MPOM 010 Service Learning Student Workbook ... MPOM 101 Service learning 2015 Page 1 FACULTY OF...
39
1 MPOM 101 Service learning 2015 Page 1 FACULTY OF HEALTH SCIENCES SCHOOL OF MEDICINE 2015 MPOM 010 Service Learning Student Workbook LONGITUDINAL SERVICE LEARNING THIS WORKBOOK BELONGS TO: NAME: ____________________________________________________________ STUDENT NUMBER: _________________________________________________ CONTACT NUMBER: _________________________________________________ E-MAIL ADDRESS: ___________________________________________________ LEARNING FACILITATOR: Name: ________________________________________ CLINIC: _______________________________ Compiled by Debbie Barnard Revised December 2014 SL Coordinator Sefako Makgatho Health Sciences University Faculty of HEALTH SCIENCES School of MEDICINE Study field: MBChB Course: Practice of Medicine Year: 1
Transcript of MPOM 010 Service Learning Student Workbook ... MPOM 101 Service learning 2015 Page 1 FACULTY OF...

1
MPOM 101 Service learning 2015 Page 1
FACULTY OF HEALTH SCIENCES
SCHOOL OF MEDICINE
2015 MPOM 010 Service Learning
Student Workbook
LONGITUDINAL SERVICE LEARNING
THIS WORKBOOK BELONGS TO: NAME: ____________________________________________________________
STUDENT NUMBER: _________________________________________________
CONTACT NUMBER: _________________________________________________
E-MAIL ADDRESS: ___________________________________________________
LEARNING FACILITATOR: Name: ________________________________________
CLINIC: _______________________________
Compiled by Debbie Barnard Revised December 2014
SL Coordinator
Sefako Makgatho Health Sciences University
Faculty of HEALTH SCIENCES
School of MEDICINE Study field: MBChB
Course: Practice of Medicine
Year: 1
2
MPOM 101 Service learning 2015 Page 2
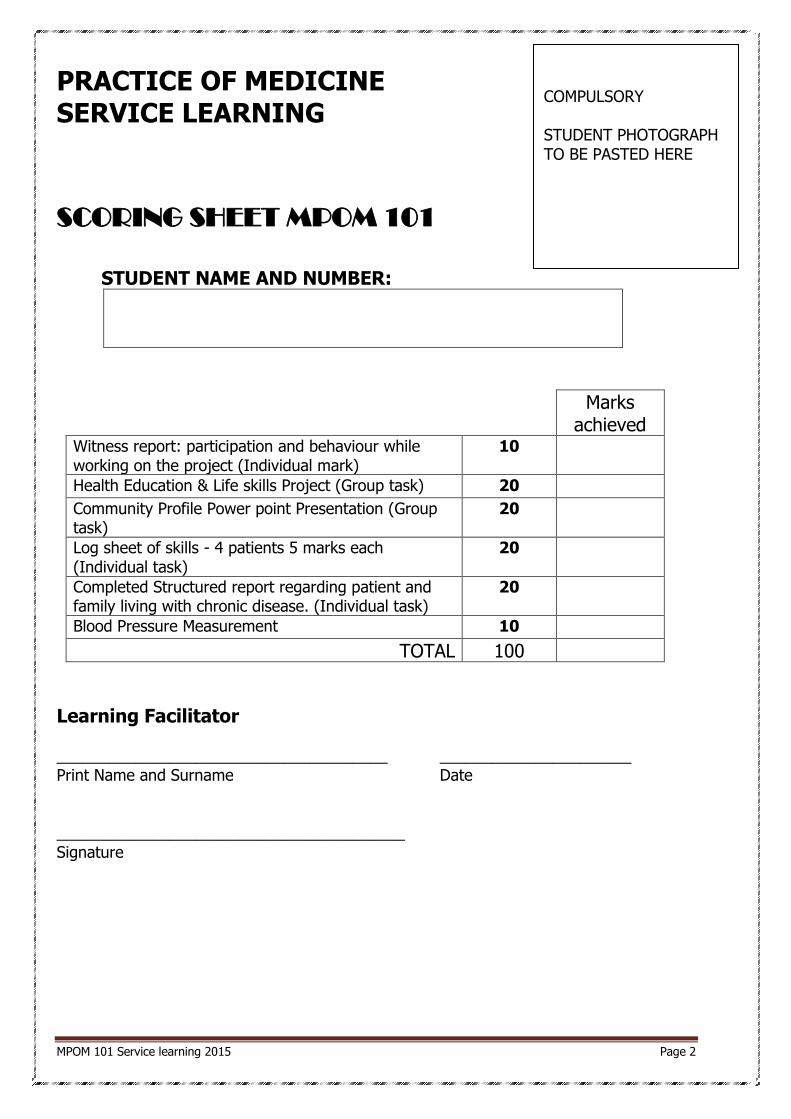
PRACTICE OF MEDICINE SERVICE LEARNING
SCORING SHEET MPOM 101
STUDENT NAME AND NUMBER:
Marks achieved
Witness report: participation and behaviour while working on the project (Individual mark)
10
Health Education & Life skills Project (Group task) 20 Community Profile Power point Presentation (Group task)
20
Log sheet of skills - 4 patients 5 marks each (Individual task)
20
Completed Structured report regarding patient and family living with chronic disease. (Individual task)
20
Blood Pressure Measurement 10
TOTAL 100
Learning Facilitator ______________________________________ ______________________ Print Name and Surname Date ________________________________________ Signature
COMPULSORY STUDENT PHOTOGRAPH TO BE PASTED HERE

3
MPOM 101 Service learning 2015 Page 3
THIS IS A
CRITICAL MESSAGE TO THE STUDENT
NO STUDENT MAY VISIT THE CLINIC IF THEY DO NOT HAVE THE
FOLLOWING EQUIPMENT WITH THEM:
A STETHOSCOPE
A BAUMANOMETER (BLOOD PRESSURE APPARATUS)
A THERMOMETER
A WATCH WITH A SECOND HAND (MAY NOT USE A CELL PHONE)
A CLEAN WHITE COAT
OWN SUPPLY OF GLOVES
HANDBOOKBOOK: Talley & O’Connor
The student also needs to take with:
- Own lunch - Water - Personal toiletries like toilet paper
If the student does not have the necessary equipment to perform practical procedures WITH them, their books will
and may not be signed by the facilitators!

