
Michael Messmer DO, CAQSM Beacon Medical Group … Annual...lecture. Differs from ... Image courtesy...
70
Michael Messmer DO, CAQSM Beacon Medical Group Sports Medicine
Transcript of Michael Messmer DO, CAQSM Beacon Medical Group … Annual...lecture. Differs from ... Image courtesy...
Michael Messmer DO, CAQSM
Beacon Medical Group Sports Medicine

I have no disclosures to reveal for this lecture.

Differs from tendinitis which is a more acute inflammatory disease state of the tendon.
Chronic tendinopathy is described as an overuse syndrome manifested with pain and tenderness due to mucoid and chondroid degeneration and formation of plump tenocytes and increased myofibroblastic and fibroblastic cells with absent inflammatory cells (1). It is reported that chronic painful tendinopathy exhibits increased occurrence of sprouting nonvascular sensory, substance P-positive nerve fibers, and altered sensory-sympathetic innervation which may play a role in the pathogenesis of it (2).

1) Reactive tendinopathy – occurs in response to acute overload. Non-inflammatory proliferative response. Shifting to larger modular proteoglycans. Tendons increase in size/thickness.
2) Tendon disrepair – Or failed healing. Resembles reactive tendinopathy but with greater matrix disorganization. Neovascularity and neuronal growth representing attempted but failed repair. Evidence exists here that in this stage with inclusive load modulation and eccentric exercise stimulus, the tendon can recover.
3) Degenerative tendinopathy – True tendinosis. Final stage of this continuum. Vast areas of hypocellularity, pooling of PG’s, and severely disorganized collagen. This stage is irreversible with Physical therapy and/or oral NSAIDs etc. Usually at this point intervention with regenerative medicine or surgery is necessary at this point.

Examples:◦ Lateral epicondylitis – effect 1-2% of the general
population. 2-3 times higher rate in patients over 40 years.
◦ Patellar tendinopathy – 6% of athletes (active people) effected, higher rates in jumping and sprinting sports or activities (e.g. plyometrics, cross fit, P90x etc.).
◦ Achilles tendinopathy – In a study by Kvist M. (19), 698 patients with achilles pain showed 66% with paratenonitis, 23% with achilles insertional problems. 89% were men, 53% were casual to competitive runners.
Define tendinopathy
Discuss various treatments of tendinopathy of the upper extremities
Discuss various treatments of tendinopathy of the lower extremities.
Discuss treatments that are falling out of favor in certain areas.
Learn new methods of treatments for chronic tendon pain.

Confluence of tendons including supraspinatous, infraspinatous, and teresminor at the greater tuberosity of the humerus. Also has the subscapularis tendon attaching on the lesser tuberosity.

Occurs most often at the insertion of the supraspinatous. Less likely to occur at the insertion of the teres minor.
Image courtesy of Physiopedia. http://www.physio-pedia.com/File:Schema_rotator_cuff_tendinopathy.png
RICE: Rest, Ice, Compression, Elevation◦ Rest should be relative. Use of pendulum exercises is warranted to
prevent frozen shoulder. Avoid sling if at all possible. If too painful, can go in sling for 1-2 weeks, but come out once an hour for pendulum exercises.
◦ Ice should be 10-20 minutes at the area of maximal pain. Can do this as much as possible. Make sure to let skin warm up completely before re-applying to avoid frost bite
◦ Compression is tough to do on the shoulder◦ Elevation only necessary if significant swelling. Resting forearm on head
for 1-5 minutes can help in this case
NSAIDS◦ Make sure no previous issues with bleeding or stomach ulcerations. ◦ Ibuprofen or Aleve in most cases works better then tylenol for it’s anti-
inflammatory effects. But make sure not to overuse. Some of the inflammatory cascade is important, and we don’t want to prevent it altogether. Recent research suggests there may be detrimental effects to use of NSAIDs in acute injuries (3).

Physical therapy
Specific modalities and exercises include:◦ Astym directed at the insertion
and scapular muscles◦ Cross friction massage directed at
the insertion◦ Spencer’s techniques◦ Rhomboid muscle stretch◦ Scapular stabilization exercises for
dyskinesia◦ Controlled ER and IR exercises
with the theraband◦ BOSU ball exercises◦ Wall walking◦ Core strengthening for throwers
with education on use of core when throwing
◦ Game ready ice therapy

Steroid injection (Kenalog, Depo Medrol, Celestone)
In most cases this is subacromial due to impingement and needle should be directed at the bursa. Use of Ultrasound is recommended to guarantee proper placement of the substrate
Sometimes GH injections of steroid are helpful to decrease capsular inflammation and help with proprioception of the rotator cuff muscles. This has a gold standard of Ultrasound use for guidance due to depth of the joint.

