Monitoring of Neonatal Haemodynamics
149
Case 1 • 35 YO G3P2, uneventful pregnancy • Presented in labour @ 39 wks • Shoulder dystocia • Pulseless, apneic, and pale • Responded to PPV and chest compressions. AS 1, 3, 6, 7
-
Upload
ayman-abou-mehrem -
Category
Health & Medicine
-
view
2.781 -
download
2
Transcript of Monitoring of Neonatal Haemodynamics

Case 1
• 35 YO G3P2, uneventful pregnancy
• Presented in labour @ 39 wks
• Shoulder dystocia
• Pulseless, apneic, and pale
• Responded to PPV and chest compressions. AS 1, 3, 6, 7

Case 1
• At 20 min of life:
• Ventilated, poor resp. effort, FiO2 0.25
• Temp 36ºC, HR 120 bpm, MBP 42 mmHg
• Mottled skin, CRT 3-4 sec

Case 1
What is the next action?

Case 2
• 25 YO, G2P1, regular ANC
• Presented 3 days prior to delivery in threatened preterm labour @ 26 wks
• No pPROM
• Received Beta x 2, Amp and Erythro
• Baby was born pink, HR>100, apneic
• Intubated, Bles, Ventilated, UAC, UVC

Case 2
• At 1 hr of age:
• AC/VG, PEEP 6, VG 4 ml/kg, FiO2 0.23
• HR 150 bpm, MBP 23 mmHg, CRT 2-3 sec

Case 2
What is the next action?

Case 3
• 25 YO, G2P1, regular ANC
• Presented 3 days prior to delivery in threatened preterm labour @ 26 wks
• No pPROM
• Received Beta x 2, Amp and Erythro
• Baby was born pink, HR>100, apneic
• Intubated, Bless, Ventilated, UAC, UVC

Case 3
• At 6 hrs of age:
• HR 150 bpm, MBP 29 mmHg, CRT 2-3 Sec
• AC/VG, PEEP 6, FiO2 0.25, VG 4 ml/kg,
VR 40, RR 50’s
• ABG: pH 7.22, PCO2 37, PO2 54,
HCO3 15, BE -12

Case 3
What is the next action?

Monitoring of Neonatal Hemodynamics*
Ayman Abou Mehrem, MD, CABP
Neonatology Fellow
University of Manitoba
* Adapted from Early Human Development 86 (2010) 135-165

Monitoring of Neonatal Hemodynamics
• Introduction
• Objective
• Part 1: Clinical Monitoring of Systemic Hemodynamics
• Part 2: Cardiac Output Monitoring
• Part 3: Functional Echocardiography
• Part 4: Peripheral Hemodynamics

Introduction
• Hemodynamics: from Greek
• αίμα (haima): blood
• Δύναμις (dynamis): power or strength
• The study of the movements of blood and the forces concerned herein1
1 Dorland's illustrated medical dictionary. Philadelphia: Saunders; 2003

Introduction
• Circulation in neonates is unique:
– Transition from low resistant placental circulation to high resistant systemic circulation
– Presence of intra- and extra-cardiac shunts
– Underdeveloped regulatory mechanism at the end organs in preterm neonates

Picture from: Kliegman: Nelson Textbook of Pediatrics, 18th ed

Introduction
• Adequate blood circulation is necessary for adequate supply of O2 and other essential nutrients, and to remove toxic metabolic products from all tissues
• O2 supply is dependent on:
– Arterial O2 content
– Blood flow
Picture from: www.learnhemodynamics.com/hemo/oxygen.htm

Introduction
• Arterial O2 content
– Hemoglobin concentration
– Arterial O2 saturation (SaO2)
• The limitation of O2 supply monitoring
– the ability to monitor blood flow to the tissues

Objective
• Review of available methods for monitoring of hemodynamics and end-organ perfusion in neonates.
• Identify best evidence-based practice in directing the management of circulatory insufficiency in neonates, achieving hemodynamic stability and avoiding deleterious effect of various interventions.

Part 1Clinical Monitoring of Systemic
Hemodynamics

What are your criteria to diagnose
“circulatory insufficiency”
in neonates?

Clinical monitoring of systemic hemodynamics
• In questionnaire across Canada:2
– 25.8% of the respondents rely on absolute BP values alone when defining hypotension
– The remainder combine BP values and clinical signs of perfusion: color, capillary refill time and urine output
– 87.1% defined hypotension as BP in mm Hg less than gestational age in weeks
2 Dempsey EM, Barrington KJ. Diagnostic criteria and therapeutic interventions for the hypotensive very low birth weight infant. J Perinatol 2006;26:677–81.

Blood Pressure
• Hypotension:– BP < 10th (or 5th) percentile of normative BP
values from a reference population with regard to GA, BW, and postnatal age
– The lower limit of normal MABP: the numeric value of GA in wks, provided no additional signs exist of hypoperfusion of endorgans
– MABP < 30 mm Hg

Blood Pressure
• Osborn et al, 2004:3
Poor correlation between BP and Systemic Blood Flow in preterm infants < 30 wks GA
3 Osborn DA, Evans N, Kluckow M. Clinical detection of low upper body blood flow in very premature infants using blood pressure, capillary refill time, and central–peripheral temperature difference. Arch Dis Child Fetal Neonatal Ed 2004;89: F168–73.

