Misery Perfusion, Blood Pressure Control, and 5-Year ... · Yamauchi et al Misery Perfusion, Blood...
14
265 C hronic hemodynamic compromise, as indicated by increased oxygen extraction fraction (OEF; misery perfu- sion [MP]) 1 on positron emission tomography, is a risk factor for subsequent strokes in patients with atherosclerotic internal carotid artery (ICA) or middle cerebral artery occlusive dis- eases. 2,3 However, the benefit of bypass surgery or strict con- trol of blood pressure (BP) for reducing the stroke risk in MP patients is controversial. 4–6 Bypass surgery has been proven to improve MP. The Carotid Occlusion Surgery Study (COSS) in patients with recent symptomatic ICA occlusion and MP failed to show that surgery compared with medical therapy reduces the risk of ipsilateral ischemic stroke in 2 years. 4 However, it was criticized that although the Kaplan–Meier curves at 2 years were not different, a continuation of the curves could result in a crossover showing a benefit to surgery. Although patients with symptomatic ICA occlusion show a decrease in stroke rate over time, 7 it is unclear whether this is true for MP patients. BP lowering may increase the stroke risk in patients with impaired perfusion, as indicated by a decreased cerebral blood flow [CBF]/cerebral blood volume [CBV] ratio on positron emission tomography. 8 In our previous study, the relationship between BP and a 2-year stroke risk was different between patients with impaired perfusion (including MP) and those without impaired perfusion. 6 The stroke risk was high in patients with lower BP with impaired perfusion and in higher BP patients without impaired perfusion. However, a recent evaluation of nonsurgical controls from the COSS reported a contradictory finding, a lower stroke risk was associated with lower BP in patients with ICA occlusion and MP. 5 Our study purposes were (1) to determine whether MP is a predictor of a 5-year risk of subsequent stroke and (2) to investigate the relationships among BP during follow-up, MP, and the 5-year stroke risk. Methods We enrolled 130 nondisabled, medically treated patients with symp- tomatic occlusion of the extracranial ICA or occlusion or stenosis (>50% diameter reduction) of the intracranial ICA or middle cere- bral artery in our observational study, as previously reported. 6,9 This included 103 men and 27 women aged 44 to 90 years (mean±SD, 64±8 years; Table I in the online-only Data Supplement). The ethics Background and Purpose—The benefit of strict blood pressure (BP) control in high-risk patients with symptomatic major cerebral artery disease and misery perfusion (MP) is controversial. Our purposes were (1) to determine whether MP is a predictor of a 5-year risk of subsequent stroke and (2) to investigate the relationships among BP during follow-up, MP, and the stroke risk. Methods—We studied 130 nondisabled patients with symptomatic major cerebral artery disease. Baseline hemodynamic measurements were obtained from 15 O-gas positron emission tomography, and patients received medical treatment and they were followed for 5 years or until stroke recurrence or death. Results—During 5 years, strokes occurred in 6 of 16 patients with MP and in 15 of 114 without MP (log-rank test; P<0.01). There were 4 (25%) ipsilateral ischemic strokes in patients with MP and 4 in those without MP (P<0.001). The risk of ipsilateral ischemic stroke declined markedly after 2 years, and there was only 1 ipsilateral ischemic stroke in a patient without MP. Normal systolic BP (<130 mm Hg) was associated with an increased risk of ipsilateral ischemic strokes in patients with impaired perfusion (including MP), whereas systolic BP outside the 130 to 149 mm Hg range was associated with an increased risk of all strokes in patients without MP. Conclusion—Patients with MP showed a high-5-year stroke recurrence, but a large part of the 5-year stroke risk disappeared after 2 years. Aggressive BP control may be hazardous in patients with impaired perfusion, including MP. (Stroke. 2015;46:265-268. DOI: 10.1161/STROKEAHA.114.007134.) Key Words: blood pressure ◼ cerebrovascular disease ◼ positron emission tomography ◼ prognosis Misery Perfusion, Blood Pressure Control, and 5-Year Stroke Risk in Symptomatic Major Cerebral Artery Disease Hiroshi Yamauchi, MD, PhD; Shinya Kagawa, MS; Yoshihiko Kishibe, RT; Masaaki Takahashi, RT; Tatsuya Higashi, MD, PhD Received August 19, 2014; final revision received October 21, 2014; accepted October 22, 2014. From the Division of PET Imaging, Shiga Medical Centre Research Institute, Shiga, Japan. The online-only Data Supplement is available with this article at http://stroke.ahajournals.org/lookup/suppl/doi:10.1161/STROKEAHA.114. 007134/-/DC1. Correspondence to Hiroshi Yamauchi, MD, PhD, Division of PET Imaging, Shiga Medical Center Research Institute, 5-4-30 Moriyama, Moriyama, Shiga 524-8524, Japan. E-mail [email protected] © 2014 American Heart Association, Inc. Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.114.007134 by guest on August 3, 2017 http://stroke.ahajournals.org/ Downloaded from by guest on August 3, 2017 http://stroke.ahajournals.org/ Downloaded from by guest on August 3, 2017 http://stroke.ahajournals.org/ Downloaded from by guest on August 3, 2017 http://stroke.ahajournals.org/ Downloaded from by guest on August 3, 2017 http://stroke.ahajournals.org/ Downloaded from by guest on August 3, 2017 http://stroke.ahajournals.org/ Downloaded from by guest on August 3, 2017 http://stroke.ahajournals.org/ Downloaded from by guest on August 3, 2017 http://stroke.ahajournals.org/ Downloaded from by guest on August 3, 2017 http://stroke.ahajournals.org/ Downloaded from by guest on August 3, 2017 http://stroke.ahajournals.org/ Downloaded from by guest on August 3, 2017 http://stroke.ahajournals.org/ Downloaded from by guest on August 3, 2017 http://stroke.ahajournals.org/ Downloaded from
Transcript of Misery Perfusion, Blood Pressure Control, and 5-Year ... · Yamauchi et al Misery Perfusion, Blood...
265
Chronic hemodynamic compromise, as indicated by increased oxygen extraction fraction (OEF; misery perfu-
sion [MP])1 on positron emission tomography, is a risk factor for subsequent strokes in patients with atherosclerotic internal carotid artery (ICA) or middle cerebral artery occlusive dis-eases.2,3 However, the benefit of bypass surgery or strict con-trol of blood pressure (BP) for reducing the stroke risk in MP patients is controversial.4–6
Bypass surgery has been proven to improve MP. The Carotid Occlusion Surgery Study (COSS) in patients with recent symptomatic ICA occlusion and MP failed to show that surgery compared with medical therapy reduces the risk of ipsilateral ischemic stroke in 2 years.4 However, it was criticized that although the Kaplan–Meier curves at 2 years were not different, a continuation of the curves could result in a crossover showing a benefit to surgery. Although patients with symptomatic ICA occlusion show a decrease in stroke rate over time,7 it is unclear whether this is true for MP patients.
BP lowering may increase the stroke risk in patients with impaired perfusion, as indicated by a decreased cerebral blood
flow [CBF]/cerebral blood volume [CBV] ratio on positron emission tomography.8 In our previous study, the relationship between BP and a 2-year stroke risk was different between patients with impaired perfusion (including MP) and those without impaired perfusion.6 The stroke risk was high in patients with lower BP with impaired perfusion and in higher BP patients without impaired perfusion. However, a recent evaluation of nonsurgical controls from the COSS reported a contradictory finding, a lower stroke risk was associated with lower BP in patients with ICA occlusion and MP.5
Our study purposes were (1) to determine whether MP is a predictor of a 5-year risk of subsequent stroke and (2) to investigate the relationships among BP during follow-up, MP, and the 5-year stroke risk.
MethodsWe enrolled 130 nondisabled, medically treated patients with symp-tomatic occlusion of the extracranial ICA or occlusion or stenosis (>50% diameter reduction) of the intracranial ICA or middle cere-bral artery in our observational study, as previously reported.6,9 This included 103 men and 27 women aged 44 to 90 years (mean±SD, 64±8 years; Table I in the online-only Data Supplement). The ethics
Background and Purpose—The benefit of strict blood pressure (BP) control in high-risk patients with symptomatic major cerebral artery disease and misery perfusion (MP) is controversial. Our purposes were (1) to determine whether MP is a predictor of a 5-year risk of subsequent stroke and (2) to investigate the relationships among BP during follow-up, MP, and the stroke risk.
Methods—We studied 130 nondisabled patients with symptomatic major cerebral artery disease. Baseline hemodynamic measurements were obtained from 15O-gas positron emission tomography, and patients received medical treatment and they were followed for 5 years or until stroke recurrence or death.
Results—During 5 years, strokes occurred in 6 of 16 patients with MP and in 15 of 114 without MP (log-rank test; P<0.01). There were 4 (25%) ipsilateral ischemic strokes in patients with MP and 4 in those without MP (P<0.001). The risk of ipsilateral ischemic stroke declined markedly after 2 years, and there was only 1 ipsilateral ischemic stroke in a patient without MP. Normal systolic BP (<130 mm Hg) was associated with an increased risk of ipsilateral ischemic strokes in patients with impaired perfusion (including MP), whereas systolic BP outside the 130 to 149 mm Hg range was associated with an increased risk of all strokes in patients without MP.
Conclusion—Patients with MP showed a high-5-year stroke recurrence, but a large part of the 5-year stroke risk disappeared after 2 years. Aggressive BP control may be hazardous in patients with impaired perfusion, including MP. (Stroke. 2015;46:265-268. DOI: 10.1161/STROKEAHA.114.007134.)
