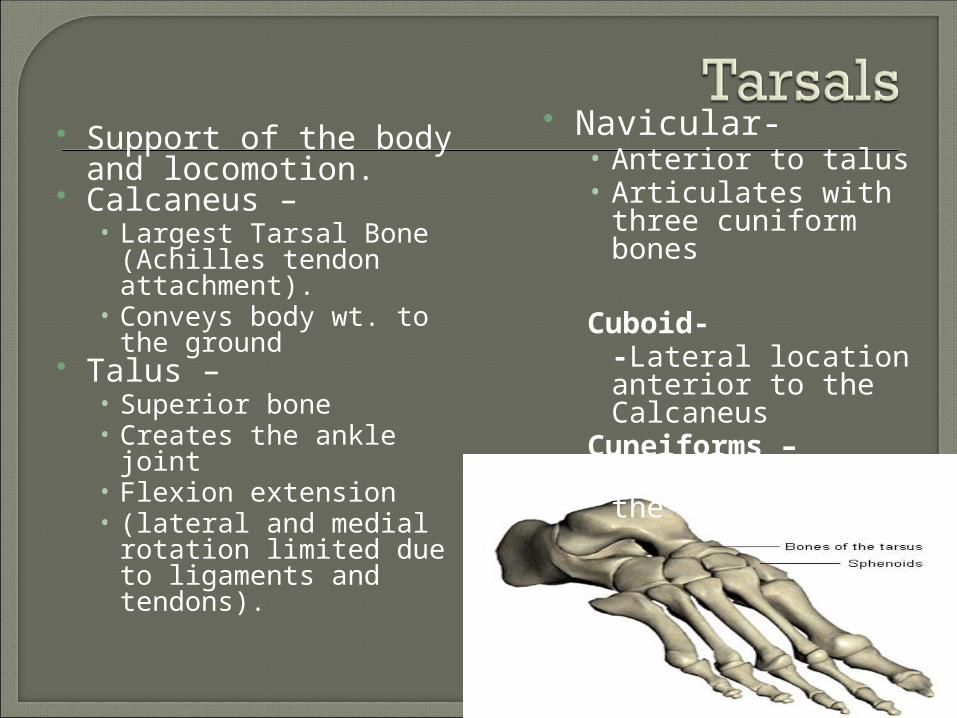
Support of the body and locomotion.
Calcaneus – • Largest Tarsal Bone
(Achilles tendon attachment).
• Conveys body wt. to the ground
Talus – • Superior bone• Creates the ankle joint• Flexion extension• (lateral and medial
rotation limited due to ligaments and tendons).
Navicular-• Anterior to talus• Articulates with three
cuniform bones
Cuboid--Lateral location anterior to the Calcaneus
Cuneiforms –- at the base of the metatarsals

found in locations where a tendon passes over a joint, such as the hand, knee, and foot. Functionally, they act to protect the tendon and to increase its mechanical effect.

Anterior Metatarsal Arch and Transverse Arch –• Lateral to medial
arch along the tarsal and Metatarsal bones.


Medial Longitudinal Arch-• Along the midline
border of the calcaneus up to the first metatarsal
• Supported by the Plantar Ligament

Lateral Longitudinal Arch –• Calcaneous to the
fifth Metatarsal

Bone Injuries• Fifth Metatarsal
Avulsion Fracture (Jones Fracture)
• Jones fracture is an injury that occurs over time non-impact
• Epiphyseal Injury of Distal Tibia and Fibula
• Stress Fractures

Bone Injuries
• While bones have viscoelastic properties, bone is fairly rigid and serves as a poor shock absorber
• Brittle nature increases under tension rather than compression
• Cylindrical nature of bones make them very strong - resistant to bending and twisting

• Bone Trauma Classifications
Periostitis - inflammation of the periosteum - result primarily of contusions and
produces rigid skin overlying muscle (acute and chronic)
Acute bone fractures - partial or complete disruption that can be either
closed or open (through skin)
- serious musculoskeletal condition

Type of fractures include, depressed, greenstick, impacted, longitudinal, oblique, serrated, spiral, transverse, comminuted, blowout, and avulsion
Stress fractureType of fractures include, depressed, greenstick, impacted, longitudinal, oblique, serrated, spiral, transverse, comminuted, blowout, and avulsion
Stress fractures- no specific cause but with a number of possible causes Overload due to muscle contraction, altered stress distribution
due to muscle fatigue, changes in surface, rhythmic repetitive stress vibrations
s- no specific cause but with a number of possible causes Overload due to muscle contraction, altered stress distribution
due to muscle fatigue, changes in surface, rhythmic repetitive stress vibrations


