MICI : nouvelles idées nouvelles thérapeutiques › ... ›...
20
MICI : nouvelles idées nouvelles thérapeutiques Guillaume Savoye
Transcript of MICI : nouvelles idées nouvelles thérapeutiques › ... ›...

MICI : nouvelles idées nouvelles thérapeutiques
Guillaume Savoye

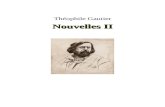
Les MICI sont des maladies progressives…
2
CDAI, Crohn's disease activity index; CDEIS, Crohn’s disease endoscopic index of severity; CRP, C-reactive protein
Inflam
mato
ryactivity
(CD
AI, C
DEIS, C
RP
)
Diseaseonset
Diagnosis Earlydisease
Surgery
Stricture
Stricture
Fistula/abscess
Dig
est
ive
dam
age
(Le
man
nin
dex
)D
isab
ility
(Dis
abili
tyin
dex
)
Pariente B, … Lemann M. Inflamm Bowel Dis 2011; Colombel JF et al. Gastroenterology 2017

Qu’il faut traiter précocément…
3
CDAI, Crohn's disease activity index; CDEIS, Crohn’s disease endoscopic index of severity; CRP, C-reactive protein
Inflam
mato
ryactivity
(CD
AI, C
DEIS, C
RP
)
Diseaseonset
Diagnosis Earlydisease
Surgery
Stricture
Stricture
Fistula/abscess
Window of opportunity?
Dig
est
ive
dam
age
(Le
man
nin
dex
)D
isab
ility
(Dis
abili
tyin
dex
)
Pariente B, … Lemann M. Inflamm Bowel Dis 2011; Colombel JF et al. Gastroenterology 2017

Pour éviter la destruction intestinale et l’invalidité associée
4
Pariente B, et al. Inflamm Bowel Dis 2011;17:1415–22
CDAI, Crohn's disease activity index; CDEIS, Crohn’s disease endoscopic index of severity; CRP, C-reactive protein
Inflam
mato
ryactivity
(CD
AI, C
DEIS, C
RP
)
Diseaseonset
Diagnosis Earlydisease
Dig
est
ive
dam
age
Dis
abili
ty
Pariente B, et al. Inflamm Bowel Dis 2011; Colombel JF et al. Gastroenterology 2017

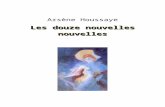
les anti-TNF rapidement diminuent la destruction intestinale
5
• 130 Crohn
– Score de destruction intestinale
Farre C, et al. Presented at UEG Week 2017
Lém
ann
Ind
ex
140
60
40
20
0
<2 years 2–10 years >10 years Early anti-TNF<2 years
Late anti-TNF>2 years
3.7(IQR: 0.6–13.1)
12.3(IQR: 2.9–22.3)
p=0.015 Lém
ann
Ind
ex
Disease durationCD, Crohn’s disease; IQR, interquartile range
80
140
60
40
20
80
0

La cible dans les MICI
van Dullemen HM et al. Gastroenterology 1995
Rémission clinique+
Mary Jy, Modigliani R. Gut 1989

“le contrôle serré”
7
Pariente B, et al. Inflamm Bowel Dis 2011;17:1415–22
CDAI, Crohn's disease activity index; CDEIS, Crohn’s disease endoscopic index of severity; CRP, C-reactive protein
Inflam
mato
ryactivity
(CD
AI, C
DEIS, C
RP
)
Diseaseonset
Diagnosis Earlydisease
Dig
est
ive
dam
age
Dis
abili
ty
Pariente B, et al. Inflamm Bowel Dis 2011; Colombel JF et al. Gastroenterology 2017
Biomarqueurs (CRP, calprotectine…)

Etude CALM ou décider sur des biomarqueurs…
8Colombel JF, et al. Lancet 2018
-9 -4 -1 0 12 24 36 48Final visit
Weeks:
Ran
do
mis
atio
n1
:1
Prednisone burst & taper
T2T (n=122): escalation driven by CDAI, FC, CRP, prednisone use
De-escalation
ADA 40 mg EOW+AZA
ADA 40 mg EOW
Clinical management (n=122): escalation driven by CDAI, prednisone use
Treatment escalation:
ADA 40 mg EW + AZA 2.5 mg/kg/day
ADA 40 mg EWADA 160/80 mg,
40 mg EOWNo
treatment
Rescue** (escalation needed before next visit)
Earlyrandomisation*