Coombes and colleagues conducted a meta-analysis on the effect of corticosteroids in various tendons in comparison with other nonsurgical interventions. Short-term effectiveness for rotator cuff tendon was inconclusive, and no significant difference was noted regarding intermediate and long-term results (4).

Healing and repair of a tendon occurs in 3 stages. The inflammatory phase in the first few days is characterized by inflammation and migration of erythrocytes and polymorphonuclear leukocytes. Monocytes and macrophages are also present for phagocytosis of necrotic tissue. Chemokines are released, leading to chemotaxis of tenocytes, which lay down collagen III.
This process is followed by the proliferative phase, which is characterized by more collagen III and increased ground substance,lasting several weeks.
From week 6 up to 1 year, remodeling takes place. Collagen I is synthesized along the path of stress (which is why physical therapy is so important), followed by scar formation. Ligament and muscle injuries undergo basic stages of healing similar to those of tendons. (4)
Based on the current literature, it is my opinion that although corticosteroids may offer short-term relief of symptoms, it is likely more harmful in the long term due to its interference in the cascade outlined above.

What I do: If I can, with good confidence, say that clinically, or with imaging there is a bursitis in the shoulder, and I am confident in my injection skills, a steroid injection into the bursa can be done. If I think there may be a tear of some kind in the rotator cuff (in particular an acute or subacute tear), then a steroid injection is not warranted.

Physical Therapy
Alternative injections:◦ Prolotherapy
◦ Platelet rich plasma
◦ Stem Cell injections

ROM To help capsular motion – I will encompass Spencer’s techniques in if I am confident in the capsular integrity
Strengthening of the rotator cuff tendons with proper eccentric and concentric loads given at the right time of remodeling to encourage proper tendon fiber deposition
Scapular motion control –essential to prevent furtehrinjury to the tendon

Prolotherapy: introduces an irritating agent to pathologic tissue to obtain a healing response (5). It is a homeopathic remedy intended not to “cure” an injury, but to stimulate the body to heal itself.
Chemical irritants - such as phenol, guaiacol or tannic acid, trigger the healing process. These substances attach themselves to the walls of the cells wherever they are injected, causing irritation that stimulates the body’s reactive healing process
Chemotactic agents – Primarily sodium morrhuate are thought to be proliferants used to attract immune cells to the area.
Osmotic Shock agents - simple compounds like dextrose and glycerine. The most commonly used prolotherapy agents, work by causing cells to dehydrate slightly which stimulates the immune response.
Particulates – Pumice flour is most commonly used. microscopic particles that attract macrophages, tiny organisms which gobble them up, in turn secreting polypetidegrowth factors that result in collagen production. Collagen production is an essential event in phase 3 of the healing response.

Platelet Rich Plasma Therapy
Defined as an ultrafiltrate of deposited autologous whole blood with a platelet count above baseline values (6). Platelet concentrations will vary from 2.5-8 times the normal concentration depending on the commercial centrifuge used.
When these platelets release their contents, there is a 3- to 5-fold increase in the number of growth factors, including platelet-derived growth factor (PDGF), transforming growth factor b (TGF-b), vascular endothelial growth factor (VEGF), basic fibroblast growth factor (bFGF), epidermal growth factor (EGF), and insulin-like growth factor (IGF). These growth factors act as powerful chemoattractants, are involved in cell proliferation and immune cell regulation, and can stimulate endothelial growth and angiogenesis (6),(7).
Numerous studies have demonstrated the ability of PRP to heal damaged tissue. These included medial collateral ligament injuries of the knee,(8) chronic elbow tendinitis, (9) Achilles tendon tears, (10) (11) bone healing, (12) muscle strains, (13) patellar tendinopathy,(14) (15) and rotator cuff repair (16) (17).
Platelet count?
Leukocyte count? New literature suggests leukocyte poor (specifically neutrophils) may be more effective for tendons and even joints.
RBC count? – less worrisome, seems to contribute more to pain response.
Ultrasound guidance vs. Landmark guided injections?
Most effective at which areas? Tendon, joint, ligament?
Acute vs. Chronic injuries?

Percutaneous needle tenotomy: Otherwise known (inaccurately) as “dry needling”. It involves introduction of a needle at an area of damage in a tendon or ligament using ultrasound for precise placement of the needle and performing multiple passes through 50% of the tendon thickness to induce inflammatory (and therefore healing) response.
A recent study by Dong-wook et al. Showed effectiveness in range of motion, pain, and disability (18).

