MODULE 3 1/113 Module 3: Treatment of BPH J. Curtis Nickel, MD, FRCSC Program Chair, Chief Editor...
113
MODULE 3 1/113 Module 3: Treatment of BPH J. Curtis Nickel, MD, FRCSC Program Chair, Chief Editor Professor of Urology, Department of Urology Queens University Kingston General Hospital Kingston, Ontario
-
Upload
ronnie-barnes -
Category
Documents
-
view
215 -
download
0
Transcript of MODULE 3 1/113 Module 3: Treatment of BPH J. Curtis Nickel, MD, FRCSC Program Chair, Chief Editor...

MODULE 3
1/113
Module 3: Treatment of BPH
J. Curtis Nickel, MD, FRCSCProgram Chair, Chief EditorProfessor of Urology, Department of UrologyQueens UniversityKingston General HospitalKingston, Ontario

MODULE 3
2/113
3.1 Learning Objectives
After reviewing this module, the learner will be better able to:
1. Describe the lifestyle modifications that are appropriate for men with BPH
2. Identify the appropriate candidates and best practices for the conservative approach of watchful waiting
3. Describe options for the pharmacological treatment of men with LUTS
BPH = Benign Prostatic Hyperplasia, LUTS = Lower Urinary Tract Symptoms

MODULE 3
3/113
After reviewing this module, the learner will be better able to:
4. Identify the indications for minimally invasive surgical therapies that are appropriate for the treatment of men with moderate to severe LUTS, who request Minimally Invasive Surgical Therapies (MIST)
5. Describe the surgical options for the treatment of men with BPH and bothersome moderate to severe LUTS who request active therapy
BPH = Benign Prostatic Hyperplasia, LUTS = Lower Urinary Tract Symptoms

MODULE 3
4/113
3.2 Introduction
Treatment of BPH is based primarily on symptomatology:
the severity of symptoms and the bother that they cause to the patient’s QoL
The risk of progression of symptoms, complications, and the need for surgery must be assessed when deciding upon treatment.
The goal of treatment is 2-fold:
1. to improve symptoms
2. to delay disease progression
BPH = Benign Prostatic Hyperplasia; QoL = Quality of Life

MODULE 3
5/113
Current guidelines recommend a formal symptom inventory to accurately assess the severity of symptoms and guide treatment choices:1,2
International Prostate Symptom Score (IPSS) / American Urological Association (AUA) Symptom Score
1. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003;170(2 Pt 1):530-47.2. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.

MODULE 3
6/113
Once severity, bother, and risk are assessed, then patient preference becomes one of the most important determinants of treatment
The benefits and harm of BPH treatment options should be explained to all patients who are bothered enough to consider therapy, and patients should be invited to participate as much as possible in the choice of treatment 3
Even patients with severe symptoms may decide to choose a less effective therapy against their physician’s advice, if they feel there is less risk
3. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.BPH = Benign Prostatic Hyperplasia

MODULE 3
7/113
The decision to Treat BPH: 4,5
Symptom severity and discomfort brings the patient to the physician
Bother of symptoms leads to treatment
Risk assessment directs the physicians treatment recommendations
The patient makes an informed choice regarding treatment
4. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003;170(2 Pt 1):530-47.5. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.BPH = Benign Prostatic Hyperplasia

MODULE 3
8/113
Canadian BPH Guidelines:6
“Treatment choices should be governed both by the severity of the symptoms, bother and patient preference. Such a decision depends upon patients being sufficiently informed about treatment options, and the harms and benefits of such treatment.”
6. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.BPH = Benign Prostatic Hyperplasia

MODULE 3
9/113
Treatment Options
Mild or minimally bothersome symptoms
may only require lifestyle modification with watchful waiting
For moderate or severe BPH (AUA/IPSS score ≥8): 7
lifestyle modifications with watchful waiting
medical therapy (e.g. alpha-blockers and/or 5-reductase inhibitors)
minimally invasive therapies (e.g., transurethral needle ablation)
surgery (e.g., transurethral resection of the prostate)
7. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.BPH = Benign Prostatic Hyperplasia; AUA = American Urological Association; IPSS = International Prostate Symptom Score

MODULE 3
10/113
Over the last two decades, treatment options for men with BPH have expanded significantly
Use of α1-blockers in ameliorating BPH symptoms is now accepted clinical practice
Introduction of 5α-reductase inhibitors and emergence of clinical evidence on their use has resulted in a paradigm shift from an emphasis on symptomatic treatment to the prevention of clinical progression in men with BPH
Parallel technological developments have introduced minimally invasive surgical procedures with less risk and comparable results to traditional surgery
Along with the conservative approach to therapy, this chapter will review these therapeutic options
BPH = Benign Prostatic Hyperplasia

MODULE 3
11/113
3.3 Deciding on a Treatment Approach and Counseling the Patient
Choosing a treatment strategy for BPH can be a difficult task
This should be a joint process involving both physician and patient
For the most severely affected patient, the obvious option may be limited to surgery
However, for most men, the clinician must balance the relative benefits and risks of each treatment option and discuss them thoroughly with the patient
Consulting the evidence regarding the benefits and risks of each treatment will enable wise treatment decisions
BPH = Benign Prostatic Hyperplasia

MODULE 3
12/113
Table 3.1 Evidence TableMEDICAL OPTIONS SURGICAL OPTIONS
Watchful Waiting
α1Blocker
5α-Reductase Inhibitor
Balloon Dilation TUIP Open
Surgery TURP
Chance for Improvement of Symptoms (90% confidence interval)
31 - 55 59 - 86 54 - 78 37 - 76 78 - 83 94 - 99.8 75 - 96
Degree of Symptom Improvement (% reduction in symptom score)
< 32 51 31 51 73 79 85
Morbidity / Complications Associated with Surgical or Medical Treatment (90 % confidence interval) Assume that about 20% of all complications are significant
1 - 5Complica-tions from
BPH progression
2.9 - 43.3 13.6 - 18.8 1.78 - 9.86 2.2 - 33.3
6.98- 42.7
5.2 - 30.7
Chance of Dying within 30-90 Days of Treatment (90% confidence interval)
.8Chance of death < 90d for 67 yo man
0.72- 9.78Pat. treated were high risk/elderly
0.2 - 1.5
0.99- 4.56
0.53 - 3.31
Risk of Total Urinary Incontinence(90% confidence interval)
?Incontinence due to aging ? 0.06 -
1.10.34- 0.74
0.68 - 1.4
Need for Operative Treatment for Surgical Complications in the Future (90% confidence interval)
0 ? 1.34 - 2.65
0.6 - 14.1
0.65 - 10.1
Adapted from Roehrborn CG. BPH: From treatment to prevention: A change in paradigm prevention. AUA 2005.TUIP = Transurethral Incision of the Prostate TURP = Transurethral Resection of the Prostate

MODULE 3
13/113
In a study where 74 men with BPH were given questionnaires, over half of patients were significantly concerned about the prospect of acute urinary retention and over two thirds were significantly concerned about the prospect of surgery 8
However, more patients considered that the insertion of a catheter for acute urinary retention would be a problem and more detrimental to their QoL than surgery 3
8. Nickel JC. Can J Urol. 1999;6:819-822. BPH = Benign Prostatic Hyperplasia; QoL = Quality of Life

