
Metabolic effects of cancer - UPV/EHUculos/CL091.pdf · 246-254 Metabolic effects of cancer R. G....
9
cc :1ii~. Review Br. J. Surg. 1990,Vol. 77. March. 246-254 Metabolic effects of cancer R. G. Douglas and J.H.F.Shaw Department o, Surgery. Auckland Hospital. Park Road, Auckland 1, New Zealand Correspondence lo: Associate ProfessorJ. H. F. Shaw The potential causesof derangedmetabolism in cancer are discussed with emphasis on changesin energy metabolism of glucose, fat and protein. Theimplications of these changes for the treatment ofcachexia are thenconsidered Key"ords: Cancer, cachexia, metabolism, glucose, fat, protein, parenteraJ nutrition presence of the tumour itself is capable of elevating the RME. However, hypermetabolism is not an invariable finding in cancerpatients who have lost weight, with large serieshaving been reported recently which have failed to demonstrate a significant increase in the resting metabolic rate of cachectic cancer patients when compared with patients with weight loss of a similar magnitude due to benign disease or with weight-stablecancer patientsI9.20. In a series consisting of 200 patients with a variety oftumour types 29 per centhad a resting metabolic expenditure that was 10 per cent higher than that predicted by the Harris-Benedict equation, 31 per cent were found to be hypometabolic using the same criterion and no relationship was demonstrated between RME and weight loss or tumour burden21. Although so me of the disparity in the findings of these studies is no doubt a reflection of difTereÍlces in experimentalmaterial and methodology, it is likely that they are reflecting a true heterogeneity ofresponseto the tumour bearingstate. It is now clear that cancers arising from certain tissues, such as sarcomas22, leukaemias23 and bronchial carcinomas24,fre- quently provoke a hypermetabolic response, whereaspatients with pancreatic and hepatobiliary tumours tend to be hypometabolic2 s. Many cancer patients with advanced disease have a reduced caloric intake. In normal people or in patients with benign disease, semistarvation is attended by a reduction in RME26.27, so in an undernourishedcancer patient even a normal metabolic rate represents a failure of this adaptive responseI4.28. The mechanism by which malignant tissuealters the energy expenditure of the host is not clear. It is unlikely that increased energy consumption by the tumour itself is responsible in human tumours as it is rafe for tumours to account for more than 5 per cent of body weightl3. More plausible is the hypothesis that mediators are released by somecancerswhich alter host metabolism29.3o, and some of the changes that may occur are discussed in subsequent sections. Cachexiais commonly the causeof death in cases of advanced malignancyl, and cancerpatients who have lost a significant percentage of their body-weight before 8urgical treatment are subjectto a much greater risk of postoperative mortality and morbidity2-4. There is no doubt that reduced oral intake resulting from anorexia or obstruction of the gastrointestinal tract plays a very significant role in the development of the cancer cachexia syndrome. However, whereas the metabolic response to uncomplicated starvation acts to limit the consumption of host reserves, in the cachectic cancer patient there is often an accelerated mobilization and oxidation of energysubstrates and loss of nitrogenS-7.Thesechanges are a consequence of alterations in intermediary metabolism associated with cancer8. Understandingthe metabolic response to cancer hasbecome increasingly important over the last two decades with the introduction of efTective and safe parenteral nutrition techniques9. It is nowpossible to provide sufficientcaloriesand nitrogen to all cancer patients, but the metabolic milieu associated with advancedcancer may retard the restoration of leanbody mass1o. In the following review the manner in which malignant tumours afTect host metabolism will be presented, and the efTectiveness of the available therapeutic options will be discussed. One consistent feature of data from metabolic studies in cancer patients is the range of response between individuals, even whencomparing those with the samediagnosisand stage of disease1l. The interpretative difficulties are compounded by many reports comparing small heterogeneous groups of cancer patients with equally small groups of controls, which may well be poorly matched for age or weight loss. To overcomesome of these problems laboratory models have beendeveloped in which malignant cells of identical genotype are transplanted into genetically uniform animalsl2. However, the growth dynamics and tumour-to-host weight ratios frequently do not resemble thoseobserved in patients, and this reviewwill present mainly data from patient studies. Changes in energy metabolism The hypothesis that tumour bearing increases energy expenditureand results in a cumulative negativeenergy balance and progressive weight loss has beenexhaustivelyinvestigated, and there is now a substantial body of supportive evidence. Bozzetti el al.13 studied a heterogeneous group of patients with advanced tumours and found a highly significant correlation between the resting metabolic expenditure (RME) and the magnitude of weight loss,and other groups of researchers have similarly found elevated RMEs in patients with cancer cachexial4-18. There are a few anecdotal reports of casesin which successful antineoplastic therapy has reduced energy expenditure in hypermetabolic patientsI4.18, suggesting that the Changes in glucose metabolism There are many reports describing an increased rate of endogenous glucoseproduction in cancer patients11.22.23.31-33 (Figure 1), and considerable research effort has beendirected towards determining the mechanismand significance of this occurrence. It is clear that the magnitude of the increase in glucose turnover is influenced by tumour stage6.3S and histology, and that it is associatedwith cancer cachexia36. In this section,some of the observationsmade in cancerpatients of changesin glucose metabolism will be summarizedand the implications that these have on energy balance ,,'ill bediscussed, Gluconeogenesis Shawand Wolfe6 have defined glucosekinetics in a group of
Transcript of Metabolic effects of cancer - UPV/EHUculos/CL091.pdf · 246-254 Metabolic effects of cancer R. G....

cc
:1ii~.
Review
Br. J. Surg. 1990, Vol. 77. March.246-254 Metabolic effects of cancer
R. G. Douglas andJ.H.F.Shaw
Department o, Surgery. AucklandHospital. Park Road, Auckland 1,New ZealandCorrespondence lo:Associate Professor J. H. F. Shaw
The potential causes of deranged metabolism in cancer are discussedwith emphasis on changes in energy metabolism of glucose, fat andprotein. The implications of these changes for the treatment of cachexiaare then consideredKey"ords: Cancer, cachexia, metabolism, glucose, fat, protein, parenteraJ nutrition
presence of the tumour itself is capable of elevating the RME.However, hypermetabolism is not an invariable finding incancer patients who have lost weight, with large series havingbeen reported recently which have failed to demonstrate asignificant increase in the resting metabolic rate of cachecticcancer patients when compared with patients with weight lossof a similar magnitude due to benign disease or withweight-stable cancer patientsI9.20. In a series consisting of 200patients with a variety oftumour types 29 per cent had a restingmetabolic expenditure that was 10 per cent higher than thatpredicted by the Harris-Benedict equation, 31 per cent werefound to be hypometabolic using the same criterion and norelationship was demonstrated between RME and weight lossor tumour burden21.
Although so me of the disparity in the findings of these studiesis no doubt a reflection of difTereÍlces in experimental materialand methodology, it is likely that they are reflecting a trueheterogeneity ofresponse to the tumour bearing state. It is nowclear that cancers arising from certain tissues, such assarcomas22, leukaemias23 and bronchial carcinomas24, fre-quently provoke a hypermetabolic response, whereas patientswith pancreatic and hepatobiliary tumours tend to behypometabolic2 s.
Many cancer patients with advanced disease have a reducedcaloric intake. In normal people or in patients with benigndisease, semistarvation is attended by a reduction in RME26.27,so in an undernourished cancer patient even a normal metabolicrate represents a failure of this adaptive responseI4.28.
The mechanism by which malignant tissue alters the energyexpenditure of the host is not clear. It is unlikely that increasedenergy consumption by the tumour itself is responsible inhuman tumours as it is rafe for tumours to account for morethan 5 per cent of body weightl3. More plausible is thehypothesis that mediators are released by some cancers whichalter host metabolism29.3o, and some of the changes that mayoccur are discussed in subsequent sections.
Cachexia is commonly the cause of death in cases of advancedmalignancyl, and cancer patients who have lost a significantpercentage of their body-weight before 8urgical treatment aresubject to a much greater risk of postoperative mortality andmorbidity2-4. There is no doubt that reduced oral intakeresulting from anorexia or obstruction of the gastrointestinaltract plays a very significant role in the development of thecancer cachexia syndrome. However, whereas the metabolicresponse to uncomplicated starvation acts to limit theconsumption of host reserves, in the cachectic cancer patientthere is often an accelerated mobilization and oxidation ofenergy substrates and loss of nitrogenS-7. These changes are aconsequence of alterations in intermediary metabolismassociated with cancer8.
Understanding the metabolic response to cancer has becomeincreasingly important over the last two decades with theintroduction of efTective and safe parenteral nutritiontechniques9. It is now possible to provide sufficient calories andnitrogen to all cancer patients, but the metabolic milieuassociated with advanced cancer may retard the restoration oflean body mass1o. In the following review the manner in whichmalignant tumours afTect host metabolism will be presented,and the efTectiveness of the available therapeutic options will bediscussed.