4
MPOM 101 Service learning 2015 Page 4
TABLE OF CONTENTS:
Page No
1 Organisational Component 5 2 Witness report 6
3 Report on health promotion workshop/talk presented in the community
8
4 Format for community profile power point presentation 10
5 Log sheet of patient examination at the clinic 12
6 Report on a family living with chronic disease 15
7 Blood pressure control 24
8 Clinic assessment 27
9 Student feedback and reflection 33
10 SL reflective diary 35
11 Conclusion and suggestions regarding the block 36
12 Checklist for documents handed in 38
Safety Guidelines and Rules of Conduct in the Community Find draft copy included in the “GENERAL GUIDELINES + YEAR SCHEDULE POME 105 OF 2013”
document as it was developed in December 2010.
You are representing Sefako Makgatho Health Sciences University and the Medical Profession.
Dress and act professionally!
WELCOME to the Service Learning program!
5
MPOM 101 Service learning 2015 Page 5
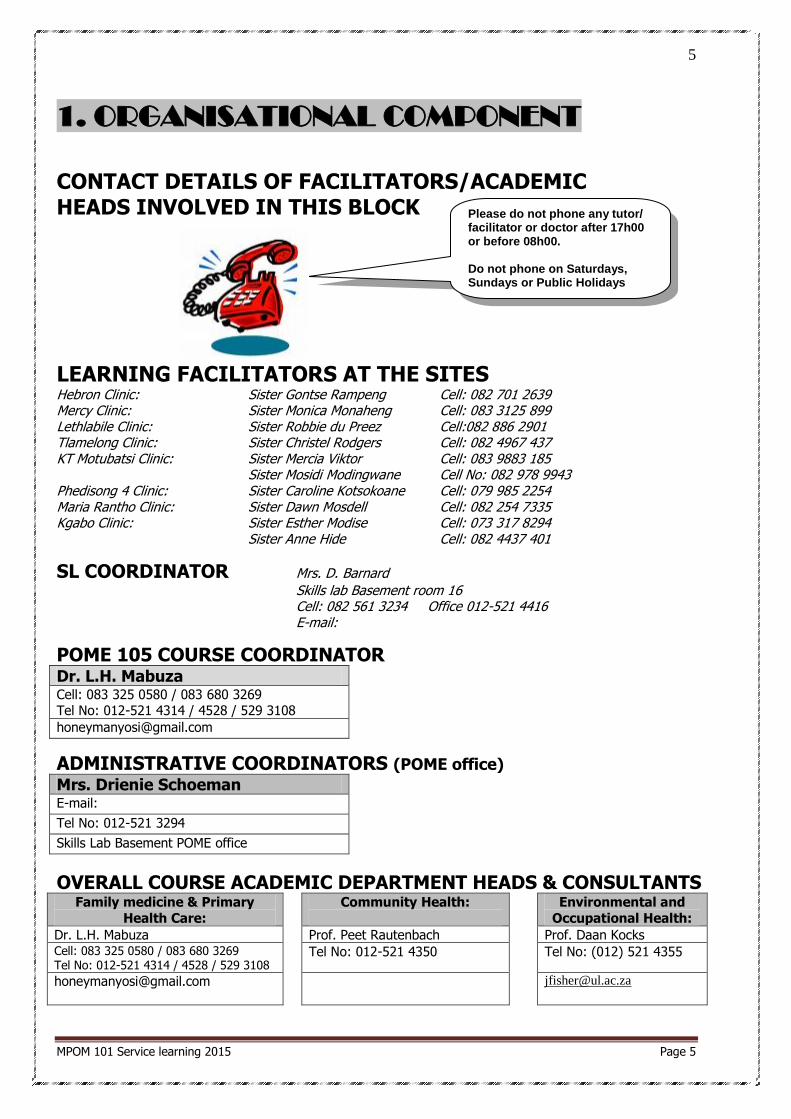
1. ORGANISATIONAL COMPONENT
CONTACT DETAILS OF FACILITATORS/ACADEMIC HEADS INVOLVED IN THIS BLOCK
LEARNING FACILITATORS AT THE SITES Hebron Clinic: Sister Gontse Rampeng Cell: 082 701 2639 Mercy Clinic: Sister Monica Monaheng Cell: 083 3125 899 Lethlabile Clinic: Sister Robbie du Preez Cell:082 886 2901 Tlamelong Clinic: Sister Christel Rodgers Cell: 082 4967 437 KT Motubatsi Clinic: Sister Mercia Viktor Cell: 083 9883 185 Sister Mosidi Modingwane Cell No: 082 978 9943 Phedisong 4 Clinic: Sister Caroline Kotsokoane Cell: 079 985 2254 Maria Rantho Clinic: Sister Dawn Mosdell Cell: 082 254 7335 Kgabo Clinic: Sister Esther Modise Cell: 073 317 8294
Sister Anne Hide Cell: 082 4437 401
SL COORDINATOR Mrs. D. Barnard
Skills lab Basement room 16 Cell: 082 561 3234 Office 012-521 4416 E-mail:
POME 105 COURSE COORDINATOR
Dr. L.H. Mabuza Cell: 083 325 0580 / 083 680 3269 Tel No: 012-521 4314 / 4528 / 529 3108
ADMINISTRATIVE COORDINATORS (POME office)
Mrs. Drienie Schoeman E-mail: Tel No: 012-521 3294 Skills Lab Basement POME office
OVERALL COURSE ACADEMIC DEPARTMENT HEADS & CONSULTANTS Family medicine & Primary
Health Care:
Community Health:
Environmental and
Occupational Health:
Dr. L.H. Mabuza Prof. Peet Rautenbach Prof. Daan Kocks Cell: 083 325 0580 / 083 680 3269 Tel No: 012-521 4314 / 4528 / 529 3108
Tel No: 012-521 4350 Tel No: (012) 521 4355
Please do not phone any tutor/ facilitator or doctor after 17h00 or before 08h00. Do not phone on Saturdays, Sundays or Public Holidays
6
MPOM 101 Service learning 2015 Page 6
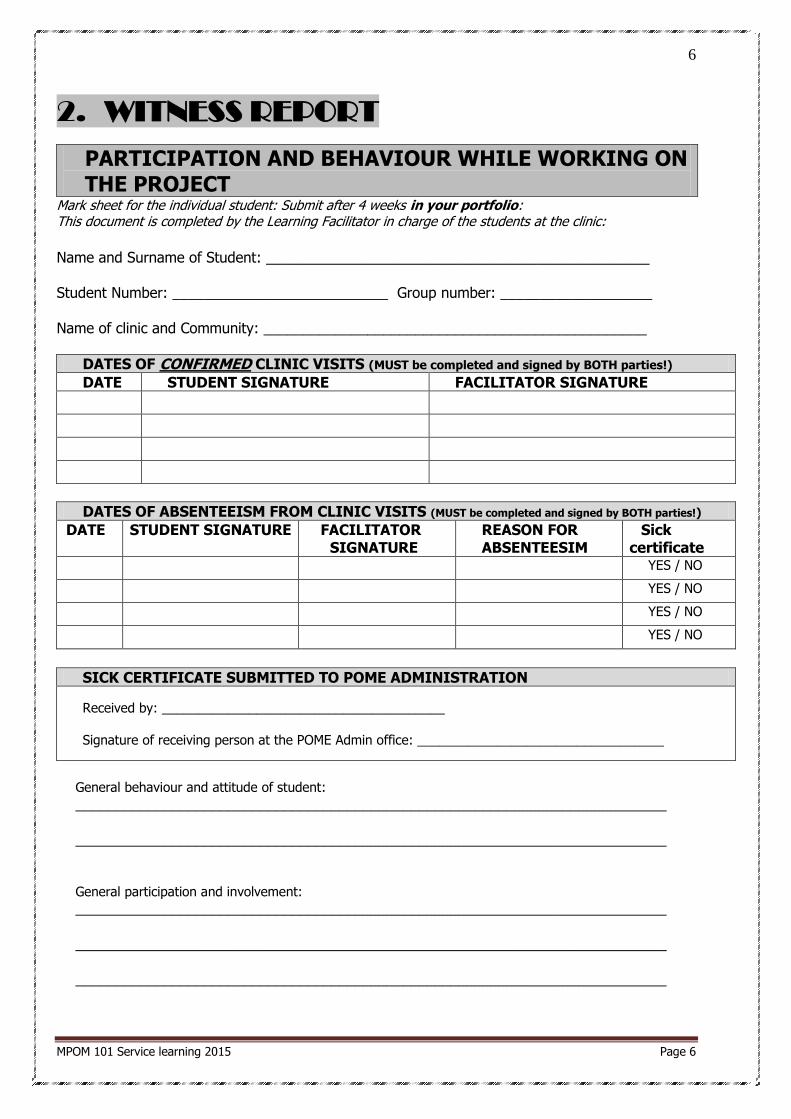
2. WITNESS REPORT
PARTICIPATION AND BEHAVIOUR WHILE WORKING ON THE PROJECT
Mark sheet for the individual student: Submit after 4 weeks in your portfolio: This document is completed by the Learning Facilitator in charge of the students at the clinic:
Name and Surname of Student: ________________________________________________ Student Number: ___________________________ Group number: ___________________ Name of clinic and Community: ________________________________________________