Bone becomes susceptible early in training due to increased muscular forces and initial remodeling and resorption of bone
Progression involves, focal microfractures, periosteal or endosteal response (stress fx) linear fractures and displaced fractures
Typical causes include Coming back to competition too soon after injury Changing events without proper conditioning Starting initial training too quickly Changing training habits (surfaces, shoes….etc) Variety of postural and foot conditions
Early detection is difficult, bone scan is useful, x-ray is effective after several weeks

Major signs and symptoms include focal tenderness and pain, (early stages) pain with activity, (later stages) with pain becoming constant and more intense, particularly at night, (exhibit a positive percussion tap test)
Common sites involve tibia, fibula, metatarsal shaft, calcaneus, femur, pars interarticularis, ribs, and humerus
Management varies between individuals, injury site and extent of injury
More easily managed and healed if on compression side of bone vs. tension (may result in complete fx)

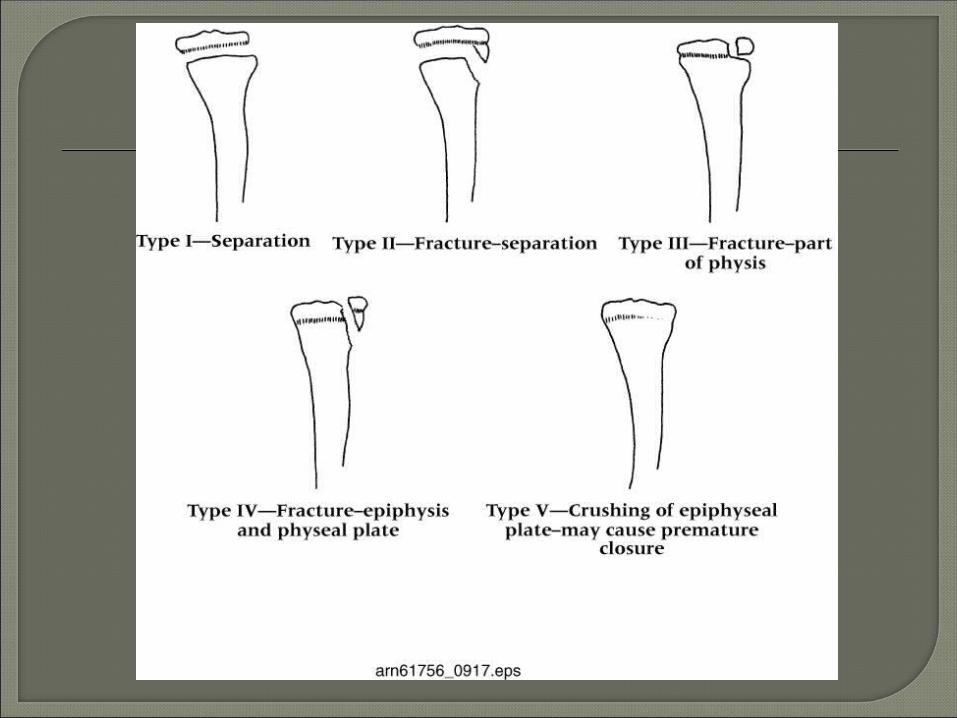
Epiphyseal Conditions - three types can be sustained by adolescents (injury to growth plate, articular epiphysis, and apophyseal injuries) Occur most often in children ages 10-16 years old
Classified by Salter-Harris into five types (see photo on next slide)
Apophyseal Injuries - Young physically active individuals are susceptible Apophyses are traction epiphyses in contrast to
pressure epiphyses. Serve as sites of origin and insertion for muscles Common avulsion conditions include Sever’s disease
and Osgood-Schlatter’s disease

P—Protection-braces, slings, crutches, taping-etc, at least 1st three days
R—Rest-stress on injured tissue should be avoided
I—Ice-no longer than 20 minutes, at least 1 hour between icings
C—Compression-pressure applied to the injured body part does not allow swelling to build
E—Elevation-10 to 12 inches above the heart

Names of ligaments give their attachment points e.g. calcaneofibular ligament.
Deltoid ligament (medial) is stronger than all lateral ligaments combined.