
Mortality After Ischemic Stroke in Patients With Acute Myocardial...
15
3050 P atients surviving an acute myocardial infarction (AMI) have an increased risk of stroke. 1–3 The risk of stroke after AMI is ≈0.9% to 1.4% during the hospital stay, 2.1% within 1 year, 1,2,4,5 and 5.7% within 4 years. 6 The most important risk factors for the occurrence of stroke are older age, diabetes mellitus, hypertension, prior stroke, heart failure, atrial fibril- lation, and coronary artery by-pass grafting. 1,4,7 Stroke after AMI is associated with an increased risk of death. One study found that patients with AMI that have a stroke have an increased risk of dying during hospitaliza- tion with an odds ratio of 4.3. 8 The short-term mortality rate (death in-hospital or during the 30-day follow-up) has been estimated to be 17.0% to 45.9%, whereas the long-term mor- tality rate (1.5–3.4 years after discharge) is estimated to be 16.9% to 27.9%. 2,4,7–10 There are several limitations to these estimates. Most previous studies did not analyze ischemic and hemorrhagic stroke separately, probably because of small sample sizes; however, hemorrhagic stroke is associ- ated with higher mortality compared with ischemic stroke. 11 One study found a 1-year mortality rate after hemorrhagic stroke of 71.8% in a selected population of patients with AMI treated with thrombolysis. 12 The risk of hemorrhagic stroke after AMI is closely related to the use of thrombolytic therapy, whereas ischemic stroke has other, partly unknown, mechanisms. It is, therefore, of interest to analyze ischemic stroke separately. Most studies describe short-term mortality, often using the duration of the hospital stay as the follow-up duration. However, the hospitalization period has decreased over time making comparisons between studies rather difficult. Moreover, the treatment of AMI has changed markedly during the past decade resulting in decreased mortality. It is unknown whether mortality after an AMI-associated stroke has changed as well. Only 1 previous study has presented a time trend of mortality after AMI-associated stroke. The results of that study suggested that the mortality increased from 1986 to 2005. However, the calculations were based on a few stroke cases making the conclusion unreliable. 2 Factors associated with increased or decreased mortality after an AMI-associated ischemic stroke remain unclear. Background and Purpose—Acute myocardial infarction (AMI) increases the risk of ischemic stroke, and mortality among these patients is high. Here, we aimed to estimate the 1-year mortality reliably after AMI complicated by ischemic stroke. We also aimed to identify trends over time for mortality during 1998–2008, as well as factors that predicted increased or decreased mortality. Methods—Data for 173 233 unselected patients with AMI were collected from the Swedish Register of Information and Knowledge about Swedish Heart Intensive Care Admissions registry for 1998–2008. Specifically, we analyzed 1-year follow-up and mortality data for patients with AMI with and without ischemic stroke. Kaplan–Meyer analysis was used to analyze mortality trends over time, and Cox regression analysis was used to identify uni- and multivariate predictors of mortality. Results—The 1-year mortality was 36.5% for AMI complicated by ischemic stroke and 18.3% for AMI without stroke. Mortality decreased over time in patients with and without ischemic stroke. The absolute decreases in mortality were 9.4% and 7.5%, respectively. Reperfusion and secondary preventive therapies were associated with a decreased mortality rate. Conclusions—Mortality after AMI complicated by an ischemic stroke is very high but decreased from 1998 to 2008. The increased use of evidence-based therapies explains the improved prognosis. (Stroke. 2013;44:3050-3055.) Key Words: mortality ◼ myocardial infarction ◼ risk factors ◼ stroke ◼ trends Mortality After Ischemic Stroke in Patients With Acute Myocardial Infarction Predictors and Trends Over Time in Sweden Anna Brammås; Stina Jakobsson; Anders Ulvenstam, MD; Thomas Mooe, MD, PhD Received March 12, 2013; final revision received July 13, 2013; accepted July 15, 2013. From the Department of Public Health and Clinical Medicine, Umeå University, Sweden (A.B., S.J., T.M.); and Department of Internal Medicine, Section of Cardiology, Östersund Hospital, Sweden (A.U., T.M.). The online-only Data Supplement is available with this article at http://stroke.ahajournals.org/lookup/suppl/doi:10.1161/STROKEAHA. 113.001434/-/DC1. Correspondence to Thomas Mooe, MD, PhD, Department of Internal Medicine, Section of Cardiology, Östersund Hospital, Östersunds sjukhus, Hus 10, Plan 5, 83183 Östersund, Sweden. E-mail [email protected] © 2013 American Heart Association, Inc. Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.113.001434 by guest on July 4, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on July 4, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on July 4, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on July 4, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on July 4, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on July 4, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on July 4, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on July 4, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on July 4, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on July 4, 2018 http://stroke.ahajournals.org/ Downloaded from
Transcript of Mortality After Ischemic Stroke in Patients With Acute Myocardial...

3050
Patients surviving an acute myocardial infarction (AMI) have an increased risk of stroke.1–3 The risk of stroke after
AMI is ≈0.9% to 1.4% during the hospital stay, 2.1% within 1 year,1,2,4,5 and 5.7% within 4 years.6 The most important risk factors for the occurrence of stroke are older age, diabetes mellitus, hypertension, prior stroke, heart failure, atrial fibril-lation, and coronary artery by-pass grafting.1,4,7
Stroke after AMI is associated with an increased risk of death. One study found that patients with AMI that have a stroke have an increased risk of dying during hospitaliza-tion with an odds ratio of 4.3.8 The short-term mortality rate (death in-hospital or during the 30-day follow-up) has been estimated to be 17.0% to 45.9%, whereas the long-term mor-tality rate (1.5–3.4 years after discharge) is estimated to be 16.9% to 27.9%.2,4,7–10 There are several limitations to these estimates. Most previous studies did not analyze ischemic and hemorrhagic stroke separately, probably because of small sample sizes; however, hemorrhagic stroke is associ-ated with higher mortality compared with ischemic stroke.11 One study found a 1-year mortality rate after hemorrhagic
stroke of 71.8% in a selected population of patients with AMI treated with thrombolysis.12 The risk of hemorrhagic stroke after AMI is closely related to the use of thrombolytic therapy, whereas ischemic stroke has other, partly unknown, mechanisms. It is, therefore, of interest to analyze ischemic stroke separately.
Most studies describe short-term mortality, often using the duration of the hospital stay as the follow-up duration. However, the hospitalization period has decreased over time making comparisons between studies rather difficult. Moreover, the treatment of AMI has changed markedly during the past decade resulting in decreased mortality. It is unknown whether mortality after an AMI-associated stroke has changed as well. Only 1 previous study has presented a time trend of mortality after AMI-associated stroke. The results of that study suggested that the mortality increased from 1986 to 2005. However, the calculations were based on a few stroke cases making the conclusion unreliable.2 Factors associated with increased or decreased mortality after an AMI-associated ischemic stroke remain unclear.
Background and Purpose—Acute myocardial infarction (AMI) increases the risk of ischemic stroke, and mortality among these patients is high. Here, we aimed to estimate the 1-year mortality reliably after AMI complicated by ischemic stroke. We also aimed to identify trends over time for mortality during 1998–2008, as well as factors that predicted increased or decreased mortality.
Methods—Data for 173 233 unselected patients with AMI were collected from the Swedish Register of Information and Knowledge about Swedish Heart Intensive Care Admissions registry for 1998–2008. Specifically, we analyzed 1-year follow-up and mortality data for patients with AMI with and without ischemic stroke. Kaplan–Meyer analysis was used to analyze mortality trends over time, and Cox regression analysis was used to identify uni- and multivariate predictors of mortality.
