
Mgt of Uterine Inversion

of 22
-
Upload
neenu-jacob -
Category
Documents
-
view
220 -
download
0
Transcript of Mgt of Uterine Inversion
-
8/12/2019 Mgt of Uterine Inversion
1/22
NEENU JACOB
-
8/12/2019 Mgt of Uterine Inversion
2/22
INTRODUCTION It is a rare but potentially life threatening
situation in which ,the uterine position ischanged from its normal situation
-
8/12/2019 Mgt of Uterine Inversion
3/22
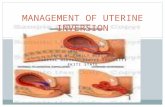
DEFINITION OF INVERSION OF UTERUS Uterine inversion is a condition where the
uterus becomes turned inside out, with thefundus prolapsing through the cervix.
-
8/12/2019 Mgt of Uterine Inversion
4/22
Types of inversionIt has been classified on the basis of its duration
and degrees
a, Acute inversion:Occurs immediately afterdelivery and before the cervix constricts (most
common >95%) occurs within 24 hoursb Subacute inversion: Occurs after the cervix
constricts after 24 hours but before 4 weeks
c,Chronic inversion: Inversion noted 4 weeks afterdelivery; rare incidence 1:2000 deliveries
-
8/12/2019 Mgt of Uterine Inversion
5/22
Management of uterine inversion involvestwo important components: Immediate treatment of Shock
Replacement/Repositioning of the uterus
-
8/12/2019 Mgt of Uterine Inversion
6/22
-
8/12/2019 Mgt of Uterine Inversion
7/22
Send blood for cross matching and start atransfusion in time
Analgesics
Use warm sterile towel to apply compressionwhile preparing for the procedure
Insert a urinary catheter
-
8/12/2019 Mgt of Uterine Inversion
8/22
REPOSITIONINGManual reductionIt is a sterile procedure. It is as follows;
Push the fundus with the palm of the hand,along the direction of the vagina towards the
posterior fornix. Apply counter support withother hand placed on the abdomen . Afterreplacement ,the hand should remain inside theuterus until the uterus becomes contracted byparentral oxytocin. The placenta is to be removed
manually only after the uterus becomescontracted.
-
8/12/2019 Mgt of Uterine Inversion
9/22
Use of tocolytics: to allow uterine relaxation.For example:
Nitroglycerin (0.25-0.5 mg) intravenouslyover 2 minutes Or terbutaline 0.1-0.25 mgslowly intravenously Or magnesium sulphate4-6 g intravenously over 20 minutes
Use of general anaesthesia: halothane
-
8/12/2019 Mgt of Uterine Inversion
10/22
Reduction by hydrostatic pressure
A sterile douche water is introduced in to
the vaginal canal to distend it This tends to stretch the vaginal vault
allowing opening of the cervical ring andpermitting replacement of the uterus
-
8/12/2019 Mgt of Uterine Inversion
11/22
ANOTHER METHODS OSullivan hydrostatic method
New technique
-
8/12/2019 Mgt of Uterine Inversion
12/22
OSullivan hydrostatic method
Materials needed: An assistant
Long tube(2m) with a large nozzle
Water reservoir/Warm Saline(2-5L)
Put patient in trendelenburg position Place the nozzle of the tube in the posterior
fornix
An assistant start the douche with fullpressure(at least 2m high)
-
8/12/2019 Mgt of Uterine Inversion
13/22
Fluid escape is prevented by blocking theintroitus by using the labia& operators hand
The fluid distend the vagina, relieves themild cervical constriction & result incorrection or replacement of the inverteduterus
-
8/12/2019 Mgt of Uterine Inversion
14/22
New technique This is described by Ogueh & Ayida Citing difficulty in maintaining an adequate
water seal to
generate the pressure required, they suggest
attaching the IV tubing to silicone cup used in vacuum
extraction. By
placing the cup in the vagina, an excellentseal is created.
-
8/12/2019 Mgt of Uterine Inversion
15/22
After repositioning: Discontinue uterine relaxant/general
anaesthesia Start infusion of oxytocin or ergot alkaloids
Continue fluid and blood replacement
Bimanual uterine compression and massageare maintained until the uterus is wellcontracted and hemorrhage is ceased
Remove placenta if retained following
replacement of the inverted uterus andoxytocics given with uterus contracted
-
8/12/2019 Mgt of Uterine Inversion
16/22
Careful manual exploration to rule out thepossibility of genital
tract trauma
Antibiotics- broad spectrum
Adequate analgesics
Oxytocics/ergot are continued for at least24hrs.
Monitor closely after replacement to avoid re-inversion
-
8/12/2019 Mgt of Uterine Inversion
17/22
Chronic uterine inversionIn this surgical replacement/intervention
Involve 2 approaches:
Abdominal
Vaginal
Abdominal
Huntingtons procedure
Haultainsprocedure
-
8/12/2019 Mgt of Uterine Inversion
18/22
Vaginal
Spinellismethod Kustnersmethod
Hysterectomy: if present late with ischaemicchanges of the uterus or non-viable uterine
tissues, removal of the uterus is performedfollowing replacement of normal anatomy
-
8/12/2019 Mgt of Uterine Inversion
19/22
Huntington procedure Locate the cup of the uterus formed by the
inversion
Dilate the constricting cervical ring digitally
Place clamps in the cup of the inversion
below the cervical ring and gentle upwardtraction is applied
Repeated clamping and traction continueuntil the inversion is corrected.
-
8/12/2019 Mgt of Uterine Inversion
20/22
Haultain procedure Under laparotomy,incision is made in the
posterior portion of the inversion ring,toincrease the size of the ring , allowrepositioning of the uterus and posteriorincision is repaired.
Spinellismethod Ant. Colpotomy is done & incision of the
cervix extending into the fundus is made
before manually correcting the incision
-
8/12/2019 Mgt of Uterine Inversion
21/22
ustnersmethod Post. Colpotomy is made & incison of the
cervix extending into the fundus is madebefore manually correcting the incision
-
8/12/2019 Mgt of Uterine Inversion
22/22
PreventionMany cases of acute uterine inversion result from
mismanagement of the third stage of labour inwomen who are already at risk. Hence thefollowing maneuvers are to be avoided:
Excessive traction on the umbilical cord
Avoid overdosage of Oxytocin Advice for institutional delivery
Avoid applying forceps if the uterus is relaxed
Excessive fundal pressure
Excessive intra-abdominal pressure Excessively vigorous manual removal of placenta







![Clinical Practice Guidelines: Obstetrics/Uterine inversion · uterine inversion. • Evidence of shock is common. [2] • Severe abdominal/pelvic pain occurs due to excessive traction](https://static.fdocuments.net/doc/165x107/5fa20d6dcb8c686e684ea4d5/clinical-practice-guidelines-obstetricsuterine-inversion-uterine-inversion-a.jpg)