Stem Cell injections: There are various sources of stem cells that have been used for a variety of medical
conditions, ranging from embryonic stem cells to human adult stem cells.
Embryonic stem cell therapy is subject to significant regulatory and religious issues with potential adverse effects, with no studies supporting its use for orthopedic conditions.
Human adult stem cells are available from various tissues including blood, adipose, bone marrow, and synovial tissue. The literature would support bone marrow as the main source and having most published research for orthopedic conditions. (20)
Harvesting mesenchymal stem cells (MSCs) from bone marrow is also associated with a lower complication rate in comparison with adipose-derived stem cell extraction.
The multipotent nature of MSCs allows them to differentiate into various cells in the mesenchymal lineage, including bone, cartilage, adipose, and other soft tissues.
Centeno and colleagues showed that stem cells were effective for severe OA in one patient they injected for a case report. The investigators found that after BMAC containing MSCs were injected into hips and knees, MRI’s confirmed thickening of cartilage within the joint space after 4 weeks in the hip as well as thickening of meniscus and cartilage in the knees after 24 weeks. Patient reported increased movement and decreased pain. (21)(22)
Most literature on stem cells is limited to case reports and animal studies. Therefore, this is still in the experimental phase as many physicians around the country are currently undergoing many studies to help further this therapy

Inflammation and irritation with possible partial tear of the common extensor tendon at the lateral epicondyle
Commonly seen in patients who do many repetitive low impact activities (i.e. typing) or short burst aggressive movements involving wrist extension (i.e. throwing boxes, or swinging a tennis racquet).

1st step: NSAIDs with icing and resting
2nd step: Home exercises for stretching the extensors and increasing grip strength
3rd step: Gradual return to work
This conservative management works fairly well in most patients. 80% of patients will improve with this strategy (23)

Physical therapy: (24) Progressive Exercise Program,
Steps 1 to 4
Step Exercises:
1 Clenching fist strongly
Resisted wrist extension
Resisted wrist flexion
Wrist rotation with a stick
Toward the little finger
Toward the thumb
End: stretching at least 30 seconds to flexion and
Extension
2 Exercises against an elastic band for:
Wrist extension
Wrist flexion
Wrist radial deviation
Wrist ulnar deviation
End: stretching as in step 1, 10 × 3 series, several repetitions daily
3 Combined wrist rotary movements using, for example, a table top as a support
Upward resisted from below
Toward the little finger
Toward the thumb
Downward resisted from above
Toward the little finger
Toward the thumb
Pressing hand against a wall
End: stretching as in step 2
4 An occupational training program including:
Softball compressing exercises
Transferring buttons from 1 cup into another
Twisting a towel into a roll
Rotating hand on a table in bo

Percutaneous needle tenotomy
Very effective in pain control and healing.
Not very well tolerated by patient.
PRP injections
Highly effective to illicit healing response
Well tolerated by patient
Not covered by insurance

Steroid injection:◦ Is effective for pain control and to decrease
inflammation, but recent literature questions the efficacy and whether long term damage can occur doing these. Especially with improper placement (25).
◦ In some cases has led to worse outcomes after a year (26).
◦ At this point if a tear is not identified, and there is known inflammation that is a direct reason for the pain, then steroid injection can be considered. If this is a chronic pain, steroid should be avoided.


One of the more common tendinopathies - as many as 20% of jumping athletes
Jumper’s Knee
Inflammation of the tendon that connects the patella to the tendon-the inferior patellar pole

Mechanism of injury: ◦ no exact mechanism, subtle onset
progressive pain
Due to repetitive jumping, kicking or cutting
Risk factors: ◦ Training frequency and intensity
muscular imbalance
◦ Poor quadriceps and hamstring flexibility

Eccentric muscle action during landing may exert the tensile loads that lead to injury
Anterior knee pain - aching quality
Symptom onset is insidious
Physical Exam:
Point tenderness -inferior patellar pole, superior patellar pole, or tibial tuberosity
Hamstring and quadriceps tightness
Swelling may be present
Intra-articular effusion of the knee - rare
Grading System:
I. Pain only after exercise
II. Discomfort during exercise with pain after exercise ceases
III. Pain during and after exercise
IV. Rupture of Tendon

Treatment:
Rest, Ice, NSAIDs
Activity Modification
PT – Stretching (quads and hip flexors) Strengthening - closed kinetic chain and eccentric exercise
Sport-specific proprioceptive training and plyometrics
Counterforce Strap (Grade I)

