Mr. Ranganathan
23
DEATH AUDIT DECEMBER 2016 Dr. Sujay Iyer I Year PG General Medicine Unit IV
-
Upload
sujay-iyer -
Category
Health & Medicine
-
view
18 -
download
0
Transcript of Mr. Ranganathan

DEATH AUDITDECEMBER 2016Dr. Sujay IyerI Year PGGeneral Medicine Unit IV

PATIENT DETAILS Name: Mr. Ranganathan Age/ Gender: 67 years/ Male MR number: 16/402110 IP number: 16/061538 DOA: 15/12/2016 at 18:54 DOD: 19/12/2016 at 01:30 Duration of Stay: 3 days

PRESENTING COMPLAINT Patient was brought to the ER on 15/12/16 at
5 pm in an unconscious state with ET tube in-situ without any ambu-bag or ventilatory support.

HISTORY OF PRESENTING ILLNESS Patient had sudden onset of loss of consciousness
after he complained of dizziness on 10/12/16 which resulted in a slip and fall.
H/O involuntary micturition (+) H/O deviation of angle of mouth to right side (+) H/O weakness of left upper and lower limb. He was taken to Manakulla Vinayagar Hospital
where he was diagnosed as right MCA territory infarct with hemorrhagic transformation after a CT scan brain was done (Large left fronto-parietao-temporal infarct with hemorrhagic transformation and significant midline shift)
He was intubated and ventilated due to poor GCS.

HOPI Patient was treated with Mannitol,
Atorvastatin, Ceftriaxone and Dexamthasone. Outside investigations on 13/12/16:
Urea: 133; Creat: 4.43 TC: 18,900 2D ECHO: Inferior wall hypokinesia (+), LVH (+),
LVEF – 45%, CAD (+). Decompressive craniotomy was advised, but
since patient’s attenders were unwilling; patient was discharged against medical advice.

HOPI Patient was taken to PIMS and East Coast
Hospital where the same advice was given, but since patient’s relatives were unwilling; he was discharged against medical advice and taken home.
He was kept at home for a day with ET tube in-situ.
On the afternoon of 15/12/16, patient started gasping and was brought to MGMCRI for further management

PAST HISTORY K/C/O Systemic Hypertension and Type 2
Diabetes Mellitus since 4 years. On irregular medication
Not a K/C/O PTB, Seizure disorder, Bronchial Asthma.

GENERAL EXAMINATION HR – 120/min BP – 80 systolic RR – 24/min SpO2 – 98% on room air with ET tube insitu Temp – 103*F GCS – 3T/15 CBG – 158 mg%
Patient was immediately mechanically ventilated by Critical Care team in Volume Control mode after airway suction was done.

SYSTEMIC EXAMINATION R/S: NVBS (+). BAE (+). B/l conducted
sounds (+) CVS: S1S2 (+). No murmurs. P/A: Soft, non-tender, no organomegaly. CNS:
GCS - 3T/15. Unresponsive to painful stimuli. Left and Right UL and LL tone – Reduced. Bilateral plantars – Mute. Left pupil – Sluggishly reacting to light.

INITIAL MANAGEMENT Patient was immediately started on Inj.
Dopamine at 5mcg/kg/min. Neurosurgery, Critical Care and
Ophthalmology opinions were sought. Neurosurgery consult was for nil intervention. Poor prognosis was explained to the patient’s
relatives. Patient was admitted under GM IV in the ICU.

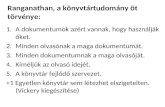
ECG

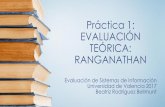
CHEST X-RAY

INITIAL INVESTIGATIONSPATHOLOGY BIOCHEMISTRY BIOCHEMISTRYCBC:Hb – 14.9TC – 13,900 (N: 80%)Plt – 96,000
URINE ROUTINE:Pus cells – (+)Bacteria – OccasionalSugar – (+)
ABG: pH – 7.45pCO2 – 37pO2 – 33HCO3 - 25
RFT:Urea – 32.9Creat – 6.7
ELECTROLYTES:Na – 143K – 4.6Cl – 107Ca – 8Ph – 4.8Mg – 1.5
LFT:T.P – 6.4Alb – 3.8T.B – 2.3D.B – 0.9
AST – 84ALT – 49AlkP - 75Amylase – 75GGT – 71PT – 16 (13.5)INR – 1.2PTT – 26 (32)
CARDIAC MARKERS:TROP I – (-)CPK T – 737CPK MB – 15

INITIAL TREATMENT Inj. Piperacillin + Tazobactum 4.5g IV stat
then 2.25 g IV TDS. Inj. 3% NS IVF at 20 ml/hr. Inj. Pantoprazole 40 mg IV OD. Inj. Noradrenaline IVF at 1.3 ml/hr (Targer
MAP of 65 mmHg) Syp. Lactulose 30 ml TDS. Inj. Dopamine was tapered off.

15/12/16 At 10 pm, patient was found to have a HR>
200/min on the monitor. ECG revealed SVT. Pulse was not felt. Patient was cardioverted twice with 50 J and
then once with 100 J. Patient reverted back to sinus rhythm. CVP line in subclavian vein was placed.
Arterial line was also placed.

16/12/16 Patient was on PCV mode with Inj.
Noradrenaline. HR – 109/min. BP – 100/70. I/O – 2070/360. Unresponsive to deep painful stimuli. Nephrology opinion was sought in view of
requirement of hemodialysis for poor urine output.
Dr. Hemachander advised hemodialysis under high risk, patient’s relatives refused.

17/12/16 Patient was on CPAP mode. Noradrenaline
had been tapered. HR – 85/min. BP – 130/70 mmHg. I/O –
4133/2175. Patient was started on Inj. Amiodarone IVF at
2.2ml/hr in view of frequent SVT. Patient’s hyperkalemia was corrected. Neurologically, patient continued to be in
status quo. Hyoptonia in all 4 limbs Right plantar – extensor. B/L pupils – sluggishly reactive.

INVESTIGATIONS17/12/16 18/12/16
Urea – 99Creat – 6.5
Na – 149K – 5.0Cl - 117
Urea – 146Creat – 5.17
Na – 149K – 4.9K - 117

18/12/16 Patient was on PCV mode. On Inj.
Amiodarone infusion. HR – 89/min. BP – 220/90 mmHg. I/O –
4428/2365. Patient was unresponsive to deep painful
stimuli. Neurologically deteriorating as pupils were
found to be dilated and fixed, not reactive to light.

18/12/16 At 11 40 pm, patient was found to have HR >
200/min. Monitor showed Ventricular Tachycardia.
BP – 70/40 mmHg. SpO2 – 62% at 100% FiO2 at PCV mode.
Patient was given 2 cycles of defibrillation at 150 J.
CPR was initiated according to ACLS protocol. Patient continued to have VT despite 5 cycles
of defibrillation and Inj. Adrenaline. At 12 30 am, Inj. Amiodarone 150mg bolus
was given.

19/12/16 At 12 45 am, patient developed SVT. Inj.
Adenosine was administered. At 1 am, patient went into bradycardia. CPR
was continued. At 1 25 am, patient went into asystole. Heart
sounds were absent. Despite all resucitative efforts, patient was
declared dead at 1 30 am.

CAUSE OF DEATH Cerebrovascular Accident – Left middle
cerebral artery infarct with hemorrhagic transformation.
Systemic Hypertension. Coronary Artery Disease. Acute Kidney Injury. Acute on Chronic Kidney Disease.

THANK YOU