Meta-Analysis of the AXP and Sepax Automated Cord Blood...
8
Meta-Analysis of the AXP® and Sepax ® Automated Cord Blood Processing Systems CHRISTY KIM, MINDY WILKE-DOUGLAS, AND MITCHEL SIVILOTTI TM META-ANALYSIS OF THE AXP® AND SEPAX® AUTOMATED CORD BLOOD PROCESSING SYSTEMS
Transcript of Meta-Analysis of the AXP and Sepax Automated Cord Blood...

Meta-Analysis of the AXP®and Sepax®Automated Cord Blood Processing Systems
CHRISTY KIM, MINDY WILKE-DOUGLAS, AND MITCHEL SIVILOTTI
TM
META-ANALYSIS OF THE AXP® AND SEPAX®
AUTOMATED CORD BLOOD PROCESSING SYSTEMS

TM
META-ANALYSIS OF THE AXP® AND SEPAX®
AUTOMATED CORD BLOOD PROCESSING SYSTEMS
Automation is the key to standardizing cord blood processing. The AutoXpress® Platform (Thermogenesis®) available from CESCA™ Therapeutics Inc. and the Sepax® (Biosafe® SA) system both provide automated cord blood (CB) processing systems in a functionally closed environment to ensure safety and sterility. Both processing systems address manual processing limitations such as technician dependent variability and inefficiencies with respect to processing time and cost. Automation is the key to standardizing CB processing to ensure efficient, reliable, and reproducible high quality cord blood units (CBUs) without compromising the consistency of stem and progenitor cell viability and potency.
In our recent paper, “Automated Cord Blood Processing: A Follow-up to the Pilar Solves’ Study Comparing the AXP® vs Sepax® Cord Blood Processing Systems,”1 we evaluated both systems looking at stem cell recoveries and red blood cell (RBC) depletion performance based on published studies.2-5 We concluded that the AXP system exhibits superior performance for volume reduction of CBUs because it provides consistently high stem cell recoveries while delivering reliably low RBC contamination without the addition of hydroxyethyl starch (HES), thereby minimizing the risks and complications associated with this additive.41-45
To further evaluate the performance of the systems and to determine if our previous findings were supported by the available literature, we conducted a comprehensive literature search of all documented studies published by cord blood banks around the world. A meta-analysis was performed from all published data (journals, posters, and abstracts) obtained in order to increase the statistical power and effect size of our former conclusions over individual studies. Thus, the results from this study may be generalized to not just one bank but to all banks using these processing methods.
Introduction
Methods
Based on our search, we found 32 references, representing various public and private cord blood banks and institutions ranging from 2001-2015.2-33 The most published automated systems, the AXP system without HES and the Sepax system with and without HES, were compared to each other and to the manual processing method (if data was provided). Studies were further narrowed to only those providing stem cell recoveries reported as mononuclear cell (MNC) and CD34+ cell recoveries and RBC depletion percentages (Table 1).2-28 Giving value to the breadth of the different studies
included, MNC and CD34+ percentages and RBC reduction were recorded for each method regardless of CB age (24-48 hrs) and mean processing volume (45-140 mL) with a maximum final volume of 25 ml. The sample size (n) for each study was weighted by multiplying each value with the n; if the n was not given, the value was excluded from the final analysis. The summation of the values for the stem cell recoveries (MNC and CD34+) and RBC reduction percentages were then divided by the total N to achieve an average value per N across all studies (Table 1).
2015
0526
PROPERT Y OF CESCA THERAPEUTICS, INC. ©2015 | 380118 [A] PAGE 2 OF 8

TM
META-ANALYSIS OF THE AXP® AND SEPAX®
AUTOMATED CORD BLOOD PROCESSING SYSTEMS
Results and Discussion
Table 1. Meta-Analysis of the AXP system without HES and the Sepax system with and without HES compared to manual CB processing.
