Microbe hunting in the joints
4
Microbe Hunting in the Joints XIANG ZHANG, 1 CESAR PACHECO-TENA, 2 AND ROBERT D. INMAN 1 Rheumatoid arthritis (RA) is considered an autoimmune disease, but the notion that the process may be triggered by an unknown infectious agent has been a longstanding concept in the pathogenesis of RA. After several decades searching for such causative agents in the joints, the direct evidence is still missing. In the June issue of Arthri- tis Care & Research, Chen et al provided new insights in this area searching with gas chromatography-mass spec- trometry (GC-MS) for muramic acid, a component de- rived from bacterial cell walls, in the joint tissues of RA patients (1). In the case of reactive arthritis (ReA), infectious agents triggering joint inflammation have been well established (2,3). Gastrointestinal infections by enteric bacterial strains, such as Yersinia, Salmonella, Campylobacter, and Shigella species, and urogential infections by Chlamydia species are known to be associated with ReA. One of the strongest links is the demonstration of Chlamydial DNA in the joints of patients with post-Chlamydia ReA by poly- merase chain reaction (PCR) (4,5). However, after a pro- longed search for bacterial DNA in RA joints, it remains unresolved whether or not an organism or its antigenic fragments persist locally in these joints. It may still be argued that the causative agent is present at such a low concentration that it cannot be detected with current mi- crobiology techniques. To date, many methods have been used in hunting for microbes in joints with RA, as well as those with ReA, ankylosing spondylitis, and osteoarthritis (OA) (Table 1). In their study, Chen et al screened for bacteria in joint tissues of RA patients using a sensitive pan-bacteria PCR, which can detect DNA of almost any bacterial species. However, no bacterial DNA was found in their study. Despite the absence of bacterial DNA, they probed for evidence of the bacterial cell wall, which rep- resents the major constituent of bacteria. The skeleton of bacterial cell walls mainly consists of polysaccharide, pep- tidoglycan, and cell wall-associated proteins. Peptidogly- can is the major constituent of the gram-positive bacterial cell wall, whereas lipopolysaccharide (LPS) is the domi- nant component of the gram-negative bacterial cell wall. The schematic structure of the gram-positive bacterial cell wall is shown in Figure 1. In the current study, Chen et al selected muramic acid, a component of the peptidoglycan moiety of the bacterial cell wall. Muramic acid is unique to bacteria and is not present in the mammalian proteome, making it an ideal chemical marker for detecting bacteria (6). Chen et al detected muramic acid by using a GC-MS with a chemical ionization method sensitive enough to detect even picogram amounts (2 pg/injected amount). GC-MS has previously been used successfully to detect muramic acid in joints of septic arthritis patients) (7,8). Chen et al were able to demonstrate the presence of mu- ramic acid in the joints of some RA patients, suggesting persistence of bacterial cell wall components, rather than bacterial DNA, in the joints of chronic RA (duration more than 5 years). Their findings are in line with earlier reports that bacterial cell wall components were present in RA joints by immunohistochemistry, using an antibody against bacterial cell wall peptidoglycan (9). However, this current study makes the important observation that the presence of bacterial cell wall components is not specific for RA, since they were also found in joint tissues of OA patients. The question has remained open how these bacterial cell wall components might play a biologic role if they persist in the joints for prolonged periods. Are they pathogenic? Several studies have implicated bacterial cell wall compo- nents as having multiple immunologic activities that may contribute to joint inflammation. 1) The recently discov- ered receptors of the first line of host defense—the Toll- like receptors (TLR)—recognize a range of microbes and their products. For example, TLR2 recognizes bacterial peptidoglycan (10). 2) Bacterial peptidoglycan is capable of stimulating synovial macrophages to express the co- stimulatory molecules CD80 and CD86, and to produce proinflammatory cytokines such as tumor necrosis factor and interleukin 6 (11). 3) Certain bacterial cell walls are able to induce experimental arthritis in rats with his- topathologic features resembling RA (12,13). 