Results—The 1-year mortality was 36.5% for AMI complicated by ischemic stroke and 18.3% for AMI without stroke. Mortality decreased over time in patients with and without ischemic stroke. The absolute decreases in mortality were 9.4% and 7.5%, respectively. Reperfusion and secondary preventive therapies were associated with a decreased mortality rate.
Conclusions—Mortality after AMI complicated by an ischemic stroke is very high but decreased from 1998 to 2008. The increased use of evidence-based therapies explains the improved prognosis. (Stroke. 2013;44:3050-3055.)
Key Words: mortality ◼ myocardial infarction ◼ risk factors ◼ stroke ◼ trends
Mortality After Ischemic Stroke in Patients With Acute Myocardial Infarction
Predictors and Trends Over Time in Sweden
Anna Brammås; Stina Jakobsson; Anders Ulvenstam, MD; Thomas Mooe, MD, PhD
Received March 12, 2013; final revision received July 13, 2013; accepted July 15, 2013.From the Department of Public Health and Clinical Medicine, Umeå University, Sweden (A.B., S.J., T.M.); and Department of Internal Medicine,
Section of Cardiology, Östersund Hospital, Sweden (A.U., T.M.).The online-only Data Supplement is available with this article at http://stroke.ahajournals.org/lookup/suppl/doi:10.1161/STROKEAHA.
113.001434/-/DC1.Correspondence to Thomas Mooe, MD, PhD, Department of Internal Medicine, Section of Cardiology, Östersund Hospital, Östersunds sjukhus, Hus 10,
Plan 5, 83183 Östersund, Sweden. E-mail [email protected]© 2013 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.113.001434
by guest on July 4, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on July 4, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on July 4, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on July 4, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on July 4, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on July 4, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on July 4, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on July 4, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on July 4, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on July 4, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Brammås et al Mortality After MI-Associated Ischemic Stroke 3051
In the present study, our primary aim was to determine the mortality rate associated with ischemic stroke during the first year after an AMI. Second, we wished to identify trends in mortality during the 1998–2008 period and to identify fac-tors associated with increased or decreased risk of death after AMI-associated ischemic stroke.
Materials and MethodsPatient data were obtained from the Swedish Web-system for Enhancement and Development of Evidence-based Care in Heart Disease Evaluated According to Recommended Therapies (SWEDEHEART) that includes Register of Information and Knowledge about Swedish Heart Intensive Care Admissions (RIKS-HIA), a national quality register of all patients admitted to a coro-nary care unit in Swedish hospitals. Patient data are reported on case record forms that include >100 variables; information is recorded on hospital admission, while the patient is in-hospital and at dis-charge. These records include patient demographics, risk factors, medical history, biochemical markers, discharge diagnosis, and discharge medications. The validity of the entered data is examined annually and shows 93% to 97% conformity between the Register of Information and Knowledge about Swedish Heart Intensive Care Admissions data and patient records. In 2008, 74 of 74 hospitals with coronary care units participated, covering >95% of Swedish coronary care units admissions, when compared with the Swedish National Patient Register.13 We collected data from patients with the index AMI during 1998–2008 with follow-up until 2009; this included a total of 173 233 patients.
We combined data from Register of Information and Knowledge about Swedish Heart Intensive Care Admissions with data from the National Patient Register to identify patients with ischemic stroke and to identify all causes of death. The National Patient Register includes dates for admission and discharge as well as diagnoses at discharge for all hospital stays in Sweden. The International Classification of Diseases-Ninth Revision (433 and 434) and International
Classification of Diseases-Tenth Revision (I63 and I64) codes for ce-rebral infarction were used. The National Patient Register has been validated and a diagnosis of stroke or transient ischemic attack has a positive predictive value of 98.6%.14 Both registers are based on the entire population in Sweden. There were no criteria for exclusion.
Patients were registered from 1998 to 2008 at the time of their in-dex AMI. The follow-up time for the major outcomes ischemic stroke and death was 1 year from AMI admission.
All patients for whom data were entered into the Register of Information and Knowledge about Swedish Heart Intensive Care Admissions were informed of their participation in the registry (patients could request to be excluded from the registry) and the long-term follow-up. The registry was approved by the National Board of Health and Welfare and the Swedish Data Inspection Board. The merging of registries was approved by the local ethics committee.
The variable “heart failure during hospitalization” was defined as the occurrence of pulmonary rales or treatment with intravenous di-uretics during hospitalization. The variable “smoking” was defined as smoking within the past month. “Atrial fibrillation” includes patients with atrial fibrillation (all types) before or during hospitalization.
Statistical AnalysisThe study period was divided into 5 time periods (1998–2000, 2001–2002, 2003–2004, 2005–2006, and 2007–2008) to study changes over time. The results are presented as mean values for continuous variables and as percentages for categorical variables. Comparisons between patient groups were performed using the Mann–Whitney U test for continuous variables and the χ2 test for categorical variables.
Kaplan–Meyer curves were calculated for the occurrence of death during the 5 different time periods and compared between groups us-ing the log-rank test. Uni- and multivariable predictors of risks were assessed using Cox proportional hazards regression analysis. The end point was defined as death within 1 year from admission to hos-pital for AMI. For our multivariable model, we used previously es-tablished predictors of risk for death and added the factors from our
Table 1. Characteristics of Patients With AMI (N=173 233) With and Without Ischemic Stroke Stratified by Survival
Variable
Ischemic Stroke Ischemic Stroke and Death No Ischemic Stroke No Ischemic Stroke and Death
n=4561 n=2624 n=135 587 n=30 461
Women, % 41.4 48.2 34.8 43.7
Age (mean) 74.8 79.6 69.1 79.2
Comorbidities, %
Prior ischemic stroke 21.8 26.0 6.2 15.3
Prior AMI 18.2 23.4 13.4 25.4
Prior heart failure 13.3 22.1 8.3 27.1
Diabetes mellitus 24.5 27.8 17.7 25.1
Prior kidney failure 1.7 3.0 1.5 5.7
Atrial fibrillation 26.2 34.8 12.7 27.8
Smoking 17.7 13.6 23.8 14.0
Clinical characteristics
Systolic blood pressure (mean) 150.1n=1971
145.5n=997
147.3n=62042
132.4n=11580
STEMI, % 34.0 31.2 36.5 31.4
Heart failure during hospitalization, % 41.6 60.1 28.2 63.5
Treatment in-hospital, %
Acute CABG 0.4 0.2 0.2 0.2
PCI 10.3 6.3 16.0 5.7
Thrombolysis 13.8 11.7 16.0 13.8
AMI indicates acute myocardial infarction; CABG, coronary artery by-pass grafting; PCI, percutaneous coronary intervention; and STEMI, ST-segment–elevation myocardial infarction.
by guest on July 4, 2018http://stroke.ahajournals.org/
Dow
nloaded from
3052 Stroke November 2013
univariable analysis. Patients who died during hospitalization were excluded from the analysis when variables on treatment at discharge were included. We excluded variables from the multivariable analy-ses that had <90% valid cases (body mass index, habitual smoking, heart rate, systolic blood pressure, diastolic blood pressure, plasma cholesterol, plasma low-density lipoprotein, plasma glucose, and the use of AT2-inhibitors at discharge). A P value <0.05 was considered significant. All statistical analyses were performed using SPSS ver-sion 20.0 software.