Cord Blood BankCB Age
Max (hr)
Mean Processing Volume (mL) Study Details n Parameter
AXP System Sepax System ManualRef. #without
HES SD without HES SD with
HES SD with HES SD
Institute for Transplantation Diagnostics and Cell Therapeutics,
Germany48 84.6 29 mL CPD, cell count was not
sufficient for banking MNC 63.0 14.6 52.2 14.8 12
Jose Carreras Cord Blood BankSepax S100 1056 MNC 86.9
20Sepax II 100 MNC 86.4
London Cord Blood Bank, UK Sepax 1156 MNC 93.4 12.8 21New York Blood Center, USA 28 93.4 23 MNC 97.9 4.9 10
CBR, San Bruno, CA USA 36 85.3 100-300g 10 MNC 99.3 6Saint Louis Cord Blood Bank 48 >45 35 ml CPD , TNC> 9.0x108 10 MNC 90.5 84.0 85.5 9
Dusseldorf Cord Blood Bank TNC mean =1.1x109 1520 (Sepax); 7415 (manual) MNC 84.5 7.6 82.0 9.5 19
Anthony Nolan , UK 117+ 26.9 Sepax1 333 MNC 80.8 14.2 22Hellenic Cord Blood Bank, Athens,
Greece 24(39.2-40.2)x2 21ml CPD, 8ml CPD for flush-
ing in satellite bag, 4C128 MNC 79.9
11140.4 106 MNC 62.8
Seoul National University 20 MNC 89.2 5.0 72.6 7.6 67.9 13.5 8
CBR, San Bruno, CA USA 48 72.9 mean age 23.59hr, mean TNC 9.94x108, 40-130mL 1414 MNC 98.7 7
New York Blood Center, USA 108 6336 MNC 92.7 27New York Blood Center, USA 11012 MNC 95.0 28
University of Texas M.D. Anderson Cancer Center, Houston, TX, USA 50-100 4 MNC 59.0 73.0 13
Japanese Red Cross Tokyo Blood Centre 24 28ml CPD, >10x108 TNCs,
n=24 (split from same CB) 24 MNC 97.3 11.2 87.8 12.6 2
Gasthuisberg University Hospital Leuven, Leuven, Belgium 750 MNC 87.7 9.7 79.1 8.9 23
Friedrich-Alexander University, Erlangen, Germany 20 20 MNC 77.9 15.7 74.7 30.7 24
Friedrich-Alexander University, Erlangen, Germany 36
75.60 + 15.56 (manual) ; 75.55 + 10.00(Sepax)
>60 mL
2-6C, WBC>5x108; Sepax CS-510 20 MNC 77.4 27.8 78.1 14.9 5
Jose Carreras Cord Blood Bank Sepax II 16 CD34+ 90.0 20London Cord Blood Bank, UK Sepax 1156 CD34+ 90.9 11.8 21
Newcastle Centre for Cord Blood, United Kingdom 24 98.7 >40mL 15(Sepax);
19(Manual) CD34+ 73.9 16.9 56.5 22.0 15
Etablissement Francais du Sang Aquitaine-Limousin Bordeaux,
France103.1 Sepax CS-530 19 CD34+ 90.2 22.0 14
New York Blood Center, USA 28 93.4 23 CD34+ 98.2 8.0 10New York Blood Center, USA CD34+ 95.0 18.0 25
Geneva University Hospital and Basel University Hospital 36 98-133 11-14x107 TNC CD34+ 81.0 13.0 16
Dusseldorf Cord Blood Bank TNC mean =1.1x109 1520 (Sepax); 7415 (manual) CD34+ 95.0 5.0 95.0 5.0 19
Besancon Cord Blood Bank, Be-sancon, France >80 CD34+>2x106, 14-20C 213 (Sepax);
447(Manual) CD34+ 86.0 11.6 81.5 9.1 3
Cord-Blood Bank Basel, CH110 Sepax 1 195 CD34+ 82.6
17116 Sepax 2; After 2011, minimal
TNC 150x107 110 CD34+ 84.8
Anthony Nolan , UK 117+ 26.9 Sepax1 333 CD34+ 88.2 21.2 22Hellenic Cord Blood Bank, Athens,
Greece 24(39.2-40.2)x2 21ml CPD, 8ml CPD for flush-
ing in satellite bag, 4C128 CD34+ 87.4
11140.4 106 CD34+ 68.6
New York Blood Center, USA 108 6336 CD34+ 97.0 27
Cord Blood Bank, Transfusion Centre, Valencia, Spain 48 108.28 + 23.29 (AXP) ;
114.95 + 24.44 (Sepax)
4C; TNC > 120-140x107 (Sepax); TNC > 100-120x107
(AXP);
670 (Sepax); 1000 (AXP) CD34+ 99.1 29.8 102.2 28.1 4
Japanese Red Cross Tokyo Blood Centre 24 28ml CPD, >10x108 TNCs,
n=24 (split from same CB) 24 CD34+ 93.4 12.0 86.7 12.6 2
Friedrich-Alexander University, Erlangen, Germany 20 20 CD34+ 87.1 28.0 85.7 15.1 24
Friedrich-Alexander University, Erlangen, Germany 36
75.60 + 15.56 (manual) ; 75.55 + 10.00(Sepax)
>60 mL
2-6C, WBC>5x108; Sepax CS-510 20 CD34+ 83.6 32.5 77.0 17.6 5
