Monitoring of bladder filling to capacity
17
Noninvasive Optical Monitoring of Bladder Filling to Capacity Using a Wireless Near Infrared Spectroscopy Device K.KEERTHI 11211A1108 DEPARTMENT OF BME 1
-
Upload
keerthi-kancharla -
Category
Devices & Hardware
-
view
39 -
download
1
Transcript of Monitoring of bladder filling to capacity
Noninvasive Optical Monitoring of Bladder
Filling to Capacity Using a Wireless Near
Infrared Spectroscopy Device
K.KEERTHI
11211A1108
DEPARTMENT OF BME1
CONTENTS
• Abstract
• Introduction
• NIRS device-Methodology
• Sensor block diagram
• Invitro setup
• Invivo setup
• Limitations
• Conclusion
DEPARTMENT OF BME
2
ABSTRACT
• Lack of bladder fullness sensation is an issue that arises in
different neurogenic conditions and in addition to influencing
patients’ quality of life, can result in serious kidney damage.
• We describe a wireless wearable sensor for detecting bladder
fullness using near infrared spectroscopy (NIRS).
• Capable of detecting changes in bladder content noninvasively.
DEPARTMENT OF BME
3

INTRODUCTION
(a) Evolution:• NIRS is a technique increasingly used in NICUs to monitor
cerebral (or peripheral) tissue oxygenation and to tailor
haemodynamic and respiratory support.
• Recently NIRS device is used to study the haemodynamics
and oxygenation of bladder and used to evaluate bladder
function in health and disease.
DEPARTMENT OF BME4
(b) Bladder Pathology
• Incontinence:It is the inability to hold urine in the bladder because voluntary
control over the urinary sphincter is either lost or weakened.
• Enuresis:
It refers to a repeated inability to control urination particularly