ResultsThis study included 173 233 patients with AMI from 1998 to 2008. The patients had a mean age of 71.2 years, and 36.8% were women. The patient characteristics are shown in Table 1. Of the 173 233 patients with AMI, 7185 (4.1%) had an isch-emic stroke within 1 year of AMI and 2624 (36.5%) of these patients died during that year. Of the patients that did not have ischemic stroke in the year after AMI, 30 461 (18.3%) died. Overall, patients with ischemic stroke were older and had more comorbidities; this was also true for the patients who died during the first year after AMI.
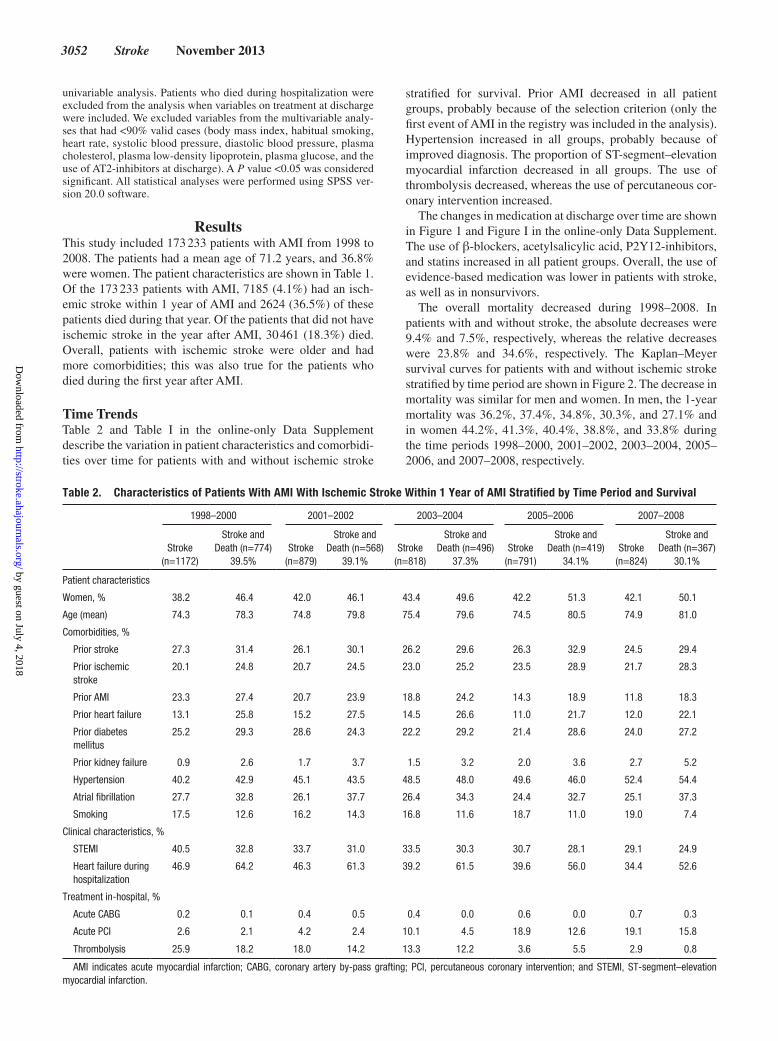
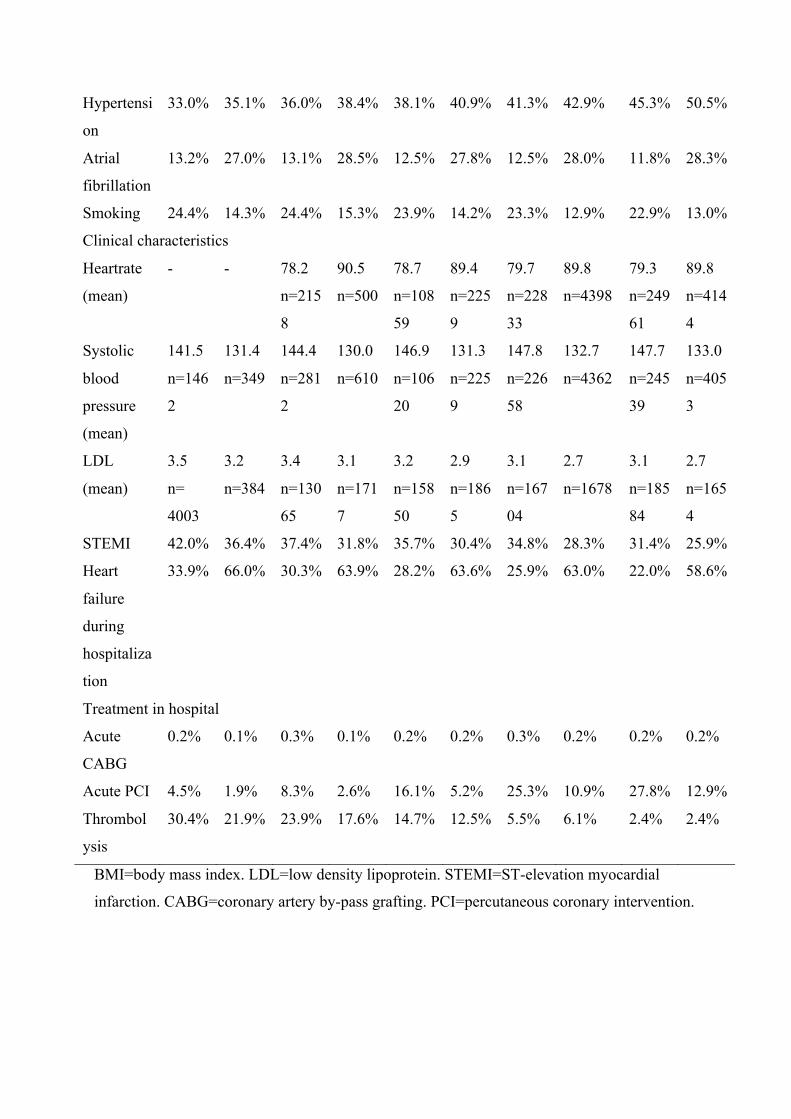
Time TrendsTable 2 and Table I in the online-only Data Supplement describe the variation in patient characteristics and comorbidi-ties over time for patients with and without ischemic stroke
stratified for survival. Prior AMI decreased in all patient groups, probably because of the selection criterion (only the first event of AMI in the registry was included in the analysis). Hypertension increased in all groups, probably because of improved diagnosis. The proportion of ST-segment–elevation myocardial infarction decreased in all groups. The use of thrombolysis decreased, whereas the use of percutaneous cor-onary intervention increased.
The changes in medication at discharge over time are shown in Figure 1 and Figure I in the online-only Data Supplement. The use of β-blockers, acetylsalicylic acid, P2Y12-inhibitors, and statins increased in all patient groups. Overall, the use of evidence-based medication was lower in patients with stroke, as well as in nonsurvivors.
The overall mortality decreased during 1998–2008. In patients with and without stroke, the absolute decreases were 9.4% and 7.5%, respectively, whereas the relative decreases were 23.8% and 34.6%, respectively. The Kaplan–Meyer survival curves for patients with and without ischemic stroke stratified by time period are shown in Figure 2. The decrease in mortality was similar for men and women. In men, the 1-year mortality was 36.2%, 37.4%, 34.8%, 30.3%, and 27.1% and in women 44.2%, 41.3%, 40.4%, 38.8%, and 33.8% during the time periods 1998–2000, 2001–2002, 2003–2004, 2005–2006, and 2007–2008, respectively.