4) Small frag- ments of the arthritogenic bacterial peptidoglycan, such as muramyl peptides, possess potent proinflammatory capac- ity (14). All these lines of evidence suggest that the bacte- rial cell wall components are potential arthritogenic 1 Xiang Zhang, MD, PhD, Robert D. Inman, MD: University Health Network and University of Toronto, Toronto, On- tario, Canada; 2 Cesar Pacheco-Tena, MD, MSc: Hospital Central Universitario, Universidad Autono ´ma de Chihua- hua, and Hospital Clı´nica del Parque, Mexico. Address correspondence to R. D. Inman, MD, Arthritis Center of Excellence, ECW 8-005, Toronto Western Hospital, 399 Bathurst Street,Toronto, ON, M5T 2S8 Canada. Submitted for publication December 11, 2002; accepted December 22, 2002. Arthritis & Rheumatism (Arthritis Care & Research) Vol. 49, No. 4, August 15, 2003, pp 479–482 DOI 10.1002/art.11186 © 2003, American College of Rheumatology EDITORIAL 479
-
Upload
xiang-zhang -
Category
Documents
-
view
213 -
download
0
Transcript of Microbe hunting in the joints

Microbe Hunting in the JointsXIANG ZHANG,1 CESAR PACHECO-TENA,2 AND ROBERT D. INMAN1
Rheumatoid arthritis (RA) is considered an autoimmunedisease, but the notion that the process may be triggered byan unknown infectious agent has been a longstandingconcept in the pathogenesis of RA. After several decadessearching for such causative agents in the joints, thedirect evidence is still missing. In the June issue of Arthri-tis Care & Research, Chen et al provided new insights inthis area searching with gas chromatography-mass spec-trometry (GC-MS) for muramic acid, a component de-rived from bacterial cell walls, in the joint tissues of RApatients (1).
In the case of reactive arthritis (ReA), infectious agentstriggering joint inflammation have been well established(2,3). Gastrointestinal infections by enteric bacterialstrains, such as Yersinia, Salmonella, Campylobacter, andShigella species, and urogential infections by Chlamydiaspecies are known to be associated with ReA. One of thestrongest links is the demonstration of Chlamydial DNA inthe joints of patients with post-Chlamydia ReA by poly-merase chain reaction (PCR) (4,5). However, after a pro-longed search for bacterial DNA in RA joints, it remainsunresolved whether or not an organism or its antigenicfragments persist locally in these joints. It may still beargued that the causative agent is present at such a lowconcentration that it cannot be detected with current mi-crobiology techniques. To date, many methods have beenused in hunting for microbes in joints with RA, as well asthose with ReA, ankylosing spondylitis, and osteoarthritis(OA) (Table 1). In their study, Chen et al screened forbacteria in joint tissues of RA patients using a sensitivepan-bacteria PCR, which can detect DNA of almost anybacterial species. However, no bacterial DNA was found intheir study. Despite the absence of bacterial DNA, theyprobed for evidence of the bacterial cell wall, which rep-resents the major constituent of bacteria. The skeleton ofbacterial cell walls mainly consists of polysaccharide, pep-
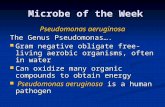
tidoglycan, and cell wall-associated proteins. Peptidogly-can is the major constituent of the gram-positive bacterialcell wall, whereas lipopolysaccharide (LPS) is the domi-nant component of the gram-negative bacterial cell wall.The schematic structure of the gram-positive bacterial cellwall is shown in Figure 1. In the current study, Chen et alselected muramic acid, a component of the peptidoglycanmoiety of the bacterial cell wall. Muramic acid is unique tobacteria and is not present in the mammalian proteome,making it an ideal chemical marker for detecting bacteria(6). Chen et al detected muramic acid by using a GC-MSwith a chemical ionization method sensitive enough todetect even picogram amounts (2 pg/injected amount).GC-MS has previously been used successfully to detectmuramic acid in joints of septic arthritis patients) (7,8).Chen et al were able to demonstrate the presence of mu-ramic acid in the joints of some RA patients, suggestingpersistence of bacterial cell wall components, rather thanbacterial DNA, in the joints of chronic RA (duration morethan 5 years). Their findings are in line with earlier reportsthat bacterial cell wall components were present in RAjoints by immunohistochemistry, using an antibodyagainst bacterial cell wall peptidoglycan (9). However, thiscurrent study makes the important observation that thepresence of bacterial cell wall components is not specificfor RA, since they were also found in joint tissues of OApatients.
