MILD TRAUMATIC BRAIN INJURY AND THE … · 2017-10-10 · •Mild TBI is an acute brain injury...
63
MILD TRAUMATIC BRAIN INJURY AND THE POSTCONCUSSIONAL SYNDROME DR ROBIN JACOBSON ROYAL COLLEGE OF PSYCHIATRISTS SEPTEMBER 2017
Transcript of MILD TRAUMATIC BRAIN INJURY AND THE … · 2017-10-10 · •Mild TBI is an acute brain injury...

MILD TRAUMATIC BRAIN INJURY AND THE POSTCONCUSSIONALSYNDROME
DR ROBIN JACOBSON
ROYAL COLLEGE OF PSYCHIATRISTS SEPTEMBER 2017

DEFINITION OF MILD TBI ACRM (1993)
• A traumatically induced physiological disruption of brain function, with at least one
of the following:
• Any period of LOC ≤30 min
• Any loss of memory for events immediately before or after the accident (PTA <24 h)
• Any alteration in mental state at the time of the accident (feeling dazed,
disorientated or confused)
• Focal neurological deficit(s) that may or may not be transient
• GCS score 13–15 after 30 min

DEFINITION OF MILD TBI WHO (2004)
• Mild TBI is an acute brain injury resulting from external physical forces.
• Confusion or disorientation
• LOC ≤30 min
• PTA ≤24 h
• And/or other transient neurological abnormalities such as focal signs, seizure and
intracranial lesion not requiring surgery
• GCS score 13–15 after 30 min post-injury or later on presentation for health care
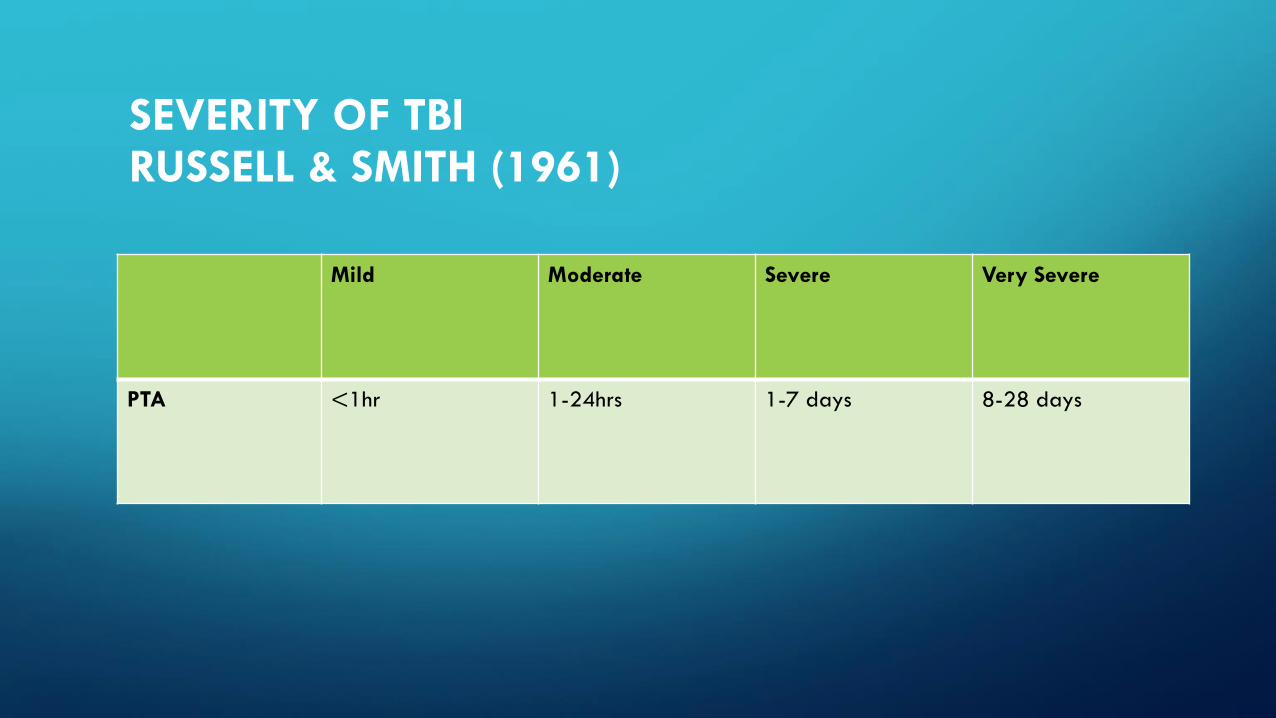
SEVERITY OF TBIRUSSELL & SMITH (1961)
Mild Moderate Severe Very Severe
PTA <1hr 1-24hrs 1-7 days 8-28 days