30,3
45,9
0
20
40
60
80
100
Pat
ien
ts (
%)
On fait mieux en prenant en compte les biomarqueurs enplus de la clinique…
CDEIS <4and no
deep ulcerations
23,0
15,6
30,3
23,8
16,4
40,236,9
29,5
45,9
29,5
18,0
50,8
0
20
40
60
80
100
Pat
ien
ts (
%)
p=0.014 p=0.006 p=0.010 p=0.229 p=0.728 p=0.067
CDAI <150,no pred ≥8 wks
CDEIS <4no deep ulceration
Clinical management Treat to target
CRP <5 mg/L,FC <250 µg/g,
CDEIS <4
CDEIS <4 CDEIS <4,CDEIS <4 in
all segments
CDEIS=0 CDEISdecrease >5
Clinicalmanagement
Treatto target
37/122 56/122
p=0.010
Deepremission
Biologicremission
Mucosalhealing
Mucosalhealing in
all segments
Completeendoscopicremission
Endoscopicresponse
9
Colombel JF, et al. Lancet 2018

HIGHRISK
Place de l’imagerie “proactive” dans le monitoring
Years: 654321
Diagnosis: Risk stratify
Years: 654321
Diagnosis: Risk stratify
‘Not-High’
RISK
Co
lon
osc
op
y
Imag
ing
Imag
ing
Co
lon
osc
op
y
Imag
ing
Imag
ing
Co
lon
osc
op
y
Co
lon
osc
op
y
Co
lon
osc
op
y
Imag
ing

S1P
Adapted from Danese S, Gut 2012 and Torres J et al. Lancet 2017
Des nouvelles cibles...
IL-23
Th1
Th0
Th17
Th2
Treg
Sagramostim
Basiliximab
Daclizumab
Tenovil
Secukinumab
Vidofiudimus
Fontolizumab
Abatacept Visilizumab
Risankizumab
Ustekinumab
TGFβIL-16
IL-12IFN-γ IL-4
T cell
IL-13
IL-22
IL-17
IL-10
TGFβ
G-CSF
IFN-γ
IL-2GM-CSF
CD3
T cellCD28
Dendriticcell
IL-12
B7
Epithelial cell
Etanercept
Golimumab
InfliximabAdalimumab
Certolizumab pegol
Activatedmacrophage
TNF-αIL-10
IL-6
Effector Th cell
NatalizumabVedolizumabEtrolizumab
PF547659
Endothelial cell
CCR9
VCAM-1MAdCAM-1
α4β1 α4β7
Leukocyte ICAM-1
Tocilizumab
RituximabOcrelizumab
Tofacitinib
Jak3p38
JNK
11
Filgotinib
Upadacitinib
B
IL, interleukin.
TES1P1
Ozanimod
Lymph node
Anti-TNF uniquement

IL-12 and IL-23 et Crohn
p35
IL12-Rβ2 IL12-Rβ1 IL-23R
IL-17IFN-ɣ
IL-12 IL-23
IL12-Rβ1
p19p40p40
Ustekinumab

Ustekinumab et CrohnRéponse à 6 semaines
Feagn B et al. NEJM 2016
28,7
51,755,5 53,6
0
10
20
30
40
50
60
Placebo(N=209)
130 mg(N=209)
~6 mg/kg(N=209)
Combined(N=418)
UNITI-2
Pro
po
rtio
n o
f su
bje
cts
(%)
Ustekinumab
p<0.001p<0.001 p<0.001
21,5
34,3 33,7 34,0
0
10
20
30
40
50
60
Placebo(N=247)
130 mg(N=245)
~6 mg/kg(N=249)
Combined(N=494)
UNITI-1
Pro
po
rtio
n o
f su
bje
cts
(%)
Ustekinumab
p=0.002 p=0.003 p<0.001
AMM: Bolus iv

Ustekinumab et Crohn: rémission à la 44ieme
semaine
35,9
48,853,1
0
20
40
60
80
100
Placebo SC*(N=131)
90 mg SC q12w(N=129)
90 mg SC q8w(N=128)
Pro
po
rtio
n o
f su
bje
cts
(%)
p=0.040p=0.005
14
Δ 12.9%Δ 17.2%
Ustekinumab
Feagn B et al. NEJM 2016 AMM: entretien sc toutes les 8 ou 12 semaines