The question has remained open how these bacterial cellwall components might play a biologic role if they persistin the joints for prolonged periods. Are they pathogenic?Several studies have implicated bacterial cell wall compo-nents as having multiple immunologic activities that maycontribute to joint inflammation. 1) The recently discov-ered receptors of the first line of host defense—the Toll-like receptors (TLR)—recognize a range of microbes andtheir products. For example, TLR2 recognizes bacterialpeptidoglycan (10). 2) Bacterial peptidoglycan is capableof stimulating synovial macrophages to express the co-stimulatory molecules CD80 and CD86, and to produceproinflammatory cytokines such as tumor necrosis factor �and interleukin 6 (11). 3) Certain bacterial cell walls areable to induce experimental arthritis in rats with his-topathologic features resembling RA (12,13). 4) Small frag-ments of the arthritogenic bacterial peptidoglycan, such asmuramyl peptides, possess potent proinflammatory capac-ity (14). All these lines of evidence suggest that the bacte-rial cell wall components are potential arthritogenic
1Xiang Zhang, MD, PhD, Robert D. Inman, MD: UniversityHealth Network and University of Toronto, Toronto, On-tario, Canada; 2Cesar Pacheco-Tena, MD, MSc: HospitalCentral Universitario, Universidad Autonoma de Chihua-hua, and Hospital Clınica del Parque, Mexico.
Address correspondence to R. D. Inman, MD, ArthritisCenter of Excellence, ECW 8-005, Toronto Western Hospital,399 Bathurst Street,Toronto, ON, M5T 2S8 Canada.
Submitted for publication December 11, 2002; acceptedDecember 22, 2002.
Arthritis & Rheumatism (Arthritis Care & Research)Vol. 49, No. 4, August 15, 2003, pp 479–482DOI 10.1002/art.11186© 2003, American College of Rheumatology
EDITORIAL
479

agents. If they appear in the joints under certain circum-stances, and persist chronically, the stage may be set inthis microenvironment of inflammation and injury for abreakdown in immune tolerance to local self antigens,thereby initiating an autoimmune response leading to selfperpetuating inflammation and ultimately to bone and car-tilage destruction.
On the other hand, it should be pointed out that thestimulatory potential of TLR ligands, such as LPS or pep-tidoglycan, is relatively short lived, raising questionsabout their potential as chronic stimuli. After an initialchallenge with LPS, dendritic cells or macrophages enterinto a programmed hyporesponsive stage in which theTLR4 signaling pathway has been shown to be downregu-lated (15,16). This hyporesponsiveness has also been ana-lyzed for TLR2 ligands, such as mycobacterial lipopep-tides and lipoteichoic acid, and cross-hyporesponsivenessinduction between TLR2 and TLR4 has been proposed(16,17). Therefore, chronic persistence of bacterial compo-
nents in the joints does not necessarily mean a chronicinflammatory stimulus in the joint. This fact may explainthe discordance between inflammation and the presence ofmuramic acid in the synovial tissues of OA. The potentialof muramic acid as a proinflammatory factor in RA syno-vitis is unsolved. Nevertheless, genetic polymorphisms inthe molecules involved in the recognition and signalingpathways for bacterial components might explain differentindividual susceptibilities. This question has been ad-dressed for TLR2 mutations and gram-positive (Staphylo-coccal) infection (18), as well as for TLR4 polymorphismsand gram-negative infections (19,20).
The study of Chen et al demonstrates the presence ofstable bacterial degradation products, rather than thewhole bacteria, not only in the joints of RA patients butalso OA patients. This raises important issues about theclinical significance of these events for RA pathogenesis.This has an interesting parallel in the PCR analysis ofReA joint tissues, in which Chlamydial nucleic acidshave been found not only in these patients but also inOA patients (21,22). On the other hand, this study illus-trates that targeting the bacterial cell wall componentsby current techniques may be an alternative way to huntmicrobes in the joints. Several methods have been usedto detect the bacterial cell wall components in the jointsof experimental cell wall-induced arthritis (Table 2).These methods detecting unique bacterial cell wall com-ponents can be considered a valuable approach to studythe role of microbes and their products in arthropathicdiseases. With these more sophisticated techniques, amore definitive statement on microbial contribution toRA pathogenesis may be forthcoming. It should be re-called that the initial report of Helicobacter pylori re-covered from the gastric tissues of patients with pepticulcer disease were met with great skepticism (23). Erad-icating this organism is now considered optimal therapyfor this disease (24)—perhaps a word of caution for thecritics and a word of encouragement for the microbehunters in the joints.