MODULE 3
14/113
Issues to discuss with the patient:
Severity of symptoms
Extent to which symptoms adversely affect the patient’s QoL (i.e., “bother”)
Risk of BPH progression
Risk of prostate cancer
Long-term efficacy and retreatment rate of each therapeutic option
Realistic expectation of improvement
Likelihood of treatment-associated morbidity or complications
Patient preference
Financial considerations
QoL = Quality of Life; BPH = Benign Prostatic Hyperplasia

MODULE 3
15/113
If the patient achieves a good understanding of why they are being given a particular treatment for BPH and the likely outcomes, they are much more likely to adhere to the treatment
BPH = Benign Prostatic Hyperplasia

MODULE 3
16/113
2005 Canadian Guidelines for the Management of BPH
Published June 2005, in The Canadian Journal of Urology 9 (See Module 4)
These guidelines stress that information on the benefits and harms of BPH treatment options should be explained to all patients who are bothered enough to consider therapy
The guidelines urge physicians to invite patients to participate as much as possible in the choice of treatment
9. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.BPH = Benign Prostatic Hyperplasia

MODULE 3
17/113
Canadian BPH Guidelines:10
“Information on the benefits and harms of BPH treatment options should be explained to all patients who are bothered enough to consider therapy. Patients should be invited to participate as much as possible in the treatment choice.”
10. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.BPH = Benign Prostatic Hyperplasia

MODULE 3
18/113
3.4 Lifestyle Modification with Watchful Waiting
Lifestyle modification with watchful waiting is the first consideration in discussions of treatment strategies for BPH and the preferred management strategy for men with mild symptoms (AUA symptom score <8) or men who have moderate-to-severe symptoms (AUA symptom score ≥8) but are not yet bothered by their symptoms or have not yet developed complications of BPH 11
11. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.AUA = American Urological Association; BPH = Benign Prostatic Hyperplasia

MODULE 3
19/113
Watchful Waiting In Canada, the treatment strategy of lifestyle modification with
watchful waiting is often a shared responsibility between the urologist and family physician 12
Patients on watchful waiting should have periodic physician-monitored visits to watch for progression, and physicians should identify patients at risk
They can use baseline age, the severity of LUTS, and serum PSA values to advise patients of: 13
risk of symptom progression
acute urinary retention
future need for BPH-related surgery
monitor risk for development of prostate cancer12. Nickel JC, Saad F. Can J Urol 2004;11:2186-93. p2189 13. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.LUTS= Lower Urinary Tract Symptoms; PSA = Prostate-Specific Antigen; BPH = Benign Prostatic Hyperplasia

MODULE 3
20/113
Lifestyle Modification
Physicians should advise all patients that certain lifestyle modifications may help to alleviate bothersome mild-to-moderate symptoms 14
14. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.

MODULE 3
21/113
Canadian BPH Guidelines:15
A variety of lifestyle changes may be suggested for patients with non-bothersome symptoms, including:
Fluid restriction in the evening
Avoiding irritating foods or beverages, e.g., alcohol or caffeine
Avoiding or monitoring certain drugs, e.g., diuretics, decongestants, antihistamines, antidepressants
Timed or organized voiding (bladder retraining)
Pelvic floor exercises
Avoiding or treating constipation
15. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.

MODULE 3
22/113
3.5 Pharmacological Therapy
Medical treatment options for BPH have expanded over the past two decades, providing physicians and patients with more choices
Several factors influence the choice of medical therapies versus MIST or surgery, including: 16
Nature and extent of symptoms
Extent to which symptoms are bothersome and affect the patients’ QoL
Whether urine flow is significantly reduced and associated with an appreciable volume of PVR urine
Complications of BPH (e.g. obstructive renal failure, bladder stones, chronic urinary tract infections, prostate related bleeding)
Patient preference
16. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p38MIST = Minimally Invasive Surgical Therapies; PVR = Post-Void Residual Urine; QoL=Quality of Life

MODULE 3
23/113
Alpha 1 (α1)-adrenoceptor Blockers
α1-adrenergic receptors mediate tension in smooth muscle tissue surrounding the prostate stroma, urethra, and bladder neck
Rationale of α1-adrenoceptor blocking agents:
by inhibiting these receptors, muscular tone along these tissues will be reduced, allowing for easier passage of urine and the reduction of LUTS 17
17. Leveillee R. Benign Prostatic Hyperplasia. eMedicine. http://www.emedicine.com/med/topic1919.htm. Accessed June 5, 2005LUTS = Lower Urinary Tract Symptoms

MODULE 3
24/113
2 6 12
11.5
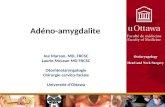
Figure 3.1 α-Adrenoceptors1
α1Aα1B α1D
0
6.5
7.5
8.5
9.5
10.5
Alfuzosin
TamsulosinMea
n T
ota
l S
ymp
tom
S
core
Buzelin JM, et al. Br J Urol 1997;80:597-605
Prostate Peripheral LiverSpleen Bladder
Vasoconstriction

MODULE 3
25/113
α1 Receptor Blockers Approved in Canada
Currently, there are four α1 receptor blockers approved in Canada for the treatment of BPH:
Terazosin
Doxazosin
Tamsulosin
Alfuzosin
The use of prazosin not approved for BPH in Canada, nor is it recommended 18
18. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.

MODULE 3
26/113
α1 receptor blockers that are selective for the α1A subtype may have a potential therapeutic advantage mainly in terms of tolerability (less effect on blood pressure)
Tamsulosin
Currently the only α1 receptor blocker that targets selectively the α1A receptor which is predominant in the prostate
Alfuzosin
Non-specific α1 receptor blocker
Shows preferential distribution in the prostate in patients with BPH
This preference distribution may play a role in the functional uroselectivity reported with α1 receptor blocker
Terazosin and doxazosin are not uroselective

MODULE 3
27/113
The four recommended α1-receptor blockers are believed to have equal clinical effectiveness, partially relieving symptoms of LUTS
On average, they produce a 4- to 6-point improvement in the IPSS
Patients generally regard this improvement as a meaningful change 19
α1-receptor blockers relax the contraction of smooth muscle in the bladder neck and prostatic urethra by blocking the α1-adrenoreceptors
19. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003.LUTS = Lower Urinary Tract Symptoms; IPSS = International Prostate Symptom Score

MODULE 3
28/113
The primary side effects of α1-receptor blockers are 20
Orthostatic hypotension
Dizziness
Tiredness (asthenia)
Ejaculatory problems
Nasal congestion
20. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003.