One consistent feature of data from metabolic studies incancer patients is the range of response between individuals,even when comparing those with the same diagnosis and stageof disease1l. The interpretative difficulties are compounded bymany reports comparing small heterogeneous groups of cancerpatients with equally small groups of controls, which may wellbe poorly matched for age or weight loss. To overcome someof these problems laboratory models have been developed inwhich malignant cells of identical genotype are transplantedinto genetically uniform animalsl2. However, the growthdynamics and tumour-to-host weight ratios frequently do notresemble those observed in patients, and this review will presentmainly data from patient studies.
Changes in energy metabolism
The hypothesis that tumour bearing increases energyexpenditure and results in a cumulative negative energy balanceand progressive weight loss has been exhaustively investigated,and there is now a substantial body of supportive evidence.Bozzetti el al.13 studied a heterogeneous group of patients withadvanced tumours and found a highly significant correlationbetween the resting metabolic expenditure (RME) and themagnitude of weight loss, and other groups of researchers havesimilarly found elevated RMEs in patients with cancercachexial4-18. There are a few anecdotal reports of cases inwhich successful antineoplastic therapy has reduced energyexpenditure in hypermetabolic patientsI4.18, suggesting that the
Changes in glucose metabolism
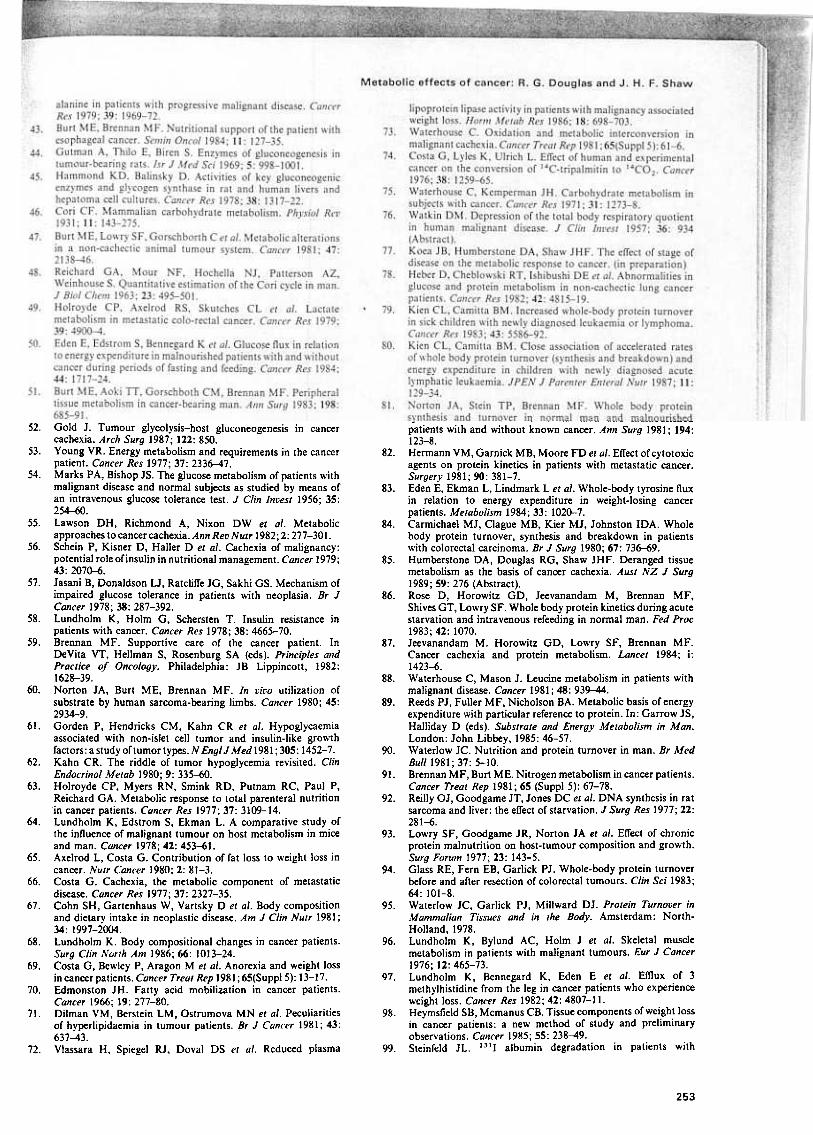
There are many reports describing an increased rate ofendogenous glucose production in cancer patients 11.22.23.31-33(Figure 1), and considerable research effort has been directedtowards determining the mechanism and significance of thisoccurrence. It is clear that the magnitude of the increase inglucose turnover is influenced by tumour stage6.3S andhistology, and that it is associated with cancer cachexia36. Inthis section, some of the observations made in cancer patientsof changes in glucose metabolism will be summarized and theimplications that these ha ve on energy balance ,,'ill be discussed,
GluconeogenesisShaw and Wolfe6 have defined glucose kinetics in a group of

Metabolic effects of cancer: R. G. Douglas and J. H. F. Shaw
t release of lactate4O. Indeed, lactic acidosis has been reportedin sorne cancer patients, particularly in those with disserninatedhaernatological rnalignancy41, and a greater rate of hepaticsynthesis of glucose frorn lactate has been reported byseveral research groups31.32. Increased gluconeogenesis frornalanine42.43 has been described in cancer patients, which wouldact to accelerate wasting of body protein and which will bediscussed in greater detail in a subsequent section. Thecontribution of glycerol toward encouraging gluconeogenesisis likely to be rninor32. The balance of available evidencesuggests that the increased rafe of gluconeogenesis is substrateled; however the isolation of induced gluconeogenic enzyrnesfrorn hepatocytes of cancer-bearing laboratory anirnals44.4Ssuggests that this rnay not be exclusively so.
35.0
¡ ..1¡j11
*
15.t
c'é~~"OE
3.,(JCIV
:v.,c.c.IV
'O.,;;a: 10
5.0
oVolunteers Lo~aljzed Advanced Sepsis
Figure 1 The influence of locali:ed or non-II'eight-losillg cancer,advanced or lI'eighl-losing cancer, and sepsis on lhe Tale of produclionof glycerol (.), free fally acids (O), and glucose (m) compared lI'i/h
Tales in heallhy t'olunleers. .P<O'OJ. tP<O.O5. (Modifiedfrom Shal"and Wolfe,.34)
patients with early (limited to the gut wall) and advancedgastrointestinal malignancies. Whereas the rate of glucoseturnover in the group of patients with early lesions wasindistinguishable from that seen in normal volunteers, glucoseproduction was significantly increased in patients withadvanced lesions. Similarly, tumour histology has al so beendemonstrated to influence the extent of increase of glucoseproduction. The glucose turnover rates in sarcoma22 andleukaemia23 patients have been reported to be respectively twoand nearly three times the value determined in normalvolunteers, whereas the glucose turnover rate in lymphomapatients does not ditTer significantly from normaJ23. Otherresearchers have studied the etTect of weight loss on glucoseturno ver. Holroyde el al. have reported that weight-stablecancer patients have rates of glucose production similar to thoseof normal volunteers. However, those with progressive weightloss have markedly elevated rates37. This is a particularlysignificant finding as progressive weight loss secondary touncomplicated starvation is attended by a reduction in glucoseturnover38.
The hepatic production of glucose becomes less sensitive tothe usual homeostatic regulating mechanisms in some patientswith cancer. If a normal volunteer is infused with glucose at arate of 4 mg kg-1 h -1 (the dose of a typical total parenteral
nutrition regimen) the suppression of endogenous glucoseproduction will approach 100 per cent39. In patients withadvanced gastrointestinal cancer, there is a 70 per centreduction in endogenous glucose production6, whereas insarcoma and leukaemia patients hepatic glucose production isreduced by less than one-third22-23.
The cause of elevated hepatic gluconeogenesis and itsreduced suppressibility in patients with malignant tumours isunclear. The plasma le veIs of the hormones involved in glucosehomeostasis (insulin, cortisol, growth hormone) are notconsistently deranged in cancer patients36 and are unlikely toplaya significant role, although insulin receptor insensitivitywould be consistent with increased gluconeogenesis. Theincreased availability of the gluconeogenic substrates lactate,alanine and glycerol presents a plausible mechanism and, ofthese, lactate is probably the most quantitatively important.More than 50 years ago, Warburn described the dependenceof malignant cells on anaerobic glycolysis and the resultant
Cori c)'clingIn the Con cycle46, lactate released as a result of glycolysis inpenpheral tissues is used as a gluconeogenic substrate by theliver. This process consumes energy, as six ATP (adenosinetriphosphate) molecules are required for the resynthesis ofgIucose from lactate whereas only two are produced by theglycolytic degradation of each glucose molecule. When theanaerobic glycolysis occurs in malignant tissue, the energy costto the host is compounded by the los s of glucose parasitizedby the tumour47. Accordingly, there has been considerableinterest in determining the extent of Con cycling in cancerpatients as it may be one ofthe fundamental metabolic changescausing cancer cachexia.