Figure 1. Schematic structure of the envelope structure of gram-positive bacteria.
Table 1. Detection of microbes in joint tissues by different methods*
Rheumatoidarthritis
Reactivearthritis
Ankylosingspondylitis Osteoarthritis
SepticArthritis
Culture � � � � �EM � �† ND ND �IF/IHC � �‡ ND ND �PCR �§, �¶ �† �**, �‡‡ �† �GC-MS �¶ �‡‡ ND �¶ �
* Culture, electron microscopy (EM), immunofluorescence (IF) and immunohistochemistry (IHC) are usedfor detecting intact organisms or their antigenic fragments, polymerase chain reaction (PCR) for theirnucleic acids and gas chromatography-mass spectrometry (GC-MS) for their cell wall components.References are in parenthesis. ND � Not done† Chlamydia only (5, 22, 24)‡ Chlamydia, Salmonella, and Yersinia (25–27)§ Pan-bacterial PCR (9, 28)¶ Current study by Chen et al (1)** In juvenile anklyosing spondylitis patients (29)†† Nested PCR (30)‡‡ Detection of muramic acid (26)
480 Zhang et al

REFERENCES
1. Chen T, Rimpilainen M, Luukkainen R, Mottonen, T, Yli-JamaT, Jalava J, et al. Bacterial components in the synovial tissue ofpatients with advanced rheumatoid arthritis or osteoarthritis:analysis with gas chromatography-mass spectrometry andpan-bacterial polymerase chain reaction. Arthritis Rheum(Arthritis Care Res) 2003;49:328–334.
2. Toivanen A, Toivanen P. Reactive arthritis. Curr Opin Rheu-matol 2000;12:300–5.
3. Hyrich KL, Inman RD. Infectious agents in chronic rheumaticdiseases. Curr Opin Rheumatol 2001;13:300–4.
4. Bas S, Griffais R, Kvien TK, Glennas A, Melby K, Vischer TL.Amplification of plasmid and chromosome Chlamydia DNAin synovial fluid of patients with reactive arthritis and undif-ferentiated seronegative oligoarthropathies. Arthritis Rheum1995;38:1005–13.
5. Branigan PJ, Gerard HC, Hudson AP, Schumacher HR Jr,Pando J. Comparison of synovial tissue and synovial fluid asthe source of nucleic acids for detection of Chlamydia tracho-matis by polymerase chain reaction. Arthritis Rheum 1996;39:1740–6.
6. Gilbart J, Fox A, Whiton RS, Morgan SL. Rhamnose and mu-ramic acid: chemical markers for bacterial cell walls in mam-malian tissues. J Microbiol Methods 1986;5:272–82.
7. Christensson B, Gilbart J, Fox A, Morgan SL. Mass spectro-metric quantitation of muramic acid, a bacterial cell wallcomponent, in septic synovial fluids. Arthritis Rheum 1989;32:1268–72.
8. Lehtonen L, Kortekangas P, Oksman P, Eerola E, Aro H, Toiv-anen A. Synovial fluid muramic acid in acute inflammatoryarthritis. Br J Rheumatol 1994;33:1127–30.
9. Van der Heijden IM, Wilbrink B, Tchetverikov I, Schrijver IA,Schouls LM, Hazenberg MP, et al. Presence of bacterial DNAand bacterial peptidoglycans in joints of patients with rheu-matoid arthritis and other arthritides. Arthritis Rheum 2000;43:593–8.
10. Pacheco-Tena C, Zhang X, Stone M, Burgos-Vargas R, InmanRD. Innate immunity in host-microbial interactions: beyondB27 in the spondyloarthropathies. Curr Opin Rheumatol2002;14:373–82.
11. Schrijver IA, Melief M-J, Tak PP, Hazenberg MP, Laman JD.Antigen-presenting cells containing bacterial peptidoglycanin synovial tissues of rheumatoid arthritis patients coexpresscostimulatory molecules and cytokines. Arthritis Rheum2000;43:2160–8.