SEVERITY OF TBI DSM-5 (2013)
Mild Moderate Severe
GCS 13-15 9-12 3-8
LOC <30 min 30 min-24
hrs
>24 hours
PTA <24hrs >24hrs – 7
days
> 7 days

THE SPECTRUM OF mTBI IS VERY WIDE: GCS 13–15
• Category 0 GCS = 15 No LOC, no PTA = head injury, no TBI
No risk factors → Discharge
• Category 1 GCS = 15 LOC < 30 min, PTA < 1 h
No risk factors → CT recommended
• Category 2 GCS = 15 and risk factors present → CT mandatory
• Category 3 GCS = 13–14 LOC < 30 min, PTA < 1 h
With or without risk factors → CT mandatory
EFNS guidelines Vos et al, 2002

DAY-OF-INJURY CT SCAN ABNORMALITIES IN MTBI(COMPLICATED MTBI)
GCS
• 15 – 5%
• 14 - 20%
• 13 – 30%
Borg et al, 2004, WHO Task Force

TAMPERE UNIVERSITY ED COHORTRATES OF COMPLICATED MTBI (N=2766)
• GCS % abnormal CT head
• 15 10.1%
• 14 40.7%
• 13 52%
• Isokuortti et al, 2017

ARE INTRACRANIAL ABNORMALITIES RELATED TO CLINICAL OUTCOMES?
COGNITIVE OUTCOMES
• Those with intra-cranial abnormalities performed more poorly on
neuropsychological testing– (11 of 19 studies – 58%)
• But only small to medium effect sizes
• Usually on few of the cognitive tests
FUNCTIONAL OUTCOMES
• In 4 of 13 studies, complicated MTBI patients had greater problems on:
- Glasgow Outcome Scale
- Functional Independence Measure
- Global Adaptive Functioning Scale
- Return to work
• Most studies, however, have not found a significant difference in functional
outcomes.

ICD-10 POSTCONCUSSIONAL SYNDROME

Rivermead Post Concussion symptoms QuestionnaireCompared with before the accident, do you now (i.e., over the
last 24 hours) suffer from:
Headaches..................................................0 1 2 3 4
Feelings of Dizziness ................................. 0 1 2 3 4
Nausea and/or Vomiting ........................... 0 1 2 3 4
Noise Sensitivity,
easily upset by loud noise ................ 0 1 2 3 4
Sleep Disturbance ...................................... 0 1 2 3 4
Fatigue, tiring more easily ......................... 0 1 2 3 4
Being Irritable, easily angered .................. 0 1 2 3 4
Feeling Depressed or Tearful .................... 0 1 2 3 4
Feeling Frustrated or Impatient ................ 0 1 2 3 4
Forgetfulness, poor memory ..................... 0 1 2 3 4
Poor Concentration .................................... 0 1 2 3 4
Taking Longer to Think .............................. 0 1 2 3 4
Blurred Vision ............................................. 0 1 2 3 4
Light Sensitivity,
Easily upset by bright light ................ 0 1 2 3 4
Double Vision ............................................. 0 1 2 3 4
Restlessness .............................................. 0 1 2 3 40 = Nil 1 = the same 2 = mild 3 = moderate 4 = severe

LEVIN ET AL 1987 J NEUROSURGERY, 66: 234 - 243.
“A single uncomplicated minor HI produces no permanent disabling
neurobehavioural impairment in the great majority of patients who are free of
pre-existing neuropsychiatric disorder and substance abuse.”
"A subacute disturbance of attention, memory, and information-processing
efficiency is common during the first few days after HI .... By 1-3 months
most patients recover to within the range of matched controls, but
neurobehavioural deficits occasionally persist for longer in a minority.
Subjective c/o's frequently occur at baseline and 1 and 3 months F-Up's, even in
patients with recovered cognitive functioning."

LISHMAN (1988)
• Organic factors are chiefly relevant in the earlier stages, whereas long-
continued symptoms are perpetuated by secondary neurotic developments,
often of a complex nature.
KING, 2003
• When PCS persists,
• Psychological features will entirely account for the symptoms in some
individuals.
• Organic or quasi-organic features will entirely account for the symptoms in
others.
MCCREA: MTBI AND PCS, 2008
Post Concussional Syndrome is a neuropsychological disorder associated with
the transient neurological effects of MTBI but maintained by a combination of
psychological and social factors in the overall majority of cases.

