Missouri Chapter American College of Surgeons, Inc ... · transcript page will be updated with the...
53
MISSOURI CHAPTER AMERICAN COLLEGE OF SURGEONS, INC. 45th Annual Professional Meeting June 8 - 10, 2012 Missouri Chapter American College of Surgeons, Inc. Chartered December 7, 1967 This Program is designed to provide a platform for Associate Fellows and Fellows to share their surgical experiences and techniques and to encourage scientific participation by resident surgeons. Accreditation Statement The American College of Surgeons is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. AMA PRA Category 1 Credits TM The American College of Surgeons designates this live activity for a maximum of 10.50 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Transcript of Missouri Chapter American College of Surgeons, Inc ... · transcript page will be updated with the...
MISSOURI CHAPTER AMERICAN COLLEGE OF SURGEONS, INC.
45th Annual Professional Meeting June 8 - 10, 2012
Missouri Chapter American College of Surgeons, Inc.
Chartered December 7, 1967
This Program is designed to provide a platform for Associate Fellows and Fellows to share their surgical experiences and techniques and to
encourage scientific participation by resident surgeons.
Accreditation Statement The American College of Surgeons is accredited by the Accreditation
Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians.
AMA PRA Category 1 CreditsTM
The American College of Surgeons designates this live activity for a maximum of 10.50 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.

2
Fellowship Pledge
Recognizing that the American College of Surgeons seeks to exemplify and
develop the highest traditions of our ancient profession, I hereby pledge myself, as a condition of fellowship in the College, to live in strict accordance with its
principles and regulations. I pledge myself to pursue the practice of surgery with honesty and to place the welfare and the rights of my patients above all else. I
promise to deal with each patient, as I would wish to be dealt with if I was in the patient’s position, and I will set my fees commensurate with the services rendered.
I will take no part in any arrangement, such as fee splitting or itinerant surgery, which induces referral or treatment for reason other than the patient’s best welfare. Upon my honor, I declare that I will advance my knowledge and skills, will respect my colleagues, and will seek their counsel when in doubt about my own abilities, in turn, I will willingly help my colleagues when requested. Finally, I solemnly pledge myself to cooperate in advancing and extending the art and science of
surgery by my Fellowship in the American College of Surgeons.

AMERICAN COLLEGE OF SURGEONS EVALUATION FORM
Missouri Chapter American College of Surgeons 45th Annual Professional Meeting
The Country Club and Spa - Lake Ozark, Missouri June 8 – 10, 2012
IN ORDER TO RECEIVE A CME CERTIFICATE, PLEASE BRING THIS COMPLETED FORM TO REGISTRATION DESK HOURS OF OPERATION ARE June 8 – 10, 2012 – 7 am to 2 pm
As a participant at this educational activity, I attended ________ hours* of sessions.
*1 hour = 1 AMA PRA Category 1 credit™
If applicable, insert the following: *Note: CME Certificates will be mailed June 30, 2012.
Please check the box if you are a member of the American College of Surgeons. Your ACS Portal MY CME transcript page will be updated with the credits earned within 3 months of this meeting. Your ACS member number is important to ensure proper transfer of credit. ACS Member # _______________________
PLEASE PRINT NAME_________________________________________email__________________________________________
Instructions: Please circle the appropriate number for each question
Excellent
Very Good Good Fair Poor
1. Overall, how would you rate this educational activity? 5 4 3 2 1
Strongly Agree Agree Neutral Disagree
Strongly Disagree
2. Program topics and content met the stated objectives 5 4 3 2 1
3. Content was relevant to my educational needs 5 4 3 2 1
4. Educational format was conducive to learning 5 4 3 2 1
5. Acquired knowledge will be applied in my practice environment 5 4 3 2 1
6. I will seek additional information on this subject 5 4 3 2 1
7. Program was fair, objective, and unbiased toward any product or program 5 4 3 2 1
Please explain any specific instance(s) of bias or conflict of interest. _________________________________________________________________________________________
_________________________________________________________________________________________
8. List a minimum of two things you are going to change in your practice as a result of what you have learned at this activity. _________________________________________________________________________________________
_________________________________________________________________________________________ 9. Describe the barriers anticipated when implementing the above changes: _________________________________________________________________________________________
_________________________________________________________________________________________
10. Do you have any suggestions for future topics to support and/or expand on what you have learned at this activity?
_________________________________________________________________________________________
_________________________________________________________________________________________
Additional Comments
______________________________________________________________________________________________
_________________________________________________________________________________________
_______________________________________________________________________________________________________ _

4
(Intentionally Left Blank)
5
LEARNING OBJECTIVES
1. Learn how to apply the ACOSOG Z-11 data to decision-making for patients
with sentinel node involvement and become familiar with its limitations.
2. Demonstrate awareness of current research activities within the Chapter and potential application to patient care.
3. Understand the future of the physician workforce over the next 20 years.
4. Recognize the internal and external factors which currently are limiting Graduate Medical.
5. Gain perspective of advances in the management of pelvic and external genitalia trauma.
6. Learn rational application of screening policies.
7. Discuss the available molecular diagnostic tools for prognostication in
patients with breast cancer.
8. Interpret the results of molecular diagnostics for patient treatment decision-making purposes.
9. Identify injury patterns that benefit from early orthopedic intervention. 10. Identify orthopedic pelvic trauma management principles and recent change.
11. Recognize the long term outcomes from pelvic trauma.
12. Describe new pharmacologic adjuncts used in contemporary trauma care.
13. Learn the current status of trauma system development in Missouri.
14. Learn about that the most common cause of familial gastric cancer is a
germline E-cadherin mutation.
15. Understand the roles and limitations of molecular staging in bladder cancer, renal cell carcinoma, and melanoma.
6
LEARNING OBJECTIVES (Continued)
16. Understand the link that is being demonstrated between hernia mesh design
and clinical failure modes.
17. Learn the differentiation between non-woven, microfiber polypropylene and historical knitted and woven hernia mesh materials.
18. Understand who the U.S. Preventive Services Task Force is and how a
recommendation of preventive services is developed.
19. Understand evidence about benefits and harms of prostate cancer screening with the PSA test.

7
2011-2012 OFFICERS
PRESIDENT Mark R. Wakefield, MD, FACS
Columbia, Missouri
VICE PRESIDENT Julie A. Margenthaler, MD, FACS
Saint Louis, Missouri
SECRETARY – TREASURER
Stanley M. Augustin, MD, FACS Kansas City, Missouri
IMMEDIATE PAST PRESIDENT William G. Hawkins, MD, FACS
Saint Louis, Missouri
EDUCATION COMMITTEE Mark R. Wakefield, MD, FACS, Chairman
William G. Hawkins, MD, FACS Julie A. Margenthaler, MD, FACS
Andrew A. Wheeler, MD
ASSOCIATION OF WOMEN SURGEONS REPRESENTATIVE
Debra G. Koivunen, MD, FACS
CANCER COMMITTEE CHAIRMAN Julie A. Margenthaler, MD, FACS
GOVERNOR-AT-LARGE
William G. Hawkins, MD, FACS
TRAUMA COMMITTEE CHAIRMAN Bryan R. Troop, MD, FACS
ADVOCACY & POLICY COMMITTEE
Glenn E. Talboy, Jr., MD, FACS

8
SPECIAL SOCIETY GOVERNORS James C. Denneny, III, MD, FACS James W. Fleshman, Jr, MD, FACS
Bryan F. Meyers, MD, FACS
COUNCILORS
TERMS EXPIRING JUNE 2012
H. Scott Bjerke, MD FACS Kansas City, Missouri
Paul S. Dale, MD, FACS
Columbia, Missouri
TERMS EXPIRING JUNE 2013 Stephen H. Colbert, MD, FACS
Columbia, Missouri
John P. Kirby, MD, FACS Saint Louis, Missouri
TERMS EXPIRING JUNE 2014
Bashar Safar, MBBS, FACS Saint Louis, Missouri
RESIDENT COUNCILORS
Dominic E. Sanford, MD Saint Louis, Missouri
Brook V. Nelson, MD Kansas City, Missouri
(term expiring June 2012)
Andrew A. Wheeler, MD Columbia, Missouri
(term expiring June 2012)

9
PAST PRESIDENTS
WILLIAM G. HAWKINS, MD, FACS – 2010 - 2011 GLENN E. TALBOY, JR, MD, FACS – 2009 - 2010
WALTER R. PETERS, MD, FACS – 2008-2009 MATTHEW J. CONCANNON, MD, FACS – 2007-2008
JOHN G. ADAMS, JR, MD, FACS – 2006-2007 C. ROBERT WETZEL, MD, FACS – 2004 - 2006 DEBRA G. KOIVUNEN, MD, FACS – 2003-2004
JOHN W. SHOOK, MD, FACS – 2002-2003 DONALD L. JACOBS, MD, FACS – 2001-2002
TODD L. DEMMY, MD, FACS – 2000-2001 BRENT ALLEN, MD, FACS – 1999-2000
MICHAEL BORKON, MD, FACS – 1998-1999 BRENT W. MIEDEMA, MD, FACS – 1997-1998
MARC J. SHAPIRO, MD, FACS – 1996-1997 CHARLES W. VANWAY, MD, FACS – 1995-1996 JOSEPH A. CORRADO, MD, FACS – 1994-1995
GREGORIO A. SICARDO, MD, FACS – 1993-1994 THOMAS S. HELLING, MD, FACS – 1992-1993 DONALD G. SESSIONS, MD. FACS – 1991-1992
JACK J. CURTIS, MD, FACS – 1990-1991 JOHN P CHRISTY, MD, FACS – 1989-1990
JOSEPH A. PINKERTON, JR., MD, FACS – 1988-1989 MICHAEL J. BUKSTEIN, MD, FACS – 1987-1988
ANTHONY E. FATHMAN, MD, FACS – 1986-1987 MARTIN J. BELL, MD, FACS – 1985-1986
EDWIN E. MACGEE, MD, FACS – 1984-1985 CHARLES B. ANDERSON, MD, FACS – 1983-1984
ROBERT S. HUNT, MD, FACS – 1982-1983 BOYD E. TERRY, MD, FACS – 1981-1982
HUGH S. HARRIS, JR., MD, FACS – 1980-1981 WILLIAM SHIEBER, MD, FACS – 1979-1980
RAYMOND A. AMOURY, MD, FACS – 1978-1979 LYNN KRAUSE, JR., MD, FACS – 1977-1978
MAX A. HEEB, MD, FACS – 1976-1977 PAUL G. KOONTZ, JR., MD, FACS – 1975-1976
HUGH E. STEPHENSON, JR., MD, FACS – 1974-1975 HARVEY R. BUTCHER, MD, FACS – 1973-1974 JOHN S. SPRATT, JR., MD, FACS – 1972-1973 ROBERT W. MAHER, MD, FACS – 1971-1972
FREDERICK J. MCCOY, MD, FACS – 1970-1971 CHARLES P. MCGINTY, MD, FACS – 1969-1970

