
Mofussil Dispensary Practice - pdfs.semanticscholar.org · cancer of the breast, stated to have...
4
Transcript of Mofussil Dispensary Practice - pdfs.semanticscholar.org · cancer of the breast, stated to have...
MOFUSSIL DISPENSARY PRACTICE.
By Surgeon W. J. Moore, L.R.C.P.,
Rajpoot ana Political Agency, and Superintendent General of Dispensaries, llajpootana.
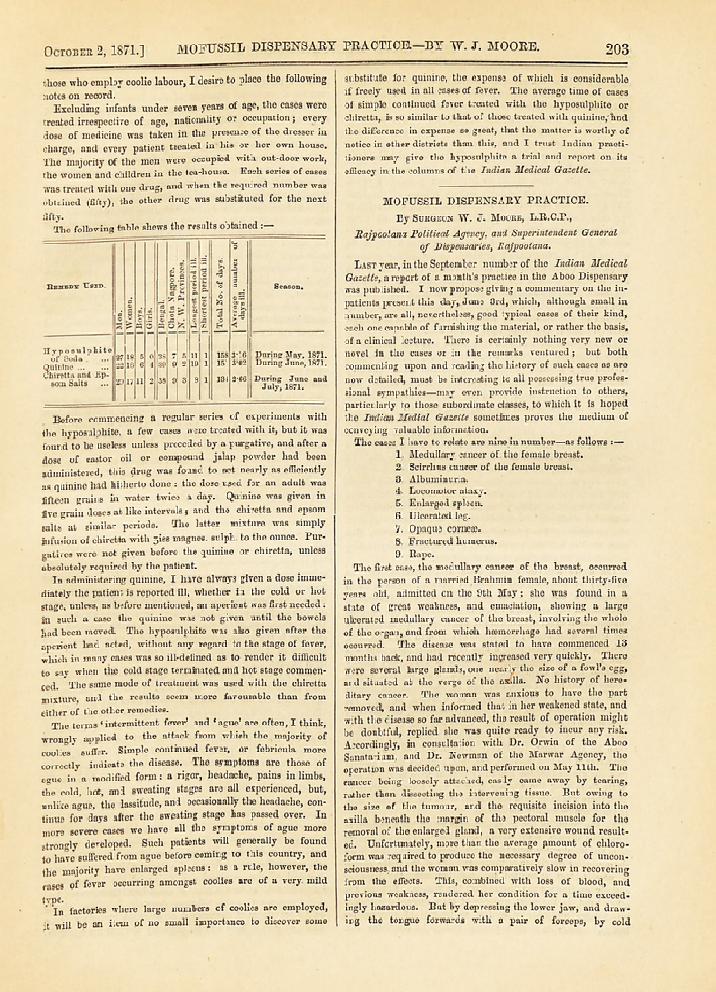
Last year, in the September number of tlie Indian Medical
Gazette, a report of a month's practice in the A boo Dispensary was published. I now propose giving a commentary on the in-
patients present this day, June 3rd, which, although small in number, are all, nevertheless, good typical cases of their kind, each one capable of furnishing the material, or rather the basis, of a clinical lecture. There is certainly nothing very new or novel in the cases or in the remarks ventured ; but both,
commenting upon and reading the history of such cases as are now detailed, must be interesting to all possessing true profes- sional sympathies?may even provide instruction to others, particularly to those subordinate classes, to which it is hoped the Indian Medial Gazette sometimes proves the medium of
conveying valuable information. The cases I liave to relate are nine in number?as follows :?
1. Medullary cancer of the female breast. 2. Scirrlius cancer of the female breast.
3. Albuminuria.
4. Locomotor ataxy. 5. Enlarged spleen. 6. Ulcerated leg. 7. Opaque cornea). 8. Fractured humerus.
9. Eape. The first case, the medullary cancer of the breast, occurred
in the person of a married Brahmin female, about thirty-five years old, admitted on the 9th May; she was found in a
state of great weakness, and emaciation, showing a largo ulcerated medullary cancer of the breast, involving the whole of the organ, and from which haemorrhage had several times occurred. The disease was stated to have commenced 13
months back, and had recently increased very quickly. There
were several large glands, one nearly the size of a fowl's egg, and situated at the verge of the axilla. No history of here-
ditary cancer. The woman was anxious to have the part
removed, and when informed that in her weakened state, and
with the disease so far advanced, the result of operation might be doubtful, replied she was quite ready to incur any risk.
