Miad CD4_14 greymatters
24
Volume 1, Issue 1 November 1, 2015 Overdiagnosis in America American mental health
-
Upload
paul-siebers -
Category
Documents
-
view
232 -
download
0
description
Â
Transcript of Miad CD4_14 greymatters

Volume 1, Issue 1 November 1, 2015
Overdiagnosis in America
American mental health

INTERVIEW WITH DR PIES
MENTAL HEALTHNOT FOR EVERYONEWritten Susan Brink
Mix mental illness with politics and the business of health insurance, then add heavy doses of stigma. it’s not surprising that providing mental treatment is complicated as ever.
Grey Matters Issue 1
TABLE OF CONTENTS
AMHCAINFOGRAPHIC
VETRANSKICK HABBITWritten Quil LawrencePhotography Paul Siebers
For many people with post-traumatic stress disorder, sleeping can return you to the worst place you’ve ever been, at the worst possible moment.
ADHD KIDWritten Kayla MasseyIllustrations Amber Pokphahn
The diagnosis and medication of mental health disoreders in children has skyrocketed in the last few years. In the US, more and more children are being put on medications for disorders such as ADHD at increasingly younger ages.

Grey Matters Issue 1
LETTER TO THE EDTIOR
THE EDITORHi my name is Paul Siebers. I care about mental
health problems. I care about America. This
magazine is a combination of my two loves. The
aim is to help people make informed opinions
about navigating our countries dizzying policies
and opinions about the ever changing state of
caring for our greatest asset, the brain.

S e v e r a l s t at e s a r e t r y i n g n ew
e x p e r i m e n t s t o e n s u r e c o m p l e t e
c o v e r a g e , o t h e r s o p t o u t a l t o g e t h e r .
Mental Health now covered Under ACA, but
Not for Everyone By Susan Brink
5

What amount of humanity is obscured by the letter of the law?

“Nearly 4 million uninsured people with mental health conditions will be locked out of the health insurance system”
—Joel Miller, American Mental Health Counselors Association
Mix mental illness with politics and the business of health insurance, add heavy doses of stigma and judgment, and it’s not surprising that providing mental and behavioral health treatment is as complicated as ever, despite promising language in the Affordable Care Act.
Provisions of the new law, along with the 2008 Mental Health Parity Act, represent the latest attempts to provide preventive services and comprehensive treatment for mental health that is equivalent to that provided for physical health. No oncologist would say, “You’re entitled to 10 treatments, and then your cancer coverage stops.” Yet that’s exactly what mental health patients have heard. No cardiologist would tell a patient, “If you relapse into high blood pressure, your treatment is considered a failure.” And yet that’s been the message to alcohol and drug addicts.
The law makes mental and behavioral health treatment one of 10 essential benefits required in new insurance policies sold on the federal health exchange as well as to patients on Medicaid. That provides a promising path toward comprehensive coverage of mental illness, equal to that of medical and surgical needs.
But coverage of care for disorders including schizophrenia, depression, bipolar disorder, childhood behavioral disorders and addiction are far from assured for all Americans.
For now, mental health coverage is rife with state-by-state disparities; and within states, attempts to include it range from almost nonexistent to a variety of creative experiments with Medicaid coverage.
“Health care systems and hospitals are expecting tsunamic change,” says Dr. Michael May, a psychiatrist, as well as vice president and medical director of Samaritan Mental Health in Corvallis, Ore. “Everybody is positioning themselves. I don’t think people realize the incredible disruption this is bringing to the health care system.”
There is at least some immediate good news from the ACA that people with mental illness can count on, regardless of where they live. The law allows young adults, up to age 26, to remain on their parents’ health plans — a major boon because half of all mental health and substance abuse conditions begin by age 14, and three-quarters begin by the age of 24. Another
provision of the act prevents insurance companies from denying coverage to people with pre-existing conditions, including schizophrenia, depression, bipolar disorder or drug or alcohol dependence.
But once people are screened and diagnosed, they and their families may run into the same frustrations as always shortages of mental health providers and treatment facilities and gaps in insurance coverage.
In some places, change is slowly coming as health care delivery systems experiment with ways that may begin to improve mental health care. Many of those changes go by various names: Accountable Care Organizations, Patient-Centered Medical Homes and Community Care Organizations. Regardless of the name, a team composed of a variety of health care experts works together to help each patient. For mental health treatment to gain true equality with treatment for physical ailments, psychiatrists, psychologists, social workers and behavioral treatment experts are beginning to be incorporated.
Stigma of Mental Illness a Barrier
The stigma often associated with mental illness prevents many people from getting the care they need, new research shows.
Although one in four people has some form of mental health disorder, the study found that in Europe and the United States, up to 75 percent of those affected do not receive the treatment they need. If left untreated certain mental health problems — such as psychosis, depression, bipolar disorder and anxiety disorder — could get worse, researchers warned.
“We now have clear evidence that stigma has a toxic effect by preventing people seeking help for mental health problems,” Dr. Graham Thornicroft, senior study author at the Institute of Psychiatry of King’s College London, said in a college news release. “The profound reluctance to be ‘a mental health patient’ means people will put off seeing a doctor for months, years, or even at all, which in turn delays their recovery.”
For the study, published Feb. 25 in Psychological Medicine, the researchers collected information from 144 studies involving 90,000 people around the world.Stigma ranked as the fourth highest of 10 barriers to care. Aside from the stigma of using mental health services or being treated for mental illness, the participants also reported feelings of shame and embarrassment.