10
CARL E. LISCHER, MD, FACS – 1968 -1969
Disclosure Information Missouri Chapter American College of Surgeons
45th Annual Professional Meeting June 8-10, 2012
In accordance with the ACCME’s Accreditation Criteria, the American College of Surgeons must ensure that anyone in a position to control the content of the educational activity has disclosed all relevant financial relationships with any commercial interest. Therefore, it is mandatory that both the program planning committee and speakers complete disclosure forms. Members of the program committee were required to disclose all financial relationships and speakers were required to disclose any financial relationship as it pertains to the content of the presentations. The ACCME defines a ‘commercial interest’ as “any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients”. It does not consider providers of clinical service directly to patients to be commercial interests. The ACCME considers “relevant” financial relationships as financial transactions (in any amount) that may create a conflict of interest and occur within the 12 months preceding the time that the individual is being asked to assume a role controlling content of the educational activity.
The ACCME also requires that ACS manage any reported conflict and eliminate the potential for bias during the session. The planning committee members and speakers were contacted and the conflicts listed below have been managed to our satisfaction. However, if you perceive a bias during a session, please advise us of the circumstances on the session evaluation form.
Please note we have advised the speakers that it is their responsibility to disclose at the start of their presentation if they will be describing the use of a device, product, or drug that is not FDA approved or the off-label use of an approved device, product, or drug or unapproved usage.
The requirement for disclosure is not intended to imply any impropriety of such relationships, but simply to identify such relationships through full disclosure, and to allow the audience to form its own judgments regarding the presentation.
SPEAKERS / MODERATORS/ CHAIRS / DISCUSSANTS
NOTHING TO
DISCLOSE
DISCLOSURE
(As it pertains to the content of the presentation)
Neeti Arora X Jordan Atkins, BS X Stanley M. Augustin, MD, FACS X Robert J. Avino X Stephen L. Barnes, MD, FACS X Stephanie Bonne, MD X Nishal Brahmbhatt X Jeffery P. Coughenour, MD, FACS X Brett D. Crist, MD, FACS X James M. Cummings, MD, FACS X Sekhar Dharmarajan, MD X Bernard J. DuBray, MD X Michelle M. Eagan, MD X Stephen Eaton, MD X Leisha Elmore, MPHS X

11
Oluwadamilola M. Fayanju, MD, MPHS X Evan N. Feldman, MD X Ryan C. Fields, MD X Gurpreet Gill, MD X William G. Hawkins, MD, FACS X Jacob R. Hopping, MD X Jason D. Keune, MD, MBA X Michael L. LeFevre, MD, MSPH X Julie A. Margenthaler, MD, FACS X Thao Marquez, MD X Tonya Martin-Dunlap, MD X Grace Montenegro, MS, MD X Eric Nelson, MS, BME BG Medical; consulting fees; employment Walter R. Peters, MD, FACS X Jacob A. Quick, MD X Stefano Schena, MD, PhD X Steven Strasberg, MD X Matthew J. Strouch, MD X William J. Symons, MD X Keith Thomae, MD, FACS X Michael Thorpe, MD X Isaiah R. Thurbull, MD, PhD X Charles W. Van Way, III, MD, FACS X Mark R. Wakefield, MD, FACS X Alison Witte, MD X Zaynab Zarrabi X
PLANNING COMMITTEE
NOTHING TO DISCLOSE
DISCLOSURE (All commercial relationships)
William G. Hawkins, MD, FACS 1) New Link Genetics; grant; Institutional PI on clinical trial 2) Gilead; grant; Institutional PI on clinical trial 3) Adura; lab processing fee; Fee charged for processing clinical trial bloodwork
Julie A. Margenthaler, MD, FACS X Mark R. Wakefield, MD, FACS X Andrew A. Wheeler, MD X
12
Schedule of Events
Thursday, June 7, 2012
6:30 P.M. Council Meeting Dinner (Officers, Councilors, Guests, and Former Presidents)
JB Hook’s Restaurant; 2260 Bagnell Dam Blvd Invitation letter has been mailed
Friday, June 8, 2012
7:00 A.M. Registration – Mediterranean A 7:00 – 8:00 A.M. Continental Breakfast – Mediterranean B
8:00 A.M. Welcome and Opening Remarks – Mediterranean A
Mark R. Wakefield, MD, FACS - President
8:10 – 9:30 A.M. Session I: Benign Surgical Disease – Mediterranean A
Moderator: Stanley M. Augustin, MD, FACS
* Resident/Fellow Paper Competition
** Student Paper Competition
(7 minute presentations and 15 minutes for group Q/A)
8:10 A.M. *Michelle M. Eagan, MD - University of Missouri - Kansas City, “Percutaneous Abscess Drainage Of Diverticulitis With Post-Procedural Complication Of An Enterostomy: Diagnosis, Treatment, And Management With Review Of The Literature.”
8:17 A.M. Sekhar Dharmarajan, MD - Washington University, “Prone Jackknife Position During Perineal Dissection Reduces Intraoperative Rectal Perforation After Abdominoperineal Resection.”

13
8:24 A.M. Stefano Schena, MD, PhD - Washington University, “Towards A Totally Robotic-Assisted Thoracic Surgery Service: Single Center Experience Within A Large Metropolitan Area.”
8:31 A.M. *Evan N. Feldman, MD - Washington University, “Covered Self-Expanding Metal Stents For Treatment Of Anastomotic Leak After Colorectal Resection.”
8:38 A.M. **Zaynab Zarrabi - Kansas City University of Medicine and Biomedical Sciences, “Head And Neck Manifestations Of Porphyria Cutanea Tarda.”
8:45 A.M. *Bernard J. DuBray, MD - Washington University, “The Importance Of CD47 In The Mediation Of Hepatic Ischemia-Reperfusion Injury.”
8:52 A.M. **Nishal Brahmbhatt - St. Luke's Hospital Plaza, “Infected Urachal Cyst: A Case Report And Literature Review In Surgical Management Techniques.”
8:59 A.M. *Jacob R. Hopping, MD - Saint Louis University, “Single Port Laparoscopic Colectomy: The Learning Curve.”
9:00 – 9:15 A.M. Group Questions and Answers
9:30 – 10:00 A.M. Break and Visit Exhibits – Mediterranean B
10:00 – 12:00 P.M. Session II and III: Committee on Cancer Abstract Contest - Mediterranean A
Moderator: Julie A. Margenthaler, MD, FACS
* Resident/Fellow Paper Competition
** Student Paper Competition
(7 Minute presentations with 3 minutes Q/A)
Session II: Oncology
10:00 A.M. Steven Strasberg, MD - Washington University, “Anatomic Basis And Long Term Results Of The RAMPS Procedure.”
10:10 A.M. *Matthew J. Strouch, MD - Washington University, “Time To Initiation Of Postoperative Chemotherapy: A Novel Surrogate Of Improved Recovery In Patients Undergoing Laparoscopic Low Anterior Resection For Rectal Cancer.”

14
10:20 A.M. *Grace Montenegro, MS, MD - Washington University, “Extent Of Colectomy In Patients Under 50 With Sporadic Colon Cancer.”
10:30 A.M. *Thao T. Marquez, MD - Washington University, “Is Distal Margin A Factor In Oncologic Outcomes For Rectal Cancer In Current Therapy?”
10:40 A.M. **Neeti Arora - Saint Louis University, “Geographical Variation In Surveillance Intensity After Curative-Intent Treatment For Ovarian Cancer Patients.”
Session III: Breast
10:50 A.M. *Tonya Martin-Dunlap, MD - Washington University, “Outcomes For Patients Who Are Diagnosed With Both Breast And Endometrial Cancer.”
11:00 A.M. *Oluwadamilola M. Fayanju MD, MPHS - Washington University, “Patient And Process Factors Associated With Late-Stage Breast Cancer Diagnosis In Safety-Net Patients: A Prospective Study.”
11:10 A.M. **Jordan Atkins - Washington University, “Which Imaging Modality Is Superior For Prediction Of Response To Neoadjuvant Chemotherapy In Patients With Triple Negative Breast Cancer?”
11:20 A.M. *Tonya Martin-Dunlap, MD - Washington University, “Patient Factors Predictive Of Unilateral Mastectomy And Contralateral Prophylactic Mastectomy.”
11:30 A.M. **Leisha Elmore - Washington University, “Reconstruction Patterns In A Single Institution Cohort Of Women Undergoing Mastectomy For Breast Cancer.”
11:40 A.M. **Robert J. Avino - Saint Louis University, “Patient Surveillance After Breast Cancer Treatment: Impact Of MCOs.”

15
12:15 – 1:15 P.M. Missouri Commission on Cancer Luncheon – Mediterranean B
Panel Lecture/Discussion: “Molecular Diagnostics For The Surgical Oncologist”
Moderator: Julie A. Margenthaler, MD, FACS
Panelists:
Julie A. Margenthaler, MD, FACS (Breast)
Ryan C. Fields, MD (Melanoma)
William G. Hawkins, MD, FACS (HPB/Gastric)
Walter R. Peters, MD, FACS (Colorectal)
Mark R. Wakefield, MD, FACS (Bladder)
1:15 – 2:00 P.M. Jeopardy (Cash Prizes)
Moderator: Walter R. Peters, MD, FACS
2:00 – 4:00 P.M. Please Enjoy The Resort
4:00 P.M. Cruise Excursion (Meet in Hotel Lobby - Shuttle to Port Arrowhead
5:00 – 7:00 P.M. Lake Cruise Excursion by Tropic Island Cruises, Inc
Families and guests welcome Cash Bar and Light fare
Cruise Drop Off at Shady Gators
Enjoy dinner on your own at Shady Gators Shuttle provided to resort (immediately and after dinner)
16
Saturday, June 9, 2012
7:00 A.M. Registration –AB Board Room 7:00 – 8:00 A.M. Breakfast – AB Board Room
“Improving Upon Historical Hernia Mesh Failure Modes” Eric Nelson, MS, BME Vice President of Technology BG Medical, LLC Speaker Introduction: Mark R. Wakefield, MD, FACS - Mediterranean A
8:15 – 9:15 A.M. “The Inner Workings Leading To Screening Recommendation From The U.S. Preventive Services Task Force” Michael L. LeFevre, MD, MSPH Future of Family Medicine Professor & Vice Chair; University of Missouri, Columbia, MO Chief Medical Information Officer; MU Health Care, Columbia, MO Co-Vice Chair, U.S. Preventive Services Task Force
9:15 – 9:45 A.M. Break and Visit Exhibits – Mediterranean B
9:45 – 12:15 P.M. Session IV: Committee on Trauma abstract/paper competition - Mediterranean A
Moderator: Stephen L. Barnes, MD, FACS
* Basic Science
** Clinical
(9 minute presentations and 3 minutes Q/A)
9:45 A.M. *Stephen Eaton, MD - Washington University, “Evaluation Of Infected Abdominal Mesh In A Murine Model Of Peritonitis.”
9:57 A.M. *Isaiah R. Turnbull, MD, PhD - Washington University, “Severe Multisystem Injury Alters Immune Cell Expression Of TLR-4 In A Mouse Model Of Trauma.”
17
10:09A.M. **Michael Thorpe, MD - Saint Louis University, “Is The Micriobiology The Answer To A Successful Lower Extremity Traumatic Free Flap.”
10:21 A.M. **Stephanie Bonne, MD - Washington University, “Duty Hour Heavy Clerkships Do Not Adversely Affect Surgery Clerkship Test Scores.”
10:33 A.M. **Alison Witte, MD - Mercy Saint Louis, “Our Experience With Open Reduction – Internal Fixation Of Rib Fractures.”
10:45 A.M. **Jason D. Keune, MD, MBA - Washington University, “Antibiotic Prophylaxis In Patients With Open Abdomen After Exploratory Laparotomy For Trauma.”
10:57 A.M. **Gurpreet Gill, MD – University of Missouri-Kansas City, “Emergency Department Thoracotomy : Case Presentation And Review Of Indications.”
11:09 A.M. **Jacob A. Quick, MD – University of Missouri-Columbia, “Less Is More: Low-Dose Prothrombin Complex Concentrate Effective In Acute Care Surgery Patients.”
11:21A.M. **Jacob A. Quick, MD – University of Missouri-Columbia, “X-Ray Exposure In The Trauma Bay: Results Of A Radiation Field Analysis.”
11:33 A.M. **Leisha Elmore – Washington University, “Operative Management Of Rib Fractures In The Setting Of Flail Chest: A Systematic Review And Meta-Analysis.”
11:45 A.M. **William J. Symons, MD – Washington University, “Trauma Rehab Outcome Score (Tros), A Quick And Simple Tool To Determine Trauma Patient’s Functional Abilities.”
12:15 – 1:45 P.M. Lunch Buffett – Mediterranean A
Session on Trauma
Moderator: Mark R. Wakefield, MD, FACS