MTBI – RECOVERY BY 90 DAYS MCCREA ET AL 2003
Concussed vs Control Athletes
Resolution of:
• PCS 7/7
• Balance 3-5/7
• Cognition 5-7/7
• No difference between groups at 90/7. Acute disturbance, exponential
recovery rate

MTBI – PROLONGED RECOVERYMCCREA ET AL, 2013
•Prolonged recovery (>7 days) in 10% concussed athletes
•↑Initial LOC, PTA, acute symptoms
•Worse initial cognitive function

MODERATORS OF NEUROPSYCHOLOGICAL OUTCOME
Belanger et al (2005) Meta-analysis:
1463 MTBI pts & 1191 controls
• Effect size D = 0.54, moderate
• In unselected or prospective samples, no residual neuropsychological impairment by 90 days post-injury. (D= 0.04).
• In clinics and litigation samples, greater cognitive sequelae at 3 months (D= 0.74)
• Sampling methods important

PERSISTENT PCS, MTBI AND META-ANALYSIS
Iverson (2010): Meta-analysis should not be used to unequivocally state that
MTBI cannot cause long term problems in a minority.

PCS: DOES IT EXIST?
• Not in DSM-5
• ? Not in ICD-11
• Meares, 2011: Acute PCS not specific to mTBI
(mTBI 43.3%; orthopaedic controls 43.5%).
• High base rates in general population (Powell, 2008)
• High rates in non-concussed school athletes (Iverson, 2015).

POST CONCUSSIONAL SYNDROME
• Commoner in women than men
• Pre-injury mental health problems a major risk factor
• Influenced by traumatic stress
• Persistent Sx at 1 or 3 months predict persistent Sx at 1 year
• Easy to misdiagnose in those with depression, anxiety, PTSD, chronic pain

PCS can be mimicked, magnified or masked by:
• Traumatic stress
• Anxiety
• Depression
• PTSD
• Chronic pain
• Sleep disturbance
• Social psychological factors at any point during recovery

PCS may be mimicked, magnified or masked by:
• Concussion
• TBI
• Vestibular damage
• Scalp, skull injury
• Headache

SYSTEMATIC REVIEW OF SELF-REPORTED PROGNOSIS IN ADULTS AFTER MTBI: RESULTS OF THE INTERNATIONAL COLLABORATION ON MILD TBI PROGNOSIS CASSIDY ET AL, 2014
•The term postconcussion syndrome should be replaced with
posttraumatic symptoms because they are common to all
injuries

MISDIAGNOSIS OF THE PERSISTENT PCS IN DEPRESSION
C. 90% of people with depression, with no prior head trauma,
meet symptom criteria for a mild or greater form of ICD-10 PCS
Iverson Archives of Clinical Psychology 21 (2006) 303-310

MISDIAGNOSIS OF THE PERSISTENT PCS IN PTSD
• Persistent “PCS” at 3 months after MTBI are not specific enough to be
identified as a unique PCS and should be considered part of the hyperarousal
dimension of PTSD
• MTBI predicted PTSD but not PCS
Lagarde et al, 2014

PREDICTORS OF SUSTAINING A HEAD INJURY?COMPARED WITH AGE & SEX MATCHED CONTROLS
• Presence or risk of psychiatric disorder
• ADHD Adeyemo 2014, Biedermann, 2015
• Alcohol abuse
• Previous head injury

PREDICTORS OF SUSTAINING AN MTBI
• Employment status - 57% of the Glasgow mTBI
unemployed at time of injury
• Life Events - those with mTBI had twice as many life
events in the year before injury as controls
• BDNF genotype met/met homozygous
Thornhill at al. BMJ 2000; Fenton et al 1993 BJPsych; Dretsch et al Brain Behav 2016

PREDICTORS OF OUTCOME OF MTBI
WHITE MATTER, COGNITION, MTBI
• 53 pts with MTBI (GCS13-15) vs Controls
• 6 days 1 year
• ↑FA ↓FA
• ↓VF VF normal
• ↓VF ∝ ↑ FA in CC in left hemisphere
• ↑FA = astrogliosis & axonal neurofilament compaction
• ↓FA = myelin sheath damage
Croall et al, 2014