Others were afraid to let anyone know they have a mental health issue or were concerned about confidentiality.
Some people with mental illness either felt they could handle their problem on their own or believed they didn’t actually need help, the study also found. Among those most affected by the stigma associated with mental illness were young people, those from minority ethnic groups, members of the military and health care professionals.
“Our study clearly demonstrates that mental health stigma plays an important role in preventing people from accessing treatment,” Dr. Sarah Clement, lead study author, also with the Institute of Psychiatry, said in the news release.
“We found that the fear of disclosing a mental health condition was a particularly common barrier,” Clement said. “Supporting people to talk about their mental health problems, for example through anti-stigma campaigns, may mean they are more likely to seek help.”
states exper iment
w i th coverageAmerica’s health care system has long been segmented, but whether people had private insurance, or were covered by a government program, the structure was the same: one set of billing codes covered physical health, another mental health and still another behavioral health.
“Say someone is admitted to the hospital with a drug overdose,” says May. “There was a constant tension between payment mechanisms.”
Would the overdose be coded as a substance abuse problem, making it a behavioral issue? Or would it be seen as a suicide attempt, a mental health problem? And what about an underlying physical condition like diabetes?
“It was a morass trying to figure out pay-ment, and everybody wanted to pass it off,”
Now, at least for Medicaid patients in Oregon, funding is going to 15 regional CCOs to cover all patient needs. Paid a set sum for each patient, the providers have a financial stake in keeping people healthy by stabilizing them and keeping them out of hospitals and emergency rooms.
“One entity is paying for all of it from the same bucket. It helps a lot with coordination,” says May.
Similar group structuring is taking place is several other states including Colorado, Massachusetts, Minnesota, New Jersey and Vermont. It is shaping up as a huge national experiment, giving providers a financial incentive to work together and making the whole team jointly account-able for the health of patients. Hospitals are buying up physician groups even as those physician groups are adding nurse practitioners, physician assistants, health care managers, dietitians, and other providers to form teams of care. Signifi-cantly, they’re also adding mental health experts. Overall, some 14 percent of Americans get their health care through an ACO, and the movement is growing.
Proving that a team approach to care can be financially viable while delivering quality mental health care remains a challenge. Evidence, however, is trickling in. Look no further than the Montefiore Medical Center in the Bronx — one of the most economically disadvantaged regions in the United States. It was one of 33 demonstration projects the Centers for Medicare and Medicaid Services tested for quality and efficiency of team care to address the physical, mental and behavioral health of patients.
“They made money in their first year,” says Rebecca Chickey, director of the American Hospital Association’s Section for Psychiatric and Substance Abuse Services. “Their chief medical officer is a psychiatrist, they put a heavy emphasis on prevention and early intervention, and they had someone who worked with patients in the community.”
Still, many uninsured Americans who are mentally ill or addicted to drugs or alcohol will continue to be left out of coverage.
Overall 21 states have refused the ACA’s provision to expand Medicaid coverage for citizens of their states, following the Supreme Court’s 2012 ruling allowing states to opt out. The District of Columbia and 26 states are expanding Medicaid, and three states are considering expansion.Mental health patients who would qualify for Medicaid but reside in those opting out states are finding themselves living in the wrong place at the wrong time.
“Nearly 4 million uninsured people with mental health conditions will be locked out of the health insurance system, and therefore lack access to timely, quality mental health services and a consistent source of care,” says Joel Miller, executive director of the AMA. “They will see their hopes dashed for a better life and better health.”
2.7Numbers, in millions, of uninsured Americans with serious mental illness.
—Koiser Family Foundation

Still others who buy commercial insurance will fall through the cracks because of how they get their health insurance.
For example, making mental health coverage one of 10 essential benefits to be included in insurance coverage originally meant all policies sold on the individual market or through the exchanges would cover a wide range of support. Included in this additional assistance would be mental and behavioral health screenings, primary prevention, stabilization of symptoms, chronic care and support through provider visits, telephone calls or email support.
“In theory, that represented a huge advance,” says John Bartlett, a psychiatrist and senior project advisor of the Primary Care Initiative of the Mental Health Program at the Carter Center in Atlanta. In practice, though, 16 states and the District of Columbia have chosen to set up their own health exchanges, and can determine their own essential benefits.
“Those states have largely chosen minimal mental health benefits” adds Bartlett. And some employer-based plans can have older, less generous mental health benefits grandfathered in.
Providers in some states, like Oregon, are cautiously optimistic. Even before the ACA took effect, Oregon created 15 regional community care organizations, teams prepared to care for all the physical, mental and behavioral needs of Medicaid patients. Those organizations are signing up people even faster than they expected.
“Last year, we had 32,000 covered lives,” says Robin Henderson, psychologist and Chief Behavior Health Officer of the St. Charles Health System in Bend, Ore. “By March 1, 2014, that number had increased to over 14,000 people.”
That means 14,000 newly insured patients will have access to comprehensive mental health coverage. A lot of work remains, not the least of which is increasing the number of mental health providers and hospital beds available to provide treatment. But Henderson remains positive.Editorial cartoon on health care exchanges and obamacare
“People who have coverage now and didn’t before the Medicaid expansion are able to get care without showing up at the emergency room,” she says.
Across the country, when a mental or behavioral health crisis hits, families will still be reading the fine print of their policies. Parents of an 8-year-old who needs a behavioral assessment may or may not have appropriate coverage for treatment. A 22-year-old college student suffering his first schizophrenic episode might be grateful to still be on his parents’ health plan, but reimbursement for ongoing treatment isn’t a sure thing. A 30-year-old with depression can be certain that the illness cannot be the grounds for denial of a future insurance policy; but payment for her ongoing therapy isn’t guaranteed.
Despite the complications, Henderson and May count themselves among those who believe that the ACA is step in the right direction.
“Even with all its flaws and faults, this is a big step forward,” says Henderson. “We have a long way to go, but we have to remember: We’re not done.”

Even with all its flaws and faults, this is a big step forward. We have a long way to go, but we have to remember:
We’re not done.

