
Midwife brief intervention mandatory training Somerset M2Bs
27
Smoking in pregnancy • A positive approach Tracey Hellyar January 2017 Version 7
-
Upload
tracey-hellyar -
Category
Healthcare
-
view
19 -
download
2
Transcript of Midwife brief intervention mandatory training Somerset M2Bs

Smoking in pregnancy• A positive approach
Tracey Hellyar January 2017Version 7

Learning Outcomes • Smoking: the risks and pregnancy• Why smokers continue when
pregnant• Barriers to offering advice• Raising the subject• Reducing resistance• How to access support

The greatest cause of premature death
• Smoking is accountable for 100,000 premature deaths in the UK annually• Smoking harms nearly every organ in the body• Smoking causes lung cancer, respiratory disease and heart disease as well as
numerous cancers in other organs including lip, mouth, throat, bladder, kidney, stomach, liver and cervix
• About half of all lifelong smokers will die prematurely, losing on average about 10 years of life
• Smoking kills more people each year than the following preventable causes of death combined
Smoking Obesity RTA Illegal drugs HIV0
20000
40000
60000
80000
100000
120000100000
34100
1775 1605 530

Saving babies lives care bundle
• In November 2015, Secretary of State for Health announced a new ambition to reduce the rate of stillbirths by 50 per cent in England by 2030, with a 20 per cent reduction by 2020
1. Reducing Smoking in Pregnancy 2. Detecting Fetal Growth Restriction 3. Raising awareness of Reduced Fetal Movement 4. Improving Effective Fetal Monitoring during labour

UK position compared to other high income countries

Element 1
Element • Reducing smoking in pregnancy by carrying out Carbon Monoxide (CO)
test at antenatal booking appointment to identify smokers (or those exposed to tobacco smoke) and referring to stop smoking service/specialist as appropriate
Intervention • Carbon monoxide (CO) testing of all pregnant women at antenatal
booking appointment and referral, as appropriate, to a stop smoking service/specialist, based on an opt out system. Referral pathway must include feedback and follow up processes