18
12:15 – 12:45 P.M. “The Current Status Of Trauma Care In Missouri” Jeffery P. Coughenour, MD, FACS Assistant Professor, Acute Care Surgery & Medical Director, Surgical Critical Care; University of Missouri, Columbia, MO Central Region Medical Director, Missouri Emergency Medical Services System
12:45 – 1:15 P.M. “Orthopedic Pelvic Trauma Update” Brett D. Crist, MD, FACS Associate Professor & Co-Director Orthopaedic Trauma Service, Associate Director Joint Preservation Service Department of Orthopaedic Surgery ; University of Missouri, Columbia, MO
1:15 – 1:45 P.M. “Male Genitalia Trauma – A Primer For General Surgeons” James M. Cummings, MD, FACS Professor, Urological Surgery University of Missouri, Columbia, MO
1:45 P.M. The Missouri American College of Surgeons Committee
on Trauma Bi-Annual Business Meeting – Mediterranean A
3:00 P.M. Golf Tournament – Osage National Golf Resort
Reservations made for 12
If interested, please contact Denise @ www.moacs.org “Contact Us”
Sunday, June 10, 2012
7:30 – 9:30 A.M. Buffet Breakfast – Mediterranean B Families and guests welcome
8:00 – 9:00 A.M. Officers and Councilors Meeting – Executive Board Room
19
9:00 – 10:30 A.M. Session V: Mediterranean A
Moderator: Mark R. Wakefield, MD, FACS
9:00 A.M. Keith Thomae, MD, FACS – Scotland County Hospital, “The Thomae Plan: The Next American Revolution To Combat The Current Medico-Legal Disaster.”
9:15 A.M. Keith Thomae, MD, FACS – Scotland County Hospital,
“Increasing Uncontrolled Downward Spiral Of Rural Trauma Care: Now Helicopter Insurance.”
9:30 A.M. “The Crisis in GME: Will We Have Enough Surgeons?”
Charles W. Van Way, III, MD Professor of Surgery Sosland/Missouri Endowed Chair of Trauma Research University of Missouri, Kansas City, MO
10:30 – 12:00 P.M. Business Meeting and Awards- Mark R. Wakefield, MD, FACS - President
President Introductions and Thank Yous Reports --
Secretary/Treasurer Report Association of Women Surgeons Committee on Cancer Committee on Trauma Governor
Announcements Nominee Slate and Vote Awards Change of the Guard
12:00 P.M. Enjoy The Resort
20
The Missouri Chapter of the American College of Surgeons gratefully acknowledges the following companies for their educational grants.
SPONSORS
Missouri Professionals Mutual Educational Grant
BG Medical, LLC Sponsored Breakfast-Saturday
21
EXHIBITORS
BG Medical
Darvol Inc, a Bard Company
Merck
Missouri Professionals Mutual
Siteman Cancer Center
Synthes CMF
22
ABSTRACTS PRESENTED 1. PERCUTANEOUS ABSCESS DRAINAGE OF DIVERTICULITIS
WITH POST-PROCEDURAL COMPLICATION OF AN ENTEROSTOMY: DIAGNOSIS, TREATMENT, AND MANAGEMENT WITH REVIEW OF THE LITERATURE
Michelle M. Eagan, MD, David A. Manning, MD, and Benoit Blondeau, MD University of Missouri-Kansas City Percutaneous abscess drainage (PAD) is frequently used for drainage of intraperitoneal abscesses related to diverticulitis, in selected patients. The reported complication rate is about 10% overall. The incidence of an inadvertent enterotomy with a drainage catheter is quoted to be around 1% or less. The management of this post-procedural complication is rarely described. Management for percutaneous bowel transgression described in the literature includes letting the tract fistulize for one to two weeks and slowly remove the catheter over the next four weeks. The objective of our paper is to design an algorithm to assist in the management of percutaneous drainage of abscesses with a special emphasis on the early detection of diagnosis and treatment. For this purpose an extensive review of the literature was conducted. CASE REPORT: We report the case of a 30 year-old man who was admitted with diverticulitis. His mildly severe diverticulitis, Hinchey II, allowed us to treat him with a percutaneous drain and intravenous antibiotics. Five days later, we diagnosed an enterotomy created by the drain. We had then to manage both the evolution of the original condition and the complication generated by the drain. The patient underwent multiple drainage procedures. His nutrition was supplied by parenteral means. A multidisciplinary approach was the basis of our therapeutics, and in the end, continuing non-operative management. The patient improved and was discharged home a few days later. The same paradigm of treatment applied to diverticulitis was applied to the enterotomy and the patient was managed non-operatively. CONCLUSION: In conclusion, non-operative management of mild diverticulitis, despite its favorable image as minimally invasive, can generate complications with their independent evolution. Concomitant treatment of diverticulitis and an enterotomy is challenging. The literature almost ignores this subset of complications. We created, based on our own observations and the scarce literature input, a decisional algorithm. Management and treatment of the post-procedural complication by early removal of the catheter from the bowel and close observation can be done in selected patients.
23
2. PRONE JACKKNIFE POSITION DURING PERINEAL DISSECTION REDUCES INTRAOPERATIVE RECTAL PERFORATION AFTER ABDOMINOPERINEAL RESECTION
Sekhar Dharmarajan, MD, Bashar Safar, MD, Matthew Mutch, MD, Elisa Birnbaum, MD, James Fleshman, MD, Steven Hunt, MD Washington University Purpose: Positive radial margins and intraoperative rectal perforation adversely affect outcome after abdominoperineal resection (APR) for low rectal cancer. Use of the prone jackknife position during the perineal dissection may improve exposure and therefore oncologic outcome. Our purpose was to determine whether performing the perineal dissection of APR in prone jackknife versus lithotomy position improves radial margin clearance and reduces intraoperative rectal perforations. Methods: An IRB-approved retrospective review of 130 cases of APRs over 8 years was performed after excluding patients with no radial margin reported, non-adenocarcinoma pathology, and pelvic exenterations. Primary endpoints of radial margin and intraoperative rectal perforation were obtained from pathology reports. Data on patient demographics, preoperative staging, preoperative therapy, and intraoperative positioning was obtained. Statistical analysis was performed using t test or Fisher’s exact test with significance set at p<0.05. Results: Perineal dissection was performed in prone jackknife position in 65 patients and in lithotomy position in 65 patients. There were no significant differences between these groups in terms of patient gender, age, percent receiving preoperative therapy, distance of tumor from dentate line, or preoperative stage. There was no significant difference in mean radial margin between patients whose perineal dissection was performed in the prone jackknife versus lithotomy position (0.54 cm vs. 0.56 cm, p=0.76). The percent of positive radial margins in each group was not significantly different (17% vs. 13%, p=0.62). The number of intraoperative rectal perforations was significantly lower in patients in the prone jackknife group than in the lithotomy group (6% vs. 17%, p=0.05). In patients with pathologic stage T4 tumors (locally advanced tumors), there was 25% intraoperative rectal perforation rate in the lithotomy group compared to 0% in the prone jackknife group. Conclusions: APR with perineal dissection performed in prone jackknife position is associated with reduced intraoperative rectal perforation compared to lithotomy position, especially in patients with locally advanced, pathologic stage T4 tumors.

24
3. TOWARDS A TOTALLY ROBOTIC-ASSISTED THORACIC SURGERY SERVICE: SINGLE CENTER EXPERIENCE WITHIN A LARGE METROPOLITAN AREA
Stefano Schena MD, PhD, Varun Puri MD, Sunil Prasad MD and Nabil Munfakh MD Christian Hospital NE, Washington University Background: Robotic technology is rapidly expanding in multiple surgical specialties. The application in thoracic surgery is new and represents a mechanical evolution of video-assisted (VATS) instrumentation with its limitations due to restricted maneuverability within a rigid cavity and lack of articulation instruments as well as tridimensional imaging. We report our early experience. Material: A robotic thoracic surgical program was initiated in February 2011 and an attempt made to perform all potential thoracoscopic procedures via a robotic-assisted approach. Patients were selected on the basis of being candidates for a minimally invasive approach including criteria such as known or suspected early-stage non small-cell lung cancer, no prior thoracotomy, no neoadjuvant therapy, and a body mass index (BMI) less than 40 kg/m2. We retrospectively assessed perioperative and early postoperative outcomes. Results: A total of 54 (18 M and 36 F, average age 61.9 ± 13.8 years) robotic-assisted thoracic procedures were performed from February 2011 to April 2012. These included lobectomies for a diagnosis of lung carcinoma (n= 21) and diagnostic/therapeutic wedge resections (n= 27). The remaining procedures were respectively thymectomies (n= 2), mediastinal mass biopsies (n= 3) and excision of pericardial cyst (n= 1). No intraoperative mortality occurred. Conversion of the robotic-assisted procedure to a thoracotomy was necessary in six patients (11%). In two instances it was due to accidental pulmonary artery injury, while the remaining cases were related to suboptimal visualization of hilar anatomical structures. There was one (1.8%) in-hospital death due to severe respiratory failure, not responsive even to ECMO treatment. One death (1.8%) occurred within a 30-day period secondary to a severe stroke. Four (7.4%) patients had postoperative complications (one severe air leak, one pneumothorax, one recurrent effusion, one acute renal failure). The mean overall length of stay was 5.4 (range 2-17) days. Conclusions: Robotic-assisted thoracic surgery is safe and feasible. Short-term outcomes for robotic-assisted lung resection appear comparable to retrospective thoracoscopic series.
25
4. COVERED SELF-EXPANDING METAL STENTS FOR TREATMENT OF ANASTOMOTIC LEAK AFTER COLORECTAL RESECTION
Evan N. Feldman MD, James W. Fleshman MD Washington University PURPOSE: To determine whether the placement of a covered self-expanding metal stent (SEMS) for a colorectal anastomotic leak will allow for anastomotic healing without the need for a diverting stoma METHODS: Retrospective cohort study of patients with leak of colorectal anastomosis treated by covered SEMS placement RESULTS: Between 8/2/2010 and 12/9/2011, covered SEMS were placed across the site of dehiscence in seven patients with anastomotic leak after anterior rectal resection. All anastomoses were stapled and no patients had received neoadjuvant chemotherapy or radiation or diverting loop ileostomy at the time of initial operation. The mean height of the stented anastomoses from the anal verge was 7.6 cm (range 4-17 cm). The mean time to diagnosis of anastomotic leak was 7 days (range 3-14 days). CT scan confirmed a contained collection in all cases. All patients were hemodynamically stable and had a drain located in the pelvic collection prior to the placement of a stent. The mean duration of stent placement was 28 days (range 10-50 days). Five of the seven patients had complete healing of the dehiscence as determined by resolution of symptoms, digital rectal exam, and proctoscopic exam. One of these patients had a non-healing dehiscence despite a loop ileostomy creation and omental flap placement after their ant erior rectal resection. This patient had a stent placed with subsequent complete healing of the anastomotic disruption. Two patients required diverting loop ileostomy creation despite placement of the stent. One patient with ischemia of the pre-anastomotic colon required anastomosis revision and diversion on post-stent day 10. The other patient developed a delayed rectovaginal fistula on post-stent day 37 and required subsequent repair and loop ileostomy. CONCLUSIONS: Stenting the disrupted colorectal anastomosis may be a viable alternative to fecal diversion in hemodynamically stable patients in an attempt to avoid ostomy formation after anastomotic leak or as an adjunct to healing after ostomy formation. Larger, prospective studies are required to validate the efficacy and safety of this approach.

