Molecular Diagnosis of Infectious...
70
Molecular Diagnosis of Infectious Diseases Gregory J. Tsongalis, Ph.D. Professor of Pathology Director, Molecular Pathology Dartmouth Medical School Dartmouth Hitchcock Medical Center Norris Cotton Cancer Center Lebanon, NH
Transcript of Molecular Diagnosis of Infectious...

Molecular Diagnosis of Infectious Diseases
Gregory J. Tsongalis, Ph.D.
Professor of Pathology
Director, Molecular Pathology
Dartmouth Medical School
Dartmouth Hitchcock Medical Center
Norris Cotton Cancer Center
Lebanon, NH

*
DHMC, Lebanon, NH
*
Boston, MA
CANADA
California
Flo
rida
Texas

The Human Genome Project
February 2001
A major impact on microbial genomics.

• 1995, first complete genome sequence of a free-living organism, Haemophilus influenzae
• Since then 1,554 complete bacterial genomes
• Species pangenome contains set of core genes that are common and set of dispensable genes that are absent in at least one strain.
• Approximately 90% of bacterial genome codes for protein whereas <2% of human genome codes for protein
Relman DA. N Engl J Med 2011;365:347-357
Microbial Genomics

Why Molecular Pathology? • Genetics
• previously unavailable tests
• carrier detection
• risk assessment
• Infectious diseases
• turn-around time
• inability to culture
• microscopic interpretation and competency
• quantitative analysis
• genotyping
• Heme/Oncology
• confirmation
• minimal residual disease
• therapeutics
• Identity testing
• most polymorphic molecule
• Therapeutics/PGx

Applications of Molecular Analyses to
Infectious Diseases
• Qualitative detection
• Quantitative detection
• Identification/speciation
• Microbial “Identity” Testing
• Genotyping/Drug Resistance

Molecular Infectious Disease (Molecular Testing Methods)
• Nucleic acid (DNA, RNA) specimens:
• Blood
• CSF
• Tissue (fresh, frozen FFPE)
• Urine
• Stool
• Amniotic fluid
• Other body fluids
• Microbial isolate

Nucleic Acid Extraction Technologies
1980- Manual Extractions:
1. Make your own buffers
2. pH your own buffers
3. Lab math
4. TAT = 1.5 days
5. Low throughput
2000- Automated Extractions:
1. Reagent contracts
2. Consumables
3. Maintenance contracts
4. TAT = 20-45 minutes
5. Higher throughput

Automation of NA Extraction
Extracton Type Instrument
Magnetic silica particles COBAS AmpliPrep, EZI,
MagnaPure Compact and
LC, Maxwell 16, NucliSens
EasyMag
Magnetic charge switch particles iPrep Purification Instrument
Silica vacuum manifold plate 6100/6700 Automated
Nucleic Acid Workstation,
QIAxtractor
Iron oxide particles m2000sp
Silica spin columns QIAcube
Persing, et.al. 2011. Molecular Microbiology – Diagnostic Principles and Practice (2nd Ed.) C. Hill, p123.

Extraction Issues to be Considered
• Specimen type
• Extraction Method
• Inhibitors
• Target sequences (DNA vs RNA)
• Controls (type and number)

Nucleic acid probes for culture confirmation and direct
detection (DNA and RNA probes)
Nucleic acid amplification (“NAT”) technologies
– Sequence amplification
• Polymerase chain reaction (PCR) and real time PCR
• Transcription-mediated amplification (TMA and NASBA)
• Strand displacement amplification (SDA)
• Ligase chain reaction (LCR)
• Loop-Mediated Isothermal Amplification (LAMP)
– Signal amplification
• Branched-chain DNA (bDNA)
• Hybrid capture
• Invader (Cleavase)
Sequencing – Sanger or Next Generation
Microarrays and Mass Spectrometry
Molecular Infectious Disease (Molecular Testing Methods)

Sample
Preparation Amplification Detection
Controls for Qualitative Molecular Diagnostic Testing
1. 2. 3. Extraction control
(pre- or post-)
Blank control
Negative control
Positive control
Internal amplification control (IAC)
(competitive vs non-competitive) efficiency inhibitors
?

