Moving The Bar in Upper GI Malignancies: A Review of Recent Upper Gastrointestinal Phase III Studies...
44
Moving The Bar in Upper GI Malignancies: A Review of Recent Upper Gastrointestinal Phase III Studies – Clinically Meaningful or Just Statistically Positive? Eileen M. O’Reilly, M.D. Associate Member, Associate Attending Memorial Sloan-Kettering Cancer Center Associate Professor Weill Medical College of Cornell University
-
Upload
bonnie-elliott -
Category
Documents
-
view
218 -
download
1
Transcript of Moving The Bar in Upper GI Malignancies: A Review of Recent Upper Gastrointestinal Phase III Studies...

Moving The Bar in Upper GI Malignancies: A Review of Recent Upper Gastrointestinal Phase III Studies – Clinically Meaningful or
Just Statistically Positive?
Eileen M. O’Reilly, M.D.Associate Member, Associate AttendingMemorial Sloan-Kettering Cancer Center
Associate ProfessorWeill Medical College of Cornell University

Three Perspectives
• Review of Recent Phase III Studies in Upper Gastrointestinal Malignancies– Eileen M. O’Reilly, M.D.
• Health Care Economics in Relation to Upper Gastrointestinal Cancers– Neal J. Meropol, M.D.
• Statistical Review of the benefit: Is it Meaningful?– Donna Niedzwicki, Ph.D.

Agenda/ Goals
• Discuss recent representative positive phase III studies in:– Gastric cancer– Pancreas neuroendocrine cancer– Pancreas adenocarcinoma
• Focus on trial design, results, application
• Cost, statistical considerations – co-speakers

Gastric Cancer
Example of clinically significant and statistically significant phase III trial with utility in a clearly defined patient subset

Rationale for Trastuzumab in Gastric Ca
• Her-2 – transmembrane receptor tyrosine kinase• 10-20% of GC, 20- 30% GE Jn ca are Her-2+• Trastuzumab
– Inhibits Her-2 signaling in Her-2+ tumors– Prevents Her-2 activation– Activates antibody-dependent cellular cytotoxicity
• Trastuzumab has benefit in Her-2 overexpressing GC cell lines and Her-2+ tumors in mice xenografts
Fujimoto, 2007. Gravolos, 2008. Kim, Int J Oncol, 2008. Kasprzyk, PG, Cancer Res, 1992

Bang, Y., et al. Lancet, 2010
ToGA Trial: Gastric CancerRandomized Phase III
Stratification₋ Location: Stomach vs GE junction₋ Measurable vs non-measurable₋ ECOG 0-1 vs 2₋ Fluropyrimidine: 5-FU (800mg/m2 IV d 1-5) vs capecitabine (1000mg/m2 PO BID d 1-14)
N= 3807 screened↓
N= 810 (22%)Her-2 Positive GC
↓N= 594 eligible
N= 294 FU + Cisplatin 80 mg/m2
x 6 cycles + Trastuzumab q 3wks
N= 290 FU + Cisplatin 80 mg/m2
x 6 cycles
RANDOMIZE

Bang, Y., et al. Lancet, 2010
ToGA Design & Endpoints
• Randomized, double-blind, placebo-controlled• Her-2 testing – central lab (Germany)
– Positive: IHC 3+ or FISH+ (> 2) in IHC 0, 1+ or 2+
• Primary endpoint: OS• Secondary endpoints: PFS, TTP, ORR, duration of response,
safety, QoL
• Biostatistical plan– Median OS 10 → 13 mths (HR 0.77)– α level 0.05, 80% power– N= 584

Bang, Y. Lancet, 2010
ToGA: Overall Survival (FISH+ or IHC3+)

Bang, Y. Lancet, 2010
ToGA: Progression-Free Survival

Bang, Y. Lancet, 2010
ToGA Survival: IHC 2+/FISH+ or IHC 3+(Post-hoc Exploratory Analysis)