12. Simelyte E, Rimpilainen M, Lehtonen L, Zhang X, ToivanenP. Bacterial cell wall-induced arthritis: chemical compositionand tissue distribution of four Lactobacillus strains. InfectImmun 2000;68:3535–40.
13. Zhang X, Rimpilainen M, Simelyte E, Toivanen P. Character-ization of Eubacterium cell wall: peptidoglycan structure de-termines arthritogenicity. Ann Rheum Dis 2001;60:269–74.
14. Zhang X, Rimpilainen M, Simelyte E, Toivanen P. Enzymedegradation and proinflammatory activity in arthritogenicand nonarthritogenic Eubacterium aerofaciens cell walls. In-fect Immun 2001;69:7277–84.
15. Sato S, Takeuchi O, Fujita T, Tomizawa H, Takeda K, Akira S.A variety of microbial components induce tolerance to lipo-polysaccharide by differentially affecting MyD88-dependentand -independent pathways. Int Immunol 2002;14:783–91.
16. Jacinto R, Hartung T, McCall C, Li L. Lipopolysaccharide- andlipoteichoic acid-induced tolerance and cross-tolerance: dis-tinct alterations in IL-1 receptor-associated kinase. J Immunol2002;168:6136–41.
17. Medvedev AE, Henneke P, Schromm A, Lien E, Ingalls R,Fenton MJ, et al. Induction of tolerance to lipopolysaccharideand mycobacterial components in Chinese hamster ovary/CD14 cells is not affected by overexpression of Toll-like re-ceptors 2 or 4. J Immunol 2001;167:2257–67.
18. Lorenz E, Mira JP, Cornish KL, Arbour NC, Schwartz DA. Anovel polymorphism in the toll-like receptor 2 gene and itspotential association with staphylococcal infection. Infect Im-mun 2000;68:6398–401.
19. Arbour NC, Lorenz E, Schutte BC, Zabner J, Kline JN, Jones M,et al. TLR4 mutations are associated with endotoxin hypore-sponsiveness in humans. Nat Genet 2000;25:187–91.
20. Agnese DM, Calvano JE, Hahm SJ, Coyle SM, Corbett SA,Calvano SE, et al. Human Toll-like receptor 4 mutations butnot CD14 polymorphisms are associated with an increasedrisk of gram-negative infections. J Infect Dis 2002;186:1522–5.
21. Schumacher HR Jr, Gerard HC, Arayssi TK, Pando JA, Brani-gan PJ, Saaibi DL, et al. Lower prevalence of Chlamydia pneu-moniae DNA compared with Chlamydia trachomatis DNA insynovial tissue of arthritis patients. Arthritis Rheum 1999;42:1889–93.
22. Olmez N, Wang GF, Li Y, Zhang H, Schumacher HR. Chla-mydial nucleic acids in synovium in osteoarthritis: what arethe implications? J Rheumatol 2001;28:1874–80.
23. Przyklenk B, Bauernfeind A, Bornschein W, Emminger G,Heilmann K, Schweighart S. The role of Campylobacter (Hel-icobacter) pylori in disorders of the gastrointestinal tract.Infection 1990;18:3–7.
24. Tulassay Z, Kryszewski A, Dite P, Kleczkowski D, RudzinskiJ, Bartuzi Z, et al. One week of treatment with esomeprazole-based triple therapy eradicates Helicobacter pylori and healspatients with duodenal ulcer disease. Eur J GastroenterolHepatol 2001;13:1457–65.
25. Schumacher HR Jr, Magge S, Cherian PV, Sleckman J, Roth-fuss S, Clayburne G, et al. Light and electron microscopicstudies on the synovial membrane in Reiter’s syndrome: im-munocytochemical identification of Chlamydial antigen inpatients with early disease. Arthritis Rheum 1988;31:937–46.
26. Nikkari S, Rantakokko K, Ekman P, Mottonen T, LeirisaloRepo M, Virtala M, et al. Salmonella-triggered reactive
Table 2. Detection of bacterial cell wall components in joints of rats with experimental cell wall-induced arthritis
Methods Cell wall components detected References
Radio-label (125I, 14C) Cell wall, peptidoglycan-polysaccharide (31,32)Solid-phase radioimmunoassay Polysaccharide (N-acetylglucosamine, rhamnose oligosaccharide),
peptidoglycan (D-alanine-D-alanine moiety of stem peptide)(33)
Enzyme-linked immunosorbent assay Polysaccharide (N-acetylglucosamine) (34)Immunofluorescence Cell wall (35,36)Immunohistology Cell wall, peptidoglycan-polysaccharide* (37)Gas chromatography-mass
spectrometryRhamnose, muramic acid (14,38)
Gas-liquid chromatography-massspectrometry
Muramic acid (39)
* Peptidoglycan-polysaccharide has also been detected in joints of patients with rheumatoid arthritis (8).