Accordingly, in consultation with Dr. Orwin of the Aboo
Sanatarium, and Dr. Newman of the Marwar Agency, the
operation was decided upon, and performed on May lltli. The
cancer being loosely attached, easily came away by tearing, rather than dissecting the intervening tissue. But owing to
the size of the tumour, and the requisite incision into the
axilla beneath the margin of the pectoral muscle for the
removal of the enlarged gland, a very extensive wound result-
ed. Unfortunately, more than the average pmount of chloro- form was required to produce the necessary degree of uncon-
sciousness, and the woman was comparatively slow in recovering from the effects. This, combined with loss of blood, and previous weakness, rendered her condition for a time exceed- ingly hazardous. But by depressing the lower jaw, and draw- ing the tongue forwards with a pair of forceps, by cold
204 THE INDIAN MEDICAL GAZETTE. [October 2, 1871.
effusion, and by arrack given at intervals, re-action was establish- ed, but removal from the recumbent position on the operating table was not considered safe for some hours afterwards. Since
the day of operation the progress, excepting the formation of an abscess in the axilla, was altogether satisfactory, and the woman left, cured, on the 9th June.
2. Omlee, also a Brahmini, aged 35, married, with children, was admitted on the 27th April with a large open scirrlius
cancer of the breast, stated to have been growing 4 years.
There was no glandular enlargement or oedema of the arm. The growth was removed by Dr. Newman, and, differently to the encephaloid tumour, required dissection from the fibres
of the pectoral muscle. The diseased condition of the sur-
rounding integument demanded the incisions being widely made, so that the resulting wound, although not extending into the
axilla, was scarcely less than in the former case. There was
also, in consequence of the intimate connection with surround-
ing tissue, much more haemorrhage, six ligatures being required. But the woman, being stronger, and not more than ordinarily affected by the chloroform, was never depressed so as to cayse anxiety. She is now (June 12th) nearly well. The after-treatment in both these cases was the same :r-the
edges supported by broad strips of plaster, and the ,W9und covered by a dressing of olive oil and carbolic acid. The only inedicine given was morphia in grain doses, at night. The
women, being Brahmins, would not take meat soup, although, especially in the first case, sadly requiring support. The size of the wounds in these cases induced me to apply
grafts of skin, taken from the arms of male relatives, in the first case, on the 13th and 21st days, in the second, on the 12th day. Although immediately applied, and retained in situ with the greatest care, neither of the portions of integument united. They were each about the size of four-anna bits, and where
they lay in the wound was afterwards marked by a bluish spot, the only result of their presence. It may be, probably, the cancex-ous diathesis is unfavourable to union, otherwise, with the exception of too profuse secretion of matter in the first
case, we had a clean, granulating, apparently healthy-looking surface, and all other favourable conditions. The above are two typical cases of their kind, and no
difficulty of diagnosis could possibly present. The general conditions of the two forms of cancer were well illustrated, excepting in one respect, afterwards mentioned. The scirrlius
tumour, as is usual in that disease, was more firmly attached to the tissue underneath ; the medullary growth was loose, and, although scarcely presenting a cyst or investing membrane?as seen round a similar tumour removed in 1870, very loosely attached to the surrounding textures. The scirrlius cancer
presented the ragged edge, and base of prominent red ulcera- tions characteristic of this form of diseased matter ; the
medullary cancer had the sloughy, unhealthy, degenerating appearance of fungus hcematodes. There was also, as customary, more debility or cachexia in the system affected by the latter, than by the former. The only departure from the typical character of the two maladies, was, that, contrary to the general rule, the glands near the medullary tumour were most affected, while those near the seirrhus growth were scarcely enlarged :
also, there was more pain complained of in the first case, than
in the second?usually the reverse. As the result of the great attention which has been paid to
cancerous disease, many morbid growths have been separated from the number f6rmerly thought to be malignant. But with
the increasing conviction of the incurability of the latter, cancer is now seldom submitted to operation with the hope of
entirely eradicating the disease from the system. But, on the other hand, in the great majority of cases successful operative interference undoubtedly confers an interval of comparative health, diminishes suffering and materially lengthens life.
Statistics inform us that the average duration of life after
removal of cancerous tumours of the breast, is twenty-four months, but there are instances on record where disease did not recur after removal, and a still greater number where it did not
return for many years. The duty of operating, therefore, ap- pears altogether unquestionable. The existence of cancerous tubercles in the skin over a
cancer, the implication of neighbouring glands, and adhesion to the pectoral muscles, have been generally advanced as
reasons forbidding the use of the knife. But with regard to
the first condition, I fail to see why it should constitute any
objection to operation. Authors ?who desire us not to operate in such cases, do not hesitate recommending interference when the cancer is an open one ; or in other words, when the tuber- cular spots have ulcerated, and even the skin containing them has disappeared. Neither does it seem that considerable
glandular implication must necessarily stay the hands of the
surgeon. For in the first case detailed, glandular enlargement was a very prominent feature, the large gland removed, pre-
senting the dark blue appearance of fungus hcematodes; and several smaller ones, not removed, subsiding altogether after
operation. In the last case, again, the diseased growth was quite attached to the adjacent muscular structure. Yet both cases were eminently successful. With regard to other points connected-with the history of cancer, it may be mentioned
that both sufferers were married women, and in neither could
any hereditary taint be discovered :?thus apparently not
supporting the frequently expressed opinion of cancer being more prevalent among the unmarried, and always furnishing the history of hereditary taint.