2015
0526
PROPERT Y OF CESCA THERAPEUTICS, INC. ©2015 | 380118[A] PAGE 3 OF 8

TM
META-ANALYSIS OF THE AXP® AND SEPAX®
AUTOMATED CORD BLOOD PROCESSING SYSTEMS
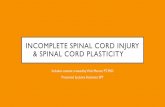
Data from the meta-analysis shows that the AXP system, when used without HES, outperforms the Sepax system (with or without HES) for cord blood processing as follows: average MNC/N: 94.5% vs 86.7% and average CD34+/N: 97.3% vs 92.3% as summarized in Figure 1 (A and B). These results are in agreement with our previous comparison between Takanashi et al. and Zingsem et al. in which the AXP without HES delivers higher recoveries of MNCs and CD34+ cells than the Sepax.1 However, the results here extend our previous finding by revealing that the AXP outperforms the Sepax system irrespective of HES.
Since total nucleated cell counts (TNCs) underestimate the ability and capacity of stem and progenitor cells by including RBCs, granulocytes, and other cell impurities, we selectively analyzed MNCs and CD34+ stem cell recoveries because these are more reliable parameters for potency.28,33 MNCs include hematopoietic stem and progenitor cells at different stages of maturation, as well as lymphocytes, monocytes, and macrophages that better reflect the quality
Results and Discussion (continued)
Table 1. (continued)
and potency of the CBU than TNCs. This is further evident in that the AXP system can be used with HES to achieve 20% higher TNC recoveries while maintaining consistently high CD34+ recoveries regardless if HES is omitted or added.25 Although the use of the colony-forming unit (CFU) assay is the gold standard for testing potency, the CD34+ cell count is known to correlate with time to engraftment and transplant related mortality (TRM) and does not require 2 weeks of culture.28,34,35
Not only are stem and progenitor cell recoveries critical in generating a potent CBU, but equally important and often overlooked is the opposing effect of RBC contamination. The results from this meta-analysis show that the AXP system when used without HES, is comparable to the Sepax system with HES, as noted in previously.1 In addition, the AXP system without HES provides for superior RBC reduction when compared to the Sepax system when used with or without HES (average RBC reduction %/N=87.5% vs 81.6%, respectively). While both automated systems
Cord Blood BankCB Age
Max (hr)
Mean Processing Volume (mL) Study Details n Parameter
AXP System Sepax System ManualRef. #without
HES SD without HES SD with
HES SD with HES SD
Jose Carreras Cord Blood Bank Sepax II 100 RBC Reduc-tion 68.9 20
London Cord Blood Bank, UK Sepax 1156 RBC Reduc-tion 83.1 10.0 21
Etablissement Francais du Sang Aquitaine-Limousin Bordeaux,
France103.1 Sepax CS-530 19 RBC Reduc-
tion 63.2 9.0 43.2 7.4 14
New York Blood Center, USA 28 93.4 23 RBC Reduc-tion 70.2 2.6 10
New York Blood Center, USA RBC Reduc-tion 69.4 2.0 25
Geneva University Hospital and Basel University Hospital 36 98-133 11-14x107 TNC RBC Reduc-
tion 75.0 16
Anthony Nolan , UK 117+ 26.9 Sepax1 333 RBC Reduc-tion 62.6 10.2 22
Barcelona Cord Blood Bank 82 RBC Reduc-tion 88.0 26
Cord Blood Bank, Transfusion Centre, Valencia, Spain 48 104.8-108.2 4C;CD34+ > 30x105 (AXP) ;
TNC > 50-100x107 (Manual)92 (Manual);
492 (AXP)RBC Reduc-
tion 86.8 4.7 86.1 5.8 18
Cord Blood Bank, Transfusion Centre, Valencia, Spain 48 108.28 + 23.29 (AXP) ;
114.95 + 24.44 (Sepax)
4C; TNC > 120-140x107 (Sepax); TNC > 100-120x107