Key Words: blood pressure ◼ cerebrovascular disease ◼ positron emission tomography ◼ prognosis
Misery Perfusion, Blood Pressure Control, and 5-Year Stroke Risk in Symptomatic Major Cerebral Artery Disease
Hiroshi Yamauchi, MD, PhD; Shinya Kagawa, MS; Yoshihiko Kishibe, RT; Masaaki Takahashi, RT; Tatsuya Higashi, MD, PhD
Received August 19, 2014; final revision received October 21, 2014; accepted October 22, 2014.From the Division of PET Imaging, Shiga Medical Centre Research Institute, Shiga, Japan.The online-only Data Supplement is available with this article at http://stroke.ahajournals.org/lookup/suppl/doi:10.1161/STROKEAHA.114.
007134/-/DC1.Correspondence to Hiroshi Yamauchi, MD, PhD, Division of PET Imaging, Shiga Medical Center Research Institute, 5-4-30 Moriyama, Moriyama,
Shiga 524-8524, Japan. E-mail [email protected]© 2014 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.114.007134
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from
by guest on A
ugust 3, 2017http://stroke.ahajournals.org/
Dow
nloaded from
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from
by guest on A
ugust 3, 2017http://stroke.ahajournals.org/
Dow
nloaded from
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from
by guest on A
ugust 3, 2017http://stroke.ahajournals.org/
Dow
nloaded from
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from
by guest on A
ugust 3, 2017http://stroke.ahajournals.org/
Dow
nloaded from
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from
by guest on A
ugust 3, 2017http://stroke.ahajournals.org/
Dow
nloaded from
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from
by guest on A
ugust 3, 2017http://stroke.ahajournals.org/
Dow
nloaded from
266 Stroke January 2015
committee of our center approved the study protocol, and all patients provided written informed consent.
Baseline hemodynamic measurements were obtained from positron emission tomography with15O-gases (C15O, C15O
2, and 15O
2).9 The CBF,
cerebral metabolic rate of oxygen, and OEF were calculated based on the steady-state method. Patients with an increased OEF (>52.9%), decreased CBF (<35.0 mL/100 g per minute), and decreased CBF/CBV ratio (<7.6 per minute) in hemispheres with arterial disease were categorized as having MP, whereas patients with a decreased CBF/CBV ratio were categorized as having impaired perfusion.8
After undergoing positron emission tomographic studies, patients were examined at 1- or 2-month intervals in the outpatient clinic of our center or of related hospitals. In patients with recurrent stroke, MRI or computed tomographic scans were obtained and compared with the initial studies to confirm recurrent stroke.
BP during the follow-up period was defined as the value of BP obtained just before stroke recurrence, death, or the end of the fol-low-up period. Continuous systolic blood pressure (SBP) measure-ments were categorized as follows: <130, 130 to 149, 150 to 169, and ≥170 mm Hg.
ResultsSixteen patients (12%) had MP and 114 did not have MP (Table I in the online-only Data Supplement). No patient char-acteristics significantly differed between the groups. Twenty-three patients had a decreased CBF/CBV ratio and normal OEF, 16 had a normal CBF/CBV ratio and increased OEF, and 75 had a normal CBF/CBV ratio and normal OEF. All patients, except 2, were treated with antiplatelet therapy.
All patients, except 4, were followed up for 5 years until stroke recurrence or death. None underwent vascular recon-struction surgery. One patient with MP and 3 patients without MP were lost to follow-up at 25 months and at 25, 40, and 43 months, respectively.
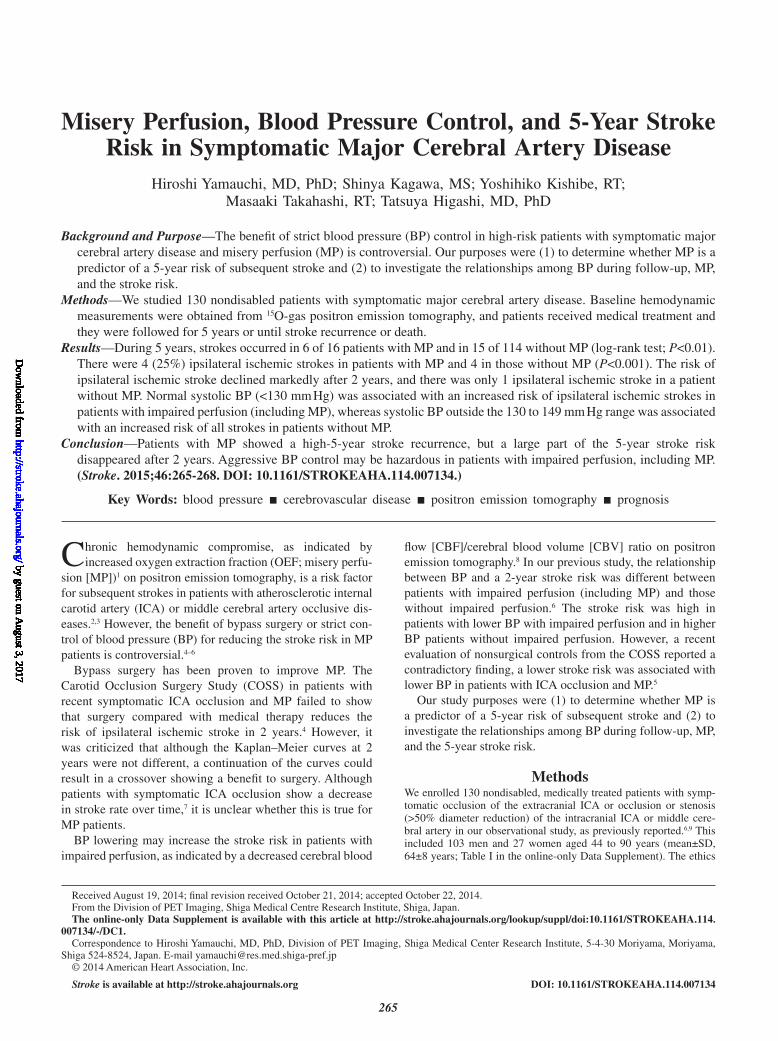
In patients with and without MP, the 5-year incidence of all strokes occurred in 6 (including 1 hemorrhage; 37.5%) and 15 (including 3 hemorrhages; 13.1%), respectively (hazard ratio [HR], 3.5; 95% confidence interval [CI], 1.4–8.9; P<0.01), and the incidence of ipsilateral ischemic stroke occurred in 4 (25%) patients and 4 (3.5%) patients, respectively (HR, 7.9; 95% CI, 1.9–31.9; P<0.005; Figure 1; Table II in the online-only Data Supplement). In patients with and without MP, the incidence of any ischemic strokes occurred in 5 (33.3%) and 12 (11.5%), respectively (HR, 3.4; 95% CI, 1.2–9.8; P<0.05). Beyond 2 years, there was only 1 ipsilateral ischemic stroke in patients without MP, whereas strokes elsewhere occurred in 2 patients with MP (1 hemorrhage) and in 5 patients without MP (1 hemorrhage). Death occurred in 3 patients with MP and in 7 patients without MP.
In patients with and without a decreased CBF/CBV ratio (impaired perfusion), the 5-year incidence of all strokes occurred in 9 of 39 (23.0%) patients and 12 of 91 (13.1%) patients, respectively (HR, 1.9; 95% CI, 0.8–4.6; P=0.13), and the incidence of ipsilateral ischemic stroke occurred in 6 (15.3%) and 2 (2.1%), respectively (HR, 7.7; 95% CI, 1.5–38.3; P<0.05). Death occurred in 4 patients with a decreased CBF/CBV ratio and in 6 patients without a decreased CBF/CBV ratio. In patients with an increased OEF but a normal CBF/CBV ratio, no stroke occurred.
Overall, there was a negative relationship between the SBP categories and the risk of ipsilateral ischemic stroke (Tables II and III in the online-only Data Supplement); the HR per
20 mm Hg was 0.26 (95% CI, 0.07–0.91; P<0.05). Alternatively, there was a positive relationship between the SBP categories and the risk of stroke in territories other than the diseased artery; the HR per 20 mm Hg was 4.5 (95% CI, 2.2–9.2; P<0.0001).
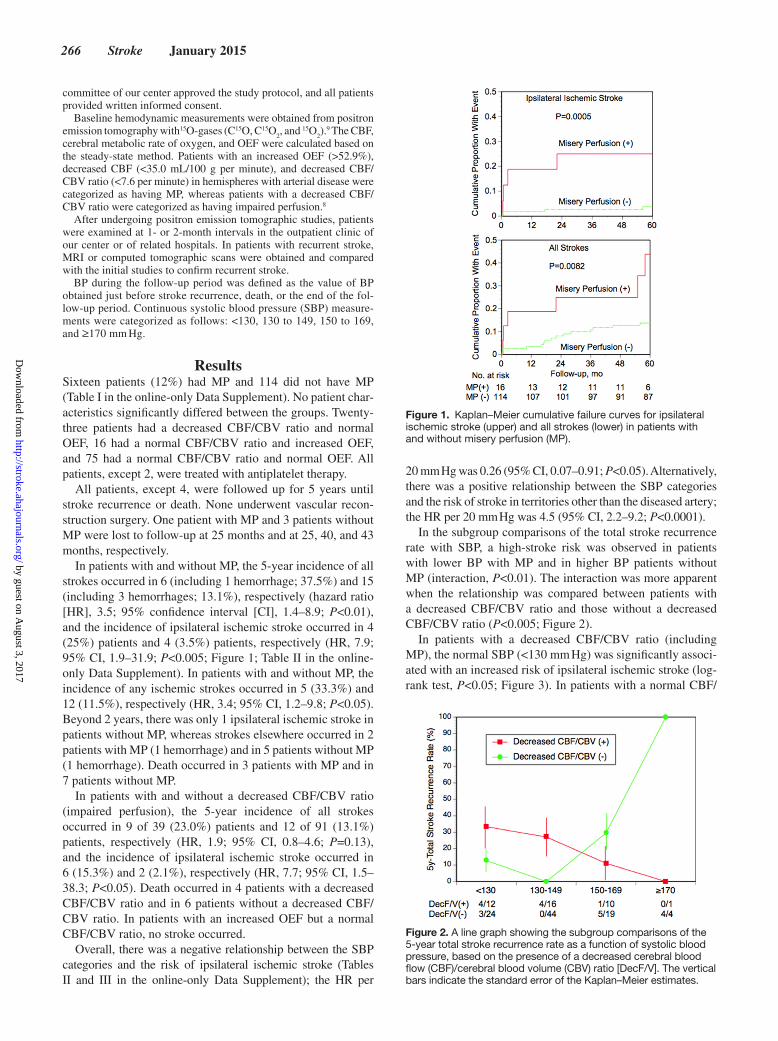
In the subgroup comparisons of the total stroke recurrence rate with SBP, a high-stroke risk was observed in patients with lower BP with MP and in higher BP patients without MP (interaction, P<0.01). The interaction was more apparent when the relationship was compared between patients with a decreased CBF/CBV ratio and those without a decreased CBF/CBV ratio (P<0.005; Figure 2).