Therese Borchard: Are we overmedicating with psychiatric drugs?
Dr. Pies: I often answer this by saying that we have a “twin peaks” phenomenon in this country, as regards prescription of psychiatric medications. I mean that there is evidence of both under- and over-prescribing, depending on the population studied and the clinicians doing the prescribing—as well as on some ethnic and economic factors. The answer also may depend on the particular type of “psychotropic” medication we are discussing, and the diagnosis in question.
Let’s start with the most widely prescribed class of agents, the antidepressants.
Dr. Pies: Mojtabai and Olfson found that the rate of antidepressant drug treatment in the United States increased more than four times between early 1990s and early 2000s. Of special concern, they found that the rate of antidepressant treatment increased more in the group of less severely ill individuals than in those with more severe psychopathology—not what we would like to see, all other things being equal, since antidepressants are probably more effective (compared with placebo) in moderate-to-severe depression.
What was you interpretation of the study?
Dr. Pies: In less severe cases, psychotherapy would be my preferred treatment of first choice, given that antidepressants may have significant side effects, such as weight gain and sexual dysfunction, depending on the particular medication and patient. I would also argue that antidepressants are over-prescribed
in bipolar disorder, often because the condition has been misdiagnosed as recurrent major depression. Although some patients with bipolar disorder may need antidepressants, most will get little benefit from them, and may even experience increased irritability or mood instability. Whenever possible, but every case must be evaluated individually.
Mojtabai and Olfson have also found that much of the growth in antidepressant prescribing has been driven by antidepressant prescriptions written by “non-psychiatrist providers” (for example, primary care physicians) without providing an accompanying psychiatric diagnosis. But—is that necessarily always a bad thing? Not necessarily. Some of these primary care prescriptions may be for “unofficial” conditions like mixed anxiety, depression and insomnia, and the PCP may not code this as a “psychiatric” disorder—but antidepressants might still be of some benefit in these circumstances.
Finally, some sedative-hypnotic and anti-anxiety agents, such as Alprazolam (Xanax) or lorazepam (Ativan) may be over-prescribed in some clinical settings, but may also be inappropriately withheld, on the mistaken idea that these are highly addictive drugs. Unless the patient has a history of alcohol or substance abuse, short-term use (2-6 weeks) of these anti-anxiety agents is often warranted for severe anxiety (such as panic disorder); or insomnia that doesn’t respond to “sleep hygiene” or behavioral therapy. That said, some patients can become physically or psychologically dependent on Valium-type drugs, when possible.
ARE WE OvERmEDICATINg WITH PSyCHIATRIC mEDICATIONS?Therese Borchard sits down with Dr. Pies to ask his expert opinion about mental health care and issues of overdiagnosis.
INFORMATION
11

How do you respond when people say we are overmedicating?
Dr. Pies: The first thing I say is that this issue is something of a distraction from the much larger problem in American health care—the fact that most people with serious psychiatric illness have great difficulty getting the proper care and treatment, whether medication or “talk therapy.” In part, this is due to problems in the way our so-called “health care system” is set up—if you don’t have insurance, or enough money, you often are denied appropriate care. Often, there is also a mismatch between the patient and the level of expertise of the clinician; for example, few patients with clinically-significant depression ever get to see a psychiatrist or psychologist, in the U.S. I don’t mean to slam primary care doctors—they are doing their best under difficult conditions—but they are often overwhelmed, and can’t do an adequate work-up in a fifteen minute encounter. By the way, neither can a psychiatrist, when first assessing the patient! So, one thing I would tell anyone who is considering medication for an emotional or behavioral disorder: make sure that your initial diagnostic evaluation is thorough, complete, and—ideally—performed by an expert in the mental health area.
So what do you recommend?
Dr. Pies: Do not accept a diagnosis and treatment plan, based on a single, 12-15 minute “evaluation”! This is especially important when distinguishing medical and neurological causes of the problem from psychological and social causes—of course, all of these factors may be relevant—and in planning treatment for bipolar disorder, as contrasted with “ordinary” depression. Getting a second exert opinion is always worth considering if you have any doubts about the diagnosis or treatment you have been given.
What other parting advice can you leave us with?
Dr. Pies: Remember that medication is a bit like fire: it can heat your home comfortably in the winter, or it can burn it down. It all depends on when and how it is used, and with what degree of care and caution! Finally, as I always tell patients: medication is just a bridge between feeling bad and feeling better. You must still “move your legs” to get across that bridge, and that means working on new ways of thinking, feeling, and living!
Ronald W. Pies, MDProfessor of Psychiatry and Lecturer on Bioethics and Humanities at SUNY
Upstate Medical University in Syracuse, New York and Clinical Professor
of Psychiatry at Tufts University School of Medicine in Boston. His most
recent book is “The Three-Petaled Rose: How the Synthesis of Judaism,
Buddhism, and Stoicism Can Create a Healthy, Fulfilled and Flourishing
Life.” He has written much on the topic of overmedication.