26
5. HEAD AND NECK MANIFESTATIONS OF PORPHYRIA CUTANEA TARDA
Zaynab Zarrabi, MS III; Gary Y. Shaw, MD, FACS Kansas City University of Medicine and Biomedical Sciences Porphyria cutanea tarda (PCT), the most common of the porphyrias, is a condition resulting from a disruption in the heme biosynthetic pathway. PCT occurs in both sporadic and familial forms. PCT most commonly occurs in the sporadic form, making up 80% of cases. Factors contributing to the development of PCT include alcohol abuse, iron excess, estrogen, human immunodeficiency virus (HIV), and most commonly hepatitis C virus (HCV). Presenting symptoms of PCT may include skin fragility, photosensitivity, vesicular and bullous skin lesions, hyperpigmentation, sclerodermatous skin changes, as well as hypertrichosis. Most commonly, lesions occur on the dorsal aspect of the hands, but may also present with head and neck manifestations. The authors present cases of PCT involving head and neck manifestations, as well as a review of the literature of this interesting disease.

27
6. THE IMPORTANCE OF CD47 IN THE MEDIATION OF HEPATIC ISCHEMIA-REPERFUSION INJURY
DuBray Jr BJ, Manning PT, Frazier WA, Gunter K, Hassan H, Balachandran P, Upadhya GA, Jia J, Anderson CD, Mohanakumar T, Chapman WC Washington University Background: Hepatic ischemia-reperfusion injury (IRI) continues to hinder the outcomes of major hepatectomy and transplantation. Vasoconstriction from reductions in nitric oxide (NO) relative to endothelin (ET) causes hepatic microcirculatory failure, which accentuates IRI. Thrombospondin-1 (TSP1) binding to the receptor CD47 potentiates sinusoidal NO/ET imbalance through inhibition of NO/cGMP signaling. The goal of this study is to investigate TSP1/CD47 in hepatic IRI. Methods: C57BL/6 wild type (WT) and CD47 knockout (KO) mice underwent 90 minutes of 70% hepatic ischemia. Separately, WT mice received a CD47 blocking monoclonal antibody (mAb) vs. no injection (control) prior to procurement of 4mm cubes of hepatic tissue. Liver cubes were then plated individually in wells containing hepatocyte medium and placed into an anaerobic chamber for 60 minutes (pO2 content of media = 33.7 mmHg). Plates were then removed and allowed to “rediffuse” under normoxic conditions. Finally, WT mice received mAb vs. control IgG prior to IRI. 6 hours following re-perfusion/diffusion, specimens were collected and examined for markers of hepatocellular injury. Data were analyzed using student’s t-test. Results: KO mice were protected from IRI with reductions in hepatic transaminase and inflammatory cytokine release compared to WT mice (p = 0.03, 0.02, and < 0.01 for AST, ALT, and IL-1β, respectively). Administration of CD47 mAb attenuated IRI both in vitro and in vivo with reductions in hepatic transaminase release compared to their respective controls (p < 0.05 for AST and ALT). CD47 mAb attenuated apoptosis in hepatic organ culture with significant reduction in TUNEL activity compared to control (p = 0.02). Conclusions: The TSP1 receptor CD47 is a significant mediator of hepatic IRI. In vitro ischemia and rediffusion of liver cubes is an efficient method of screening potential therapies prior to in vivo experimentation. Mitigation of hepatic IRI with in vivo mAb blockade of the CD47/TSP1 interaction may have a therapeutic role.

28
7. INFECTED URACHAL CYST: A CASE REPORT AND LITERATURE REVIEW IN SURGICAL MANAGEMENT TECHNIQUES
Nishal Brahmbhatt, Dr. Daniel Margolin St. Luke's Hospital Plaza The urachus is a fibrous remnant of the allantois which is usually obliterated in the fourth month of gestation. Complications associated with a persistent urachus have been identified and treated since the 1550’s. Of the known complications, infection of the urachus is the most common. Patients presenting with signs and symptoms of an infection should be initially treated with antibiotic therapy followed by surgical excision of the cyst to prevent further serious complications such as urachal cancer. Surgical techniques that maybe used are the two stage open procedure, one stage open procedure, traditional laparoscopic procedure and robot assisted laparoscopic procedure. While surgical excision is the general consensus, there is no mention as to which procedure is the best. Over the years there has been transition from two stage open procedure to the one stage open procedure. With improvements in laparoscopic procedures, the trend has been to move towards minimally invasive surgery (MIS). From the literature reviewed between 1994 - 2010, it is safe to say that if one were to require an open procedure, the two stage procedure is definitely more superior to the one stage. Given an option to choose between an open procedure and MIS, minimally invasive surgery is definitely the superior option. Robot assisted surgery is an up and rising field but it is too soon to make a decision as to where it lies in relation to the other three procedures. Laparoscopic surgery has been found to have the shortest length of stay, fewer to no intra-operative and post-operative complications, a shorter recovery period.

29
8. SINGLE PORT LAPAROSCOPIC COLECTOMY: THE LEARNING CURVE
Jacob R. Hopping MD, Ovunc Bardakcioglu MD FACS Saint Louis University Author A has no disclosures. Author B is a proctor with Intuitive Surgical BACKGROUND: Single port laparoscopic colectomy (SPLC) is described as a new technique. These initial case reports show the safety and feasibility, but the learning curve for this technique is unknown. METHODS: Between July 2009 and September 2010, 20 consecutive patients with indication for right hemicolectomy underwent a SPL approach. The patients were followed for 30 days. RESULTS: The median age was 65 (59-88). 90% of patients were male. The median BMI was 28 (20-35). 75% of patients had significant co-morbidities with an ASA class of 3 and 4. The estimated blood loss was 25ml (25-250). The median number of lymph nodes for patients diagnosed with adenocarcinoma was 16 (8-23). There was one conversion to hand-assisted-laparoscopic (case 6) and one to open colectomy (case 9) due to the inability of safe vessel ligation. The median hospital stay was 4.5 days (3 to 7). The LOS for the first 10 patients was 5.1 days, and 3.9 for the last 10 (p=0.045). There were no significant postoperative complications within 30 days. The mean operative time for the first 10 cases was 198 min (148 to 272) and 123 min (98-150) for the subsequent 10 cases (p=0.0001). CONCLUSION: Single port laparoscopic right hemicolectomy can be safely performed in patients who are candidates for laparoscopy with a very low intraoperative and post-operative complication rate. The higher technical difficulty compared to conventional laparoscopy is reflected in the longer initial operative times. The learning curve for a surgeon with advanced laparoscopic skills and adequate procedure numbers seems to be short, requiring approximately 10 cases to decrease operative times to baseline. The role and feasibility of broad adaptation for single incision laparoscopy in colorectal surgery needs to be further evaluated in larger trials.
30
9. ANATOMIC BASIS AND LONG TERM RESULTS OF THE RAMPS PROCEDURE
Steven Strasberg, David Linehan, William Hawkins, and Ryan Fields Washington University BACKGROUND: The radical antegrade modular pancreatosplenectomy (RAMPS) procedure is a modification of standard distal pancreatosplenectomy. It was designed to provide the operative approach developed for cancers of the head of the pancreas to cancers of the body and tail of the pancreas, particularly with respect to the extent of node dissection and emphasis on obtaining microscopically negative tangential margins. The purpose of this report is to discuss the anatomical basis of the procedure and to provide long-term survival results. STUDY DESIGN: Forty-seven patients had RAMPS between 1999 and 2008. The decision to perform anterior vs posterior RAMPS was based on the position of the tumor as assessed by preoperative computed tomograms. Patients were entered in a prospective database and followed at intervals. RESULTS: Thirty-two patients had anterior RAMPS and 15 had posterior RAMPS. Twenty-four patients had resection of 33 organs in addition to the left adrenal gland in the posterior RAMPS. Specimens were inked in the operating room.Mean tumor size was 4.4 cm. Negative tangential margins were obtained in 89% of specimens. Overall, the R0 rate was 81%.Mean lymph node count was 18. There were no 30-day or in-hospital mortalities. Mean and median follow-uptimes of living patients were 44.4 and 26.4 months.Median survival was 26 months and 5-year overall actuarial survival was 35.5%. The actual survival of 23 patients whose surgery was performed more than 5 years before the time of analysis was 30.4%. CONCLUSIONS: RAMPS is associated with high negative tangential margin rates and very satisfactory survival rates for this aggressive tumor.

31
10. TIME TO INITIATION OF POSTOPERATIVE CHEMOTHERAPY: A NOVEL SURROGATE OF IMPROVED RECOVERY IN PATIENTS UNDERGOING LAPAROSCOPIC LOW ANTERIOR RESECTION FOR RECTAL CANCER.
Matthew J. Strouch MD, Gongfu Zhou PhD, James W. Fleshman MD, Matthew G. Mutch MD Washington University Purpose: This study aims to assess the effect of laparoscopic vs. open rectal cancer surgery on the time to induction of postoperative chemotherapy as a surrogate for patient recovery. Methods: A retrospective review of 150 consecutive patients who underwent low anterior resection (75 open, 75 laparoscopic) for stage II or III rectal cancer was performed. All patients included received postoperative chemotherapy, of which timing was at the discretion of the medical oncologist. Patient demographics, clinicopathologic variables, and time to induction of postoperative chemotherapy were compared between surgery groups. Multivariate analysis was performed to identify whether the approach of surgery or other pre-operative variables affect time to induction of postoperative chemotherapy. Results: There was no signficant difference in clinicopathologic variables between the groups including age, BMI, gender, preoperative albumin, preoperative hemoglobin, utilization of diverting ileostomy, preoperative radiation therapy, tumor grade, T stage, N stage, or final pathologic stage. On univariate analysis there were significant differences in intraoperative blood loss (300 vs. 448cc, p<0.01), length of stay (7.6 vs. 8.9 days, p<0.05), wound infection (12.0 vs. 24.0%, p<0.05), and tumor location (8.0 vs. 6.9 cm from anal verge, p<0.05) for laparoscopic vs. open patients, respectively. A significant decrease in median time to induction of postoperative chemotherapy was found for patients undergoing laparoscopic vs. open surgery (46 vs. 60 days, p<0.0001). Multivariate analysis adjusting for intraoperative blood loss, length of stay, tumor location, and wound infection demonstrated that approach of surgery was an independent predictor of time to postoperative chemotherapy (p<0.01). Conclusions: Laparoscopic rectal cancer surgery patients receive postoperative chemotherapy a median of 14 days earlier than open surgery patients. Time to induction of postoperative chemotherapy serves as a novel surrogate for improved recovery in laparoscopic rectal cancer surgery.