Blood Pressure

Blood Pressure• Groves et al, 2008:4
• Low blood pressure does not correlate with poor perfusion in the first 48 h of postnatal life in sick preterm infants < 30 wks GA
• Infant with reduced systemic perfusion (SVC flow < 41 ml/kg/min) tend to have normal or high blood pressure in the first hours of life.
• High systemic vascular resistance may lead to reduced blood flow.
4 Groves AM, Kuschel CA, Knight DB, Skinner JR. Relationship between blood pressure and blood flowin newborn preterm infants. Arch Dis Child Fetal Neonatal Ed. 2008 Jan;93(1):F29-32. Epub 2007 May 2.

Heart Rate
• In neonate,
It is supposed that cardiac output is almost entirely dependent on HR !!!??

Heart Rate
• Kluckow and Evans, 2000:5
• No correlation between HR and systemic blood flow (SBF)
– The normal range of SBF: being above the lowest recorded SVC flow at each of the four scans, that is, above 30, 34, 42, and 46 ml/kg/min respectively at 5, 12, 24, and 48 hours of age
5 Kluckow M, Evans N. Low superior vena cava flow and intraventricular haemorrhage in preterm infants. Arch Dis Child Fetal Neonatal Ed 2000;82: F188–94.

Heart Rate

Color
• Skin and mucosal membranes color is influenced by:– Oxygenation– Hb concentration– Skin temperature– Skin thickness– Peripheral perfusion– Race– Gestational age– Ambient temperature– Light

Color
• O'Donnell et al, 2007:6
• Among clinicians observing the same videos there was disagreement about whether newborn infants looked pink with wide variation in the SpO2 when they were considered to become pink
6 O'Donnell CP, Kamlin CO, Davis PG, Carlin JB, Morley CJ. Clinical assessment of infant colour at delivery. Arch Dis Child Fetal Neonatal Ed 2007;92:F465–7.

Capillary refill time (CRT)
• The time required for the return of color after the application of a blanching pressure to a distal capillary bed
• Raichur et al, 2001:7
• There was good interobserver agreement when CRT was measured on the chest but not the forehead, palm or heel
7 Raichur DV, Aralihond AP, Kasturi AV, Patil DH. Capillary refill time in term neonates: bedside assessment. Indian J Pediatr. 2001 Jul;68(7):613-5.

Capillary refill time (CRT)
• Osborn et al, 2004:3
• CRT > 3 sec had a sensitivity of 55% and a specificity of 80% for predicting low SVC flow
3 Osborn DA, Evans N, Kluckow M. Clinical detection of low upper body blood flow in very premature infants using blood pressure, capillary refill time, and central–peripheral temperature difference. Arch Dis Child Fetal Neonatal Ed 2004;89: F168–73.

Capillary refill time (CRT)

Urine Output
• Miletin et al, 2009:8
• There was a poor correlation between the capillary refill time, MBP, urine output and low SVC flow (< 40 ml/kg/min)
8 Miletin J, Pichova K, Dempsey EM. Bedside detection of low systemic flow in the very low birth weight infant on day 1 of life. Eur J Pediatr 2009;168:809–13.

Urine Output

Lactate
• Blood Lactate ≠ Lactic Acidosis
• Cause of lactate production in neonates:– Anaerobic metabolism (e.g. circulatory failure)– Increased glycogenolysis– Administration of sympathicomimetic drugs– Inborn errors of metabolism.

Lactate• Elevated lactate may be associated with:
– Normal pH, acidosis, alkalosis
– Normoxia, hypoxia or anoxia
• Deshpande and Platt, 1997:9
– There was no correlation between common acid-base parameters such as pH, base excess, bicarbonate concentrations and blood lactate concentrations
9 Deshpande SA, Platt MP. Association between blood lactate and acid–base status and mortality in ventilated babies. Arch Dis Child Fetal Neonatal Ed 1997;76: F15–20.

Lactate
• Despite circulatory insufficiency, lactate may not increase when :– Lactate clearance is in balance with lactate
production
– Oxygen delivery meets the oxygen demand in the tissues by increased oxygen extraction
• Lactate may accumulate locally and remain undetectable until perfusion improves

Lactate
• Miletin et al, 2009:8
• Serum lactate ≥ 2.8 mmol/l has sensitivity of 100% and specificity 60% for detecting low flow states.
8 Miletin J, Pichova K, Dempsey EM. Bedside detection of low systemic flow in the very low birth weight infant on day 1 of life. Eur J Pediatr 2009;168:809–13.

Lactate

Central–peripheral temp. difference (CPTd)
• Osborn et al, 2004:3
• There was no correlation between CPTd and SVC flow
3 Osborn DA, Evans N, Kluckow M. Clinical detection of low upper body blood flow in very premature infants using blood pressure, capillary refill time, and central–peripheral temperature difference. Arch Dis Child Fetal Neonatal Ed 2004;89: F168–73.

Central–peripheral temp. difference (CPTd)

Acid–base balance
• Kluckow and Evans, 2001:10
• No correlation between low SVC flow and pH or base excess
10 Kluckow M, Evans N. Low systemic blood flow and hyperkalemia in preterm infants. J Pediatr 2001;139:227–32.