BY KAYLA MASSEYILLUSTRATIONS BY AMBER POKPHANH
13

BY KAYLA MASSEYILLUSTRATIONS BY AMBER POKPHANH

Grey Matters
T October 2015
GREY MATTERSADHD KID
16
he diagnosis and medication of
mental health disorders in children
has skyrocketed in the last few years. In
the US, more and more children are be-
ing put on medications for disorders such
as attention deficit hyperactivity disorder
(ADHD) at increasingly younger ages.
With these growing numbers there is
concern of misdiagnoses. A recent study
by Michigan State University, suggests
that up to one million children could
have been misdiagnosed with ADHD.
The same study estimates that between
320 –500 million dollars a year is spent
on medication for children who were
misdiagnosed, most of which was paid
by Medicaid. The MSU study is only one
Alarming example of many such studies,
suggesting that something needs to be
addressed and drastically changed.
ADHD is notoriously hard to diagnose with
certainty. There is no blood test or brain
scan that can give anything close to that
certainty. The only way to tell if anyone,
adult or child has the disorder is through
a series of observations and questions to
the person and especially with children,
those around them. Things to look for
include things as simple as “blurts out
answers”, “easily distracted”, “loses
pencils or toys”, “tendency not to listen”
or “runs about or climbs excessively in
situations when it is not appropriate.”
Childhood is a critical phase of develop-
ment and while little is known even of
the adult brain, even less is known about
the development of a child’s brain. Al-
most nothing is also known about most
of the medications that are being giving
to children. On top of that almost noth-
ing at all is known of the brain itself.
Marcela Gaviria is an award-winning
journalist and producer that created the
PBS Frontline documentary in 2008
called The Medicated Child. In which it
questions the unknown side effects and
the long term consequences of psychi-
atric drugs in children. To illustrate this
point, Dr. Marianne Wamboldt the chief
of psychiatry at Denver Children’s Hos-
pital, tersely summarizes the risk we are
engaged in. “The brain is the most com-
plex thing we know, changing, rewiring
itself. And so what we measure are very
crude, preliminary things. But we’ve only
been at it for about ten or twelve years.”
LEARNING CURVEThere are several reasons known for
the misdiagnoses of ADHD in children.
The first and foremost of these that
was discovered by same MSU study
mentioned earlier, is the birth date of the
child in correlation with the cutoff date for
the school that they are attending. Say a
child is born August 31st when the school
would stop accepting children born on and
after September 1st, that child is about
60 percent more likely to be diagnosed
with ADHD than those born right after
the cut off date. This is because the
teachers of these children are comparing
all of them as if they are the same age
because they are in the same grade.
Since these teachers see the children in
settings where they are not actually being
compared with peers of the same age how
they are viewing the child is very different
then how a parent is. However, teachers
and others who have a similar jobs are one
of the leading reasons for children being
diagnosed or taken to see a doctor for
further tests and studies, not the parent.
In the end for one reason or another they
listen to the advice they do not fully believe
in. Even the best intentioned parents can
make mistakes. The weight of responsibility
felt by a parent can make the added
pressure to medicate, overwhelming.
Iris and Ron Solomon are two such par-
ents. When their son was just two years
old they started to feel the pressure of
turning to medication for their son, Ja-
cob. The first determining incident occur-
ring when he was kicked out of a Mom-
my and Me class for not having impulse
control. Then again, what two-year-old
is going to be incredibly well behaved?
For years however this continued un-
til finally they caved in to the demands
of his teachers and took him to a doctor.
By the age of ten Jacob was on ten
different medications. His father Ron
described it, as “That whole—there was
an old lady who swallowed the fly. And
then the fly—she had to swallow the spider
to get rid of the fly. And then she had to
swallow a mouse to get rid of the spider.
That’s what the meds were like.” Jacob
had to take more and more medications
because each new medication introduced
into his system caused yet another
problem. Once they finally had enough of
this the made the decision to strip him of
all of his medications. However it was not
even a full 24 hours off of the medications
before there was a new diagnosis and new
medications for Jacob, bipolar disorder
CRAPSHOOTDr. Patrick Bacon who stands behind
the use of medication with children says
when trying to figure out the medication
for ADHD or children with bipolar, “It
really is to some extent an experiment,
trying medications in these children of
this age. It is a gamble.” Even when a
medication is thought to start working
with a child, often as they grow old-
er and start to change the medication
will stop working and new medication
combinations will have to be tried.
Once a child is diagnosed with ADHD
the next steps taken are to figure out
how to treat and manage it. The drugs
being prescribed are almost entirely
untested; especially in children and have
unknown long term side effects. When
asked about the Dr. Wamboldt goes on to
say,“Medications have a whole different
impact in the young developing child
than they do in an adult, and we don’t
understand that impact very well. That’s
where we’re still in the dark ages.” Even
worse, only just recently has testing of
these drugs and how they affect children
“...we don’t understand that impact very well. That’s where we’re still in the dark ages.”
“...trying these medications in children of this age is a gamble.”
“The brain is the most complex thing we know, changing,
rewiring itself...we measure very crude, preliminary things.”
Grey Matters
T October 2015
GREY MATTERSADHD KID
16
he diagnosis and medication of
mental health disorders in children
has skyrocketed in the last few years. In
the US, more and more children are be-
ing put on medications for disorders such
as attention deficit hyperactivity disorder
(ADHD) at increasingly younger ages.
With these growing numbers there is
concern of misdiagnoses. A recent study
by Michigan State University, suggests
that up to one million children could
have been misdiagnosed with ADHD.
The same study estimates that between
320 –500 million dollars a year is spent
on medication for children who were
misdiagnosed, most of which was paid
by Medicaid. The MSU study is only one
Alarming example of many such studies,
suggesting that something needs to be
addressed and drastically changed.
ADHD is notoriously hard to diagnose with
certainty. There is no blood test or brain
scan that can give anything close to that
certainty. The only way to tell if anyone,
adult or child has the disorder is through
a series of observations and questions to
the person and especially with children,
those around them. Things to look for
include things as simple as “blurts out
answers”, “easily distracted”, “loses
pencils or toys”, “tendency not to listen”
or “runs about or climbs excessively in
situations when it is not appropriate.”
Childhood is a critical phase of develop-
ment and while little is known even of
the adult brain, even less is known about
the development of a child’s brain. Al-
most nothing is also known about most
of the medications that are being giving
to children. On top of that almost noth-
ing at all is known of the brain itself.
Marcela Gaviria is an award-winning
journalist and producer that created the
PBS Frontline documentary in 2008
called The Medicated Child. In which it
questions the unknown side effects and
the long term consequences of psychi-
atric drugs in children. To illustrate this
point, Dr. Marianne Wamboldt the chief
of psychiatry at Denver Children’s Hos-
pital, tersely summarizes the risk we are
engaged in. “The brain is the most com-
plex thing we know, changing, rewiring
itself. And so what we measure are very
crude, preliminary things. But we’ve only
been at it for about ten or twelve years.”
LEARNING CURVEThere are several reasons known for
the misdiagnoses of ADHD in children.
The first and foremost of these that
was discovered by same MSU study
mentioned earlier, is the birth date of the
child in correlation with the cutoff date for
the school that they are attending. Say a
child is born August 31st when the school
would stop accepting children born on and
after September 1st, that child is about
60 percent more likely to be diagnosed
with ADHD than those born right after
the cut off date. This is because the
teachers of these children are comparing
all of them as if they are the same age
because they are in the same grade.
Since these teachers see the children in
settings where they are not actually being
compared with peers of the same age how
they are viewing the child is very different
then how a parent is. However, teachers
and others who have a similar jobs are one
of the leading reasons for children being
diagnosed or taken to see a doctor for
further tests and studies, not the parent.
In the end for one reason or another they
listen to the advice they do not fully believe
in. Even the best intentioned parents can
make mistakes. The weight of responsibility
felt by a parent can make the added
pressure to medicate, overwhelming.
Iris and Ron Solomon are two such par-
ents. When their son was just two years
old they started to feel the pressure of
turning to medication for their son, Ja-
cob. The first determining incident occur-
ring when he was kicked out of a Mom-
my and Me class for not having impulse
control. Then again, what two-year-old
is going to be incredibly well behaved?
For years however this continued un-
til finally they caved in to the demands
of his teachers and took him to a doctor.
By the age of ten Jacob was on ten
different medications. His father Ron
described it, as “That whole—there was
an old lady who swallowed the fly. And
then the fly—she had to swallow the spider
to get rid of the fly. And then she had to
swallow a mouse to get rid of the spider.
That’s what the meds were like.” Jacob
had to take more and more medications
because each new medication introduced
into his system caused yet another
problem. Once they finally had enough of
this the made the decision to strip him of
all of his medications. However it was not
even a full 24 hours off of the medications
before there was a new diagnosis and new
medications for Jacob, bipolar disorder
CRAPSHOOTDr. Patrick Bacon who stands behind
the use of medication with children says
when trying to figure out the medication
for ADHD or children with bipolar, “It
really is to some extent an experiment,
trying medications in these children of
this age. It is a gamble.” Even when a
medication is thought to start working
with a child, often as they grow old-
er and start to change the medication
will stop working and new medication
combinations will have to be tried.
Once a child is diagnosed with ADHD
the next steps taken are to figure out
how to treat and manage it. The drugs
being prescribed are almost entirely
untested; especially in children and have
unknown long term side effects. When
asked about the Dr. Wamboldt goes on to
say,“Medications have a whole different
impact in the young developing child
than they do in an adult, and we don’t
understand that impact very well. That’s
where we’re still in the dark ages.” Even
worse, only just recently has testing of
these drugs and how they affect children
“...we don’t understand that impact very well. That’s where we’re still in the dark ages.”
“...trying these medications in children of this age is a gamble.”
“The brain is the most complex thing we know, changing,
rewiring itself...we measure very crude, preliminary things.”