DATES OF CONFIRMED CLINIC VISITS (MUST be completed and signed by BOTH parties!)
DATE STUDENT SIGNATURE FACILITATOR SIGNATURE
DATES OF ABSENTEEISM FROM CLINIC VISITS (MUST be completed and signed by BOTH parties!)
DATE STUDENT SIGNATURE FACILITATOR SIGNATURE
REASON FOR ABSENTEESIM
Sick certificate
YES / NO
YES / NO
YES / NO
YES / NO
SICK CERTIFICATE SUBMITTED TO POME ADMINISTRATION
Received by: _______________________________________
Signature of receiving person at the POME Admin office: __________________________________
General behaviour and attitude of student: __________________________________________________________________________ __________________________________________________________________________ General participation and involvement:
__________________________________________________________________________ __________________________________________________________________________ __________________________________________________________________________
7
MPOM 101 Service learning 2015 Page 7
Ability to work in a team: __________________________________________________________________________ __________________________________________________________________________ Ability to build relationships with patient(s):
__________________________________________________________________________ __________________________________________________________________________ __________________________________________________________________________ Comments on the quality of work as performed by this student:
__________________________________________________________________________ __________________________________________________________________________ __________________________________________________________________________
Overall global score - Use as guideline 9-10 Student is excellent, CANNOT BE FAULTED at all, NO room for improvement!
6-8 Student has good abilities and all objectives & critical issues was acceptably addressed
5 Student is borderline, has abilities in at least half of the areas with no critical errors
3-4 Student’s performance is poor, only competent is some areas, but has major weaknesses
0-2 Student is incompetent, does not meet the objectives, critical errors
Recommendations / actions that student must take in order to improve: __________________________________________________________________________ __________________________________________________________________________ __________________________________________________________________________
Student : ________________________________________ Print Name and Surname
________________________________________ ______________________ Signature Date
Learning Facilitator in charge: ________________________________________ ______________________ Print Name and Surname Date
________________________________________ Signature
Final mark: _________
10
STUDENT MUST SIGN!!

