Microcirculation of the Islets of Langerhans Long Beach Veterans
8
-- Perspectives in Diabetes Microcirculation of the Islets of Langerhans Long Beach Veterans Administration Regional Medical Education Center Symposium F. Charles Brunicardi, John Stagner, Susan Bonner-Weir, Harold Wayland, Robert Kleinman, Edward Livingston, Paul Guth, Michael Menger, Robert McCuskey, Marcos Intaglietta, Arthur Charles, Stanley Ashley, Anthony Cheung, Eli Ipp, Stewart Gilman, Thomas Howard, and Edward Passaro, Jr. three models of islet n~icrocirculation discussed at thr symposiunl. T o discuss the controversy of the current concept of islet microcirculation, an international symposium was held at the Long Beach Veterans Administra- tion Regional Medical Education Center (Long Beach, C:A) and broadcast over the Internet via the world Wide Web to 14 international stations. Studies concerning three models of islet microcirculation, mantle-to-core, core- to-mantle, and polar, were presented. One presentation, including an interactive question and answer session, was broadcast from the Massachusetts Institute of Technology (Cambridge, MA) and received by the symposium partici- pants in Long Beach, as well as by the 14 stations. The fundamental differences between the models, i.e., the rela- tionship of the microcirculation flow pattern and the islet cell composition, were discussed in an open forum with critiques of techniques, results, and interpretations. Each islet has from one to five arterioles, which penetrate into the islet and divide into numerous capillaries (1-4). The capillaries, resembling a glomerulus, course through the islet in a tortuous fashion that is ideal for cell-blood and blood- cell interactions. The a-, p-, 6-, and PP-cells, which secrete glucagon, insulin, somatostatin, and pancreatic polypeptide, respectively, are nestled between the capillaries and receive their nutrient, hormonal, and neurohormonal regulatory sig- nals across the capillary endothelium, as well as through the interstitial space (5,6). Since the cell types have specific locations within the islet, the pattern of blood flow through the islet should have a significant impact on the ability of cells to intercommunicate within the islet. It is this relation- ship that represents the controversial topic that was the focus of the symposium. The following is a review of the From the Dsepartment of SurgeIy, Veterans Administration Medical Center-West Los Angeles, Los Angeles, California Address correspondence and reprint requests to Dr. F. Charles Brunicardi, Department of SurgeIy, Baylor College of Medicine, One Baylor Plaza, Houston, TX 77030. Received for publication 6 November 1995 and accepted in revised form 22 December 1'995. FITC, fluorescein isothiocyanate; SAb, somatostatin n~onoclonal antibody; SFab, somatostatir~ Fab fragment antibody. MODEL ONE Model one represents primarily the combined works of Fyjita, Ohtani, Nagata, Nishino, and Murakami and was presented by Wayland and Kleinman at the symposium. Model one describes a pattern of microcirculation in which non-p-cells are perfused before p-cells (Fig. 1). In this model, the secretory products of the non-p-cells, (glucagon, somato- statin, and pancreatic polypeptide) would have a regulatory effect on the p-cell secretion (insulin). Insulin, in turn would be secreted from the islet without aifecting the secretions of the other cell types. The studies evaluated the islet microcir- culation of numerous species, including rat, mouse, rabbit, guinea pig, cow, horse, monkey, and human, using a combi- nation of scanning electron microscopy of corrosion vascu- lar casts, light microscopy with india ink idections, histochemical staining of islet cell types, as well as in vivo microscopy using intravital stains. The studies demonstrate differing patterns of microvascular flow that are species- dependent (1,7-16). Despite the differences in patterns, the non-p-cells would be perfused before the p-cells in all species in model one. In anatomic studies of mouse, rat, and rabbit pancreases using scanning electron microscopy-corrosion cast images, the islet vasculature was found to consist of a two-layered meshwork of fine capillaries with an outer superficial plexus (mantle) surrounding an inner deep plexus (core) (1,7,8). One to five feeding arterioles lead to the outer superficial plexus; this plexus courses in a tortuous fashion resembling a glomerulus and then communicates with the inner deep plexus of the core. These capillaries then coalesce into the efferent plexus, which exits from the core of the islet. Each islet has from one to six exiting venules, which empty into the veins of the pancreas. Another group of vessels that are the size of capillaries exit the islet and drain to the acijacent exocrine tissue, known as the insulo-acinar portal system (1,4,7,17-20). An islet can have from 1 to 30 of these vessels, the number of which appears to be dependent on the size and location of the islet (7,8,17). The extralobular islets have fewer insulo-acinar vessels; their secretory products drain DIABETES, VOL. 45, APRIL 1996
Transcript of Microcirculation of the Islets of Langerhans Long Beach Veterans

--
Perspectives in Diabetes Microcirculation of the Islets of Langerhans Long Beach Veterans Administration Regional Medical Education Center Symposium F. Charles Brunicardi, John Stagner, Susan Bonner-Weir, Harold Wayland, Robert Kleinman, Edward Livingston, Paul Guth, Michael Menger, Robert McCuskey, Marcos Intaglietta, Arthur Charles, Stanley Ashley, Anthony Cheung, Eli Ipp, Stewart Gilman, Thomas Howard, and Edward Passaro, Jr.
three models of islet n~icrocirculation discussed at thr symposiunl.
T o discuss the controversy of the current concept of islet microcirculation, an international symposium was held at the Long Beach Veterans Administra- tion Regional Medical Education Center (Long
Beach, C:A) and broadcast over the Internet via the world Wide Web to 14 international stations. Studies concerning three models of islet microcirculation, mantle-to-core, core- to-mantle, and polar, were presented. One presentation, including an interactive question and answer session, was broadcast from the Massachusetts Institute of Technology (Cambridge, MA) and received by the symposium partici- pants in Long Beach, as well as by the 14 stations. The fundamental differences between the models, i.e., the rela- tionship of the microcirculation flow pattern and the islet cell composition, were discussed in an open forum with critiques of techniques, results, and interpretations.
Each islet has from one to five arterioles, which penetrate into the islet and divide into numerous capillaries (1-4). The capillaries, resembling a glomerulus, course through the islet in a tortuous fashion that is ideal for cell-blood and blood- cell interactions. The a-, p-, 6-, and PP-cells, which secrete glucagon, insulin, somatostatin, and pancreatic polypeptide, respectively, are nestled between the capillaries and receive their nutrient, hormonal, and neurohormonal regulatory sig- nals across the capillary endothelium, as well as through the interstitial space (5,6). Since the cell types have specific locations within the islet, the pattern of blood flow through the islet should have a significant impact on the ability of cells to intercommunicate within the islet. It is this relation- ship that represents the controversial topic that was the focus of the symposium. The following is a review of the
From the Dsepartment of SurgeIy, Veterans Administration Medical Center-West Los Angeles, Los Angeles, California
Address correspondence and reprint requests to Dr. F. Charles Brunicardi, Department of SurgeIy, Baylor College of Medicine, One Baylor Plaza, Houston, TX 77030.