Smoking At Time Of Delivery: Our goal
6% By the end of 2020
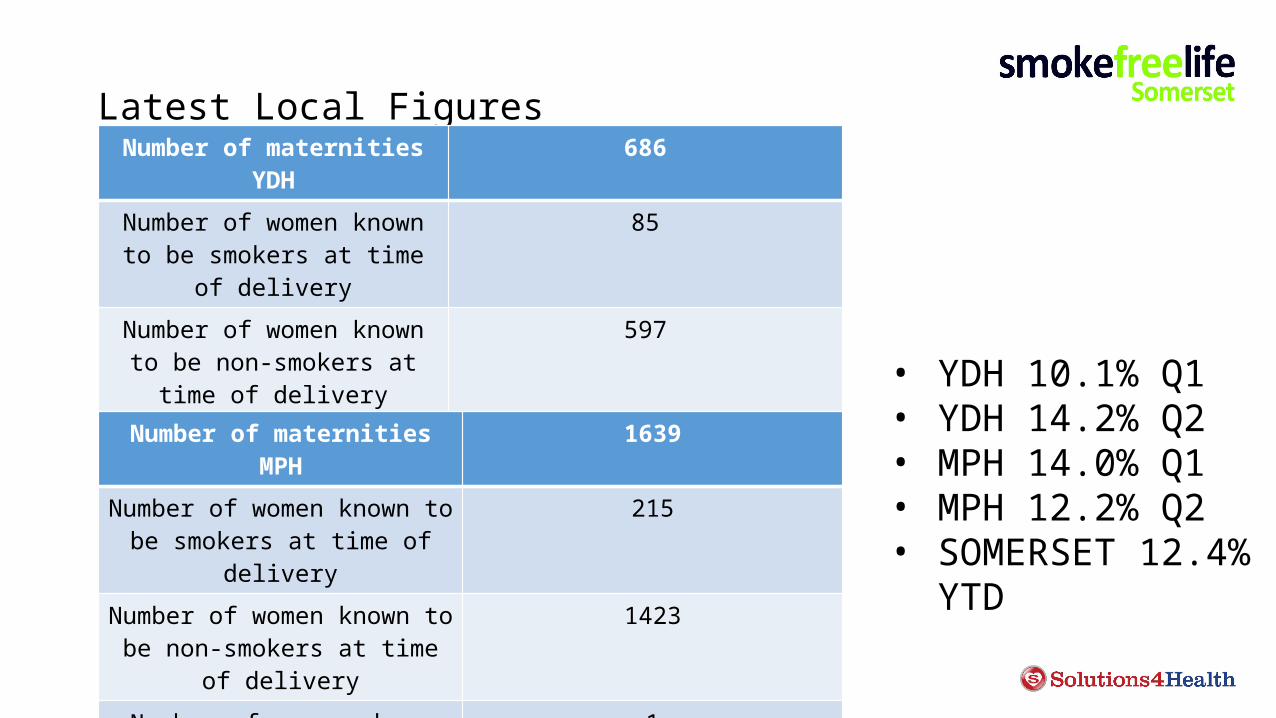
Latest Local FiguresNumber of maternities YDH 686
Number of women known to be smokers at time of delivery
85
Number of women known to be non-smokers at time of delivery
597
Number of women whose smoking status was unknown at
time of delivery
4
Number of maternities MPH 1639
Number of women known to be smokers at time of delivery
215
Number of women known to be non-smokers at time of delivery
1423
Number of women whose smoking status was unknown at time of
delivery
1
• YDH 10.1% Q1• YDH 14.2% Q2• MPH 14.0% Q1• MPH 12.2% Q2• SOMERSET 12.4%
YTD
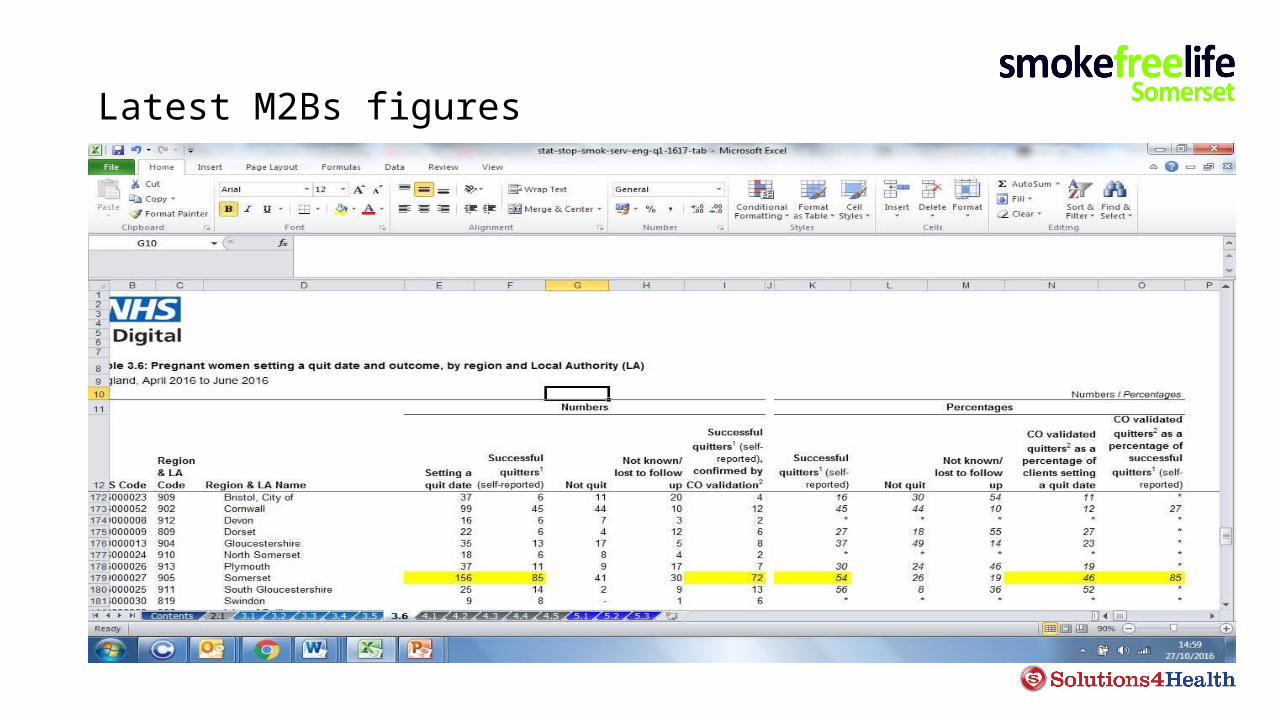
Latest M2Bs figures