Venous oxygen saturation (SvO2)
• Mixed SvO2 represents the oxygen reserve after tissue oxygen extraction
• SvO2 depends on:– Arterial O2 concentration– O2 consumption– Cardiac output– Hb concentration
• Main PA is most optimal site for mixed venous blood sampling

• In NB, we can measure central SvO2
• Mixed SvO2 ≠ Central SvO2
• Difference is influenced by:– Sampling site of central venous blood– Presence of left-to-right shunts– Incomplete mixing of venous blood– Redistribution of blood flow through upper and lower
body– Level of consciousness (anaesthesia)– Myocardial O2 consumption
Venous oxygen saturation (SvO2)

Venous oxygen saturation (SvO2)
• In healthy adults:
SVC saturation is 2–3% lower than the true mixed venous saturation

Venous oxygen saturation (SvO2)
• In Shock:– The relationship between SVC saturation and
mixed venous saturation reverses, with the reported difference ranging from 5–18%
• SVC saturation will typically overestimate Mixed SvO2 , whereas IVC saturation may underestimate it
11 Martin J, Shekerdemian LS. The monitoring of venous saturations of oxygen in children with congenitally malformed hearts. Cardiol Young 2009;19:34–9.

Venous oxygen saturation (SvO2)
• Hart et al, 2006:12
• No linear relationship has been found between IVC SvO2, obtained from UVC, and systemic blood flow (SVC flow)
12 Hart J, Vemgal P, Cocks-Drew S, Harrison C, Andersen C. The relation between inferior vena cava oxygen saturation, superior vena cava flow, fractional oxygen extraction and haemoglobin affinity in sick newborns: a pilot study. Acta Paediatr 2006;95:50–5.

Venous oxygen saturation (SvO2)
• de Oliveira et al, 2008:13
• Aiming at a central SvO2 ≥ 70%, improves outcome of pediatric septic shock
13 de Oliveira CF, de Oliveira DS, Gottschald AF, et al. ACCM/PALS haemodynamic support guidelines for paediatric septic shock: an outcomes comparison with and without monitoring central venous oxygen saturation. Intensive Care Med 2008;34:1065–75.

Combination of different clinical hemodynamic variables
de Boode. Clinical monitoring of systemic hemodynamics in critically ill newborns. Early Human Development 86 (2010) 137–141

Conclusion
• The clinical assessment of cardiac output by the interpretation of indirect parameters of systemic blood flow is inaccurate, irrespective of the level of experience of the clinician

Conclusion
• Using BP to diagnose low systemic blood flow will consequently mean that too many patients will potentially be undertreated or overtreated, both with substantial risk of adverse effects and iatrogenic damage.

Conclusion
• Combining different clinical hemodynamic parameters enhances the predictive value in the detection of circulatory failure, although accuracy is still limited.

Conclusion
• Variation in time (trend monitoring) might possibly be more informative than individual, static values of clinical and biochemical parameters to evaluate the adequacy of neonatal circulation.

Part 2Cardiac Output Monitoring in the
Newborns
* Adapted from Early Human Development 86 (2010) 135-165

Cardiac Output Monitoring in the Newborns
• Introduction
• Fick Principle
• Indicator Dilution Techniques
• Doppler Ultrasound
• Arterial Pulse Contour Analysis (APCA)
• Thoracic Electrical Impedance (TEI)
• Conclusion

Introduction
• Low cardiac output is associated with an increased mortality in children14
• Delay in the diagnostic process of shock increases mortality15
14 Ceneviva G, Paschall JA, Maffei F, Carcillo JA. Hemodynamic support in fluid refractory pediatric septic shock. Pediatrics 1998;102:e19.
15 Han YY, Carcillo JA, Dragotta MA, et al. Early reversal of pediatric–neonatal septic shock by community physicians is associated with improved outcome. Pediatrics 2003;112:793–9.

Introduction• Low systemic blood flow in preterm infants
is associated with:– Increased risk of IVH and death.5, 16
– Oligouria and hyperkalemia10
– Compromised EEG activity17
– Impaired neurodevelopmental outcome18
5 Kluckow M, Evans N. Low superior vena cava flow and intraventricular haemorrhage in preterm infants. Arch Dis Child Fetal Neonatal Ed 2000;82:F188–94.
16 Miletin J, Dempsey EM. Low superior vena cava flow on day 1 and adverse outcome in the very low birth weight infant. Arch Dis Child Fetal Neonatal Ed 2008;93:F368–71.
10 Kluckow M, Evans N. Low systemic blood flow and hyperkalemia in preterm infants. J Pediatr 2001;139:227–32.17 West CR, Groves AM, Williams CE, et al. Early low cardiac output is associated with compromised
electroencephalographic activity in very preterm infants. Pediatr Res 2006;59:610–5.18 Osborn DA, Evans N, Kluckow M, Bowen JR, Rieger I. Low superior vena cava flow and effect of inotropes on
neurodevelopment to 3 years in preterm infants. Pediatrics 2007;120:372–80.

