Mitral regurgitation in hypertrophic cardiomyopathy: Relationship to obstruction and relief with...
1
Journal of the American SocieD" of Echocardiography 392 Abstracts May-June 1996 402D DOPPLER ECtIOCARDIOGRAPHIC ASSESSMENT OF LEFT VENTRICULAR FILLING PRESSURE IN PATIENTS WITH CORONARY ARTERY DISEASE: LIMITATIONS IN PATIENTS WITH PRESERVED SYSTOLIC FUNCTION Kazuhiro Yamamoto, ND, Rick A. Nishimura, MD, John C. Burnett, Jr., MD, Stuart T. Higano, MD, Margaret M. Redfield, MD, Mayo Clinic, Rochester, MN Recent studies have reported that the deceleration time (DT) of early diastolic transmitral flow velocity measured with pulsed wave Doppler echocardiography correlates well with LV filling pressures in patients (pts) with systolic dysfunction. However, it is unknown whether this can be applied to pts with elevated filling pressures and preserved systolic function (primary diastolic dysfunction). The Doppler-derived difference in the duration of pulmonary venous and transmitral flow at atrial contraction (Ad) has been reported to correlate well with filling pressures, but pulmonary venous flow velocity curves may be difficult to obtain. To clarify the accuracy and the limitations of Doppler assessment of filling pressures, transmitral and pulmonary venous flow velocity curves and LV pressure were recorded in 56 pts with coronary artery disease. In 14% of the pts, pulmonary venous flow velocity curves could not be adequately recorded. The correlation coefficients between the Doppler parameters and LV end-diastolic pressure (EDP) were: (*p<0.05 vs coefficient in pts with EF < 50%) EF _< 50% EF > 50% DT r=0.82 (p<0.01) r=-0.19" (p=N.S.) Ad r=0.79 (p<O.O1) r=-0.63 (p<0.01) The sensitivity / specificity of Ad _>0 msec for detecting an LVEDP _> 20 mmHg were 100% / 100% in pts with an EF < 50% and 100% / 90% in pts with an EF > 50%. Conclusion: In pts with coronary artery disease and systolic dysfunction, the transmittal flow velocity curve alone can be used to detect elevated filling pressures. However, in pts with preserved systolic function, the combined analysis of transmitral and pulmonary venous flow velocity curves is recom- mended. 402F MITRAL REGURGITATION IN HYPERTROPHIC CARDIOMYOPATHY: RELATIONSHIP TO OBSTRUCTION AND RELIEF WITH MYECTOMY Eric H.C. Yu MD, Abroad S. Omran MD, E. Douglas Wigle MD, William G. Williams MD, Samuel C. Siu MD, Harry Rakowsld MD, The Toronto Hospital, Toronto, Canada. Mitre/regurgitation (MR) in hypertrophic obstructive cardiomyopathy (I-IOCM) is usually due to systolic anterior motion and incomplnte mitre/lea/let coaptation. In 10-20% ofpatiants, independant mitre/valve disease (IMVD) contributes to the degree of MR. Methods: We studied 93 patients undergoing septal myectomy (64 male, mean age 45 + 11 years). To define the relationship between the LVOT peak gradient (PC;) and the etiology and severity of MR, all patients had pro- and post-op echo- Doppler and intraoperative TEE studies. MR was quantitated using regurgitant jet area and pulmonary vein flow data. All studies were read independently by two blinded observers. ~ ,,, Res~!ts; In patients without ~ relationship between the severity of MR and the PG. ~ i i ! Mean PG +SD, for trivial ~ (1), mild (2), moderate (3), severe (4) MR, were 23.7 ~1 I +15, 34.9 + 8, 69+15, and 105 +16 mmHg respectively 1 = 3 4 (p<0.001 by ANOVA and uR ~ pair-wise testing). Early post- op, MR was absent or trivial in 78%, mild in 21%, and moderate in 1%. No patient required concomitant mitral valve surgery. Conclusions: In patients with HOCM and MR not due to IMVD, the severity of MR is related to the PG determined by echo. In these patients, myeetomy alone dramatically improves MR. 402E CAN THE VALSALVA MANEUVER BE