(AXP);
670 (Sepax); 1000 (AXP)
RBC Reduc-tion 88.3 5.6 88.3 7.9 4
Japanese Red Cross Tokyo Blood Centre 24 28ml CPD, >10x108 TNCs,
n=24 (split from same CB) 24 RBC Reduc-tion 84.8 4.2 80.7 4.5 2
Gasthuisberg University Hospital Leuven, Leuven, Belgium 750 RBC Reduc-
tion 83.2 7.8 76.7 6.7 23
Friedrich-Alexander University, Erlangen, Germany 36
75.60 + 15.56 (manual) ; 75.55 + 10.00(Sepax)
>60 mL
2-6C, WBC>5x108; Sepax CS-510 20 RBC Reduc-
tion 47.5 9.1 76.7 10.2 5
PAGE 4 OF 8 2015
0526
PROPERT Y OF CESCA THERAPEUTICS, INC. ©2015 | 380118[A]

TM
META-ANALYSIS OF THE AXP® AND SEPAX®
AUTOMATED CORD BLOOD PROCESSING SYSTEMS
Results and Discussion (continued)
surpass manual processing (77.1%) (Figure 1C), whether differences in CB product regarding RBC content result in a therapeutic difference remains to be determined. In particular, CB RBCs are less osmotically tolerant than adult RBCs and are therefore even more sensitive to post-thaw swelling after cryopreservation;36 this poses the risk
94.5
86.7 81.7
50 55 60 65 70 75 80 85 90 95
100
AXP without HES N=18849
SEPAX with HES N=5179
MANUAL N=8263
% R
ecov
erie
s
Average MNC Recovery %/N
87.5
81.6 77.1
50
55
65
70
75
80
85
90
95
100
N=1539 SEPAX with HES
N=3110 MANUAL
N=905
% R
ecov
erie
s
Average RBC Reduction %/N
97.3 92.3 94.1
50 55 60 65 70 75 80 85 90 95
100
AXP without HES N=7383
SEPAX with HES N=4501
MANUAL N=7945
% R
ecov
erie
s
Average CD34+ Cell Recovery %/N
87.5
81.6 77.1
50
55
60
65
70
75
80
85
90
95
100
AXP without HES N=1539
SEPAX with HES N=3110
MANUAL N=905
% R
ecov
erie
s
Average RBC Reduction %/N
of hemolysis-induced cellular damage to the carefully processed and stored CBUs. High concentrations of RBCs have been shown to negatively affect stem cell viability and functionality in both CB27,37,38 and bone marrow (BM)39 via secreted inhibitory factors.
Figure 1. (A,B) Average stem cell recovery % per N (MNC and CD34+) and (C) average RBC reduction % per N for AXP without HES and Sepax with HES compared to manual CB processing across all studies with recorded n. *Statistical significance via a two-tailed Student’s t-test was further confirmed with all the data sets reporting standard deviations from Table 1 for all three parameters (MNC, CD34+, and RBC reduction) comparing the AXP to the SEPAX (p<0.0001) and to manual processing (p<0.0001).
A B
C
PROPERT Y OF CESCA THERAPEUTICS, INC. ©2015 | 380118[A] PAGE 5 OF 8 2015
0526

TM
META-ANALYSIS OF THE AXP® AND SEPAX®
AUTOMATED CORD BLOOD PROCESSING SYSTEMS
The results of our comprehensive meta-analysis demonstrate that the AXP system is a superior automated CB processing system that outperforms not only manual CB processing but also other automated technologies such as the Sepax system, including the Sepax 2 which uses the same core technology with modified external design, user interface, and software.40 Further studies using Sepax 2 confirm that there is no statistical difference between Sepax 2 and Sepax 1 for stem cell recoveries (MNC and CD34+) because they use the same technology.17,20,22 Although there have been noted volume discrepancies in the Sepax 2 vs the Sepax 1 due to enhanced sensitivity of available Sepax 2 protocols, the resulting product is at the expense of an unacceptable level (63.1+5.7%) of hematocrit in a 20 ml volume sample.22 Therefore, the conclusions based on this meta-analysis are relevant to the AXP system and all current Sepax systems.