Received for publication 6 November 1995 and accepted in revised form 22 December 1'995.
FITC, fluorescein isothiocyanate; SAb, somatostatin n~onoclonal antibody; SFab, somatostatir~ Fab fragment antibody.
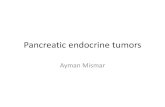
MODEL ONE Model one represents primarily the combined works of Fyjita, Ohtani, Nagata, Nishino, and Murakami and was presented by Wayland and Kleinman at the symposium. Model one describes a pattern of microcirculation in which non-p-cells are perfused before p-cells (Fig. 1). In this model, the secretory products of the non-p-cells, (glucagon, somato- statin, and pancreatic polypeptide) would have a regulatory effect on the p-cell secretion (insulin). Insulin, in turn would be secreted from the islet without aifecting the secretions of the other cell types. The studies evaluated the islet microcir- culation of numerous species, including rat, mouse, rabbit, guinea pig, cow, horse, monkey, and human, using a combi- nation of scanning electron microscopy of corrosion vascu- lar casts, light microscopy with india ink idections, histochemical staining of islet cell types, as well as in vivo microscopy using intravital stains. The studies demonstrate differing patterns of microvascular flow that are species- dependent (1,7-16). Despite the differences in patterns, the non-p-cells would be perfused before the p-cells in all species in model one.
In anatomic studies of mouse, rat, and rabbit pancreases using scanning electron microscopy-corrosion cast images, the islet vasculature was found to consist of a two-layered meshwork of fine capillaries with an outer superficial plexus (mantle) surrounding an inner deep plexus (core) (1,7,8). One to five feeding arterioles lead to the outer superficial plexus; this plexus courses in a tortuous fashion resembling a glomerulus and then communicates with the inner deep plexus of the core. These capillaries then coalesce into the efferent plexus, which exits from the core of the islet. Each islet has from one to six exiting venules, which empty into the veins of the pancreas. Another group of vessels that are the size of capillaries exit the islet and drain to the acijacent exocrine tissue, known as the insulo-acinar portal system (1,4,7,17-20). An islet can have from 1 to 30 of these vessels, the number of which appears to be dependent on the size and location of the islet (7,8,17). The extralobular islets have fewer insulo-acinar vessels; their secretory products drain
DIABETES, VOL. 45, APRIL 1996

Mantle
FIG. 1. Model one. In the depicted islet of mouse, rat, and rabbit, the afferent plexus divides in the mantle and perfuses the a-, 6-, and PP-cells first. Flow then enters into the deep plexus of the core to perfuse the p-cells. Thus, flow is from mantle to core, with the a-, 6-, and PP-cells perfused before the p-cells. The efferent plexus emanates from the core. In the monkey and horse islet, the afferent plexus enters into the core and first perfuses the a-, S-, and PP-cells, which are located in the core. Flow then enters into the mantle to perfuse the p-cells. Thus, Row is from core to mantle, with the a-, 6-, and PP-cells perfused before the p-cells. The efferent plexus emanates from the mantle. Other species (dog, guinea pig, pig, cow, human) show a mixed pattern; the afferent plexus enters the mantle and/or the core of islets. Since the a- and &-cells are scattered throughout the islet, it is possible that the a- and 6-cells are perfused before the p-cells in these species.
mostly into the venules of the pancreas and proceed directly to the liver. The intralobular islets have a greater number of these vessels; therefore, their secretory products drain mostly to the acinar cells before emptying into the venules of the pancreas.
Studies using ink-perfused islets and in vivo microscopy support the concept of mantle-to-core flow in the rat islet. The superficial outer plexus of the mantle was perfused first (9). The flow of ink was seen to leave the mantle and then enter into the deep plexus of the core; from the deep plexus, the flow exited the islet through the efferent plexus emanat- ing from the core. To relate the microvascular flow pattern to islet cell composition, stainings of islets were performed. In the mouse, rat, and rabbit islets, the non-p-cells were located in the mantle and the p-cells were located in the core (1,2 1-23).
These studies support the concept of mantle-to-core islet blood flow in the rat, mouse, and rabbit. The location of the islet cells suggests that the a-, 6-, and PP-cells would be perfused before the p-cells, since the mantle is perfused before the core, therefore suggesting that glucagon, somato- statin, and pancreatic polypeptide would have an intra-islet regulatory effect on insulin secretion. In turn, insulin would be secreted from the islet without affecting the secretions of the other cell types.
However, important species-specific differences in islet microvasculature and location of islet cell types were found. In islets of larger species (dog, cow, horse, pig, monkey, and human), mixed patterns of islet microvasculature were ob- served (1,13). In the scanning electron microscopy-corro- sion cast studies of the monkey and the horse, the afferent plexus entered into the core of the islet, whereas the efferent plexus emanated from the mantle. In the staining studies, the islets of the horse and the monkey had the non-p-cells located within the core and the p-cells in the mantle (1,13,14). In contrast to those in the rat islet, these findings suggest a core-to-mantle direction of flow. Nevertheless,
since the locations of the non-p-cells and p-cells were reversed, these findings imply that the a-, 6-, and PP-cells are perfused before the p-cells in the monkey and the horse; thus, the pattern of flow from the non-(3-cells to the p-cells seen in rat, mouse, and rabbit islets is preserved.
The other species studied (dog, guinea pig, pig, cow, human) were found to have a mixed pattern of microvascu- lature. Scanning electron microscopy-corrosion cast studies of islets from these species demonstrated that the afferent plexus enters both the core and the mantle of the islet. In the staining studies of islets in these species, the islets consisted of a mixture of cell types, with a- and &-cells scattered throughout the islet (1,24,25). It is difficult to draw conclu- sions on the order of cellular perfusion from these studies; however, the authors concluded that the studies do not exclude the possibility in these species that the a- and &-cells are perfused before the p-cells. It was suggested at the symposium that the differences could be related to sampling of different islets from the pancreases of these species.
Thus, this block of studies demonstrates that the structure of islet microvasculature is species-dependent. In mouse, rat, and rabbit islets, the pattern of microcirculation is from mantle to core. In the monkey and the horse, the pattern of microcirculation is from core to mantle. In cattle, pigs, dogs, cats, guinea pigs, and humans, the pattern of microcircula- tion is variable. The authors conclude that the order of cell type perfusion remains consistent across species-lines and hypothesize that non-p-cells are perfused before p-cells. Model one supports the ability of glucagon, somatostatin, and pancreatic polypeptide to exert a regulatory effect on insulin secretion within the islet. Because the p-cells are perfused last, insulin would have no intra-islet effect on the a, 6-, and PP-cells in this model. These studies emphasize that species differences must be taken into account in evaluating the pattern of islet microcirculation.