Microbe Hunting 481

arthritis: use of polymerase chain reaction, immunocyto-chemical staining, and gas chromatography-mass spectrome-try in the detection of bacterial components from synovialfluid. Arthritis Rheum 1999;42:84–9.
27. Granfors K, Jalkanen S, von Essen R, Lahesmaa-Rantala R,Isomaki O, Pekkola-Heino K, et al. Yersinia antigens in syno-vial-fluid cells from patients with reactive arthritis. N EnglJ Med 1989;320:216–21.
28. Gerard HC, Wang Z, Wang GF, El-Gabalawy H, Goldbach-Mansky R, Li Y, et al. Chromosomal DNA from a variety ofbacterial species is present in synovial tissue from patientswith various forms of arthritis. Arthritis Rheum 2001;44:1689–97.
29. Pacheco-Tena C, Alvarado De La Barrera C, Lopez-Vidal Y,Vazquez-Mellado J, Richaud-Patin Y, Amieva RI, et al. Bacte-rial DNA in synovial fluid cells of patients with juvenile onsetspondyloarthropathies. Rheumatology (Oxford) 2001;40:920–7.
30. Braun J, Tuszewski M, Ehlers S, Haberle J, Bollow M, EggensU, et al. Nested polymerase chain reaction strategy simulta-neously targeting DNA sequences of multiple bacterial spe-cies in inflammatory joint diseases. II. Examination of sacro-iliac and knee joint biopsies of patients withspondyloarthropathies and other arthritides. J Rheumatol1997;24:1101–5.
31. Stimpson SA, Esser RE, Cromartie WJ, Schwab JH. Compari-son of in vivo degradation of 125I-labeled peptidoglycan-po-lysaccharide fragments from group A and group D strepto-cocci. Infect Immun 1986;52:390–6.
32. Lehman TJ, Allen JB, Plotz PH, Wilder RL. Lactobacillus casei
cell wall-induced arthritis in rats: cell wall fragment distribu-tion and persistence in chronic arthritis-susceptible LEW/Nand -resistant F344/N rats. Arthritis Rheum 1984;27:939–42.
33. Eisenberg R, Fox A, Greenblatt JJ, Anderle SK, Cromartie WJ,Schwab JH. Measurement of bacterial cell wall in tissues bysolid-phase radioimmunoassay: correlation of distributionand persistence with experimental arthritis in rats. InfectImmun 1982;38:127–35.
34. Anderle SK, Allen JB, Wilder RL, Eisenberg RA, CromartieWJ, Schwab JH. Measurement of streptococcal cell wall intissue of rats resistant or susceptible to cell wall-inducedchronic erosive arthritis. Infect Immun 1985;49:836–7.
35. Dalldorf FG, Cromartie WJ, Anderle SK, Clark RL, Schwab JH.The relation of experimental arthritis to the distribution ofstreptococcal cell wall fragments. Am J Pathol 1980;100:383–402.
36. Wilder RL, Allen JB, Wahl LM, Calandra GB, Wahl SM. Thepathogenesis of group A streptococcal cell wall-induced poly-arthritis in the rat. Arthritis Rheum 1983;26:1442–51.
37. Simelyte E, Rimpilainen M, Rantakokko K, Lehtonen L,Zhang X, Aho H, et al. Tissue distribution and persistence ofarthritogenic and nonarthritogenic Eubacterium cell walls.Clin Exp Rheumatol 1999;17:281–8.
38. Gilbart J, Fox A. Elimination of group A streptococcal cellwalls from mammalian tissues. Infect Immun 1987;55:1526–8.
39. Fox A, Schwab JH, Cochran T. Muramic acid detection inmammalian tissues by gas-liquid chromatography-mass spec-trometry. Infect Immun 1980;29:526–31.
482 Zhang et al