MODULE 3
29/113
Slight differences in the adverse-event profiles of the four recommended agents:
Tamsulosin: appears to have a lower probability of orthostatic hypotension but a higher risk of ejaculatory problems than other α1-receptor blockers
Doxazosin: In men with hypertension and cardiac risk factors, doxazosin has been associated with a higher incidence of congestive heart failure than other antihypertensive agents and this agent should not be assumed to constitute optimal hypertension management in men with concomitant LUTS 21
21. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003.LUTS = Lower Urinary Tract Symptoms

MODULE 3
30/113
α-Blockers: Overview
Similar efficacy
Efficacy remains long-term (5-year data is currently available)
Difference between α1-adrenoceptor blockers is related to the side effect profile (uroselective agents are better tolerated)
Alfuzosin and tamsulosin appear to be better tolerated than doxazosin and terazosin
Roehrborn CG. Urol 2001;58(Suppl 6A):55-64

MODULE 3
31/113
Canadian BPH Guidelines:22
“Although there are differences in the adverse-event profiles of these agents, the Committee believes that all four agents have equal clinical effectiveness. Choice of agent should depend on patient’s comorbidities, side effect profiles, and tolerance.”
22. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.BPH = Benign Prostatic Hyperplasia

MODULE 3
32/113
5α-Reductase Inhibitors
Unlike α1-receptor blockers, 5α-reductase inhibitors address the underlying pathophysiology of BPH, shrinking the prostate size and reversing the clinical progression
BPH = Benign Prostatic Hyperplasia

MODULE 3
33/113
5-Reductase Inhibitors: Overview
Types:
Finasteride and Dutasteride
Improves LUTS in men with large prostate (DRE, PSA, TRUS)
Reduces risk of acute retention and surgery
Has long latency period before effect
Reduces PSA (50% at 6 months to one year)
Alters sexual function in some men
Gurunadha Rao Tunuguntla HS. Clin Geriat 2002;10(5):20-5; Kasraeian A. www.dcmsonline.org; Gormley GJ, et al. NEJM 1992;327:1185-91
LUTS = Lower Urinary Tract Symptoms, DRE = Digital Rectal Examination, PSA = Prostate-Specific Antigen TRUS = Transrectal Ultrasound of the Prostate

MODULE 3
34/113
The 5α-reductase inhibitors act by inhibiting the enzyme, 5α-reductase, which occurs as two isoforms, 5α-reductase types 1 and 2
These enzymes convert testosterone to dihydrotestosterone (DHT), which binds to receptors on prostatic cell nuclear membranes and stimulates prostate tissue growth (see Module 1)

MODULE 3
35/113
In addition to preventing disease progression, 5α-reductase inhibitors increase peak urinary flow rate and reduce BPH symptoms
The average patient will experience a 3-point reduction of AUA symptom scores
This improvement can be greater in men with larger prostates
5α-reductase inhibitors are not appropriate treatments for men with LUTS who do not have clinical evidence of prostatic enlargement
These agents do not appear to be as effective for symptomatic relief as α1-receptor blockers 23,24
23. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p4324. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p44AUA = American Urological Association ; LUTS = Lower Urinary Tract Symptoms

MODULE 3
36/113
Figure 3.2 Finasteride 5mg Daily, 12-months
Adapted from McConnell JD, et al. NEJM 1998;338(9):557-63
0
Mean Change
a) Symptom Score
-0.5-1-1.5-2-2.5-3-3.5
1
2
3
4
Year
Finasteride
Placebo

MODULE 3
37/113
1
2
3
4
Year
Finasteride
Placebo
0-5 5 10 15-10-15-20-25Mean Change (%)
b) Prostate Volume
Adapted from McConnell JD, et al. NEJM 1998;338(9):557-63
Figure 3.2 Finasteride 5mg Daily, 12-months

MODULE 3
38/113
00.5 1 1.5 2 2.5
1
2
3
4
Year
Finasteride
Placebo
Mean Change (mL/sec)
c) Maximal Urinary Flow Rate
Adapted from McConnell JD, et al. NEJM 1998;338(9):557-63
Figure 3.2 Finasteride 5mg Daily, 12-months

MODULE 3
39/113
Long-term clinical trials have shown that, due to the progressive nature of BPH, 5α-reductase inhibitors can prevent BPH-related complications, such as acute urinary retention and the need for surgery25
25. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003.BPH = Benign Prostatic Hyperplasia

MODULE 3
40/113
Currently, two 5α-reductase inhibitors are available: finasteride and dutasteride
Finasteride specifically blocks 5α-reductase type II, whereas dutasteride blocks both isoforms
Randomized clinical trials have shown that both agents have similar efficacy in reducing prostatic size and preventing disease progression
Both produce similar improvements in AUA symptom scores/IPSS and urinary flow rates. They have a similar safety profile 26
The side effects of each agent will be discussed in the following sections
26. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003.AUA = American Urological AssociationIPSS = International Prostate Symptom Score

MODULE 3
41/113
Table 3.3 Clinical Efficacy of 5-Reductase Inhibitors is Similar*
*Not from a comparative trial.** McConnell JD et al. NEJM. 1998;338:557-563. *** Roehrborn C et al. Urology. 2002;60:434-441.AUR = Acute Urinary Retention; IPSS = International Prostate Symptom Score
Finasteride**
48-Mo Controlled Trial in 3,040 Men
Dutasteride***
24-Mo Controlled Trial in 4,325 Men
Finasteride Placebo Dutasteride Placebo
Volume changes -18% +14% -26% -2%
IPSS reduction -3.3 -1.3 -4.5 -2.3
Qmax improvement (mL/sec) +1.9 +0.2 +2.2 +0.6
AUR risk reduction 57% 57%
Surgery risk reduction 55% 48%

MODULE 3
42/113
Table 3.4(a) Adverse Events of 5α-Reductase Inhibitors Are Similar*
Finasteride** Placebo
Year 1 (% of Patients)
Years 2-4 (% of
Patients)
Year 1 (% of Patients)
Years 2-4 (% of Patients)
Erectile dysfunction 8.1 5.1 3.7 5.1
Altered libido 6.4 2.6 3.4 2.6
Ejaculatory disorder 0.8 0.2 0.1 0.1
Gynecomastia and breast tenderness
0.4 0.7 0.1 0.3
*Not from a comparative trial.
** McConnell JD et al. NEJM. 1998;338:557-563.

MODULE 3
43/113
Table 3.4(b) Adverse Events of 5-Reductase Inhibitors Are Similar*
Dutasteride*** Placebo
Month 0-6(% of Patients)
Month 7-12 (% of
Patients)
Month 13-18 (% of Patients)
Month 19-24 (% of Patients)
Erectile dysfunction4.71.7
1.41.5
1.00.5
0.80.9
Altered libido3.01.4
0.70.6
0.30.2
0.30.1
Ejaculatory disorder1.40.5
0.50.3
0.50.1
0.10.0
Gynecomastia and breast tenderness
0.50.2
0.80.3
1.10.3
0.60.1
*Not from a comparative trial.
*** Roehrborn C et al. Urology. 2002;60:434-441.

MODULE 3
44/113
5α-Reductase Inhibitors (5 ARIs) Are Similarly Effective in Treating BPH
Both 5 ARIs (finasteride and dutasteride) have similar efficacy and safety profiles
They improve symptoms and flow rate and shrink prostate volume by 15-25%, onset 3-6 months
They decrease the risk for acute urinary retention (AUR) and surgery
Adverse events are mainly sexually related
Effect in general is greater in patients with larger glands or higher PSA values
Serum PSA is reduced by ~50% requiring adjustment (multiplication x 2 of PSA) after 6 months of treatment
PSA = Prostate-Specific Antigen

MODULE 3
45/113
Single Versus Dual Inhibition
A comparison of data from two studies done in different populations is difficult at best, incorrect at worst
However, in regards to most BPH related measures single and dual 5 AR inhibition achieve similar clinical results
Current data suggests that the additional reduction of serum DHT with dual inhibition does not translate into greater clinical efficacy
Intraprostatic DHT data for the 0.5 mg dutasteride dosage is not available
BPH = Benign Prostatic HyperplasiaDHT = Dihydrotestosterone