Fick Principle
• Adolf Eugen Fick (1829–1901)• Blood flow to an organ can be calculated
using a marker substance if the following information is known:– Amount of marker substance taken up by the
organ per unit time– Concentration of marker substance in arterial
blood supplying the organ– Concentration of marker substance in venous
blood leaving the organ

Oxygen Fick
CO = VO2_________
Ca - Cv
CO: Cardiac output
VO2: Oxygen consumption in ml of pure gaseous oxygen per minute.
Ca: The oxygen content of blood from a cannula in a peripheral artery.
Cv: The oxygen content of blood taken from the pulmonary artery

Oxygen Fick
• Gold standard in cardiac output monitoring in a research setting
• Limitations:– Technical difficulty– PA catheter required– Affected by shunt

Assumed O2 Fick Determination
• Assumed value for Oxygen Consumption
• Problem:– Significant errors in the determination of
cardiac output.19
19 Fakler U, Pauli C, Hennig M, Sebening W, Hess J. Assumed oxygen consumption frequently results in large errors in the determination of cardiac output. J Thorac Cardiovasc Surg. 2005 Aug;130(2):272-6.

Modified CO2 Fick
• Pulmonary CO2 exchange is measured at the ETT.
• Simultaneous measurement of total CO2 concentration in arterial and central venous blood is required.20
• It is reliable and easily applicable in ventilated newborn lambs, also in the presence of a significant left-to-right shunt.21
20 de Boode WP, Hopman JC, Daniels O, van der Hoeven HG, Liem KD. Cardiac output measurement using a modified carbon dioxide Fick method: a validation study in ventilated lambs. Pediatr Res 2007;61:279–83.
21 de Boode WP, Hopman JC, Wijnen MH, Tanke RB, van der Hoeven HG, Liem KD. Cardiac output measurement in ventilated lambs with a significant left-to-right shunt using the modified carbon dioxide Fick method. Neonatology 2010;97:124–31.

Modified CO2 Fick
• Major limitation:– Steady state required– Blood loss due to blood sampling
– Inaccuracy due to error in calculation of CO2 concentration in blood

Indicator Dilution Techniques
• Blood flow can be calculated if the change in concentration of a known quantity of injected indicator is measured in time distal to the point of injection
• Indicator dilution curve can be obtained
• Cardiac output: calculated with using Stewart–Hamilton equation

Indicator Dilution Techniques
Miller RD. Miller’s Anesthesia, 7th edition. 2009 Churchill Livingstone, An Imprint of Elsevier. Chapter 16: Cardiac Physiology

Indicator Dilution Techniques
• Indicators used:– Dye Dilution:
• Indocyanine green• Evans blue• Brilliant red
– Thermodilution: cold solutions– Lithium Dilution: lithium– Ultrasound Dilution: normal saline

Pulse dye densitometry (PDD)
• Injection of indocyanine green
• Detection noninvasively via a fingertip sensor
• Validated in adults only
• Very difficult to obtain reliable pulse waveforms from small children and neonates

Pulmonary Artery Thermodilution (PATD)
• Injection of a cold fluid in the RA
• Measure change in blood temperature with a thermistor-tipped PA catheter
• Most widely used method in adults
• Very invasive (smallest 5F)
• Transient bradycardia in response to fast injection of cold saline
• Results affected by shunts

Thermodilution Flow-directed Balloon Flotation PAC
Kliegman: Nelson Textbook of Pediatrics, 18th ed. 2007 Saunders, An Imprint of Elsevier. Chapter 64 – Monitoring Techniques for the Critically Ill Infant and Child

Transpulmonary Thermodilution (TPTD)
• 3–5 ml NS (cold or at room temp) is used as an indicator, injected via a CVC
• Detected by a thermistor-tipped catheter positioned in the femoral, brachial or axillary artery.
• Calibrate the software for continuous arterial pulse contour analysis.

Transpulmonary Thermodilution (TPTD)
• Regarded as the clinical ‘gold standard’ for pediatric CO measurement
• Limitations:– Specific thermistor-tipped catheter required– Catheterization of femoral, brachial or axillary artery
necessary– Enhanced loss of indicator due to pulmonary edema
and in non-homogeneously perfused lungs– Repeated calibration required– Repetitive measurements affect fluid balance

Lithium dilution (LiDCO)
• Li sensitive electrode, attached to a peripheral arterial catheter
• Li is i.v. injected in a known quantity• A correction is needed for Na+ and Hct• Limitations:
– Lithium toxicity– Blood sampling– Not compatible with non-depolarising muscle
relaxants– unreliable during hyponatraemia– Affected by shunts– Repeated calibration required

Ultrasound Dilution (UDCO)
• Injection of NS into the blood stream will lead to a decrease in the velocity of ultrasound in blood.
• Extracorporeal circuit: a disposable arteriovenous (AV) loop in between regular arterial and central venous catheters for placement of flow and dilution sensors

Ultrasound Dilution (UDCO)
• Krivitski 2008: 22
In vitro validation confirmed the ability of the ultrasound dilution technology to accurately measure small flows and volumes required for hemodynamic assessments in small pediatric and neonatal patients.
22 Krivitski NM, Kislukhin VV, Thuramalla NV. Theory and in vitro validation of a new extracorporeal arteriovenous loop approach for hemodynamic assessment in pediatric and neonatal intensive care unit patients. Pediatr Crit Care Med 2008;9: 423–8.