8
MPOM 101 Service learning 2015 Page 8
3. HEALTH PROMOTION WORKSHOP/ TALK
PRESENTED IN THE COMMUNITY
REPORT ON HEALTH PROMOTION WORKSHOP/TALK PRESENTED IN THE COMMUNITY
Specific topic: ________________________________________________________________ Content areas covered in the talk: What specifically did you talk about?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ Why and how did you decide to choose this topic?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ Specify your target audience (To whom did you present, how many people attended)?
__________________________________________________________________________________________________________________________________________________________________________________________ Where were the talk presented / which facilities were used? Was this sufficient?
__________________________________________________________________________________________________________________________________________________________________________________________ How did you present your talk and poster? E.g. only talked, talked and allowed discussion (which
questions/comments did you get), activities e.g. condom demonstration, role-plays etc.
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ ______________________________________________________________ What materials did you develop to enhance the efficiency of your talk? E.g. pamphlet was develop and
handed to all who attended, or a poster was developed and put on the wall.
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
9
MPOM 101 Service learning 2015 Page 9
What were the outcomes of your talk? How did your talk contribute to developments in the community?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ Recommendations / comments from target audience:
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Student : ________________________________________ Print Name and Surname ________________________________________ ______________________ Signature Date
Learning facilitator in charge: ________________________________________ ______________________ Print Name and Surname Date
________________________________________ Signature
Final mark: _________
20 -10% for poor participation of the student
10
MPOM 101 Service learning 2015 Page 10
4. COM
MUNITY PROFILE POWER POINT
PRESENTATION
FORMAT FOR COMMUNITY PROFILE POWER POINT PRESENTATION
GROUP REPORT:
1. Each group of students attending a clinic/visiting the community must develop a power point
presentation of the students’ and community’s activities and findings that were witnessed during the
visits. 2. CONTENT: slides must cover the following information regarding the Community
Describe the geographical area (approximate size, boundaries)
Indicate the population numbers
Indicate the Ethnical group in dominance
Indicate the literacy levels amongst the community
Indicate the economic activities in the community and surrounding areas
Describe the disease profile (commonest diseases) patients present with
Indicate the governance of the community (e.g. chief vs. municipality etc.)
NB Indicate the risk areas and situations in the community (risk to mental and physical health)
NB Show/indicate resources in the area e.g. water supply, transport, health care, education,
housing, religion, sanitation, economic activities etc. (how many and type of schools, crèches, churches, clinics etc.).
Show/indicate resources in the health care facility you visited (sponsors, equipment, facilities,
building, beds, staff, medicines, storeroom etc.) Show/indicate services offered to the community by the health care facility (e.g. describe and
provide photographs of home based care programme, types of clinic, outreach activities such as
mobile clinics, food gardens, sewing/baking programmes, computer literacy etc.)
Show/indicate strengths and weaknesses of the facility and the environment
Show what the students did during their visit.
Indicate what you have done and learnt during the block (NB! Action photographs speak a
thousand words! – do NOT include a group of students posing, rather take a photograph of a student interacting with a patient!)
Present your recommendations to better health related services to the community – be realistic!
3. The mark that the student group will be given will be used as a TEST MARK for exam admission – no
re-do’s will be allowed 4. Try to restrict the written slides to below 20 and the photographs to 20 as well. 5. Do NOT use photographs or slides from other groups/year groups! You will get NO MARK
for your assignment as it is plagiarism!
6. Indicate the group and the year clearly on the cover of the CD.
Remember:
MARKS: 20
THIS POWER POINT PRESENTATION IS AN
EXTREMELY IMPORTANT DOCUMENT! Give a lot of
attention to it!
11
MPOM 101 Service learning 2015 Page 11
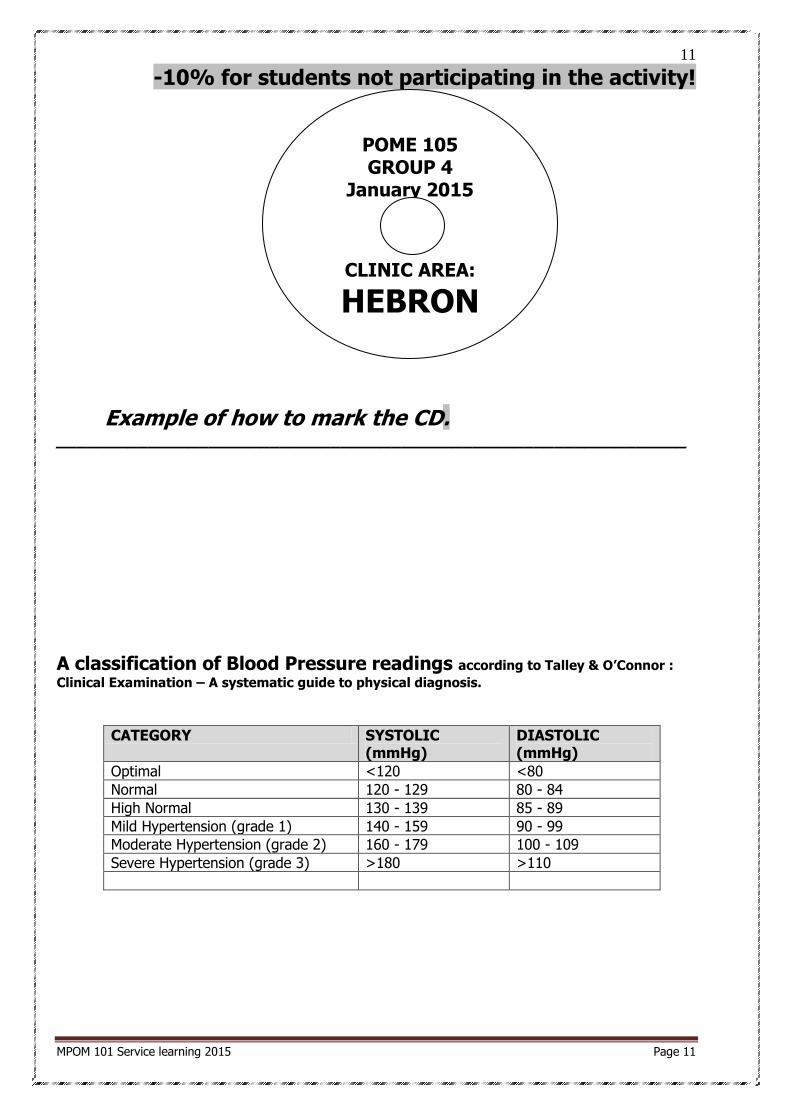
-10% for students not participating in the activity!
Example of how to mark the CD. ______________________________________________________________
A classification of Blood Pressure readings according to Talley & O’Connor :
Clinical Examination – A systematic guide to physical diagnosis.
CATEGORY SYSTOLIC (mmHg)
DIASTOLIC (mmHg)
Optimal <120 <80
Normal 120 - 129 80 - 84
High Normal 130 - 139 85 - 89
Mild Hypertension (grade 1) 140 - 159 90 - 99
Moderate Hypertension (grade 2) 160 - 179 100 - 109
Severe Hypertension (grade 3) >180 >110
POME 105 GROUP 4
January 2015
CLINIC AREA:
HEBRON