UTILIZED TO ESTIMATE LEFT VENTRICULAR FILLING PRESSURES? A SIMULTANEOUS CARDIAC CATHETERIZATION/DOPPLER ECHOCARDIOGRAPHIC STUDY David G. Hurrell, Rick A. Nishimura, *Christopher P, Appleton Mayo Clinic, Rochester, MN; *Scottsdale, AZ The non-invasive estimation of left ventricular filling pressures by Doppler echocardiography has utilized mitral inflow indices and pulmonary venous flow velocities and flow durations. This technique has been hampered by poor sensitivity for mitrel inflow indices alone, because a subset of patients have a "pseudonormal' mitral filling pattern (E/A ratio 0.8 - 2.0) with elevated LV diastolic pressures. Changes in load may aid in detecting this phenomenon. Thus, 31 patients were studied in the cardiac catheterization laboratory using high-fidelity catheters comparing simultaneous pre-A LV pressure with Doppler mitral inflow indices [E, A, and DT(deceleration time)] at baseline and at peak Valsalva. The absolute A (abs A) was also incorporated to account for variations in heart rate and defined as the maximum A-wave velocity minus the velocity at the onset of atrial contraction. All patients performed a 12 second Valsalva. An adequate Valsalva was defined as a >10% decline in the E-wave velocity at maximum Valsatva. E(m/s) Abe A(mts) DT(rns) E/A._b~, A Pre-A < 15 mm Hg (mean 10.9_+2.8) Base 0.65_+0.14 0.57_+0.08 233_+53 1.16_+1.29 Valsalva 0.33_+0.12 0.45_+0.15 320_+84 0.81_+0.38 Pro A _>15 mm Hg (mean 20.8_+3.1) Base 0.88+0.26 0.48_+0.22 192_+54 2.30-+1.55 Valsalva 0.47_+0.12 0,52+_0.18 300+106 1.04_+0.71 At peak Valsalva compared to baseline, there was no correlation between pre-A LV pressure and percent change or absolute difference in E velocity, A velocity, or DT. However, an absolute difference of 0.5 in the Elabs A ratio at peak Valsalva compared to baseline was highly sensitive and specific for a pre-A LV pressure of ->15 mm Hg, 86% and 100% respectively. In addition, the positive predictive value(PPV) was 100% and the negative predictive valae(NPV) 77% for this Doppler index. In a subset of 18 patients with a normal baseline E/A ratio, the sensitivity and specificity of the E/abs A difference >0.5 was 80% and 100% respectively. The PPV was 100% and the NPV 67% for this subset, thus correctly separating those patients with normal vs. "pseudonormal" mitral filling. Conclusion: Doppler echocardiography ufilizing the Elabs A difference >0,5 before and at peak Valsalva reliably predicts pre-A LV filling in this selected group of patients and specifically is of additional benefit in those patients with a "pseudonormal" mitral filling pattern. 402G LEFT VENTRICULAR MASS MEASUREMENT: COMPARISONOF THREE METHODS OF M-MODE ECHOCARDIOGRAPHYUSING MAGNETIC RESONANCE IMAGING AS THE STANDARD Constantinos G Missouris, MRCP, Sandy M Forbat* MRCP, S Richard Underwood* MD, MRCP, Donald RJ Singer, MD, MRCP, Graham A MacGregor, FRCP. St George's Hospital Medical School & *National Heart Lung Instilute,ImperialCollege,London, UK Magneticresonanceimaging(MRI)is an accuratemethodfor measurement of left ventricular mass (LVM). We compared three methods of LVM measurement by M-mode echocardiography (echo) using MRI as the standard in 24 untreated patients with essential hypertension, average supine blood pressure 159/102195%C1:154-165/99-1041 mm Fig (Arteriosonde),mean age 51147-55 years], 19M:5F; ll black;ll white; 2 Asian. LVM was calculated from one dimensional M-mode (Fiewlett~ Packard 1000c; short axis view) recordings obtained in diastole using (1) tile American Societyof Echocardiography (ASE) convention, (2) the Penn convention and (3) the Teichholz's volume corrected formula. For MRI (Picker 2055, 0.5 Tesla, short axis images in systole),myocardialarea was measured