Injections: Steroid, Sclerosing Agents, PRP
Steroid- Ultrasound imaging shows that steroids can reduce inflammation and edema in a tendon, but cannot repair degenerative changes (Fredberg et al, 1998)
-Steroid injections demonstrated improvements in pain scores in the short term (3/12), however improvements deteriorated in the long term (6/12) and in some cases even relapsed to their initial pain scores after 4wks (Fredberg et al (2004), Kongsgaard et al (2009) and Capasso et al (1997) )
-adverse effects including slowing and weakening of collagen synthesis leading to a higher risk of tendon rupture has been shown with the use of repeated steroid injections
Sclerosing injections
Sclerosis, the act of injecting a chemical irritant
(e.g. polidocanol) into the tendon, is thought to
destroy the neovessles and accompanying
nerves, thus ridding the patient of pain.
Alfredson and Ohberg (2005): significant reductions in pain during activity, and increases in knee function up to 4/12 post treatment

PRP Platelet rich plasma (PRP) is blood plasma
enriched with platelets containing growth factors, and is utilized to stimulate soft tissue healing with low healing potential.
Volpi et al (2007), Kon et al (2009) and Filardo et al (2010) investigated the use of PRP injections combined with varying exercise and stretching programs they showed significant reductions in pain and, in some cases, an improvement in regeneration of the tendon tissue


inflammation of the tendon or paratendon
resulting from overuse, or hyperextension injury
change in playing surface, footwear, or intensity of an activity


Risk Factors:
Achilles tightness
Excessive pronation
Compensatory posturing up and down the kinetic chain such as hip external rotation
Functional genurecurvatum
Midtarsal rotation
Associated Sports:
Runners
Gymnasts
Cyclists
Volleyball
Tendon subjected to 8-10x
a person's body weight
during strenuous exercise

Presentation:
Paratenonitis: Localized/burning pain during or following activity occurs; as the disease progresses, onset of pain may occur earlier during activity, with decreased activity level, or even at rest.
Tendinosis: Usually, this injury is an asymptomatic, noninflammatory, degenerative disease process (mucoid degeneration); the patient may complain of a sensation of fullness or a nodule in the back of the leg
Paratenonitis with tendinosis: Activity-related pain and diffuse swelling of the tendon sheath with nodularity is present

Exam:
Tendinosis: is often pain free; may be palpable intratendinous nodule that accompanies the tendon
Paratenonitis: typically present with warmth, swelling, and diffuse tenderness localized 2-6 cm proximal to the tendon's insertion; crepitation may be present
Paratenonitis with tendinosis: patients with activity-related pain, as well as swelling of the tendon sheath and tendon nodularity.

Treatment:
- Relative rest, Icing, NSAIDs, cross training ok
- Runners reducing mileage and eliminating hills for a while
- Crutches, walking cast or boot may be needed for a short time
- Physical Therapy eccentric exercises, with most patients achieving 60-80% pain relief
- Night splint (Strassburg sock) - ankle at 5°dorsiflexion

Glyceryl Trinitrate Patches
Theory: dilates blood vessels leading to increased blood flow; increases levels of NO which may stimulate healing
Regiment: off-label use of an FDA-approved medication ¼ patch 0.2mg/hr for 18-24hrs,6mth duration
Side Affects: HA

Achilles tendinopathy - showed 78% of the treatment group asymptomatic with activities of daily living at 6 months versus 49% of the control group (Paolini 2003)
At 3 years, 88% of the treatment group was completely asymptomatic compared to 67% of the control group (Paolini 2007)

Injections:
Several cases of Achilles tendon rupture have beenreported after corticosteroid injections to this
region(Bedi SS, Ellis W.; Kleinman M)
Gill et al. described a series of 83 injections to theAchilles region without serious complicationinjected the steroid under fluoroscopic guidance around the tendon but not within the substance of the tendon.

Platelet rich plasma – Can be effective in the treatment for chronic recalcitrant Achilles tendinosis. This was seen in a recent study by Monto (2012) showing 27 out of 29 patients getting clinical resolution in the 6 month follow up.