12
MPOM 101 Service learning 2015 Page 12
5. PATIENT EXAMINATIONS AT CLINIC
LOG SHEET OF PATIENT EXAMINATIONS AT CLINIC
Example: Mrs Y visits the clinic with the presenting complaint of an abscess on the right arm. She has a fever. Her vital signs and observations are recorded in the table below:
Patient 1: __________________________________________________________________ __________________________________________________________________________ Patient 2: __________________________________________________________________ __________________________________________________________________________ Patient 3: __________________________________________________________________ __________________________________________________________________________ Patient 4: __________________________________________________________________ __________________________________________________________________________
Example Patient 1 Patient 2 Patient 3 Patient 4 File no
Y 007
BP
125
80 (Normal)
Pulse
102 beats/min (Fast heart rate / regular)
Respiratory rate
14 per min (Normal)
Temperature
38.2 ᵒ C Axillary
(Fever)
Height
1.72m
Weight
82 kg
BMI*
27.7 (Grade 1
obesity)
Blood sugar
5.4 mmoll/L
Urine test
Ketones ++
Glucose +++ pH 7
SG 1020
NB! See information in Talley & O’Connor for values

13
MPOM 101 Service learning 2015 Page 13
BODY MASS INDEX: How to calculate body mass index (BMI):
BMI = weight/ height² = 82 / (1.72 x 1.72)
= 82/ 2.96 = 27.7
Interpretation of BMI:
Below 18.5: Underweight 18.5 – 24.9: Normal
25 -29.9: Grade 1 obesity 30 – 39.9: Grade 2 obesity
40 +: Grade 3 obesity
STUDENT INTERPRETATION OF ABOVE FINDINGS:
Example The patient’s diabetes is not well controlled. She has a fever. She has repeated infections like
urinary tract infections. Leg ulcers that do not want to heal. Lifestyle advice needed as she is
also overweight according to her BMI.
Patient 1
Patient 2

14
MPOM 101 Service learning 2015 Page 14
Patient 3
Patient 4
Ask your mentor to assist you in this learning.
The challenge is that you have to read and ask as much as possible regarding the patients seen. We
want you to learn what you can!. Do not sit back and wait for learning to occur. Actively search for knowledge and skills and make the best of this opportunity.
If you are finished with your 4 patients and there is time left, then you see more patients.
COMMENTS ABOUT THE STUDENT BY THE LEARNING FACILITATOR: _________________________________________________________________________ __________________________________________________________________________ __________________________________________________________________________
Signature Learning Facilitator: _______________________________
Date: _________________
Final mark: _________
20

15
MPOM 101 Service learning 2015 Page 15
6. FAMILY LIVING WITH CHRONIC DISEASE
PATIENT INFORMATION Initials: ___________ Gender: _________ Date of birth: _________ Age: _____ Clinic file no: _______________ Chronic medical illness: ____________________________________________________________
__________________________________________________________________________________________________________________________________________________________________________________________ Brief history of the current illness you are studying, in the example it was diabetes. When was it diagnosed, has the patient been admitted to hospital, any complications such as kidney failure:
____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ Previous medical history (briefly):
Example: patient was admitted to hospital for kidney infection in 2001 and had malaria in 2003.
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Family history regarding hereditary/chronic diseases. E.g. two brothers also has diabetes:
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Hobbies and interests ______________________________________________________________
____________________________________________________________________________________________________________________________
Educational history: ________________________________________________________________
__________________________________________________________________________________________________________________________________________________________________________________________
Habits (smoking, drinking and recreational drugs): _________________________________________

16
MPOM 101 Service learning 2015 Page 16
____________________________________________________________________________________________________________________________ Health promotion and/or awareness: (Exercise, healthy food, hygiene):
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Medicine allergies:
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
The following section on Current treatment should be seen as a challenge for the student and part of active learning. After the student has seen the patient, he/she should read up about the medication and declare if the reason that the patient gave the student why he/she is taking the medication is correct or not. Then look up and describe the general information that you would give the patient regarding the use of medicine.

17
MPOM 101 Service learning 2015 Page 17
CURRENT TREATMENT (PRESCRIPTION, OVER THE COUNTER AND HERBAL MEDICINES):
Name of medication Indication (Why is the patient taking the medicine?) Patient’s knowledge of the medication (what used for, how to drink)
Example: Glucophage 500mg tablets
According to the patient, for what reason is the pt taking the medication? How is the patient drinking the medication (dosage) To manage his Diabetes, Used for high sugar, drink one tablet every day, same time, cannot drink 2 if skipped
1.
According to the patient, for what reason is the pt taking the medication? How is the patient drinking the medication (dosage)
2.
According to the patient, for what reason is the pt taking the medication? How is the patient drinking the medication (dosage)
3.
According to the patient, for what reason is the pt taking the medication? How is the patient drinking the medication (dosage)
4.
According to the patient, for what reason is the pt taking the medication? How is the patient drinking the medication (dosage)
5.
According to the patient, for what reason is the pt taking the medication? How is the patient drinking the medication (dosage)
6.
According to the patient, for what reason is the pt taking the medication? How is the patient drinking the medication (dosage)
18
MPOM 101 Service learning 2015 Page 18
Describe the general education regarding medicine use that you would give a patient:
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
_________________________________________________________________________________
Insert extra page if the above space is not sufficient.
What difficulties does the patient face in dealing with his disease? (implications on lifestyle) Example: The diabetes has affected her eyesight so she cannot read. This leads to big frustration as it was her only pastime. Or the patient has to rely on her neighbour for transport to the clinic for repeat prescriptions...
__________________________________________________________________________________________________________________________________________________________________________________________
19
MPOM 101 Service learning 2015 Page 19
____________________________________________________________________________________________________________________________ Describe the family and community’s attitude and the support of the patient:
____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ If possible a family member can be interviewed to hear about their frustrations in dealing with the patient’s illness. How has it affected their lives?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Family Profile – who forms part of the family Patient Patient
partner or spouse
Person sharing
Person sharing
Person sharing
Person sharing
Male/ female
Age
Highest level of education
Diseases or conditions
What needs does the member have in order to cope with the pt e.g. support,
income, transport, wheelchair
Employment
Source of income (including grant)
20
MPOM 101 Service learning 2015 Page 20
Surroundings This differs from an Ecomap. Do not indicate the relationship (energy flow).
Please give a detailed description. Listen to the community’s needs.
DESCRIPTION Housing (Number of rooms, ventilation, bathroom(s), toilet, type of structure (e.g. brick building)
Property (fencing, water, energy source, roads etc.)
Schools
Churches
Nearby shops e.g. spaza, supermarket. What don’t they sell
Municipal offices or other local authorities
Police station and Magistrates office Medical clinic
Private doctor(s)
Traditional healers
Places that sell alcohol or other recreational Drugs
Welfare organizations including places that render services such as food parcels
Social clubs and recreational facilities for adults and children
Sports facilities
Put yourself in the family’s position. Are there any other systems that impact on the family? Elaborate
Ask the patient and family to identify their health needs
Comments
21
MPOM 101 Service learning 2015 Page 21
GENOGRAM