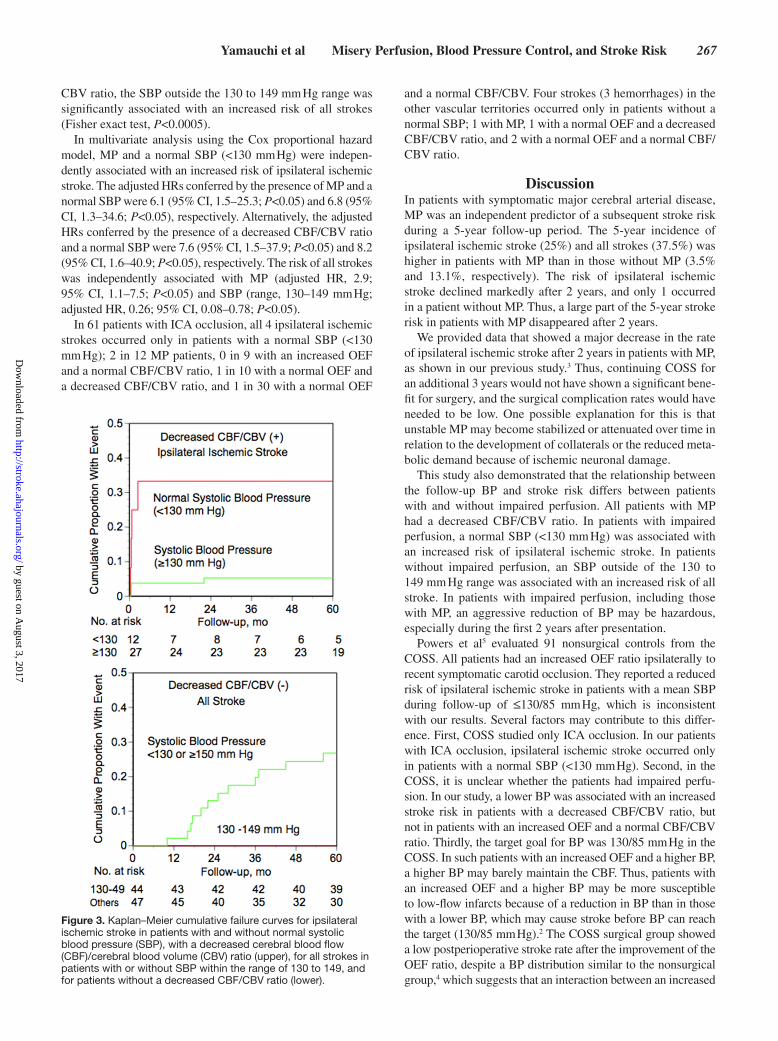
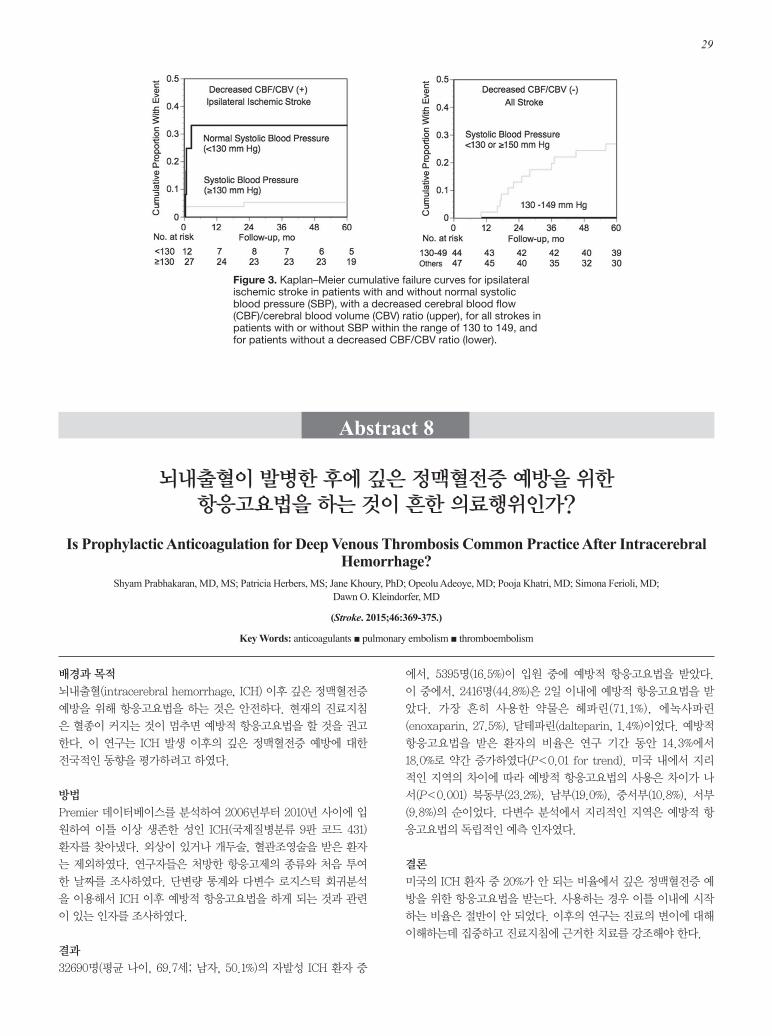
In patients with a decreased CBF/CBV ratio (including MP), the normal SBP (<130 mm Hg) was significantly associ-ated with an increased risk of ipsilateral ischemic stroke (log-rank test, P<0.05; Figure 3). In patients with a normal CBF/
Figure 1. Kaplan–Meier cumulative failure curves for ipsilateral ischemic stroke (upper) and all strokes (lower) in patients with and without misery perfusion (MP).
Figure 2. A line graph showing the subgroup comparisons of the 5-year total stroke recurrence rate as a function of systolic blood pressure, based on the presence of a decreased cerebral blood flow (CBF)/cerebral blood volume (CBV) ratio [DecF/V]. The vertical bars indicate the standard error of the Kaplan–Meier estimates.
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from
Yamauchi et al Misery Perfusion, Blood Pressure Control, and Stroke Risk 267
CBV ratio, the SBP outside the 130 to 149 mm Hg range was significantly associated with an increased risk of all strokes (Fisher exact test, P<0.0005).
In multivariate analysis using the Cox proportional hazard model, MP and a normal SBP (<130 mm Hg) were indepen-dently associated with an increased risk of ipsilateral ischemic stroke. The adjusted HRs conferred by the presence of MP and a normal SBP were 6.1 (95% CI, 1.5–25.3; P<0.05) and 6.8 (95% CI, 1.3–34.6; P<0.05), respectively. Alternatively, the adjusted HRs conferred by the presence of a decreased CBF/CBV ratio and a normal SBP were 7.6 (95% CI, 1.5–37.9; P<0.05) and 8.2 (95% CI, 1.6–40.9; P<0.05), respectively. The risk of all strokes was independently associated with MP (adjusted HR, 2.9; 95% CI, 1.1–7.5; P<0.05) and SBP (range, 130–149 mm Hg; adjusted HR, 0.26; 95% CI, 0.08–0.78; P<0.05).
In 61 patients with ICA occlusion, all 4 ipsilateral ischemic strokes occurred only in patients with a normal SBP (<130 mm Hg); 2 in 12 MP patients, 0 in 9 with an increased OEF and a normal CBF/CBV ratio, 1 in 10 with a normal OEF and a decreased CBF/CBV ratio, and 1 in 30 with a normal OEF
and a normal CBF/CBV. Four strokes (3 hemorrhages) in the other vascular territories occurred only in patients without a normal SBP; 1 with MP, 1 with a normal OEF and a decreased CBF/CBV ratio, and 2 with a normal OEF and a normal CBF/CBV ratio.
DiscussionIn patients with symptomatic major cerebral arterial disease, MP was an independent predictor of a subsequent stroke risk during a 5-year follow-up period. The 5-year incidence of ipsilateral ischemic stroke (25%) and all strokes (37.5%) was higher in patients with MP than in those without MP (3.5% and 13.1%, respectively). The risk of ipsilateral ischemic stroke declined markedly after 2 years, and only 1 occurred in a patient without MP. Thus, a large part of the 5-year stroke risk in patients with MP disappeared after 2 years.
We provided data that showed a major decrease in the rate of ipsilateral ischemic stroke after 2 years in patients with MP, as shown in our previous study.3 Thus, continuing COSS for an additional 3 years would not have shown a significant bene-fit for surgery, and the surgical complication rates would have needed to be low. One possible explanation for this is that unstable MP may become stabilized or attenuated over time in relation to the development of collaterals or the reduced meta-bolic demand because of ischemic neuronal damage.