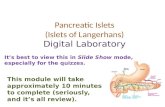
MODEL TWO Model two represents the combined works of Bomer-Weir, Stagner, Samols, Orci, and Menger and was presented by Bonner-Weir, Stagner, and Menger at the symposium. Model two describes a pattern of microcirculation in which the p-cells are perfused before the non-p-cells, such that insulin exerts a regulatory effect upon glucagon and somatostatin secretion within the islet (Fig. 2). This model is based on morphological and physiological studies.
The microvascular system of the islet has been defined by correlating scanning electron microscopic analysis of methac- rylate corrosion casts of the pancreatic blood vessels and reconstructions from serial sections of immunostained, india ink-infused rat islets (3,17). The islets of most mammal'ian species have a mantle-core cellular pattern, but those of humans and other primates are somewhat more complex, with the human pancreas showing many different islet pro- files, including oval and cloverleaf patterns, causing contro- versy over their having a layered or mantle-core cellular arrangement (1,14,21,26-30). Nonetheless, in three dimen- sions, human islets can be considered as composites of several mantle-core cellular structures or subunits or as being lobulated with mantle-core lobules. On examination of sectioned tissue, incomplete fusion of such subunits, com- bined with the penetration of the islet vasculature, can appear as invaginations of the islet periphery toward the islet
DIABETES, VOL. 45, APRIL 1996

FIG. 2. Model two. In this model, a core-to-mantle pattern of islet microcirculation with p-to-a-to-S order of cell perfusion is described. The afferent arteriole penetrates into the core through a gap in the mantle; thus, arterial blood first reaches the p-cells in the core. Insulin and other p-cell secretory products (islet amyloid polypeptide, C-peptide, proinsulin) are carried from the core to the mantle, where they influence the secretions of a-, 6-, and PP-cells. Conversely, the secretory products of the mantle cella leave the islet without influencing the p-cell. Shown here diagrammatically is the organization of the lwger rat islet, in which the efferent capillaries coalesce into collecting venules within the islet capsule; UI small islets, the efferent capillaries extend iuto the exocrine tissue before coalescing, providing the basis of the insular-acinar portal system. From Bonner-Weir and Orci (3).
interior. Most of the non-p-cells are found along these invaginations and the periphery, thus maintaining a layered or mantle-and-core islet cellular arrangement. A new ad- vance, confocal microscopy, allows better appreciation of the three-dimensional organization of islet cells (24). With this technology, a-cells are seen as a sheet or a peel at the islet periphery and &cells are seen as more peripheral to the a-cells in the human but less peripheral than in the rat.
There are from one to three afferent arterioles supplying each islet, depending upon islet size. Each arteriole pene- trates the islet through discontinuities of the non-p-cell mantle and enters directly into the p-cell core, where it branches into a number of fenestrated capillaries (3,17). These capillaries follow a tortuous path first through the p-cell core and then through the non-p-cell mantle, which is one to three cells thick. Often the arteriolar vessels pass along the inside of the mantle before penetrating to the core. In large islets, efferent vessels coalesce into collecting (post- capillw) venules within the subcapsulak space of the islet, but in small islets, the efferent capillaries extend into the exocrine tissue for 50-100 pm before coalescing into col- lecting venules. The evidence is for a single continuous circulation through the islet. These studies provide physical evidence for a core-to-mantle direction of intra-islet blood flow and cellular interaction in which the p-cells are per- fused before the a-, €I-, and PP-cells. Recently, Menger, using intravital photomicroscopy on both in situ and transplanted hamster islets, has confirmed these findi~gs, adding another species to those in which a core-to-mantle microcirculation has been shown (31,32).
The above anatomic studies provided a model for the physiological testing of intra-islet blood flow and interaction. The majority of the studies of intra-islet cellular perfusion described in model two have been accomplished by the use of isolated perfused pancreases (33-38). This technique offers many advantages over in vivo models and is unique in that retrograde perfusion can be used to reverse the normal sequence of intra-islet cellular perfusion. In vitro perfusion models are removed from the influences of the extrapancre- atic autonomic nervous system and the fluctuations of the corporal hormonal and metabolic milieu. One may control the influx of nutrients, hormones, and other effectors to produce a standard controlled system in which one or more components may be added or subtracted in order to examine their effects upon islet hormone secretion. The control exercised by the in vitro perfused pancreas model provides a powerful method in which to examine intra-islet hormone interactions under strictly defined conditions in which the dynamics of cellular interactions may be tested.
To establish the relationship between the islet microvas- culature and the specific order of islet cellular perfusion and interaction as a regulatory mechanism, Stagner and Samols have performed rat, dog, monkey, and human pancreas perfusions with the infusion of arginine in high and low glucose concentrations and the anterograde and retrograde infusion of specific hormone antibodies (33-42). The logic underlying these studies was that if there were a preferred order of islet cellular vascular perfusion and interaction based on the microvascular sequence of perfusion, the reversal of the direction of perfusion would also reverse the order of islet cellular blood flow and interaction.
These studies using both anterograde and retrograde per- fusion of rat, dog, monkey, and human pancreas confirm the anatomic models proposed by Bonner-Weir and Menger. In each species tested, the anterograde infusion of anti-insulin gamma globulin resulted in a prompt increase in glucagon and insulin secretion (14-23). Rat and monkey pancreas produced larger increases of glucagon and somatostatin than did dog and human pancreas (3338). The retrograde perfu- sion of intra-insulin gamma globulin had no effect on gluca- gon or somatostatin secretion in any of the species tested. In experiments in which antiglucagon antibodies were infused anterogradely, there was no effect on the p-cell and insulin secretion; however, there was a decrease in somatostatin secretion. Retrograde perfusion of antiglucagon antibodies had no effect on somatostatin secretion, but resulted in a diminution of baseline insulin secretion. The anterograde infusion of antisomatostatin antibodies did not effect insulin or glucagon secretion. However, during retrograde perfusion there was a small increase in glucagon and insulin secretion in the presence of somatostatin antibodies. The majority of the a-cells are apparently perfused before the majority of the &cells (33-38), suggesting that the &cell is the last in line in the sequence of perfusion and is thus vascularly neutral in the islet. Because an increase in endogenous somatostatin during anterograde perfusion did not change insulin or glucagon secretion, it was concluded that the &cell has limited or no function within the islet as a direct p-cell regulator. These observations strongly indicate that the target for endogenous islet somatostatin is the adjacent exocrine tissue (33-38,42). The latter conclusion has been supported by recent studies using hormone binding, radio tracer infusion, and microdialysis (43-46).