1 million visits per year in the US
most cases are from overuse stresses
degenerative irritation at the insertion of the plantar fascia on the medial process of the calcaneal tuberosity
Heel spur partial association
…however asymptomatic individuals have bony heel spurs, whereas many patients with plantar fasciitis do not have a spur

3 distinct parts: medialcentrallateral
development of microtrauma damage at the calcaneal-fascial interface secondary to repetitive stressing of the arch with weight bearing
Risks:multifactorialTraining errors, pes planus, overpronation, pes cavus,tightness in the hamstrings, gastrocnemius, soleus,overweight, DM, etc…
Key Findings:
- worse pain with 1st step in the AM
- pain with barefoot walking
- no symptoms & signs of neurologic involvement
- pain and tenderness over plantar fascia origin; tight achilles

Treatment:- Rest, Ice, Stretching, NSAIDs
- Night Splints
- Proper foot support – orthotics, arch support
- Injections
- ESWT

Injections: majority of studies show short term effect for steroid injections
- Crawford et al 106 patients, decrease in pain levels steroid after 1 month; however, after 3 months there was no statistical significant difference concluded that steroid injections can provide short-term relief

ESWT (Extracorporeal shockwave therapy
FDA-approved for plantar fasciitis
Entails delivering a series of low-energy shock waves directly over the painful area of the tendon.
The mechanism by which ESWT would provide pain relief or enhance tendon healing is not clear
About 34 clinical trials and systematic reviews investigating ESWT- half favorable and half neutral
Most convincing data are seen in the treatment of calcific tendonitis
Twenty patients had ESWT and 75% of patients were completely satisfied at six month post treatment with an ESWT device that required local anesthesia (Othman et al)
Haake et al. Assessed the efficacy of extracorporeal shockwave therapy (ESWT) in 272 subjects; Consequently, they showed that ESWT was ‘ineffective in the treatment of chronic plantar fasciitis’

Percutaneous tenotomy – microtiptenotomy/fasciotomy
What is it?
New technology delivers optimized ultrasonic energy to end of Microtip that precisely cuts diseased tendon tissue while sparing healthy tissue
Cutting of tissue achieved through longitudinal movement of needle at speed of sound (ultrasonic) – cut tissue at tip only via “jack-hammer effect”
Continuous saline irrigation cools Microtip to control unwanted heat and coupled to simultaneous removal of target tissue
Effectively, diseased or ineffective tissue is removed in a percutaneous fashion with minimal side effects.


Shoulder –rotator cuff tendinosis or calcific tendinosis
Elbow – lateral epicondylosis
Knee – patellar tendinosis
Foot – plantar fasciosis
Ankle – achillestendinosis
Proximal hamstring tendinosis
Gluteus mediustendinosis
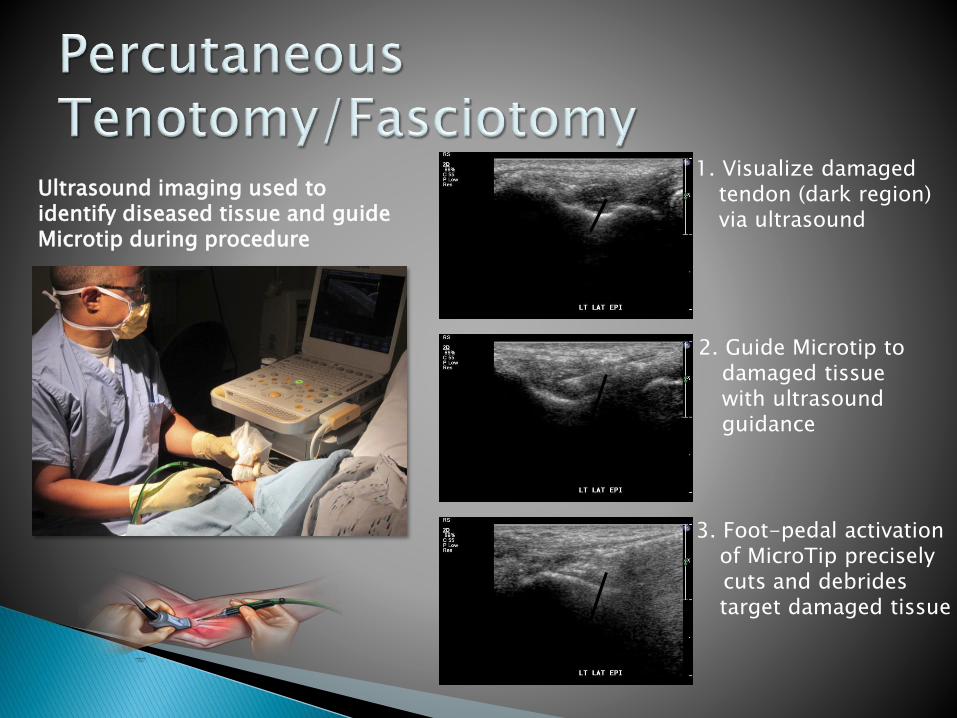
Ultrasound imaging used to identify diseased tissue and guide Microtip during procedure Diseased tendon tissue
TX1 MicroTip placed intohypoechoic region
Removal of hypoechoic region
1. Visualize damaged tendon (dark region) via ultrasound
3. Foot-pedal activation of MicroTip preciselycuts and debrides target damaged tissue
2. Guide Microtip to damaged tissue with ultrasound guidance

