Copyright © 2008 Delmar. All rights reserved. Chapter 24 Rural and Migrant Populations.
description

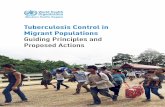
Mexico´s strategy to Health Services for Migrant
Populations
7th Summer Institute on Migration and Global Health
Los Angeles, CaliforniaJune 26, 2012

• + ¼ of Hispanic adults lack a usual health care provider (69% are male) (41% 18-29 years)
• 69% of those with no usual place for health care are of Mexican origin
• More than 8 in 10 receive health info from radio or TV
• Hispanic women are more likely to get health info from doctors and medical community (77%)
• Source: PHC: Hispanics and health care in the US
Health care and Hispanic population

• 45% of Hispanics with no usual place for health care have health insurance.
• 23% who received poor treatment cited 4 reasons: inability to pay, race or ethnicity; lack of English proficiency and medical history
• 1 in 4 Hispanics who get no health information score low on diabetes knowledge, compared to 1 in 11 who get some information.
Health Information of Hispanic population

Health Determinants
Risks for migrant health
Changes in lifestyles• Sedentary lifestyle• Lack of proper housing (overcrowding)• High consumption of saturated fats (fast
food)• Increase comsumption of alcohol and
drugs
Vulnerability due to:
• Lack of education• Social isolation• Occupational hazards• Language and cultural barriers
Health conditions• Obesity
• Diabetes• Depresion and addictions
• Workplace accidents• HIV/AIDS
• Other sexually transmitted infections

• To protect its nationals abroad
• Building health bridges:• Information exchange• Training and education• Health prevention and promotion• Binational health research
projects
Objectives

Components
1.VENTANILLAS DE SALUD (Health windows)
2.BINATIONAL HEALTH WEEKS
3.REPATRIATION OF SERIOUSLY ILL MIGRANTS

Information centers to increase awareness and access to health
centers among the Mexican population living in the US and to disseminate programs of health
prevention and promotion.
Health Windows ProgramVentanillas de Salud

Health Window ProgramVentanillas de Salud (VDS)
ActionsIncrease dissemination of the VDS
through Communication Strategy
Radio spots, television and Printed media
VDS website www.ventanillas.org
VDS Communication Plan and Training Plan
Webinars, Obesity, Seguro Popular (Popular Insurance Scheme)
and Cancer
VDS Operation Diagnosis of VDS, Operating Manual and reporting indicators
Developing Migrants’ Health Guide Guide for migrant health care in Mexico and USA
Free Discount Card Provide discounts on prescription drugs.(300 medicines) Discounts also provided on
genericdrugs; VDS operating staff will be trained

HEALTH WINDOW PROGRAMVENTANILLAS DE SALUD
MAIN SERVICES OFFERED (data until Dec. 31st 2011) TOTAL
Number of individuals Services
Asistance and inscription to Medical Services in the United States:
Adults 16,000 26,000 Minors 10,000
Establishment of medical homes: Adults referred 60,000 Minors referred 7,000 67,000
Asistance and Inscription to the “Seguro Popular.” Informed 40,000 40,600 Pre-Afiliated 600
Early Detection (Screening) 400,000 400,000
Education Sessions on prevention topics (in groups) 1,014,400 1,200,000
Total population and services offered 1,548,000 1,733,600
Source: Ventanillas de Salud: Reporte de indicadores/Health Windows Indicator Report*The population attended and the number of services given do not coincide with the total of the population attended (1,548,000), on occasions more than one service is given to each person.

Health Windows ProgramVentanillas de Salud
Total number of Ventanillas in operation 50
Each ventanilla offers services to Between 100 to 300 people
Free screening tests during health fairs and health training workshops.
More than 138,000
People refered to community clinics, health centers, and public hospitals.
More than 137,000
Information about health insurance programs to which the population is elegible for.
136,000 people
Pre-afiliation to the “Seguro Popular.” 1,200 migrants.

Health Windows ProgramVentanillas de Salud
New Projects
Project “Second Generation VDS”
Washington, D.C., New York; Kansas, City; Portland, Oregon; Fresno, California;
and strengthening the VDS in the Border.
o Plan for continuous training, through distance and face to face workshops on:• Priority topics (HIV/AIDS, Obesity, Addictions, Mental Health,
Reproductive Health, Occupational Health, Child Health, Cancer, Tuberculosis)
• Access to Health Services
o Technical Assistance to Manage Resources. o Advisory Board for the VDS integrated by the different partnerships
that support the VDS and the Federal Government. o For the VDS at the border an additional component to increase the
population attended.

• NEXT STEPS Logic Model developed to reflect the Second Generation
Programming.
Top three health concerns identified by all 5 VDS are: Diabetes (includes obesity, nutrition,.) Cancer (includes breast, cervical.) Sexual Health (includes HIV, STDs, Woman’s reproductive
health)
Based on the success and effectiveness of the influenza vaccination campaign, through the VDS in collaboration with the National Vaccine Program Office and the Office of Minority Health, identify new immunization campaigns' Identify available tools that assist in tracking immunizations for immigrants in the U.S. and Mexico.
Template report for funding purposes
VDS TRAINING IN WASHINGTON D.C.

Binational Health Week

Binational Health WeekResults
Approximately 500,000 people received health information
6,000 activities on prevention and health promotion
Chronic degenerative diseases
Communicable DiseasesMental Health
Women's HealthHealth Services in the US
Oral Health

Binational Health Week (2012)
XII Edition of the Binational Health WeekInaugural Ceremony: Oaxaca, México
Closing Ceremony: United States
Topics:
Access to Health ServicesWomen’s HealthObesity and DiabetesHIV/AIDSAdolescent HealthAddictions Occupational Health

Repatriation of Seriously Ill Mexicans
Ensure the medical treatment of ill repatriated nationals to the country

• ARTICULATION OF ACTIVITIES AND INFORMATION NETWORKS
• SYNCHRONIZATION FOR MULTIPLYING EFFECTS
• SUSTAINABILITY OF INSTITUTIONAL EFFORTS
• SIMULTANEOUS PUBLIC HEALTH INTERVENTIONS

BUILDING BINATIONAL PARTNERSHIP:
• SHARING PERSPECTIVES AND RESOURCES
• DECISION MAKING CAPABILITIES• EVIDENCE: SOLID BASIS FOR ACTION