The rate of Con cycling can be easily measured using14C- and 63H-labelled glucose tracers48. Increased rates ofcycling have been measured by Holroyde et al.49 in a group of20 patients with metastatic colorectal cancer when comparedwith control subjects of comparable age and sexo It was inferredthat tumour glycolysis was responsible for the excess lactateproduction, although this supposition was not confirmed bythe lack of correlation between the extent of tumour burdenand the increased rate of Con cycling. Evidence for the cancerper se being responsible for increasing the rate of Con cyclinghas been provided by the study of Eden et al. s°, who comparedthe rate of Con cycling in patients with cancer cachexia witha control group of patients who had suffered a similar degreeof weight loss but from benign causes. The rate of Con cyclingin both the fasted and enterally red states was significantlyhigher in the patients with malignant disease, suggesting thatit was the cancer per se that was responsible for this increase.However, Burt et al.s1 have measured an increased rate ofrelease of lactate from the forearm of a small group of patientswith localized carcinoma of ~he oesophagus, implying that thetumour is capable of effecting a distant influence on themetabolism of carbohydrate in host tissue. It is likely, althoughstill conjectural, that increases in both tumour and host tissueglycolysis are responsible for the observed changes in wholebody lactate metabolismo :
The raJe played by such futile cycles in the pathogenesis ofcancer cachexia has been the subject of much debate. Gold hasperformed considerable work in this field and describes the'fundamental position of tumour glycolysis-host gluconeo-genesis in the production of cancer cachexia'S2. The rate ofCori cycling has been measured by Holroyde et al.37 in twogroups of cancer patients, one with progressive weight loss andthe other with stab]e weight. The rate of Con cycling wasconsiderably e]evated in the first group but normal in thesecond, suggesting that the energy ]ost by the futi]e cycling wasresponsib]e for the weight loss. However, such findings havenot been universally reproduced: Kokal et al. were unable todemonstrate any significant differences in g]ucose cycling ratesas a function of pre-illness weight IOSS3S.
Eden el al., having demonstrated an increase i~ glucoseturnover and g]ucose cycling in cancer patients, esti~ated thepotential energy cost to the cancer patientSl. They calculatedthat, ir the incomp]ete oxidation of glucose wete to besubstituted by the complete oxidation of fat, this would lead
25.
20.0

Metabolic effects of cancer: R. G. Douglas and J. H. F. Shaw
an accelerated rafe, the extra glucose production is beingconsumed in Cori cycling38.
to an increase in energy expenditure of 250-300 kcaljday anda loss of 0.9 kg fatjmonth. However, a contrary argument hasbeen forwarded by YoungS3, who estimated that if only15 per cent of the total lactate production is <1xidizedcompletely and 85 per cent is conve{ted to glucose then 'therewill be maintenance of high energy phosphate balance. ..andit is difficult to accept therefore that changes in Cori cycleactivity are a significant cause of the marked body wasting inpatients with progressive neoplasia'. These conflicting butequally well considered viewpoints underscore the greatdifficulty in accurately determining a long-term energy balancein cancer patients and, accordingly, the influence that changes inmetabolic efficiency have on that balance. Nevertheless, theaccelerated activity of energy wasting cycles is likely to playsome rol e in the development of cancer cachexia.
Fat metabolismIn many cases of cancer cachexia the greater proportion ofweight loss is caused by depletion of body fat 18.65.66. Loss ofbody fat with malignant disease has been confirmed by a varietyof anthropometric techniquesI4.67.68, and muscle biopsysamples from patients with cancer have been found to haveonly half the amount of fat present in normal controls69.Although the consumption of fat reserves in cancer patients ispartlya reflection of reduced caloric intake, several changes inlipid metabolism have been described which probably resultfrom cancer bearing itself, and these will be discussed in thefollowing paragraphs. Fat metabolism in cancer patients hasbeen the subject of far les s research effort iban carbohydratemetabolism, and correspondingly fewer conclusions can bedrawn.
Fat mobili=ation
Triglyceride in adipocytes, which represents the majar storagefonn of fat, is mobilized by hydrolysis to glycerol and free fattyacids which are released into the plasma. Using stable isotopictracers Shaw and Wolfe7 have measured the tumover rates ofglycerol and free fatty acids in weight-stable and weight-losingpatients with gastrointestinal malignancies and compared thesewith rates in normal volunteers (Figure 1). There were nosignificant difTerences in whole body glycerol and fatty acidkinetics between the weight-stable patients and the nonnalvolunteers, but those with weight loss had significantly elevatedrates of release into the plasma of both glycerol and free fattyacids. These data, which are in agreement with the work ofothersl 5.70, suggest that the loss of fat reserves seen in patientswith cancer cachexia results from increased fat mobilization
.rather than decreased synthesis. However, definitive studies ofthe inf1uence of cancer on lipogenesis in human subjects havenot been perfonned, so it is possible that both mechanisms areoperating to reduce body fat stores.
Insu/iI! and g/ucase uptakeImpaired glucose tolerance in patients with leukaemia,lymphoma and a variety of epithelial tumours was describedin the 1950s by Marks and Bishop54 and resistance to bothexogenous and endogenous insulin has been subsequentlydemonstrated in cancer patients55. The insulin bindingreceptors of monocytes extracted from cancer patients arenormal, implying that the defect is postreceptor in site56. Jasaniel al. have reported a decrease in the sensitivity of pancreatic1>' cells to insulinogenic stimuli57, while others have determinedthat reductions in both peripheral sensitivity and pancreaticreleáse are responsible for the observed glucose intolerance58.However, the cause of the glucose intolerance in the setting ofmalignancy has undergone some critical reappraisal in recentyears, and it has been suggested that it mar be due tointercurrent factors such as weight loss, bed rest and sepsisrather than to the cancer per se36.3 7.
For the plasma glucose concentration to remain constant,the increase in glucose production observed in some cancerpatients must be attended by an equal increase in the rafe ofclearance of glucose from the plasma compartment. This occursdespite the prevailing state of insulin resistance. Resultsobtained from animal tumour models have suggested that thetumour acts as a 'glucose trap', consuming large quantities ofglucose in the process of anaerobic glycolysis59. The hightumour-hostweight ratio in such models (sometimes exceeding40 per cent) casts a shadow on their applicability to patients;human tumours rarely exceed 5 per cent of body weight andtherefore only very substantial metabolic changes within thetumour itself would be detectable at the whole body level.However, the glucose trap concept is supported by thedemonstration of increased glucose uptake across soft tissuesarcoma-bearing limbs compared with the opposite non-tumour-bearing limb6°. Interestingly, the forearm glucoseuptake in patients with oesophageal cancer has been found tobe significantly greater than in healthy controls by Burt el al.51.The plasma insulin levels were lower in the cancer patients soit is unlikely that this hormone mediated the observed changes.The authors speculate that increased non-suppressible insulinlike activity (NSILA) mar be responsible. NSILA is the likelycause of the hypoglycaemia seen with some non-islet celltumours in humans61, and is probably elaborated by thetumour itself62. The wider Tole of tumour-related NSILAremains a matter of conjecture.
Lipid c/earanceLipoprotein lipase is the enzyme responsible for the clearanceof triglyceride molecules from the plasma. Although hyper-lipidaemia is not a marked finding in cancer patients, it has beenfound in association with some tumours i 1, and the proposed
mechanism is a reduction in activity of this enzyme. Supportfor this hypothesis has recently been provided by Vlassara elal.72 who found that the plasma lipoprotein activity ina groupof cancer patients was reduced and that there was a correlationbetween weight loss and the extent of reduction of enzymeactivity. The decreased lipoprotein lipase activity that occursin uncomplicated starvation is mediated by a reduction in theplasma level of insulin. However, the insulin levels in thepatients in Vlassara's study were normal, suggesting that thiswas not the mechanism responsible for the observed changes.
Fal oxidalionThere is a considerable body of data to suggest that fat isoxidized at an increased rate in cancer patients 14.1 5.50.63.74,
although as is common in studies involving small numbers ofpatients with heterogeneous conditions this finding is notuniversal75. Fat oxidation rates determined in a series of 70patients with colorectal or gastric cancer by a combination ofindirect calorimetry and urinary nitrogen excretion have beenrecently reported by Hansell el al.19. They found that thepatients with cancer had significantly higher fat oxidation rates(and significantly lower carbohydrate oxidation rates) thancontrol patients with benign disease. Patients with cancer andweight loss oxidized fat more rapidly than either patients withcancer and no weight loss or patients with weight loss causedby benign disease. Similarly, patients with hepatic metastases
G/ucose oxidationAlthough several studies ha ve reported modest increases in therate of glucose oxidation in cancer patientsI9.37.63, the increasesare not commensurate with the greater glucose availability,which implies a reduction in efficiency ofthe oxidative process6.In skeletal muscle isolated from patients with cancer, theactivities of enzymes regulating oxidative metabolism have beenfound to be reduced64, which is consistent with data gatheredfrom studies of whole body glucose oxidation. It is likely that,in cancer patients in whom glucose production is occurring at

Metabolic effects of cancer: R. G. Douglas and J. H. F. Shaw
had a significantly greater fat oxidation rate than patients withlocalized malignant disease. Others have reported that in cancerpatients a greater percentage ofthe body's energy requirementsis provided by fat than in normal volunteers, and that fat ismobilized and oxidized with at least the same efficiency as inhealth 1 S. It is unlikely that malignant tissue per se is responsible
for the increased fat oxidation, but rather that the changesinduced in the regulation of metabolic pathways occurring innormal host tissues in the cancer-bearing state favour fatoxidation.
hypothesis has recently been examined in substantial groups ofcancer patients and normal controls2° and, although the cancerpatients had a significantly higher rate of protein turnover, theirresting metabolic expenditure was not increased nor was thereany correlation between individual rates of protein turnoverand energy expenditure. These results suggest that when proteinturnover is increased in cancer patients it is unlikely to playamajor role in the development of cancer cachexia.