32
11. EXTENT OF COLECTOMY IN PATIENTS UNDER 50 WITH SPORADIC COLON CANCER
G Montenegro, MS MD, N Jamal, MBBS, WO Wolff, BS, E Birnbaum, MD, JW Fleshman, MD, S Hunt, MD, IJ Kodner,MD, M Mutch, MD, B Safar, MBBS MRCs, S Dharmarajan, MD Washington University Background: There is controversy as to whether sporadic colorectal cancer (CRC) in young patients (age < 50) has a more aggressive phenotype and therefore requires a more aggressive primary surgical approach. Total or subtotal colectomy may reduce the risk of metachronous cancer and the inconvenience of continued colonoscopic surveillance in these young patients however this must be balanced against functional outcomes and possible negative impact on quality of life. The aim of this study was to determine metachronous cancer rates, disease recurrence and overall survival following segmental (SR) versus extensive (ER) resection for sporadic CRC in patients under 50. Methods: The study was performed as an IRB-approved retrospective review of an institutional database of patients under the age of 50 who underwent surgical resection of CRC with curative intent from 1991 to 2009. Patients were excluded from the study if they had a diagnosis of hereditary CRC syndrome either known preoperatively or diagnosed postoperatively. Patients who underwent palliative surgical resection were excluded as well as those whose pathology was not available for review. ER was defined as subtotal or total abdominal colectomy or total proctocolectomy. Statistical analysis was performed using Fishers exact test for categorical variables and student’s t-test for continuous variables using graph pad instat with significance set at p < 0.5. Results: A total of 346 patients under the age of 50 who underwent surgical resection for CRC were identified. Average age of the cohort at time of surgery was 42.8 ± 6.4 years. Of these, 42 (12%) underwent ER and 304 (88%) underwent SR. There was no significant difference in pathologic stage distribution between the two groups (Stage 1- 19% vs 16%, Stage 2 – 25% vs 23%, Stage 3 – 25% vs 23%, Stage 4 – 31% vs 37%, p = 0.86). 9 patients (3%) in the SR group developed metachronous CRC versus 0 patients in the ER group (p= 0.61). Disease recurrence was identified in 86 (28%) patients in the SR group versus 12 (29%) patients in the ER group (p= 1.0). Mortality rates were 13% for the SR group versus 24% for the ER group (p= 0.06). Conclusions: For patients with sporadic CRC under the age of 50, there is no difference in metachronous CRC rates, disease recurrence or overall survival following segmental or extensive surgical resection. Given the functional compromise and potential negative impact on quality of life, there appears to be no oncologic benefit to extensive surgical resection for the treatment of sporadic CRC in patients under the age of 50.

33
12. IS DISTAL MARGIN A FACTOR IN ONCOLOGIC OUTCOMES FOR RECTAL CANCER IN CURRENT THERAPY?
Marquez TT, Mutch MG, Birnbaum EH, Fleshman JW, Safar, B Washington University Introduction: We sought to evaluate the oncologic outcomes of very close distal margins (< 2mm and <1cm) in the setting of current chemoradiation treatment. Methods: We retrospectively reviewed charts from our experience of consecutive rectal cancer patients with distal surgical resection margins <1cm between 1995 and 2010. All patients underwent preoperative radiation therapy followed by low anterior resection. We defined those with positive or very close distal margins as surgical distal margins 0-2mm (Group A) and compared outcomes to a group with close distal margins 3mm-1cm (Group B). We compared disease-free survival between these groups and evaluated for risk factors for disease recurrence in univariate and multivariate modeling. Results: Our institutional database revealed 82 patients with close distal resection margins <1cm and met our criteria of having neoadjuvant radiation treatment and low anterior resection. All patients had disease-free circumferential margins. There were 10 patients with positive or very close distal margins <2mm (Group A; n=10). There were 72 patients with distal margins 3mm-1cm (Group B). Mean follow-up time was 45.9 months. Overall, 15 patients had disease recurrence on follow-up (local=3, distant=12). Group A had one recurrence (local) while group B had 14 recurrences (local=2, distant =12). Of the local recurrences, one occurred in a patient with a positive margin, whereas two occurred in patients with 5mm and 1cm distal margin resections. Disease-free survival and recurrence did not differ significantly between these two groups (log rank test p=0.6259). Univariate analysis showed postoperative chemotherapy and pathologic stage were significant predictors of disease recurrence. Age was the only predictor of disease recurrence in multivariate model. Conclusion: Disease free survival was not affected by distal margin in patients who underwent neoadjuvant therapy. Pathologic stage and adjuvant chemotherapy in univariate analysis, and age on multivariate analysis, were predictors of disease recurrence. This suggests that close distal margins, given adequate chemoradiation and favorable tumor biology, does not affect oncologic outcomes.
34
13. GEOGRAPHICAL VARIATION IN SURVEILLANCE INTENSITY AFTER CURATIVE-INTENT TREATMENT FOR OVARIAN CANCER PATIENTS
N Arora, K Virgo, R Gibb, D Mutch, F Johnson St Louis University Introduction: Ovarian cancer is a major health problem. Most patients have advanced disease at the time of diagnosis. Curative treatment is offered to most patients but relapse is common. Post-treatment surveillance is felt to be useful. We used a survey instrument sent by convention mail to document the current practice of surveillance employed by the 943 members of the Society of Gynecologic Oncology (SGO). Methods: Our survey featured vignettes describing 4 patients with ovarian carcinoma with different prognoses. The SGO members were asked how often they recommended 11 surveillance modalities in the first 10 post-operative years. Only those members indicating that they performed surgery for ovarian carcinoma and also participated in post-treatment surveillance were considered evaluable. The responses documented remarkable variation in surveillance intensity. We determined whether the geographic location of the physician or the local health maintenance organization (HMO) penetration rate were responsible for the observed variation. Statistical analysis featured a generalized linear model with a Poisson distribution. The effects of physician location (US Census Region and Consolidated Metropolitan Statistical Area) and HMO penetration rate were calculated using generalized estimating equations (Statistical Analysis System). All tests were two sided. Results: 274 responses (29%) were evaluable. Many statistically significant differences were noted. For example, doctors in areas with low HMO penetration rate (0-29%) recommended 4.1±1.1 (mean ± SD) physical exams/year for a stage I ovarian carcinoma patient in post-treatment year 1; those in areas with 30-40% HMO penetration rate recommended 4.0±0.9 physical exams/year (p= 0.008). All such statistically significant differences were clinically small. Conclusions: The variation in practice is prima facie evidence of overuse and/or underuse and/or misuse of scarce medical resources. Geographical factors appear to account for only a small portion of the previously observed variation. Well-designed clinical trials are needed to rationalize surveillance.

35
14. OUTCOMES FOR PATIENTS WHO ARE DIAGNOSED WITH BOTH BREAST AND ENDOMETRIAL CANCER
Tonya Martin-Dunlap, MD, Mitchell S. Wachtel, MD, and Julie A. Margenthaler, MD Washington University Introduction: Of all new cancers diagnosed in women each year, approximately 30% are attributed to breast cancer and 6% to endometrial cancer. As the population ages and treatment modalities become more effective, it will become more common to diagnose both cancers during a single patient’s lifetime. The overall survival outcomes for patients who are diagnosed with both cancers have not been previously reported. Methods: Using the 1988-2007 Surveillance, Epidemiology, and End Results data, we conducted a retrospective, population-based cohort study of women diagnosed with both breast and endometrial cancer. Kaplan-Meier survival curves were created for disease-specific survival. Wald chi square tests evaluated differences between survival estimates. Results: We identified 2,027 women who were diagnosed with both breast and endometrial cancer. Of these, 1,296 (63.9%) were diagnosed with breast cancer first and 731 (36.1%) were diagnosed with endometrial cancer first. The median age at the second cancer diagnosis was 68 years (range 60-76), and the median time between the first cancer diagnosis and the second cancer diagnosis was 45 months (range 17-81). Regional lymph node involvement was significantly more common with a breast cancer diagnosis [522 (25.8%) women] compared to an endometrial cancer diagnosis [87(4.3%) women] (p<0.05). Factors associated with decreased survival included high tumor grade, nodal positivity, and estrogen receptor-negative breast cancer (p<0.05 for each). At the end of the study, 1,703 (84%) patients were still living. There were 83 (4.1%) deaths due to breast cancer, 63 (3.1%) deaths due to endometrial cancer, and 178 (8.8%) deaths due to other causes (p<0.05). Discussion: For women diagnosed with both breast and endometrial cancer, the cumulative risk of death at 5 years following the second cancer diagnosis is nearly four times more likely to be due to breast cancer than endometrial cancer. Breast cancer-specific mortality increases with time, while endometrial cancer-specific mortality decreases with time. Consideration should be given to these findings when discussing prognosis and making treatment decisions.

36
15. PATIENT AND PROCESS FACTORS ASSOCIATED WITH LATE-STAGE BREAST CANCER DIAGNOSIS IN SAFETY-NET PATIENTS: A PROSPECTIVE STUDY
Oluwadamilola M. Fayanju MD, MPHS, Donna B. Jeffe PhD, Leisha Elmore BS, Deborah N. Ksiazek BS, Julie A. Margenthaler MD Washington University BACKGROUND Following reforms to our city’s Safety-Net (SN) breast cancer referral process, we investigated whether factors often associated with late-stage diagnosis would differ by referral source – SN versus non-Safety-Net (NSN) – or, among SN patients, by stage at diagnosis. METHODS From September 2008 to June 2010, SN patients with any-stage (0-IV) and NSN patients with late-stage (IIB-IV) breast cancer were identified prospectively during initial cancer-center consultations. Data were analyzed using logistic regression, chi-square, and t-tests; two-tailed p<0.05 was considered significant. RESULTS 57 women completed interviews (SN-referred: 33/47 invited [70%], mean age 53 [30-68]; NSN-referred: 24/35 invited [69%], mean age 53 [33-76]) completed interviews. 52% of SN-referred patients were diagnosed with late-stage disease. Compared with NSN late-stage patients, SN late-stage patients were more likely to be African-American (83% vs. 21%, p<0.001), to have an annual household income <$25,000 (89% vs. 38%, p<0.001), and to report having a health problem in the preceding year but not being able to see a doctor because of cost (67% vs. 25%, p=0.012); they were less likely to be married/partnered (22% vs. 79%, p<0.001) and to have post-college education (0% vs. 25%, p<0.03), any insurance (61% vs. 96%, p<0.005), and to have sought medical attention within 1 week of realizing they had concerning breast findings (50% vs. 79%, p=0.047). Married/partnered patients were more likely to delay medical care by > 1 week (odds ratio = 9.90, p=0.038). CONCLUSIONS SN patients presented with higher-than-expected rates of late-stage disease despite improvements in mammography rates and the referral process. Efforts to further facilitate access to care for this vulnerable SN patient population are needed.
37
16. WHICH IMAGING MODALITY IS SUPERIOR FOR PREDICTION OF RESPONSE TO NEOADJUVANT CHEMOTHERAPY IN PATIENTS WITH TRIPLE NEGATIVE BREAST CANCER?
Jordan Atkins BS, Amy Cyr MD, Catherine M. Appleton MD, Carla S. Fisher MD, and Julie A. Margenthaler, MD Washington University Introduction: Triple negative breast cancer is a unique subtype of breast cancer that has been shown to be generally chemosensitive. We sought to investigate the accuracy of mammography (MMG), ultrasonography (US), and breast magnetic resonance imaging (MRI) in predicting the extent of breast residual disease in patients with triple negative breast cancer following neoadjuvant chemotherapy. Methods: We performed a retrospective chart review and identified 153 patients with Stage II-III triple negative breast cancer who were treated with neoadjuvant chemotherapy between 2000-2010. Residual tumor size was estimated by MMG, US, and/or MRI following neoadjuvant chemotherapy but prior to definitive surgical intervention. The longest diameter of residual tumor measured with imaging was compared with the infiltrating residual tumor size at pathologic evaluation. Data were compared using Chi-square and p<0.05 was considered significant. Results: Of 153 patients, 37 (24%) did not have imaging performed prior to surgical treatment, including 13 (35%) who underwent breast-conserving therapy and 24 (65%) who underwent mastectomy. The remaining 116 (76%) patients did have one or more imaging studies performed following neoadjuvant chemotherapy but prior to surgical treatment. Thirty-one (20%) patients had a pathologic complete response (pCR); a pCR was suspected by imaging in 10 (33%), residual disease was suspected by imaging in 19 (61%), and imaging was not performed in 2 (6%). Of 122 (80%) patients with residual invasive disease on final pathology, 21 (17%) had MMG only, 8 (7%) had MRI only, 49 (40%) had MMG and US, 9 (7%) had MMG, US, and MRI, and 35 (29%) had no imaging. The imaging modality was accurate to within 1 cm of the final pathologic residual disease in 43 (35%) patients and within 2 cm in 70 (57%) patients. Accuracy was highest for US (57%) and MRI (53%), which were significantly more accurate than MMG (24%) (p<0.05). The patients in each imaging modality schema did not differ with regards to patient age, patient race, tumor histology, tumor size, tumor grade, clinical stage, or clinical nodal status (p>0.05). Conclusions: Breast US and MRI were more accurate than mammography in predicting residual tumor size following neoadjuvant chemotherapy in patients with triple negative breast cancer. None of the imaging modalities were superior in predicting patients with a pCR. The relatively low accuracy of all three standard imaging modalities illustrates the need for alternative systems with improved sensitivity.