Real-Time PCR
Permits rapid target Id; <30 min
Eliminate post-PCR processing
Highly specific; Hybridization probes
Allows multiplexing
Permits quantification
Signal intensity is directly proportional to the amount of
amplified DNA
Threshold cycle (Ct) determination; the cycle at which
target is first detected

Detection Chemistries
Intercalating/binding dyes
–SYBR® green I
Dual label probes/ Quenched probes
-TaqMan® (5’ nuclease assay)
-Molecular beacons, Scorpions
-FRET probes

Increase in Reporter Signal “Reports”
Amplification of Target

Ct: Primary Signal Analysis
Threshold Line
Threshold
penetration
Threshold Cycle
Threshold Value

Melt Curve Analysis
• Following amplification temperature is slowly increased (ie. 60oc to 95oc, 0.2oc/sec)
• Strands denature
• Dye released, fluorescence decreases
• Melting curve; Temperature (x) vs. Fluorescence (y)
• Tm function of %GC and length

Melt Curve Analysis
Phase Transition
Target
Primer dimer

Melt Curve Analysis
BKV JCV

Sample
Preparation Amplification Detection/Analysis
PCR Testing Steps
Automated extraction + Real Time PCR = STAT DNA Analysis

• Positive or negative
• Increased sensitivity
• Decreased TAT
• Low to high throughput
• Becoming more automated
• Applications are limitless but questionable
clinical utility
• Major impact with real time PCR
Molecular Infectious Disease (Qualitative)

• Misperception of prevalence
• Asymptomatic
• Non-specific symptoms
• Coinfections
• Unreliable diagnostic tests
• Asymptomatic individuals serve as a
reservoir of infection
Issues: high volume, STD (social), high throughput
“THE SILENT EPIDEMIC”
Qualitative Molecular Infectious Disease Testing
(Chlamydia trachomatis)

Abbott LCx® System
Sample Prep Amplification Detection
LCx®
Analyzer LCx®
Thermocycler

LCR Amplification
(LCx® MEIA System)
MEIA particle linked to enzymatic
conversion
of fluorescent dyes


BD Viper (ProbeTec System)
GenProbe TIGRIS DTS

Assay Gene Target NAAT Amp. Control
M2000 v2
(Abbott)
Plasmid (2 targets) Real-time
PCR
Yes
ProbeTec
(BD)
Plasmid SDA Yes
Hybrid Capture II
(Digene)
Plasmid and
genome
Hybridization No
PACE 2 CT
(Gen-Probe)
23S rRNA Hybridization No
Aptima Combo 2 23S rRNA TMA No
Aptima CT 16S rRNA TMA No
TaqMan48 v2 Plasmid and omp1 PCR Yes
Molecular Infectious Disease Molecular Diagnostic Methods for C. trachomatis

• Home brew (Laboratory Developed Tests)
• Analyte Specific Reagents
• Primers > PCR > Gel
• Real time PCR
• Near patient testing???
Qualitative Molecular Infectious Disease Testing (Non-Kit Based Assays)

1.
2.
Bam HI-W repetitive region (296 bp)
Conserved Among EBV Strains
Qualitative Molecular Infectious Disease Testing (EBV)

NE
GA
TIV
E
PO
SIT
IVE
SP
EC
IME
N 1
SP
EC
IME
N 1
SP
EC
IME
N 2
SP
EC
IME
N 2
DN
A M
AR
KE
R
EBV BETA-ACTIN

Real Time PCR Detection of EBV
EBV DNA,
5000, 500, 50 and 5
copies/ml
Target gene = BNT p143ORF38