When we consider the advancements in cord blood processing, we have crossed milestones in time, cost, efficiency, and quality. The AXP system is a FDA-cleared, functionally closed automated system with technologies that allow for greater throughput by reducing processing time. It can be easily and cost effectively scaled up to run 6 devices at a time in one centrifuge and does not require HES for efficient stem cell recoveries and RBC depletion, eliminating the additional risks associated with HES.41-45
The disparity between current global CBU inventories and physician selection criteria of CBUs for hematopoietic stem cell transplantation remains a major concern impacting CB banking sustainability.46,47 The ever increasing demands for higher TNC requirements call into question the value of the current CBUs banked, particularly in comparison to increasing competition from other cell sources in the wake of improving patient conditioning regimens and
Summary
immune suppression (i.e. haploidentical). It is well known that TNC homing and viability are negatively affected by RBC contamination and yet, it is not a banking requirement to report RBC levels.27,37-39 The further reduction of RBCs is possible using current technology at the risk of also reducing TNC numbers, however, we are left to ponder whether or not “ultra-low” RBC CBUs would perform better than their high RBC (and higher TNC) counterparts. The answer to this question may never be answered due to the maturity and inertia surrounding the drive for high TNCs. Additionally, we should also call into question the current standards for determining cell viability. When reported/registered pre-cryopreservation, methods such as PI and 7AAD do not reliably quantify functionally viable and actively metabolizing cells; dye penetration methodologies do not adequately assess more subtle damage leading to irreversible apoptosis.33,47 Although the selection of CBUs for transplantation is by convention linked with high TNCs, more relevant parameters like MNCs and CD34+ cells better predict time to engraftment and TRM than TNCs.28,33-
35 Why, then, does the CB banking industry continue to place such high value on TNC numbers when assessing CBUs, inextricably dismissing the significance of the true predictors of transplant outcomes and encouraging the faulty selection of CBUs for transplantation? The education of prospective parents and transplant centers to select based on MNCs and CD34+ cells may be the only way to encourage a change in the banking industry to adjust their registering parameters to those that will better reflect the true potential of the CBU. To advance the field of CB transplantation, quality standards relative to viable and functional stem and progenitor cells and not just empty counts must be continually pursued and improved in order to guarantee the safety, purity, potency and consistency of each CBU.
PAGE 6 OF 8 2015
0526
PROPERT Y OF CESCA THERAPEUTICS, INC. ©2015 | 380118[A]

TM
META-ANALYSIS OF THE AXP® AND SEPAX®
AUTOMATED CORD BLOOD PROCESSING SYSTEMS
1. Kim. C., et al. (2015). “Automated Cord Blood Processing: A Follow-up to the Pilar Solves’ Study Comparing the AXP® vs Sepax® Cord Blood Processing Systems.” CESCA Therapeutics White Paper.
2. Takanashi, M., et al. (2010). “Red blood cell depletion of cord blood using an automated System- Evaluation of the AXP System.” Japanese Journal of Transfusion and Cell Therapy 56(1): 62-67.
3. Lapierre, V., et al. (2007). “Cord blood volume reduction using an automated System (Sepax) vs. a semi-automated System (Optipress II) and a manual method (hydroxyethyl starch sedimentation) for routine cord blood banking: a comparative study.” Cytotherapy 9(2): 165-169.
4. Solves, P., et al. (2013). “Qualitative and quantitative cell recovery in umbilical cord blood processed by two automated devices in routine cord blood banking: a comparative study.” Blood Transfus 11(3): 405-411.
5. Zingsem, J., et al. (2003). “Cord blood processing with an automated and functionally closed System.” Transfusion 43(6): 806-813.
6. GE Healthcare Data File 28-4090-31 AD7. Rosenthal, J., et al. “Stem Cell Recovery Following Implementation
of an Automated Cord Blood Processing System in a High Volume Laboratory.” Biology of Blood and Marrow Transplant 2008. 14 (2): 42.