38
17. PATIENT FACTORS PREDICTIVE OF UNILATERAL MASTECTOMY AND CONTRALATERAL PROPHYLACTIC MASTECTOMY
Tonya Martin-Dunlap MD, Carla S. Fisher MD, Jared Atkins BS, Feng Gao PhD, and Julie A. Margenthaler MD Washington University Objectives: Recent data suggest an increased rate of mastectomy with or without contralateral prophylactic mastectomy despite potential eligibility for breast conservation. The reasons women choose to undergo mastectomy and/or contralateral prophylactic mastectomy are likely multifactorial and are not clearly understood. We sought to determine the patient and clinical characteristics impacting this decision-making process. Methods: A questionnaire was administered to patients who had undergone previous unilateral mastectomy (UM) or bilateral mastectomy (BM) for breast cancer during the years 2006 to 2010. The survey queried on demographics, surgical choices, and rationale for those choices. A retrospective chart review was performed to determine tumor characteristics and treatment information. The data were analyzed using Fisher’s Exact and Chi Square tests. A p-value <0.05 was considered significant. Results: Of 310 patients queried, 175 underwent UM and 135 underwent BM (mean age 56 + 12 years). Of the 135 women undergoing BM, 16 (12%) had documented bilateral breast cancer, while 119 (88%) had unilateral breast cancer. Women who were <50 years and Caucasian were more likely to choose BM over UM (p=0.0001 for both). The choice for UM versus BM was not affected by tumor size, stage, grade, lymph node status, or ER/PR/Her2neu status (p>0.05 for each). Of 106 patients who underwent genetic testing, 34 (32%) had a BRCA or p53 mutation, while 72 (68%) had no known genetic abnormality. Patients with a known genetic mutation were more likely to undergo BM compared to those without a known mutation (p=0.003). Women who underwent BM were more likely to report that they “felt mastectomy would improve my survival” or “felt I would live long enough to be at risk for another cancer” on the questionnaire than those who underwent UM [36 (57%) vs. 25 (37%), p=0.035 and 20 (32%) vs. 5 (7%), p=0.001, respectively]. Patient responses of “a friend/family member encouraged mastectomy” or “want to improve cosmesis/appearance and facilitate reconstruction” were not reported more significantly by either the UM or BM group. Conclusions: Although tumor characteristics did not impact the decision for UM versus BM in our study population, patient factors were significant. Younger women, Caucasian women, and women with a known hereditary cancer syndrome were significantly more likely to undergo BM compared to UM when undergoing mastectomy for breast cancer. The most common reasons cited for choosing BM over UM were a perceived improved survival and reducing risk for recurrence and/or second primaries. Future studies will focus on the role of patient education in altering this decision-making process.
39
18. RECONSTRUCTION PATTERNS IN A SINGLE INSTITUTION COHORT OF WOMEN UNDERGOING MASTECTOMY FOR BREAST CANCER
Leisha Elmore BS, Carla S. Fisher MD, Jared Atkins BS, Feng Gao PhD, and Julie A. Margenthaler MD Washington University Objectives: Recent data suggest increasing numbers of women choosing mastectomy and contralateral prophylactic mastectomy for treatment of breast cancer. The impact of various reconstructive practices is unclear. The aim of the current study was to conduct a patient-centered investigation of reconstruction practices following mastectomy at our institution. Methods: A questionnaire was administered to patients who had undergone previous unilateral mastectomy or bilateral mastectomy for breast cancer during the years 2006 to 2010. The survey queried on demographics, surgical choices, and rationale for those choices. Patients were specifically asked about their decision to undergo breast reconstructive, the method by which they were introduced to reconstructive choices, the type of definitive reconstruction performed, and the timing of reconstruction. Descriptive statistics were utilized for data summary and were compared using Chi Square tests. A p-value <0.05 was considered significant. Results: Of 310 patients queried, 175 (56%) underwent unilateral mastectomy and 135 (44%) underwent bilateral mastectomy (mean age 56 + 12 years), including 68 (22%) with Stage IIB-III disease. Overall, 192 (62%) of women underwent breast reconstruction, which is significantly higher than reported national rates of 10-25% (p<0.05), while 118 (38%) did not. Of those undergoing reconstruction, 182 (96%) reported that their surgical oncologist was the first person to discuss reconstructive options; 10 (4%) reported self-directed referral for reconstruction. Immediate breast reconstruction was performed in 125 of 192 (69%) women, while 67 of 192 (31%) underwent delayed reconstruction. The method of definitive reconstruction included 137 of 192 (71%) prostheses (tissue expander and/or implant), 36 of 192 (19%) abdominal tissue flap, 14 of 192 (7%) latissimus flap (+/- implant), and 5 of 192 (3%) with a combination of prostheses and tissue flaps. Of the 118 patients who did not undergo reconstruction, 68 (58%) reported lack of desire for reconstruction as their motive, while the remaining 50 (42%) reported either medical contraindications for reconstruction or did not report a specific reason. Conclusions: The majority of women undergoing unilateral or bilateral mastectomy for breast cancer at our institution elect to undergo reconstruction. Prosthetic reconstruction was the most common method utilized in our cohort. The impetus for referral to the reconstructive surgeon was nearly always initiated by the surgical oncologist. Further research is needed to evaluate the impact of patient preference, provider bias, and barriers to care on the utilization of breast reconstruction nationwide.
40
19. PATIENT SURVEILLANCE AFTER BREAST CANCER TREATMENT: IMPACT OF MCOS
Robert J. Avino, BA, Emad S. Allam, MD, Ling Chen, PhD, Katherine S. Virgo, PhD, MBA, Julie A. Margenthaler, MD, Frank E. Johnson, MD Saint Louis University, Washington University, American Cancer Society Introduction: There are about 2.5 million breast cancer survivors in the US. Virtually all are candidates for post-treatment surveillance. We have previously documented remarkable variation in surveillance intensity. The only surveillance modalities endorsed by ASCO for asymptomatic patients are office visit and mammogram. It is believed that managed care organizations (MCOs) often restrict test utilization. We estimated how MCO penetration rate affects the known variation in surveillance strategies. Methods: The 3245 ASCO members who had indicated that breast carcinoma was a major clinical focus were surveyed to determine their surveillance practices. Members were asked to consider 4 idealized clinical vignettes and indicate their surveillance plan for each. A menu of 12 testing modalities was offered. Practice patterns were stratified in quartiles by MCO penetration rates (0-14%, 14-22%, 22-33%, 33-61%) in each physician’s practice location. Repeated-measures ANOVA was used for analysis. Results: Of the ASCO members surveyed, 915 responses were evaluable. LFTs, CBC, office visit, and diagnostic mammogram were the modalities most frequently recommended. There was significant variation among MCO cohorts in the recommended frequency of utilization of diagnostic mammogram (p<0.05), but in no other modalities. In year 1, diagnostic mammogram was recommended 1.9 ± 1.8 (mean ±SD) times for the 0-14% penetration rate cohort and 1.7 ± 1.4 times for the 22-33% cohort. Conclusions: We found little evidence that MCOs limit test utilization. The MCO penetration rate in the clinician’s practice location cannot account for the overall variation in surveillance strategies we previously documented.