Ultrasound Dilution (UDCO)

Ultrasound Dilution (UDCO)
• Blood US velocity: 1560 –1585 m/sec
• Saline US velocity: 1533 m/sec

Ultrasound Dilution (UDCO)

Ultrasound Dilution (UDCO)
• de Boode 2010: 23, 24
– UDCO measurement is reliable in piglets with the use of a small volume of a nontoxic indicator (NS).
– UDCO does not cause clinically relevant changes in cerebral and systemic circulation and oxygenation in a piglet model.
23 de Boode WP, van Heijst AF, Hopman JC, Tanke RB, van der Hoeven HG, Liem KD. Cardiac output measurement using an ultrasound dilution method. A validation study in ventilated piglets. Pediatr Crit Care Med 2010;11:103–8.
24 de Boode WP, van Heijst AFJ, Hopman JC, Tanke RB, van der Hoeven HG, Liem KD. Application of the ultrasound dilution technology for cardiac output measurement: cerebral and systemic hemodynamic consequences in a juvenile animal model. Pediatr Crit Care Med 2010 (published ahead of print January 29, 2010).

Ultrasound Dilution (UDCO)
• Limitations:– Repetitive measurements affect fluid balance– Possible indicator loss in nonhomogeneous
perfused lungs– Use of extracorporeal loop

Doppler Ultrasound
• Ultrasound beam• Moving erythrocytes will cause a
frequency shift in the reflected signal (Doppler shift)
• Spectral analysis of the Doppler shift will produce velocity–time waveforms
• The area under the velocity–time curve gives the stroke distance or velocity–time integral (VTI).

Doppler Ultrasound
• Stroke volume through a vessel, e.g. MPA, can be calculated if the blood velocity–time integral and the cross sectional area (CSA) of the vessel are known
• CO = Stroke volume X Heart rate

Doppler Ultrasound• Chew 2003: 25
– Literature review of the accuracy and repeatability of Doppler CO measurements in children
– Doppler derived CO measurements are most useful as trend monitoring instead of measurement of absolute values
– The bias of Doppler CO measurements is <10%, with a rather wide range −37% to 16%
– The precision, defined as ±2 SD, is 30%– The intraobserver variability: 2.1 to 22 %– The interobserver variability: 3.1 to 21.7 %
25 Chew MS, Poelaert J. Accuracy and repeatability of pediatric cardiac output measurement using Doppler: 20-year review of the literature. Intensive Care Med 2003;29:1889–94.

Doppler Ultrasound
• Variation is caused by several factors: 26
– Difficulty in assessment of the VTI– Calculation error due to the angle of
insonation and problems with correct measurement of the CSA.
– An error of 5°―10° in the intercept angle will lead to an error of ± 20% in blood flow velocity measurement
26 Bengur AR, Meliones JN. Continuous monitoring of cardiac output: how many assumptions are valid? Crit Care Med 2000;28:2168–9.

Doppler Ultrasound
• Transthoracic echocardiography (TTE)
• Transesophageal echocardiography (TEE)
• Transesophageal Doppler (TED)
• Transcutaneous Doppler (TCD)

TEE and TED
• TEE is mainly used in children with CHD for functional and structural imaging during cardiac surgery
• TED is used to assess the CO by measuring the flow in the descending Ao
• Body wt > 3 kg

Doppler Ultrasound
• Limitation:– Significant training required– Highly operator dependent– Inaccuracy due to error in assessment of VTI
& CSA and angle of insonation– Complications with TEE and TED

Arterial Pulse Contour Analysis (APCA)
• Measures stroke volume on a beat-to-beat basis from the arterial pulse pressure waveform.
• The waveform will vary– aortic root impedance– Aortic compliance– Systemic vascular resistance.
• Frequent calibration required• No published data in neonates

Thoracic Electrical Impedance (TEI)
• The electrical conductivity of blood is higher than that of muscle, fat and air.
• Application of a high frequency, very low-magnitude current across the chest via topical electrodes distributes therefore mainly to blood.

Thoracic Electrical Impedance (TEI)
• Pulsatile changes in thoracic blood volume will cause changes in electrical thoracic impedance.
• The changes in impedance during systole are proportional to cardiac output.
• Limitations:– Inaccuracy due to alteration in position or contact of
the electrodes– Irregular heart rates and acute changes in tissue
water content

Conclusion
• CO monitoring in neonates is challenging.
• Usefulness is probable but uncertain
• ACCM recommended to titrate therapy to achieve CO 3.3–6.0 L/min/m2 in patients with persistent catecholamine-resistant shock. 27
27 Brierley J, Carcillo JA, Choong K, et al. Clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock: 2007 update from the American College of Critical Care Medicine. Crit Care Med 2009;37: 666–88.

Conclusion
• Concern about the clinician's ability to interpret the assessed hemodynamic variables correctly
• Anyone who uses any method of cardiac output monitoring is obliged to thoroughly understand the basic principles of the applied technology and its respective advantages and limitations

Part 3Functional Echocardiography
(fECHO)
* Adapted from Early Human Development 86 (2010) 135-165

Functional Echocardiography
• Introduction
• Hypotension during 1st 24 hrs
• Assessment and monitoring of the DA
• Assessment and monitoring of PH
• Infants with Perinatal Asphyxia
• Assessment during sepsis
• Developing a local fECHO service
• Conclusion

Functional Echocardiography
• The bedside use of US to longitudinally assess:
– Myocardial function
– Systemic and pulmonary blood flow
– Intra and extracardiac shunts
– Organ flow and tissue perfusion

Does fECHO replace the formal
echocardiography?
Are neonatologists going to be
cardiologists?