The influence of the cancer per se on whole body proteinmetabolism has been a matter for some conjecture. The conceptofthe tumour having a 'nitrogen trap' which parasitizes aminoacids from healthy tissues was developed by researchersworking with rapidly growing transplantable animal tumourmodels92.93, but it is unlikely to be applicable to patients inwhom tumour bulk is usuaJly a much smaller percentage ofbody weight. It is more plausible that the tumour is releasinga humoral agent or agents which efTect the observed metabolicchanges. Glass el al.94 attempted to quantify the influence oftumour bearing on protein dynamics by studying a group ofpatients with colorectal carcinomas just before and 12 weeksafter resection. They were unable to demonstrate a significantdifTerence in whole body protein metabolism after tumourexcision, and concluded that the primary tumour does not alterprotein kinetics. However, the study group comprised patientswith localized lesions whose nitrogen flux was comparable tothat of normal controls, and so it is perhaps not surprising thattumour excision caused no change.
Protejo metabolism
Loss of body protein in patients with cancer cachexia ismanifested clinicalIy as skeletal muscle atrophy and hypo- 'albuminaemia, and is associated \\'ith an impaired tolerance oftreatment procedures2, Significant protein loss may occur inpatients who are maintaining what would be in health anadequate intake ofnitrogen and calories, implying that tumourbearing per se is able to exert a detrimental influence on wholebody nitrogen balance. However, a negative nitrogen balanceis not an inevitable accompaniment of malignancy. Nearly 30years ago, Watkin 76 measured nitrogen balance in a large group
of cancer patients and found a range of responses from positiveto very negative balances, and he thoughtfully related the morenegative nitrogen balances with increased disease 'activity'(reflecting weight loss, increased resting energy expenditure andother factors). This concept concurs with OUT own observations,in which patients with aggressive metastatic disease 77 or thosewith histological tumour types frequently associated with apoor prognosis (e.g. sarcoma22) tend to lose proteinsignificantly more rapidly than those with less aggressivedisease.
Skeletal muscle metabolismWhole body protein turnover studies reflect the sum total ofsynthesis and degradation rates in the individual tissues.Accordingly, it is possible for synthesis andfor catabolism tobe reduced in one particular tissue while whole body turno veris increased9s. Several investigators have attempted todetermine the manner in which the protein kinetics ofindividualtissues are affected by cancer. Lundholm et al. used the rate ofincorporation of [14C]leucine by skeletal muscle biopsiesincubated in vitro to compare synthesis rates in a heterogeneousgroup of 43 cancer patients with 55 age- and sex-matchedcontrols96. They found that the capacity of the muscle libresremoved from the cancer patients to incorporate the aminoacid tracer was signilicantly impaired, and that having beenincorporated the rate of loss of tracer was al so greater in thecancer patients. The group concluded that malignant tumoursprovoke a decrease in protein synthesis and an increase inprotein degradation. In a subsequent series of experiments thesame group used arteriovenous differences in levels of3-methylhistidine, an amino acid which is relatively specilic toskeletal muscle, and found that there was no signilicantdifference in the rate of appearance of this marker in patientswith cancer and control s who were depleted with benigndisease91. They concluded that the effect of malignant tissuewas to reduce the rate of protein synthesis. As skeletal musclecomprises the majority of the body's protein, changes inskeletal muscle protein kinetics are subsequently likely to bemanifested at the whole body level. The results of Lundholm'sgroup are therefore at odds with a substantial body of wholebody kinetic data which suggests that whole body proteinsynthesis is either unchanged or increased2O.18-80.83.84.Recently, Shaw and colleagues have determined in vivofractional synthesis rates (FSR) of muscle in patients withbenign disease, weight-stable patients with malignant disease,and patients with cancer cachexia8s. There were no signilicantdifferences in the rate of muscle FSR between patients withbenign disease and weight-stable cancer patients, but there wasa signilicant increase in FSR in those patients with cancercachexia. Given that these patients had lost weight (andpresumably protein), this implies the occurrence of an evengreater increase in the rate of degradation of muscle protein,and indeed increased activities of Iysozymal enzymes isolatedfrom skeletal muscle of cancer patients have been reported64,96
Whole body protein kinetics
The rate ofwhole body protein turnover can be measured usingisotopically labelled amino acids as metabolic tracers, and anumber of such studies in cancer patients have produced aspectrum of results. A consistent 50-70 per cent increase inturnover rates in large groups of patients with lung andcolorectal cancer has been reported2O and there have beensimilar findings in patients with small cell cancer78 and inchildren with leukaemia 79.8°. Norton et al.81 found aninconsistent res pon se in a di verse group of cancer patients,whereas others have found no difference between patients withcancer and age-matched normal controls82. Several investigatorshave suggested that whole body protein turnover is increasedwith advancing stage of disease and weight loss 78,83-85.
This accelerated protein turnover seen in many cancerpatients contrasts with the reduction in total protein turnoverobserved in cases of simple starvation86. Recently, to distinguishthe metabolic effect of pure malnutrition from those of cancerbearing, Jeevanandam et al. compared the protein kinetics ofmalnourished cancer patients with those of patients who wereequally malnourished as a result of benign disease and withthose of a group of starved normal subjects87. Compared withthe non-cancer patients and starved normal subjects, wholebody protein turnover in the cancer patients was elevated by32 and 35 per cent respectively. These results confirm theobservations made by Brennan nearly a decade earlier that incancer cachexia there is a maladaptation to the starved state,with a continued mobilization of protein and calorie reservesin the Cace of a reduced intake5. An example of this is thedecreased efficiency with which simple substrates limit the rateof gluconeogenesis and protein flux in patients with advancedcancer31,73,88.
Protein turnover is an energy expensive process whichaccounts for 10-20 per cent of basal metabolic expenditure89.The reduction in protein turnover seen in simple starvationaccordingly represents an adaptive response90, and it has beensuggested that its failure to occur in some cases of malignancyis responsible for the development of cancer cachexia91. This

Metabolic effects of cancer: R. G. Douglas and J. H. F. Shaw
Hepatic protein s}'nthesisThere is a paucity of data on the rate ofhepatic protein synthesisand catabolism in cancer patients. Using the same in vitromethodology employed in their study of skeletal musclemetabolism, Lundholm et al. ,have reported an increase in therate of protein synthesis in liver biopsies from cancer patients64.These results are consistent with those from our own laboratory,in which we have demonstrated in vivo a significant increase inthe fractional synthetic rate of protein of hepatic tissue inpatients with cancer cachexia, but no dilTerence between thehepatic FSR of weight-stable cancer patients and patients withbenign disease8S. There are no data describing the rate ofcatabolism of structural hepatic proteins in cancer-bearingpatients. However, a recent report in which organ imagingtechniques were used to determine liver size in a small numberof patients with cancer cachexia suggested that there wasrelative sparing of visceral protein98, which implies that theobserved increase in hepatic protein synthesis is likely to beattended by an equal increase in protein catabolism.
Many patients with advanced malignancy are hypo-albuminaemic, which may result from a reduced rate ofsynthesis, an increased rate of breakdown or a loss of albuminfrom the intravascular volume. As albumin degradation rateshave been demonstrated to be normal in cancer patients99,100and with the exception of cases of malignant elTusion thedistribution of albumin is relatively unchanged, this impliesthat the rate of synthesis is decreased. However, this is contraryto some recent data from our laboratory in which we measuredthe rate ofsynthesis of albumin using a [14C]leucine marker1ol.A significantly higher rate of albumin synthesis wasfound in those patients with cancer cachexia compared withrates in cancer patients who were weight stable, and in patients\\lth benign disease. It is clear that the influence of malignancyon hepatic structural and secretory protein synthesis has Jetto be clearly resolved.
protein at a maximal rate and that its rate of growth cannotbe significantly affected by the provision ofextra nutrientslO9.
It is generaIly agreed that approximately 130 per cent oftheRME needs to be provided to cancer patientsllO, but there arefew data that clearly indicate which is the optimal caloric source.Despite some cancer patients having marked changes inintermediate metabolism, they have been shown to be able tooxidize efficiently both infused glucose and fatlll. There is someevidence from a laboratory tumour model that the provisionof calories as fat retards tumour groWth 112, but this has notbeen duplicated in other animal models 113 and there is no
evidence from human studies to support these findings. Shawand Holdaway have demonstrated that infusion of isocaloricvolumes of glucose and fat (administered as Intralipid 20,KabiVitrum Laboratories, Stockholm, Sweden) have an equalability to spare protejo at the whole body level, although lipidinfusion fails to suppress endogenous glucose productionl14.Infused glucose is able to suppress gluconeogenesis in cancerpatients42, but it does not do so with the same efficiency as inhealthy volunteers6.