DIABETES, VOL. 45, APRIL 1996

Although pancreatic and islet efferent capillaries are richly fenestrated, gamma globulin nlolecules are confined to the vascular space and cannot readily cross the unbroken vas- cular endothelial barrier (32,47-49). Therefore, one must conclude that all hormone or cellular interactions within the islet are determined by the microvascular system. These results, as well as those obtained from binding studies and antibody infusion studies, strongly argue against paracrine interactions as significant regulatory mechanisms within the islet (44-46). A measurable unequivocal intra-islet paracrine event has not been reported as of the date of this writing.
It is interesting and important that the sequence of islet cellular perfusion predicted by early arginine infusion stud- ies by Stagner and San~ols (40-41) was confinned by anti- body infusion studies. These early studies were not subject to the influences of antibodies, which nlay react with more than one hormone or perfusate component, such as bovine serum albumin, and were free of potential contan~inants from the dialysates often used to isolate or presenre antibod- ies, such as sodium azide, citrate, sulfate, acetate, or other divalent inorganic ions, all of which may effect islet hormone secretion (50; J.S., unpublished observations). In the anti- body infusion studies, all antibodies were hormone specific and free of any substances that could interfere with hormone binding or radioimmunoassays. All antibodies were rigor- ously tested for cross-reactivity with other islet hormones by both binding studies and charcoal and double-antibody sep- aration methods.
It is also interesting that although species differences have been noted in the net secretion of glucagon and somatostatin in the presence of anti-insulin gamma globulin (33-38), the same P-to-a-to-6 pattern of intra-islet interaction and perfu- sion has been obtained in all the species with several antibodies obtained from different sources. It is almost intuitive that islet structure or architecture may profoundly affect islet hormone secretion and interaction (3,31,32,34,51- 53). Indeed, it has recently been shown that alterations in both islet cellular content and microvascular architecture significantly affect islet hormone secretion (51). Most mam- malian islets have the same organization of a p-cell core and a non-p-cell mantle. However, the cellular arrangement of the monkey (Macaca) islet appears to be reversed (1,14,28- 30). Studies of methacrylate casts of these islets show afferent vessels running deep into the islet before breaking into capillaries and efferent vessels leaving from the super- ficial parts of the islets. Unfortunately, there was no corre- lation of the blood vessels and the pattern of islet cellular composition and organization, as has been done in the rat. Upon the infusion of anti-insulin gamma globulin into the monkey pancreas, perfusate concentrations of glucagon and somatostatin were markedly increased, as with other mam- mals. For this result to be obtained, a P- to a- to &cell order of perfusion is required, despite the apparent rearrangement of the islet architecture.
The results of the physiological studies of Stagner and Samols and the anatomic studies reported by Bonner-Weir, Orci, and Menger support the presence of a directed micro- vascular sequence of intra-islet cellular perfusion and inter- action from the p-cell outward to the a - and &cells. This work supports the concept that the p-cell is the primary regulator of islet hormone secretion.
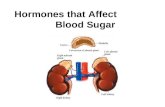
FIG. 3. Model three. In this model, the pattern of flow is polar and is regulated by internal and external gates. Flow enters the islet at the afferent pole and travels across the islet to the efferent pole. Flow reaches all cell types in the hemisphere of the afferent pole before reaching the cell types in the hemisphere of the efferent pole. Flow to the islet is controlled by external gates, and flow within the islet is controlled by internal gates. The external gate is most likely an arteriolar sphincter located at the branch point of the parent arteriole and the supplying arteriole to the islet. The internal gates are independently contractile endothelial cells within the insular capillaries. Thus, the pancreas has the capability to shunt blood to the islet mass during hyperglycernia, and the islet has the capability to shunt blood to and from specific regions within the islet to produce the appropriate hormonal milieu required for glucose homeokinesis. In this model there exist autoregulatory hormonal feedback loops between the islet cells, in which the S-cell plays a significant inhibitory role.
MODEL THREE Model three represents the combined works of McCuskey, Guth, Livingston, Jansson, and Brunicardi and was presented by McCuskey, Guth, Howard, and Brunicardi at the sympo- sium. Model three is described as a gated portal pattern of microcirculation (Fig. 3). In this model, blood flow travels across the islet from the afferent pole to the efferent pole via a portal network that is regulated by internal and external gates. External gates located at the level of the feeding arteriole regulate flow to the islet mass, whereas internal gates at the level of the capillaries regulate flow within the islet. In this pattern of microcirculation, there is no set order of perfusion: cells in one hemisphere of the islet are perfused before cells located in the other hemisphere, i.e., p-cells in one hemisphere could affect p-cells located in the other hemisphere. In addition, in model three, the 6-cell has an important role in the regulation of both p- and a-cell secre- tion. Model three was derived from microsphere studies, in vivo microscopy studies using intravital stains in rat and mouse islets, immunostaining of islets, and isolated perfused human pancreas studies (4,18,25,54-57).
Studies on the microcirculatory pattern in the islets by in vivo microscopy of rat and mouse pancreas suggest polar flow across the islets (4,18,58). After intravenous and/or intra-arterial infusions of fluorescent markers (fluorescein isothiocyanate [FITCI-labeled red cells, FITC-albumin, FITC- somatostatin antibodies, and fluorescent microspheres), the patterns of flow were examined under fluorescent light and recorded. All video images were analyzed both in real time and in slow motion. The passage of the fluorescent markers in real time moved as a wave across the islet from the afferent to the efferent pole. Slow-motion analysis of the pattern of flow in most islets demonstrated that the fluores- cent markers are delivered to one hemisphere of the islet
DIABETES, VOL. 45, APRIL 1996

through the afferent arteriole before perfusing across to the other hemisphere. The fluorescent markers then exit through one or several exiting venules into either the insulo-venous system or surrounding exocrine tissue via insulo-acinar portal vt~ssels. The observation of polar fhow suggests that all cell types of one hemisphere are perfused before the flow reaches the cells of the opposite hemisphere, i.e., all cell types of one hemisphere could potentially influence the cell types located in the other hemisphere. For example, somato- statin secreted from 6-cells in one hemisphere could influ- ence insulin secretion from p-cells and glucagon secretion from a-cells in the other hemisphere. Any given cell type could also influence its own cell type: insulin secreted from p-cells in one hemisphere could influence insulin secretion of p-cells of the other hemisphere. The limitations of in vivo microscopy are that only a single islet per experiment is observed and the islet image is viewed and analyzed in two dimensions. Nevertheless, analysis of numerous images of islets in both rats and mice suggests that flow across the islet is polar.