Grey Matters
T October 2015
GREY MATTERSADHD KID
16
he diagnosis and medication of
mental health disorders in children
has skyrocketed in the last few years. In
the US, more and more children are be-
ing put on medications for disorders such
as attention deficit hyperactivity disorder
(ADHD) at increasingly younger ages.
With these growing numbers there is
concern of misdiagnoses. A recent study
by Michigan State University, suggests
that up to one million children could
have been misdiagnosed with ADHD.
The same study estimates that between
320 –500 million dollars a year is spent
on medication for children who were
misdiagnosed, most of which was paid
by Medicaid. The MSU study is only one
Alarming example of many such studies,
suggesting that something needs to be
addressed and drastically changed.
ADHD is notoriously hard to diagnose with
certainty. There is no blood test or brain
scan that can give anything close to that
certainty. The only way to tell if anyone,
adult or child has the disorder is through
a series of observations and questions to
the person and especially with children,
those around them. Things to look for
include things as simple as “blurts out
answers”, “easily distracted”, “loses
pencils or toys”, “tendency not to listen”
or “runs about or climbs excessively in
situations when it is not appropriate.”
Childhood is a critical phase of develop-
ment and while little is known even of
the adult brain, even less is known about
the development of a child’s brain. Al-
most nothing is also known about most
of the medications that are being giving
to children. On top of that almost noth-
ing at all is known of the brain itself.
Marcela Gaviria is an award-winning
journalist and producer that created the
PBS Frontline documentary in 2008
called The Medicated Child. In which it
questions the unknown side effects and
the long term consequences of psychi-
atric drugs in children. To illustrate this
point, Dr. Marianne Wamboldt the chief
of psychiatry at Denver Children’s Hos-
pital, tersely summarizes the risk we are
engaged in. “The brain is the most com-
plex thing we know, changing, rewiring
itself. And so what we measure are very
crude, preliminary things. But we’ve only
been at it for about ten or twelve years.”
LEARNING CURVEThere are several reasons known for
the misdiagnoses of ADHD in children.
The first and foremost of these that
was discovered by same MSU study
mentioned earlier, is the birth date of the
child in correlation with the cutoff date for
the school that they are attending. Say a
child is born August 31st when the school
would stop accepting children born on and
after September 1st, that child is about
60 percent more likely to be diagnosed
with ADHD than those born right after
the cut off date. This is because the
teachers of these children are comparing
all of them as if they are the same age
because they are in the same grade.
Since these teachers see the children in
settings where they are not actually being
compared with peers of the same age how
they are viewing the child is very different
then how a parent is. However, teachers
and others who have a similar jobs are one
of the leading reasons for children being
diagnosed or taken to see a doctor for
further tests and studies, not the parent.
In the end for one reason or another they
listen to the advice they do not fully believe
in. Even the best intentioned parents can
make mistakes. The weight of responsibility
felt by a parent can make the added
pressure to medicate, overwhelming.
Iris and Ron Solomon are two such par-
ents. When their son was just two years
old they started to feel the pressure of
turning to medication for their son, Ja-
cob. The first determining incident occur-
ring when he was kicked out of a Mom-
my and Me class for not having impulse
control. Then again, what two-year-old
is going to be incredibly well behaved?
For years however this continued un-
til finally they caved in to the demands
of his teachers and took him to a doctor.
By the age of ten Jacob was on ten
different medications. His father Ron
described it, as “That whole—there was
an old lady who swallowed the fly. And
then the fly—she had to swallow the spider
to get rid of the fly. And then she had to
swallow a mouse to get rid of the spider.
That’s what the meds were like.” Jacob
had to take more and more medications
because each new medication introduced
into his system caused yet another
problem. Once they finally had enough of
this the made the decision to strip him of
all of his medications. However it was not
even a full 24 hours off of the medications
before there was a new diagnosis and new
medications for Jacob, bipolar disorder
CRAPSHOOTDr. Patrick Bacon who stands behind
the use of medication with children says
when trying to figure out the medication
for ADHD or children with bipolar, “It
really is to some extent an experiment,
trying medications in these children of
this age. It is a gamble.” Even when a
medication is thought to start working
with a child, often as they grow old-
er and start to change the medication
will stop working and new medication
combinations will have to be tried.
Once a child is diagnosed with ADHD
the next steps taken are to figure out
how to treat and manage it. The drugs
being prescribed are almost entirely
untested; especially in children and have
unknown long term side effects. When
asked about the Dr. Wamboldt goes on to
say,“Medications have a whole different
impact in the young developing child
than they do in an adult, and we don’t
understand that impact very well. That’s
where we’re still in the dark ages.” Even
worse, only just recently has testing of
these drugs and how they affect children
“...we don’t understand that impact very well. That’s where we’re still in the dark ages.”
“...trying these medications in children of this age is a gamble.”
“The brain is the most complex thing we know, changing,
rewiring itself...we measure very crude, preliminary things.”