Although it is possible to restore the weight of a cachecticcancer patient with parenteral nutrition, it has been questionedwhether the weight gain is primarily as fat II s or whether it
represents a useful replenishment of the lean body mass. Thereare several reports of positive nitrogen balances being achievedin cancer patients on TPN43.116, but these studies requiremeticulous sample coIlection and may be difficult to interpretin the presence of a growing tumour. However, longitudinalstudies of body composition ayer a 1 month course of TPNhave shown no increase in total body nitrogen, despite increasesin body fat and total body potassiumlo. These data arecompatible with the results of isotopic studies, which havedemonstrated an attainment ofnitrogen equilibrium with TPN,but not the protein anabolism which is readily achievable inpatients depleted by benign diseasel17 (Figure 2). There isevidence to suggest that leucine is central in the regulation ofprotejo metabolisml18, and leucine-enriched TPN has beenprovided to cachectic cancer patients in an attempt to improvethe nitrogen balance I 19.12°, with a smaIl improvement in
nitrogen balance being demonstrated.It is likely that the difficulty in achieving restoration of lean
body mass with TPN in cachectic cancer patients is partlyresponsible for the paucity of convincing evidence of itstherapeutic efficacyl03. Prospective randomized trials of lessthan 1 week of TPN have failed to demonstrate any advantageto the study group ayer the control group red ad libitumI21.122.A recently published analysis of the pooled results of 18
Treatment of cancer cachexia
,"/utritional supportFollowing the introduction of gafe total parenteral nutrition(TPN) techniques nearly 20 years ago, it was hoped that thegreat majority of cachectic cancer patients could be repletedbefore surgical treatment, radiotherapy or chemotherapy, andthat a reduction in treatment morbidity would be effected. Theenthusiasm of the initial reports describing the efficacy of TPNin cancer patientslO2 has not always been reaffirmedlO3. It hasbecome clear that providing sufficient nitrogen and calories toa patient with cancer cachexia does not augment lean bodymass as efficiently as can be achieved in a malnourished patientwith benign disease. The use of TPN in cancer patients raisesseveral questions, such as whether hyperalimentation pro motesgrowth in malignant tissue, how the TPN prescription can betailored to ameliorate the metabolic defects associated withcancer, and whether the provision ofTPN leads to an improvedpatient outcome.
The concern of clinicians that the protein and energysubstrates provided by TPN will be consumed preferentiallyby the tumour has some support from the results ofexperiments performed with animal tumour models, in whichtumour growth is encouraged more than repletion of hosttissuesIO4--IO6. However, to date, stimulation oftumour growthby TPN has not been observed in patientslO7. The most elegantevidence that TPN does not have a deleterious effect has beenprovided by Mullen el al.los who used the in rivo rate ofincorporation of [1 SN]glycine as a measure of protein synthesis.They found that the tumours of patients who were given TPNfor 7-10 days bef9re surgery were synthesizing protein no morerapidly than the tumours of the control patients who were onan ad libilum oral diet. Although some caution must be exercisedin the interpretation of these results as a net increase in tumoursize may have resulted from a reduction in the rate of proteincatabo)ism, it is most )ikely that ma)ignant tissue is synthesizing
Benign disease, Cancer, Cancer,.-.depleted depleted not depleted
Figure 2 Response 10 total parenleral nulrilion (.) 01 depleled palienlsM'ilh benign disease. cancer palienls M'ilh deplelion and cancer palienlsM'ilhoul deplelion compared wilh basal values (O). .P<O,OI, tP<O.O5.(Modifled Irom Shaw'l')

Metabolic effects of cancer: R. G. Douglas and J. H. F. Shaw
randomized trials assessing the efTectiveness of perioperativeTPN (16 of which consisted of cancer patients) concluded thatthere was little evidence supporting the routine use ofperioperative TPN, but that it may have a role in supportinga subgroup ofpatients who are at high risk123. The authors ofthis paper were generally critical ofthe methodology ofthe trialsperformed to date, and comment that the efTectiveness of TPNmay have been underestimated by inclusion of patients whowere not maInourished. Certainly, some trials have demonstrateda:dvantages to the patient who received TPN: Heatley el al.followed the postoperative course of 70 patients with gastriccancer who were randomized 10 receive either TPN for 7-10days or a nonnal diet, and reported a significant reduction inthe occurrence of wound infection in the group who receivedTPN124. A preoperative course of TPN of a similar length in'a group of patients with gastrointestinal malignancies reducedthe incidence of complications from 19 per cent in the controlgroup to 11 per cent in the treatment group, and the mortalityfrom 11 to 3 per cent12S. However, any advantage attributedto TPN must be weighed against the risks of pneumothoraxand catheter-related septicaemia.
been several attempts to counter adverse tumour-associatedmetabolic changes by administration of pharmacologícalagents. Anexample is a trial involving 101 intensively pretreatedcancer patients who were randomly assigned to receive eitherhydrazine sulphate, which inhibits a key enzyme in thegluconeogenic pathway, or a placebol26. The treatment groupexperienced significan ti Y improved weight stabilization andglucose tolerance. Megestrol acetate, an anabolic steroid, hasbeen recently reported to produce enhanced appetite andincreased weight in a group of28 patients with breast cancerl27.Nearlya decade ago Schein et al.128 argued lucidly that manyof the cancer-related metabolic derangements were a result ofinsulin resistance and suggested that many of these could beameliorated by the provision of exogenous insulin. Thisproposal has .been supported by the results obtained fromanimal model experimentationl29-131 but to date no humanstudies have been published.
Although these and other trials involving anticachecticagents have shed some light on the mechanisms of cancercachexia, no agent has yet been demonstrated meaningrully toimprove the clinical course of cancer patients.
Pharmacological manipulationAs the provision of adequate caJones and nitrogen does notensure protein accretion in cachectic cancer patients, there have
.
~ .~ Li ver .;~:;~~_.-::::..~ s
I Glucose ). r"t '"
I1 LactateCancer
~Mediators ~ co Cytokine:..'_!:~:~_hOrmonall 2
resp~nse I Free fatty.( Fat stores
Mediators of the metabolic response to cancerIt was long held that the metabolic changes observed in cancerpatients at the whole body level were a ret1ection of themetabolic activity of the malignant tissue per se. From thissupposition was born the concept of the tumour acting as aninternal parasite, trapping nitrogen and energy substrates as thehost tissues became progressively more malnourished132.Despite the alluring simplicity of this hypothesis it fails toaccount for the profound metabolic changes that have beendocumented in some patients with apparently trivial tumourburdens133, nor does it explain the changes in metabolismdetected in host tissue distant from the tumour siteS1.
An alternative theory advanced to explain these observationsis that tumours release small molecular weight proteins whichalter the activities ofvarious host enzymes30 (Figure 3). A largenumber of polypeptides and other substances secreted bytumour cells have been described, such as toxohormone134 andlipid mobilizing factor13S, to which have been attributed variousroles in the causation of cancer cachexia, largely on the basisof animal experiments. However, there is little evidence thatconvincingly relates these substances to the metabolic changesseen in cancer patients.
The similarities between the metabolic responses to sepsisand trauma to that provoked by tumours have been clearlydescribed by Brennans. The loss of nitrogen and increasedturnover of glucose and mobilization of fat which occur inFigure 3 Overview o/ Ihe proposed melabolic changes associaled wilh
advanced cancer
TabIe 1 Melabolic changes commonly associaled wilh ad¡;anced or weighl-losing cancer, severe sepsis or mulliple trauma, and deplelion due lo benign
disease (or insome cases slarvalion in normal volunleers)
Starvation ReferenceSepsisjtraumaCancer
6,31,32,37,38,141,14222,49,50,141,14255,58,143
!!-...
111
iii
7, 15, 144, 14514,15,19,145,146
t1.
ii
ii
20,77,89,141,142,1476,22,141,142116,117
!ff
ii!
i
!
13, 16, 18, 21, 25, 26, 27, 146, 148!i!/N-¡i
CarbohydratesGluconeogenesisGlucose recyclingInsulin resistance
FatLipolysisFat oxidation
ProteinWhole body fluxNet catabolism (NPC)Responsiveness of NPC to total parenteral
nutrition
EnergyResting metabolic expenditure
.No change
! (251

Ilij
Metabolic effects of cancer: R. G. Douglas and J. H. F. Shaw
severely septic or injured patients result from the combinedinfluences of counter-regulatory hormone secretion and therelease of inflammatory mediators from cells of the immunesystem136. It has been suggested that similar mediators releasedby immunocytes in response to tumour cells are respon~ible forthe metabolic response to cancel:. Cachectin, a 17 kDapolypeptide released by macrophages which acts as a mediatorofendotoxic shock137, has recently been found to share strongsequence homology with tumour necrosis factor (TNF)138, alsoa macrophage producto It may be that cachectin¡TNF is centralto the mediation of the metabolic response to both sepsis andcancer139. Recently, Wilmore andcoworkers have reported anegative nitrogen balance in cancel patients infused over a5-day period with recombinant TNF, which they attributed tothe anorexia induced by the TNF rather than to acytokine-specific efTect on protein metabolism14°. Kern andNorton have proposed a mechanism explaining the metabolicderangements of cancel cachexia in which the tumourstimulates the host's immune cells to secrete factors such ascachectin¡TNF whose primary rol e is cytotoxic, but which havesecondary metabolic efTects8.