Functional Echocardiography
• Provides detailed real time information concerning physiology and hemodynamics
• Allowing targeting of therapy
• Integral component of point of care US, or clinician performed US (CPU)

Functional Echocardiography• fECHO is different from echocardiography
performed by a pediatric cardiologist:
– Consultative
– Crosssectional
– High-end opinion regarding structural heart disease and an assessment of function at the time of the measurement
• Provides functional information required by the neonatologist that is not always provided by the pediatric cardiologist.

Hypotension During the 1st 24 hrs
• The critical clinical questions are:
– Does hypotension (however defined) has a detrimental effect on end organ perfusion?
– What conditions contribute to the hypotension?
– Is hypotension in the setting of a normal cardiac output is acceptable?

Hypotension During the 1st 24 hrs
• Al-Aweel 2001, 6 NICUs in USA: 28
– Observational study of 1288 VLBWI
– To assess variations in BP stability among NICUs, inter-NICU differences in vasopressor use, and to address the association between IVH and abnormal BPs
– Lowest and highest MBP in 1st 12 hrs of life
28 Al-Aweel I, Pursley DM, Rubin LP, Shah B, Weisberger S, Richardson DK. Variations in prevalence of hypotension, hypertension, and vasopressor use in NICUs. J Perinatol. 2001;21: 272–278

Hypotension During the 1st 24 hrs
• Al-Aweel 2001, 6 NICUs in USA:
– 3-fold differences among sites in the odds of hypotension that could not be explained by differences in the populations.
– 2 of the 6 sites had 5-fold to 30-fold higher use of vasopressors than other sites after risk adjusting for the occurrence of hypotension
– A borderline association between severe IVH and hypotension but not hypertension.

Hypotension During the 1st 24 hrs
• Fanaroff 2006: 29
– Retrospective chart review of 156 ELBWI
– Treated hypotension in the 1st 72 hours of life and perinatal factors, morbidity, mortality, and neurosensory outcome.
29 Fanaroff JM, Wilson-Costello DE, Newman NS, Montpetite MM, Fanaroff AA. Treated hypotension is associated with neonatal morbidity and hearing loss in extremely low birth weight infants. Pediatrics 2006;117:1131–5.

Hypotension During the 1st 24 hrs
• Fanaroff 2006:

Hypotension During the 1st 24 hrs
• Fanaroff 2006:

Hypotension During the 1st 24 hrs
• Fanaroff 2006:

Hypotension During the 1st 24 hrs
• SBF can be estimated with fECHO:
– SVC flow: unaffected by cardiac shunts
– RVO: minimally affected by PFO LR shunt
– LVO: less informative during transition, PDA

Hypotension During the 1st 24 hrs
• Normal SBF
• No studies have explored the absolute threshold of low SBF
• Increased morbidity and mortality: 5, 30
– SVC flow < 30 ml/kg/min at 5 h of age– and < 45 ml/kg/min thereafter– RVO or LVO < 150 ml/kg/min
5 Kluckow M, Evans N. Low superior vena cava flow and intraventricular haemorrhage in preterm infants. Arch Dis Child Fetal Neonatal Ed 2000;82: F188–94.
30 Evans N, Kluckow M. Early determinants of right and left ventricular output in ventilated preterm infants. Arch Dis Child Fetal Neonatal Ed 1996;74:F88–94.

Hypotension During the 1st 24 hrs
• Response to treatment is not always what we expect.
• Lundstrøm 2000: 31
– RCT, 36 PT < 33 wks, MABP 29-40 mmHg– Ø Tx, Dopa 5 μg/kg/min, or Alb 20% 15ml/kg
– CBF, LVO, MABP, HR, SaO2, PaO2, and PaCO2 were measured before and 2 h after the treatment
31 Lundstrøm K, Pryds O, Greisen G. The haemodynamic effects of dopamine and volume expansion in sick preterm infants. Early Hum Dev 2000;57:157–63.

Hypotension During the 1st 24 hrs
• Lundstrøm 2000:

Hypotension During the 1st 24 hrs
• Osborn 2002: 32
– RCT, 42 PT < 30 wks, < 24 hrs age
– SVC flow < 41 ml/kg/min
– NS 10 ml/kg then either dopamine or dobutamine
32 Osborn D, Evans N, Kluckow M. Randomized trial of dobutamine versus dopamine in preterm infants with low systemic blood flow. J Pediatr 2002;140:183.

Hypotension During the 1st 24 hrs
• Osborn 2002:– At the highest dose, dobutamine resulted in a
significantly greater increase in SVC flow than dopamine
– Dopamine resulted in a significantly greater increase in blood pressure.

Hypotension During the 1st 24 hrs
• Osborn 2002:– Infants receiving dobutamine only at 24 hours
had a greater RVO than infants receiving dopamine
– 40% failed to increase or maintain SVC flow in response to either inotrope.
– No significant differences in mortality or morbidity were found.