This study also demonstrated that the relationship between the follow-up BP and stroke risk differs between patients with and without impaired perfusion. All patients with MP had a decreased CBF/CBV ratio. In patients with impaired perfusion, a normal SBP (<130 mm Hg) was associated with an increased risk of ipsilateral ischemic stroke. In patients without impaired perfusion, an SBP outside of the 130 to 149 mm Hg range was associated with an increased risk of all stroke. In patients with impaired perfusion, including those with MP, an aggressive reduction of BP may be hazardous, especially during the first 2 years after presentation.
Powers et al5 evaluated 91 nonsurgical controls from the COSS. All patients had an increased OEF ratio ipsilaterally to recent symptomatic carotid occlusion. They reported a reduced risk of ipsilateral ischemic stroke in patients with a mean SBP during follow-up of ≤130/85 mm Hg, which is inconsistent with our results. Several factors may contribute to this differ-ence. First, COSS studied only ICA occlusion. In our patients with ICA occlusion, ipsilateral ischemic stroke occurred only in patients with a normal SBP (<130 mm Hg). Second, in the COSS, it is unclear whether the patients had impaired perfu-sion. In our study, a lower BP was associated with an increased stroke risk in patients with a decreased CBF/CBV ratio, but not in patients with an increased OEF and a normal CBF/CBV ratio. Thirdly, the target goal for BP was 130/85 mm Hg in the COSS. In such patients with an increased OEF and a higher BP, a higher BP may barely maintain the CBF. Thus, patients with an increased OEF and a higher BP may be more susceptible to low-flow infarcts because of a reduction in BP than in those with a lower BP, which may cause stroke before BP can reach the target (130/85 mm Hg).2 The COSS surgical group showed a low postperioperative stroke rate after the improvement of the OEF ratio, despite a BP distribution similar to the nonsurgical group,4 which suggests that an interaction between an increased
Figure 3. Kaplan–Meier cumulative failure curves for ipsilateral ischemic stroke in patients with and without normal systolic blood pressure (SBP), with a decreased cerebral blood flow (CBF)/cerebral blood volume (CBV) ratio (upper), for all strokes in patients with or without SBP within the range of 130 to 149, and for patients without a decreased CBF/CBV ratio (lower).
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from

268 Stroke January 2015
OEF and an aggressive reduction in BP may cause a high-stroke rate in the nonsurgical group. In our cohort, the BP was mildly controlled depending on the level of BP in each patient. Finally, recurrent thromboembolic stroke may occur more frequently in carotid occlusion patients with a higher BP than in those with a lower BP. Derdeyn et al10 reported that most recurrent strokes were thromboembolic in patients with ICA occlusion and an increased OEF ratio. In our cohort, subcortical infarcts were a major type of recurrent ipsilateral strokes, in which the throm-boembolic mechanism was less likely.9
Both BP studies were post hoc analyses of observational stud-ies based on a small number of events in a small sample. A ran-domized, controlled trial is needed to determine the level at which the BP should be lowered to achieve maximal benefits in patients with or without hemodynamic compromise.11 We must establish strategies for selecting treatments based on hemodynamic mea-surements in atherosclerotic major cerebral artery disease.
Sources of FundingThis study was supported by a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science (No. 26461323).
DisclosuresNone.
References 1. Baron JC, Bousser MG, Rey A, Guillard A, Comar D, Castaigne P.
Reversal of focal “misery-perfusion syndrome” by extra-intracranial
arterial bypass in hemodynamic cerebral ischemia. A case study with 15O positron emission tomography. Stroke. 1981;12:454–459.
2. Klijn CJ, Kappelle LJ. Haemodynamic stroke: clinical features, progno-sis, and management. Lancet Neurol. 2010;9:1008–1017.
3. Yamauchi H, Fukuyama H, Nagahama Y, Nabatame H, Ueno M, Nishizawa S, et al. Significance of increased oxygen extraction frac-tion in five-year prognosis of major cerebral arterial occlusive diseases. J Nucl Med. 1999;40:1992–1998.
4. Powers WJ, Clarke WR, Grubb RL Jr, Videen TO, Adams HP Jr, Derdeyn CP; COSS Investigators. Extracranial-intracranial bypass surgery for stroke prevention in hemodynamic cerebral ischemia: the Carotid Occlusion Surgery Study randomized trial. JAMA. 2011;306:1983–1992.
5. Powers WJ, Clarke WR, Grubb RL Jr, Videen TO, Adams HP Jr, Derdeyn CP; COSS Investigators. Lower stroke risk with lower blood pressure in hemodynamic cerebral ischemia. Neurology. 2014;82:1027–1032.
6. Yamauchi H, Higashi T, Kagawa S, Kishibe Y, Takahashi M. Impaired perfusion modifies the relationship between blood pressure and stroke risk in major cerebral artery disease. J Neurol Neurosurg Psychiatry. 2013;84:1226–1232.
7. Persoon S, Luitse MJ, de Borst GJ, van der Zwan A, Algra A, Kappelle LJ, et al. Symptomatic internal carotid artery occlusion: a long-term follow-up study. J Neurol Neurosurg Psychiatry. 2011;82:521–526.
8. Schumann P, Touzani O, Young AR, Morello R, Baron JC, MacKenzie ET. Evaluation of the ratio of cerebral blood flow to cerebral blood vol-ume as an index of local cerebral perfusion pressure. Brain. 1998;121(Pt 7):1369–1379.
9. Yamauchi H, Higashi T, Kagawa S, Nishii R, Kudo T, Sugimoto K, et al. Is misery perfusion still a predictor of stroke in symptomatic major cere-bral artery disease? Brain. 2012;135(Pt 8):2515–2526.
10. Derdeyn CP, Carpenter DA, Videen TO, Grubb RL Jr, Powers WJ. Patterns of infarction in hemodynamic failure. Cerebrovasc Dis. 2007;24:11–19.
11. Persoon S, van Berckel BN, Bremmer JP, Boellaard R, Algra A, de Borst GJ, et al. Intervention versus standard medical treatment in patients with symptomatic occlusion of the internal carotid artery: a randomised oxy-gen-15 PET study. EJNMMI Res. 2013;3:79.
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from
HigashiHiroshi Yamauchi, Shinya Kagawa, Yoshihiko Kishibe, Masaaki Takahashi and Tatsuya
Cerebral Artery DiseaseMisery Perfusion, Blood Pressure Control, and 5-Year Stroke Risk in Symptomatic Major
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2014 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/STROKEAHA.114.007134
2015;46:265-268; originally published online November 13, 2014;Stroke.
http://stroke.ahajournals.org/content/46/1/265World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org/content/suppl/2016/04/07/STROKEAHA.114.007134.DC2 http://stroke.ahajournals.org/content/suppl/2014/11/13/STROKEAHA.114.007134.DC1
Data Supplement (unedited) at:
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from
1
SUPPLEMENTAL MATERIAL Title: Misery perfusion, blood pressure control, and a 5-year stroke risk in symptomatic major cerebral artery disease Authors: Hiroshi Yamauchi, Shinya Kagawa, Yoshihiko Kishibe, Masaaki Takahashi, Tatsuya Higashi Academic affiliation: Division of PET Imaging, Shiga Medical Centre Research Institute, Shiga, Japan Address correspondence to: Hiroshi Yamauchi, Division of PET Imaging, Shiga Medical Center Research Institute, 5-4-30 Moriyama, Moriyama 524-8524, Japan Tel: +81-77-582-6034; Fax: +81-77-582-6041 E-mail: [email protected]
2
Supplemental Methods Materials and methods Patients We analyzed data collected from 130 medically treated patients enrolled in our observational study. We investigated the relationship between hemodynamic compromise and stroke risk in symptomatic patients with atherosclerotic occlusive disease of the major cerebral arteries other than extracranial ICA stenosis. Patients were first referred to the PET unit at Shiga Medical Center from the outpatient clinic or other hospitals in the Shiga Prefecture to undergo hemodynamic parameter evaluation as part of a clinical assessment to determine the need for extracranial-to-intracranial (EC-IC) bypass.
Inclusion criteria for the observational study were as follows: 1) occlusion of the extracranial ICA or occlusion or stenosis (>50% diameter reduction) of the intracranial ICA or MCA as documented by conventional or magnetic resonance angiography; 2) the ability to independently perform daily life activities (modified Rankin scale score <3); and 3) history of transient ischemic attack (TIA) or complete stroke involving the relevant ICA or MCA territory at any time before PET examination. TIA was defined as the development of focal symptoms of presumed ischemic cerebrovascular origin lasting <24 h. The exclusion criteria were as follows: 1) history of vascular reconstruction surgery; or 2) the presence of potential sources of cardiogenic embolism. Overall, 35 of the 165 patients enrolled in the study underwent bypass surgery due to hemodynamic impairment observed on PET and were excluded from the present study. Hypertension, diabetes mellitus, ischemic heart disease, and hypercholesterolemia were judged as present based on treatment history at the time of PET examination. The ethics committee of our center approved the study protocol, and all patients provided written informed consent prior to participation. Positron emission tomography measurements All patients underwent PET scans with a whole-body Advance PET scanner (General Electric Medical System, Wauwatosa, WI, USA), which permits simultaneous acquisition of 35 image slices with inter-slice spacing of 4.25 mm.1 The intrinsic scanner resolutions were 4.6–5.7 mm and 4.0–5.3 mm in the transaxial and axial directions, respectively. As part of the scanning procedure, but before tracer administration, 68Ge/68Ga transmission scanning was performed for 10 min for attenuation correction. Functional images were reconstructed as 128 × 128 pixels, with each pixel representing an area of 2.0 × 2.0 mm.