MODULE 3
46/113
Canadian BPH Guidelines:27
“5α-reductase inhibitors are not appropriate for men with LUTS who do not have clinical evidence of prostatic enlargement.”
27. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.DHT = DihydrotestosteroneLUTS = Lower Urinary Tract Symptoms

MODULE 3
47/113
Finasteride
Shown to reduce prostate volume by approximately 20% and improves both symptom scores and peak urine flow rate 28
After 1 year of treatment, symptom scores improve by approximately one-third and peak urine flow increases by 1.3 to 1.6 mL/second
In one study, peak urine flow increased by 2.3 mL/second after 4 years of treatment with finasteride 29
The clinical effects of finasteride often become evident after 3 to 6 months of treatment, and patients with large prostates and serum PSA values >1.4ng/mL seem to derive the most benefit 30,31
28. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p4429. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p4430. McConnell JD et al. N Engl J Med. 1998;338:557-63.31. Roehrborn CG et al for the PLESS Study Group. Urology 1999;53(3):473-80PSA = Prostate-Specific Antigen

MODULE 3
48/113
Figure 3.3 PLESS Design
4-year studyCompleted trial (n=1000)
4-year studyCompleted trial (n=883)
Randomization (n= 3040)
Finasteride 5mg/day (n=1524)
Visit every 4 months: BPH symptom score, urinary flow rate Outcomes (BPH-related surgery & urinary
retention) and safety assessment
Annual visit: Physical examination, laboratory testing Prostate volume (subset, n=157)
Placebo (n=1516)
Visit every 4 months: BPH symptom score, urinary flow rate Outcomes (BPH-related surgery & urinary
retention) and safety assessment
Annual visit: Physical examination, laboratory testing Prostate volume (subset, n=155)
Moderate to severe symptoms of BPH, Decreased Urinary Flow Rate, Enlarged Prostate on DRE
Screening PSA and prostate biopsy for patients with PSA between 4.0 to 9.9 ng/mL, symptom score, urinary flow rate, prostate volume (subset)
1-month placebo run-in period (single blind) Baseline measurements
Adapted from McConnell JD et al. N Engl J Med 1998; 338(9):557-63BPH = Benign Prostatic Hyperplasia; DRE = Digital Rectal Examination; PLESS = Proscar Long-term Efficacy & Safety Study; PSA = Prostate-Specific Antigen

MODULE 3
49/113
Figure 3.4 Effect of Finasteride on Development of AUR Through 4 years in PLESS
Years
15
Pro
bab
ilit
y o
f A
UR
(%
)
1 2 3 40
3
6
9
12
Placebo
Finasteride 5mg o.d.
57% Risk
Reduction*p<0.001
*At year 4; 95% confidence interval: 40-69%
Adapted from McConnell JD et al. N Engl J Med 1998;338(9):557-63.AUR = Acute Urinary Retention; PLESS = Proscar Long-term Efficacy and Safety Study

MODULE 3
50/113
Figure 3.5 Effect of Finasteride on Development of BPH-Related Surgery Through 4 years in PLESS
Years
15
*At year 4; 95% confidence interval: 41-65%
Pro
bab
ilit
y o
f S
urg
ery
(%)
1 2 3 40
3
6
9
12
Placebo
Finasteride 5mg o.d.
55% Risk
Reduction*p<0.001
Adapted from McConnell JD et al. N Engl J Med 1998;338(9):557-63.AUR = Acute Urinary Retention; PLESS = Proscar Long-term Efficacy and Safety Study

MODULE 3
51/113
Figure 3.6 MTOPS: Study Design Multicenter, double-blind, placebo-controlled, randomized trial Mean follow-up 4.5 years Primary study endpoint: Overall clinical progression* of BPH
*defined as an increase of ≥ 4pts over baseline in AUA symptom score, AUR, urinary incontinence, renal insufficiency, or recurrent urinary tract infection.**8-35 points during pilot phase, *** Qmax=maximal urinary flow rate†Participants were titrated upto 8mg. Those not able to tolerate 8mg received 4mg. Those not able to tolerate either dosage were counted as having discontinued doxazosin.MTOPS=Medical Therapy of Prostatic Symptoms TrialAdapted from McConnell JD et al. N Engl J Med 2003;349:2385-96.
- Men ≥ 50 years of age- AUA symptom score 8-30 points**- Qmax*** 4-15mL/s- Voided volume ≥ 125mL
Entry Criteria:
Randomized (n=3047)
Finasteride 5mg o.d. (n=768)
Doxazosin†
4mg or 8mg o.d. (n=756)
Combination Therapy
Finasteride 5mg o.d. and Doxazosin†
4mg or 8mg o.d. (n=786)
Placebo (n=737)

MODULE 3
52/113
MTOPS
The primary outcome defined was overall clinical progression of BPH
DRE, measurements of serum PSA and urinalysis were performed annually
Prostate volume was assessed by transrectal ultrasonography, once at baseline and at the end of Year 5 or at the end of the study follow-up, whichever came first
Mean follow-up was 4.5 years in the full-scale study and 6.0 years in the pilot phase 35
35. PROSCAR Product Monograph. Merck Frosst Canada & Co. 2004MTOPS = Medical Therapy of Prostatic Symptoms; DRE = Digital Rectal Examination; PSA = Prostate-Specific Antigen

MODULE 3
53/113
Figure 3.7 MTOPS: Reduction in Risk of AUR
*Risk Reduction: Finasteride vs. Placebo (0.2 vs 0.6 events/100 person-years, p=0.009)
**Risk Reduction: Combination Therapy vs. Placebo (0.1 vs 0.6 events/100 person-years, p<0.001)
Adapted from McConnell JD et al. N Engl J Med 2003; 349:2385-96
Finasteride (5mg o.d)
YEARS0
1.5
2.0
2.5
3.0
Cu
mu
lati
ve I
nci
de
nce
of
Acu
te
Uri
nar
y R
eten
tio
n (
%)
0.0 0.5 1.0 1.5 2.0 2.53.0 3.5 4.0 4.5
5.0 5.5
68*% 81**%
1.0
0.5
Table of values (Number of Men at Risk) Follows†Defined as the inability to void (AUR in men with an obvious precipitating cause, such as anesthesia, was included as a primary outcome only after a voiding trial without a catheter was unsuccessful).
Cumulative Incidence of †AUR over a mean follow-up of 4.5 years
CombinationTherapy (Finasteride 5 mg o.d + Doxozosin 4mg or 8mg o.d)
Placebo
Doxazosin (doubled each week beginning at 1mg o.d until 4mg or 8mg o.d)

MODULE 3
54/113
Figure 3.8 MTOPS: Reduction in Need for Invasive Therapy
YEARS0
2
4
6
8
Cu
mu
lati
ve I
nci
de
nce
of
Inva
sive
T
her
apy
(%)
0.0 0.5 1.0 1.5 2.0 2.53.0 3.5 4.0 4.5
5.0 5.5
64*% 67**%
*Risk Reduction: Finasteride vs. Placebo (0.5 vs 1.3 events/100 person-years, p<0.001)
**Risk Reduction: Combination Therapy vs. Placebo (0.3 vs 1.3 events/100 person-years, p<0.001)
Adapted from McConnell JD et al. N Engl J Med 2003; 349:2385-96
Table of values (Number of Men at Risk) Follows
Cumulative Incidence of BPH Invasive Therapy† over a mean follow-up of 4.5 years
†Invasive Therapy: Transurethral prostatectomy, transurethral incision of the prostate, laser therapy, stenting, open prostatectomy, and transurethral microwave therapy.
CombinationTherapy (Finasteride 5 mg o.d + Doxozosin 4mg or 8mg o.d)
Placebo
Doxazosin (doubled each week beginning at 1mg o.d until 4mg or 8mg o.d)
Finasteride (5mg o.d)