for each slice and the mean areas summed to give myocardial volume. Using the three slandardM-modeformulae,widelydifferentvaluesof LVM were obtained with echocardiography: ASE 319+21(SEM)g; Penn 273+19g; Teichholz 191+11 g. By MRI, LVM was 232+__11g (P<0.0I. Wilcoxon vs all M-mode formulae). Using the ASE and the Penn conventions, the difference between echocardiographyand MRI became greater the higher the underlyingvalue of LVM When the ASE and Penn formulaewere applied to relevantone dimensionalMR imagesthere was a similar pauem of overestimation. As a further comparison of echo and MRI, systolicmeasurements of M-mode tracings were also made and LVM estimatedfrom these using the ASE formula.These results were compared with those obtained using the ASE formula applied to single slice one dimensional MR measurements in systole. Mean LVM was significantly higher by MRI than by echo using tile systolic measurementsapplied to the ASE formula (387+21gand 312 _+16g respectively;P<0.01). Our findingssuggestthat the echocardiographic ASE and Penn conventions may overestimate LVM, particularly in patients with more severe hypertrophy. In contrast the Teiehholz volume-corrected formula gives average values lower than MRI. These large differences appear to result from false assumptions in the M-mode echocmdiographicformulae and may have importantclinical implicationsfor tile measurementof LVM in hypertensivesubjects and for the assessment of the changes in LVM that may occur with treatmentin these patients.
Transcript of Mitral regurgitation in hypertrophic cardiomyopathy: Relationship to obstruction and relief with...

Journal o f the American SocieD" o f Echocardiography 392 Abstracts May-June 1996
4 0 2 D DOPPLER ECt IOCARDIOGRAPHIC ASSESSMENT OF LEFT VENTR IC ULAR F I L L I N G PRESSURE IN PATIENTS W I T H C O R O N A R Y ARTERY DISEASE: L I M I T A T I O N S IN PATIENTS W I T H PRESERVED SYSTOLIC FUNCTION Kazuhiro Yamamoto, ND, Rick A. Nishimura, MD, John C. Burnett, Jr., MD, Stuart T. Higano, MD, Margaret M. Redfield, MD, Mayo Clinic, Rochester, MN
Recent studies have reported that the deceleration time (DT) of early diastolic transmitral flow velocity measured with pulsed wave Doppler echocardiography correlates well with LV filling pressures in patients (pts) with systolic dysfunction. However, it is unknown whether this can be applied to pts with elevated filling pressures and preserved systolic function (primary diastolic dysfunction). The Doppler-derived difference in the duration of pulmonary venous and transmitral flow at atrial contraction (Ad) has been reported to correlate well with filling pressures, but pulmonary venous flow velocity curves may be difficult to obtain. To clarify the accuracy and the limitations of Doppler assessment of filling pressures, transmitral and pulmonary venous flow velocity curves and LV pressure were recorded in 56 pts with coronary artery disease. In 14% of the pts, pulmonary venous flow velocity curves could not be adequately recorded. The correlation coefficients between the Doppler parameters and LV end-diastolic pressure (EDP) were: (*p<0.05 vs coefficient in pts with EF < 50%)
EF _< 50% EF > 50% DT r=0.82 (p<0.01) r=-0.19" (p=N.S.) Ad r=0.79 (p<O.O1) r=-0.63 (p<0.01)
The sensitivity / specificity of Ad _> 0 msec for detecting an LVEDP _> 20 mmHg were 100% / 100% in pts with an EF < 50% and 100% / 90% in pts with an EF > 50%. Conclusion: In pts with coronary artery disease and systolic dysfunction, the transmittal flow velocity curve alone can be used to detect elevated filling pressures. However, in pts with preserved systolic function, the combined analysis of transmitral and pulmonary venous flow velocity curves is recom- mended.