8. Roh, E., et al. “Cord Blood Volume Reduction Using the Automated Devices Sepax(R) S-100 and AXP(TM) AutoXpress Platform. Korean J Blood Transfus.” 2007 Dec 18 (3):219-226. Korean.
9. Henderson, C. et al. “Evaluation of Processing Technologies for Umbilical Cord Blood (UCB).” Saint Louis Cord Blood Bank, SSM Cardinal Glennon Children’s Medical Center.
10. Dobrila L., et al. (2006). “ThermoGenesis AXP AutoXpress Platform and BioArchive System for Automated Cord Blood Banking.” Presented at BMT Tandem Meetings. Honolulu, HI, USA. February 2006.
11. Papassavas, A. C., et al. (2008). “A strategy of splitting individual high volume cord blood units into two half subunits prior to processing increases the recovery of cells and facilitates ex vivo expansion of the infused haematopoietic progenitor cells in adults.” Int J Lab Hematol 30(2): 124-132.
12. Aktas, M., et al. (2010). “Good manufacturing practice-grade production of unrestricted somatic stem cell from fresh cord blood.” Cytotherapy 12(3): 338-348.
13. Sepulveda, C., et al. “Evaluation of an Automated Ficoll Procedure to Enrich for Mononuclear Cells for Use in Clinical Trials.” Blood (ASH Annual Meeting Abstracts) 2007 110: Abstract 1216
14. Dazey, B., et al. (2005). “Cord blood processing by using a standard manual technique and automated closed System “Sepax” (Kit CS-530).” Stem Cells Dev 14(1): 6-10.
15. Basford, C., et al. (2010). “The cord blood separation league table: a comparison of the major clinical grade harvesting techniques for cord blood stem cells.” Int J Stem Cells 3(1): 32-45.
16. Kindler, V., et al. “Evaluation of umbilical cord blood unit processing efficiency in routing laboratory conditions.” EBMT Abstract, 2009.
REFERENCES
17. Lehmann, T., et al. (2012). “The new cord blood processing System, Sepax 2 provides higher recovery of total nuclear counts after volume reduction.” Clinical Hematology. Freitag, 25. Mai 2012, 13:00 - 13:45.
18. Solves, P., et al. (2009). “A new automatic device for routine cord blood banking: critical analysis of different volume reduction methodologies.” Cytotherapy 11(8): 1101-1107.
19. Koerschgen, M., et al. (2007) “Clinical outcome data using unseparated and volume-reduction of cord blood units including an automated system- the Duesseldorf experience.” 33rd Annual Meetign of the European Group for Blood and Marrow Transplantation. Lyon, France.
20. Aktas, M., et al. “Cutting-edge of cord blood banking: experience of the Jose Carreras Cord Blood Bank Dusseldorf with the new cell-separation system Sepax II (Biosafe).” www.eurocord-ed.org. Poster 1: 2008.
21. Armitage, S. (2006). “Cord Blood Processing: Volume Reduction.” Cell Preservation Technology 4(1): 9-16.
22. Naing, M. W., et al. (2015). “Improving umbilical cord blood processing to increase total nucleated cell count yield and reduce cord input wastage by managing the consequences of input variation.” Cytotherapy 17(1): 58-67.
23. Theunissen, K., et al. “Highly efficient and reproducible cord blood banking using the Biosafe Sepax and Coolmix Devices.” 10th Annual Meeting of the International Society of Cellular Therapy. Dublin, Ireland: May 2004.
24. Zingsem, J., et al. (2001). “Processing of Human Umbilical Cord Blood Cells Using an Automated Functionally Closed System.” American Association of Blood Banks, San Antonio.
25. Dobrila L., et al. (2014) “Increasing Post-Processing Total Nucleated Cell (TNC) Recovery in Cord Blood Banking: Hespan Addition in cGMP Environment.” 56th ASH Annual Meeting and Exposition. San Francisco, CA.
26. Querol, S. et al. “An automated and closed procedure for cord blood processing, freezing, and thawing: the Barcelona cord blood bank experience. 30th Annual Meeting of the European Group for Blood and Marrow Transplantation.
27. Rubinstein, P. (2009). “Cord blood banking for clinical transplantation.” Bone Marrow Transplant 44(10): 635-642.
28. Scaradavou, A., et al. “Cord Blood (CB) Unit Mononuclear Cell (MNC) Dose: Effect on Transplantation Outcome and Relevance to Processing Method and CBU Selection. Blood. 2008;112:1969.