A series of 15O-gas studies was also performed. C15O2 and 15O2 were inhaled continuously through a mask. The total scan time was 5 min. Bolus inhalation of C15O with 3-min scanning was used to measure CBV. Arterial samples were manually obtained during the scanning.
The CBF, cerebral metabolic rate of oxygen, and oxygen extraction fraction (OEF) were calculated based on the steady-state method.2, 3The ratio of CBF to CBV was calculated pixel-by-pixel as an indicator of the cerebral perfusion pressure.4 Data analysis We analyzed 10 tomographic planes from 46.25–84.5 mm above and parallel to the orbitomeatal line, which corresponded to the levels from the basal ganglia and thalamus to the centrum semiovale.5 The region of interest (ROI) was placed on the CBF images. Each image was examined by placing 10–12 circular ROIs (16 mm in diameter) compactly over the grey matter of the outer cortex in each hemisphere. According to the atlas, the ROIs in all 10 images covered the distribution of the MCA and the watershed areas. The same ROIs were transferred to the other images. The mean hemispheric

3
values in each hemisphere were calculated as the average of the values of all circular ROIs. In patients with cerebral cortex infarction, the circular ROIs that overlapped low-intensity areas on T1-weighted magnetic resonance imaging (MRI) scans were excluded from analysis using a simple method of correlating the PET scans with the MRI scans.6
Normal control values of the 15O-gas PET variables were obtained from seven normal volunteers (4 men, 3 women) aged 47 ± 7 years old (mean ± standard deviation [SD]) who underwent normal routine neurological examinations and MRI scans. The mean OEF value obtained from these 14 control hemispheres was 44.5% ± 3.8%. Hemispheric OEF values defined beyond the upper 95% limit in normal subjects (>52.9%) represented increased OEF. Comparative values for CBF and the CBF/CBV ratio in normal controls were 44.6 ± 4.5 and 11.4 ± 1.8, respectively. Hemispheric CBF and CBF/CBV ratio values <35.0 mL/100 g/min and 7.6/min, respectively, were considered abnormal.
Patients with an increased OEF, decreased CBF, and decreased CBF/CBV ratio in hemispheres with arterial disease were categorized as having MP, while patients with a decreased CBF/CBV ratio were categorized as having decreased cerebral perfusion pressure (i.e., impaired perfusion). Patients were categorized by an investigator who was blinded to their clinical status. Follow-up and outcomes Attending physicians were informed of the PET findings, but treatment of risk factors and the use of drugs was left to their clinical judgment. All patients were examined at 1- or 2-month intervals after undergoing PET studies in the outpatient clinic of our center or of related hospitals in the Shiga Prefecture. At each visit, an interim history was obtained, BP was measured, and a neurological examination was performed. Patients were followed for 5 years or until stroke recurrence or death. Recurrent ischemic stroke was defined as the acute onset of a new focal neurological deficit of cerebral origin persisting for >24 h without primary intracranial hemorrhage on CT or MRI scan. Statistical analysis The patients’ clinical backgrounds were compared between the groups using Student’s t tests or chi-squared tests, as appropriate; significance was established at p < 0.05. The incidence of recurrent stroke was compared between the groups using Mantel-Cox log-rank statistics and the Kaplan-Meier survival curves. Survival analysis of the subsequent endpoints began on the day of PET examination, which was considered the date of study entry. Multivariate analysis using the Cox proportional hazards model was used to test the effect of multiple variables on stroke recurrence. Covariate selection was performed by including the following covariates in a stepwise model: age, sex, recurrent symptoms (i.e., recurrent episodes of ischemic attack prior to PET scan or after angiographic demonstration of arterial disease), the time between the last symptoms and the PET scan, symptomatic arterial occlusion, extracranial ICA occlusion, complications (e.g., hypertension, diabetes mellitus, prior ischemic heart disease, hypercholesterolemia), smoking habit, BP during follow-up (categorization or normal BP), and misery perfusion or decreased CBF/CBV ratio. A forward stepwise selection was performed, and covariates were included and selected based on a significant relationship (p < 0.05) with an outcome event to enter into the model so that p < 0.05 remained in the model. The selected covariates were then included in a final model for analysis. The differences in the relationship between the follow-up BP with recurrent strokes in the subgroups were evaluated by adding an interaction term to the model.

4
References 1. Okazawa H, Yamauchi H, Sugimoto K, Takahashi M, Toyoda H, Kishibe Y, et
al. Quantitative comparison of the bolus and steady-state methods for measurement of cerebral perfusion and oxygen metabolism: Positron emission tomography study using 15O gas and water. J Cereb Blood Flow Metab. 2001;21:793-803
2. Frackowiak RSJ, Lenzi GL, Jones T, Heather JD. Quantitative measurement of regional cerebral blood flow and oxygen metabolism in man using 15O and positron emission tomography: Theory, procedure, and normal values. J Comput Assist Tomogr. 1980;4:727-736
3. Lammertsma AA, Jones T. Correction for the presence of intravascular oxygen-15 in the steady-state technique for measuring regional oxygen extraction ratio in the brain: 1. Description of the method. J Cereb Blood Flow Metab. 1983;3:416-424
4. Rothwell PM, Howard SC, Spence JD. Relationship between blood pressure and stroke risk in patients with symptomatic carotid occlusive disease. Stroke. 2003;34:2583-2590
5. Yamauchi H, Fukuyama H, Kimura J, Konishi J, Kameyama M. Hemodynamics in internal carotid artery occlusion examined by positron emission tomography. Stroke. 1990;21:1400-1406
6. Yamauchi H, Fukuyama H, Harada K, Yamaguchi S, Miyoshi T, Doi T, et al. White matter hyperintensities may correspond to areas of increased blood volume: Correlative MR and PETobservations. J Comput Assist Tomogr. 1990;14:905-908
5
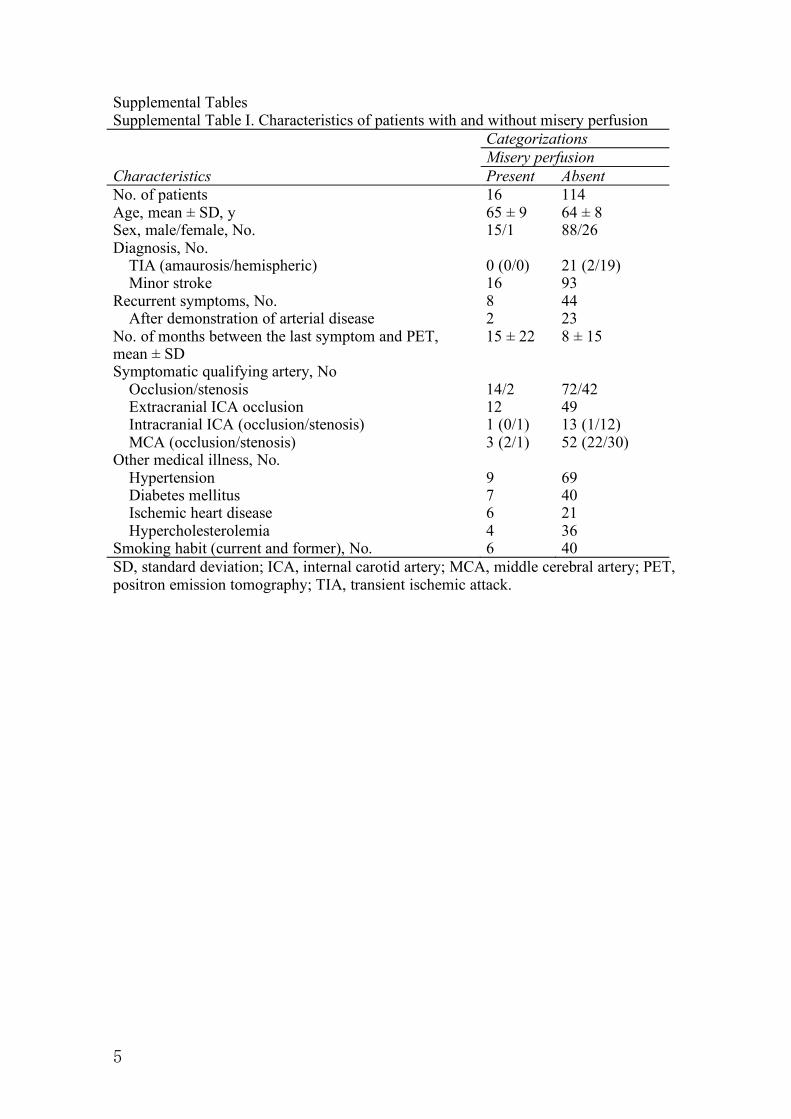
Supplemental Tables Supplemental Table I. Characteristics of patients with and without misery perfusion Categorizations Misery perfusion Characteristics Present Absent No. of patients 16 114 Age, mean ± SD, y 65 ± 9 64 ± 8 Sex, male/female, No. 15/1 88/26 Diagnosis, No. TIA (amaurosis/hemispheric) 0 (0/0) 21 (2/19) Minor stroke 16 93 Recurrent symptoms, No. 8 44 After demonstration of arterial disease 2 23 No. of months between the last symptom and PET, mean ± SD
15 ± 22 8 ± 15
Symptomatic qualifying artery, No Occlusion/stenosis 14/2 72/42 Extracranial ICA occlusion 12 49 Intracranial ICA (occlusion/stenosis) 1 (0/1) 13 (1/12) MCA (occlusion/stenosis) 3 (2/1) 52 (22/30) Other medical illness, No. Hypertension 9 69 Diabetes mellitus 7 40 Ischemic heart disease 6 21 Hypercholesterolemia 4 36 Smoking habit (current and former), No. 6 40 SD, standard deviation; ICA, internal carotid artery; MCA, middle cerebral artery; PET, positron emission tomography; TIA, transient ischemic attack.