Bang, Y. Lancet, 2010
Response Rate
CharacteristicF + C
N= 290F + C +
TrastuzumabN= 294
Complete response 2.4% 5.4%
Partial response 32% 42%
Overall response rate 34.5% 47.3%p= 0.0017

Toxicity: Non-Hematologic AE’s
Adverse eventF+C
N= 290F+C + Trastuzumab
N= 294
All Grade 3-4 All Grade 3-4
NauseaVomitingFatigueDiarrheaConstipationAstheniaStomatitisWeight decreaseAbdominal painCardiac AE’s
63%46%28%28%32%18%15%14%14%6%
7%8%2%4%2%3%2%2%1%3%
67%50%35%37%26%19%24%23%16%6%
7%6%4%9%
<1%4%
<1%2%1%1%
AEs occurring in >10% of patients

TOGA Trial: Quality of Life
• EORTC QLQ-C30, gastric cancer specific module STO22– Global health scores increased during and after
chemotherapy in both arms– Disease specific symptoms (dysphagia) improved
both arms– No negative impact in QoL for addition of
trastuzumab

Ruschoff, J. Virchows Arch, 2010
Summary Her-2 Targeting in Esophago-Gastric Cancer
• Her-2 validated target– Survival endpoint substantiated, clinically signficant
• Improved OS, PFS, RR, TTP, QoL, similar safety• Standardized scoring system• Better in high Her-2 expression (IHC 2+ /FISH+ IHC 3+)• Trastuzumab
– FDA approved for GC (10/ 2010): Her-2 overexpressing– EMEA approval: IHC3+ or IHC2+/FISH+– NICE (UK): IHC3+ only

Pancreas Neuroendocrine Tumors (PNET’s)
Examples of trials statistically challenging to design; full clinical impact remains to be seen but benefits appear meaningful

Pancreas Neuroendocrine Tumors (PNET’s)
• Rare malignancies– 1.3% of all pancreas malignancies– 2-4 per million– 1,000 yr new diagnoses US, rising incidence
• Variable natural history, median OS with metastases > 2 yrs
• FDA drug approvals– 1982 Streptozotocin (+/- 5FU, doxorubicin)– 1998 Somatostatin (symptomatic NET’s)
Yao, JC. Ann Surg Oncol, 2007. Moertel, CG. NEJM, 1980. Jensen, RT. Cancer, 2008

Everolimus (RAD001)
• mTOR serine-threonine kinase– Central regulator of protein synthesis– Autocrine activation via IGF-1 in PNET’s
• Antiproliferative effect on PNET cell lines by binding to FKBP-12
• Prior activity demonstrated in PNET’s
von Wichert, G. Cancer Res, 2000. Yao, JC. J Clin Oncol, 2008. Yao, JC. J Clin Oncol, 2010

Yao, JC. NEJM, 2011
RADIANT-3: Phase III Everolimus vs Placebo
Randomization 1: 1Stratification₋ Prior chemotherapy Y vs N₋ WHO performance status 0 vs 1-2Option for cross-over from placebo arm on POD
N= 410 PNET‘sWell-differentiated
Low-intermediate gradePOD within 12 mthsMeasurable disease
WHO performance 0-2N= 203 Placebo
N= 207 Everolimus 10mg daily
RANDOMIZE

Yao, CJ. NEJM, 2011
RADIANT-3 Design & Endpoints
• Randomized, double-blind, placebo-controlled• Primary endpoint: PFS
– Local, central, independent RECIST (1.0) reviews• Secondary endpoints:
– OS, ORR, duration response, safety
• Biostatistical plan– 33% reduction in risk of POD/death (HR 0.67)
prolonging mPFS from 6 → 9 mths– N= 282 progression-free events; 92.6% power, 1-sided
significance 2.5%, estimated 10% lost to follow-up– N= 392