Table 2. Characteristics of Patients With AMI With Ischemic Stroke Within 1 Year of AMI Stratified by Time Period and Survival
1998–2000 2001–2002 2003–2004 2005–2006 2007–2008
Stroke (n=1172)
Stroke and Death (n=774)
39.5%Stroke
(n=879)
Stroke and Death (n=568)
39.1%Stroke
(n=818)
Stroke and Death (n=496)
37.3%Stroke
(n=791)
Stroke and Death (n=419)
34.1%Stroke
(n=824)
Stroke and Death (n=367)
30.1%
Patient characteristics
Women, % 38.2 46.4 42.0 46.1 43.4 49.6 42.2 51.3 42.1 50.1
Age (mean) 74.3 78.3 74.8 79.8 75.4 79.6 74.5 80.5 74.9 81.0
Comorbidities, %
Prior stroke 27.3 31.4 26.1 30.1 26.2 29.6 26.3 32.9 24.5 29.4
Prior ischemic stroke
20.1 24.8 20.7 24.5 23.0 25.2 23.5 28.9 21.7 28.3
Prior AMI 23.3 27.4 20.7 23.9 18.8 24.2 14.3 18.9 11.8 18.3
Prior heart failure 13.1 25.8 15.2 27.5 14.5 26.6 11.0 21.7 12.0 22.1
Prior diabetes mellitus
25.2 29.3 28.6 24.3 22.2 29.2 21.4 28.6 24.0 27.2
Prior kidney failure 0.9 2.6 1.7 3.7 1.5 3.2 2.0 3.6 2.7 5.2
Hypertension 40.2 42.9 45.1 43.5 48.5 48.0 49.6 46.0 52.4 54.4
Atrial fibrillation 27.7 32.8 26.1 37.7 26.4 34.3 24.4 32.7 25.1 37.3
Smoking 17.5 12.6 16.2 14.3 16.8 11.6 18.7 11.0 19.0 7.4
Clinical characteristics, %
STEMI 40.5 32.8 33.7 31.0 33.5 30.3 30.7 28.1 29.1 24.9
Heart failure during hospitalization
46.9 64.2 46.3 61.3 39.2 61.5 39.6 56.0 34.4 52.6
Treatment in-hospital, %
Acute CABG 0.2 0.1 0.4 0.5 0.4 0.0 0.6 0.0 0.7 0.3
Acute PCI 2.6 2.1 4.2 2.4 10.1 4.5 18.9 12.6 19.1 15.8
Thrombolysis 25.9 18.2 18.0 14.2 13.3 12.2 3.6 5.5 2.9 0.8
AMI indicates acute myocardial infarction; CABG, coronary artery by-pass grafting; PCI, percutaneous coronary intervention; and STEMI, ST-segment–elevation myocardial infarction.
by guest on July 4, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Brammås et al Mortality After MI-Associated Ischemic Stroke 3053
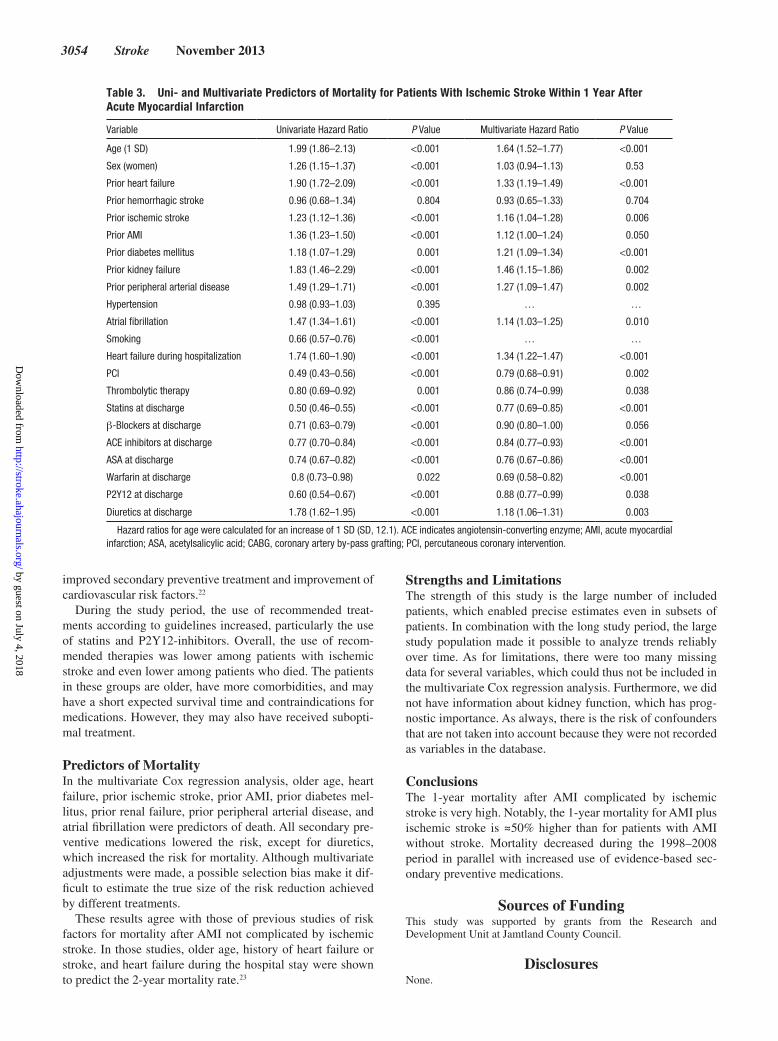
Predictors of Mortality After Ischemic StrokeTable 3 shows the results of the Cox regression analy-ses in patients who had an ischemic stroke after AMI. Heart failure, renal disease, peripheral arterial disease, and diabetes mellitus had the strongest association with death. Evidence-based treatments were associated with a decreased risk of death. Diuretic use was associated with an increased risk of death. Table II in the online-only Data Supplement shows the corresponding analyses for patients without ischemic stroke.
DiscussionThis is the first study with an adequate size and duration of follow-up to assess trends over time and predictors of mor-tality after AMI-associated ischemic stroke reliably. The main findings were as follows: first, the mortality after AMI-associated ischemic stroke decreased during the 1998–2008 period. Second, patients with an AMI-associated ischemic
stroke have an absolute mortality rate during the first year after the AMI that is 16% to 19% higher than the mortal-ity rate of those without ischemic stroke. Third, evidence-based treatments are associated with decreased mortality in an adjusted analysis.
The large number of patients in this study allowed us to make a reliable estimate of the mortality in this fairly unselected population. The 1-year mortality of 36.5% was only slightly higher than in most previous studies of short-term mortality (in-hospital and 30 days).2,4,7,8 Most studies have not separated ischemic and hemorrhagic stroke, which causes a higher mor-tality estimate. The mortality, as well as the risk of stroke, rap-idly declines after an AMI, which can explain the rather low difference between 30-day and 1-year mortality.3,5 We did not subclassify stroke events because ischemic strokes occurring after AMI are generally classified as cardioembolic. This clas-sification can be questioned because other mechanisms may be more important than embolism.15
We found that mortality decreased during the 1998–2008 period, both in patients with and without an ischemic stroke after AMI. The relative risk reduction was larger in the popu-lation without ischemic stroke, whereas the absolute decrease was slightly greater for patients with stroke. There was a simi-lar decrease in mortality in men and in women with stroke, but the women had a higher mortality during the study period. There is only 1 previous study, by Saczynski et al,2 that reported results for a time trend of mortality after stroke fol-lowing an AMI. On the basis of 132 stroke cases and 43 deaths during 1986–2005, the authors suggested that the mortality after stroke has increased. However, a reliable time trend can-not be based on such a small patient population.
