Minister Departement WVG Youth Welfare Flemish Agency forCare and Health Care Inspectorate PC Geel...
58
Minister Departement WVG Youth Welfare Flemish Agency forCare and Health Care Inspectorate PC Geel PC Rekem Flemish Agency of Disabled Persons Child and Family Strategic Advisory Council Flemish Care Fund Fund for Youth Welfare Policy Council Management committee Flemish Ministry of Welfare, Public Health and Family (WVG)
-
Upload
may-willis -
Category
Documents
-
view
215 -
download
1
Transcript of Minister Departement WVG Youth Welfare Flemish Agency forCare and Health Care Inspectorate PC Geel...

Minister
DepartementWVG
Youth Welfare
Flemish Agency forCare
and Health
Care
InspectoratePC Geel
PCRekem
Flemish Agency of Disabled Persons
Child and Family
Strategic Advisory Council
Flemish Care Fund
Fund for Youth Welfare
Policy Council
Management committee
Flemish Ministry of Welfare, Public Health and Family (WVG)

1. Health and health care policy in Flanders (Machteld Wauters - VAZG)
2. VIPA: funding health care infrastructure (Christophe Cousaert - VIPA)
3. Innovation initiatives: Primary Care Safe and Flanders’ Care (Machteld Wauters)

Health and health care policy in Flanders
Machteld WautersFlemish Agency for Care and Health

Health in Flanders
• Belgium: regions and communities
• Competences in health
• Flemish policy in health– Public health – Health care

Belgium


Political situation
• (De)federalisation process: since 1980 responsibilities for health care are increasingly delegated to regional level (‘devolution’)
• Complex: 6 authorities responsible for health matters in Brussels!
• Interministerial conferences to ensure consistency and complementarity of policies

Belgium Flanders (person-related matters)
Health/Health Care
- Organic laws
- Basis rules planning/ financing infrastructure
- Financing regulation operating costs hospitals/nursing homes
- Health insurance system
- Preventive health care
- Health promotion
- Implementation hospital standards, quality assurance policy
- Ambulatory mental health care
- Coordination home care
Infrastructure - DBF 40%
- Basic rules planning/financing infrastructure
- Subsidizing 60%
- Specific legislation quality
Competences healthcare Belgium/Flanders

Health care budget
107
17200
0 5000 10000 15000 20000
x 1 000 000 euro
Budget
FedHinsur
Flanders

Flanders
• Competences in health and health care
• Policy in public health
• Policy in health care

Flemish competences in health
• Health promotion
• Prevention of noncommunicable and communicable diseases
• Implementation of hospital standards, quality assurance policy in health services
• Subsidizing health care infrastructure
• Ambulatory mental health care
• Coordination of home care
Objectives of the Flemish health policy• Promote the choice for healthy
lifestyles
• Prevent diseases, their risk factors and complications
• Stimulate and monitor the performance of health care services
• Tune the supply of health care to the needs of the population
• Provide accessible and affordable care
• Strengthen active participation and correct treatment of users of care
Flemish agency

Flemish Agency for Care and Health
• The mission of the Agency is to create the conditions to promote, protect and restore the welfare and health of the current and future population of Flanders, aiming for an optimal level of welfare and health of all citizens.

Flemish preventive policy
Decree on preventive health care 2003
working with health targetsMETHODOLOGY

Decree on preventive health care 2003
• Epidemiological basis for policy • Health conference large societal basis
– Health targets (SMART)– Prevention strategies
• Approved by Parliament• Executed by government political
commitment