~
Surnrnary
Malignant tumours do not have a consistent effect on theintermediary metabolism of the host. However, patients withadvanced disease and/or those demonstrating cancer-relatedcachexia typically have accelerated rates of energy substrateand protein turnover despite reduced calorie and nitrogenintake. In this manner the metabolic response to cancercachexia is opposite to that seen in uncomplicated starvation,but rather bears many similarities to the changes described inpatients with sepsis and trauma. The rates of gluconeogenesisand Cori cycling, fat mobilization and oxidation, and proteinsynthesis and degradation tend to be increased, and there isgreater difficulty in replenishing lean body mass with methods ofnutritional support (Table 1). The metabolic response to cancermay be largely effected by mediators released by cells of theimmune system, but this matter remains conjectural. Beyondthe provision of adequate calories and nitrogen, and removalof malignant tissue, there are presently no metabolic therapiesavailable which have been demonstrated to influence clinicaloutcome.
References1. Warren S. The immediate cause of death in cancer. Am J Med
Sci 1932; 185: 610-15.2. Meguid MM, Debonis D, Meguid V ec al. Nutritional support
in cancer. Lancec 1983; ii: 230-1.3. Hickman DM, Miller RA, Rambeau lL ec al. Serum albumin
and body weight as predictors of postoperative course incolorectal cancer. JPEN J Parencer En/eral Nulr 1980;4: 314-16.
4. Con ti S, West lP, Fitzpatrick HF. Mortality and morbidityafter esophagogastrectomy for cancer of the esophagus andcardia. Am Surg 1977; 43: 92-6.
5. Brennan MF. Uncomplicated starvation ¡;ersus cancer cachexia.Cancer Res 1977; 37: 2359-64.
6. Shaw lHF, Wolfe RR. Glucose and urea kinetics in patients"ith early and advanced gastrointestinal cancer: the responseto glucose infusion, parenteral feeding, and surgical resection.Surgical1987; 101: 181-91.
7. Shaw lHF, Wolfe RR. Fatty acids and glycerol kinetics in septicpatients and in patients with gastrointestinal cancer: theresponse to glucose infusion and parenteral feeding. Ann Surg1987; 205: 368-76.
8. Kern KA, Norton lA. Cancer cachexia. J P EN J Paren/er EnceralNucr 1988; 12: 286-98.
9. Dudrick Sl, Steiger E, Long 1M, Rhoads lE. Role of parenteralhyperalimentation in management of multiple catastrophiccomplications. Surg Clin Norch Am 1970; 50: 1031-8.
10. Shike M, Russell DM, Detsky A ec al. Changes in bodycomposition in patients with small-cell lung cancer: the efTectoftotal parenteral nutrition as an adjunct to chemotherapy. AnnInCern Med 1984; 101: 305-8.
11. Holroyde CP, Skutches CL, Boden G el al. Glucose metabolismin cachectic cancer patients with colorectal cancer. Cancer Res1984; 44: 5910-13.
12. Garratini S, Guatani A. Animal models for the study ofcancer-induced anorexia. Cancer Treal Rep 1981; 65 (Suppl 5):23-35.
13. Bozzetti F, Pagnoni AM, Del Vecchio M. Excessive caloricexpenditure as a cause of malnutrition in patients with cancel.Surg Gynecol Obslel 1980; ISO: 229-34.
14. Arbeit JM, Lees DE, Corsey R, Brennan MF. Resting energyexpenditure in controls and cancel patients with localized anddiffuse disease. Ann Surg 1984; 199: 292-8.
15. Legaspi A, Jeevanandam M, Starnes HF, Brennan MF. Wholebody lipid and energy metabolism in the cancel patient.Melabolism 1987; 10: 958-63.
16. Macfie J, Burkinshaw L, Oxby C, Holmfield JHM, HiIl GL.The effect of gastrointestinal malignancy on resting metabolicexpenditure. Br J Surg 1982; 69: 443-6.
17. Hansell DT, Davies JWL, Burnott JG et al. Does increasingresting energy expenditure cause cancel cachexia? Br J Surg1985; 72: 410 (Abstract).
18. Warnold 1, Lundholm K, Schersten T. Energy balance andbody composition In cancel patients. Cancer Res 1978; 38:1801-7.
19. Hansell DT, Davies JWL, Burns HJG. The relationship betweenresting energy expenditure and weight loss in benign andmalignant disease. Ann Surg 1986; 203: 240-5.
20. Fearon KCH, Hansell DT, Prestan T el al. Innuences ofwholebody protein turnover Tale on resting energy expenditure inpatients with cancel. Cancer Res 1988; 48: 2590-5.
21. Knox L, Crosby LO, Feurer ID et al. Energy expenditure andgynecological cancel. Clin Res 1980; 38: 620A (Abstract).
22. Shaw JHF, Humberstone DM, Wolfe RR. Energy and proteinmetabolism in sarcoma patients. Ann Surg 1988; 207: 283-9.
23. Humberstone DA, Shaw JHF. Metabolism in hematologicmalignancy. Cancer 1988; 62: 1619-24.
24. Shike M, Field R, Evans WK et al. Energy expenditure inrelation to caloric intake in patients with lung carcinoma. J P ENJ Parenler Enteral NUlr 1981; 5: 562 (Abstract).
25. Dempsey DT, Feurer ID, Knox LS et al. Energy expenditurein malnourished gastrointestinal cancel patients. Cancer 1984;53: 1265-73.
26. Garrow JS. Factors affecting energy output. In: Energy BalanceandObesity in Man. Amsterdam: North-Holland, 1974: 125-75.
27. Grande F, Anderson JT, Keys A. Changes of basal metabolicrafe in man in semistarvation and refeeding. J Appl Physiol1958; 12: 230-8.
28. Fearon KCH, Cartel DC. Cancel cachexia. Ann Surg 1988; 208:1-5.
29. Theologides A. Pathogenesis ofcachexia in cancel: a review anda hypothesis. Cancer 1972; 29: 484-8.
30. Theologides A. Cancel cachexia. Cancer 1979; 43: 2004-12.31. Waterhouse C. Lactate metabolism in patients with cancel.
Cancer 1974; 33: 66-71.32. Lundholm K, Edstrom S, Karlberg I el al. Glucose turnover,
gluconeogenesis from glycerol, and estimation of net glucosecycling in cancel patients. Cancer 1982; SO: 1142-50.
33. Heber D, Byerly LO, Chlebowski RT et al. Medicalabnormalities in the cancel patient. Cancer 1985; 55: 225-9.
34. Shaw JHF, Wolfe RR. Energy and protein metabolism in sepsisand trauma. Ausl NZ J Surg 1987; 57; 41-7.
35. Kokal W A, McCullough A, Weight PO, Johnston IDA. Glucoseturnover and recycling in colorectal carcinoma. Ann Surg 1983;198: 146-50.
36. Chlebowski RT, Heber D. Metabolic abnormalities in cancelpatients: carbohydrate metabolismo Surg Clin Norlh Am 1986;66: 957-68.
37. Holroyde CP, Gabuzda TG, Putnam RC et al. Altered glucosemetabolism in metastatic carcinoma. Cancer Res 1975; 35:3710-14.
38. Holroyde CP, Reichard GA. Carbohydrate metabolism incancel cachexia. Cancer Treal Rep 1981; 65(SuppI5): 55-9.
39. Long CL, Spenser JL, Kinney JM, Geiger JW. Carbohydratemetabolism in normal man and effect of glucose infusion. J ApplPh}'sioI1971; 31: 102-9.
40. Warburg O. The Melaholism o/ Turnours. New York: RichardF. Smith, 1930.
41. Block JB. Lactic acidosis in malignancy and observations onits possible pathogenesis. Ann NY Acad Sci 1974; 230: 94-102.
42. Waterhouse C, Jeanpetre N, Keilson J. Gluconeogenesis from
Metabolic effects of cancer: R. G. Douglas and J. H. F. Shaw
lipoprotein lipase activity in patients with malignancy associatedweight loss. Horm Metab Res 1986; 18: 698-703.
73. Waterhouse C. Oxidation and metabolic interconversion inmalignant cachexia. Cancer Treat Rep 1981 ;6S(SuppI5): 61-6.
74. Costa G, Lyles K, Ulrich L. EfTect of human and experimentalcancer on the conversion of J4C-tripalmitin to 14C02. Cancer1976; 38: 1259-65.
75. Waterhouse C, Kemperman lH. Carbohydrate metabolism insubjects with cancer. Cancer Res 1971; 31: 1273-8.
76. Watkin DM. Depression of the total body respiratory quotientin human malignant disease. J Clin Invest 1957; 36: 934(Abstract).