The present results are in agreement with earlier stud-ies of mortality after stroke without a previous AMI, which show a decreasing mortality even though time periods and populations differ.16–19 There are probably several explana-tions for the decrease in mortality. Some studies have shown that specific stroke units have improved the prognosis of patients with stroke,19,20 and the 30-day mortality is lower for patients admitted to a stroke unit.21 Other explanations include
Figure 1. Time trends for discharge medication use (%) for patients with acute myocardial infarction with ischemic stroke who have survived (solid line) or died (broken line). ACE indicates angiotensin-converting enzyme; and ASA, acetylsalicylic acid.
Figure 2. Cumulative survival for patients with (left) and without (right) ischemic stroke within 1 year after acute myocardial infarction stratified by time period.
by guest on July 4, 2018http://stroke.ahajournals.org/
Dow
nloaded from
3054 Stroke November 2013
improved secondary preventive treatment and improvement of cardiovascular risk factors.22
During the study period, the use of recommended treat-ments according to guidelines increased, particularly the use of statins and P2Y12-inhibitors. Overall, the use of recom-mended therapies was lower among patients with ischemic stroke and even lower among patients who died. The patients in these groups are older, have more comorbidities, and may have a short expected survival time and contraindications for medications. However, they may also have received subopti-mal treatment.
Predictors of MortalityIn the multivariate Cox regression analysis, older age, heart failure, prior ischemic stroke, prior AMI, prior diabetes mel-litus, prior renal failure, prior peripheral arterial disease, and atrial fibrillation were predictors of death. All secondary pre-ventive medications lowered the risk, except for diuretics, which increased the risk for mortality. Although multivariate adjustments were made, a possible selection bias make it dif-ficult to estimate the true size of the risk reduction achieved by different treatments.
These results agree with those of previous studies of risk factors for mortality after AMI not complicated by ischemic stroke. In those studies, older age, history of heart failure or stroke, and heart failure during the hospital stay were shown to predict the 2-year mortality rate.23
Strengths and LimitationsThe strength of this study is the large number of included patients, which enabled precise estimates even in subsets of patients. In combination with the long study period, the large study population made it possible to analyze trends reliably over time. As for limitations, there were too many missing data for several variables, which could thus not be included in the multivariate Cox regression analysis. Furthermore, we did not have information about kidney function, which has prog-nostic importance. As always, there is the risk of confounders that are not taken into account because they were not recorded as variables in the database.
ConclusionsThe 1-year mortality after AMI complicated by ischemic stroke is very high. Notably, the 1-year mortality for AMI plus ischemic stroke is ≈50% higher than for patients with AMI without stroke. Mortality decreased during the 1998–2008 period in parallel with increased use of evidence-based sec-ondary preventive medications.
Sources of FundingThis study was supported by grants from the Research and Development Unit at Jamtland County Council.
DisclosuresNone.
Table 3. Uni- and Multivariate Predictors of Mortality for Patients With Ischemic Stroke Within 1 Year After Acute Myocardial Infarction
Variable Univariate Hazard Ratio P Value Multivariate Hazard Ratio P Value
Age (1 SD) 1.99 (1.86–2.13) <0.001 1.64 (1.52–1.77) <0.001
Sex (women) 1.26 (1.15–1.37) <0.001 1.03 (0.94–1.13) 0.53
Prior heart failure 1.90 (1.72–2.09) <0.001 1.33 (1.19–1.49) <0.001
Prior hemorrhagic stroke 0.96 (0.68–1.34) 0.804 0.93 (0.65–1.33) 0.704
Prior ischemic stroke 1.23 (1.12–1.36) <0.001 1.16 (1.04–1.28) 0.006
Prior AMI 1.36 (1.23–1.50) <0.001 1.12 (1.00–1.24) 0.050
Prior diabetes mellitus 1.18 (1.07–1.29) 0.001 1.21 (1.09–1.34) <0.001
Prior kidney failure 1.83 (1.46–2.29) <0.001 1.46 (1.15–1.86) 0.002
Prior peripheral arterial disease 1.49 (1.29–1.71) <0.001 1.27 (1.09–1.47) 0.002
Hypertension 0.98 (0.93–1.03) 0.395 … …
Atrial fibrillation 1.47 (1.34–1.61) <0.001 1.14 (1.03–1.25) 0.010
Smoking 0.66 (0.57–0.76) <0.001 … …
Heart failure during hospitalization 1.74 (1.60–1.90) <0.001 1.34 (1.22–1.47) <0.001
PCI 0.49 (0.43–0.56) <0.001 0.79 (0.68–0.91) 0.002
Thrombolytic therapy 0.80 (0.69–0.92) 0.001 0.86 (0.74–0.99) 0.038
Statins at discharge 0.50 (0.46–0.55) <0.001 0.77 (0.69–0.85) <0.001
β-Blockers at discharge 0.71 (0.63–0.79) <0.001 0.90 (0.80–1.00) 0.056
ACE inhibitors at discharge 0.77 (0.70–0.84) <0.001 0.84 (0.77–0.93) <0.001
ASA at discharge 0.74 (0.67–0.82) <0.001 0.76 (0.67–0.86) <0.001
Warfarin at discharge 0.8 (0.73–0.98) 0.022 0.69 (0.58–0.82) <0.001
P2Y12 at discharge 0.60 (0.54–0.67) <0.001 0.88 (0.77–0.99) 0.038
Diuretics at discharge 1.78 (1.62–1.95) <0.001 1.18 (1.06–1.31) 0.003
Hazard ratios for age were calculated for an increase of 1 SD (SD, 12.1). ACE indicates angiotensin-converting enzyme; AMI, acute myocardial infarction; ASA, acetylsalicylic acid; CABG, coronary artery by-pass grafting; PCI, percutaneous coronary intervention.
by guest on July 4, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Brammås et al Mortality After MI-Associated Ischemic Stroke 3055
References 1. Witt BJ, Ballman KV, Brown RD Jr, Meverden RA, Jacobsen SJ, Roger
VL. The incidence of stroke after myocardial infarction: a meta-analysis. Am J Med. 2006;119:354.e1–354.e9.
2. Saczynski JS, Spencer FA, Gore JM, Gurwitz JH, Yarzebski J, Lessard D, et al. Twenty-year trends in the incidence of stroke complicating acute myocardial infarction: Worcester Heart Attack Study. Arch Intern Med. 2008;168:2104–2110.
3. Witt BJ, Brown RD Jr, Jacobsen SJ, Weston SA, Yawn BP, Roger VL. A community-based study of stroke incidence after myocardial infarction. Ann Intern Med. 2005;143:785–792.
4. Budaj A, Flasinska K, Gore JM, Anderson FA Jr, Dabbous OH, Spencer FA, et al.; GRACE Investigators. Magnitude of and risk factors for in-hospital and postdischarge stroke in patients with acute coronary syn-dromes: findings from a Global Registry of Acute Coronary Events. Circulation. 2005;111:3242–3247.