October 201518
ADHD KID GREY MATTERS
has begun, and the results are far from
encouraging, “In fact ‘it’s become clear
that many of the drugs that work in adults
do not work well or at all, in children.”
Over the last years the amount of medi-
cations being prescribed has skyrocketed,
especially in the United States, which con-
stitutes 83-90 percent of the total market
share by volume. A study preformed by
Health Affairs showed a global increase in
ADHD medication at an increase of 274
percent from just 1993-2000. The amount
of money that was spent on medication for
one year alone, 2003, was an astounding
$2.4 billion in U.S. currency, 92-95 per-
cent of that from the United States alone.
A recent study done by The British Journal
of Psychiatry showed that many of the
children being treated with stimulant
drugs did not actually meet the criteria
for ADHD. In the United States alone, 50
percent of the participants did not have
ADHD but were taking the medications to
treat it. In a sample of just North Carolina
that percentage jumped all the way up to
66.4 percent. The next closest country to
the United States was Australia at 22.9%,
less than half of the amount as in the
United States. Many children are being
prescribed drugs when they only have
a very mild subtype of ADHD and only
those with a severe case should really
be taking the medication. The actual
number of severe cases that require
medication is incredibly small, only 1%
Even their own parents might start to see
and treat them differently. On one end
they might became much more relaxed
with their raising of the child because
it is no longer their own fault, there is
something wrong with them. On the other
end the could become even more harsh
because what is wrong with them should
be being fixed with the massive amounts
of medications that they are on and are
spending a good amount of money on to
make them happy. Both of these are not
good at all to the health of the child. In the
first instance the child is then being given
an excuse to act out, to become out of
control, to have no rules. It is not their own
fault that they do not have self-control; it
is because there is something really wrong
with them. They no longer try to develop
and learn the rules and how to act, to
naturally mature like children normally
would because they now have a very good
excuse to take advantage of. The later is
no better for then the child, if there really
is something going on with them and the
medication is not doing what it is supposed
to be doing which is often the case in these
situations, they are not able to fix what is
wrong with them on their own and are
being punished for that and treated more
harshly than needed when in the beginning
all that would have been needed was a
small amount of patience with that child.
Jessica, another child that was interviewed
by the Frontline crew, had an increase
in the amount of medications that she
was taking after talking with her doctor,
Dr. David Axelson, about what is going
on in her life. Jessica told him how she
was worried about returning to school
because there was a girl there that was
always mean to her. On top of that she is
a 12-year-old girl, it is not uncommon in
the least to have worries about going to
school. On top of that her father was just
deployed to Iraq. Even though in almost
any situation it would be normal for her to
be sad in even just one of these instances,
her doctor felt it was necessary for Jessica
to become even more heavily medicated
that she is. Because of what her doctor
and what her mother has been telling her
sense she was a little girl, she now fully
believes that there is something wrong with
her and that she is incapable of handling
these very normal circumstances without
the aid of very dangerous medications.
She tells reporters, “Taking my medication
makes me more calmer, more like- like
I’m supposed to be.” Her she is telling
the reporter, telling the world really that
she is unable to accomplish anything on
her own even though that is something
no one truly knows. This dependency is
reiterated later on in the movie, this time
however by her mother. She states, “No,
she’ll have to take meds for the rest of
her life, if she wants to go to college or
have a job or have a family.” Her mother
has become absolutely positive that her
daughter does not have the ability to
function on her own and is something that
she will forever be telling her daughter. She
has become dependent on these drugs
that she has never really lived without to
have a comparison to. And even now if she
were to stop talking them, the permanent
damage they could have done to her,
physically and mentally is beyond knowing.
ADHD KIDBeing told every day from the age of two
that there is something chemically wrong
with you can become a crutch. The idea
that what you are feeling is not normal
and never will be, places a child in a world
where that what they feel and what they
think, whether happy or sad is always
out of proportion with what is acceptable.
They will always be told that they cannot
help it, there is nothing that they can do
for themselves and that the only answer is
to be placed on yet more medications that
alter the way they think, the way the feel and
act. They grow up with idea that they are
forever wrong, forever somehow broken.
How is anyone really able to know what is the
true amount of sadness, or nervousness,
the true amount of joy and happiness for
a situation? How is anyone really able to
know how much energy a child should
have at a given time? Anyone living with a
child would think they must all have ADHD
because the amount of energy they seem
to have seems to defy everything that
people know about how the world works.
It comes from nowhere and it lasts forever,
sun up to sun down and often well beyond.
Children are at a critical point in life
when they have the greatest opportunity
for learning and growth. Medication
will not truly solve any problems, but
rather stifle opportunities for real growth.
How is anyone really able to know what is the true amount of sadness, or nervousness, the true amount of joy and happiness for a situation?
“...she’ll have to take meds for the rest of her life, if she
wants to go to college or have a job or have a family.”