MODULE 3
55/113
Figure 3.9 MTOPS: Reduction in AUA Symptom Scores
p=0.001
p=0.001
p<0.001 p=0.006
p<0.001
p<0.001
0
-2
-4
-6
-8
-4.9
-5.6
-6.6
-7.4
Mea
n C
han
ge
fro
m B
asel
ine
Combination Therapy**
Finasteride 5mg o.d.*
Doxazosin 4mg to 8mg o.d.*
Placebo
Adapted from McConnell JD et al. N Engl J Med 2003; 349:2385-96
*Once Daily**Finasteride 5mg & Doxazosin 4mg
to 8mg o.d.
Mean Reduction in AUA Symptom Score from Baseline at Year 4
MTOPS=Medical Therapy of Prostatic Symptoms Study; AUA = American Urological Association

MODULE 3
56/113
There is no evidence of increased adverse experiences with increased duration of treatment with finasteride. The incidence of new drug related sexual adverse experiences decreased with duration of treatment 38
38. PROSCAR Product Monograph. Merck Frosst Canada & Co. 2004

MODULE 3
57/113
Dutasteride
Due to its dual inhibition of both isoforms of 5α-reductase enzyme, dutasteride exhibits greater suppression of DHT than finasteride. 39
However, the clinical relevance of this is unknown
In three 2-year, placebo-controlled studies (n=4325), dutasteride achieved a statistically significant improvement in symptom scores and urine flow, compared to placebo. 40 Men with larger prostate volumes benefited most
DHT = Dihyrdotestosterone39. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. Fifth edition. Oxford: Health Press, 2005, p4640. AVODART® Product Monograph. GlaxoSmithKline 2003

MODULE 3
58/113
Dutasteride
Dutasteride has also been shown to reduce the BPH-related risks of acute urinary retention and need for surgery by 48 and 57%, respectively 41
The incidence of impotence, decreased libido, and ejaculatory disorders with dutasteride is similar to finasteride. In clinical trials, breast enlargement and nipple tenderness occured in 1 to 1.9% of patients each year 42
41. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. Fifth edition. Oxford: Health Press, 2005, p4642. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. Fifth edition. Oxford: Health Press, 2005, p46BPH = Benign Prostatic Hyperplasia

MODULE 3
59/113
Combination Therapy
There is a strong rationale for combining drugs with different mechanisms to treat a single disease
For example, bronchodilators and inhaled steroids are often used together to treat asthma, and coronary heart disease is commonly treated with drugs that lower cholesterol, inhibit angiotensin II, decrease blood pressure, and increase high-density lipoprotein cholesterol
This rationale has also proven to be valid for treating BPH
BPH = Benign Prostatic Hyperplasia

MODULE 3
60/113
The 5-year MTOPS study demonstrated that the combination of an α1-receptor blocker (doxazosin) and a 5α-reductase inhibitor (finasteride) was more effective than either drug alone in delaying the clinical progression of BPH and improving LUTS and flow rate 43
43. McConnell JD et al. N Engl J Med. 2003;349:2387-98.MTOPS = Medical Therapy of Prostatic Symptoms; BPH = Benign Prostatic Hyperplasia; LUTS = Lower Urinary Tract Symptoms

MODULE 3
61/113
Figure 3.8 MTOPS: Reduction in Need for Invasive Therapy
YEARS0
2
4
6
8
Cu
mu
lati
ve I
nci
de
nce
of
Inva
sive
T
her
apy
(%)
0.0 0.5 1.0 1.5 2.0 2.53.0 3.5 4.0 4.5
5.0 5.5
64*% 67**%
*Risk Reduction: Finasteride vs. Placebo (0.5 vs 1.3 events/100 person-years, p<0.001)
**Risk Reduction: Combination Therapy vs. Placebo (0.3 vs 1.3 events/100 person-years, p<0.001)
Adapted from McConnell JD et al. N Engl J Med 2003; 349:2385-96
Table of values (Number of Men at Risk) Follows
Cumulative Incidence of BPH Invasive Therapy† over a mean follow-up of 4.5 years
†Invasive Therapy: Transurethral prostatectomy, transurethral incision of the prostate, laser therapy, stenting, open prostatectomy, and transurethral microwave therapy.
CombinationTherapy (Finasteride 5 mg o.d + Doxazosin 4mg or 8mg o.d)
Placebo
Doxazosin (doubled each week beginning at 1mg o.d until 4mg or 8mg o.d)
Finasteride (5mg o.d)

MODULE 3
62/113
The reduction in the risk of clinical progression with combination therapy was 66% compared to placebo (p<0.001)
The MTOPS study clearly shows that combination therapy is more effective than monotherapy in the long-term management of BPH
Patients most likely to benefit from combination therapy are those with a significantly higher baseline risk of progression, in other words, those with larger glands and higher PSA values 44
The side effects of combination therapy reflect the combined adverse-event profiles of the α1-receptor blocker and 5α-reductase inhibitor 45
44. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003.45. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003.MTOPS = Medical Therapy of Prostatic Symptoms ; BPH = Benign Prostatic Hyperplasia; LUTS = Lower Urinary Tract Symptoms

MODULE 3
63/113
Canadian BPH Guidelines:46
“Patients successfully treated with combination therapy may be given the option of discontinuing the α1-blocker after 6-12 months. If symptoms recur, the α1-blocker should be restarted.”
46. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.BPH = Benign Prostatic Hyperplasia

MODULE 3
64/113
Phytotherapy
Phytotherapeutic agents for LUTS/BPH have become increasingly popular since about 1990
First popular in Europe, they have crossed the Atlantic and become more popular in Canada than the medications discussed previously
The increase in the use of herbs for treating BPH is closely correlated with the rising interest in alternative or complementary medicine seen across the continent
LUTS = Lower Urinary Tract Symptoms; BPH = Benign Prostatic Hyperplasia

MODULE 3
65/113
Indeed, an increasing number of patients are taking various over the counter preparations to treat or prevent the occurrence of prostatic conditions, on the recommendations of friends, family or even advertisements in the media
Usually, they do not even consider that it is important to mention this fact to the physician at a consultation
As a significant number of these plants extracts may indeed have a significant impact on the prostate, it is important that practicing physicians are aware of this fact

MODULE 3
66/113
Table 3.5 Some Plant Extracts Used to Treat BPHSpecies Common Name
Serenoa repens, Sabal serrulataSaw palmetto berry/American dwarf palm
Hypoxis rooperi South African star grass
Pygeum africanum African plum tree
Urtica dioica Stinging nettle
Secale cereale Rye pollen
Cucurbita pepo Pumpkin seed
Opuntia Cactus flower
Pinus Pine flower
Picea Spruce
Adapted from Walsh PJ, Campbell’s Urology, 8th ed, p1368.BPH = Benign Prostatic Hyperplasia

MODULE 3
67/113
Plant extracts are complex compounds containing substances with different mechanisms of action
It is poorly understood how these phytochemicals act on BPH, but the three that have received the most attention are:
Anti-inflammatory effects
5α-reductase inhibition
Interference with growth factor 47
47. Walsh PC. Campbell’s Urology, 8th Edition (2002), p1368BPH = Benign Prostatic Hyperplasia