5. Mooe T, Olofsson BO, Stegmayr B, Eriksson P. Ischemic stroke. Impact of a recent myocardial infarction. Stroke. 1999;30:997–1001.
6. Udell JA, Wang JT, Gladstone DJ, Tu JV. Anticoagulation after anterior myocardial infarction and the risk of stroke. PLoS One. 2010;5:e12150.
7. Mahaffey KW, Harrington RA, Simoons ML, Granger CB, Graffagnino C, Alberts MJ, et al. Stroke in patients with acute coronary syndromes: incidence and outcomes in the platelet glycoprotein IIb/IIIa in unstable angina. Receptor suppression using integrilin therapy (PURSUIT) trial. The PURSUIT Investigators. Circulation. 1999;99:2371–2377.
8. Spencer FA, Gore JM, Yarzebski J, Lessard D, Jackson EA, Goldberg RJ. Trends (1986 to 1999) in the incidence and outcomes of in-hospital stroke complicating acute myocardial infarction (The Worcester Heart Attack Study). Am J Cardiol. 2003;92:383–388.
9. Wienbergen H, Schiele R, Gitt AK, Schneider S, Heer T, Gottwik M et al. Incidence, risk factors, and clinical outcome of stroke after acute myocardial infarction in clinical practice. Mir and mitra study groups. Myocardial infarction registry. Maximal individual therapy in acute myocardial infarction. Am J Cardiol. 2001;87:782–785, A788
10. Kaplan RC, Heckbert SR, Furberg CD, Psaty BM. Predictors of subse-quent coronary events, stroke, and death among survivors of first hospi-talized myocardial infarction. J Clin Epidemiol. 2002;55:654–664.
11. Xian Y, Holloway RG, Pan W, Peterson ED. Challenges in assessing hospital-level stroke mortality as a quality measure: comparison of isch-emic, intracerebral hemorrhage, and total stroke mortality rates. Stroke. 2012;43:1687–1690.
12. Giugliano RP, Giraldez RR, Morrow DA, Antman EM, Gibson CM, Mohanavelu S, et al. Relations between bleeding and outcomes in patients with ST-elevation myocardial infarction in the ExTRACT-TIMI 25 trial. Eur Heart J. 2010;31:2103–2110.
13. Jernberg T, Attebring MF, Hambraeus K, Ivert T, James S, Jeppsson A, et al. The Swedish Web-system for enhancement and development of evi-dence-based care in heart disease evaluated according to recommended therapies (SWEDEHEART). Heart. 2010;96:1617–1621.
14. Ludvigsson JF, Andersson E, Ekbom A, Feychting M, Kim JL, Reuterwall C, et al. External review and validation of the Swedish national inpatient register. BMC Public Health. 2011;11:450.
15. Mooe T. Risk, mechanisms and prevention of stroke after an acute myo-cardial infarction. Expert Rev Neurother. 2002;2:177–186.
16. Arboix A, Cendrós V, Besa M, García-Eroles L, Oliveres M, Targa C, et al. Trends in risk factors, stroke subtypes and outcome. Nineteen-year data from the Sagrat Cor Hospital of Barcelona stroke registry. Cerebrovasc Dis. 2008;26:509–516.
17. Rautio A, Eliasson M, Stegmayr B. Favorable trends in the incidence and outcome in stroke in nondiabetic and diabetic subjects: findings from the Northern Sweden MONICA Stroke Registry in 1985 to 2003. Stroke. 2008;39:3137–3144.
18. Sturgeon JD, Folsom AR. Trends in hospitalization rate, hospital case fatality, and mortality rate of stroke by subtype in Minneapolis-St. Paul, 1980-2002. Neuroepidemiology. 2007;28:39–45.
19. Lee LK, Bateman BT, Wang S, Schumacher HC, Pile-Spellman J, Saposnik G. Trends in the hospitalization of ischemic stroke in the United States, 1998-2007. Int J Stroke. 2012;7:195–201.
20. Eriksson M, Carlberg B, Eliasson M. The disparity in long-term sur-vival after a first stroke in patients with and without diabetes per-sists: the Northern Sweden MONICA study. Cerebrovasc Dis. 2012;34:153–160.
21. Xian Y, Holloway RG, Chan PS, Noyes K, Shah MN, Ting HH, et al. Association between stroke center hospitalization for acute ischemic stroke and mortality. JAMA. 2011;305:373–380.
22. Eriksson M, Holmgren L, Janlert U, Jansson JH, Lundblad D, Stegmayr B, et al. Large improvements in major cardiovascular risk factors in the population of northern Sweden: the MONICA study 1986-2009. J Intern Med. 2011;269:219–231.
23. Coles AH, Fisher KA, Darling C, McManus D, Maitas O, Yarzebski J, et al. Recent trends in post-discharge mortality among patients with an initial acute myocardial infarction. Am J Cardiol. 2012;110: 1073–1077.
by guest on July 4, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Anna Brammås, Stina Jakobsson, Anders Ulvenstam and Thomas Mooeand Trends Over Time in Sweden
Mortality After Ischemic Stroke in Patients With Acute Myocardial Infarction: Predictors
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2013 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/STROKEAHA.113.001434
2013;44:3050-3055; originally published online August 20, 2013;Stroke.
http://stroke.ahajournals.org/content/44/11/3050World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org/content/suppl/2013/08/20/STROKEAHA.113.001434.DC1Data Supplement (unedited) at:
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on July 4, 2018http://stroke.ahajournals.org/
Dow
nloaded from

ONLINE SUPPLEMENT
Mortality after ischemic stroke in patients with acute myocardial
infarction: Predictors and trends over time in Sweden
Anna Brammås1, Stina Jakobsson2, Anders Ulvenstam3, Thomas Mooe4
1Medical student, Department of Public Health and Clinical Medicine, Umeå University,
Sweden
2Medical student, Department of Public Health and Clinical Medicine, Umeå University,
Sweden
3MD, Department of Internal Medicine, Section of Cardiology, Östersund Hospital, Sweden
4MD, Ass Prof, Department of Public Health and Clinical Medicine, Umeå University and
Department of Internal Medicine, Section of Cardiology, Östersund Hospital, Sweden
Correspondence to:
Thomas Mooe; Östersunds sjukhus; Hus 10, Plan5; 83183 Östersund; Sweden
Phone: +46706400778, Fax: +4663153030, E-mail: [email protected]

Supplemental methods- Explanation of used registers
The Swedish Web-system for Enhancement and Developmend of Evidence-based care in Heart disease Evaluated According to Recommended Therapies (SWEDEHEART)
SWEDEHEART is a Swedish national registry of patients admitted to hospital for acute coronary syndrome (ACS) or undergoing coronary or valvular intervention. About 80 000 patients is registred each year, of which 20 000 with myocardial infarction (MI). The coverage is about 60% for all ACS cases and almost 100% for ACS cases admitted to a coronary care unit.1
At admission, information for 106 variables is collected such as risk factors, past medical history, medical treatment in hospital etc. Patients with MI and younger than 75 years is followed up after 6-10 weeks and after 12-14 months for collection of information for another 75 variables about for example smoking habits, blood pressure and lipid levels.
Every year SWEDEHEART is merged with the National Cause of Death register (including information about the vital status of all Swedes), with the National Patient Registry (including diagnoses at discharge for all hospital stays in Sweden), and with the National Registry of Drug prescriptions.