Decree on preventive health care 2003
• Epidemiological basis for policy
• Health targets
• Prevention strategies
• Implementation of policy
Health in all policies
•Partner organisations
•Organisations in the field
•Logo’s
•Individual providers
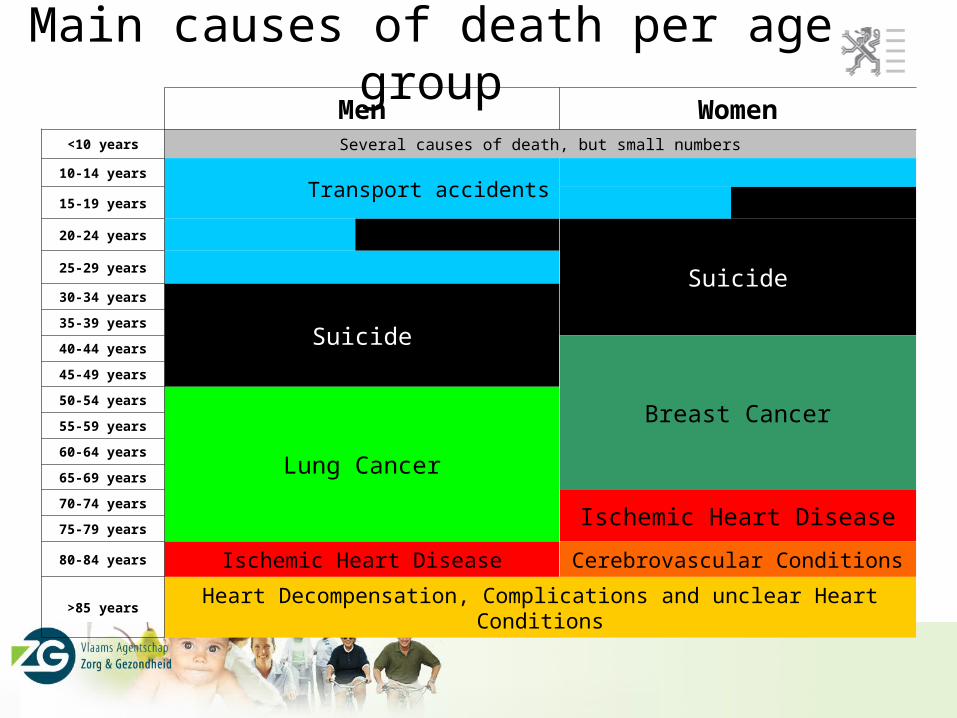
Main causes of death per age groupMen Women
<10 years Several causes of death, but small numbers
10-14 years
Transport accidents15-19 years
20-24 years
Suicide25-29 years
30-34 years
Suicide35-39 years
40-44 years
Breast Cancer
45-49 years
50-54 years
Lung Cancer
55-59 years
60-64 years
65-69 years
70-74 yearsIschemic Heart Disease
75-79 years
80-84 years Ischemic Heart Disease Cerebrovascular Conditions
>85 years Heart Decompensation, Complications and unclear Heart Conditions

Evolution of deaths preventable by primary prevention (1999 – 2008)

Flemish health targets
1. Diet and physical activity 2. Tobacco, alcohol and drugs3. Breast cancer screening4. Suicide prevention5. Injury prevention6. Prevention of infectious diseases by
vaccination

Health care
• Belgian Health care system
• Flemish competences and policy

Belgian health care system
• Compulsory public health insurance system• Independent medical practice• Free choice of health care provider by the
patient• Fee-for-service payment of providers, with
reimbursement

Flemish competences in health care
Implementation of hospital standards, quality assurance policy in hospitals and nursing homes
Subsidizing health care infrastructure

FLEMISH LEVELFEDERAL LEVELEXPLOITATION
INFRASTRUCTURE
€
Division of competences in Belgian health care policy : hospitals
Basic legislation
Basic legislation
Execute (recognitions)
Inspection of recognitions
Strict legislationVIPA
Funding 40% (BFM) €
- BFM (budget financial resources)
- RIZIV €
Subsidy/guarantee60% €

Flemish competences in health care
Implementation of hospital standards, quality assurance policy in hospitals and nursing homes
Subsidizing health care infrastructureCoordination of primary care and home
careAmbulatory mental health care

Flemish policy in health care
Priorities:Stimulate and monitor the performance of health care
servicesTune the supply of health care to the needs of the
populationProvide accessible and affordable careStrengthen active participation and correct treatment
of users of care

VIPA - Flemish Infrastructure Fund
Christophe Cousaert
Flanders, Belgium

1. VIPA: Flemish Infrastructure Fund
2. Funding hospital infrastructure
3. Facts and figures
4. Policy health infrastructure