3. Albuminuria.? Boonna, male, set. about 40, was admitted May 13tli, in a condition of general anasarca, which he states
commenced in the lower extremities ten weeks back. He also
shows a large scrotal but reducible hernia, and largo liaeuior-
rhoidal swelling round the anus. The heart's action is natural, but there is some dulness and crepitation about the lower lobes of both lungs. No enlargement of the liver or spleen is discern- ible. Urine contains a considerable percentage of albumen, but is free from uriniferous tubes on examination under the
microscope. This case was treated by elaterium, given every morning, first in quarter grain, half grain, and eventually grain doses. At the same time, six ounces of arrack were allowed
daily as a stimulant, and iodine paint applied over the kidneys. Under these remedies, the anasarca gradually subsided, the albumen in the urine disappeared, and the man became to all appearance, although still weak and somewhat emaciated, free from disease.
Now, was this a pure case of Bright's disease or albuminuria ? I am inclined to think so. But if so, the total disappearance of the oedema and the absence of albumen from the urine is re-
markable, even if these healthy conditions are only temporary ; for in my experience, cases of albuminuria so far advanced, generally proceed from bad to worse.' My impression is, that the condition of the kidneys was one of acute congestion, which subsided under the treatment afforded, but which has probably left changes in those organ? which will ultimately result in chronic Bright's disease.
As a general rule, there is nothing different in albuminuria
presenting in this country, to a similar class of cases at home.
But, contrary to the prevailing idea, or at least, what used to be the prevailing idea, albuminuria is, in India, quite as common as in colder climates, although more often complicated with other maladies, as of liver and spleen, which also producing dropsical effusion, cause the condition of the kidneys to be
ignored or to occupy a place of secondary importance. And
this frequency of renal affection depends, I believe, chiefly on the prevalence of paroxysmal, or so-called mnlarious fever, which appears to have a direct tendency towards the establish-
October 2, 1871.] MUFUSSIL DISPENSARY PRACTICE.-BY TV. J. MOORE. 205
ing of that particular state of kidney, constituting Brigiit's affections. The varying condition, and the varying quantity of the urine, during a paroxysm of ague, and the fact that albumen is often present at such times?according to Solons in one-fourth the number of cases presenting?is evidence that the
kidneys participate, perhaps more tlian most other organs, in that congestion marking the cold stage. As this matter is im-
portant under many aspects, and as the intimate connection, as a, sequel, of albuminuria with paroxysmal fever, is scarcely recognized, or but lightly touched upon in all medical works, I venture to quote the following observations from my essay on Malarious Fevers, published in the 21st and 22nd vol. of the Indian Annals of Medical Science (vide p. 281, vol. 22.)
" It has already been remarked that affections of the kidney characterized by albuminuous urine, may be excited by the congestions taking place in the kidneys, in common with all abdominal organs, during paroxysmal fever. And these may be of two kinds?either temporary congestion, passing away in the course of a few days or weeks, or the chronic form, terminating in the deposition between the cortical and tubular structures, attended, perhaps, with absorption of the renal
tissue proper. Frequent attacks of congestion gradually and
imperceptibly lay the foundation of the chronic malady. The
latter, however, may arise as a result of chronic malarious
degeneration, without the additional exciting cause of prior fever paroxysms. It is well known that impure air and other unwholesome influences to which the inhabitants of large towns are subjected, are fertile predisposing causes of one or
other of the forms of albuminuria. And in India, we have added another debilitating agent in the presence of malaria. If the urine passed during or immediately after a fever
paroxysm is examined, it will very frequently, indeed, show
evidence of albumen. When fever becomes habitual or of
frequent recurrence, albumen is more constantly present. In
the more severe forms of malarious cachexy, albuminous urine
is quite as often present as absent. As an examination of the
urinary secretion in such cases is not a common practice, the passing of albumen during these maladies is not recognized as an ordinary occurrence. But any medical man may satisfy himself as to the correctness of these statements by applying the albumen tests. When there is tendency to the scrofuious diathesis in a constitution deteriorated by malarious cachexy, the kidney affection may be foretold with almost certainty. Or, if iu Europe an individual has suffered from albuminous
urine, consequent either on congestion or more chronic con- ditions, the recurrence of the malady, under malarious in-
fluences, is most probable. I mention this with emphasis, because it is diametrically opposed to the opinions entertained
but a decennial period past. Change to semi-tropical or even
tropical climates, was commonly regarded as beneficial in
Bright's disease. The question sometimes presenting, whether a person once the subject of this malady, should or should not proceed to India, has, I have reason to know, been decided in the affirmative by eminent living physicians. Some, indeed, have even recommended the change. Experience has, how- ever, convinced me that tropical, semi-tropical and malarious countries, should be forbidden lands to all who have ever
passed albumen in the urine ; unless as an accidental occur-
rence depending on errors of diet. If the kidney has been once congested or inflamed, or if chronic degeneration has
commenced, the danger of confirmed albuminuria, result-
ing from paroxysmal fever or malarious cachexia, is great
indeed. The idea once prevalent at home, that albumi-
nuria is not a malady of hot climates, is totally erroneous.