Extent of incision – 1cm

Chronic pain (> 3 months) at the affected joint and not responsive to conservative medical treatment (rest, ice, brace, physical therapy)
Point tenderness – point of maximum pain typically corresponds to the location of the damaged tissue and can be identified one finger by the patient
Ultrasound confirmation – placement of ultrasound transducer on the site of maximum tenderness should identify a region of degenerated tendon tissue visualized as a hypoechoic region due to irregular/disorganized fibers and thickened tendon tissue.
No restrictions before procedure
Total procedure time from cleaning of skin to placing band-aid is less than 20 min.
No pain or discomfort during procedure
Permitted to go home afterwards - no PT
Post-procedure …• Over-the-counter pain meds and ice as
needed• Refrain from heavy lifting or in boot for 2
weeks• Return to full activity in 4 to 6 weeks (if
some comorbidities can be 8-12 weeks in my experience)

Published/Accepted Koh et al – Am. Journal of Sports Medicine,2013 (elbow)
Hackel – Orthopedics Today 2013 (procedure overview / mixed tendons)
Morrey – Techniques in Elbow and Hand Surgery 2013 (elbow)
ElAttrache – Operative Techniques in Sports Medicine 2013 (knee)
Barnes – Operative Techniques in Sports Medicine 2013 (procedure overview/mixed tendons)
Khanna et al – Am Academy of Physical Med & Rehab Poster 2013 (mixed tendons)
Traister et al – Am Med Society for Sports Medicine Presentation 2014 (mixed tendons)
Barnes et al – Journal of Shoulder and Elbow Surgery 2014 (elbow)
Patel – in print, American Journal of Orthopedics 2014 (plantar fascia)
Mayo Clinic Epidemiology study – in print, American Journal of Sports Medicine 2014 (elbow)
Stowers – accepted, Orthopedics (knee)
Submitted/In Preparation Kamineni (Univ. of KY) – Controlled animal model study
Koh et al (Singapore/Mayo) – Two year clinical efficacy and safety follow-up in elbow tendonosis
Yanish (Des Moines, IA) – Cost effectiveness study: Tenex vs Surgery (elbow)
Vanderwoude (Lincoln, NE) – Plantar fascia study
Ellis et al (Phoenix, AZ) – Achilles tendon study
Patel (Indianapolis) – Plantar fibroma study

Elbow: Prospective studies (2) revealed > 90% patients pain free – 12 & 24 month follow-upStatistical significant improvement in quality of life (QOL) measurement vs baseline
Knee/Patellar: Clinical evaluations (2) revealed 93 % patient pain free – 6 month follow-upStatistical significant improvement in QOL measurement vs baseline
Achilles: Prospective study revealed 91% patients pain free – 12 month follow-upStatistical significant improvement in QOL measurement vs baseline
Plantar Fascia: Case evaluation revealed 92% patients pain free – 6 month follow-upStatistical significant improvement in QOL measurement vs baseline
Animal Model: Precise removal of damaged tendon tissue leaving healthy tissue intactRemodeled tendon has physical and biochemical make-up of healthy tissue
Economic Analysis: Efficacy (6 month follow-up): Tenex = 91% vs Open = 74 % Average work weeks missed: Tenex = 1.1 vs Open = 8.2
Total cost savings/patient: Tenex was $ 11,753 less than Surgery