1. VIPA: Flemish Infrastructure Fund
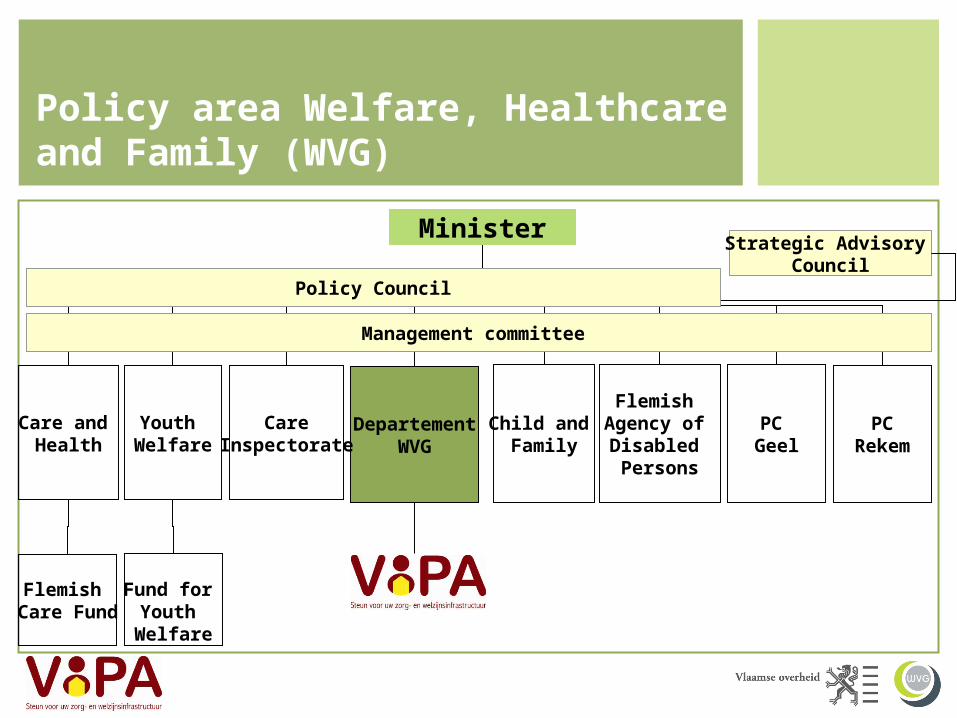
Minister
DepartementWVG
Youth Welfare
Care and Health
Care
InspectoratePC Geel
PCRekem
Flemish Agency of Disabled Persons
Child and Family
Strategic Advisory Council
Flemish Care Fund
Fund for Youth Welfare
Policy Council
Management committee
Policy area Welfare, Healthcare and Family (WVG)
“VIPA’s mission is to develop initiatives and provide funding for a high-quality, accessible and affordable infrastructure for the provision of care and services
within the framework of matters relating to the individual.”
Mission

Key assignments
The funding, in any way, of infrastructure of welfare and care 1.
The coördination, steering and direction of public-public and public-private partnership (PPS)
2.
The promotion of knowledge and expertise in terms of concept, finances
and technical engineering3.
The building up and management of financial reserves4.

Scope of application
Hospitals, psychiatric care homes, psychiatric hospitals
Elderly homes, day care centers, short stay centers, local service centers
Preventive and ambulatory healthcare
Facilities for youth welfare
Facilities for disabled persons
Creches
General welfare centers
1.
2.
3.
4.
5.
6.
7.

2. Funding hospital infrastructure

Funding hospital infrastructure
40%
60%

New building, renovation, purchase + renovation
Max. m²/resident (f.e.: 110 m²/res. general + 25% university; 90 m²/res. psychiatric)
Moveable investments = 60% accepted costs
Basic rules
60% accepted costs < max. cost price 1.100 €/m²(priority renovations = 10% Flanders)
Budget Financial Resources – 40% write-off amounts

Alternative funding hospital infrastructure
Agreement in principleFlemish minster
20 years utilisation grants linked to utilisation norms
(f.e.: occupancy rates, …)

I. Approved strategic care plan (ticket to start)
II. Approved technical-financial plan (businessplan + plans of architect)
II.1. Agreement in principle (no commitment) (= spreading funding over economic life of infrastructure (20 years))
II.2. Funding (utilisation grants) during 20 years linked to functional application to be justified
(by reviewing utlisation norms)
Procedure alternative funding

3. Facts and figures

Facts and figures
10,6 mio inhabitants 6 mio inhabitants
45.000 hospitalbeds 31.000 hospitalbeds
100 general hospitals 71 general hospitals