Hypotension During the 1st 24 hrs
• Paradisis 2009: 33
– RCT, 90 PT, < 6 hrs age– Predicted low SVC flow:
• < 28 wks• 28-29 wks + MAP ≥ 8 cm H2O + FiO2 ≥ 0.3
– Prophylactic milrinone vs. placebo– NS 15 ml/kg with starting milrinone– Indomethacin (if PDA > 2mm)– Dopamine for hypotension
33 Paradisis M, Evans N, Kluckow M, Osborn D. Randomized trial of milrinone versus placebo for prevention of low systemic blood flow in very preterm infants. J Pediatr 2009;154:189–95.

Hypotension During the 1st 24 hrs
• Paradisis 2009:– Maintenance of SVC flow ≥ 45 mL/kg/min was
measured by echocardiography throughout the first 24 hours.

Hypotension During the 1st 24 hrs
• Paradisis 2009:– No difference in SVC flow– Milrinone group had significantly higher HR
and lower mean BP, but no hypotension.– No difference in Dopamine use– Milrinone group had significantly larger PDA– No difference in late indomethacin use or
ligation– No difference in IVH, BPD, NEC

Assessment and monitoring of DA
• Strong disagreement on the definition of a hemodynamically significant DA (HSDA)
• Management varies accordingly across regions and even within NICUs. 34, 35
34 Amin SB, Handley C, Carter-Pokras O. Indomethacin use for the management of patent ductus arteriosus in preterms: a web-based survey of practice attitudes among neonatal fellowship program directors in the United States. Pediatr Cardiol 2007;28:193–200.
35 Hoellering AB, Cooke L. The management of patent ductus arteriosus in Australia and New Zealand. J Paediatr Child Health 2009;45:204–9.

Assessment and monitoring of DA
• Large unconstricted DA can contribute to early hypotension in VLBWI
• fECHO can easily determine DA size
• Measurement at the narrowest point

Assessment and monitoring of DA
• A DA diameter > 1.5 mm is associated with retrograde or absent post ductal aortic diastolic flow.36
• Large DA can lead to decreased lower body perfusion.37
36 Evans N, Iyer P. Longitudinal changes in the diameter of the ductus arteriosus in ventilated preterm infants: correlation with respiratory outcomes. Arch Dis Child Fetal Neonatal Ed 1995;72:F156–61.
37 Groves AM, Kuschel CA, Knight DB, Skinner JR. Does retrograde diastolic flow in the descending aorta signify impaired systemic perfusion in preterm infants? Pediatr Res 2008;63:89–94.

Assessment and monitoring of DA
• Sarkar 2007: 38
– Evaluation for early ductal shunting and closure of the ductus, if patent, should be attempted before hydrocortisone is considered in hypotensive infants with escalating needs for vasopressors.
38 Sarkar S, Dechert R, Schumacher RE, Donn SM. Is refractory hypotension in preterm infants a manifestation of early ductal shunting? J Perinatol 2007;27:353–8.

Assessment and monitoring of DA
• Currently, there is 3 practice variations:– Prophylactic treatment (within 12 h after birth)– Early targeted treatment (at 6–72 h after birth)– Treatment when clinical signs associated with
a DA appear

Assessment and monitoring of DA
• Prophylactic treatment:– No need for fECHO prior to Tx– All infants at risk for developing a HSDA will
receive treatment soon after birth.

Assessment and monitoring of DA
• Fowlie, Cochrane review July 7, 2010: 39
– Prophylactic indomethacin has short-term benefits for preterm infants including a reduction in the incidence of symptomatic PDA, PDA surgical ligation, and severe intraventricular hemorrhage.
– There is no evidence of effect on mortality or neurodevelopment.
39 Fowlie PW, Davis PG, McGuire W. Prophylactic intravenous indomethacin for preventing mortality and morbidity in preterm infants. Cochrane Database Syst Rev. 2010 Jul 7;7:CD000174.

Assessment and monitoring of DA• Fowlie, Cochrane review July 7, 2010:
Symptomatic PDA

Assessment and monitoring of DA• Fowlie, Cochrane review July 7, 2010:
PDA ligation

Assessment and monitoring of DA
• Early targeted treatment:– Select patients based on fECHO– Parameters of non-constriction
• Ductal diameter• Flow pattern or flow velocity in the duct• Turbulence in the main pulmonary artery• Reverse flow in the descending aorta• LA/Ao ratio

Assessment and monitoring of DA
• Early targeted treatment:
• Cooke, Cochrane review 2003: 40
– Indomethacin for asymptomatic patent ductus arteriosus in preterm infants
– No benefit apart from decreased incidence of symptomatic PDA and small but statistically significant decrease in the duration of requirement for supplemental oxygen
40 Cooke L, Steer P, Woodgate P. Indomethacin for asymptomatic patent ductus arteriosus in preterm infants. Cochrane Database Syst Rev. 2003;(2):CD003745.

Assessment and monitoring of DA
• Early targeted treatment:
• Aranda 2008:41
– RCT, ELBW, ibuprofen L-lysine, asymptomatic PDA
– No difference in death, IVH, NEC, daily fluid intake/output, liver function, BPD, and ROP.
– A trend toward decreased PVL was noted.
41 Aranda JV, Clyman R, Cox B, Van Overmeire B, Wozniak P, Sosenko I, et al. A randomized, double-blind, placebo-controlled trial on intravenous ibuprofen Llysine for the early closure of nonsymptomatic patent ductus arteriosus within 72 hours of birth in extremely low-birth-weight infants. Am J Perinatol 2009;26: 235–45.