Register of Information and Knowledge About Swedish Heart Intensive Care Admissions (RIKS- HIA)
RIKS-HIA is a part of SWEDEHEART collecting information about acute cardiac care, and was started as a national quality register in 1995. RIKS-HIA was reviewed in 2007 with a 96.1% (92.6-97.4%) variable agreement when collected variables were compared to patient records.
National Patient Registry (NPR)
NPR includes different registers, of which we have used the Swedish National Inpatient Register (IPR). IPR was started in 1964 and has a complete national coverage since 1987. More than 99% of hospital discharges are registered. Diagnoses are coded according to the International Classification of Disease (ICD).2 IPR has a good coverage for diagnoses as Myocardial infarction (91.5%).3
1. Jernberg T, Attebring MF, Hambraeus K, Ivert T, James S, Jeppsson A et al. The swedish web-system for enhancement and development of evidence-based care in heart disease evaluated according to recommended therapies (swedeheart). Heart. 2010;96:1617-1621
2. Ludvigsson JF, Andersson E, Ekbom A, Feychting M, Kim JL, Reuterwall C et al. External review and validation of the swedish national inpatient register. BMC Public Health. 2011;11:450
3. Elo SL, Karlberg IH. Validity and utilization of epidemiological data: A study of ischaemic heart disease and coronary risk factors in a local population. Public Health. 2009;123:52-57

Supplemental tables
Table S I. Characteristics of acute myocardial infarction (AMI) patients without ischemic
stroke within one year of AMI stratified by time period and survival.
1998-2000 2001-2002 2003-2004 2005-2006 2007-2008 No
stroke
n=
32757
No
stroke
and
death n=
9055
21.7%
No
stroke
n=
25028
No
stroke
and
death n=
6417
20.4%
No
stroke
n= 25565
No
stroke
and
death n=
5651
18.1%
No
stroke
n=
25519
No
stroke
and
death n=
4903
16.1%
No
stroke
n=
26795
No
stroke
and
death n=
4435
14.2%
Patient characteristics
Woman 34.0% 42.2% 35.4% 43.9% 35.2% 43.7% 34.9% 43.7% 34.9% 46.6%
Age
(mean)
68.7 78.2 69.2 79.1 69.2 79.5 69.4 80.0 69.1 80.2
BMI
(mean)
26.7
n=390
4
25.3
n=
571
26.7
n=463
9
24.9
n=686
26.7
n=105
87
25.5
n=151
2
26.7
n=152
72
24.9
n=2017
26.9
n=192
11
25.1
n=228
7
Co morbidity
Prior
stroke
8.2% 18.3% 8.6% 20.0% 8.4% 20.3% 8.4% 19.8% 8.0% 19.1%
Prior
ischemic
stroke
5.6%
13.0% 6.3% 16.0% 6.4% 16.6% 6.6% 16.1% 6.4% 16.2%
Prior AMI 17.4% 28.3% 15.0% 25.6% 12.7% 25.0% 11.2% 23.2% 9.9% 22.0%
Prior heart
failure
9.2% 27.4% 9.0% 27.9% 8.1% 26.8% 7.8% 26.4% 7.1% 26.8%
Prior
diabetes
mellitus
16.0% 23.7% 17.6% 24.3% 17.3% 25.3% 18.2% 26.6% 19.7% 27.4%
Prior renal
failure
1.1% 4.2% 1.4% 5.1% 1.4% 6.4% 1.6% 6.4% 1.9% 7.9%
Hypertensi
on
33.0% 35.1% 36.0% 38.4% 38.1% 40.9% 41.3% 42.9% 45.3% 50.5%
Atrial
fibrillation
13.2% 27.0% 13.1% 28.5% 12.5% 27.8% 12.5% 28.0% 11.8% 28.3%
Smoking 24.4% 14.3% 24.4% 15.3% 23.9% 14.2% 23.3% 12.9% 22.9% 13.0%
Clinical characteristics
Heartrate
(mean)
- - 78.2
n=215
8
90.5
n=500
78.7
n=108
59
89.4
n=225
9
79.7
n=228
33
89.8
n=4398
79.3
n=249
61
89.8
n=414
4
Systolic
blood
pressure
(mean)
141.5
n=146
2
131.4
n=349
144.4
n=281
2
130.0
n=610
146.9
n=106
20
131.3
n=225
9
147.8
n=226
58
132.7
n=4362
147.7
n=245
39
133.0
n=405
3
LDL
(mean)
3.5
n=
4003
3.2
n=384
3.4
n=130
65
3.1
n=171
7
3.2
n=158
50
2.9
n=186
5
3.1
n=167
04
2.7
n=1678
3.1
n=185
84
2.7
n=165
4
STEMI 42.0% 36.4% 37.4% 31.8% 35.7% 30.4% 34.8% 28.3% 31.4% 25.9%
Heart
failure
during
hospitaliza
tion
33.9% 66.0% 30.3% 63.9% 28.2% 63.6% 25.9% 63.0% 22.0% 58.6%
Treatment in hospital
Acute
CABG
0.2% 0.1% 0.3% 0.1% 0.2% 0.2% 0.3% 0.2% 0.2% 0.2%
Acute PCI 4.5% 1.9% 8.3% 2.6% 16.1% 5.2% 25.3% 10.9% 27.8% 12.9%
Thrombol
ysis
30.4% 21.9% 23.9% 17.6% 14.7% 12.5% 5.5% 6.1% 2.4% 2.4%
BMI=body mass index. LDL=low density lipoprotein. STEMI=ST-elevation myocardial
infarction. CABG=coronary artery by-pass grafting. PCI=percutaneous coronary intervention.
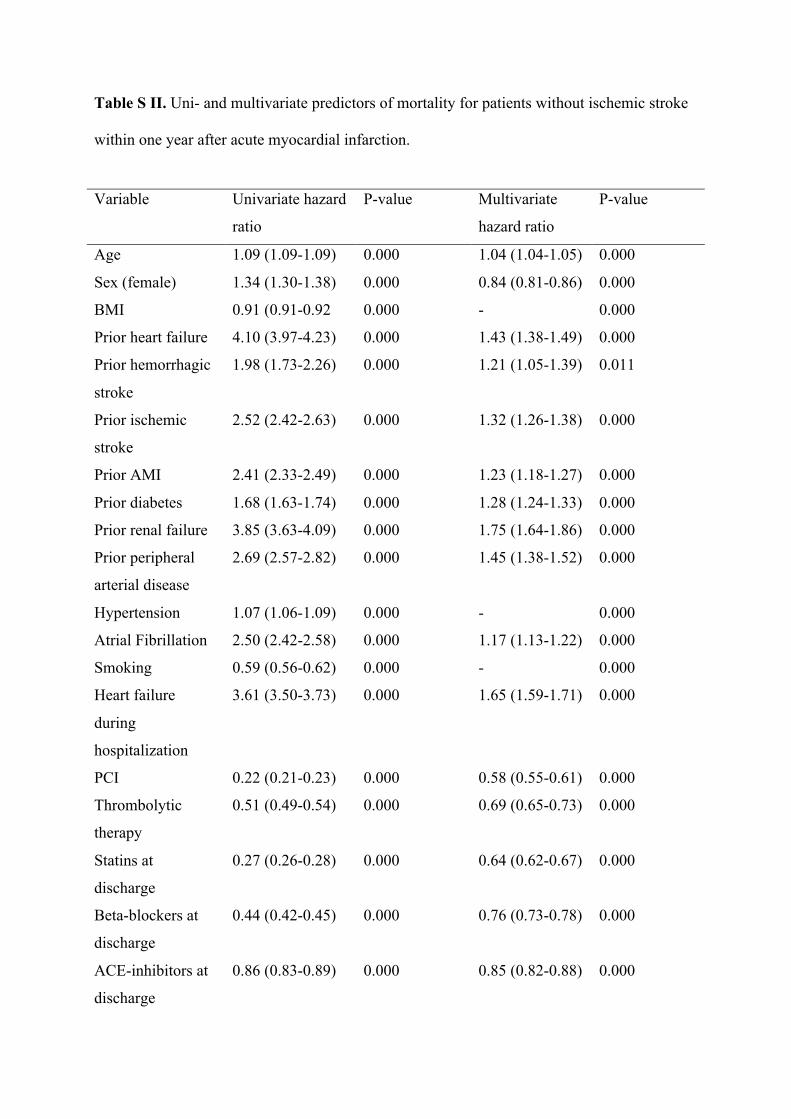
Table S II. Uni- and multivariate predictors of mortality for patients without ischemic stroke
within one year after acute myocardial infarction.