Number of general hospitals (incl. university hospitals)
2000-2010
91 88 85 85 83 81 7975 74 71
0
10
20
30
40
50
60
70
80
90
100
2000 2001 2002 2003 2004 2005 2006 2007 2008 2010
Facts and figures - evolution
- 20%
Incl. 4 university hospitals – excl. 39 psychiatric hospitals

Evolution number of hospital beds (general + university)
2000-2010
31.474 31.279 31.115 31.141 30.939 30.952 30.844 30.872 30.840 30.787
25.000
26.000
27.000
28.000
29.000
30.000
31.000
32.000
33.000
34.000
35.000
2000 2001 2002 2003 2004 2005 2006 2007 2008 2010
Incl. 4.600 university beds – excl. 10.000 psychiatric beds
One day hospital: 34% in 2000 to 47% in 2008 (+ 85% treatments)
Facts and figures - evolution

Average capacity general hospitals2000-2010
362 372 384 384 392 402 411435 441
460
0
50
100
150
200
250
300
350
400
450
500
2000 2001 2002 2003 2004 2005 2006 2007 2008 2010
800 mio € (80 mio €/year)
2010-2014: 1.800 mio € (360 mio €/year)!
Facts and figures - evolution
4. Policy health infrastructure

Quality of infrastructure Comfort
Healing environment: accent on userscomfort
Indoor climate: lower CO2-emissions
Sustainable and energy-efficiënt construction: sustainability criteria
Evolution to high-tech hospitals: best practices?

Quality of infrastructure Art
Design meets art – art meets design
Flemish government subsidizes art works integrated ininfrastructure projects
Networking
Future challenges = working together
Evolution to centers of excellence in specific segments

Innovation and Entrepreneurship in Care

Care: large economic impact
16% active population
8% GDP Flanders(unchanged policy)source: Planbureau
+ 70.000 jobs 2014

• Investing in qualitative and accessible care – Maximizing societal added value
• Investing in innovative care– Maximizing new perspectives in (health) care
• Investing in strong entrepreneurship in view of– Market innovation in Flanders– Maximizing economic added value– International valorization
Flanders’ Care

Care & Innovation & Economy
Kris Peeters, Flemish Minister-president
economy
Jo Vandeurzen,Flemish Minister
care
Ingrid Lieten, Vice Minister-presidentinnovation
Flanders’ Care mission statement
To measurably improve the quality of care through innovation and responsible entrepreneurship

Governance Structure

Innovation perspective
RESEARCH &DEVELOPMENT
Quality of Care
IMPLEMENTATION INTERNATIONALVALORIZATIONDEMONSTRATION
Economic Development

Policy instruments: finding synergies!
CareInnovation Entrepreneurship
Policy
Impulse office
Seed CapitalDemonstration projects
Innovativetendering

““Bridging the Gap”Bridging the Gap”
• Inform and sensitize stakeholders: – Care organizations– SMEs and other private companies– Knowledge sources
• Guidance:– Guide initiatives through the different government instruments of policy domains:
• Welfare, Public Health and Family Affairs (WVG, VIPA, …) • Economy, Science and Innovation (EWI: IWT, AO, PMV,…)• Flanders International (VI: FIT, VAIS,..)
• Brokerage:– Direct towards the most optimal government instrument for optimal use and
exploitation• Customized service • Start up: end of October
Impulse office Flanders’ Care

• €20 mio venture fund• Managed by PMV (Participatie Maatschappij Vlaanderen)• Supports entrepreneurship in care • for a more effective implementation of care technology• And a more innovative product and service offering in care• Target group: start-ups, young companies (SMEs) and
companies starting up new activities.• Complementary to the existing sources of seed capital• Necessary because of barriers specific to the care sector
– Long pre-commercialization trajectory– Diversity of stakeholders– Reimbursement system(s)– …
• Strong involvement care stakeholders in decision making process
Seed Capital in Care

Care for Talent• Competence buildup • For innovative solutions in care• Concept document: ‘making work of work’• General practitioners and specialists• Nurses and other care professionals• Primary healthcare conference
(December 2010)+ 70.000
Jobs in care

• Similar challenges all over EU• Importance of regional positioning
– Regions holding the implementation key– ‘Smart specialization’ – Requires a bottom-up approach
• Collaboration will yield societal benefits– Innovation absorption– Market development– Quality of care increase
• Benchmarking
EU perspective

• Flemish health portal:
www.zorg-en-gezondheid.be
• Contact: – [email protected]– [email protected]