22
MPOM 101 Service learning 2015 Page 22
CLINICAL EXAMINATION OF YOUR PATIENT
Result Interpretation (What does this mean?)
O
BS
ER
VA
TIO
NS
BP
Pulse
Respiratory Rate
Temp
Blood glucose
M
EA
SU
RE
ME
NT
S
Waist
Hip
Height
Waist to hip ratio (Talley & O’Connor)
Estimated weight
BMI
General appearance e.g. gait, looks healthy (Talley & O’Connor)
Fully conscious /stable/unstable
Do you think that the patient’s illness has an impact on the rest of the family? Explain.
______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ Do you think that the community, with its limited resources, has an effect on the patient? Explain.
__________________________________________________________________________________________________________________________________________________________________________________________
23
MPOM 101 Service learning 2015 Page 23
____________________________________________________________________________________________________________________________ In your opinion, what could be done by the community and other partners involved to improve the activities
of daily living for your patient and family.
Example: My diabetic patient can be educated to grow fresh vegetables to improve his diet. I could also give advice on other hobbies after consulting with occupational therapy. The patient can also be motivated to start, or join a support group for people with Diabetes.
____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ What lessons have you learnt from spending time with your family living with chronic illness?
______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ How did you contribute in the wellbeing of your family living with chronic illness?
__________________________________________________________________________________________________________________________________________________________________________________________
Student : ________________________________________ Print Name and Surname ________________________________________ ______________________ Signature Date
Learning facilitator in charge: ________________________________________ ______________________ Print Name and Surname Date
________________________________________ Signature
Final mark: _________
20
24
MPOM 101 Service learning 2015 Page 24
7. BLOOD PRESSURE MONITORING
VITAL SIGN OBSERVATIONS
MEASURING A BLOOD PRESSURE
STUDENT NAME: _____________________________ DATE: ________________
SECTION A – Knowledge MARKS
1. Give the definition of Blood pressure
- it is the pressure or force of the blood against the walls of the arteries
/1
2. Give the definition of Systolic Blood pressure
- it is the pressure or force of the blood against the walls of the arteries during the
CONTRACTION of the heart
/0.5
3. Give the definition of Diastolic Blood pressure
- it is the pressure or force of the blood against the walls of the arteries when the heart is at rest/relaxed/not contracting
/0.5
4 Give the definition of Hypotension
- it is a low blood pressure
/0.5
Give the definition of Hypertension
- it is a high blood pressure
/0.5
5. Name 4 factors that could affect the blood pressure reading
- Cardiovascular disorders - Neurological disorders
- Kidney and urological disorders - Pre-eclampsia in pregnant woman
- Psychological factors- stress, anger
- Medication - White coat hypertension
/0.5
6. How would you determine if the BP cuff is the right size? - it should cover 2/3 of the upper arm
/0.5
SUBTOTAL /4
25
MPOM 101 Service learning 2015 Page 25
PROCEDURE: BLOODPRESSURE MEASUREMENT
SECTION B – Skill evaluation MARKS
1. Wash hands
Why? – to prevent cross infection
/0.5
2. Explain procedure to the pt
Why? – a well-informed patient is better prepared and less fearful.
/0.5
3. Have the pt sit or lie down with arm supported on pillow, table or side of the bed
- the room should be quiet and the patient must not talk
- If the pt is exerted/ walked a distance let the pt sit for + 5 minutes before commencing
Why? – exertion can influence the BP
/0.5
4. Position the pt’s arm so that it is + level to the pt’s heart
Expose the upper arm and remove restrictive clothing to avoid obstruction
/0.5
5. Squeeze the BP cuff to expel any air /0.5
6. Wind the BP cuff around the upper arm
- Use appropriate size cuff - the bottom ridge of the cuff should be + 2,5 cm above the bend of the arm (cover 2 thirds of the upper arm)
- Undersized cuff- overestimated BP, oversized cuff – underestimated BP
- the inflating part should be directly over the brachial arteries at the inner aspect of the arm, or as indicated on the cuff of the apparatus
- turn the pt’ palm upwards - keep the arm straight and relaxed
*
/0.5
7. Locate the radial pulse with finger tips
- While feeling the radial pulse with the one hand, inflate the apparatus very slowly until the radial pulse disappears
- note this reading as the estimated systolic blood pressure - cuff must not be hyper inflated – it may be painful for the patient
- deflate the cuff completely Why this procedure?
To determine the estimated systolic blood pressure
Student should be informed to indicate to the examiner what the reading was at which the pulse disappeared and the facilitator should confirm this by palpating the
radial pulse
/0.5
8. Locate the brachial artery to determine where the stethoscope should be placed NB – correct placement of the stethoscope!
- student should know where to locate the brachial artery
/0.5
9. Place the stethoscope earpieces in ears and test if it is working by tapping the bell
- position the stethoscope over the brachial artery – do not occlude the opening of the bell with fingers
- inflate the cuff to 20mmHg higher than your estimated systolic blood pressure
/0.5
10. Release the valve and deflate the cuff at 3-4mm/sec and listen for the first consecutive
sound of pulsations - note the reading as the systolic blood pressure.
- the sound is called Karotkoff 1
- it should be near the reading of the estimated systolic blood pressure. - continue to deflate the cuff slowly and note the point at which the sound disappears
- note the reading as the diastolic blood pressure
*
26
MPOM 101 Service learning 2015 Page 26
- the sound is called Karotkoff 5 - deflate completely NB!
- the student may repeat the BP measurement to ensure a correct reading, but only after
complete deflation and movement of the pt's arm and fingers to re-establish circulation
- avoid slow and repeated inflation of the cuff, as it can cause the blood flow to become inadequate and lead to incorrect readings
- document the blood pressure as systolic reading over diastolic reading
Student’s deflation and measuring method should be evaluated as a whole. Correct method is important. Student should show competence and confidence.
/0.5
11. Remove the cuff and ensure the pt’s comfort
- interpret findings and give the patient feedback
/0.5
12. Record the findings
The reading should be correct **** ****
/0.5
SUBTOTAL /6 TOTAL /10
* - 10% if not done/done incorrectly **** - fail if not done/done incorrectly
Student: ________________________________________ Print Name and Surname ________________________________________ ______________________ Signature Date
Learning facilitator in charge: ________________________________________ ______________________ Print Name and Surname Date
________________________________________
Final mark: _________
10
27
MPOM 101 Service learning 2015 Page 27
8. ASSESSMENT OF CLINIC FUNCTION
CLINIC INFRASTRUCTURE Does the clinic have electricity? Yes No
Does the clinic have running water? Yes No
Does the clinic have warm running water? Yes No
Is there a patient waiting area that provides shelter from the Yes No
weather?
Is there sufficient seating for patients in the waiting area? Yes No
What happens to the weak/bedridden patients waiting for the doctor – wheelchairs? ________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________
Does the clinic have a working telephone? Yes No
If NO, how do they communicate?
________________________________________________________________________________________________________________________________________________________________________________
________________________________________________________________________________________
Does the clinic have a link to the internet? Yes No
Does the clinic have transport? Yes No
If YES, describe the transport available and what it is used for:
________________________________________________________________________________________________________________________________________________________________________________
________________________________________________________________________________________
How do very ill or emergency patients get to hospital?
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
Does the clinic have a refrigerator? Yes No
If YES, what is stored in the refrigerator? LOOK!
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
Clinic transport Taxi
Emergency services Own transport
Other means ( Specify)