• PCR is both sensitive and specific
• Viability (post treatment still detectable)
• Use of multiple primer sets
• Specimen types for PCR testing
• Nasopharyngeal swab (Dacron not Ca alginate
or use of a mucolytic agent to avoid PCR
inhibition)
• Other specimens may serve as alternatives
• Other laboratory testing (Culture or DFA)
• Bordet and Gengou (Starch Blood Agar)
• Antibiotic selection plate (Cephalexin)
• Synthetic media
Molecular Infectious Disease (Bordetella pertussis)

Bordetella Target Genes
IS481 500-1,000 present not present present
IS1001 10-20 not present present present
PTxs1 1 present present not present
pertussis parapertussis holmesii Copy#

• Specimen types
• Extraction efficiencies
• Automation vs manual
• Importance of controls
• Assessing performance characteristics
– Sensitivity, specificity, precision, accuracy
– Limit of blank, limit of detection
• Armbruster and Pry. Clin Biochem Rev 2008;29 (Si):S49-
S52
• Regulatory: FDA vs ASR vs RUO
Qualitative Molecular Infectious Disease Testing
(What did we learn?)

• How much is present
• Limit of quantification (LoQ)
• Automation
• Low to high throughput
• Which applications are clinically relevant
• Is the LLoQ the same as LoD?
• Why quant vs qual?
Molecular Infectious Disease (Quantitative)

Qualitative Genotyping Quantitative
Molecular Infectious Disease (HIV-1)

HIV-1 Subtypes
• Group M (Major)
– Subtypes A - H
• Group O (Outlier)
• Group N (New)

HIV-1 Viral Load Testing
• Not diagnostic (?)
– Designed to monitor infection
– Sensitivity may be higher than proviral DNA PCR
• Indications
– Disease progression
– Prognosis
– Response to antiviral agents
• 0.5 log10 units is considered clinically significant

Molecular Assays for the Qualitative Detection of HIV-1 RNA
Assay Method Target Application
COBAS® AmpliScreen
HIV-1 Test, v1.5 (IVD)
RT-PCR HIV-1 gag gene Qualitative detection of
viral RNA from plasma,
organs and tissues
COBAS®
AmpliPrep/COBAS®
TaqMan® HIV-1
Qualitative Test (RUO)
PCR HIV-1 gag gene Qualitative detection of
HIV-1 RNA and proviral
DNA in plasma,
anticoagulated fresh
whole blood and dried
blood spots
COBAS® TaqScreen
MPX Test (IVD)
PCR Multiple Simultaneous testing
for multiple viruses in a
single sample: HIV-1
group M, HIV-1 group
O, HIV-2, HCV and
HBV

Molecular Assays for Quantification of HIV-1 RNA Assay Method Target Dynamic Range
(copies/mL)
Roche Amplicor HIV
Monitor v1.5 test,
Standard (IVD)
RT-PCR HIV-1 gag gene 400 – 750,000
Roche Amplicor HIV
Monitor v1.5 test,
Ultrasensitive (IVD)
RT-PCR HIV-1 gag gene 50 – 100,000
Roche Cobas
AmpliPrep/Cobas TaqMan
HIV Test v.1.0 (IVD)
Real-time PCR - TaqMan HIV-1 gag gene
48 – 10,000,000
Roche Cobas
AmpliPrep/Cobas TaqMan
HIV Test v.2.0
(IVD)
Real-time PCR - TaqMan
HIV-1 gag gene, LTR 20 – 10,000,000
Siemens Versant HIV RNA
3.0 Assay (IVD)
bDNA HIV-1 pol gene 75 – 500,000
Biomerieux NucliSENS
EasyQ® HIV-1 V2.0 (RUO)
NASBA HIV-1 gag gene 25 – 10,000,000
Abbott RealTime HIV-1
Assay (IVD)
Real-time PCR
HIV-1 integrase gene 40 – 10,000,000

Viral Load Testing –
Interpretation of Results
• Results should be presented as Log10 Values
– Prevents clinicians from over interpreting small variations
in viral load
• Changes in viral load must exceed 0.5 log10 (3 fold)
to represent biologically relevant changes in viral
replication
• Due to differences in performance, viral load should
be quantified at follow-up by the same version of the
same assay that was used initially