Demographic Information
CharacteristicEverolimus
N= 207PlaceboN= 203
SexMale / Female 53% / 47% 58% / 42%
Age, years (median) 58 (23-87) 57 (20- 82)
Prior somatostatin (on study) ~50% (~40%) ~50% (~40%)
WHO performance status012
139 (67%)62 (30%)
6 (3%)
133 (66%)64 (32%)
6 (3%)
HistologyWell differentiatedModerately differentiated
170 (82%)35 (17%)
171 (84%)30 (15%)
Time from initial diagnosis > 2 yrs 118 (57%) 127 (63%)

Yao, JC. NEJM, 2011
RADIANT-3: PFS & Response
Characteristic EverolimusN= 207
PlaceboN= 203
PFS events (%) 109 (53%) 165 (81%)
Censored data (%) 98 (47%) 38 (19%)
Median PFS months 11 mths 4.6 mths
HR 0.35 (0.27- 0.45), p< 0.001
Median duration exposure 38 weeks 16 weeks
Response rate 5% 2%
Stable disease 73% 51%

Yao, JC. NEJM, 2011
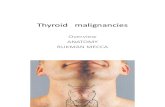
Progression-Free and Overall Survival and
Overall Survival.
Yao JC et al. N Engl J Med 2011;364:514-523.
Progression-Free Survival
Overall Survival

Yao, JC. NEJM, 2011
RADIANT-3: Toxicity
Adverse event, %
EverolimusN= 204
PlaceobN= 203
All Grade 3-4 All Grade 3-4
StomatitisRashDiarrheaFatigueInfectionsNauseaAnemiaLow plateletsPneumonitisHyperglycaemiaCough
131 (64%)99 (49%)69 (34%)64 (31%)46 (23%)41 (20%)35 (17%)27 (13%)35 (17%)27 (13%)22 (11%)
14 (7%)1 (<1%)7 (3%)5 (2%)5 (2%)5 (2%)
12 (6%)8 (4%)5 (2%)11 (5%)
-
34 (17%)21 (10%)20 (10%)29 (14%)12 (6%)
37 (18%)6 (3%)
1 (<1%)-
9 (4%)4 (2%)
---
1 (<1%)1 (<1%)
----
4 (2%)-
AEs occurring in >10% of patients

Everolimus in PNET’s
• 65% risk reduction in POD/(death)• Mostly grade 1-2 side effects• Mature survival data pending• Benefit in subpopulations (further data poster
discussion session 6/6)• Long-term use question• Combination therapy?

PNETs and Sunitinib
• PNET’s– Angiogenesis key role in development PNET’s– High VEGF expression correlated with poorer prognosis– Express PDGFR, c-KIT, VEGFR2, VEGFR3, EGF
• Sunitinib– Broad spectrum oral tyrosine kinase inhibitor
VEGFR 2, 3, c-kit, PDGF, FLT– Activity in preclinical model RIP1-Tag2 transgenic mouse model
of NET – decreased endothelial cell density, pericytes on vessels– Phase I, II clinical activity in NET’s observed
Couvelard, A. Br J Can, 2005. Zhang, J. Can, 2007. Pietras, K. J Clin Oncol, 2005. Faivre, S. J Clin Oncol, 2006. Kulke, MH. J Clin Oncol, 2008

Raymond, E. NEJM, 2011
Randomized Phase III Sunitinib vs PlaceboSUN 1111
Randomization 1: 1, balanced by country/regionNo other stratification factors used
N= 171 PNET‘s
Well-differentiatedPOD within 2-12 mthsMeasurable disease
ECOG performance 0-1 N= 85 Placebo
N= 86 Sunitinib 37.5 mg PO daily
RANDOMIZE

Raymond, E. NEJM, 2011
Phase III Sunitinib vs Placebo Design & Endpoints
• Randomized, double-blind, placebo-controlled• Primary endpoint: PFS• Secondary endpoints:
– ORR, duration response, OS, safety
• Biostatistical plan– N= 340 pts – 260 events, 90% power
50% increase PFS (placebo arm: 5.1 months)– 2-sided log-rank– Interim analysis after N= 130 events