28
MPOM 101 Service learning 2015 Page 28
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
What happens if the electricity goes off? ________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
Is the refrigerator temperature recorded daily? Yes No
Is the facility (clinic) clean and tidy? Yes No
Does the clinic have toilet facilities for the public? Yes No
If Yes, describe the toilet facilities. ________________________________________________________________________________________________________________________________________________________________________________
________________________________________________________________________________________
Does the toilets have lids and seats? Yes No
Amount of toilets for the public/patients? ______________________________________________________
Amount of patients seen per day? ____________________________________________________________
Are there enough toilets for the public/patients? Motivate your answer.
________________________________________________________________________________________________________________________________________________________________________________
________________________________________________________________________________________ ________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
Are hand-washing facilities available at the toilets? Yes No
Does the clinic have separate toilet facilities for the staff? Yes No
If YES, describe these facilities. Are hand-washing facilities available? ________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________ ________________________________________________________________________________________
________________________________________________________________________________________
Is clinic cleaning carried out daily? Yes No
Is the clinic in need of repairs or maintenance? Yes No
If YES, list the repairs or maintenance required. ________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________ ________________________________________________________________________________________
________________________________________________________________________________________
Describe the ventilation of the clinic. Is it compliant with the requirements?
29
MPOM 101 Service learning 2015 Page 29
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________ ________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________
Conclusions / comments on the clinic infrastructure
________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________
________________________________________________________________________________________
HEALTH CARE SERVICE PROVISION
Are the Batho Pele Principles displayed in the clinic? Yes No
Is the patient charter displayed in the clinic? Yes No
Is there a clear list of the services available posted in the Yes No
clinic?
If YES, are the times that the services are provided posted as well? Yes No
Is there a patient complaints mechanism in place at the clinic? Yes No
If YES, how are complaints handled?
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
Are waiting times at the clinic tracked periodically? Yes No
Is the facility accessible to disabled persons? Yes No
Does the clinic have at least one member of staff that has Yes No
completed a recognised PHC course?
Can any problem be seen at any time at the clinic? Yes No
(i.e. the supermarket approach)
Does the clinic have a visiting doctor? Yes No
Does the clinic make use of a standardised referral form for Yes No
patients being referred elsewhere?
If YES, what details are captured on the referral form?
________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________

30
MPOM 101 Service learning 2015 Page 30
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
How are patient records kept?
Hand written file Computer records
Patient retained record Other (Specify)
Does the clinic have a health committee with representatives Yes No
from the community?
If YES, who all serve on the committee?
________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________
Does the clinic make use of community health workers? Yes No
If YES, do these CHW receive in-service training Yes No
Is there privacy for consultations (auditory privacy)? Yes No
If not, describe: ________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________ ________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________
Is there privacy for examination (visual privacy)? Yes No
If not, describe:
________________________________________________________________________________________________________________________________________________________________________________
________________________________________________________________________________________ ________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
Is there privacy for the patients visiting the VCT/HIV/AIDS section? ________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________
Does the clinic make use of standard treatment guidelines? Yes No
If YES, are these guidelines (STGs) readily available for staff? Yes No
How is patient treatment statistics kept at the clinic?
31
MPOM 101 Service learning 2015 Page 31
Comments:
________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________
Is there a mechanism in place for reporting of notifiable Yes No
medical conditions.
If Yes, describe how this is done?
________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________
List the services that are provided by the clinic: What services, and when?
________________________________________________________________________________________________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________
________________________________________________________________________________________
Conclusions / Comments on health care provision
________________________________________________________________________________________________________________________________________________________________________________
________________________________________________________________________________________ ________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
HEALTH AND SAFETY
Is an organogram listing staff and duties available for the clinic? Yes No
Is there a copy of the Occupational Health and Safety Act in Yes No
the clinic?
Does the clinic have an occupational health and safety policy? Yes No
Has a risk assessment been done for all the clinic activities? Yes No
Do clinic staff get a pre-employment medical examination? Yes No
Is any form of medical surveillance carried out for occupational Yes No
diseases in staff?
Is a mechanism in place for the reporting of occupational Yes No
diseases and injuries?
If YES, describe the procedure.
Manual registers Electronic registers
Not kept Other (Specify)