It is as common, if not more so, in India as in England.
This lias, indeed, been admitted since the publication of Moorhead's work. But this author, while attempting the elaboration of an etiology for the malady, almost altogether ignores malarious influences. The influences of occupation, of vicissitudes of temperature, of spirits, opium, and gunjah, are noted as they deserve ; but the powerful actions of congestive fever and malarious cachexia are allotted a very minor posi- tion. It is certainly difficult to separate the effects of malaria from the other causes named, as they are so frequently com-
bined ; but there can be little doubt that the deleterious
results of malaria, either through the actual fever paroxysm or
through malarious cachexia, are more than sufficient to coun- terbalance any advantage derived from residence in a tropical climate. In the latter, either with natives or Europeans, the actual exposure to vicissitudes of weather, or to cold, may be
less; the liabit3 of drinking spirits, specially gin, may not
prevail, and scarlatina, so frequently the forerunner of albumi-
nuria, may be unknown, but notwithstanding sucli conservative
influences, the tendency to disease of the kidneys is more than
equalized in India by the constant presence of malaria. " The symptoms of albuminuria, as it occurs in its chronic
form, as a consequence of malarious cachexia, are,?obscure
pains in the loins, frequent micturition, especially at night, and more confirmed debility. The urine is generally scanty, as-
sumes a muddy appearance, has a low specific gravity, and furnishes albumen by the usual tests." When the peculiar cachexia, the result of Bright's disease,
is recollected?the uraernic blood poisoning, with its dropsical, cerebral, cardiac, and other secondary affections?the exceeding gravity of the complication of albuminuria and malarious
cachexia will be admitted.
4. The instance of locomotor ataxy occurred in the person of a man, aged about 40, and is reported to have been gradual in its approach during some years back. On admission, on the 9th
May, the state of the patient was very characteristic. The
awkward unsteady gait, as if the lower extremities to the loins were stiff, or as of a person trying to walk on his heel3 without
bending his knees, was sufficient to point the diagnosis. As
often happens in these cases, the gait and some emaciation
were the only recognizable symptoms. In other respects, the man appeared in good health, without urinary, abdominal, thoracic or any other affection, and without evidence of any
diseased condition of the spinal column to be derived from
manipulation. This patient was treated with strychnine, and during the
first three or four weeks was evidently much benefited, walking stronger and even gaining flesh. But he is still in hospital, and no improvement has latterly taken place.
5. The case of enlarged spleen, in the person of a man,
aged 35, was also a typical instance of the kind. Without a
history of severe febrile attacks, tlie man confesses to have
been out of health for some years past, the spleen having been observed large during the past eighteen months. The patient ?
was evidently the subject of masked malarious fever, with its
sequelaj of enlarged sploen, and general anaemic and leucoey- thaemic condition. On admission, the bulging of the spleen was easily discernible by the naked eye, and its edge coulcl be felt far below the margin of the ribs. There was also some
slight degree of ascites, but no oedema of the feet. Previ- ous to applying at the dispensary, the man had been sub-
jected by some village " hakeem" to the universal panacea of
this part of the country, or " dagh," by burning and sooring the integument over the part affected by hot irons. The treatment pursued in the dispensary was the biniodide of
mercury ointment, as recoinmeuded by Macnamara, followed

206 THE INDIAN MEDICAL GAZETTE. [October 2, 1871.
by pressure over the organ, made with strips of plaster and a bandage, with some quinine and opium internally. Under
these measures, three weeks sufficed to render the splenic pro- minence invisible, and in two more weeks the patient left, fancying himself well, although the organ could be felt still
unduly prominent. In the treatment of these cases of enlarged spleen, I cannot
say I have found the biniodide ointment always successful.
In some instances it has appeared to do little good, and in
the case reported, I am disposed to place change of atmosphere from his village, 20 miles distant, in the first category of
curative agents ; the tonics exhibited, doubtless excited some influence on the general system, and the bandage probably aided subsidence of the enlarged organ. The plaster mentioned is only used as a means of inducing confidence, and there-
from the application of the roller; as not understanding the effects of pressure, many persons would have little faith in
such an apparently simple measure, as the application of a common bandage.?{To be continued.")


