Latest M2Bs figures

Activity One
• What are the risks associated with smoking in pregnancy?
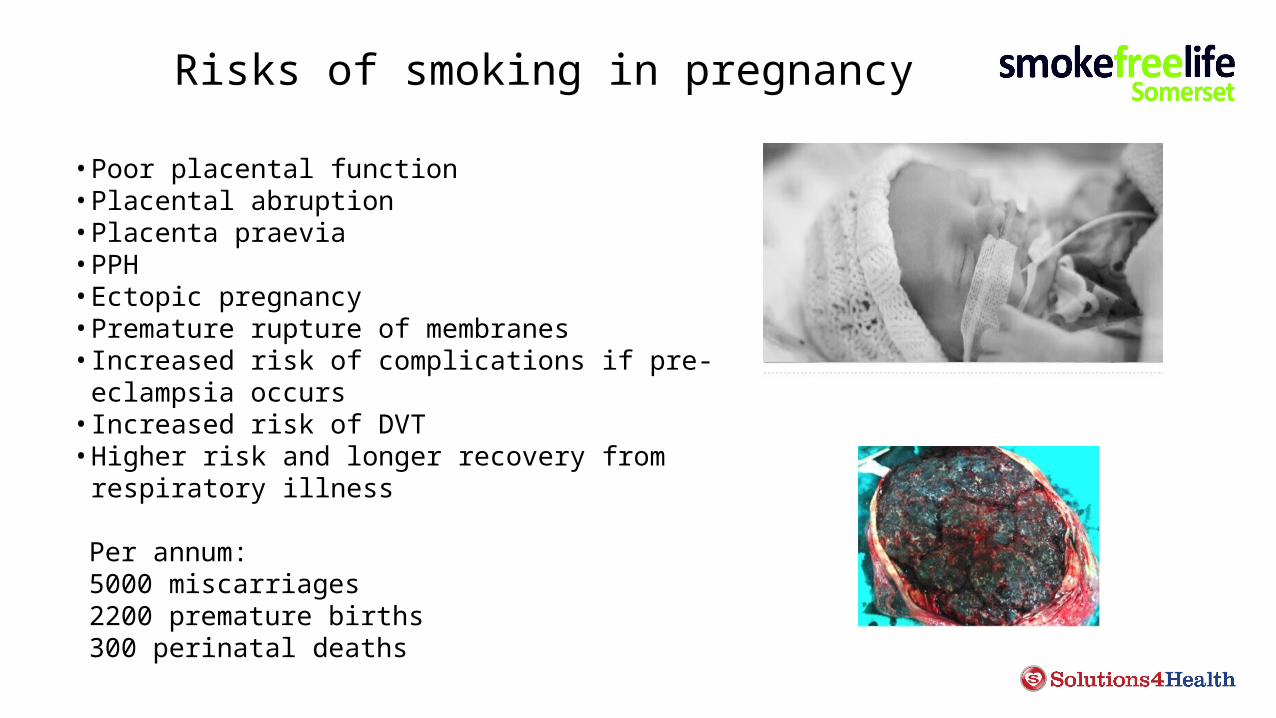
Risks of smoking in pregnancy
• Poor placental function• Placental abruption• Placenta praevia• PPH• Ectopic pregnancy• Premature rupture of membranes• Increased risk of complications if pre-eclampsia occurs• Increased risk of DVT• Higher risk and longer recovery from respiratory illness
Per annum: 5000 miscarriages 2200 premature births 300 perinatal deaths