Vascular permeability
Blood
vessel
Gut submucosa
Vedolizumab
Ly
α4β7
Soler D, Chapman T, Yang L-L, et al. J Pharmacol Exp Ther 2009;330(3):864–875.
Inhibition spécifique interaction
α4β7/MADCAM1
von Andrian UH, N Engl J Med 2000;343(14):1020–1034.
Vedolizumab = Entyvio® – Anti intégrine α4β7
Lymphocyte
Tethering Rolling ArrestActivation Gut submucosa
Blood vessel

6,8
25,7
14,5
31,4
0
5
10
15
20
25
30
35
Clinical remission CDAI-100 response
Pat
ien
ts, %
PBO (n=148)
VDZ (n=220)
p=0.02
p=0.23
CDAI-100 response
• Entyvio® = VedolizumabAMM
et remboursement : RCH et Crohn
AMM et remboursement : RCH et Crohn
Voie intraveineuseInduction puis entretien 300 mg/8S
Feagan BG, N Engl J Med 2013;369(8):699–710Sandborn WJ, N Eng J Med 2013;369:711–721.
23,819,8
8,7
56,651,6
20,5
52.056.0
24.0
0
10
20
30
40
50
60
Durable clinical response Mucosal healing Durable clinical remission
VDZ/PBO (n=126)VDZ Q8W (n=122)VDZ Q4W (n=125)
Pat
ien
ts, %
p<0.001 p<0.001
p=0.008
p=0.001
p<0.001 p<0.001
RCH S52
MC S6MC S52

Spadaccini M, et al. Int. J. Mol. Sci. 2017, 18, 1276
Sandborn WJ, et al. N Engl J Med 2016;374:1754–1762
Peyrin-Biroulet L, et al. Autoimmun Rev 2017;16:495–503.
L’arrivée des petites molécules par voie orale
InternalisedS1P1R
ExternalS1P1
JAK
stat P-stat
PDE4
cAMP AMP
apremilast3
ozanimod4
etrasimod5,6
tofacitinib1
filgotinib1
upadacitinib1,2
Internal S1P1
Cytokines Immune cells

Sandborn W, et al. N Engl J Med 2017;376:1723–1736
Tofacitinib, inhibiteur panJAK: Phase III dans la RCH
P=0.007 P<0.001
8,218,5
3,6
16,6
0
20
40
60
80
100
Placebo (n=122)
tofacitinib10 mg
(n=476)
Placebo (n=112)
tofacitinib10 mg
(n=429)
11,1
34,340,6
0
20
40
60
80
100
Placebo (n=198)
tofacitinib5 mg
(n=198)
tofacitinib10 mg
(n=197)
15,6
31,3
11,6
28,4
0
20
40
60
80
100
Placebo (n=122)
tofacitinib10 mg
(n=476)
Placebo (n=112)
tofacitinib10 mg
(n=429)
13,1
37,445,7
0
20
40
60
80
100
Placebo (n=198)
tofacitinib5 mg
(n=198)
tofacitinib10 mg
(n=197)
Pa
tie
nts
(%
)P
atie
nts
(%
) Week 8
OCTAVE Induction 1 OCTAVE Induction 2 OCTAVE Sustain
Week 52
P<0.001P<0.001
P<0.001 P<0.001P<0.001
P<0.001
Endoscopic remission
Clinical remission
Nom commercial XeljanzAMM et remboursement dans la PR

Nouvelles approches : cellules souches
51,5
35,6
0
20
40
60
80
100
Cx601 Control
Pati
ents
, %
Δ= 15.8 percentage pointsP=0.021
53/103 36/101
56,3
38,6
0
20
40
60
80
100
Cx601 Control
Pati
ents
, %
Δ= 17.7 percentage pointsP=0.010
Des cellules souches d’origine graisseuses
Co
mb
ined
clin
ical
an
d M
RI r
emis
sio
n
Panes J et al. Lancet 2017 and Gastroenterology 2018Panes J et al. Nat Rev Gastroenterol Hepatol 2017

conclusion