4 0 2 F MITRAL REGURGITATION IN HYPERTROPHIC CARDIOMYOPATHY: RELATIONSHIP TO OBSTRUCTION AND RELIEF WITH MYECTOMY Eric H.C. Yu MD, Abroad S. Omran MD, E. Douglas Wigle MD, William G. Williams MD, Samuel C. Siu MD, Harry Rakowsld MD, The Toronto Hospital, Toronto, Canada.
Mitre/regurgitation (MR) in hypertrophic obstructive cardiomyopathy (I-IOCM) is usually due to systolic anterior motion and incomplnte mitre/lea/let coaptation. In 10-20% ofpatiants, independant mitre/valve disease (IMVD) contributes to the degree of MR. Methods: We studied 93 patients undergoing septal myectomy (64 male, mean age 45 + 11 years). To define the relationship between the LVOT peak gradient (PC;) and the etiology and severity of MR, all patients had pro- and post-op echo- Doppler and intraoperative TEE studies. MR was quantitated using regurgitant jet area and pulmonary vein flow data. All studies were read independently by two blinded observers.
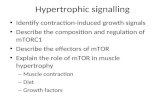
~ ,,, Res~!ts; In patients without
~ relationship between the severity of MR and the PG.
~ i i ! Mean PG +SD, for trivial ~ (1), mild (2), moderate (3),
severe (4) MR, were 23.7 ~1 I +15, 34.9 + 8, 69+15, and
105 +16 mmHg respectively 1 = 3 4 (p<0.001 by ANOVA and
uR ~ pair-wise testing). Early post- op, MR was absent or trivial in 78%, mild in 21%, and moderate in 1%. No patient required concomitant mitral valve surgery. Conclusions: In patients with HOCM and MR not due to IMVD, the severity of MR is related to the PG determined by echo. In these patients, myeetomy alone dramatically improves MR.
4 0 2 E CAN THE VALSALVA MANEUVER BE UTILIZED TO ESTIMATE LEFT VENTRICULAR FILLING PRESSURES? A SIMULTANEOUS CARDIAC CATHETERIZATION/DOPPLER ECHOCARDIOGRAPHIC STUDY David G. Hurrell, Rick A. Nishimura, *Christopher P, Appleton Mayo Clinic, Rochester, MN; *Scottsdale, AZ
The non-invasive estimation of left ventricular filling pressures by Doppler echocardiography has utilized mitral inflow indices and pulmonary venous flow velocities and flow durations. This technique has been hampered by poor sensitivity for mitrel inflow indices alone, because a subset of patients have a "pseudonormal' mitral filling pattern (E/A ratio 0.8 - 2.0) with elevated LV diastolic pressures. Changes in load may aid in detecting this phenomenon. Thus, 31 patients were studied in the cardiac catheterization laboratory using high-fidelity catheters comparing simultaneous pre-A LV pressure with Doppler mitral inflow indices [E, A, and DT(deceleration time)] at baseline and at peak Valsalva. The absolute A (abs A) was also incorporated to account for variations in heart rate and defined as the maximum A-wave velocity minus the velocity at the onset of atrial contraction. All patients performed a 12 second Valsalva. An adequate Valsalva was defined as a >10% decline in the E-wave velocity at maximum Valsatva.