REVIEW OF 50 DTI STUDIES IN MTBI(Wäljas et al, 2014)
Findings Yes No Not Reported
Abnormal White Matter 88% 12% ---
Correlated With:
Return to Work 0% 2% 98%
Post-Concussion Symptoms 12% 6% 82%
Cognitive Functioning 54% 8% 38%
Mental Health Problems 6% 8% 86%

DTI & PCS AFTER MTBI: SYSTEMATIC REVIEW TO MAY 2016
• ↓Fractional Anisotropy, ↑mean and radial diffusivity associated
with
• Development of PCS
• Severity of PCS
• Corpus callosum vulnerable
Khong et al, 2016 (10 studies)

23 patients with mTBI vs 18 age matched healthy
controls
↓ Connectivity posteriorly correl w. impaired
cognition
↑ Connectivity anteriorly correl w. post traumatic sx
Zhou et al Radiology, 2012, 265, 882-892.
PREDICTORS OF OUTCOME AFTER TBI:CONNECTIVITY – DEFAULT MODE NETWORK

DTI FOR OUTCOME PREDICTION IN MTBI: A TRACK-TBI STUDY
•Predictors of 6 month outcome (GOS-E, RPQ-13)
Severely reduced FA OR 3
Neuropsychiatric history OR 4
Years education OR 3
MRI surpassed all other predictors for 3- and 6-month outcome
prediction in those with no h/o psych or substance abuse.
Yuh et al 2014

CHALLENGES OF DTI
• To identify Traumatic Axonal Injury in an individual
• Specificity
• Clinical significance
• Relationship to
• Cognition and behaviour
• Outcome

WHITE MATTER ABNORMALITIES FOUND IN:
• Depression
• ADHD
• Dyslexia and LD
• Adolescent substance misuse
• Hypertension
• Cigarette smokers
• Obesity and metabolic syndrome
• Some healthy controls

MORE INTELLIGENT MEN SHOWED HIGHER FA IN THE GENU AND BODY OF THE CORPUS CALLOSUM DUNST ET AL, 2014
NOT ALL DTI STUDIES ARE POSITIVE

PROSPECTIVE BIOPSYCHOSOCIAL STUDY OF PERSISTENT PCS FOLLOWING
MTBI (WALJAS ET AL, 2015, J. NEUROTRAUMA)
• Sample not involved in litigation
• N = 126, Control Group
• DTI, cognitive testing and questionnaires at 1 month
and 1 year post-injury
• DTI abnormalities in 50% of the sample (12% of
controls)

WALJAS ET AL, 2015
• Abnormalities on DTI and MRI NOT sig. assoc. with greater PCS
• Abnormalities on DTI and MRI NOT sig. assoc. with worse neuropsychology
• Prior mental health problems & extra-cranial injuries predict PCS at 1 month
• PCS at 1 month predict PCS at 1 year
• Depression predicts PCS at 1 month & 1 year.

PERSISTENT SYMPTOMS AFTER MTBICOHORT OF TATOR
• 221 patients referred 1997 to 2013 to
neurosurgeon
• majority (2/3) sports injuries
•many with 3 or more concussions
• many with chronic PCS
Tator et al. 2011; 2016; Hiploylee et al. 2017

TATOR ET AL
• Follow –up (55% response rate)
• Excluded contusions, haemorrhages, TOMM +ve cases, litigants
• None recovered who had PCS> 3 years
• Best predictor of recovery = number of PCS

A BIO-PSYCHOSOCIAL CONCEPTUALISATION OF OUTCOME FROM mTBI (IVERSON, 2011)
IVERSON IS THE LEAD AUTHOR

BIO-PSYCHOSOCIAL CONCEPTUALISATION OF OUTCOME: THE BELFAST STUDIES OF MILD AND MODERATE TBI
FENTON, MCCLELLAND, MONTGOMERY, MACFLYNN, RUTHERFORD

BELFAST STUDIES OF MILD AND MODERATE TBI G FENTON, R MCCLELLAND, A MONTGOMERY, G MACFLYNN, W RUTHERFORD
Post Concussional Symptoms (PCS)
Time 0 6 weeks 6months
44% 42% 54%