Study Conduct
• 6/07- 4/09 N= 171 accrued from 42 centers, 11 countries
• 2/09 Data Safety Monitoring Committee– N= 154 accrued (340 planned)– Recommended discontinuation of trial
• High rate of progression (49 on placebo, 24 on sunitinib); deaths in control arm (15 on placebo, 5 on S)
• Delayed progression in sunitinib arm

Demographic Information
CharacteristicSunitinib
N= 86PlaceboN= 85
Sex, %Male / Female 49% / 51% 47% / 53%
Age, years (median) 56 (25-84) 57 (26-78)
ECOG performance status01
53 (62%)33 (38%)
41 (48%)43 (51%)
TumorNon-functioningFunctioning
42 (49%)25 (28%)
44 (52%)21 (24%)
Ki67 ≤ 5% (where available) 23 (63%) 20 (56%)Time from initial diagnosis
(median) 2.4 years 3.2 years

Raymond, E. NEJM, 2011
Sunitinib vs Placebo: Endpoints
CharacteristicSunitinib
N= 86PlaceboN= 85
PFS events (%) 30 (35%) 51 (60%)
Censored data (%) 56 (65%) 34 (40%)
Estimated median PFS 11.4 mths 5.5 mths
HR 0.42 (0.26- 0.66), p< 0.001
# Deaths at study termination 9 (10%) 21 (25%)
Censored data (%) 77 (90%) 64 (75%)
Median overall survival NR NR
Response rate (%) 8 (9%) - (0%)
Stable disease (%) 54 (63%) 51 (60%)

Raymond, E. NEJM, 2011
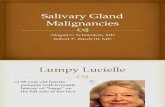
Overall Survival: Sunitinib vs Placebo1.0
0.8
0.6
0.4
0.2
0
Pro
po
rtio
n o
f p
atie
nts
0 5 10 15 20 25
86 60 38 16 3 085 61 33 12 3 0
Number at risk
SunitinibPlacebo
Time (months)
Sunitinib
Placebo
HR=0.42 (95% CI 0.19, 0.89)
P=0.02

Raymond, E. NEJM, 2011
Sunitinib vs Placebo: Toxicity
Adverse event
SunitinibN= 83
PlaceobN= 82
All Grade 3-4 All Grade 3-4
DiarrheaNauseaAstheniaVomitingFatigueNeutropeniaHypertensionHand-FootStomatitisRashPlatelets
49 (59%)37 (45%)28 (34%)28 (34%)27 (32%)24 (29%)22 (26%)19 (23%)18 (22%)15 (18%)14 (17%)
4 (5%)1 (1%)4 (5%)
-4 (5%)
10 (12%)14 (10%)
5 (6%)3 (4%)
-3 (4%)
32 (39%)24 (29%)25 (30%)29 (14%)22 (27%)
3 (4%)4 (5%)2 (2%)2 (2%)4 (5%)4 (5%)
2 (2%)1 (1%)3 (4%)2 (2%)7 (8%)
-1 (1%)
----
AEs occurring in >10% of patients

Summary: Sunitinib in PNET’s
• EMEA approved 12/10; FDA approved 05/11 • Concerns about study design
– Small trial, N= 171– Only 28% of 260 planned PFS events – inflated
effect?– Several unplanned analyses– High cross-over rate – Side effects of sunitinib

Integration of Therapy in PNET
• Everolimus, sunitinib – new options in rare malignancy• What’s the best time to start therapy?• Which therapy first?• Toxicity profile• How to sequence with other systemic/regional
treatment approaches?• Combination of targeted medications?• Role of systemic chemotherapy, e.g., temozolomide +
capecitabine

Pancreas Adenocarcinoma
Example of statistically significant phase III trial but clinically limited therapeutic impact