The flow to the islet mass and within a single islet appears to be regulated by external and internal gates. The first highly detailed in vivo microscopic study of islet microcirculation was performed by McCuskey et al. (18) in 1969. The islets of the mouse were ovoid in structure and had an extensive individual capillary network resembling the renal glomeru- lus. The flow of the red blood cells through the islet was noted to be intermittent and regulated at two levels: 1 ) indepenldently contractile endothelial cells within the insular capillaries were able to slow flow in one portion of the islet while keeping flow constant in other portions, 2 ) sphincters noted at the supplying arteriole were able to stop flow in the entire islet (18). This observation has recently been con- firmed by other groups (1,4,59,60). Studies on the microcir- culatoly pattern in the islets by in vivo microscopy of rat and mouse pancreas demonstrated similarly regulated flow at two levels (4,58). The flow of the cells through the islet was intermittent, while the flow through the parent arteriole was constanl,. Flow to and within the islet would stop approxi- mately three times per minute at irregular intervals. The control of flow appeared to be regulated at the point where the supplying arteriole to the islet branched off from its parent ,arteriole, supporting the concept of an external regulatory gate. The presence of internal gates was sup- ported by using fluorescent microspheres and other fluores- cent markers; flow of the fluorescent markers was noted to randomly stop and go within selected capillaries of the islet, while flow continued unimpeded in other capillaries of the same islet, suggesting the presence of internal gates regulat- ing flow within the islet.
The presence of external gates is supported by the studies of Jansson and Hellerstrom (61,62). Using the static micro- sphere technique in a rat model, it was demonstrated that glucose administration almost doubled the total blood flow to the islet mass. During hyperglycemia, the islet received 85% more blood than in basal conditions, which suggests that hyperglycemia causes a significant shunting of the blood flow from the exocrine pancreas to the islet mass (61-63). This selective increase in islet flow after glucose infusion was previously described as being mediated by a vagal cholinergic mechanism (62). These studies suggest that the pancreas has the ability to shunt blood to the islets during hyperglycemia, which supports the external gate hypothesis.
The presence of a glucose-related shunting mechanism was supported by an in vivo microscopy study by Moldovan et al. (58). The effect of hyperglycemia on capillary flow within a single islet was investigated using in vivo micros- copy of mouse pancreas; under fluorescent light a bolus of FITC-albumin was injected through a carotid catheter during baseline and hyperglycemic conditions. During hyperglyce- mia, there was a significant shortening of the FITC-albumin bolus transit time through the capillary network, suggesting an increase in blood flow through the islet microvasculature during hyperglycemia. The increase was ablated in the presence of a nitric oxide synthase inhibitor, implicating nitric oxide as a regulator of islet microcirculation (58,64- 68). These studies suggest that glucose participates in the physiological control of islet microcirculation, possibly through preferential shunting of blood to or within the islet. The increase in islet blood flow due to hyperglycemia supports the idea that islet hormone secretion may be influenced by microcirculatory changes as well as by neural, hormonal, or nutritional stimuli within the cellular environ- ment.
Model three is supported and expanded by perfusion studies in the isolated perfused human pancreas model (25,54-57). In analyzing simultaneous responses of insulin, glucagon, and somatostatin to anti-hormone antibodies and islet hormone infusions, autoregulatory hormonal feedback loops within the islet have been hypothesized, in which the 6-cell has an important inhibitory regulatory role on the secretion of insulin and glucagon.
Several studies have supported a role for somatostatin within the islet (69,76). Low doses of a somatostatin analog ([D-Ala5-D-Trp8]SS), specific for the 6-cell, indirectly stimu- lated glucagon and insulin secretion by suppressing pancre- atic somatostatin release in dogs (77). In isolated rat islets, insulin and glucagon secretion were stimulated in the pres- ence of a polyclonal somatostatin antibody (78). Other studies have demonstrated no effect of somatostatin within the islet (33-42). In studies by Kleinman and Brunicardi and colleagues (25,54) and Wong (79), the technique of passive immunoneutsalization was used in the isolated perfused human pancreas model. Human pancreases were obtained from cadaveric organ donors after brain death. The somato- statin monoclonal antibody (SAb) and the somatostatin Fab fragment antibody (SFab) used in these studies satisfy the requirements for optimal immunoneutralization: 1 ) the anti- body should have a high affinity for the putative regulatory factor, 2 ) the antibody should have a high specificity for the factor, 3) the antibody should bind the factor at its biologi- cally active site, 4) delivery of a high concentration of the antibody is necessary, and 5 ) there should be absence of nonspecific effects from the antiserum (54,55). The SAb and SFab have high afinity for somatostatin, are highly specific for somatostatin, and are directed at the biologically active somatostatin ring structure (79). SAb and SFab were infused into the splenic artery of the isolated perfused pancreas at a final concentration of 50 pglml(3.3 X man). While islet interstitial levels have never been measured directly, it has been estimated that intra-islet somatostatin levels may reach as high as lo-'' to lop9 moYl(78). The concentration of the SAb and SFab infused in the present study was calculated as an amount that would neutralize over 100-fold in excess of the estimated islet somatostatin concentration. In response to neutralization of intra-islet somatostatin by the infusion of
DIABETES, VOL. 45, APRIL 1996

--
the SAb or SFab, mean insulin secretion increased by 88 and 81%, respectively. The rise in insulin secretion in the pres- ence of the antibody or the Fab fragment could be attributed to either intravascular neutralization of somatostatin (endo- crine effect) or interstitial neutralization of somatostatin (paracrine effect). It is possible that a percentage of SAb and SFab interacts with somatostatin in the islet interstitium, either as a physiological phenomenon or as an aberration related to the isolated perfused pancreas model. It has been demonstrated in rats that 10% of nondegraded SAb and 4090 of nondegraded SFab are able to pass from plasma to lymph, indicating a difference in penetrance of the interstitial space (81). The equal response of increased p-cell secretion seen in these studies caused by the neutralization of somatostatin by the SAb and its Fab fragment suggests that somatostatin is acting as an endocrine mediator within the human islet, possibly via a somatostatin receptor subtype 2 (82). The immunoneutralization of somatostatin resulted in a rise in glucagon secretion, suggesting that intra-islet somatostatin might have an inhibitory effect on a-cell secretion as well (55).
The feasibility of a regulatory effect by intra-islet somato- statin requires that the &cell be able to interact with the P- and a-cells either via the islet microvasculature or by direct contact through the interstitium. The concept of polar flow through the islet enables &cells in the mantle to have vascular access to the p- and a-cells. Furthermore, &cells have been identified in both core and mantle of the human islet, which would enable the &cell to have direct contact via the interstitium with the p- and a-cells (24,25). Thus, the potential exists for intra-islet somatostatin to regulate a- and p-cell secretion via both endocrine and paracrine mecha- nisms.
Model three supports the concept of highly regulated islet flow that permits cell-to-cell communication to occur through a gated portal network. The complexity of a gated portal network would allow the endocrine pancreas to respond to an enormous variety of systemic hormonal and nutrient signals in order to produce the appropriate hor- monal milieu required for glucose homeokinesis.