1. Wang CJ, Ko JY, Chan YS, Weng LH, Hsu SL: Extracorporeal shockwave for chronic patellar tendinopathy. Am J Sports Med 2007, 35(6): 972-8
2. Lian O, Dahl J, Ackermann PW, Frihagen F, Engebretsen L, Bahr R: Pronociceptive and antinociceptive neuromediators in patellar tendinopathy. Am J Sports Med 2006, 34(11): 1801-8.
3. Coombes BK, Bisset L, Vicenzino B. Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: a systematic review of randomized controlled trials. Lancet 2010;376:1751–67
4. Coombes BK, Bisset L, Brooks P, et al. Effect of corticosteroid injection, physiotherapy, or both on clinical outcomes in patients with unilateral lateral epicondalgia: a randomized controlled trial. JAMA 2013;309(5):461–9.
5. DeChellis DM, Cortazzo MH. Regenerative medicine in the field of pain medicine: prolotherapy, platelet-rich plasma therapy, and stem cell therapy-theory and evidence. Tech Reg Anesth Pain Manag 2011;15(2):74–80
6. Hall MP, Band PA, Meislin RJ, Jazrawi LM, Cardone DA. Platelet-rich plasma: current concepts and application in sports medicine. J Am Acad Orthop Surg. 2009;17(10):602-608.
7. Lopez-Vidriero E, Goulding KA, Simon DA, Sanchez M, Johnson DH. The use of platelet-rich plasma in arthroscopy and sports medicine: optimizing the healing environment. Arthroscopy. 2010;26(2):269-278.
8. Foster TE, Puskas BL, Mandelbaum BR, Gerhardt MB, Rodeo SA. Platelet-rich plasma: from basic science to clinical applications. Am J Sports Med. 2009;37(11):2259-2272.
9. Creaney L, Wallace A, Curtis M, Connell D. Growth factor-based therapies provide additional benefit beyond physical therapy in resistant elbow tendinopathy: a prospective, single-blind, randomised trial of autologous blood injections versus platelet-rich plasma injections. Br J Sports Med. 2011;45(12):966-971
10. Sanchez M, Anitua E, Azofra J, Andia I, Padilla S, Mujika I. Comparison of surgically repaired Achilles tendon tears using platelet-rich fibrin matrices. Am J Sports Med. 2007;35(2):245-251.

11. Gaweda K, Tarczynska M, Krzyzanowski W. Treatment of Achilles tendinopathy with platelet-rich plasma. Int J Sports Med. 2010; 31(8):577-583
12. Dallari D, Savarino L, Stagni C, et al. Enhanced tibial osteotomy healing with use of bone grafts supplemented with platelet gel or platelet gel and bone marrow stromal cells. J Bone Joint Surg Am. 2007;89(11):2413-2420.
13. Hammond JW, Hinton RY, Curl LA, Muriel JM, Lovering RM. Use of autologous platelet-rich plasma to treat muscle strain injuries. Am J Sports Med. 2009;37(6):1135-1142.
14. Kon E, Filardo G, Delcogliano M, et al. Platelet-rich plasma: new clinical application. A pilot study for treatment of jumper’s knee. Injury. 2009;40(6):598-603.
15. Filardo G, Kon E, Della Villa S, Vincentelli F, Fornasari PM, Marcacci M. Use of platelet-rich plasma for the treatment of refractory jumper’s knee. Int Orthop. 2010;34(6):909-915
16. . Randelli P, Arrigoni P, Ragone V, Aliprandi A, Cabitza P. Platelet rich plasma in arthroscopic rotator cuff repair: a prospective RCT study, 2-year follow-up. J Shoulder Elbow Surg. 2011;20(4):518-528.
17. Randelli PS, Arrigoni P, Cabitza P, Volpi P, Maffulli N. Autologous platelet rich plasma for arthroscopic rotator cuff repair: a pilot study. Disabil Rehabil. 2008;30(20-22):1584-1589
18. Dong-wook Rha, Gi-Young Park, Yong-Kyun Kim, Min Tae Kim and Sang Chul Lee: Comparison of the therapeutic effects of ultrasound-guided platelet-rich plasma injection and dry needling in rotator cuff disease: a randomized controlled trial. Clinical Rehabilitation 2012, 27(2) 113–122
19. Kvist M. Achilles tendon injuries in athletes. Ann Chir Gynaecol 1991; 80:188-201
20. Steinert AF, Noth U, Tuan RS. Concepts in gene therapy for cartilage repair. Injury2008;39(Suppl 1):S97–113
21. Centeno CJ, Kisiday J, Freeman M, et al. Partial regeneration of the human hip via autologous bone marrow nucleated cell transfer: a case study. Pain Physician 2006;9:135–7.
22. Centeno CJ, Busse D, Kisiday J, et al. Increased knee cartilage volume in degenerative joint disease using percutaneously implanted, autologous mesenchymal stem cells. Pain Physician 2008;11:343–53.
23. Verhaar JA: Tennis elbow: Anatomical, epidemiological and therapeutic aspects. Int Orthop 1994;18:263-267
24. P. A. A. Struijs,*† PhD, G. M. M. J. Kerkhoffs,† MD, W. J. J. Assendelft,‡ MD, PhD, and C. N. van Dijk,† MD, PhD. Conservative Treatment of Lateral Epicondylitis Brace Versus Physical Therapy or a Combination of Both—A Randomized Clinical Trial. The American Journal of Sports Medicine 2004; 32: 462-469
25. Osborne H. Stop injecting corticosteroid into patients with tennis elbow, they are much more likely to get better by themselves! J Sci Med Sport. 2010;13(4):380-381
26. Brooke K. Coombes, PhD; Leanne Bisset, PhD; Peter Brooks, MD, FRACP; AsadKhan, PhD; Bill Vicenzino, PhD. Effect of Corticosteroid Injection, Physiotherapy, or Both on Clinical Outcomes in Patients With Unilateral Lateral Epicondylalgia A Randomized Controlled Trial. JAMA. 2013;309(5):461-469.
27. Michael F. Joseph, PhD,PT; Craig R Denegar, PhD,PT, ATC, FNATA. Treating Tendinopathy perspective on anti-inflammatory intervention and therapeutic exercise. Clinics in Sports Medicine. 2015; 34: 363-374