41
20. EVALUATION OF INFECTED ABDOMINAL MESH IN A MURINE MODEL OF PERITONITIS
Stephen Eaton, MD (Fellow); Carey-Ann Burnham, Phd; Chris Bowley, Chris Davis, Stephen Jarman, BSN, RN; Robert Southard, MD; Richard Hotchkiss, MD, Grant V Bochicchio, MD; John P. Kirby, MD (Sponsor) Washington University BACKGROUND: Although trauma patients often have contaminated abdominal wall tissue defects closed with mesh, little is known about the tolerance or engraftment of these meshes. We have developed a mouse model of peritonitis containing bilateral implants of various abdominal meshes in order to evaluate their short term response to bacterial contamination. METHODS: A cecal slurry method of inducing abdominal infection was utilized in three separate sets of experiments in which a polypropylene mesh was compared to three different positive control mesh types (n=3-4 per group). Each mouse received two meshes (½ X 1 cm.), one polypropylene and one selected positive control, sewn bilaterally into the abdominal wall just below a midline incision. Prior to closure of the incision, a measured volume of cecal slurry (5mg/kg) from a donor mouse was injected into the abdominal cavity. Mice were followed for one week post-implantation and received antibiotic (Imipenem) on days five and six. On day seven the mesh material was explanted, cultured, and assessed for bacterial counts. RESULTS:
CONCLUSIONS: Mesh characteristics determine statistically significant bacterial colonization counts in this murine model. Although much has been done to study the biomechanics of mesh closures, less is known about their immunological tolerance and subsequent engraftment. This murine model provides a necessary immunological component to previously studied models so that optimal mesh techniques can be designed.
0
1
2
3
4
5
6
7
Log To
tal
All Mesh Types
Polyprop. Mesh A Mesh B
42
21. SEVERE MULTISYSTEM INJURY ALTERS IMMUNE CELL EXPRESSION OF TLR-4 IN A MOUSE MODEL OF TRAUMA
Isaiah R. Turnbull, MD, PhD; Sarbani Ghosh, MS; Julia Hilliard; Katherine Chang; Robert E Southard, MD Washington University Introduction: Pneumonia is twice as common after trauma as compared to elective surgery. Elderly patients are three times more likely to die of pneumonia after trauma than are younger patients. Toll-like receptor-4 (TLR-4), a receptor for LPS, contributes to the immune response of injured patients. We recently developed a murine model of severe injury that recapitulates the increased mortality from pneumonia after geriatric trauma. We hypothesized that the differential response to pneumonia after injury may reflect changes in TLR-4 expression on monocyte/macrophages and neutrophils. Methods: Aged mice (male retired breeders, >6 months) were subjected to partial liver laceration, bilateral hind limb crush injury with intramuscular injection of bone fragments, and withdrawal of 15% of total blood volume. Mice were sacrificed 24 hours after injury; blood and lungs were harvested. The fraction of ciculating moncytes, granulocytes and lung parenchymal cells expressing TLR-4 was assessed by flow cytometry. Serum BUN, Creatinine, AST, and ALT were measured. Uninjured animals served as controls. Results: As compared to uninjured mice, injury increased expression of TLR-4 on circulating monocytes (84% vs. 66%; p=0.02) and lung macrophages (74% vs. 57%; p=0.01) but decreased expression on circulating granulocytes (32% vs. 53%; p<0.01.) There was no difference in TLR-4 expression by parenchymal granulocytes. Injury also significantly increased serum levels of AST (1800 U/L v 63 U/L, p<0.01) and ALT (1000 U/L v 50 U/L, p<0.01.) There was no difference in BUN or creatinine. Conclusion: Multisystem trauma increases TLR-4 expression on circulating monocytes and lung resident macrophages but decreases expression on circulating neutrophils. Increased TLR-4 expression by monocyte/macrophage cells may exacerbate the inflammatory response to bacterial infection, contributing to increased mortality from pneumonia after multisystem injury in aged mice.
43
22. IS THE MICRIOBIOLOGY THE ANSWER TO A SUCCESSFUL LOWER EXTREMITY TRAUMATIC FREE FLAP
Johnny Franco MD, Michael Thorpe MD, Mathew Nykiel MD, Bruce Kraemer MD FACS, J Tracy Watson MD Saint Louis University
Purpose: Lower extremity reconstruction is a comp problem that many plastic surgeons face. The classic teaching involves early stabilization and flap coverage of Gustilo 3B fractures, this is based largely on the work done by Godina and Francel. Godina recommended free tissue coverage within the first 72 hours and Francel within 15 days. At our institution patients undergo definitive fixation by the orthopedic service almost immediately at the time of their initial presentation / irrigation and debridement. Definitive wound closure / coverage is delayed until a healthy biologically stable wound is achieved. This is determined by the achievement of negative post debridement intra-operative cultures during serial debridements. Thus we examined this patient population in terms of free tissue outcomes when flap coverage was based on cultures rather than a defined time. Method: A single institution retrospective review was performed from July 2006 to December 2010 evaluating all Gustilo 3B lower extremity fractures that required free tissue transfer. All patients over the age of 17 that were treated acutely for their fracture using an Orthopaedic protocol based on culture results prior to closure/coverage were included in the study. Chart review was then performed with data collected in an excel sheet. Results: Nine patients were found to meet the above criteria and were included in the study. The mean age of the patients in this study was 37 years old. The mean time to free tissue transfer was 15 days. 100 percent free flap survival, one major complication - a donor site hematoma, and one minor complication - a partial skin graft loss over a free muscle flap. The average number of debridements prior to free tissue transfer was 5.3. Discussion: Lower extremity trauma can be a difficult problem for the reconstructive surgeon due to the devastating morbidity caused by free flap failure. Godina in 1986 set the standard of free tissue reconstruction for lower extremity trauma when he found a 0.75% flap failure rate when completed within 72 hours. The flap failure rate however increased to 12% in patients treated between 72 hours and 3 months. However, in our series all patients were taken for debridement at the time of presentation followed by post debridement cultures. The patients’ were then returned to the operating room every 48 hours thereafter until the patient demonstrated negative post debridement cultures. At this juncture closure /coverage was performed. Patients with positive cultures were treated with culture specific antibiotics in concert with negative pressure therapy and the protocol continued until negative cultures were achieved. The advent of culture based wound management along with negative pressure therapy has allowed us to have positive outcomes in this small series.

44
23. DUTY HOUR HEAVY CLERKSHIPS DO NOT ADVERSELY AFFECT SURGERY CLERKSHIP TEST SCORES
Stephanie Bonne, MD (Fellow); Douglas Brown, PhD; Douglas J. E. Schuerer, MD; Grant V. Bochicchio, MD, MPH; John P. Kirby, MS, MD (Sponsor) Washington University BACKGROUND: Some claim excessive clinical duties diminish student learning as well as other undesirable effects. We studied students who chose surgical rotations with higher clinical duty hours, such as trauma, and their subsequent NBME Surgery Subject Test Scores at WUSM. METHODS: Retrospective student record review and the students’ self reported duty hours for their rotations during the third year surgical clerkship. The rotations taken before the exam were classified by their duty hours into three groups: light (<50 hrs/week), moderate (50 – 60 hrs/week), and heavy (60 – 80 hrs/week). We then looked at the distribution of test scores and those rotations. RESULTS: 50% of students selected light duty hour rotations, 33% of students selected heavy duty hour rotations and 17% selected moderate duty hour rotations. 35% of students who took heavy clinical duty achieved an honors grade on the exam. 18% of students who took light clinical duty received an honors test score. Pearson Correlation testing showed no association. CONCLUSIONS: Choosing to take heavy clinical duty hour rotations before the NBME Surgery Subject Exam was NOT correlated with lower examination scores. Further analyses may be able to better dissect out co-variables for designing an optimal mix of clinical work, didactics and other educational opportunities for medical students.
45
24. OUR EXPERIENCE WITH OPEN REDUCTION – INTERNAL FIXATION OF RIB FRACTURES
Alison Witte, MD; Pascal Nyachowe, MD; Ann Peick, MD; Anil Srivastava, MD; Bryan Troop, MD Mercy Hospital BACKGROUND: Open reduction – internal fixation of rib fractures after trauma is a controversial topic, to say the least. Opinions regarding the value of rib fixation have fluctuated for over a century now with the current trend appearing to favor the intervention over traditional supportive treatment. Small studies appear to show a significant decrease in pain/disability, pneumonia, ventilator dependence, and ICU/hospital days associated with early skeletal stabilization in patients with multiple serial rib fractures, and most notably, flail physiology. A handful of systems are currently marketed for this indication. We present our single institution experience with the Acute Innovations RibLoc System in six trauma patients between September 2011 and March 2012. METHODS: Six consecutive trauma patients with severe flail chest following blunt injuries at a single institution are outlined in this pilot study. All patients underwent 3D CT reconstruction as part of the pre-operative planning workup. A single system, Acute Innovations RibLoc, was utilized for all six patients. RESULTS: All six patients tolerated the procedure well. Patients had an average age of 46.5 years and included only 1 woman. Five out of the six patients were smokers with an average BMI of 29.1. All 6 patients presented as blunt injuries. They had an average of 8.3 rib fractures with two-thirds of the patients having notable flail physiology and two-thirds of the patients having associated pulmonary contusions. All four patients with flail chests had resolution of this physiology post-fixation. An average of 3.2 ribs were stabilized during each operation. On-Q submuscular local anesthetic pain pumps were inserted at the end of each case. Only two patients developed pneumonia during the hospitalization. The average days requiring mechanical ventilation was 10.3, and the average hospital stay was 18.2 days. All six patients were liberated from the ventilator during their hospitalization with only one requiring a tracheostomy. There were no deaths. CONCLUSION: The morbidity and mortality associated with severe blunt chest wall injury mandates that we investigate viable treatment options that could be potentially superior to supportive care. While current studies evaluating the benefit of operative reduction – internal fixation of rib fractures over supportive treatment are relatively sparse and low in power, they are growing considerably. We present our small and growing case series in an effort to examine what is shaping up to be not only a safe treatment option, but a more effective strategy to manage this painful and debilitating injury pattern.
46
25. ANTIBIOTIC PROPHYLAXIS IN PATIENTS WITH OPEN ABDOMEN AFTER EXPLORATORY LAPAROTOMY FOR TRAUMA
Jason D. Keune, MD, MBA, Kareem D. Husain, MD, John E. Mazuski, MD, PhD Washington University Background. Patients who undergo exploratory laparotomy for trauma are at high risk for intra-abdominal and surgical site infection (SSI). In an earlier study, we showed that the infection rate in patients who met ideal antibiotic prophylaxis criteria was significantly less than those who did not. As part of the study on infectious complications following laparotomy for trauma, we identified patients treated with an open abdominal technique as being as very high risk for these complications. Methods. All patients undergoing exploratory laparotomy whose fascia is not closed at the initial operation at a level 1 trauma center from November 2009 - June 2011 were analyzed. Prophylactic antibiotic administration was graded as ideal if antibiotics were given within one hour of incision, redosed when two antibiotic half-lives had passed, redosed intraoperatively if greater than one blood volume had been lost, and if the antibiotic covered anaerobes when a bowel injury was present. Patients were characterized as having no infection, a minor SSI only, an infection related to laparotomy, or an unrelated infection such as pneumonia. Results. A total of 19 patients underwent exploratory laparotomy for trauma and were managed with an open abdomen during the time period. One patient died of a non-infectious cause immediately after leaving the operating room, so was excluded from this analysis. Of these patients, 77.8% suffered a postoperative infection, while 22.2% did not; 55.6% had infections directly related to laparotomy (50% major related infection, 5.6% minor SSI), and 22.2% had unrelated infections. Only 4 patients (22%) met criteria for ideal prophylactic antibiotic administration. Of these, two patients had a significant intraabdominal infection and one had a minor SSI. Conclusions. Though ideal administration of prophylactic antibiotics is associated with decreased infectious complications following exploratory laparotomy for trauma, such protocols may not be appropriate for patients who are managed with an open abdomen. Further work is needed to develop protocols of this group of patients.

47
26. EMERGENCY DEPARTMENT THORACOTOMY: CASE PRESENTATION AND REVIEW OF INDICATIONS.
Gill G MD, Shatto J MD, Blondeau B MD, Geehan D University of Missouri-Kansas City Since its introduction in 1900, the emergency department thoracotomy (EDT) has been a subject of intense debate. Injury mechanism and location, signs of life (SOLs), initial cardiac rhythm, and presence of vital signs are usually used to predict outcome after Emergency thoracotomy. Reported survival for penetrating thoracic injuries ranges between 1.8 - 33 % . We are presenting a case that suggests EDT was used with success in a patient who lost vital signs in route. A 25 y/aam was brought in as type B trauma with a stab wound to anterior chest. The wound was 2 cm inferior to left nipple areolar complex. The patient had vital signs at the scene but no other signs of life; BP of 110/90 and HR 135. He lost his VS during transport. EMT dispatched to hospital arriving at the ER 13 minutes later. Pt arrived with absent pulses and no blood pressure. Chest compressions were initiated by ER team. Initial FAST was negative, but repeat FAST did show fluid in pericardium. Time of injury to ED thoracotomy was 38 minutes. The time between loss of vital signs and ED thoracotomy was 24 min. The thoractomy revealed that the patient had cardiac tamponade. Upon opening the pericardium a 2 cm laceration to the right ventricle was identified and approximated in the trauma bay. Patient’s vital signs spontaneously returned and he was taken to the operating room to inspect the integrity of the repair with formal closure. Postoperative course was uneventful. Patient recovered well, neurologically intact, and was discharged home on POD 8.
We emphasize that ED thoracotomy is a rational option for anterior chest stab wounds with pericardial tamponade. We are presenting a patient with no signs of life and absence vital signs for at least 24 min with normal neurological outcome. The length of time between loss of vital signs and indicated ED thoractomy may be extended for certain patient presentations beyond the accepted guideline of 15 minutes.