Variable Univariate hazard
ratio
P-value Multivariate
hazard ratio
P-value
Age 1.09 (1.09-1.09) 0.000 1.04 (1.04-1.05) 0.000
Sex (female) 1.34 (1.30-1.38) 0.000 0.84 (0.81-0.86) 0.000
BMI 0.91 (0.91-0.92 0.000 - 0.000
Prior heart failure 4.10 (3.97-4.23) 0.000 1.43 (1.38-1.49) 0.000
Prior hemorrhagic
stroke
1.98 (1.73-2.26) 0.000 1.21 (1.05-1.39) 0.011
Prior ischemic
stroke
2.52 (2.42-2.63) 0.000 1.32 (1.26-1.38) 0.000
Prior AMI 2.41 (2.33-2.49) 0.000 1.23 (1.18-1.27) 0.000
Prior diabetes 1.68 (1.63-1.74) 0.000 1.28 (1.24-1.33) 0.000
Prior renal failure 3.85 (3.63-4.09) 0.000 1.75 (1.64-1.86) 0.000
Prior peripheral
arterial disease
2.69 (2.57-2.82) 0.000 1.45 (1.38-1.52) 0.000
Hypertension 1.07 (1.06-1.09) 0.000 - 0.000
Atrial Fibrillation 2.50 (2.42-2.58) 0.000 1.17 (1.13-1.22) 0.000
Smoking 0.59 (0.56-0.62) 0.000 - 0.000
Heart failure
during
hospitalization
3.61 (3.50-3.73) 0.000 1.65 (1.59-1.71) 0.000
PCI 0.22 (0.21-0.23) 0.000 0.58 (0.55-0.61) 0.000
Thrombolytic
therapy
0.51 (0.49-0.54) 0.000 0.69 (0.65-0.73) 0.000
Statins at
discharge
0.27 (0.26-0.28) 0.000 0.64 (0.62-0.67) 0.000
Beta-blockers at
discharge
0.44 (0.42-0.45) 0.000 0.76 (0.73-0.78) 0.000
ACE-inhibitors at
discharge
0.86 (0.83-0.89) 0.000 0.85 (0.82-0.88) 0.000
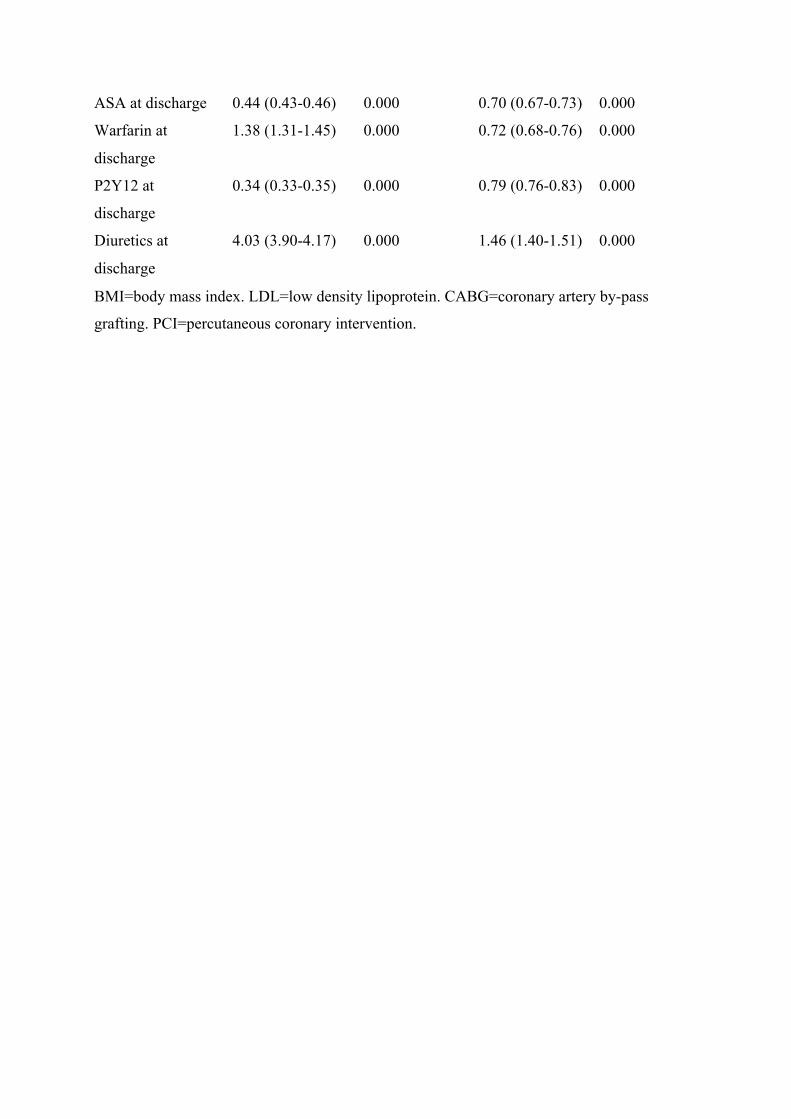
BMI=body mass index. LDL=low density lipoprotein. CABG=coronary artery by-pass
grafting. PCI=percutaneous coronary intervention.
ASA at discharge 0.44 (0.43-0.46) 0.000 0.70 (0.67-0.73) 0.000
Warfarin at
discharge
1.38 (1.31-1.45) 0.000 0.72 (0.68-0.76) 0.000
P2Y12 at
discharge
0.34 (0.33-0.35) 0.000 0.79 (0.76-0.83) 0.000
Diuretics at
discharge
4.03 (3.90-4.17) 0.000 1.46 (1.40-1.51) 0.000

Supplemental figures
Figure SI
Figure S I. Time trends for discharge medication use for acute myocardial infarction (AMI) patients without ischemic stroke that has survived (solid line) or died (broken line).
0
10
20
30
40
50
60
70
80
90
100
1998-‐2000 2001-‐2002 2003-‐2004 2005-‐2006 2007-‐2008
Sta0ns
ACE-‐inhibitors
Beta-‐blockers
ASA
Warfarin
P2Y12
Diure0cs

Figure SII
Figure SII. Cumulative survival for men (left) and women (right) with ischemic stroke within one year after myocardial infarction stratified by time period.


