Moore, M. J Clin Oncol, 2007
NCI PA.3 Phase IIIGemcitabine/Erlotinib vs Gemcitabine/Placebo
Randomization 1: 1Stratification Locally advanced vs M1 Center PS 0-1 vs 2
N= 569 LA or M1 Untreated Pancreas Adenoca
N= 284 Gemcitabine + Placebo
N= 285 Gemcitabine + Erlotinib
(100mg, 150mg)
RANDOMIZE

PA.3 Study Design & Endpoints
• Randomized phase III, double-blind, placebo-controlled
• Primary: OS• Secondary: PFS, RR, duration response, safety,
QoL, correlative EGFR• Biostatistics
– Designed to detect HR 0.75– Minimum of 381 deaths, 80% power, 2-sided 5%– N= 450

CharacteristicG + Erlotinib
N= 285G + Placebo
N= 284
Median overall survival 6.24 mths 5.91 mths
HR. 0.82 (0.69- 0.99), p= 0.038
1-year overall survival 23% 17%Progression-free survival 3.75 mths 3.55 mths
HR 0.77 (0.64- 0.92), p= 0.004
Disease control rate 57.5% 49.2%
PA.3 Results
Moore, MJ. J Clin Oncol, 2007

Moore, MJ. J Clin Oncol, 2007
PA.3 Toxicity
Adverse event
G + ErlotinibN= 282
G + PlaceboN= 280
All Grade 3-4 All Grade 3-4
DiarrheaFatiguePneumonitisInfectionRashStomatitis
56%89%2.1%43%72%23%
6%15%
-17%6%
<1%
41%86%0.4%34%29%29%
2%15%
-16%1%1%
AEs occurring in >10% of patients

Moore, MJ. J Clin Oncol, 2007
Exploratory: Rash and Outcome

Miskad, R. J Clin Oncol, 2007
Summary: Gemcitabine + Erlotinib
• Solid rationale in pancreas adenoca• Statistically significant improved OS, PFS and disease
control• Targeted group – subset with ≥ grade 2 rash• FDA approval in 11/05• Concern relates to the clinical import of results
– Modest effect, higher rates of rash, diarrhea, infection, stomatitis
– Cost effectiveness analyses – limited value• Perspective of FOLFIRINOX

Gemcitabine
FOLFIRINOX
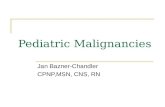
FOLFIRINOX vs Gemcitabine: Overall Survival
Number at riskGemcitabineFOLFIRINOX
171 134 89 48 28 14 7 6 3 3 2 2 2171 146 116 81 62 34 20 13 9 5 3 2 2
1 .0 0
0 .7 5
0 .5 0
0 .2 5
0 .0 0
Pr o
ba
bili
ty
M o n th s0 3 6 9 1 2 1 5 1 8 2 1 2 4 2 7 3 0 3 3 3 6
Median 11.1 mths
Median 6.8 mths
HR= 0.57P < 0.0001
Conroy TJ. NEJM, 2011

CharacteristicFOLFIRINOX
N= 171Gemcitabine
N= 171
Median survival 11.1 mths 6.8 mthsHR. 0.57 (0.45- 0.73), p< 0.001
1-Year overall survival 48% 21%Progression-free survival 6.4 mths 3.3 mths
HR 0.47 (0.37- 0.59), p< 0.001
Overall response rate 32% 9.4%Stable disease 39% 42%Rate of disease control 70% 51%
FOLFIRINOX vs Gemcitabine
Conroy, T. NEJM, 2011

Phase III Trials in Upper GI Malignancies:Clinically Meaningful or Statistically Significant?
• Practice changing results in some cases– Trastuzumab, FOLFIRINOX
• Statistically significant: Erlotinib• We don’t fully now yet: Everolimus, sunitinib • Drug approvals in rare diseases – PNET• New FDA precedent: PFS in diseases with long hx• Era of cost constraints: all agents palliative, all
expensive and all have added toxicity• Future – strength of rationale for agent, robustness
of earlier phase results, trial design