October 201518
ADHD KID GREY MATTERS
has begun, and the results are far from
encouraging, “In fact ‘it’s become clear
that many of the drugs that work in adults
do not work well or at all, in children.”
Over the last years the amount of medi-
cations being prescribed has skyrocketed,
especially in the United States, which con-
stitutes 83-90 percent of the total market
share by volume. A study preformed by
Health Affairs showed a global increase in
ADHD medication at an increase of 274
percent from just 1993-2000. The amount
of money that was spent on medication for
one year alone, 2003, was an astounding
$2.4 billion in U.S. currency, 92-95 per-
cent of that from the United States alone.
A recent study done by The British Journal
of Psychiatry showed that many of the
children being treated with stimulant
drugs did not actually meet the criteria
for ADHD. In the United States alone, 50
percent of the participants did not have
ADHD but were taking the medications to
treat it. In a sample of just North Carolina
that percentage jumped all the way up to
66.4 percent. The next closest country to
the United States was Australia at 22.9%,
less than half of the amount as in the
United States. Many children are being
prescribed drugs when they only have
a very mild subtype of ADHD and only
those with a severe case should really
be taking the medication. The actual
number of severe cases that require
medication is incredibly small, only 1%
Even their own parents might start to see
and treat them differently. On one end
they might became much more relaxed
with their raising of the child because
it is no longer their own fault, there is
something wrong with them. On the other
end the could become even more harsh
because what is wrong with them should
be being fixed with the massive amounts
of medications that they are on and are
spending a good amount of money on to
make them happy. Both of these are not
good at all to the health of the child. In the
first instance the child is then being given
an excuse to act out, to become out of
control, to have no rules. It is not their own
fault that they do not have self-control; it
is because there is something really wrong
with them. They no longer try to develop
and learn the rules and how to act, to
naturally mature like children normally
would because they now have a very good
excuse to take advantage of. The later is
no better for then the child, if there really
is something going on with them and the
medication is not doing what it is supposed
to be doing which is often the case in these
situations, they are not able to fix what is
wrong with them on their own and are
being punished for that and treated more
harshly than needed when in the beginning
all that would have been needed was a
small amount of patience with that child.
Jessica, another child that was interviewed
by the Frontline crew, had an increase
in the amount of medications that she
was taking after talking with her doctor,
Dr. David Axelson, about what is going
on in her life. Jessica told him how she
was worried about returning to school
because there was a girl there that was
always mean to her. On top of that she is
a 12-year-old girl, it is not uncommon in
the least to have worries about going to
school. On top of that her father was just
deployed to Iraq. Even though in almost
any situation it would be normal for her to
be sad in even just one of these instances,
her doctor felt it was necessary for Jessica
to become even more heavily medicated
that she is. Because of what her doctor
and what her mother has been telling her
sense she was a little girl, she now fully
believes that there is something wrong with
her and that she is incapable of handling
these very normal circumstances without
the aid of very dangerous medications.
She tells reporters, “Taking my medication
makes me more calmer, more like- like
I’m supposed to be.” Her she is telling
the reporter, telling the world really that
she is unable to accomplish anything on
her own even though that is something
no one truly knows. This dependency is
reiterated later on in the movie, this time
however by her mother. She states, “No,
she’ll have to take meds for the rest of
her life, if she wants to go to college or
have a job or have a family.” Her mother
has become absolutely positive that her
daughter does not have the ability to
function on her own and is something that
she will forever be telling her daughter. She
has become dependent on these drugs
that she has never really lived without to
have a comparison to. And even now if she
were to stop talking them, the permanent
damage they could have done to her,
physically and mentally is beyond knowing.
ADHD KIDBeing told every day from the age of two
that there is something chemically wrong
with you can become a crutch. The idea
that what you are feeling is not normal
and never will be, places a child in a world
where that what they feel and what they
think, whether happy or sad is always
out of proportion with what is acceptable.
They will always be told that they cannot
help it, there is nothing that they can do
for themselves and that the only answer is
to be placed on yet more medications that
alter the way they think, the way the feel and
act. They grow up with idea that they are
forever wrong, forever somehow broken.
How is anyone really able to know what is the
true amount of sadness, or nervousness,
the true amount of joy and happiness for
a situation? How is anyone really able to
know how much energy a child should
have at a given time? Anyone living with a
child would think they must all have ADHD
because the amount of energy they seem
to have seems to defy everything that
people know about how the world works.
It comes from nowhere and it lasts forever,
sun up to sun down and often well beyond.
Children are at a critical point in life
when they have the greatest opportunity
for learning and growth. Medication
will not truly solve any problems, but
rather stifle opportunities for real growth.
How is anyone really able to know what is the true amount of sadness, or nervousness, the true amount of joy and happiness for a situation?
“...she’ll have to take meds for the rest of her life, if she
wants to go to college or have a job or have a family.”

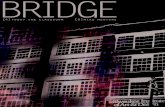
WHaT aRE sOME Of THE causEs Of THIs IncREasE?
Studies estimate that 14–38 percent of ADHD cases are actually OVER-DIAGNOSES.
LOWERED THREsHOLDFor ADHD by DSM-IV which prompted an unreal epidemic.
unDuE PREssuRETo diagnose ADHD so that a child can receive benefits.
sOcIETaL facTORsWhich reduced tolerance for a child’s range of behavior.
OvER PROMOTIOnBy various types of marketing by pharmaceutical companies.
The previous article, ADHD KID highlighted the some of the issues that America has been facing an increasing number of diagnosises. SInce 2003 diagnosis of ADHD
have been increasing at a steady rate. Why does this happen? More importantly what can we do about it.
Rates of ADHD diagnosis have increased an average 5 percent per year from 2003–2014
WHAT’S THE DIAgNOSIS?
less than 7% 7%–9% 9%–11% 11%–13% greater than 13%
20072003
INFORMATION
19

Hyperactivity, inattention and impulsivity are traits found in many children,are also indicators for ADHD the most commonly diagnosed neurological disorder in children.
a POssIBLE sOLuTIOn
2014
A validated biomarker test can determine whether the child has ADHD or something else. In other words, there’s much less guesswork.