DISCUSSION These models and the current understanding of islet micro- circulation were discussed openly at the symposium, and constructive criticisms were exchanged at a roundtable discussion. The limitations of the different technologies were acknowledged: corrosion casting only allows a static view of the islet; in vivo microscopy pennits only a two dimensional view; the pancreas perfusion studies only examine changes in the hormonal milieu from the entire endocrine pancreas and not from an individual islet. Several observations made during in vivo microscopy of both rat and mouse were interesting but difficult to explain (Y. Liu, S. Moldovan, R.K., P.H.G., E.H.L., E.C.B.) For example, reversal of flow was noted both in small pancreatic arterioles and within capillar- ies of the islets. Furthermore, vasomotion within the pancre- atic arterioles was observed, which has been seen in other tissues (83,84). Investigations are needed to determine whether these phenomena are artifacts of the model or
communication within the pancreas. Perhaps the greatest limitation of most techniques is the sampling ability: only a single islet per pancreas can be examined in the cast and in vivo studies, whereas only changes in the entire pancreatic hormonal milieu can be studied in the isolated perfused pancreas studies.
Both morphological and intravital evidence was presented suggesting that each of these models is valid under some circumstances as pointed out by Wayland. The corrosion casting work of Murakami in the human pancreas clearly shows the capability of some islets of carrying on all three types of perfusion. There are also intravital observations of al l three models: model one by Nagata et al., model two by Menger, and model three by McCuskey et al. Wayland suggested that in vivo studies be performed with careful attention to the particular physiological state under which the experiments are undertaken. Any one islet may have a single mode of perfusion, but many islets for which data was shown showed the probability, if not the certainty, that more than one pattern will occur depending on the physiological demand. This then emphasizes the need for greater attention to control signals to the islets and to the manner in which the flow into and out of the islets is locally controlled.
Suggestions were made for future research projects that would shed light on the controversies of islet microcircula- tion. As we seek to design drug therapy for improved control of glucose metabolism, the order of perfusion of the target cells and the way in which the target cells communicate become important considerations.
ACKNOWLEDGMENTS The symposium and review were supported by the surgical service, Veterans Administration Medical Center-West Los Angeles, Long Beach Regional Medical Education Center and by the National Institutes of Health Grant lR29DK46441-01.
The symposium was dedicated to the outstanding work on pancreas blood flow of Dr. Jansson, who could not attend because of illness.
REFERENCES 1. Murakami T, Fqjita T, Miyake T, Ohtsuka A, Taguchi T, Kikuta A: The
insulo-acinar portal and insulo-venous drainage systems in the pancreas of the mouse, dog, monkey and certain other animals: a scanning electron microscopic study of corrosion casts. Arch Histol Cytol56:127-147, 1993
2. Bonner-Weir S: The microcirculation of the islet of Langerhans. In The Endocrine Patmeas. Samols E, Ed. New York, Raven, 1994
3. Bonner-Weir S, Orci L: New perspectives on the microvasculature of the islets of Langerhans in the rat. Diabetes 31:883-889, 1982
4. LiuY, Guth PH, Kaneko K, Livingston EH, Bmnicardi FC: Dynamic in vivo observation of rat islet microcirculation. Pancreas 8:15-21, 1993
5. Goldstein MB, Davis EA Jr: The three dimensional architecture of the islets of Langerhans. Acta Anat 71:161-171, 1968
6. Orci L: Macro- and micro-domains in the endocrine pancreas. Diabetes 31538-566, 1982
7. Murakami T, Fqjita T: Microcirculation of the rat pancreas, with special reference to the insulo-acinar portal and insulo-venous drainage systems: a further scanning electron microscope study of corrosion casts. Arch Histol Cytol 55453-476, 1992
8. Ohtani 0 , Ushiki T, Kanazawa H, Fqjita T: Microcirculation of the pancreas in the rat and rabbit with special reference to the insuli-acinar portal system and emissary vein of islet. Arch Histol Jpn 49:4&60, 1986
9. Ohtani 0 : Microcirculation of the pancreas: a correlative study of intravital microscopy with scanning electron microscopy of vascular corrosion casts. Arch Histol Jpn 46:315-325, 1983
10. Ohtani 0 : Review of scanning electron and light microscopic methods in microcirculation research and their application to pancreatic studies. Scannino Electron Microsc 2:653-661. 1984
normal physiological events. If normal, the observations 11. Nagata k, Nishhino H, Iwasaki T, ~obayashi R, Omasa R, ~oshigoe F, Hirano Y, Kuriyama K, Tamura T, Watanabe Y: Microcirculatory dynam- have important implications in the interpretation of hormone ics and microvascular structure of pancreas in the rat-with
secretory data and on our considerations of intercellular reference to endocrine-endocrine relationship in the pancreas. In Intra-
390 DIABETES, VOL. 45, APRIL 1996

vital Observation of Organ Microcirculation. Tsuchiya M, Wayland H, Oda M, Okazaki I, Eds. Princeton, NJ, Excerpta Medica, 1983, p. 139-157
12. Miyake T, Murakami T, Ohtsuka A: Incomplebe vascular casting for a scanning electron microscope study of the microcirculatory patterns in the rat. pancreas. Arch Histol Cylol 55397-406, 1992
13. wits T: Insulo-acinar portal system in the horse pancreas. Arch Histol Jpn 3Ei:161-170, 1973
14. Ewita T, Murakami T: Microcirculation of monkey pancreas with special reference to the insulo-acinar portal system: a scanning electron micro- scope study of vascular casts. Arch Histol Jpn 35:255263, 1973
15. Ohtani 0, Q i t a T: Microcirculation of the pancreas with special refer- ence to periductular circulation: a scanning electron microscope study of vascular casts. Biomed Res 1:130-140, 1980