MODULE 3
68/113
Serenoa repens (Saw Palmetto Berry Extract) Received the most clinical study and is furthest along in development
The anti-BPH mechanism of action of Serenoa repens is most likely 5α-reductase inhibition,48 although studies have shown evidence of other mechanisms, including:49
Inhibition of DHT binding to the androgen receptor in prostate cells
Inhibition of nuclear prostatic estrogen receptors
Inhibition of fibroblast growth factor-induced prostatic epithelial proliferation
Anti-proliferative effects; Anti-inflammatory effects; Anti-edematous effects on prostatic tissues
Noncompetitive α-adrenergic antagonism
Modulation of prolactin-induced prostatic growth by receptor signal transduction
48. Fong YK, Milani S, Djavan B. Curr Opin Urol 2005;15:45-48.49. Fong YK, Milani S, Djavan B. Curr Opin Urol 2005;15:45-48, p45-6BPH = Benign Prostatic Hyperplasia; DHT = Dihydrotestosterone

MODULE 3
69/113
In a properly designed randomized placebo controlled trial, Serenoa repens was found to be only slightly better than placebo in ameliorating symptoms, improving flow rate and decreasing prostate volume 50
50. Bent S et al. J Urol 173(Suppl 4):443 Abstract # 1637

MODULE 3
70/113
Pygeum africanum (African Plum Tree)
Extract used since the mid-1960s to treat men suffering from BPH and currently the most commonly used medicine in France for BPH 51
Mechanism of action is unclear, but has been shown in animal studies to modulate bladder contractility by reducing the sensitivity of the bladder to electrochemical stimulation 52
51. Pygeum africanum (Prunus africanus) (African plum tree). Monograph. Altern Med Rev 2002;7:71-4. 52. Monograph, p71BPH = Benign Prostatic Hyperplasia

MODULE 3
71/113
Also demonstrated to have: 53
Anti-inflammatory activity
Inhibit fibroblast production
Increase adrenal androgen secretion
Restore the activity of the prostate and bulbourethral epithelium
Several small clinical studies have been conducted, but they are inconclusive and more research is needed before it can be considered as standard treatment 54
53. Monograph, p7154. Nickel JC, Herschorn S, Corcos J, et al. Can J Urol 2005;12:2677-2683.

MODULE 3
72/113
Canadian BPH Guidelines:55
“If patients are interested in complementary approaches (phytotherapeutic or other supplements) for LUTS secondary to BPH, they may be counseled that some plant extracts (particularly saw palmetto berry extract and pygeum Africanum) have shown some efficacy in small but unconvincing studies. Further proof is required before phytotherapy can be recommended as standard therapy; however, these agents do appear to be safe.”
55. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.LUTS = Lower Urinary Tract Symptoms; BPH = Benign Prostatic Hyperplasia

MODULE 3
73/113
3.6 Minimally Invasive Surgical Therapies
The number of MIST for BPH has grown substantially over the last two decades, paralleling technological innovations in other medical spheres
This is an area where experimentation is rich with possibility, but clinical evidence is often inadequate to support the inclusion of such procedures in the treatment recommendations of national and international guidelines
Over the years, MIST have fallen in and out of favour as further evidence of their safety and efficacy has emerged from clinical data
MIST = Minimally Invasive Surgical Therapies; BPH = Benign Prostatic Hyperplasia

MODULE 3
74/113
At present, only three MIST are recommended for treatment of BPH in Canada: 56
1. Transurethral microwave therapy (TUMT)
2. Transurethral needle ablation of the prostate (TUNA)
3. Prostatic stents
56. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.

MODULE 3
75/113
Transurethral Microwave Thermotherapy
Transurethral microwave thermotherapy (TUMT) is one of a group of thermal-based therapies designed to produce coagulation necrosis of the prostate through the application of high temperatures
Several TUMT devices are currently available, although there is no data to suggest superiority of one device over another 57
Evidence shows that for the average patient, TUMT is more effective than medical therapy but less effective than surgery in relieving symptoms.
57. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003.

MODULE 3
76/113
Canadian BPH Guidelines:58
“TUMT is a reasonable treatment choice for the patient who has moderate symptoms, small to moderate gland size, and a desire to avoid more invasive therapy for potentially less effective results.”
58. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.BPH = Benign Prostatic Hyperplasia

MODULE 3
77/113
Transurethral Needle Ablation
Transurethral needle ablation (TUNA) involves the use of radio frequency (RF) waves (490 KHz) to heat and coagulate hyperplastic prostatic tissue
The RF waves are transmitted through two 18-gauge needles at the tip of a TUNA catheter, which contains a lens to visually guide placement in the urethra
After advancing into the prostate parenchyma through the urethra, tissue in the lateral prostatic lobes is heated to 100ºC

MODULE 3
78/113
According to AUA guidelines, the ideal patient for TUNA is a man who has obstructive BPH, i.e., a prostate of ≤ 60 grams with predominantly lateral lobe enlargement 59
The Canadian guidelines recommend TUNA as a reasonable option for the relief of symptoms in younger, active men in whom sexual function remains an important quality-of-life issue (less risk of retrograde ejaculation). Limited data are available on long-term outcomes 60
59. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003.60. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.AUA = American Urological Association ; TUNA = Transurethral Needle Ablation; BPH = Benign Prostatic Hyperplasia

MODULE 3
79/113
Canadian BPH Guidelines: 61
“TUNA may be a reasonable option for the relief of symptoms in the younger, active individual in whom sexual function remains an important quality of life issue (less risk of retrograde ejaculation). Limited data is available on long-term outcomes.”
61. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.TUNA = Transurethral Needle Ablation; BPH = Benign Prostatic Hyperplasia

MODULE 3
80/113
Prostatic Stents
Metal or polyurethane stents may be placed into the prostatic urethra where, when expanded, they mechanically relieve the obstruction from the surrounding hyperplastic prostatic tissue
Over a period of weeks to a few months, the permanent stents could become covered with normal transitional epithelial tissue
Temporary stents are also available but the problem of migration is a significant issue 62
62. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003;170(2 Pt 1):530-47.

MODULE 3
81/113
Canadian BPH Guidelines: 63
“Temporary and permanent stents may be considered for patients with severe urinary obstruction secondary to BPH who are medically unfit for surgery (or waiting to become medically fit for surgery or MIST). Stents are not recommended as standard therapy for LUTS associated with BPH.”
63. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.MIST = Minimally Invasive Surgical TherapiesLUTS = Lower Urinary Tract SymptomsBPH = Benign Prostatic Hyperplasia

MODULE 3
82/113
3.7 Surgery Surgical intervention is the appropriate treatment for patients with
refractory or recurrent AUR or BPH-related complications (hematuria, stones, infection, obstructive renal failure)
Surgery is also recommended for patients who have moderate-to-severe LUTS and are either inadequately controlled by medical therapy or who opt for a more definitive treatment 64
64. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003;170(2 Pt 1):530-47. p538AUR = Acute Urinary RetentionBPH = Benign Prostatic HyperplasiaLUTS = Lower Urinary Tract Symptoms