Veterans Kick The Prescription
Pill Habit...Written by Quil Lawrence
21

“I always see his face,” says Will, who did tours in Iraq and Afghanistan with the Army. “And in my dreams it’s the same thing. ... I always walk over to him, and instead of this Afghani kid that’s laying there, it’s my little brother.”
The memory that triggers Will’s nightmare happened during his tour in Afghanistan. Will, 33, who asked that NPR not use his last name, was on patrol when a kid came up to the Humvee asking for water. Then he bashed Will’s medic in the face with a rock. The boy’s father appeared with a gun and started shooting. Amid a scuffle, the child picked up the gun and Will shot him at close range.
“After I did that, all I remember is that I was shaking,” Will says. “And one of my soldiers took my weapon away and said: ‘It’s OK primo [cousin]. It’s gonna be OK.“
Troops coming home from war, like Will, are often prescribed drugs for PTSD and other conditions. Hundreds of thousands of veterans are on opiates for pain, and 1 in 3 veterans polled say they are on 10 different medications.
While there is concern about
overmedicating and self-medicating ,using alcohol or drugs without a doctor’s approval — there are also some veterans who are trying to do the opposite: They’re kicking the drugs, against doctor’s orders.
Long Lists Of DrugsBryan McDonel and his father, Mike, both served multiple tours in Iraq with the National Guard. Bryan was first prescribed painkillers before his deployment, and his dependence on medication prompted a downward spiral.
Will has other upsetting stories. They’re noteworthy not for the intensity of the firefight or the size of the bombs, but for the bad pictures they conjure up in his
head. Some patients with PTSD suffer recurring nightmares of a single event.
He remembers pulling a friend out of a river in Iraq, only to find there was nothing left of him below the waterline. He recalls discovering his buddy is dead by finding a huge scrap of his tattoo.
And there’s guilt: “Those guys had wives and kids. You know, everybody in my Humvee, we were all single. I felt guilty. It should have been us; it shouldn’t have been them.”
Will came away, he says, with “only” two ruined knees, a wrecked back, a piece of bone fragment that sort of floats on his hip, a mild traumatic brain injury and PTSD. And for all those things, Will has been prescribed medications — lots and lots of medications. It takes him about six minutes to list all his pills.
There are other veterans with similarly long lists. On average, servicemen and women are prescribed narcotic painkillers three times more often than civilians. But despite the pain and PTSD, some of them have decided, without telling their doctors, to stop taking their medications.
Leo Kalberg served in the Army for 6 years. His medication list includes escitalopram, Prozac, Klonopin, morphine, Percocet, Vicodin, tramadol, Motrin, cortisone, lidocaine and Seroquel, among others. Total pill count: over 20.
He realized he was addicted to Percocet because he’d get nervous if he only had a few pills left. Plus, Karlberg says the side effects make him feel like a zombie.
“I’d take all my medication, and I’d sit down, and a whole entire day would pass, and I would just get up and go to bed,” Karlberg says. That’s when he decided to quit taking his medications.
I just scrape my name off all the pill bottles and throw them all away.- Will, who has served in Iraq and Afghanistan with the U.S. Army

Nancy Bryant, who served in the Air Force for almost 15 years, was in a similar situation. Cymbalta, Maxalt, trazodone, tizanidine, dicyclomine, hydrocodone and her list goes on and on.
Bryant came upon the idea of stopping her medications by accident. She got the stomach flu and couldn’t keep any food or medications down.
“After a few days of that — those medications clearing my system — I just realized, wow, I felt like a totally different person,” she says.
Rachel Stokes was in the Army, and she too has a long list crowded with similar medications. She started looking into what all those medications are really for.
She was prescribed Seroquel to help her sleep. “But it’s not even for sleep,” Stokes says. “Seroquel is for people that have bipolar [or] schizophrenia. And I’m like, that is not me.”
Using Drugs ‘Way, Way, Way Off Label’Dr. Richard Friedman, director of the Psychopharmacology Clinic at Weill Cornell Medical College, has heard this before. “They’re using psych drugs off label — way, way, way off label,” he says. “Obviously, they are not using them to treat the major disorders for which these drugs are designed.”
Friedman researched the military’s use of antipsychotics like Seroquel, and stimulants like Adderall and Ritalin. He says those drugs have no official purpose that fits a combat zone. He figures the military was using whatever drugs they could to keep troops sleeping, waking up and functioning during wartime.
“They were in a different situation, where they had unprecedented levels of stress in a group of otherwise healthy people,” Friedman says. “So, I think they resorted to psychopharmacology as a means to keep people in active duty.”
Friedman says it’s like giving a football player painkillers so he can finish the game: It gets him back on the field, but might hurt him worse in the long term.
The Pentagon says it has safeguards to prevent overprescription or the use
of drugs in harmful combinations, and the Department of Veterans Affairs’ guidelines warn about using many of these drugs off-label.
Off-label use is common in medicine, and Friedman says doctors do it with good intentions. He also says stopping medications without a doctor’s guidance can be dangerous.
But Rachel Stokes says she’s sick of
doctors and their pills.“The medications I hate all the medications,” she says. “If the scientist actually went through and did research, and then really found out what really worked, then that’s different. But it doesn’t seem like they’re doing that.”
She may have a point. A study by the Institute of Medicine last month concluded that the VA and the Pentagon do a poor job tracking what happens when they treat PTSD with drugs, although there is a brand-new effort at the VA to educate its doctors.
Gavin West, who heads the Opioid Safety Initiative at the VA, says, “We’ve undertaken a psychopharmacologic safety initiative, where we’re looking across the board at more safe and more effective use of medications.”
Flushing Drugs Down The ToiletWill, the veteran whose list of medications takes six minutes to read, has stopped taking those drugs.
“I always keep at least one month on supply,” Will says. “My next month’s supply comes next week, so as soon as they come in, I take those and I flush them. And then I just scrape my name off all the pill bottles and throw them out.”
Will, who is in the process of medically retiring from the Army, keeps that month’s supply of pills on hand for a reason: He gets drug-tested to make sure he is taking his medications. That’s to ensure he’s not selling his drugs on the street.
I’m actually feeling pretty good...- Will, who has served in Iraq and Afghanistan with the U.S. Army

So every few months, when he has an appointment coming up, Will gets himself back on his drugs. He gradually works up to the dose he’s supposed to be on. He recently cycled himself off the medications again after an appointment.
“I’m actually feeling pretty good,” Will says. “I’ve now been fully off the meds for nine days. The first three days of being off them were really bad; just real bad nausea, diarrhea, shaky.”
Will hopes he’ll be out of the Army soon and can stop the roller coaster of getting on and off the drugs. But for now, he says, it’s worth it. When he was on the medications, he was a shut-in, he says, depressed and too doped up to drive.
As for dealing with his PTSD without the drugs — he’s still working on it.

ALARMINGHEADLINES like this
This ad brought to you by a sensible font like this.
DRAMATICbACkgRounDs
lIke ThIs
HIGHLIGHTED ACCUSATIONS
LIKE THIS
Seen this before?
And I look like this too
THIS Guy SAyS THIS —This guy
“I really said this”
FactCheck.org