tourette's syndrome in children.
• Urinary retention:
It is also known as ischuria, is an inability to completely
empty the bladder.
DEPARTMENT OF BME 5
(c)Techniques:
• Ultrasonic Scanning:
This technique uses ultrasonic imaging to differentiate the
urinary bladder from surrounding tissues and organs, produce
volume information, and estimate urine level.
• Bioelectrical impedance analysis:This technique is principally used for determining extracellular
and total body water, for the changes in electrical impedance
used for detection of urine volume to be measured
DEPARTMENT OF BME6
NIRS device-Methodology
• This method employs the absorption properties of human
tissue and water in the near infrared (NIR) light wavelength
range to measure changes in water content in the field beneath
a NIRS device.
• When the bladder rises into the NIR light field as it fills, the
water in the urine it contains results in high light absorption
that generates an abrupt decrease in the light intensity sensed
returning to the NIRS device.
• This event can be set to activate an alarm.
DEPARTMENT OF BME 7
DEPARTMENT OF BME8
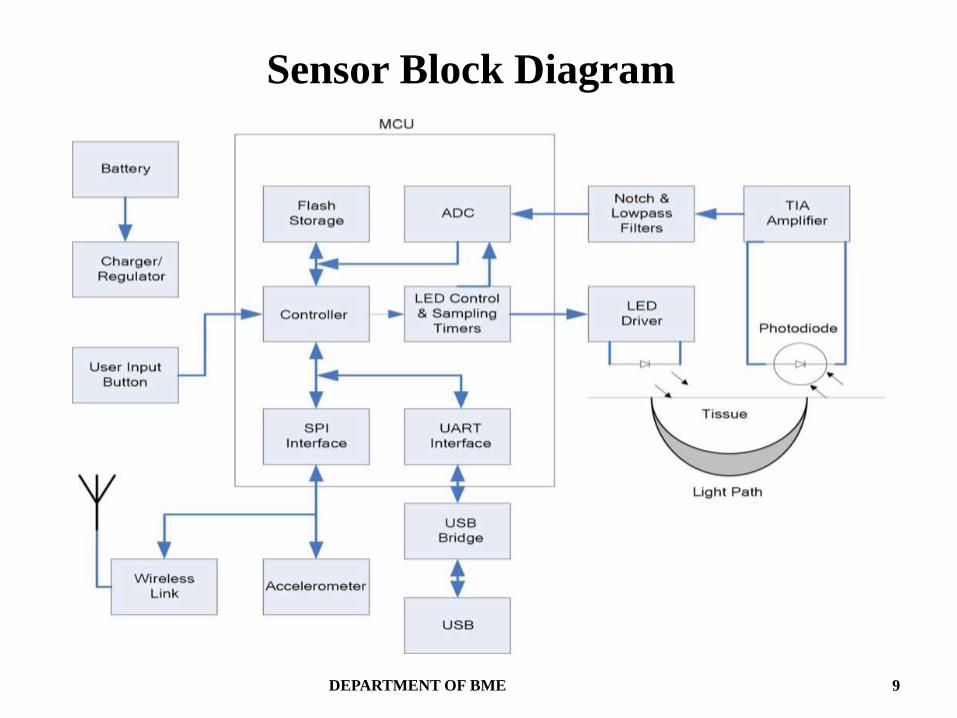
Sensor Block Diagram
DEPARTMENT OF BME 9

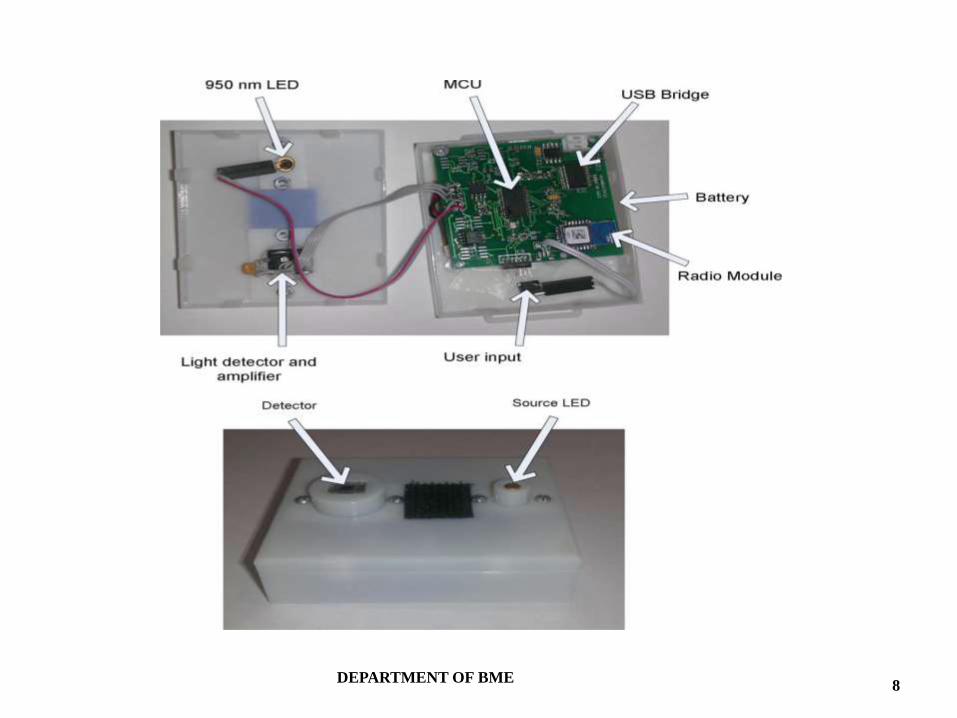
Source led:• It is a 950 nm LED.
• Driven by a constant current driver, that in turn is controlled by a hardware timer.
Light detector:
• It is a 5.22 mmsq silicon photodiode.
• Integrated with a trans.-impedance amplifier.
Filter:
• Active twin-T notch filter is used.
• Center frequency at 60 Hz
Micro-controller:
• 16-bit low power microcontroller(MSP430F2274 Texas Instruments, TX,USA)
• Running at 16MHz.