6
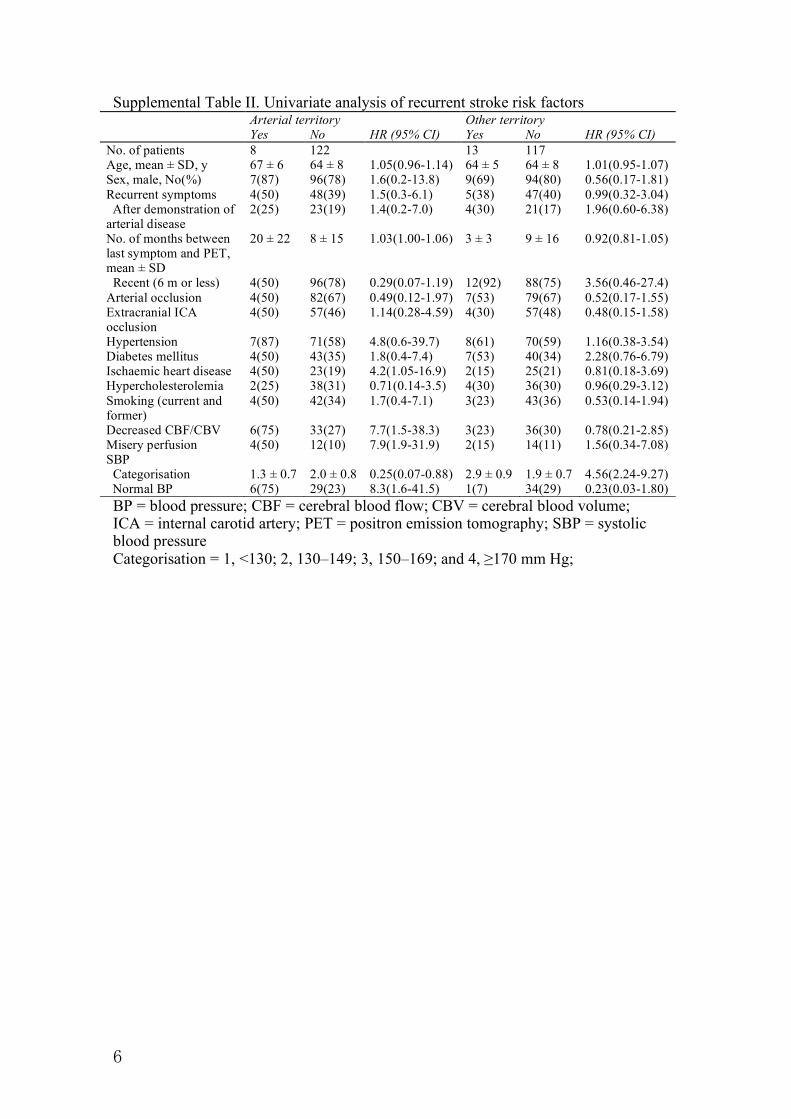
Supplemental Table II. Univariate analysis of recurrent stroke risk factors Arterial territory Other territory Yes No HR (95% CI) Yes No HR (95% CI) No. of patients 8 122 13 117 Age, mean ± SD, y 67 ± 6 64 ± 8 1.05(0.96-1.14) 64 ± 5 64 ± 8 1.01(0.95-1.07) Sex, male, No(%) 7(87) 96(78) 1.6(0.2-13.8) 9(69) 94(80) 0.56(0.17-1.81) Recurrent symptoms 4(50) 48(39) 1.5(0.3-6.1) 5(38) 47(40) 0.99(0.32-3.04) After demonstration of arterial disease
2(25) 23(19) 1.4(0.2-7.0) 4(30) 21(17) 1.96(0.60-6.38)
No. of months between last symptom and PET, mean ± SD
20 ± 22 8 ± 15 1.03(1.00-1.06) 3 ± 3 9 ± 16 0.92(0.81-1.05)
Recent (6 m or less) 4(50) 96(78) 0.29(0.07-1.19) 12(92) 88(75) 3.56(0.46-27.4) Arterial occlusion 4(50) 82(67) 0.49(0.12-1.97) 7(53) 79(67) 0.52(0.17-1.55) Extracranial ICA occlusion
4(50) 57(46) 1.14(0.28-4.59) 4(30) 57(48) 0.48(0.15-1.58)
Hypertension 7(87) 71(58) 4.8(0.6-39.7) 8(61) 70(59) 1.16(0.38-3.54) Diabetes mellitus 4(50) 43(35) 1.8(0.4-7.4) 7(53) 40(34) 2.28(0.76-6.79) Ischaemic heart disease 4(50) 23(19) 4.2(1.05-16.9) 2(15) 25(21) 0.81(0.18-3.69) Hypercholesterolemia 2(25) 38(31) 0.71(0.14-3.5) 4(30) 36(30) 0.96(0.29-3.12) Smoking (current and former)
4(50) 42(34) 1.7(0.4-7.1) 3(23) 43(36) 0.53(0.14-1.94)
Decreased CBF/CBV 6(75) 33(27) 7.7(1.5-38.3) 3(23) 36(30) 0.78(0.21-2.85) Misery perfusion 4(50) 12(10) 7.9(1.9-31.9) 2(15) 14(11) 1.56(0.34-7.08) SBP Categorisation
1.3 ± 0.7
2.0 ± 0.8
0.25(0.07-0.88)
2.9 ± 0.9
1.9 ± 0.7
4.56(2.24-9.27)
Normal BP 6(75) 29(23) 8.3(1.6-41.5) 1(7) 34(29) 0.23(0.03-1.80) BP = blood pressure; CBF = cerebral blood flow; CBV = cerebral blood volume; ICA = internal carotid artery; PET = positron emission tomography; SBP = systolic blood pressure Categorisation = 1, <130; 2, 130–149; 3, 150–169; and 4, ≥170 mm Hg;

7
Supplemental Table III. Five-year stroke occurrence and SBP SBP, mmHg <130 130–149 150–169 >170 Ischemic stroke in the territory Total (n = 130)
6/36 (16.6%)
1/60 (1.7%)
1/29 (3.4%)
0/5 (0%)
With misery perfusion* (n = 16)
3/7 (42.9%)
0/5 (0%)
1/3 (33.3%)
0/1 (0%)
Decreased CBF/CBV, normalOEF (n = 23)
1/5 (20%)
1/11 (9.0%)
0/7 (0%)
0/0 (0%)
Normal CBF/CBV, increased OEF (n = 16) Normal CBF/CBV, normal OEF (n = 75)
0/4 (0%) 2/20 (10%)
0/11 (0%) 0/33 (0%)
0/1 (0%) 0/18 (0%)
0/0 (0%) 0/4 (0%)
Any ischemic stroke Total (n = 130)
7/36 (19.4%)
3/60 (5%)
6/29 (20.6%)
1/5 (20%)
With misery perfusion* (n = 16)
3/7 (42.9%)
1/5 (20%)
1/3 (33.3%)
0/1 (0%)
Decreased CBF/CBV, normalOEF (n = 23)
1/5 (20%)
2/11 (19.0%)
0/7 (0%)
0/0 (0%)
Normal CBF/CBV, increased OEF (n = 16) Normal CBF/CBV, normal OEF (n = 75)
0/4 (0%) 3/20 (15%)
0/11 (0%) 0/33 (0%)
0/1 (0%) 5/18 (27%)
0/0 (0%) 1/4 (25%)
Stroke in other vascular territory Total (n = 130)
1/36 (2.7%)
3/60 (5.0%)
5/29 (17.2%)
4/5 (80%)
With misery perfusion* (n = 16)
0/7 (0%)
2/5 (40%)
0/3 (0%)
0/1 (0%)
Decreased CBF/CBV, normalOEF (n = 23)
0/5 (0%)
1/11 (9.0%)
0/7 (0%)
0/0 (0%)
Normal CBF/CBV, increased OEF (n = 16) Normal CBF/CBV, normal OEF (n = 75)
0/4 (0%) 1/20 (5%)
0/11 (0%) 0/33 (0%)
0/1 (0%) 5/18 (27%)
0/0 (0%) 4/4 (100%)
All stroke Total (n = 130)
7/36 (19.3%)
4/60 (6.7%)
6/29 (20.6%)
4/5 (80%)
With misery perfusion* (n = 16)
3/7 (42.9%)
2/5 (40%)
1/3 (33.3%)
0/1 (0%)
Decreased CBF/CBV, normalOEF (n = 23)
1/5 (20%)
2/11 (18.0%)
0/7 (0%)
0/0 (0%)
Normal CBF/CBV, increased OEF (n = 16) Normal CBF/CBV, normal OEF (n = 75)
0/4 (0%) 3/20 (15%)
0/11 (0%) 0/33 (0%)
0/1 (0%) 5/18 (27%)
0/0 (0%) 4/4 (100%)
CBF, cerebral blood flow; CBV, cerebral blood volume; OEF, oxygen extraction fraction; SBP, systolic blood pressure *Misery perfusion or decreased CBF/CBV in the territory.
28 Stroke 한국어판 Vol. 8, No. 2
Abstract 7
증상성 주요 대뇌동맥질환 환자에서의 극단적 관류 저하, 혈압 조절 및 5년 뇌졸중 위험성
Misery Perfusion, Blood Pressure Control, and 5-Year Stroke Risk in Symptomatic Major Cerebral Artery Disease
Hiroshi Yamauchi, MD, PhD; Shinya Kagawa, MS; Yoshihiko Kishibe, RT; Masaaki Takahashi, RT; Tatsuya Higashi, MD, PhD
(Stroke. 2015;46:265-268.)