77. Koea lB, Humberstone DA, Shaw lHF. The efTect of stage ofdisease on the metabolic response to cancer. (in preparation)
78. Heber D, Cheblowski RT, Ishibushi DE er al. Abnormalities inglucose and protein metabolism in non-cachectic lung cancerpatients. Cancer Res 1982; 42: 4815-19.
79. Kien CL, Camilla BM. Increased whole-body protein turnoverin sick children with newly diagnosed leukaemia or Iymphoma.Cancer Res 1983; 43: 5586-92.
80. Kien CL, Camilla BM. Close association of accelerated Talesofwhole body protein turnover (synthesis and breakdown) andenergy expenditure in children with newly diagnosed acuteIymphatic leukaemia. JPEN J Paren ter Enteral Nurr 1987; 11:129-34.
81. Norton lA, Stein TP, Brennan MF. Whole body proteinsynthesis and turnover in normal man and malnourishedpatients with and without known cantero Ann Surg 1981; 194:123-8.
82. Hermann VM, Garnick MB, Moore FD er al. Effect of cytotoxicagents on protein kinetics in patients with metastatic canteroSurgery 1981; 90: 381-7.
83. Eden E, Ekman L, Lindmark L er al. Whole-body tyrosine fluxin relation to energy expenditure in weight-Iosing cancerpatients. Merabolism 1984; 33: 1020-7.
84. Carmichael MJ, Clague MB, Kier MJ, Johnston IDA. Wholebody protein turnover, synthesis and breakdown in patientswith colorectal carcinoma. Br J Surg 1980; 67: 736-69.
85. Humberstone DA, Douglas RG, Shaw JHF. Deranged tissuemetabolism as the basis of cancer cachexia. Aust NZ J Surg1989; S9: 276 (Abstract).
86. Rose D, Horowitz GD, Jeevanandam M, Brennan MF,Shives GT, Lowry SF. Whole body protein kinetics during acutestarvation and intravenous refeeding in normal mano Fed Frac1983; 42: 1070.
87. Jeevanandam M. Horowitz GD, Lowry SF, Brennan MF.Cancer cachexia and protein metabolismo Lancet 1984; i:1423-6.
88. Waterhouse C, Mason J. Leucine metabolism in patients withmalignant disease. Cancer 1981; 48: 939-44.
89. Reeds PJ, Fuller MF, Nicholson BA. Metabolic basis of energyexpenditure with particular reference to protein. In: Garrow JS,Halliday D (eds). Subsrrate and Energy Merabolism in Man.London: John Libbey, 1985: 46-57.
90. Waterlow JC. Nutrition and protein turnover in mano Br MedBu111981; 37: 5-10.
91. Brennan MF, Burt ME. Nitrogen metabolism in cancerpatients.Cancer Trear Rep 1981; 6S (Suppl 5): 67-78.
92. Reilly OJ, Goodgame lT, 10nes DC er al. DNA synthesis in ratsarcoma and liver: the efTect of starvation. J Surg Res 1977; 22:281-6.
93. Lowry SF, Goodgame IR, Norton lA er al. EfTect of chronicprotein malnutrition on host-tumour composition and growth.Surg Forum 1977; 23: 143-5.
94. Glass RE, Fern EB, Garlick PJ. Whole-body protein turnoverbefore and after resection of colorectal tumours. Clin Sci 1983;64: 101-8.
95. Waterlow JC, Garlick PJ, Mi1Iward DJ. Prorein Turnover in;\1ammalian Tissues and in rhe Body. Amsterdam: North-Holland,1978.
96. Lundholm K, Bylund AC, Holm 1 er al. Skeletal musclemetabolism in patients with malignant tumours. Eur J Cancer1976; 12: 465-73.Lundholm K, Bennegard K, Eden E er al. Effiux of 3methylhistidine from the leg in cancer patients who experienceweight loss. Cancer Res 1982; 42: 4807-11.
98. Heymslield SR, Mcmanus CS. Tissue components of weight lossin cancer patients: a new method of study and preliminaryobservations. Cancer 1985; SS: 238-49.
99. Steinfeld lL. 1311 albumin degradation in patients with
alanine in patients with progressive malignant disease. CancerRes 1979; 39: 1969-72.
43. Burt ME, Brennan MF. Nutritional support ofthe patient withesophageal cancer. Semin Onco11984; 11: 127-35.
44. Gutman A, Thilo E, Biren S. Enzymes of gluconeogenesis intumour-bearing rats. Isr J Med Sci 1969; 5: 998-1001.
45. Hammond KD, Balinsky D. Activities of key gluconeogenicenzymes and glycogen synthase in rat and human livers andhepatoma cell cultures. Cancer Res 1978; 38: 1317-22.
46. Cori CF. Mammalian carbohydrate metabolismo Physiol Rev1931; 11: 143-275.
47. Burt ME, Lowry SF, Gorschborth C el al. Metabolic alterationsin a non-cachectic animal tumour system. Cancer 1981; 47:2138-46.
48. Reichard GA, Mour NF, Hochella NJ, Patterson AZ,Weinhouse S. Quantitative estimation of the Cori cycle in manoJ Biol Chem 1963; 23: 495-501.
49. Holroyde CP, Axelrod RS, Skutches CL el al. Lactatemetabolism in metastatic colo-rectal cancer. Cancer Res 1979;39: 4900-4.
50. Eden E, Edstrom S, Bennegard K el al. Glucose flux in relationto energy expenditure in malnourished patients withand withoutcancer during periods of fasting and feeding. Cancer Res 1984;44: 1717-24.
51. Burt ME, Aoki TT, Gorschboth CM, Brennan MF. Peripheraltissue metabolism in cancer-bearing mano Ann Surg 1983; 198:685-91.
52. Gold J. Tumour glycolysis-host gluconeogenesis in cancercachexia. Arch Surg 1987; 122: 850.
53. Young VR. Energy metabolism and requirements in the cancerpatient. Cancer Res 1977; 37: 2336-47.
54. Marks PA, Bishop JS. The glucose metabolism ofpatients withmalignant disease and normal subjects as studied by means ofan intravenous glucose tolerance test. J Clin Invesl 1956; 35:254--60.
55. Lawson DH, Richmond A, Nixon DW el al. Metabolicapproaches tocancercachexia. Ann Rev Nulr 1982;2: 277-301.
56. Schein P, Kisner D, Haller D el al. Cachexia of malignancy:potential rol e ofinsulin in nutritional management. Cancer 1979;43: 207(}-6.
57. Jasani B, Donaldson U, Ratcliffe JG, Sakhi GS. Mechanism ofimpaired glucose tolerance in patients with neoplasia. Br JCancer 1978; 38: 287-392.
58. Lundholm K, Holm G, Schersten T. Insulin resistance inpatients with cancer. Cancer Res 1978; 38: 4665-70.
59. Brennan MF. Supportive care of the cancer patient. InDeVita VT, Hellman S, Rosenburg SA (eds). Principies andPraclice o/ Oncology. Philadelphia: JB Lippincott, 1982:1628-39.
60. Norton JA, Burt ME, Brennan MF. In vivo utilization ofsubstrate by human sarcoma-bearing limbs. Cancer 1980; 45:2934-9.
61. Gorden P, Hendricks CM, Kahn CR el al. Hypoglycaemiaassociated with non-islet cell tumor and insulin-like growthfactors:a studyoftumortypes. N EnglJ Med 1981; 305: 1452-7.
62. Kahn CR. The riddle of tumor hypoglycemia revisited. ClinEndocrinol Melab 1980; 9: 335-60.
63. Holroyde CP, Myers RN, Smink RD, Putnam RC, Paul P,Reichard GA. Metabolic response to total parenteral nutritionin cancer patients. Cancer Res 1977; 37: 3109-14.
64. Lundholm K, Edstrom S, Ekman L. A comparative study ofthe influence of malignant tumour on host metabolism in miceand mano Cancer 1978; 42: 453-61.
65. Axelrod L, Costa G. Contribution of fat loss to weight loss incancer. Nulr Cancer 1980; 2: 81-3.
66. Costa G. Cachexia, the metabolic component of metastaticdisease. Cancer Res 1977; 37: 2327-35.Cohn SH, Gartenhaus W, Vartsky D el al. Body compositionand dietary intake in neoplastic disease. Am J Clin Nulr 1981;34: 1997-2004.
68. Lundholm K. Body compositional changes in cancer patients.Surg Clin Norlh Am 1986; 66: 1013-24.
69. Costa G, Bewley P, Aragon M el al. Anorexia and weight lossincancer patients. Cancer Treal Rep 1981 ; 65(Suppl 5): 13-17.
70. Edmonston JH. Fatty acid mobilization in cancer patients.Cancer 1966; ]9: 277-80.
71. Dilman VM, Berstein LM, Ostrumova MN el al. Peculiaritiesof hyperlipidaemia in tumour patients. pr J Cancer 1981; 43:637-43.