Viral Load Testing –
Interpretation of Results
• Clinical infections can increase viral load by
as much as 1 log
– HSV infections
– Opportunistic infections
– Vaccinations
• Influenza
• Tetanus
• Pneumococcal
– Viral load testing should not be performed for
1 month following such infections

Patient Monitoring
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50
5.00
5.50
6.00
1/99 2/99 3/99 5/99 8/99 12/99 4/00 5/00 9/00 2/02 6/02 7/02 8/02
Initiate Rx
Resistance Testing
Vir
al L
oad
(lo
g10
co
pie
s/m
l)
1. Compliance
2. Resistance

HIV-1 Resistance Genotyping
• Determine the sequence RT and protease genes
VGI (FDA approved), ABI, laboratory developed
• Compare sequence to wild type virus Identify mutations
• Associate mutations with resistance Knowledge of genetics of resistance
Data base, rules based system
Different interpretations of same mutations

Viral Genotyping –
Antiretroviral Resistance Testing
FDA Approved Systems Assay Name Manufacturer Methodology
Truegene HIV-1
Genotyping Kit
Siemens Medical
Solutions Diagnostics,
Tarrytown, NY
DNA Sequencing
(polyacrylamide gel
electrophoresis)
ViroSeq HIV-1
Genotyping System
Abbott Molecular, Des
Plaines, IL
DNA Sequencing
(Capillary
electrophoresis)

Viral Genotyping

The BK Virus
• BKV is a member of the polyomavirus family.
• BKV typically presents with respiratory infection and about
80% of adults are seropositive for BKV antibodies.
• After primary infection, the virus enters a latent phase in the
kidneys, brain, and uterus.
• The virus usually remains dormant but may reactivate during
pregancy, HIV infection, diabetes, or after transplant surgery.

Rejected kidney transplant exhibiting BK nephropathy
and chronic rejection.
BKV Reactivation with Immunosupression
• Following Bone Marrow Transplant Hemorrhagic
Cystitis
• Following Renal Transplant polyomavirus-
association nephropathy (PVAN or BKVN)

Typical intranuclear inclusion pre- and post- micro-dissection
a b

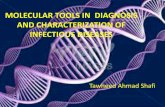
Melt Curve Analysis for BKV/JCV From Microdissected Samples
B
0
20
40
60
80
100
120
140
78.1 78.9 79.7 80.4 81.3 82.1 82.9 83.7 84.5 85.2 86.0 86.9
Temperature
-dF
/dT
27412 Glom
27412 Tubules
BK Virus
JC Virus
NTC
A
0
20
40
60
80
100
120
140
78.1 78.9 79.7 80.4 81.3 82.1 82.9 83.7 84.5 85.2 86.0 86.9
Temperature
-dT
/dT
14084 Glom
14084 Tubules
BK virus
JC virus
NTC
Adeyi OA, Belloni DR, Dufresne SD, Schned AR, Tsongalis GJ.
Real-time polymerase chain reaction and laser capture microdissection techniques
in the diagnosis of BK virus infection of renal allografts.
Am J Clin Pathol 124(4):537-542, 2005

Monitoring with PCR
• BK Viruria and Viremia relatively frequent in
immunosuppressed renal transplants
• Positive PCR results alone not very useful
• Quantitative Testing (real-time PCR)
– BKV levels over time
– With viral level cut-offs BKV PCR useful for
determining PVAN (Viscount 2007):
• In Urine: 100% Sensitivity; 78% Specificity
• In Plasma: 100% Sensitivity; 91% Specificity

Requirements for BKV PCR
• Quantitative
• Analytic Specificity: Only detects BKV
• Analytic Sensitivity: Low limit of detection?
• Wide dynamic range (concentrations above
10 log10 copies/mL)
• Specimen type: Urine and plasma

Plasma MGB vs. Eragen Assays

Urine MGB vs Eragen Assays

BKV PCR Obstacles
• No FDA-approved assays (IVDs): must use
laboratory-developed tests (with ASRs)
• No international standards defining BKV
concentrations
• Limited options for calibrators for standard
curve-Lack of standarization

BKV PCR Obstacles
• Urine specimens can be difficult: PCR
inhibitors
• Assay should be specific for BKV but detect
various strains of BKV equally (robust vs
stringent)
– Gene target
– Primer/probe location

• Performance
• Variants
• Clinical implications
• QC of numerical data
• Automation
Quantitative Molecular Infectious Disease Testing
(What did we learn?)