Key Words: blood pressure ■ cerebrovascular disease ■ positron emission tomography ■ prognosis
배경과 목적
증상성대뇌동맥질환 및 극단적 관류저하(misery perfusion, MP)
가 있는 고위험 환자에서, 엄격한 혈압(blood pressure, BP) 조절
의 유용성은 아직 논란의 여지가 있다. 연구자들은 (1) MP가 5년
뇌졸중 위험도의 예측 인자인지, (2) 추적 관찰 기간의 BP, MP 및
뇌졸중 위험도 사이의 상호 관계를 분석하고자 하는 목적을 갖고
본 연구를 진행하였다.
방법
증상성 주요 대뇌동맥 질환을 갖고 어느 정도 일상 생활이 가능한
130명의 환자를 수집하였다. 초기 혈역학적 측정은 15O-기체 양전
자방출단층영상(positron emission tomography)을 이용하여 측
정하였으며, 대상 환자들을 의학적 치료를 받으며 5년 간 혹은 뇌
졸중 재발 또는 사망이 발생할 시점까지 추적 관찰하였다.
결과
5년의 추적 관찰 기간 동안, 뇌졸중은 MP가 있는 환자 16명 중 6
명 그리고 MP가 없는 환자 114명 중 15명에서 발생하였다(로그-
순위 검정; P<0.01). MP가 있는 환자에서 4건(25%)의 동측 허혈
뇌졸중이 발생하였고, MP가 없는 환자에서는 4건이 발생하였다
(P<0.001). 동측의 허혈뇌졸중 발생 위험은 2년이 지나면서 급격
히 감소하였고, MP가 없는 환자에서는 단 한 건의 동측 허혈뇌졸
중만 발생하였다. 관류가 저하된 환자(MP 포함)에서 정상적인 수
축기 BP(<130 mmHg)을 유지할 때 동측 허혈뇌졸중의 위험이 증
가하였으나, MP가 없는 환자에서 수축기 BP가 130-149 mmHg
범위 밖으로 유지되면 모든 종류의 뇌졸중 위험도가 증가하였다.
결론
MP가 있는 환자는 5년 뇌졸중 재발 위험도가 증가하는데, 그러한
추가 위험의 상당수는 2년이 지나면서 감소한다. MP를 비롯하여
관류가 저하된 환자에서 적극적인 BP 조절은 위해를 입힐 가능성
이 있다.
162 Stroke January 2015
renal dysfunction further increases the risk of ischemic stroke significantly after accounting for other known thromboembolic risk factors. In addition, our study demonstrated that adding renal dysfunction to the CHADS
2 score yields a small but sta-
tistically significant improvement in c-statistic. Given these findings, further studies are warranted to elucidate the additive predictive value of renal dysfunction to CHA
2DS
2-VASc score.
Strengths of this meta-analysis include the strict inclusion crite-ria, the large number of patients analyzed, the robustness of the find-ings in sensitivity analyses, and the fact that all subgroup analyses
were prespecified a priori. The absence of important publication bias supports the robustness of the study findings. A possible limita-tion of our study is the heterogeneity of the studies with regard to adjustment of the estimates for potential confounders. Although dif-ferences in number of events and the outcomes of interest, at least in part, explain this finding, the specific mechanism remains unclear. Inclusion of different types of studies into one meta-analysis may also introduce heterogeneity into the results. Despite this, the con-sistency of the finding of an increased thromboembolic risk among cohort studies and randomized controlled trials suggests that the association is valid. Another limitation was the lack of individual participant data, which precluded determining the independent associations of individual variables with study outcomes. Instead, we used between-study meta-regressions, when possible.
In conclusion, impaired renal function is a predictor of incident stroke and systemic embolism in patients with non-valvular AF taking and not taking OACs, independent of conventional thromboembolic risk factors. Adding CKD to the CHADS
2 stroke risk scores slightly improved the risk dis-
crimination, and consideration of renal function may improve stroke risk stratification in patients with AF.
DisclosuresNone.
References 1. Albertsen IE, Rasmussen LH, Overvad TF, Graungaard T, Larsen TB,
Lip GY. Risk of stroke or systemic embolism in atrial fibrillation patients treated with warfarin: a systematic review and meta-analysis. Stroke. 2013;44:1329–1336.
2. Kokubo Y, Nakamura S, Okamura T, Yoshimasa Y, Makino H, Watanabe M, et al. Relationship between blood pressure category and incidence of stroke and myocardial infarction in an urban Japanese population with and without chronic kidney disease: the Suita Study. Stroke. 2009;40:2674–2679.
3. Di Angelantonio E, Chowdhury R, Sarwar N, Aspelund T, Danesh J, Gudnason V. Chronic kidney disease and risk of major cardiovascular disease and non-vascular mortality: prospective population based cohort study. BMJ. 2010;341:c4986.
4. Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–1305.
5. Go AS, Fang MC, Udaltsova N, Chang Y, Pomernacki NK, Borowsky L, et al. Impact of proteinuria and glomerular filtration rate on risk of throm-boembolism in atrial fibrillation: the anticoagulation and risk factors in atrial fibrillation (ATRIA) study. Circulation. 2009;119:1363–1369.
6. Soliman EZ, Prineas RJ, Go AS, Xie D, Lash JP, Rahman M, et al. Chronic kidney disease and prevalent atrial fibrillation: the Chronic Renal Insufficiency Cohort (CRIC). Am Heart J. 2010;159:1102–1107.
7. Baber U, Howard VJ, Halperin JL, Soliman EZ, Zhang X, McClellan W, et al. Association of chronic kidney disease with atrial fibrillation among adults in the United States: REasons for Geographic and Racial Differences in Stroke (REGARDS) Study. Circ Arrhythm Electrophysiol. 2011;4:26–32.
8. Tonelli M, Muntner P, Lloyd A, Manns B, Klarenbach S, Pannu N, et al. Impact of age on the association between CKD and the risk of future coronary events. Am J Kidney Dis. 2014;64:375–382.
9. Friberg L, Benson L, Lip GY. Balancing stroke and bleeding risks in patients with atrial fibrillation and renal failure: the Swedish Atrial Fibrillation Cohort study [publishead online ahead of print April 10, 2014]. Eur Heart J. doi: 10.1093/eurheartj/ehu139. http://eurheartj.oxfordjournals.org/content/early/2014/04/09/eurheartj.ehu139.long. Accessed July 4, 2014.
10. Reinecke H, Engelbertz C, Schäbitz WR. Preventing stroke in patients with chronic kidney disease and atrial fibrillation: benefit and risks of old and new oral anticoagulants. Stroke. 2013;44:2935–2941.
11. January CT, Wann LS, Alpert JS, Calkins H, Cleveland JJ, Cigarroa JE, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the american
Table 3. AUC Analysis for 3 Risk Stratification Models in Predicting Thromboembolic Events in AF Patients
CHADS2
CHA2DS
2−VASc CHADS
2+CKD
Study AUC (95% CI)c AUC (95% CI) AUC (95% CI)
Swedish Atrial Fibrillation Cohort study
0.72 (0.72–0.73) 0.71 (0.71–0.72) 0.72 (0.71–0.72)
Roldan V 0.65 (0.62–0.68) 0.62 (0.59–0.65) 0.64 (0.61–0.67)
Chao TF NA 0.83 (0.73–0.93) 0.87 (0.79–0.95)
ROCKET AF 0.57 (0.55–0.60) 0.58 (0.55–0.60) 0.59 (0.56–0.61)
Leipzig Heart Center AF Ablation Registry
0.72 (0.70–0.74) 0.74 (0.72–0.75) 0.74 (0.72–0.75)
AMADEUS Trial 0.64 (0.56–0.73) 0.67 (0.60–0.75) 0.69 (0.62–0.76)
The Loire Valley Atrial Fibrillation Project
0.64 (0.61–0.67) 0.64 (0.62–0.67) 0.64 (0.61–0.67)
ATRIA Study 0.66 (0.62–0.70) 0.69 (0.67–0.71) 0.71 (0.69–0.74)
Pooled AUC estimates 0.66 (0.62–0.70) 0.68 (0.64–0.71) 0.69 (0.65–0.73)
AF indicates atrial fibrillation; AMADEUS, Evaluating the Use of SR34006 Compared to Warfarin or Acenocoumarol in Patients With Atrial Fibrillation; ATRIA, Anticoagulation and Risk Factors in Atrial Fibrillation; AUC, area under the curve; CHADS
2, congestive heart failure, hypertension, age, diabetes mellitus,
stroke/transient ischemic attack; CHA2DS
2-VASc, congestive heart failure,
hypertension, age (>75 y), diabetes mellitus, stroke/transient ischemic attack, vascular disease, age (65–74 y), sex (female); and ROCKET, Rivaroxaban Once-Daily, Oral, Direct Factor Xa Inhibition Compared With Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation.