• The filter’s output is sampled by a 10-bit analog to digital converter (ADC) integrated on the MCU.
DEPARTMENT OF BME10
Battery:
• The sensor is powered by a 3.7 V, 850 mAh lithium-ion
polymer rechargeable battery.
• Provides up to 20 hours of continuous monitoring.
USB connection
Memory storage:• The sensor can log data on the 16 KB onboard flash memory
storage.• The data can be later downloaded into a PC for further
analysis.
DEPARTMENT OF BME11
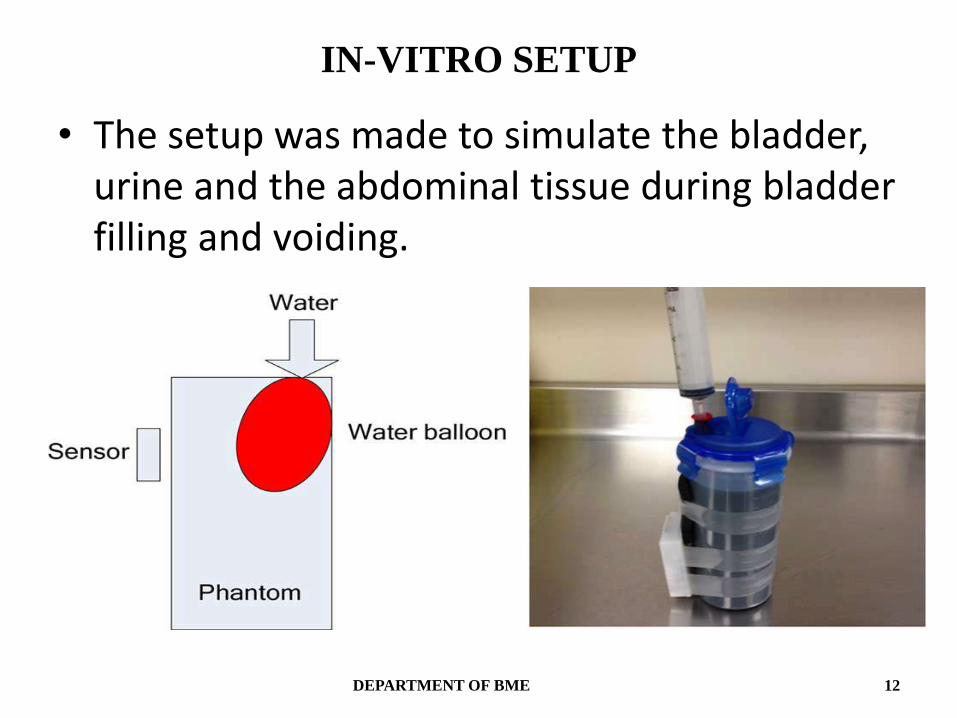
IN-VITRO SETUP
• The setup was made to simulate the bladder, urine and the abdominal tissue during bladder filling and voiding.