Effects of smoking on baby & child
• Increased childhood illness• Prematurity/IUGR• Childhood diabetes• Obesity• Stunts growth• Impaired lung function/respiratory disease• Earlier menopause• Slows fetal breathing at delivery• Increases fetal HR in utero• Reduces fetal oxygen• Transmits carcinogens• Damages fetal development through
transmission of heavy metals• Nicotine withdrawal• ADHD, behavioural problems, learning
difficulties, speech and language problems, reduced educational performance
• Asthma• Cot death• Middle ear infections

Good news
• Benefits both mother and your baby immediately• Less morning sickness and fewer complications in
pregnancy • More likely to have a healthier pregnancy and a healthier
baby• Reduce the risk of stillbirth • Baby is less likely to be born too early and have to face the
additional breathing, feeding and health problems that often go with being premature
• Baby is less likely to be born underweight• Reduces the risk of sudden infant death• Less likely to suffer from Asthma and other more serious
illnesses that require hospital treatment
What are the barriers for the women
Guilt
Fear
Concern for the baby
People nagging
Low self esteem
Mixed messages
Don’t understand the risks
Nicotine addiction
Stress
Habit
Partner smokes
Normal
So how do we raise the issue?
• Remember that most smokers expect to be asked about their smoking
• Research shows that pregnant women want convincing evidence of the risks and to be given practical advice on how to stop
When to ask the question
Booking (plus CO screening) and each A/N
apptIntrapartum Each P/N contact
Midwives responsibilities Identify Refer Accurately document
SATOD
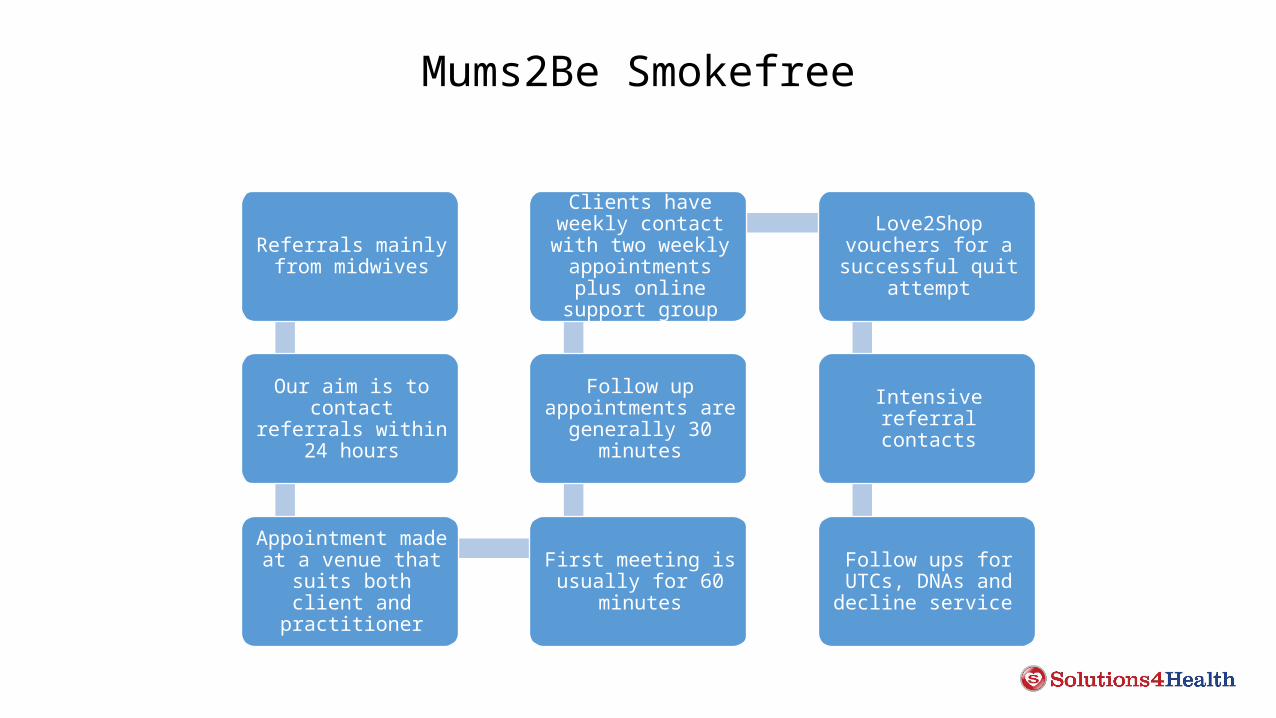
Mums2Be Smokefree
Referrals mainly from midwives
Our aim is to contact referrals within 24
hours
Appointment made at a venue that suits
both client and practitioner
First meeting is usually for 60
minutes
Follow up appointments are
generally 30 minutes
Clients have weekly contact with two
weekly appointments plus online support
group
Love2Shop vouchers for a successful quit
attempt
Intensive referral contacts
Follow ups for UTCs, DNAs and decline
service
Mums2Be Smokefree 2015/2016
• 423 Quit dates set• 232 Quit at 4 weeks• 161 Quit at time of delivery