MODULE 3
83/113
Although surgery can produce the best improvements in symptoms and flow rates, it does have a higher incidence of complications.
The standard options are:
Transurethral resection of the prostate (TURP)
Transurethral incision of the prostate (TUIP)
Open prostatectomy

MODULE 3
84/113
Transurethral Resection of the Prostate (TURP)
The main goal of prostatic surgery is to remove the hyperplastic tissue obstructing the urethra, while minimizing damage to the surrounding tissues
TURP is an endoscopic procedure that accesses this tissue through the urethra, thus avoiding the invasiveness of open surgery
For many years, TURP has been considered the gold standard for the surgical treatment of BPH
BPH = Benign Prostatic Hyperplasia

MODULE 3
85/113
After preparation, the surgeon distends the bladder with fluid in order to better visualize the prostate, bladder neck, median lobe, and bladder wall
A resectoscope sheath is inserted into the urethra, through which an electrified loop is inserted into the region of the prostate
Surgery consists of excision and removal of hyperplastic tissue through the urethra

MODULE 3
86/113
Although TURP can be performed under spinal epidural or light general anesthesia, it usually requires a short hospital stay
After TURP, symptoms are improved in about 70 to 90% of patients, and peak urine flows of 15-20 mL/sec or more can be achieved 65 Reductions in symptom scores have been reported to be 85% with a 16 to 20% likelihood of further surgery within 8 years 66
65. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p58.66. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p58. (table)TURP = Transurethral Resection of the Prostate

MODULE 3
87/113
Complications of TURP are not infrequent, with an overall rate of 16.1% being reported 67
Complications include:
Incontinence (0.2-1%)
Erectile dysfunction (2-5%)
Need for further surgery to address complications (3.3%),
Small but not insignificant likelihood of death within 90 days of surgery (0.2-1.5%)
67. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p58. (table)TURP = Transurethral Resection of the Prostate

MODULE 3
88/113
Most common complication is retrograde ejaculation, which occurs in 70 to 90% of men. As a result of the loss of the bladder-neck sphincter mechanism, the bladder neck may fail to close during ejaculation, allowing semen to pass into the bladder instead of through the urethra 68
Another complication is the TURP syndrome, a dilutional hyponatremia that occurs when irrigant solution is absorbed into the bloodstream during the procedure 69
68. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p59.69. Issa MM et al. Urology. 2004;64:298-301.TURP = Transurethral Resection of the Prostate

MODULE 3
89/113
Sexual dysfunction is thought not to be attributable to surgery in all cases but rather to a psychosomatic response or the result of aging 70
Thermal damage to the nerves near the apical tissue of the prostate could be one of the explanations 71
70. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p58.71. In a conversation with Dr. Mostafa Elhilali (July 2005).

MODULE 3
90/113
Canadian BPH Guidelines: 72
Absolute indications to recommend TURP include:
Failure of medical therapy
Intractable urinary retention
Renal insufficiency (caused by BPO)
Relative indications to recommend TURP include:
Recurrent cystitis
Bladder calculi
Persistent prostatic bleeding
72. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.TURP = Transurethral Resection of the ProstateBPO = Benign Prostatic Obstruction

MODULE 3
91/113
Transurethral Incision of the Prostate (TUIP)
TUIP is an outpatient endoscopic procedure in which the surgeon makes a deep cut in the prostate from the bladder neck to the veru montanum using a Collings knife, thus relieving pressure on the urethra
TUIP is limited to patients with smaller prostates (<30 grams) with an elevated bladder neck
TUIP can result in levels of symptomatic improvement similar to TURP, and has the advantage of having a lower incidence of retrograde ejaculation 73
However, TUIP is associated with a slightly higher rate of secondary procedures.
73. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003;170(2 Pt 1):530-47. p538TURP = Transurethral Resection of the Prostate

MODULE 3
92/113
Canadian BPH Guidelines: 74
“TUIP is appropriate surgical therapy for prostate glands less than 30 cc or grams. These patients should experience results similar to TURP with lower incidence of retrograde ejaculation than TURP.”
74. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.TUIP = Transurethral Incision of the ProstateTURP = Transurethral Resection the ProstateBPH = Benign Prostatic Hyperplasia

MODULE 3
93/113
Transurethral Electrovaporization of the Prostate (TUVP)
TUVP is a procedure which applies electrical energy to electrosurgically vaporize or remove the obstructive hyperplastic prostatic tissue
The technique involves the application of a simple, specially designed, grooved rollerball electrode, which allows the surgeon to vaporize the prostatic tissue thus opening the obstructed urethral lumen
The rollerball is put into the resectoscope and, using a technique similar to TURP, rolled over the hyperplastic tissue
The electrical wattage is higher than that of TURP, so that the rollerball rapidly heats the tissue cells, vaporizing them into steam
TURP = Transurethral Resection of the Prostate

MODULE 3
94/113
One advantage of this technique is the reduction of bleeding due to the cauterization of tissues surrounding the ablated region 75
Laser therapy, which operates on a similar principle, is discussed later
Compared to TURP, TUVP results in equivalent, short-term improvements in symptom severity scores, urinary flow rate, and quality of life
However, there is a higher incidence of postoperative irritative voiding symptoms, dysuria, urinary retention, and the need for unplanned secondary catheterization 76
75. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003;170(2 Pt 1):530-47. p53876. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003;170(2 Pt 1):530-47. p538TURP = Transurethral Resection of the ProstateTUVP = Transurethral Electrovaporization of the Prostate

MODULE 3
95/113
Canadian BPH Guidelines: 77
“TUVP is an alternative operation to TURP or TUIP and short-term results are comparable to TURP, particularly in men with small prostates. Patients experience higher incidence of irritative symptoms, dysuria, and urinary retention and few long-term studies are available.”
77. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol 2005;12:2677-2683.TUVP = Transurethral Electrovaporization of the ProstateTURP = Transurethral Resection of the ProstateTUIP = Transurethral Incision of the ProstateBPH = Benign Prostatic Hyperplasia

MODULE 3
96/113
Laser Prostatectomy
Laser energy is used to produce coagulation necrosis, tissue vaporization, or tissue resection
A variety of lasers (KTP, Holmium:YAG) and delivery systems (end-firing, side-firing, interstitial) are available for prostatic tissue coagulation or ablation
Investigators of laser systems do not agree on the optimal technique or energy delivery.
Each offers particular features and potential benefits
In Canada, the two most popular lasers used are the KTP and Holmium lasers

MODULE 3
97/113
The Holmium laser enucleation of the prostate (HoLEP) procedure may require a steep learning curve, however, other techniques like Holmium laser ablation of the prostate (HoLAP) and KTP laser or photoselective vaporization of the prostate (PVP) are very easy to learn
Holmium laser enucleation of the prostate is the only laser technology to date that has had its efficacy documented in randomized trials against TURP and open prostatectomy 78
78. In a conversation with Dr. Mostafa Elhilali (July 2005).TURP = Transurethral Resection of the Prostate

MODULE 3
98/113
Transurethral Laser Vaporization (TLV)
TLV uses laser energy to vaporize prostatic tissue
The laser fibre is held in contact with hyperplastic tissue to carve a series of furrows, until a wide channel is obtained
Like TUVP, TLV leads to short-term improvement in symptom scores, urinary flow rate, and QoL indices comparable to TURP
However, the incidence of postoperative urinary retention and the need for unplanned secondary catheterization with TLV are higher than that observed with TURP 79
79. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003;170(2 Pt 1):530-47. p539TUVP = Transurethral Electrovaporization of the ProstateTURP = Transurethral Resection of the ProstateQoL = Quality of Life