32
MPOM 101 Service learning 2015 Page 32
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
Is there a plan available for clinic evacuation in case of a fire or Yes No
other hazardous situation?
Is personal protective equipment (PPE) such as gloves, masks Yes No
and goggles readily available for use by staff?
Does the clinic deal with TB patients? Yes No
If YES, what measures / precautions are taken to avoid transmission the disease to staff and other patients.
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
Are appropriate containers available for the disposal of medical Yes No
waste?
If YES, are the containers sealed and stored properly before Yes No
disposal?
How is medical waste disposed of at the clinic?
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
Is HIV post-exposure prophylaxis available at the clinic? Yes No
Conclusions / comments on health and safety.
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________ ________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________
Collected by medical waste Incinerated (in incinerator)
company Burnt on open fire
Buried Other (Specify)

33
MPOM 101 Service learning 2015 Page 33
9. STUDENT FEEDBACK AND REFLECTION
INTRODUCTION TO SERVICE LEARNING:
Group number: _____________
Community/Clinic visited: _______________________________________
Dates on which communities/clinics were visited: _______________________________________________
Were these visits worthwhile? (tick)
Give a rating mark for this CSL block or section of the block out of 10:
Mark to choose from
1 2 3 4 5 6 7 8 9 10
Mark given (tick)
Very poor mark
Excellent mark
List the 3 most important things that made the visits and learning successful:
a._________________________________________________________________________________________________________________________________________________________________________________________________________ b.___________________________________________________________________________________________________________________________________________ c.___________________________________________________________________________________________________________________________________________ What did not work? List the 3 biggest problems with these visits and learning.
a.___________________________________________________________________________________________________________________________________________ b.___________________________________________________________________________________________________________________________________________ c.______________________________________________________________________________
______________________________________________________________ How did you apply knowledge from previous lectures and/or textbooks in a practical way during this block?
__________________________________________________________________________________________________________________________________________________________________________________________
Yes No

34
MPOM 101 Service learning 2015 Page 34
____________________________________________________________________________________________________________________________ Did your team become stronger through the experience of working in the community – elaborate on your statement
__________________________________________________________________________________________________________________________________________________________________________________________ Has your presence in the community made a difference in terms of the growth/ development in this community – elaborate on your statement
__________________________________________________________________________________________________________________________________________________________________________________________ What problems did you face that may have awakened your curiosity or made you search for answers?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ How did this block prepare you for involvement in rural communities in future?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ Do you think you made a difference in your patients Health orientation and lifestyle – elaborate on your
statement
__________________________________________________________________________________________________________________________________________________________________________________________ What did you enjoy most?
__________________________________________________________________________________________________________________________________________________________________________________________ Have you any suggestions for the facilitators on how we could improve this experience for you as a student?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Student :
35
MPOM 101 Service learning 2015 Page 35
______________________________________ ________________________ Print Name and Surname Date
________________________________________ Signature
10. SERVICE LEARNING - REFLECTIVE DIARY Dear student For your learning to be really effective, you need to think a moment and reflect on what you have gained
from the learning experience (close the loops, so to say). Please therefore at the end of each day after you have visited a community/clinic (HIV block, Primary Health Care block, Introduction to SL block) think about
the visit and complete the following questions:
Student name and surname: ____________________________________________ Student number: _______________________ Group number: ________ Block: _______________________________ Block session and date: _______ What was my purpose in the community/clinic today?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ What have I learnt today that I did not know before? (You can reflect on new knowledge that you have
acquired, any new skills that you have learnt and applied competently, any values/beliefs that have
expanded your vision about yourself or medicine)
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ How did I live my social responsibility towards the community today? Or how have I behaved ethically and
professionally?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ What is the most important message I want to take home/back to campus?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

36
MPOM 101 Service learning 2015 Page 36
If the space provided is not enough, you are welcome to write at the back of this page. You are also
welcome to add photos or pictures in order to illustrate the points that you have made above.
11. CONCLUSION AND SUGGESTIONS
REGARDING THE BLOCK How did you apply knowledge from previous lectures and/or textbooks in a practical way during this block?
__________________________________________________________________________________________________________________________________________________________________________________________
How did your team become stronger through the experience of working in the community?
__________________________________________________________________________________________________________________________________________________________________________________________ How has your presence in the community made a difference in terms of the growth/ development in this
community?
__________________________________________________________________________________________________________________________________________________________________________________________ What problems did you face that may have awakened your curiosity or made you search for answers?
__________________________________________________________________________________________________________________________________________________________________________________________ How did this block prepare you for involvement in rural communities in future?
__________________________________________________________________________________________________________________________________________________________________________________________ What did you enjoy most?
____________________________________________________________________________________________________________________________ What frustrated you?
______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ Have you any suggestions for the facilitators on how we could improve this experience for you as a student?
______________________________________________________________

37
MPOM 101 Service learning 2015 Page 37
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ Student: ______________________________________ ________________________ Print Name and Surname Date ________________________________________ Signature
Learning Facilitator in charge: ______________________________________ ________________________ Print Name and Surname Date ________________________________________ Signature

38
MPOM 101 Service learning 2015 Page 38
12. CHECKLIST FOR HANDING IN POME 105
SL ASSIGNMENTS
ASPECTS TO BE INCLUDED Witness report as completed by your Mentor
Report on Health Education as completed by you and your group.
Remember to attach a copy of your poster / leaflet / Brochures and all other documents which you have used to develop and present your talk.
Community profile Power Point presentation (Print black and white copies of your power point
presentation, 2 slides per page) as developed by you and your group.
Electronic copy (CD) of Power Point presentation handed in at the POME office, together
with a hard copy Both clearly marked with the group number and student names
Log sheet of patient examinations at clinic. At least 4 documented patients as completed by
yourself with feedback from your mentor.
Report about Family living with Chronic disease as completed by yourself after having visited
your patient in his/her home.
Student Feedback form (you tell us what we can do to improve your learning) as completed by
yourself.
Clinic assessment form
All reports and feedback forms must be completed and filed in a learning portfolio on Service Learning and submitted to your Learning Facilitator on
the last Friday of the block.
Please hand in your reflective diaries to POME Administrative lady at the end
of the block. She will send a copy of your diary to your facilitator for note-taking and comments (if any). You will have to collect your original
reflection sheets from her again and file it in your portfolio on SL.
Good luck and enjoy! Debbie Barnard
39
MPOM 101 Service learning 2015 Page 39
See Blackboard for the SL lectures for POME 105 – information to be included in the examinations.