29. Li, J., et al. “Automated volume reduction of human cord blood using the AXP AutoXpress Platform: A study with HES.” ISSCR, 2007.
30. Fisk, M., et al. “Umbilical cord blood processing analysis: comparison of methodologies.” 2008-S-16-AATB
31. Karandish, S., et al. “Routine Automated Processing of Cord Blood Units Using the Sepax Cell Processing System.” Blood (ASH Annual Meeting Abstracts) 2006 108: Abstract 3646.
32. Ivolgin, D., et al. “Isolation of nucleated cells fraction from umbilical cord blood- choice of method.” Clinical Researches. Клітинна та органна трансплантологія Том 2, № 1, травень 2014.
PAGE 7 OF 8 2015
0526
PROPERT Y OF CESCA THERAPEUTICS, INC. ©2015 | 380118[A]

CESCA THERAPEUTICS INC.2711 Citrus RoadRancho Cordova, CA 95742USA
33. Patterson, J., et al. (2015). “Detecting primitive hematopoietic stem cells in total nucleated and mononuclear cell fractions from umbilical cord blood segments and units.” J Transl Med 13: 434.
34. Yoo, K. H., et al. (2007). “The impact of post-thaw colony-forming units-granulocyte/macrophage on engraftment following unrelated cord blood transplantation in pediatric recipients.” Bone Marrow Transplant 39(9): 515-521.
35. Purtill, D., et al. (2014). “Dominant unit CD34+ cell dose predicts engraftment after double-unit cord blood transplantation and is influenced by bank practice.” Blood. 124;19:2905-2912.
36. Zhurova, M., et al. (2014). “Osmotic tolerance limits of red blood cells from umbilical cord blood.” Cryobiology 69(1): 48-54.
37. Querol, S., et al. (2002). “Effect of red blood cell content on progenitor function after cryopreservation of cord blood buffycoat products.” Bone Marrow Transplant 29 (Suppl 2): S202(poster 740).
38. Hauck-Dlimi, B., et al. (2014). “The effect of cell concentrations from different cell populations on the viability of umbilical blood stem cells.” Clin Lab 60(10): 1635-1640.
39. Assmus, B., et al. (2010). “Red blood cell contamination of the final cell product impairs the efficacy of autologous bone marrow mononuclear cell therapy.” J Am Coll Cardiol 55(13): 1385-1394.
40. Sepax Cell Separation System and Single-Use Kits, Sepax 2 S-100. BK110022 http://www.fda.gov/BiologicsBloodVaccines/BloodBloodProducts/ApprovedProducts/SubstantiallyEquivalent510kDeviceInformation/ucm278382.
htm 28 Oct 2011.41. Yang, H., et al. (2001). “High-efficiency volume reduction of cord
blood using pentastarch.” Bone Marrow Transplant 27(4): 457-461.
42. Trivedi, S. M., et al. (1984). “Hydroxyethyl starch serum levels in leukapheresis donors measured by modified periodic acid-Schiff staining technique.” Transfusion 24(3): 260-263.
43. Szepfalusi, Z., et al. (1993). “Human monocytes and keratinocytes in culture ingest hydroxyethylstarch.” Arch Dermatol Res 285(3): 144-150.
44. Jurecka, W., et al. (1993). “Hydroxyethylstarch deposits in human skin--a model for pruritus?” Arch Dermatol Res 285(1-2): 13-19.
45. “FDA Safety Communication: Boxed Warning on increased mortality and severe renal injury, and additional warning on risk of bleeding, for use of hydroxyethyl starch solution in some settings.” www.fda.gov/biologicsbloodvaccines/safetyavailability/ucm358271.htm. 25 Nov. 2013
46. Bart, T., et al. (2013). “Impact of selection of cord blood units from the United States and swiss registries on the cost of banking operations.” Transfus Med Hemother 40(1): 14-20.
47. Querol, S., et al. (2010). “Quality rather than quantity: the cord blood bank dilemma.” Bone Marrow Transplantation 45, 970-978.
2015
0526
PROPERT Y OF CESCA THERAPEUTICS, INC. ©2015 | 380118[A]