72. Vlassara H, Spiegel RJ, Doval DS el al. Reduced plasma
~~~~~~~
67
~~
97
~~
253

Metabolic effects of cancer: R. G. Douglas and J. H. F. Shaw
parenteral nutrition: a meta-analysis. Ann ¡nI Med 1987; 107:195-203.
124. Heatley RV, Williams RHP, Lewis MH. Preoperativeintravenous feeding: a controlled clinical trial. Poslgrad Med J1979; 55: 541-5.
125. Muller JM, Dienst D, Brenner U et al. Preoperative parenteralfeeding in patients with gastrointestinal carcinoma. Lancel 1982;i: 68-72.
126. Chlebowski RT, Grosvenor M. Scrooc M et al. Infiuence ofhydranne sulphate on food intake and weight maintenance inpatients with cancer. Frac Am Sor C/in Onco11985; 4: C-I029(Abstract).
127. Tchekmed)ian NW, Tait N, Moody M et al. High dosemegestrol acetate: a possib]e treatment for cachexia. JAMA1987; 257: 1195-8.
128. Schein PS, Kisner D, HaUer D. Cachexia of malignancy:potentiaJ Tole ofinsulin in nutritional management. Cancer 1979;43: 2070-4.
129. Muggia-Sullam M, Chance WT, Chen MH el al. Insulin reversesanorexia and biochemical changes in tumour-bearing rats. SurgForunl 1984; 35: 66-9.
130. Moley JF, Morrison SD, Norton JA. Insulin reversal of cancercachexia in rats. Cancer Res 1985; 45: 4925-31.
131. Chance WT, Cao L, Fischer lE. Insulin and acivicin improvehost nutrition and prevent tumour growth during totalparenteral nutrition. Ann Surg 1988; 208: 524-31.
132. Fenttinger LD, Mider GB. Energy and nitrogen metabolism incancer. Adv Cancer Res 1954; 2: 229-52.
133. Morrison SD. Control of food intake in cancer cachexia: achallenge and a tool. Ph)'siol Behav 1976; 17: 705-14.
134. Nakuhara W, Fukuoka F. Toxohormone. Jpn J Med 1948; 1:271-7.
135. Liebelt RA, Gehring G, Delmonte L el al. Paraneoplasticsyndromes in experimental animal model systems. Ann NY AcadSci 1974; 230: 547-64.
136. Douglas RG, Shaw JHF. Metabolic response to sepsis andtrauma. Br J Surg 1989; 76: 115-22.
137. Beutler B, Milsark IW, Cerami AC. Passive immunizationagainst cachectin/tumour necrosis factor protects mice fromlethal elTects ofendotoxin. Science 1985; 229: 869-71.
138. Beutler B, Greenwald D, Hulmes JD el al. Identity of tumournecrosis factor and the macrophage secreted factor cachectin.Nalure 1985; 316: 552-4.
139. Beutler B, Cerami A. Cachectin: more iban a tumour necrosisfactor. N Engl J Med 1987; 316: 379-85.
140. Michie HR, Sherman ML, Spriggs DR, Rounds J, Christie M,Wilmore DW. Chronic TNF infusion causes anorexia but notaccelerated nitrogen loss. Ann Surg 1989; 209: 19-24.
141. Shaw JHF, Wolfe RR. An integrated analysis of glucose, fat andprotein metabolism in severely traumatized patients: studies inthe basa] state and the response to intravenous nutrition. AnnSurg 1989; 207: 63-72.
142. Shaw JHF, Wolfe RR. Determination of glucose turnover andoxidation in normal volunteers and septic patients using stableand radio isotopes: theresponse to glucose infusion and totalparenteral nutrition. AuSI ,VZ J Surg 1986; 56: 785-91.
143. BJack PR, Brooks DC, Bessey PQ, Wolfe RR, Wilmore DW.Mechanisms of insulin resistance following injury. Ann Surg1982; 196: 420-9.
144. Frayn KN. Substrate turnover after injury. Br Med Bu111985;41: 232-9.
145. Cahill GF. Starvation in mano N Engl J Med 1970; 282: 668-75.146. Stoner HB, Little RA, Frayn KN, Elebute AE, Tresaderm l,
Gross E. The elTect of sepsis on the oxidation of carbohydrateand fato Br J Surg 1983; 70: 32-5.
147. Birkhan RH, Long CL, Fitkin D, Dyger JW, BJakemore WS.ElTects of major skeletal trauma on whole body protein turnoverin man measured by l-[l4C]leucine. Surgery 1980; 80: 294-9.
148. Long CL. Energy balance and carbohydrate metabolism ininfection and sepsis. Am J Clin NUlr 1977; 30: 301-10.
c neoplastic diseases. Cancer 1960; 13: 974-83.100. Waldman T, Trier J, Fallon H. Albumin metabolism in patients
with Iymphoma. J Clin lnvest 1963; 42: 171-8.101. Humberstone DA, Douglas RG, Shaw JHF. Leucine kinetics
in patients with benign disease, non weight losing cancer andcancer cachexia: studies at the whole body and 1issue level.Surgery (in press).
102. Copeland EM 111, MacFayden BY, Dudrick STo Intravenoushyperalimentation in cancer patients. J Surg Res 1974; 16:241-7.
103. Brennan MF. Total parenteral nutrition in the cancer patient.N Engl J Med 1981; 305: 375-82.
104. Cameron IL. EfTects oficial parenteral nutrition on tumour-hostresponses in rats. Cancer Treat Rep 1981; 65(Suppl 5): 93-9.
105. Fried RC, Mullen J, Stein TP el al. The efTects of glucose andamino acids on tumour and host DNA synthesis. J Surg Res1985; 39: 461-9.
106. Grube BJ, Gamelli RL, F oster RS. Refeeding difTerentially afTectstumourand hostcell proliferation.J Surg Res 1985;339: 535-42.
107. Rumley TO, Copeland EM 111. Intravenous hyperalimentationas nutritional support for the cancer patient; an update. J SurgOnco11985; 30: 164-73.
108. Mullen JL, Buzby GP, Gertner MH et al. Protein synthesisdynamics in human gastrointestinal malignancies. Surgery 1980;87: 331-8.
109. Landel AM, Hammond WG, Meguid MM. Aspects of aminoacid and protein metabolism in cancer-bearing states. Cancer1985; 55: 230-7.
110. Dempsey DT, Mullen JL. Macronutrient requirements in themalnourished cancer patient. How much oíwhat and why?Cancer 1985; 55: 290--4. '
111. Lindmark L, Eden E, Ternell M el al. Thermic efTect andsubstrate oxidation in response to intravenous nutrition incancer patients who lose weight. Ann Surg 1986; 204: 628-36.
112. Buzby GP, Mullen JL, Stein TP el al. Host tumour interactionand nutrient supply. Cancer 1980; 45: 1246-52.
113. Hak LJ, Raasch RH, Hammer VB, Mathes T, Sandler RS,Heizer WD. Comparison ofintravenous glucose and fat calorieson host and tumour growth. JPEN J Paren ter Enteral Nutr1984; 8: 657-9.
114. Shaw JHF, Holdaway CM. Protein sparing efTect of substrateinfusion in surgical patients is governed by the clinical state, andnot by the individual substrate infused. J P EN J Paren ter Enteral ~
Nutr 1988; 12: 433-40.115. Nixon D, Rudman D, Heymsfield S, Ansley J, Kutner M.
Abnorrnal hyperalimentation response in cachectic cancerpatients. Frac Am Assoc Cancer Res Am Soc Clin Onco/1979;20: 173 (Abstract).
116. Bozzetti F, Migliavacca S, Papa A, Ammatuna M el al. Totalparenteral nutrition prevents further nutritional deteriorationin patients with cancer cachexia. Ann Surg 1987; 205: 138-43.
117. Shaw JHF. Influence of stress, depletion, and/or malignantdisease on the responsiveness of surgical patients to totalparenteral nutrition. Am J Clin Nutr 1988; 48: 144-7.
118. Meguid MM, Landel A, Lo CC et al. Branched-chain aminoacid solutions enhance N accretion in postoperative cancerpatients. In: Blackburn G, Grant J, Young VR (eds). AminoAcids: Metabolism and Medical Application. Boston: JohnWright PSG, 1983: 421-7.
119. Kurzer M, Meguid MM. Cancer and protein metabolismo SurgClin North Am 1986; 66: 969-1001.
120. Hunter DC, Weintraub M, Blackburn GL, Bistrian BR.Branched chain amino acids as the protein component ofparenteral nutrition in cancer cachexia. Br J Surg 1989; 76:149-53.
121. Holter AR, Fisher JE. The efTects of perioperative hyper-alimentation on complications in patients with cancer andweight loss. J Surg Res 1977; 13: 31-4.
122. Moghissi K, Hernshaw J, Teasedale PR et al. Parenteralnutrition in carcinoma of the oesophagus treated by surgery:nitrogen balance and clinical studies. BrJ Surg 1977;64: 125-8.
123. Detsky AS, Baker JP, O'Rourke K, Goel V. Perioperative Paper accepted 22 September 1989
Br. J. Surg.. Vol. 77. No. 3. March 1990


