E(m/s) Abe A(mts) DT(rns) E/A._b~, A Pre-A < 15 mm Hg (mean 10.9_+2.8) Base 0.65_+0.14 0.57_+0.08 2 3 3 _ + 5 3 1.16_+1.29 Valsalva 0.33_+0.12 0.45_+0.15 3 2 0 _ + 8 4 0.81_+0.38 Pro A _>15 mm Hg (mean 20.8_+3.1) Base 0.88+0.26 0.48_+0.22 192_+54 2.30-+1.55 Valsalva 0.47_+0.12 0,52+_0.18 300+106 1.04_+0.71 At peak Valsalva compared to baseline, there was no correlation between pre-A LV pressure and percent change or absolute difference in E velocity, A velocity, or DT. However, an absolute difference of 0.5 in the Elabs A ratio at peak Valsalva compared to baseline was highly sensitive and specific for a pre-A LV pressure of ->15 mm Hg, 86% and 100% respectively. In addition, the positive predictive value(PPV) was 100% and the negative predictive valae(NPV) 77% for this Doppler index. In a subset of 18 patients with a normal baseline E/A ratio, the sensitivity and specificity of the E/abs A difference >0.5 was 80% and 100% respectively. The PPV was 100% and the NPV 67% for this subset, thus correctly separating those patients with normal vs. "pseudonormal" mitral filling. Conclusion: Doppler echocardiography ufilizing the Elabs A difference >0,5 before and at peak Valsalva reliably predicts pre-A LV filling in this selected group of patients and specifically is of additional benefit in those patients with a "pseudonormal" mitral filling pattern.
4 0 2 G LEFT VENTRICULAR MASS MEASUREMENT: COMPARISON OF THREE METHODS OF M-MODE ECHOCARDIOGRAPHY USING MAGNETIC RESONANCE IMAGING AS THE STANDARD Constantinos G Missouris, MRCP, Sandy M Forbat* MRCP, S Richard Underwood* MD, MRCP, Donald RJ Singer, MD, MRCP, Graham A MacGregor, FRCP. St George's Hospital Medical School & *National Heart Lung Instilute, Imperial College, London, UK
Magnetic resonance imaging (MRI) is an accurate method for measurement of left ventricular mass (LVM). We compared three methods of LVM measurement by M-mode echocardiography (echo) using MRI as the standard in 24 untreated patients with essential hypertension, average supine blood pressure 159/102195%C1:154-165/99-1041 mm Fig (Arteriosonde), mean age 51147-55 years], 19M:5F; ll black;ll white; 2 Asian. LVM was calculated from one dimensional M-mode (Fiewlett~ Packard 1000c; short axis view) recordings obtained in diastole using (1) tile American Society of Echocardiography (ASE) convention, (2) the Penn convention and (3) the Teichholz's volume corrected formula. For MRI (Picker 2055, 0.5 Tesla, short axis images in systole), myocardial area was measured for each slice and the mean areas summed to give myocardial volume. Using the three slandard M-mode formulae, widely different values of LVM were obtained with echocardiography: ASE 319+21(SEM)g; Penn 273+19g; Teichholz 191+11 g. By MRI, LVM was 232+__11g (P<0.0I. Wilcoxon vs all M-mode formulae). Using the ASE and the Penn conventions, the difference between echocardiography and MRI became greater the higher the underlying value of LVM When the ASE and Penn formulae were applied to relevant one dimensional MR images there was a similar pauem of overestimation. As a further comparison of echo and MRI, systolic measurements of M-mode tracings were also made and LVM estimated from these using the ASE formula. These results were compared with those obtained using the ASE formula applied to single slice one dimensional MR measurements in systole. Mean LVM was significantly higher by MRI than by echo using tile systolic measurements applied to the ASE formula (387+21g and 312 _+16g respectively; P<0.01). Our findings suggest that the echocardiographic ASE and Penn conventions may overestimate LVM, particularly in patients with more severe hypertrophy. In contrast the Teiehholz volume-corrected formula gives average values lower than MRI. These large differences appear to result from false assumptions in the M-mode echocmdiographic formulae and may have important clinical implications for tile measurement of LVM in hypertensive subjects and for the assessment of the changes in LVM that may occur with treatment in these patients.