Capasso G, Testa V, Maffulli N. (1997) Aprotinin, corticosteroids and normosaline in the management of patellar tendinopathy in athletes: a prospective randomized study. Sports Exerc Injury; 3 :111–15
Kongsgaard, M. Kovanen, V. Aagaard, P. (2009) Corticosteroid injections, eccentric decline squat training and heavy slow resistance training in patellar tendinopathy. Scand J Med Sci Sports; 19: 790 – 802 .
Van Ark, Mathijas. Zwerver, J. van den Akker-Scheek, I. (2011) Injection treatments for patellar tendinopathy. British Journal of Sports Medicine. 45: 1068-1076
Gill SS, Gelbke MK, Mattson SL, Anderson MW, Hurwitz SR.Fluoroscopically guided low-volume peritendinous corticosteroid injection for Achilles tendinopathy. A safety study. J Boneoint Surg Am. 2004;86-A:802–806.
Bedi SS, Ellis W. Spontaneous rupture of the calcaneal tendoninrheumatoid arthritis after local steroid injection. Ann RheumDis. 1970;29:494–495.
Jonathan T. Finnoff, DO, Steven P. Fowler, MD,etc. Treatment of Chronic Tendinopathy with Ultrasound-Guided Needle Tenotomy and Platelet-Rich Plasma Injection. PM&R Vol. xx, Iss. x, 2011
Paoloni JA, Murrell GA. Three-year followup study of topical glyceryltrinitrate treatment of chronic noninsertional Achilles tendinopathy. Foot Ankle Int. 2007;28:1064–1068.
Paoloni JA, Appleyard RC, Nelson J, Murrell GA. Topical nitricoxideapplication in the treatment of chronic extensor tendinosis at the elbow: a randomized, double-blinded, placebo-controlled clinical trial. Am J Sports Med. 2003;31:915–920.
Alfredson, H. Ohberg, L. (2005) Neovascularisation in chronic painful patellar tendinosis– promising results after sclerosing neovessels outside the tendon challenge the need for surgery. Knee Surg Sports Traumatol Arthrosc; 13: 74–80
Volpi, P. Marinoni, L. Bait, C. (2007) Treatment of chronic patellar tendinosiswith buffered platelet rich plasma: a preliminary study. Kon, E. Filardo, G. Delcogliano, M. (2009) Platelet-rich plasma: new clinical application: a pilot study for treatment of jumper’s knee. Injury; 40: 598 – 603.Med Sport; 60: 595–603.
Filardo, G. Kon, E. Della Villa, S. (2010) Use of platelet-rich plasma for the treatment of refractory jumper’s knee. Int Orthop; 34: 909 – 15.

Paoloni, J., de Vos, R.J., Hamilton, B., et al. Platelet rich plasma treatment for ligament and tendon injuries. Clin J Sport Med, Vol 21, (2011), pp. 37-45
Rompe JD, Nafe B, Furia JP, Maffulli N. Eccentric loading,shock-wave treatment, or a wait-and-see policy for tendinopathyof the main body of tendo Achillis: a randomized controlled trial. Am J Sports Med. 2007;35:374–383
Monto, RR. Platelet rich plasma treatment for chronic achillestendinosis. Foot and Ankle Int, Vol 33 (5), (2012), pp. 379-85.









![Cervicogenic Headache - Physiopedia · Another possibility to distinguish cervicogenic headache from migraine and tension headache is the use of a Cybex dynamometry. [20] Testing](https://static.fdocuments.net/doc/165x107/5cc7f9b088c993c4398ca482/cervicogenic-headache-physiopedia-another-possibility-to-distinguish-cervicogenic.jpg)









{kind=link}