PATTERNS OF RECOVERY AND BRAINSTEM DYSFUNCTION IN MILD HI(MONTGOMERY ET AL, 1991)
ABNORMAL BAEPs
1. ACUTE GROUP - 52% Day 0 6 weeks
Recovery within
6 weeks 54% 6%
2. CHRONIC GROUP - 16%
Symptoms persist over
6 months 100% 100%
3. SYMPTOM EXACERBATION GROUP - 32%
Symptoms from
6 weeks to 6 months 12.5% 0%
BAEP = Brainstem auditory evoked potential

MEDICO LEGAL ASPECTS
ASSESSMENT OF PTA
EFFORT TESTS
THE GCS 15 SEVERE TBI OR SUBTLE BRAIN DAMAGE

DEFINITION OF PTA
• Disorder of episodic memory
• Other abnormalities:
- confusion
- disorientation
- agitation
- semantic errors
- impaired backward digit span
- ↓verbal fluency
- Slowed RT
Wilson et al, 1992; Ahmed et al 2000; Marshman et al, 2013
VALIDITY OF PTA 1: NAN RECOMMENDATIONS. RUFF ET AL, 2009
• PTA vs LOC
• Recall vs reconstruction
• PTA vs Psychogenic amnesia
• Alcohol/drug intoxication
• Severe physical injury + pain bias recall
• Opiates and benzodiazepines
• Timeline of events eg sleep
• Late onset amnesia is not PTA
VALIDITY OF PTA 2:
• Definite vs patchy gaps
• Course of islands of memory
• Specific vs general memories
• Abruptness of ending
• Learned responses in repeated testing (Friedland &
Swash, 2016)

VALIDITY OF PTA 3: KEMP ET AL, 2010
• 38% of orthopaedic and non-head injured patients report
“PTA” >24 hours (Rivermead Protocol)
• Risk factors: Opioids, surgery, anxiety (57.5% variance)
• ≥ I predictive factor required for apparent “PTA”
• Mimicked PTA = 4 – 96hrs

VALIDITY OF PTA 4:
• PTA major estimator of severity “but it should not necessarily be the sole
determining factor”
• “The validity of PTA as the sole measure of severity of TBI has never been
objectively tested”
King et al, 1996; Friedland & Swash, 2016
PTA – IS RETROSPECTIVE ASSESSMENT RELIABLE? - 1
Severe TBI
• Good correlation retro and prospectively (GOAT 0.87) 3.5 – 6 years later
• Mean pro-PTA = 34 days (2-185)
• Mean retro-PTA = 39 days (1-244)
McMillan et al, 1996

PTA – IS RETROSPECTIVE ASSESSMENT RELIABLE? -2
Minor TBI
• Good correlation retro and pro in 75% at 1-3 months
• 1st and 2nd retrospective PTAs differ in 11%
• Discrepancies are longer PTAs
Gronwall & Wrightson (1980)

PTA – IS RETROSPECTIVE ASSESSMENT RELIABLE? - 3
• Inter-rater reliability = 0.79, but lower (0.59) for PTA < 24
hours or for long delay btw assessments (0.64) (King et al,
1997)
• After 5 years, retrospective PTA unreliable (does not correl with
cognitive deficits. Ashla et al, 2009)

UNDER-ESTIMATION OF PTA
• Islands of memory
• Confabulation
• False memories
• Reconstruction of events from accounts by others

BASE RATE OF FAILED EFFORT IN THE MEDICO-LEGAL CONTEXT
• Mittenberg et al: Survey of 388 members of the
American Board of Clinical Neuropsychologists, 2002.
• 29% of personal injury claims (n=6371) thought to have
probable malingering.

BASE RATE OF FAILED EFFORT IN THE MEDICO-LEGAL CONTEXT: ESTIMATES OF MALINGERING
• mTBI 40% (range 15-64%).
• chronic pain 31%
• fibromyalgia/chronic fatigue 35%
• moderate-severe TBI 26%
• neurotoxic exposure 26%
• electrical injury 22%
Mittenberg et al, 2002; Larrabee, 2003.

MEASUREMENT OF EFFORT
• Stand alone tests – WMT, TOMM
• Embedded measures

GREEN ET AL, 2001
•Effort has a greater effect on test scores than
severe brain injury in compensation claimants

THE CONCEPT OF THE GCS 15 SEVERE TBI HAS BEEN PROMOTED IN THE MEDICO-LEGAL CONTEXT
• DAI found in mild TBI
- Neuropathology, biomarkers & SWMRI
• LOC & GCS poor guides to DAI
• PTA > 24 hrs & presence of “chronic symptoms” of DAI
prove “severe” TBI = DAI = permanent symptoms and disability