MODULE 3
99/113
Transurethral Holmium Laser Resection/Enucleation of the Prostate (HoLEP)
HoLEP is a relatively new technique in which the prostate hyperplastic tissue is resected using a holium laser fibre and a specially adapted resectoscope 80
Studies by Gilling and colleagues suggest that in the intermediate-term, symptomatic improvement obtained after holmium laser treatment is similar to that of TURP, with a lowered risk of bleeding and need for blood transfusion 81,82
80. Gilling PJ et al. Urology 1996;47:48-51. 81. Gilling PJ et al. Urology 1996;47:48-51.82. Gilling PJ et al. J Urol 1999;162:1640-4.TURP = Transurethral Resection of the Prostate

MODULE 3
100/113
HoLEP has been successfully applied to the treatment of very large prostates with results comparable to open prostatectomy, and long-term data on this technique show that the benefits are durable 83
While the AUA Guidelines Committee recommends that TURP remains the treatment of choice for patients who elect or require surgery for BPH 84, this recommendation may change as more data becomes available in regard to laser resection/enucleation of the prostate. The Canadian guidelines recommend its use as a therapeutic option for BPH
83. Elzayat E, Habib E, Elhilali M. Holmium Laser Enucleation of the Prostate (HOLEP): A Size Independent New Gold Standard. Urology. In press84. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003;170(2 Pt 1):530-47. p539TURP = Transurethral Resection of the ProstateAUA = American Urological AssociationBPH = Benign Prostatic Hyperplasia

MODULE 3
101/113
Photoselective Vaporization of the Prostate (PVP)
Recent improvements in laser technology have led to promising new treatment modalities, including the potassium-titanyl-phosphate (KTP) laser
This high-power photoselective technique effectively vaporizes the obstructing prostatic tissue in an outpatient surgical procedure
Current results show that this procedure is a feasible option for men seeking relief of BOO due to BPH 85
The technique does not require a steep learning curve and most urologists familiar with TURP have little problem picking it up
85. Backmann A, Ruszat R, Wyler S, Reich O, et al. Eur Urol. 2005;47:798-804.TURP = Transurethral Resection of the ProstateBOO = Bladder Outlet ObstructionBPH = Benign Prostatic Hyperplasia

MODULE 3
102/113
Short-term results of a study of 108 patients who underwent 80W KTP laser vaporization of the prostate showed that this procedure is safe and effective for surgical treatment of BPH-related LUTS
Low complication rate, and efficacy at 12 months is comparable to that of TURP and other laser therapies over the same period
Data on the long term durability of the benefits are pending
However, since neither comparison trials nor long-term studies are available, this therapy has not been recommended by AUA guidelines
The Canadian guidelines recommend its use as a therapeutic option for BPH
LUTS = Lower Urinary Tract SymptomsTURP = Transurethral Resection of the ProstateAUA = American Urological AssociationBPH = Benign Prostatic Hyperplasia

MODULE 3
103/113
Open Prostatectomy
Involves the surgical removal of the inner portion of the prostate via a suprapubic or retropubic incision in the lower abdomen
This procedure is normally performed on patients with prostate volumes greater than 80 to 100 mL 86
86. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003;170(2 Pt 1):530-47. p539

MODULE 3
104/113
3.8 Summary
The choice of treatment for BPH is primarily based on symptomatology, severity and bother of LUTS, and patient preference
Other considerations include the risk of progression, complications, and the need for surgery
Patients should be informed of the risks and benefits of all therapeutic options and actively participate in the choice of therapy
LUTS = Lower Urinary Tract SymptomsBPH = Benign Prostatic Hyperplasia

MODULE 3
105/113
For most men with mild BPH and little or no bothersome symptoms, a conservative approach of lifestyle modification with watchful waiting is appropriate
Periodic physician-supervised visits are essential
Prior to the decision to choose this treatment plan, the physician should assess the patient’s risk of progression
BPH = Benign Prostatic Hyperplasia

MODULE 3
106/113
The choice of medical agents depends largely on patient symptoms, bother, age, size of prostate gland, baseline PSA, comorbidities, and expected drug tolerance.
Medical therapies are appropriate for men with moderate / severe LUTS and significant bother
Two drug classes are available:
α1-receptor blockers and 5α-reductase inhibitors
Both are effective in managing LUTS secondary to BPH; however, combination therapy with an agent from each class is more effective in controlling the symptoms and clinical progression of BPH
PSA = Prostate-Specific AntigenLUTS = Lower Urinary Tract SymptomsBPH = Benign Prostatic Hyperplasia

MODULE 3
107/113
Minimally invasive surgical therapies (MIST) are appropriate for men with moderate to severe LUTS secondary to BPH, who opt for more active therapy
The indications for these procedures vary, and clinical evidence of long-term efficacy may be lacking
In Canada, the following procedures are recommended as optional therapy:
TUMT
TUNA
StentsTUMT = Transurethral Microwave ThermotherapyTUNA = Transurethral Needle AblationLUTS = Lower Urinary Tract SymptomsBPH = Benign Prostatic Hyperplasia

MODULE 3
108/113
TURP is the gold standard for the surgical treatment of men with bothersome moderate to severe LUTS who request active treatment with a moderately enlarged prostate (<60-80 cc)
TUIP is appropriate in men with smaller prostate (<30 cc)
For glands over 80-100 cc, open prostatectomy is the gold standard
Other surgical options include:
TUVP
Laser prostatectomy (Holmium/YAG)
Laser vaporization of the prostate (PVP, HoLAP)
TURP = Transurethral Resection of the ProstateLUTS = Lower Urinary Tract SymptomsTUIP = Transurethral Incision of the ProstateTUVP = Transurethral Electrovaporization of the Prostate

MODULE 3
109/113
3.9 Quiz
1. Which treatment option is preferred for men with a moderate size prostate and IPSS (AUA) symptom score of ≤ 7?
a) 5α-reductase inhibitor
b) TUMT
c) α1-receptor blocker
d) Watchful waiting (Correct)
IPSS = International Prostate Symptom ScoreAUA = American Urological AssociationTUMT = Transurethral Microwave Thermotherapy

MODULE 3
110/113
2. What measure can physicians use to assess a patient’s individual risk of clinical progression?
a) Prostate size
b) Patient age
c) PSA
d) All of the above (Correct)
PSA = Prostate-Specific Antigen

MODULE 3
111/113
3. The MTOPS study reported that finasteride could significantly reduce clinical progression in men with BPH when combined with which of the following drugs?
a) testosterone
b) doxazosin (Correct)
c) saw palmetto
d) dutasteride

MODULE 3
112/113
4. Transurethral incision of the prostate (TUIP) is indicated for men with moderate to severe LUTS and which of the following limitations?
a) Smaller prostates (<30 g) (Correct)
b) Larger prostates (>30 g)
c) Obstructive BPH
d) Sexually active men
LUTS = Lower Urinary Tract Symptoms; BPH = Benign Prostatic Hyperplasia

MODULE 3
113/113
5. Transurethral electrovaporization of the prostate (TUVP) employs which form of technology to vaporize obstructive hyperplastic prostatic tissue?
a) KTP laser
b) Rollerball electrode
c) Holmium:YAG laser
d) All of the above (Correct)