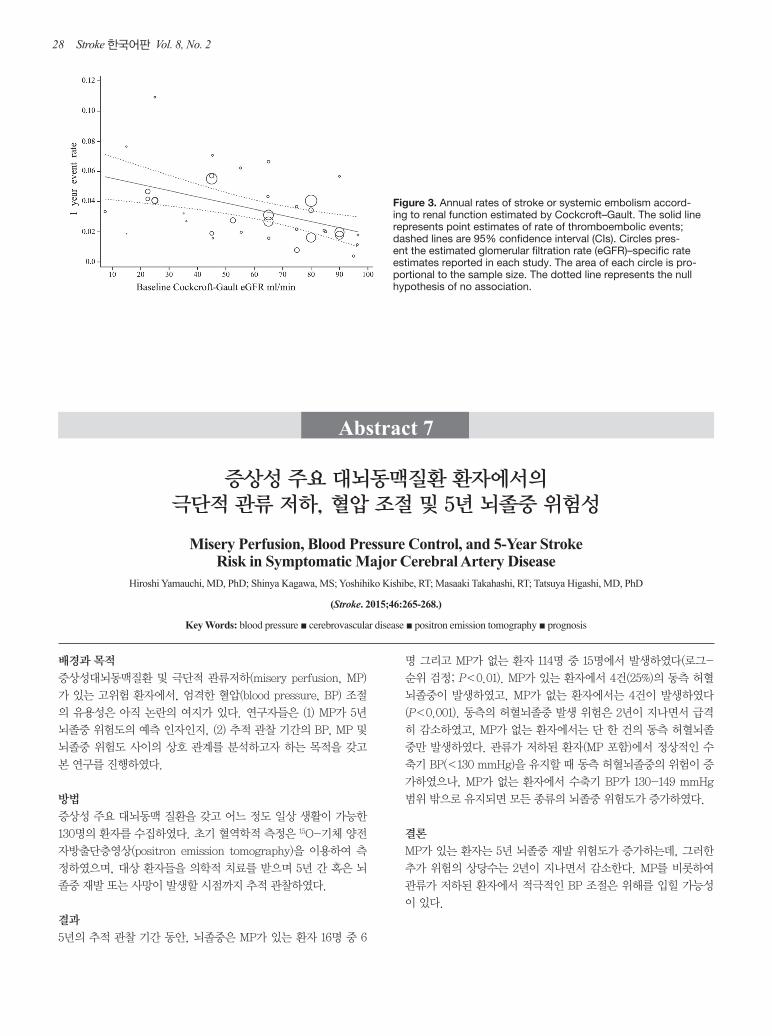
Figure 3. Annual rates of stroke or systemic embolism accord-ing to renal function estimated by Cockcroft–Gault. The solid line represents point estimates of rate of thromboembolic events; dashed lines are 95% confidence interval (CIs). Circles pres-ent the estimated glomerular filtration rate (eGFR)–specific rate estimates reported in each study. The area of each circle is pro-portional to the sample size. The dotted line represents the null hypothesis of no association.
29
Abstract 8
뇌내출혈이 발병한 후에 깊은 정맥혈전증 예방을 위한 항응고요법을 하는 것이 흔한 의료행위인가?
Is Prophylactic Anticoagulation for Deep Venous Thrombosis Common Practice After Intracerebral Hemorrhage?
Shyam Prabhakaran, MD, MS; Patricia Herbers, MS; Jane Khoury, PhD; Opeolu Adeoye, MD; Pooja Khatri, MD; Simona Ferioli, MD; Dawn O. Kleindorfer, MD
(Stroke. 2015;46:369-375.)
Key Words: anticoagulants ■ pulmonary embolism ■ thromboembolism
배경과 목적
뇌내출혈(intracerebral hemorrhage, ICH) 이후 깊은 정맥혈전증
예방을 위해 항응고요법을 하는 것은 안전하다. 현재의 진료지침
은 혈종이 커지는 것이 멈추면 예방적 항응고요법을 할 것을 권고
한다. 이 연구는 ICH 발생 이후의 깊은 정맥혈전증 예방에 대한
전국적인 동향을 평가하려고 하였다.
방법
Premier 데이터베이스를 분석하여 2006년부터 2010년 사이에 입
원하여 이틀 이상 생존한 성인 ICH(국제질병분류 9판 코드 431)
환자를 찾아냈다. 외상이 있거나 개두술, 혈관조영술을 받은 환자
는 제외하였다. 연구자들은 처방한 항응고제의 종류와 처음 투여
한 날짜를 조사하였다. 단변량 통계와 다변수 로지스틱 회귀분석
을 이용해서 ICH 이후 예방적 항응고요법을 하게 되는 것과 관련
이 있는 인자를 조사하였다.
결과
32690명(평균 나이, 69.7세; 남자, 50.1%)의 자발성 ICH 환자 중
에서, 5395명(16.5%)이 입원 중에 예방적 항응고요법을 받았다.
이 중에서, 2416명(44.8%)은 2일 이내에 예방적 항응고요법을 받
았다. 가장 흔히 사용한 약물은 헤파린(71.1%), 에녹사파린
(enoxaparin, 27.5%), 달테파린(dalteparin, 1.4%)이었다. 예방적
항응고요법을 받은 환자의 비율은 연구 기간 동안 14.3%에서
18.0%로 약간 증가하였다(P<0.01 for trend). 미국 내에서 지리
적인 지역의 차이에 따라 예방적 항응고요법의 사용은 차이가 나
서(P<0.001) 북동부(23.2%), 남부(19.0%), 중서부(10.8%), 서부
(9.8%)의 순이었다. 다변수 분석에서 지리적인 지역은 예방적 항
응고요법의 독립적인 예측 인자였다.
결론
미국의 ICH 환자 중 20%가 안 되는 비율에서 깊은 정맥혈전증 예
방을 위한 항응고요법을 받는다. 사용하는 경우 이틀 이내에 시작
하는 비율은 절반이 안 되었다. 이후의 연구는 진료의 변이에 대해
이해하는데 집중하고 진료지침에 근거한 치료를 강조해야 한다.
Yamauchi et al Misery Perfusion, Blood Pressure Control, and Stroke Risk 267
CBV ratio, the SBP outside the 130 to 149 mm Hg range was significantly associated with an increased risk of all strokes (Fisher exact test, P<0.0005).
In multivariate analysis using the Cox proportional hazard model, MP and a normal SBP (<130 mm Hg) were indepen-dently associated with an increased risk of ipsilateral ischemic stroke. The adjusted HRs conferred by the presence of MP and a normal SBP were 6.1 (95% CI, 1.5–25.3; P<0.05) and 6.8 (95% CI, 1.3–34.6; P<0.05), respectively. Alternatively, the adjusted HRs conferred by the presence of a decreased CBF/CBV ratio and a normal SBP were 7.6 (95% CI, 1.5–37.9; P<0.05) and 8.2 (95% CI, 1.6–40.9; P<0.05), respectively. The risk of all strokes was independently associated with MP (adjusted HR, 2.9; 95% CI, 1.1–7.5; P<0.05) and SBP (range, 130–149 mm Hg; adjusted HR, 0.26; 95% CI, 0.08–0.78; P<0.05).
In 61 patients with ICA occlusion, all 4 ipsilateral ischemic strokes occurred only in patients with a normal SBP (<130 mm Hg); 2 in 12 MP patients, 0 in 9 with an increased OEF and a normal CBF/CBV ratio, 1 in 10 with a normal OEF and a decreased CBF/CBV ratio, and 1 in 30 with a normal OEF
and a normal CBF/CBV. Four strokes (3 hemorrhages) in the other vascular territories occurred only in patients without a normal SBP; 1 with MP, 1 with a normal OEF and a decreased CBF/CBV ratio, and 2 with a normal OEF and a normal CBF/CBV ratio.
DiscussionIn patients with symptomatic major cerebral arterial disease, MP was an independent predictor of a subsequent stroke risk during a 5-year follow-up period. The 5-year incidence of ipsilateral ischemic stroke (25%) and all strokes (37.5%) was higher in patients with MP than in those without MP (3.5% and 13.1%, respectively). The risk of ipsilateral ischemic stroke declined markedly after 2 years, and only 1 occurred in a patient without MP. Thus, a large part of the 5-year stroke risk in patients with MP disappeared after 2 years.
We provided data that showed a major decrease in the rate of ipsilateral ischemic stroke after 2 years in patients with MP, as shown in our previous study.3 Thus, continuing COSS for an additional 3 years would not have shown a significant bene-fit for surgery, and the surgical complication rates would have needed to be low. One possible explanation for this is that unstable MP may become stabilized or attenuated over time in relation to the development of collaterals or the reduced meta-bolic demand because of ischemic neuronal damage.
This study also demonstrated that the relationship between the follow-up BP and stroke risk differs between patients with and without impaired perfusion. All patients with MP had a decreased CBF/CBV ratio. In patients with impaired perfusion, a normal SBP (<130 mm Hg) was associated with an increased risk of ipsilateral ischemic stroke. In patients without impaired perfusion, an SBP outside of the 130 to 149 mm Hg range was associated with an increased risk of all stroke. In patients with impaired perfusion, including those with MP, an aggressive reduction of BP may be hazardous, especially during the first 2 years after presentation.
Powers et al5 evaluated 91 nonsurgical controls from the COSS. All patients had an increased OEF ratio ipsilaterally to recent symptomatic carotid occlusion. They reported a reduced risk of ipsilateral ischemic stroke in patients with a mean SBP during follow-up of ≤130/85 mm Hg, which is inconsistent with our results. Several factors may contribute to this differ-ence. First, COSS studied only ICA occlusion. In our patients with ICA occlusion, ipsilateral ischemic stroke occurred only in patients with a normal SBP (<130 mm Hg). Second, in the COSS, it is unclear whether the patients had impaired perfu-sion. In our study, a lower BP was associated with an increased stroke risk in patients with a decreased CBF/CBV ratio, but not in patients with an increased OEF and a normal CBF/CBV ratio. Thirdly, the target goal for BP was 130/85 mm Hg in the COSS. In such patients with an increased OEF and a higher BP, a higher BP may barely maintain the CBF. Thus, patients with an increased OEF and a higher BP may be more susceptible to low-flow infarcts because of a reduction in BP than in those with a lower BP, which may cause stroke before BP can reach the target (130/85 mm Hg).2 The COSS surgical group showed a low postperioperative stroke rate after the improvement of the OEF ratio, despite a BP distribution similar to the nonsurgical group,4 which suggests that an interaction between an increased
Figure 3. Kaplan–Meier cumulative failure curves for ipsilateral ischemic stroke in patients with and without normal systolic blood pressure (SBP), with a decreased cerebral blood flow (CBF)/cerebral blood volume (CBV) ratio (upper), for all strokes in patients with or without SBP within the range of 130 to 149, and for patients without a decreased CBF/CBV ratio (lower).