YDH pregnancy stop smoking voucher incentive scheme study 2013
Data was collected on all YDH maternity referrals (416) to the stop smoking service fromJuly 2009 until October 2012.
114 women engaged with the service and 302 did not (Opt In Scheme)
Birth weight (grams) of babies born to women delivering at YDH July 2009 – Oct 2012 who smoked at booking.

Why is cutting down of no benefit• Often this is in response to nagging• It exonerates from further effort• The smoker will compensatory smoke• Consumption can rise at any time• In practice women cheat on themselves and make
insignificant reduction
Women should always be encouraged to quit

E-Cigs and Vapes
E-cigarettes as a harm reduction strategy
• in contrast to ‘reduced risk’ cigarettes no combustion takes place in e-cigarettes
• in contrast to smokeless tobacco, e-cigarettes are not tobacco products
• they contain nicotine and flavourings which can be toxicants, but toxicants present are at much lower levels than in tobacco
• all the evidence suggests e-cigarettes are safer than tobacco cigarettes


Advising on e-cig use
• Tell people that some nicotine products are not regulated by the MHRA and therefore their effectiveness, quality and safety cannot be assured. Also advise them that these products are likely to be less harmful than cigarettes
• PHE and Health Scotland agree that cessation services can offer behavioural support to those using e-cigs in a quit attempt
• NCSCT recommend 1. be open to e-cig use 2. provide advice and support 3. be positive about e-cigs


Nicotine replacement therapy
Direct supply from Smokefreelife SomersetPharmacotherapy on wards to compliment
smoke free site

We make a difference

References
• Blooming Health 2009 Smoking and your baby www.bloominghealth.co.uk
• Department of Health (1998) Smoking Kills https://www.gov.uk/government/publications/a-white-paper-on-tobacco
• NICE PH26 http://www.nice.org.uk/guidance/PH26
• ASH Smoking in Pregnancy a call to action http://www.ash.org.uk/files/documents/ASH_893.pdf
• ASH smoking and reproduction http://www.ash.org.uk/files/documents/ASH_112.pdf
• Miller and Rollnick 1991 http://www.motivationalinterview.net/clinical/whatismi.html
• Department of Health Stop Smoking Services monitoring and guidance 2011/2012 https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/213755/dh_125939.pdf
• NCSCT http://www.ncsct.co.uk/ Very brief advice on smoking for pregnant women
• NMC http://www.ilearn.rcm.org.uk/ I Learn Very brief advice on smoking for pregnant women
• Saving Babies Lives Care Bundle https://www.england.nhs.uk/wp-content/uploads/2016/03/saving-babies-lives-car-bundl.pdf
• https://www.tommys.org/pregnancy-information/i%E2%80%99m-pregnant/smoking-and-pregnancy/what-happens-when-pregnant-woman-smokes


