So what is next in molecular infectious
disease testing?

• Gram positive
• Bacillus (coccobacillus , “diphtheroid”)
• Anaerobe
• Non-spore forming
• Slow grower
• Non-motile
• Many strains are indole & catalase positive
• Frequent contaminant of blood cultures.
Diagnostic challenges of
Propionibacterium acnes
McPherson: Henry's Clinical Diagnosis and Management by
Laboratory Methods, 22nd ed. 2011 Saunders Elsevier
Accessed Online, 8/31/11.
Isabella Martin, M.D.

Habitat

• Three categories:
– Acnes in teenagers & adults.
– Invasive deep-seated infections
• Pacemakers, valves, shunts.
– Surgical wound infections
• Prosthetic joints, spinal hardware.
Infections
Mandell, Douglas, and Bennett's Principles and
Practice of Infectious Diseases, 7th ed. 2009
Churchill Livingstone Accessed online 8/31/2011.
Clinicaladvisor.com Accessed online 8/31/11.

Orthopaedics Quandary
1-2
years
- +
Revision
Arthroplasty
Removal of
hardware
Ultra-sound
guided joint
aspiration
with culture
6 Wks IV
Antibiotics
Implantation
of new
hardware
Oops!
+ -
Good

• Real time PCR Taqman assay.
• Quantitative
– Ct – detect contamination.
• Internal control: beta-actin?
• Multi-plexed?
PCR for P. acnes

The Automation Revolution Continues -2011
BD MAX™ System
(HandyLab Jaguar)
1.fully automates cell lysis,
nucleic acid extraction,
PCR set-up, amplification
and detection
2.24 samples per run
Enigma Diagnostics
Enigma ML
1. portable
2. self-contained
3. ultra-rapid,
laboratory-
standard results
4. point-of-care
testing

Smaller is Better
Idaho Technologies
Film Array
IQuum
Liat Analyzer

PathoGenetix
An automated system for identification and strain typing of pathogens in complex
sample types.
Does not require specific reagents for detection of each pathogen, this approach
uses a single reagent set to create genomic barcodes which are then used to
detect and identify thousands of strains from hundreds of species.
No PCR or other amplification technique is applied.
Genome Sequence Scanning (GSS) technology. GSS enables high throughput,
single molecule DNA analysis to be used for pathogen identification and
characterization in complex biological samples.

Biocartis
Compact platforms whose ease of use will lower the entry barrier to
diagnostic testing.
Developing a platform that integrates sample preparation of nucleic acids,
amplification, detection, and the generation of a result without user
intervention and a detection platform that includes encoded micro carriers, a
micofluidic cartridge, and an instrument for low to high multiplexing
detection of biomarkers.

Lumora
BART (Bioluminescent Assay in Real-Time) is a novel reporter system which is
used with isothermal nucleic acid amplification technologies.
Easy-to-use, affordable, robust hardware.

What if………..
• Miniaturize
• Low cost
• Fast
• Multiplex
• Smart phone
ready

DHMC Molecular Pathology Laboratory and
Translational Research Program
Samantha Allen
Betty Dokus
Susan Gallagher
Carol Hart
Arnold Hawk
Claudine Lefferts, Ph.D.
Joel Lefferts, Ph.D.
Rebecca O’Meara
Elizabeth Reader
Mary Schwab
Heather Steinmetz
Laura Tafe, M.D.
Brian Ward
Eric York