Assessment and monitoring of DA
• Treatment when DA is symptomatic:– Signs and symptoms appear late– Significant steal from the lower body
circulation via a large DA might take place before signs appear.
– No study compared this approach to placebo

Assessment and monitoring of DA
• More research is needed:– Definition of a HSDA– Best timing of treatment

Assessment and monitoring of PH
• PH: increased pulmonary artery pressure according to age.
• PPHN: failure of normal pulmonary vascular relaxation at or shortly after birth.
• PPHN: combination of PH and clinical or fECHO signs of extrapulmonary shunting

Assessment and monitoring of PH
• Diagnosis by fECHO:– Using the open DA to determine the amount
and severity of the right-to-left shunt.– Systemic hypotension can influence the
results

Assessment and monitoring of PH
• Doppler measurements have been validated using cardiac catheterization.42
• A right-to-left ductal shunt > 30% of the cardiac cycle is considered significant PH
42 Musewe NN, Smallhorn JF, Benson LN, Burrows PE, Freedom RM. Validation of Doppler-derived pulmonary arterial pressure in patients with ductus arteriosus under different hemodynamic states. Circulation 1987;76:1081–91.

Assessment and monitoring of PH
• Diagnosis by fECHO:– Estimating peak velocity of the tricuspid
incompetence jet– Only validated in the absence of an
unrestricted duct

Assessment and monitoring of PH
• Diagnosis by fECHO:– Peak ejection/right ventricular ejection time
ratio– Presence of pulmonary incompetence– Direction of ventricular septal wall motion– Foramen ovale shunt direction
• Ventricular dysfunction and low CO

Assessment and monitoring of PH
• There is often a significant component of intrapulmonary shunting causing ventilation–perfusion mismatch
• Optimizing ventilation and lung volume
• It is important to diagnose severe LV dysfunction before administering iNO.

Assessment and monitoring of PH
• fECHO can identify newborns who are most likely to respond to iNO, and may guide weaning.
• fECHO can assess the response to inotrpes and inodilators.

Assessment and monitoring of PH
• Myocardial performance index and tissue Doppler of the RV may be able to differentiate an afterload effect from contractile dysfunction.
• These measurements have to be further validated

Infants with Perinatal Asphyxia
• After a hypoxic–ischemic event, newborn infants may appear pale, with weak pulses and delayed capillary refill and have persistently high or low heart rates despite effective resuscitation.

Infants with Perinatal Asphyxia• Wyckoff 2005:43
– Retrospective review of term and near term babies who needed CPR
– VE is rarely given for overt hypovolemia
– More often for asphyxiated infants who are slow to respond to intensive CPR.
– Persistent postnatal hypotension in VE infants suggests that other factors, e.g., myocardial dysfunction, may be important contributors to lack of response to CPR.
43 Wyckoff MH, Perlman JM, Laptook AR. Use of volume expansion during delivery room resuscitation in near-term and term infants. Pediatrics 2005;115:950–5.

Infants with Perinatal Asphyxia
• Transient myocardial ischemia:– Impaired LV function– Mitral and/or tricuspid regurgitation– Wall motion abnormalities of the LV– Reduced CO

Infants with Perinatal Asphyxia
• In the long axis or 4 chamber views:– LV appear dilated with diminished movement
of the ventricle wall and septum.
• In hypovolemia:– Reduced end-diastolic volume of the LV– Increased ventricular wall and septal
movement

Assessment during sepsis
• Literature in neonates is limited
• de Waal 2010:44
– Studied the central circulation in 20 preterm infants in the NICU with a suspected infection and signs of cardiovascular compromise.
– Relatively high left and right CO and low SVR.– Decrease in RVO or LVO >50% is associated
with mortality.
44 de Waal K, Evans N. Hemodynamics in preterm infants with late-onset sepsis. J Pediatr. 2010 Jun;156(6):918-22, 922.e1. Epub 2010 Mar 16.

Developing a local fECHO service
• A dedicated ultrasound machine kept in close approximation to clinical areas with unlimited access
• A core group of interested clinicians and a training and accreditation program with a commitment to continuing professional development

Developing a local fECHO service
• Support of a local pediatric cardiology service, as pediatric cardiologists are an essential part of any fECHO service, providing advice and backup when the limitations of the neonatologist are reached

Developing a local fECHO service
• As fECHO is not a consultative service, but rather used as an adjunct to clinical care, billing for a referred service is rarely relevant.

Conclusion
• fECHO provides a wealth of hemodynamic information, often different from the assumed underlying physiology when based on clinical assessment and blood pressure alone.

Conclusion
• fECHO allows targeting of cardiovascular support and monitoring of the response to treatment.

Conclusion
• Developing a fECHO service will allow collection of real time, longitudinal point of care information, assisting the clinician to understand cardiac function and hemodynamic changes.


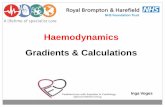
Figure 1 Shows the hypothesised direct relationship between cerebral blood flow (CBF) and mean blood pressure (MBP) with the limited dautoregulatory plateauT with a cut point below which CBF may fall with lower MBP.Evans N. Assessment and support of the preterm circulation. Early Hum Dev 2006; 82:803–10