48
27. LESS IS MORE: LOW-DOSE PROTHROMBIN COMPLEX CONCENTRATE EFFECTIVE IN ACUTE CARE SURGERY PATIENTS
Jacob A. Quick MD (resident), Jennifer M. Meyer RPh, Jeffrey P. Coughenour MD FACS, Stephen L. Barnes MD FACS (sponsor) University of Missouri-Columbia Background: Optimal dosing of prothrombin complex concentrate (PCC) has yet to be defined and varies widely from 3-100IU/kg. We hypothesized a dose of 15 IU/kg actual body weight of a three-factor PCC would effectively correct coagulopathy in acute care surgery patients. Methods: Retrospective review of 41 acute care surgery patients over 36 months who received 15 IU/kg (+/- 10%) actual body weight PCC for correction of coagulopathy. Demographics, laboratory results, PCC dose, blood product utilization, Vitamin K use and complications were analyzed. Results: Mean age was 69 years (18-94 years), with 29 (71%) taking prehospital warfarin. Thirty (73%) trauma patients, 9 (22%) emergency surgery patients, and 2 (5%) burns were included. Mean PCC dose was 1305.4 IU (14.2 IU/kg actual body weight). Mean initial PT and INR were 28.5 sec. and 2.52. Average PT and INR were 18.64 sec. and 1.42 after PCC. Success (INR <1.5) was seen in 78% of patients after a single dose of PCC. Treatment failures had a higher mean initial INR (4.3, p 0.02) and mean post treatment INR (1.84, p 0.002). Mean units of FFP transfused was 1.46. Mean 24-hour blood (PRBC) transfusion was 1.61 units. Twenty (49%) patients received no FFP in addition to PCC, while 25 (61%) patients received no PRBC transfusion. No statistical differences were seen with Vitamin K (n=12). One thrombotic event occurred. Conclusion: Administration of low-dose PCC, 15 IU/kg actual body weight, effectively corrects coagulopathy in acute care surgery patients with a low risk of thrombotic events.
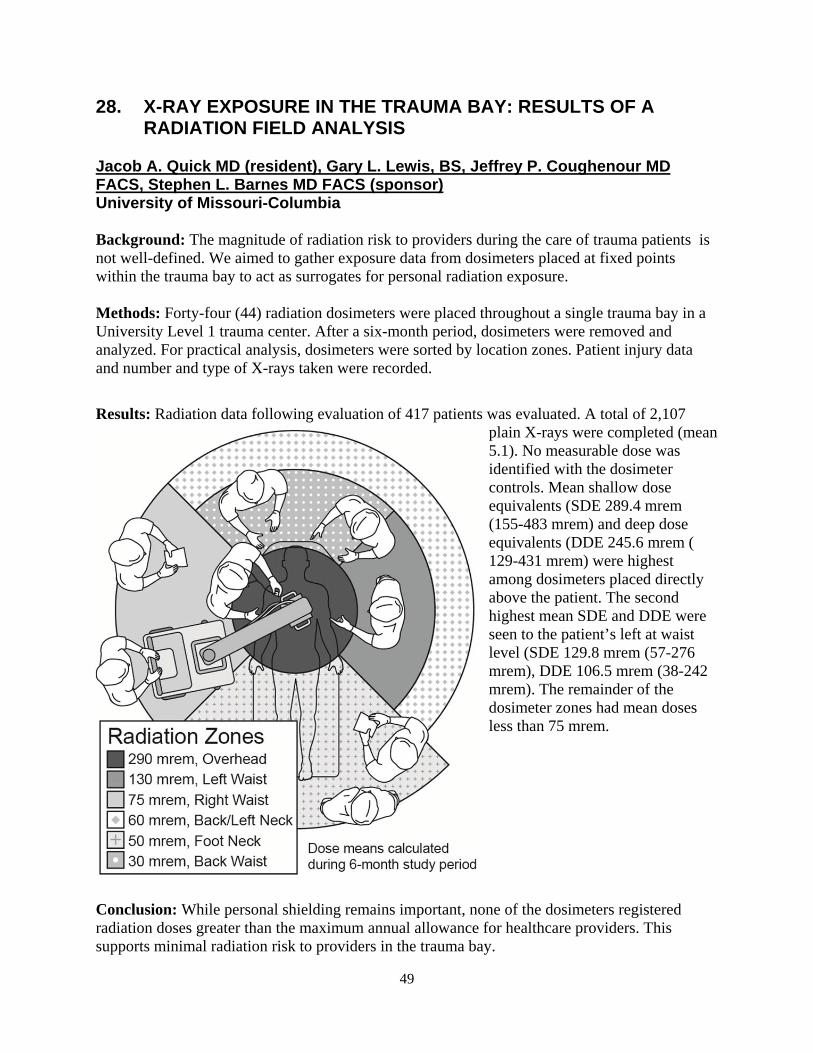
49
28. X-RAY EXPOSURE IN THE TRAUMA BAY: RESULTS OF A RADIATION FIELD ANALYSIS
Jacob A. Quick MD (resident), Gary L. Lewis, BS, Jeffrey P. Coughenour MD FACS, Stephen L. Barnes MD FACS (sponsor) University of Missouri-Columbia Background: The magnitude of radiation risk to providers during the care of trauma patients is not well-defined. We aimed to gather exposure data from dosimeters placed at fixed points within the trauma bay to act as surrogates for personal radiation exposure. Methods: Forty-four (44) radiation dosimeters were placed throughout a single trauma bay in a University Level 1 trauma center. After a six-month period, dosimeters were removed and analyzed. For practical analysis, dosimeters were sorted by location zones. Patient injury data and number and type of X-rays taken were recorded.
Results: Radiation data following evaluation of 417 patients was evaluated. A total of 2,107 plain X-rays were completed (mean 5.1). No measurable dose was identified with the dosimeter controls. Mean shallow dose equivalents (SDE 289.4 mrem (155-483 mrem) and deep dose equivalents (DDE 245.6 mrem ( 129-431 mrem) were highest among dosimeters placed directly above the patient. The second highest mean SDE and DDE were seen to the patient’s left at waist level (SDE 129.8 mrem (57-276 mrem), DDE 106.5 mrem (38-242 mrem). The remainder of the dosimeter zones had mean doses less than 75 mrem.
Conclusion: While personal shielding remains important, none of the dosimeters registered radiation doses greater than the maximum annual allowance for healthcare providers. This supports minimal radiation risk to providers in the trauma bay.

50
29. OPERATIVE MANAGEMENT OF RIB FRACTURES IN THE SETTING OF FLAIL CHEST: A SYSTEMATIC REVIEW AND META-ANALYSIS
Jennifer A. Leinicke, MD; Leisha Elmore, BS; Bradley D. Freeman, MD, FACS Washington University Objective: Blunt trauma resulting in flail chest is a common problem. Despite advancements in ventilatory management, flail chest is associated with significant morbidity and mortality. Operative fixation of the flail segment has been advocated as an adjunct to supportive care in this setting, but there is no definitive clinical study defining the role of surgery. Numerous small studies have been conducted and report varied results. The objective of this study was to determine if there is a net-beneficial effect for operative management of flail chest as compared to non-operative therapy. Methods of Study Selection and Analysis: We searched electronic databases (MEDLINE, EMBASE, Scopus, Cochrane, and Trial Registries, 1966-present) to identify randomized controlled trials (RCTs), cohort, and case-control studies involving adult flail chest patients comparing operative (any method) to non-operative therapy. The primary outcome was duration of mechanical ventilation (DMV). Secondary outcomes included intensive care unit length of stay (ICULOS), hospital length of stay (HLOS), mortality, incidence of pneumonia (PNA), and rate of tracheostomy (TRACH). Pooled effect size (ES) or odds ratios (OR) were calculated using a fixed or random effects model, as appropriate. Heterogeneity was assessed using χ2 and I2 tests. We assessed publication bias using funnel plots and Egger test. Results: Our search returned 1,407 unique publications. Nine studies with a total of 538 patients met inclusion criteria: 2 RCTs, 4 cohort studies, and 3 case-control studies. All 9 studies reported DMV, although 1 study was excluded from analysis of this outcome due to inability to calculate an ES with standard error based on data reported. Studies that failed to report data for a given secondary outcome were excluded from individual analyses. A total of 5 studies reporting ICULOS, HLOS, mortality, and PNA, and 4 studies reporting TRACH were included in secondary analyses. Compared to control treatment, operative management of flail chest was associated with a shorter DMV (pooled ES -4.08 days, 95% confidence interval [CI] -4.37,-3.79), decreased ICU LOS (-3.40 days; 95%CI -6.01,-0.79), decreased HLOS (-3.82 days; 95%CI -7.12,-0.54), decreased mortality (pooled OR .44; 95%CI 0.28, 0.69), decreased PNA (0.45; 95%CI 0.30, 0.69), and decreased TRACH (0.25; 95%CI 0.13, 0.47). Conclusion: As compared to non-operative therapy, there appears to be a net-beneficial effect of operative management of flail chest with respect to mortality, morbidity, and resource expenditure. These findings support the need for an adequately powered clinical study to define the role of this intervention.
51
31. TRAUMA REHAB OUTCOME SCORE (TROS), A QUICK AND SIMPLE TOOL TO DETERMINE TRAUMA PATIENTS’ FUNCTIONAL ABILITIES.
William J. Symons, MD, Douglas J.E. Schuerer, MD, Sharon Allen, OTD/S, Cresencia Burhans, OTD/S, M Carolyn Baum, PhD, OTR/L, FAOTA Washington University Introduction: The degree to which trauma patients can reintegrate into society and live a productive life after an injury is a key indicator of success, but how to measure this is still uncertain. The functional independence measure (FIM) is currently used to evaluate the motor and cognitive function in a rehabilitation setting. The FIM has many draw backs: it requires training, takes significant time to administer, and does not predict functional needs or outcomes. To address the limitations of the FIM we developed the Trauma Rehab Outcome Score (TROS). The TROS, which is specifically developed for the trauma patient, is a quick and simple tool that can be applied by anyone to rapidly assess trauma patient's function in approximately 5 minutes. This study determined the reliability and the validity of the TROS compared to the FIM and the Montreal Cognitive Assessment (MoCA). Methods: The TROS, FIM, and MoCA were compared in a prospective manner at a level 1 trauma center on trauma patients after informed consent was obtained. Evaluations were done by 5 FIM trained OT students. Baseline demographic and mechanism of injury data were also collected. Results: Over a 5 month period 109 patients were enrolled, of whom the average age was 40 and 64% were male. The TROS took 5-10 minutes per patient, the FIM over 40 minutes. The Cronbach Alpha for the TROS was 0.801, showing good internal consistency. The TROS correlated well with the total FIM, the motor components of the FIM, and the MoCA. Conclusion: The TROS is highly internally reliable across all 7 components. The TROS correlates well with the FIM, but is significantly easier and timelier to perform. The TROS cognitive component needs to be improved compared to the MOCA, but still outperforms the cognitive component of the FIM. The TROS can now be used in further studies to predict patient’s resource needs and functional improvement.

52

53
Acknowledgments The Missouri Chapter of American College of Surgeons would like to take this opportunity to thank all of our technical exhibitors for their continued support of our professional meeting. We would also like to give special thanks to those exhibitors who were not only exhibitors but were sponsors and gave (unrestricted) educational grants to provide our fine speakers, activity, and food expenses for this year’s program. The Missouri Chapter of American College of Surgeons is committed to the free exchange of medical education. Inclusion of any presentation in this program, including presentations on off-label uses, does not imply an endorsement by the Missouri Chapter of American College of Surgeons of the uses, products, or techniques presented.