16. Ohtani 0 , Kikuta A, Ohtsuka A, Taguchi T, Murakami T: Microvascular as studied by the microvascular corrosion castingbcanning electron micro- scope method. I. Endocrine and digestive system. Arch Histol Jpn 46315-325, 1983
17. Bonner-Weir S: The microvasculature of the pancreas, with emphasis on that of the islets of Langerhans: anatomy and functional implications. In The P~zncreas: Biolowu. Patlzobioloou and Disease. Go VLW. DiMaeno EP, Gmdner JD, ~ebenthal E, ~ e b e ; HA, Scheele G.4, Eds. New ~ g r k , Raven, 1993, p. 759-768
18. McCuskey RT, Chapman TM. Microscopy of the living pancreas In situ. Am J Anat 126:39&406, 1969
19. Willia~ns JA, Goldfine ID: The insulin-pancreatic acinar axis. Diabetes 34980-986, 1985
20. Samols E, Stagner JI: Intraislet and islet-acinar portal systems and their significance. In The Endocrine Pancreas. Samols E, Ed. New York, Raven, 1993, p. 93-124
21. Orci L: The microanatomy of the islets of Langerhans. Metabolism 25: 1303-1313, 1976
22. Orci L. Baetens D. Ravazzola M. Stefan Y. Malaisse-Laeae I? Pancreatic polypf.ptide and glucagon: non-;andom distriblltion in pancreatic islets. Life SSci 19:1811-1816, 1976
23. Orci I,, Unger RH: Functional subdivision of islets of Langerhans and possible role of D-cells. Lancet ii:1243-1244, 1975
24. ~ r e ~ e TC, Scharp DW, Sorenson RL: Three-dimensional imaging of intact isolated islets of Langerhans with confocal microscopy. Diabetes 38:808- 814, 1!389
25. Kleinnnan R, Gingerich R, Wong H, Walsh J, Lloyd K, Ohning G, DeGiorgio R, Stemini C, Brunicardi FC: Use of the Fab fragment for imrnunoneu- tralization of somatostatin in the isolated perfwed human pancreas. Am J Surg 167114-119, 1994
26. Erlantlsen SL, Hegre OD, Parsons JA, McEvory RC, Elde RP: Pancreatic islet cell hormones distribution of cell types in the islet and evidence for the presence of somatostatin and gastrin within the D cell. J Histochem Cytochem 24883-897, 1976
27. Grube D, Eckert I, Speck PT, Wagner HJ: Immunohistochemistry and micm:matomy of the islets of Langerhans. Biww~ed Res 4 (Suppl. 46):25, 1983
28. Jones CW, Reynolds WA, Hoganson GE: Streptozotocin in the monkey: p1asm;s levels of glucose, insulin, glucagon, and somatostatin with corresponding morphometric analysis of islet endocrine cells. Diabeles 29536-546, 1980
29. Girod C, Durand N, Raccurt M: Immunostaining of a cell type in the islets of Langerhans of the monkey macaca ims by antibodies against S-100 protein. Cell Tissue Res 24711-16, 1987
30. Wolfe--Coole SA, Du Toit DF: Distribution of cell types of the islets of Langerhans throughout the pancreas of the chacma baboon. Anat Rec 217172-177, 1987
31. Menger MD, Hammersen F, Messmer K: The microcirculation of the islets of Langerhans: state of the art. In Gastrointestinal Microcirculation. Vol. 1'7. Messmer K, Hammersen F, Eds. Basel, Karger, p. 192-215, 1990
32. Menger MD, Valoczy P, Beger C, Messmer K: Orientation of microvas- cular blood flow in pancreatic islet isografts. J Clin Invest 93:2280-2285, 1994
33. Samols E, Stagner J1, Ewart RBL, Marks V: The order of microvascular cellular perfusion is B-A-D in the perfused rat pancreas. J Clin Invest 82:350354, 1988
34. Samols E, Stagner JI: Intra-islet regulation. Arn J Med 8531-35, 1988 35. Stagner JI, Samols E, Bonner-Weir S: B-A-D pancreatic islet cellular
perfusion in dogs. Diabetes 41: 1715-1721, 1988 36. Stagner JI, Samols E, Marks V: Anterograde and retrograde infusion of
glucagon antibodies suggests the A cells are vascularly perfused before D cells within the rat islet. Diabetologia 32:203-206, 1989
37. Stagner JI, Samols E, Koerker DJ, Goodner CJ: Perfusion with anti- insulin gamma globulin indicates a B to A to D cellular perfusion sequence in the pancreas of the rhesus monkey, rnacaca mulatta. Pancreas 726-29, 1992
38. Stagner J1, Samols E: The vascular order of islet cellular perfusion in the human pancreas. Diabetes 41:93-97, 1992
39. Stagner JI, Samols E: Retrograde perfusion as a method for testing the relative effects of glucose on the A cell. J Clin Invest 771034-1037, 1986
40. Stagner JI, Sanlols E: A test of concepts of islet blood flow and compartmentalization (Abstract). Diabetes 33145A, 1984
41. Samols E, Stagner JI: Flow versus compartmentalization in the determi-
nation of intra-islet hormone interactions (Abstract). Clin Res 34387.4, 1986
42. Samols E, Stagner JI: Intra-islet and islet-acinar portal systems and their significance. In The Endocrine Pancreas. Samols E, Ed. New York, Raven, 1991, p. 93-124
43. Nakagawa A, Stagner JI, Samols E: In situ binding of islet hormones in the isolated rat pancreas: evidence for local high concentrations of islet hormones in the islet-acnlar axis. Diabetologin 38:262-268, 1996
44. Nakagawa A, Stagner JI, Samols E: Suppression of the islet-acinar axis in the perfused rat pancreas. Gastrarnterol 105:868-875, 1993
45. Nakagawa A, Samols E, Stagner JI: Interstitial acinar islet hormone concentrations in the dog pancreas. Am J Physiol264:G728-G734, 1993
46. Stagner JI, Samols E, Nakagawa A: The role of the islet-acinar portal system in the regulation of exocrine function. In Ga,strointestirtal Tract and Endocrine System. Singer MV, Ziegler R, Rohr G, Eds. Lancaster, U.K., Kluwer, 1995, p. 518-536
47. Rippe B, Harldsson B: Transport of macromolecules across microvascu- lar walls: the two pore theory. Physiol Reo 74163-219, 1994
48. Kvietys PR, Peny MA, Granger DN: Permeability of pancreatic capillaries to small molecules. Am J Physiol 245G519-G52.1, 1983
49. Maruyama H, Hisatomi A, Orci L, Grodsky GM, Unger RH: Insulin within islets is a physiological glucagon release inhibitor. J Clir~ Irivest 742296- 2299, 1984
50. Samols E, Stagner JI: Reinterpretation of the effects of haloperidol and ethanol on insulin secretion. Diabetologia 19:81-83, 1980
51. Stagner JI, Mokshagundam S, Samols E: Hormone secretion from trans- planted islets is dependent upon changes in islet revascularization and islet architecture. Trartsplant Proc 273251-3254, 1995
52. Weir GC, Samols E, Loo S, Pate1 YC, Gabbay KH: Somatostatin and pancreatic polypeptide secretion: effects of glucagon, insulin and ar- ginine. Diabetes 28:3&40, 1979