DEPARTMENT OF BME 12
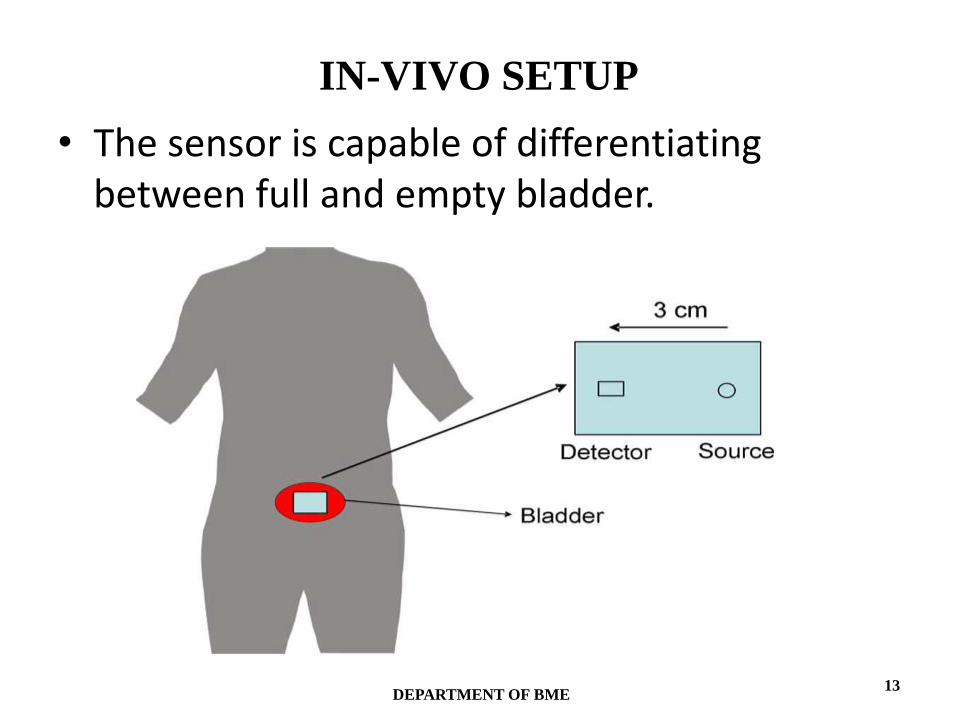
IN-VIVO SETUP
• The sensor is capable of differentiating between full and empty bladder.
DEPARTMENT OF BME13
LIMITATIONS
• Fat tissue layer under the optical opcode location for bladder.
• Output drifts due to slight temperature changes.
• Signal attenuation due to systemic interferences.
DEPARTMENT OF BME 14
CONCLUSION
• A compact wireless optical sensor prototype is designed for continuous noninvasive monitoring of the bladder in patients who are unable to sense when their bladder is full.
• The device is capable of differentiating between when the
bladder is empty or contains a small volume of urine and
when it becomes full, by using the absorption properties of
water at a wavelength of 950 nm.
• This would potentially enable patients at risk for urinary
retention to protect themselves from renal damage, elderly
subjects prone to incontinence to retain the ability to void
voluntarily, and children with problematic enuresis to become
conditioned to when they need to wake to void.
DEPARTMENT OF BME15
REFERENCES• A. Macnab and B. Shadgan, “Biomedical applications of wireless continuous wave near
infrared spectroscopy,” Biomed. Spectrosc. Imag., vol. 1, no. 3, pp. 205–222, 2012.
• A. Macnab, B. Shadgan, K. Afshar, and L. Stothers, “Near-infrared spectroscopy of the bladder: New parameters for evaluating voiding dysfunction,” Int. J. Spectrosc., vol. 2011, pp. 1–8, 2011.
• A. Macnab, B. Friedman, B. Shadgan, and L. Stothers, “Bladder anatomy physiology and pathophysiology: Elements that suit near infrared spectroscopic evaluation of voiding dysfunction,” Biomed. Spectrosc. Imag., vol. 1, no. 3, pp. 223–235, 2012.
• C. H. vander Vaart, J. R. J. de Leeuw, J. P. W. R. Roovers, and A. P. M. Heintz, “The effect of urinary incontinence and overactive bladder symptoms on quality of life in young women,” BJU Int., vol. 90, no. 6, pp. 544–549, Oct. 2002.
• S. Vaidyanathan, G. Singh, B. M. Soni, P. L. Hughes, K. F. Parsons, and P. Sett, “Vesicoureteral reflux and bladder management in spinal cord injury patients.,” Spinal Cord, vol. 40, no. 3, pp. 150–152, Mar. 2002.
• P. Petrican and M. A. Sawan, “Design of a miniaturized ultrasonic bladder volume monitor and subsequent preliminary evaluation on 41 enuretic patients.,” IEEE Trans. Rehabil. Eng., vol. 6, no. 1, pp. 66–74, Mar. 1998.
DEPARTMENT OF BME 16

DEPARTMENT OF BME17