53. Asplin CM, Paquete TL, Palmer JP: In vivo inhibition of glucagon secretion by paracrine beta cell activity in man. J Clin Invest 68:314318, 1981
54. Kleinman R, Ohning G, Wong H, Watt P, Walsh J, Brunicardi FC: The regulatory role of intraislet somatostatin on insulin secretion in the isolated pelfused human pancreas. Pancreas 9: 172-178, 1993
55. Kleinman R, Gingerich R, Ohning G, Wong H, Olthoff K, Walsh J, Brunicardi FC: The influence of somatostatin on glucagon and pancreatic polypeptide secretion in the isolated perfused human pancreas. Int J Pancreatol 18:51-57, 1995
56. Brunicardi FC, Druck P, Seymour NE, Sun YS, Elahi D, Andelsen DK: Selective neurohormonal interactions in islet cell secretion in the iso- lated perfused human pancreas. J Surg Res 48:273-278, 1990
57. Bmnicardi FC, Sun YS, Dmck P, Goulet RJ, Elahi D, Andelsen DK: Splanchnic neural regulation of insulin and glucagon secretion in the isolated perfused human pancreas. Am J Surg 15334-40, 1987
68. Moldovan S, Livingston E, Zhang RS, Kleinman R, Guth P, Brunicardi FC: Glucose induced islet hyperemia is mediated by nitric oxide. Am J Surg 171:16-20, 1996
59. Aharinejad S, MacDonald IC, Schmidt EE, Bock P, Hagen D, Groom AC: Scanning and transmission electron microscopy and high resolution intravital videomicroscopy of capillaries in the mouse exocrine pancreas, with special emphasis on endothelial cells. Anat Rec 237163-177, 1993
60. McCuskey RS: Sphincters in the microvascular system. Micravasc Rus 2428-433, 1971
61. Jansson L, Hellerstrom C: Stimulation by glucose of the blood flow to the pancreatic islets of the rat. Diabetologia 25:4550, 1983
62. Jansson L, Hellerstrom C: Glucose-induced changes in pancreatic islet blood flow mediated by central nervous system. Am JPhysiol251:E644- E647, 1986
63. Jansson L: Influence of adrenaline on blood perfusion and vascular conductance of the whole pancreas and the islets of Langerhans in the rat. Arch Int Phaimacodyn 313:90-97, 1991
64. De Giorgio R, Parodi JE, Brecha NC, Bmnicardi FC, Becker JM, Go VL, Sternini C: Nitric oxide producing neurons in the monkey and human digestive system. J Corrtp Neurol 342519-627, 1994
65. Corbett JA, Mikhael A, Shimizu J, Frederick K, Misko TP, McDaniel ML, Kanagawa 0 , Unanue ER: Nitric oxide production in islets from non- obese diabetic mice: aminoguanidine-sensitive and -resistant stages in the immunological diabetic process. &or Nat Acad Sci USA 90:8992- 8995, 1993
66. Ekbad E, Alm P, Sundler F: Distribution, origin and projections of nitric oxide synthase-containing neurons in gut and pancreas. Neuroscience 63:23P248, 1994
67. Schmidt HW. Warner TD. Ishii K. Shene H. Murad F: Insulin secretion , - ~ " --, ~ -~
from pancreatic B cells caused by Larginine-derived nitrogen oxides. Science 255:721-723, 1992
68. Svensson AM, Ostenson CG, Sandler S, Efendic S, Jansson L: Inhibition of nitric oxide synthase by NG-nitro-Largilune causes a preferential decrease in pancreatic islet blood flow in normal rats and spontaneously diabetic GK rats. Endocrinology 135:849-863, 1994
69. Brown M, Rivier J , Vale W: Biological activity of somatostatin and somatostatin analogs on inhibition of arginine-induced insulin and glu- cagon release in the rat. Endocrinology 98:336-343, 1976
70. Santerre RF, Cook RA, Crisel RMD, Sharp, JD, Schmidt RJ, Williams DC,
DIABETES, VOL. 45, APRIL 1996

Wilson CP: Insulin synthesis in a clonal cell line of simian virus 40-transformed hamster pancreatic beta cells. Proc Natl Acad Sri CISA 78:4339-4343, 1981
71. SchusdziarraV, Lawcki J. Ditschunheit HH, Lukas B, Meier V, Pfeiffer EF: Effect of low-dose somatostatin infusion on pancreatic and gastric endocrine function in lean and obese nondiabetic human subjects. Diabetes 34595-601, 1981
72. Schusdziarra V, Zyznar E, Rouiller D, Boden G, Brown JC, Arimura A, Ilnger RH: Splanchnic somatostatin: a hormonal regulator of nutrient homeostasis. Scir)lce 207530-532, 1980
73. Mortimer CH, Turnbridge WMG, Carr D, Yeomena L, Lind T, Coy DH, Schally AV, Drouin J, Ferland L, Beaulieu M, Labrie F: Somatostatin analogs which inhibit glucagon and growth hormone more than insuline release. Biochem Bioplrys Res Cwmmun 74:630-636, 1977
74. Reichlin S: Somatostatin. N Engl JMed 3091495-1501, 1983 75. Patrl YC, Wheatlet T, Ning C: Multiple forms of immunoreactive somato-
statin: comparison of distribution in neural and nonneural tissues and portal plasma of the rat. Endom'nology 109:194%1949, 1981
76. Amherdt M, Pate1 YC. Orci L: Selective binding of somatostatin-14 and somatostatin-28 to islet cells revealed by quantitative electron micro- scopic autoradiography. J Clin Invest 80: 1455-1458, 1987
77. Taborsky GJ: Evidmce of a pararrine role for pancreatic somatostatin in vivo. Am .I Physiol245:3598-E603, 1983
--
78. Itoh M, Mandarin~ L, Gerich JE: Antisomatostatin gamma globulin augments secretion of both insulin and glucagon in vitro: evidence for a physiologic role for endogenous somatostatin in the regulation of pan- creatic A- and B- cell function. Diabetes 29:69%696, 1980
79. Wong HC, Walsh JH, Yang H, Tache Y, Buchan AM: A monoclonal antibody to somatostatin with potent in vivo immunoneutralizing activity. Peptides 11:707-712, 1990
80. Samols E, Stagner JI: Intraislet and islet-acinar portal systems and their significance. In Comprehm~siz~e Endocrinology: The Endocritw Pan- creos. Samols E, Ed. New Pork, Raven Press, 1991, p. 9%124
81. Ohning GV, Lloyd KCK, Granger DN, Walsh JII: Distribution of somato- statin monoclonal IgG and its Fab-1 fragment from plasma to intestinal lymph in rats (Abstract). Dig Dis 98:A516, 1991
82. Moldovan S, Atiya A, Adrian TE, Kleinman RM, Lloyd K, Olthoff K, Imagawa D, Shevlin L, Coy D, Walsh J, Bmnicardi FC: Somatostatin inhibits insulin secretion by a type 2 receptor in the isolated perfused human pancreas. J Surg Res 59:8590, 1995
83. Intaglietta M: Arteriolar vasomotion: implications for tissue ischemia. Blood Vessels 28: 1-7, 1991
84. Colantuoni A, Bertuglia S, Intaglietta M: The effects of alpha or beta adrenergir receptor agonists and antagonists and calcium entry blockers on the spontaneous vasomotion. Microvosc Rrs 28:143-158, 1984
DIABETES, VOL. 45, APRIL 199G